-
8/11/2019 01 Anterior Pituitary Disijorders (1)
1/9
LCRS: Endocrinology Usama Asif
ENDOCRINOLOGY SESSION 1:
Anterior pituitary disorders
NB: Before we start, most of the functional lectures in this
years endocrinology course are a revision of last
years endocrinology course. Therefore, I will refer heavily to
them in these notes. If there is anything in
this years course that wasnt there last year, then itll be here.
The main things to take away are the
pharmacology lecture. They will contain new information on drugs
and other things
Also, some of these lectures are all over the place, Ive tried
to order them properly, so the information is all
there, just not in the order that the lectures have them in
LECTURE 1:
Hyposecretion of anterior pituitary hormonesPROFESSORJOHN
LAYCOCK([email protected])
Learning objectives
1. Distinguish between primary, secondary and tertiary disease
states relating to pituitary function.
2. Define the term pan-hypopituitarism (Simmonds disease) and
describe the specific aetiology of the
form of hypopituitarism called Sheehans syndrome.
3. Describe the more common signs and symptoms of
pan-hypopituitarism.
4. Describe how a) anatomical pituitary disruption and b)
pituitary hormone deficiency can be evaluated,
including the use of stimulation tests.
5.
Describe how the endocrine consequences of pan-hypopituitarism
can be treated, using the termhormone replacement therapy
6. List the various possible individual pituitary hormone
deficiencies that can occur and explain how the
conditions can be diagnosed and treated (when appropriate).
7. List the principal endocrine causes of short stature,
identifying those that are caused by lack or excess of
specific hormones and those that are related to receptor and
post-receptor defects (e.g. Laron dwarf).
8. State that short stature can also be related to non-endocrine
causes such as malabsorption, malnutrition
and psychological deprivation.
9. Explain how the diagnosis of endocrine-related short stature
can be made, including a description of the
use of standard growth charts and stimulation tests.
10.
Explain why provocative tests are useful in the diagnosis of
pituitary insufficiency. Give examples oftests used to diagnose GH
deficiency.
11.Describe the pharmacodynamic and pharmacokinetic properties
of human growth hormone (hGH) and
explain the rationale governing its use in the treatment of GH
deficiency in (a) children and (b) adults.
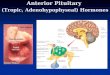
- To the right is an overview of the hypothalamo-
adenohypophysial axis
- Hypopituitarism is the decreased production of all
anterior pituitary hormones(panhypopituitarism), or
the decreased production of specific hormones
-
Panhypopituitarism is very rare and even rarer is itcaused by
congenital defects (such as developmental
defects) and gene mutations(such as in PROP1)
- It can also occur after radiotherapy
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
2/9
LCRS: Endocrinology Usama Asif
- In adults, there is progressivelossof pituitarysecretion,
often(but not invariably) in the following
order:
o Gonadotrophins (LH and FSH)
o GH
o TSH
o
ACTHo (Prolactin deficiency is uncommon)
Simmonds disease
-
The German physician Dr. Morris Simmonds made the first
description of hypopituitarism in
1914
- Simmonds diseaseis insidious (slow) in onset
- It is causedby variousthings, including by not limited to:
o Infiltrativeprocesses(e.g. lymphocytic)
o
Pituitary adenomaso Craniopharyngiomas
o Cranial injury
o Followingsurgery
- Unsurprisingly so, the symptoms are due mainly to decreased
thyroidal, adrenal and gonadal
function
- The result is:
o Secondary amenorrhoeaor oligomenorrhoeain women
o Impotencein men
o Lossof libido
o
Tirednesso Waxy skin
o Lossof body hair
o Hypotension
o Other things to do with a lossof the hormones, etc.
Sheehans syndrome
- Sheehans syndromeis hypopituitarism specificallyin women
- It develops acutely following post-partum haemorrhage, whereby
blood loss and hypovolaemic
shock causes vasoconstrictor spasm of the hypophysial arteries,
leading to ischaemia andsubsequentnecrosisof the pituitarygland
- The pituitary is enlargedduring pregnancy, so this loss of
blood supply is bad
Pituitary apoplexy
- Pituitary apoplexyis also an infarctionor haemorrhageof the
pituitarygland, but in the presence
of a pituitary adenoma
- It has dramatic presentation in patients who have pre-existing
pituitary tumours that suddenly
infarct
-
Many patients can be treated with supportive treatment alone. In
some cases surgicaldecompression can be necessary although
indications for intervention are controversial
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
3/9
LCRS: Endocrinology Usama Asif
Lack in individual hormones, specifically GH
- As we discovered last year, it is possible to have a
deficiency in a single adenohypophysial
hormone, resulting in secondary endocrine glandfailure
-
For example, a lackof gonadotrophins leading to hypogonadismetc.
These lacksare covered in
future lectures- Lack of somatotrophin(GH) in childrenresults in
pituitary dwarfismor short stature
- In adults, the effect of the loss of GH is uncertainbecause by
that point most of the growing is
complete
- Causesof short stature include:
o Genetic determination
o Malnutrition
o Emotional deprivation
o Endocrine disorders see image to
the right:
Laron dwarfismis caused by aGH receptor defect on the
liver, meaning that there is no
responseto any amount of GH
that the body makes
Hypopituitary dwarfism is
when there is a lack of GH
made by the body
A pygmy is when there is an
IGF-I receptor defect so IGF-I
doesnt worko Other various and often unknown causes.
- GH deficiencyin childrencan be congenitalbut this is rare. It
can be due to:
o Deficiencyof hypothalamicGHRH
o Mutationsof the GHgene(very rare)
o Developmentalabnormalities(e.g. aplasiaor hypoplasiaof the
pituitary)
- Acquired GH deficiencyis more common, and can be due to:
o Tumoursof the hypothalamusor pituitary
o Other intracranialtumoursnearby(e.g. opticnerveglioma)
o Secondary to cranial irradiation
o
Head injuryo Infectionor inflammation
o Severe psychosocial deprivation
- It must be remembered that the hormone can only work if the
receptor and post-receptor
mechanisms are working, so it is not always a disorder of
hormone production see above
Tertiary hypopituitarism
o Tertiary hypopituitarisminvolves
specifichypothalamichormonedefects
o For example, Kallmanns syndrome iscaused by a deficiency of
GnRH and leads to
decreased
functioningof the glandsthat produce sex hormoneso Prader-Willi
syndrome is a rare genetic disorder in which seven genes on
chromosome 15 are
deleted or unexpressed on the paternal chromosome. One of the
symptoms manifests itself as
hypogonadism
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
4/9
LCRS: Endocrinology Usama Asif
Diagnosing hypopituitarism
- In order to make a diagnosisof hypopituitarism, one must take
basal plasma valuesof pituitaryor
target endocrine gland hormones
- These are particularly useful if measured after a stimulation
or provocation test, for example
using a combined function test involving rapid IV sequential
administration of GHRH, CRH,
GnRHand TRH- For example, growth hormoneinsufficiencymay be
diagnosedby measuringplasmaGH before
and afterone of the following:
o GHRH (IV)
o Insulin (IV)
o Arginine (IV)
o Exercise (e.g. 10 minute step climbing)
All of the above are meantto stimulate GH production
- The graph shows typical GH responses to insulin in a
normal
subjectand one with GH deficiency
-
For individual hormones, more specific tests can be used
e.g.insulin-induced hypoglycaemia for GH
-
This is known as insulin-induced growth hormone secretion
- Twohoursis the windowneeded to see the GH level response
to administration of insulin
Treating hypopituitarism
- The principalaim of the treatmentof pituitarydeficiency is to
restore homeostasisby replacing
missinghormones
-
An accuratediagnosisis therefore critical- ACTH, TSH and LH/FSH
produce their biological actions largely through stimulating
the
productionof hormonesby the adrenal cortex, thyroidand
gonadsrespectively
- As these hormones (or analogues) are easier to administer than
the pituitary hormones
themselves, they are used in preferencein replacementtherapy
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
5/9
LCRS: Endocrinology Usama Asif
Growth hormone therapy
- Growthhormonetherapyin childrenaccelerateslineargrowthand
decreases body fat
- The effects are most marked in the firstyearof treatmentand
youngerchildrenrespondbetterand
obesechildrenrespond better
-
However, resistancemay developvia antibodyformation
-
If GH deficiency is associated with generalisedhypopituitarism,
then replacement therapywithother hormones will be required
- In growth hormone therapy, the preparation is human
recombinant GH (approved name
somatotropin)
- The administration is a subcutaneous or intramuscular
injection given daily, or 4-5 times per
week, and the doseis adjustedto the patients size
- The absorptionand distributiongives a maximal plasma
concentrationin 2 to 6 hours
- Metabolismis hepaticor renal, and the half-lifeis
short(approximately 20 minutes)
- The duration of action lasts well beyond plasma clearance with
peak IGF-1 levels at
approximately 20 hours
-
The adverseeffectsof growthhormonetherapyinclude:o Lipoatrophyat
the injectionsite
o Intracranialhypertension
o Headaches
o Increasedincidenceof leukaemia
Growth hormone deficiency in adults
- Growth hormone deficiency in adultspresents with various
signsand symptoms. This includes
o Reducedlean mass
o Increasedadiposity
o
Increasedwaistto hip ratioo Reducedmuscle strength/bulk
o Reduced exercise performance
o Decreased plasma HDL-cholesteroland raisedLDL-cholesterol
o Impairedpsychological wellbeing
o Reducedqualityof life
- GH production tends to decreasein peopleover 60
- A diagnosis is made by a lack of responseto the
GHstimulationtest(e.g. to insulin), marked by a
lowplasmaIGF-I andlow plasma IGF-BP3
- The potential benefitsof GH therapy inadultsinclude:
o
Improved body compositiono Improved muscle strength
o Exercise capacity
o Normalisation of HDL-cholesterol
o Increased bone mineral content
o Improved psychological wellbeing and quality of life.
- The potentialrisksof GHtherapyin adultsinclude:
o Increasedriskof cardiovascularaccidents
o Increasedsofttissuegrowth(leading to e.g. cardiomegaly)
o Increasedsusceptibilityto cancer
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
6/9
LCRS: Endocrinology Usama Asif
LECTURE 2:
Hypersecretion of anterior pituitary hormonesPROFESSORJOHN
LAYCOCK([email protected])
Learning objectives
1. Explain why suppression tests are useful in the diagnosis of
excessive pituitary hormone secretion.
How do the GH responses to oral glucose differ in acromegalics
and normal subjects?
2. List the individual pituitary hormone excess states that can
develop, and describe the principal
consequences of each hypersecretory state.
3. Describe the principal signs and symptoms of growth hormone
hypersecretion in the child and the
adult.
4. Describe how gigantism and acromegaly are diagnosed.
5. List the principal treatments available for the treatment of
gigantism and acromegaly.
6.
State that prolactinoma is the most common tumour of the
pituitary gland.7. Describe the principal signs and symptoms of
hyperprolactinaemia.
8. Describe how hyperprolactinaemia is diagnosed.
9. List the principal treatments available for the treatment of
hyperprolactinaemia.
10.Explain why hyperthyroidism, precocious puberty and Cushings
syndrome can be primary, secondary
(or even tertiary) disease states depending on the site of the
lesion.
11.Name two dopamine receptor agonists used in the treatment of
hyperprolactinaemia. Explain the
unwanted effects of these drugs and note their main
pharmacokinetic features.
12.Name a somatostatin analogue used in the treatment of growth
hormone excess and describe its main
biological actions and pharmacokinetic features. List the
potential unwanted effects of these drugs and
identify other conditions in which they may also be
useful.13.State that acromegaly may also be treated with dopamine
receptor agonists.
- Hyperpituitarismis usually due to isolatedpituitarytumoursbut
can also be due to ectopic (i.e.
from non-endocrine tissue) hormone
production
- It can quite oftenbe associatedwith visual
field(namely bitemporal hemianopia)and
other(e.g. cranial nerve) defects, as well as
endocrine-relatedsignsand symptoms
-
The symptoms are associated with theexcess production of the
adenohypophysial
hormones, as covered later on
- Bitemporal (heteronymous) hemianopia
occurs when a pituitary tumour presses
nerves that run through the optic chiasm
(which site above the pituitary), which
leads to the disruption of vision
- Excessof pituitaryhormonescan resultin
a number of differentscenarios. For example:
o
Excess corticotrophin(ACTH) can lead toCushings diseaseo Excess
thyrotrophin(TSH) can lead to thyrotoxicosis
o Excess gonadotrophins(LHand FSH) can lead to
precociouspubertyin children
o Excess prolactincan lead to hyperprolactinaemia
o Excess somatotrophincan lead to gigantismor acromegaly
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
7/9
LCRS: Endocrinology Usama Asif
Hyperprolactinaemia
- Hyperprolactinaemia is caused by excess circulating prolactin
when not due to a physiological
cause such as pregnancyor breast-feeding
-
It is usually due to a prolactinoma(often microadenomasless than
10mm in diameter)
-
In women this results in galactorrhoea (milk production),
secondary amenorrhoea oroligomenorrhoea, lossof libidoand
infertility
- In menthis results in galactorrhoea (uncommonsince appropriate
steroidbackgroundis usually
inadequate), lossof libido, impotenceand infertility
Excess GH gigantism and acromegaly
- Excess somatotrophinin childhoodresults in gigantism, and in
an adultresults in acromegaly
- Gigantismresults in large people. They usually die younger,
due to cardiovascular eventsthough
- Acromegaly is insidious in onset, with signs and symptoms
progressing gradually over many
years; it can remain undiagnosedfor 15-20 years- Untreated,
gigantismand acromegalyare associatedwith an increasedmorbidityand
mortality
due to cardiovascularand/or respiratorycomplications
- Acromegalyinvolves:
o Increased growth of periosteal bonecausing things such as
prognathism(protruding jaw),
overdevleoped supraorbital ridesand soft tissues
o Cartilage, fibroustissue
o Connectivetissue
o Internalorgans(cardiomegaly, splenomegaly, hepatomegaly,
etc.)
- The metaboliceffects of increased GH is a cascadeA
o
An increased plasma insulin response to oral glucose load leads
to increased insulinresistance, resulting in
o an impaired glucose tolerancetest in 50% of patientsand
o diabetes mellitusin 10% of patients
- Acromegalic people commonly clinically manifest with:
o Enlargementof supraorbital ridgesand nose,handsandfeet
o Thickeningof lipsand generalcoarsenessof features
o Excessivesweating
o Mandiblegrowth(leading to protrusionof lower jaw aka
prognathism)
o Carpaltunnelsyndromeand jointpain
o
Barrelchestand curvatureof spine(kyphosis) leading to
respiratorycomplicationso Galactorrhoea
o Menstrualabnormalities
o Decreasedlibidoand impotence
o Hypertension
o Abnormalglucosetolerance
o Symptoms of diabetesmellitus
Diagnosing hyperpituitarism
-
Diagnosis of pituitary hypersecretorystatesuses
suppressiontests- As for pituitary underactivity,
preliminarydiagnosismay be made on the basisof the signsand
symptomsthe patient presents with
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
8/9
LCRS: Endocrinology Usama Asif
- However, a definitivediagnosisrequires
biochemicalmeasurementsof the hormone concerned
- Since hormones are secretedepisodicallyand
the normalrangeis broad, testsfor pituitary
overactivity normally involve measurement
of circulating hormone levels before and
after treatment with an agent that normallycauses suppressionof
hormone release
- For example, acromegaly may be diagnosed
by measuring plasma GH before and after
an oralglucoseloadthis should decrease it,
but in acromegaly, it will not
Treating excess GH
- Treatment options are variable, including somatostatin
analogues such as octreotide and
dopamine agonistssuch as bromocriptine(yes, GH is also inhibited
by dopamine)
-
Other non-drug treatments include trans-sphenoidal surgery,
radiotherapyand chemotherapyforadenomas
- Octreotidecan be used as short-term treatment before pituitary
surgery(trans-sphenoidal), or as
long-term treatmentin those not controlled by othermeans
o As it inhibits GH release, it can also be used to treat other
neuroendocrine tumourse.g.
carcinoidtumours
o Octreotide is administered subcutaneously or intramuscularly 3
times per day, with a
depotpreparationonce GH levelsare undercontrol
o The dose is adjusted accordingto need
o It is distributedby being retainedin the
extracellularfluid
o
Its metabolismis hepatic/renalo It has a half-lifeof 2 to 4
hours
o Unwanted side effects may include GI tract disturbances,
initial reduction in insulin
secretion; transient hyperglycaemia; and in rare cases,
gallstones
Treating hyperprolactinaemia
- Hyperprolactinaemiais treatedusing dopaminereceptoragoniststo
decreaseprolactinsecretion
and reducetumoursize
- Examples of dopamineagonistsinclude bromocriptineand
cabergoline
- Bromocriptineis a D2agonist, administered by mouthonce
daily
o
It is highly plasma protein bound(93%) with a typical
half-lifeof about 7 hourso Hepatic metabolism
o Unwanted effectsof bromocriptineinclude:
Nausea/vomiting/abdominal cramps
Dyskinesias
Psychomotorexcitation
Posturalhypotension
Vasospasmin fingersand toes(caution: Raynauds disease)
o Other uses of bromocriptine include suppression of lactation,
cyclical benign breast
tumours, acromegalyand Parkinsonsdisease
-
Cabergolineis a D2receptor agonistwith moderate D1receptor
activity. It is longer lastingthanbromocriptine, taken orally once
or twice a weekwith a half-lifeof over 45 hours. The unwanted
effectsare thoseof bromocriptine, but lesspronounced
-
8/11/2019 01 Anterior Pituitary Disijorders (1)
9/9
LCRS: Endocrinology Usama Asif
TUTORIAL 1:
Anterior pituitary hormonesPROFESSOR KARIM
MEERAN([email protected])
Case historyA 58-year old woman complaining of frequent
headachesand general tirednesswas seen by her GP. Her
body mass indexwas calculated to be 31 kg/m2. On questioning,
she remarked that she often felt thirsty
and was drinkingmorethan usual. Also, shewas having problemswith
her feet, and had recently bought
some shoeswith an increasedwidthsizeto improvethe comfortof
walking. She could no longer remove
the ring on her finger. She was not aware of any specific
neuromuscular problems other than the
occasional annoying tingling of her fingers and back pain; her
knee reflex was normal. She also
complained of slight lossof peripheral vision in bothher eyes.
The GP had a urinesample analysed for
glucoseand a low positive findingwas made. Perimetry indicated
some loss of peripheral visionin both
eyes. On the basis of the initial findings, the GP arranged for
the woman to visit an endocrineclinicat the
local general hospital. Her consultant there arranged for her to
have a) a glucose tolerance test (GTT), andb) a MRI scan of the
brain. The results of these tests are given below.
a) GTT (after overnight fast)
Time (min) Blood glucose (mmol/l)
0 7.9
30 13.8
60 13.6
90 12.7
120 11.5
GH levels measured at the same time intervals indicated a raised
initial valuewith subsequent values
fluctuatingbut not decreasingmuch despitethe increased blood
glucose concentration.
b) MRI scan: The MRI scan showed evidence of a
pituitarytumourwith suprasellarextensionimpinging
on the optic chiasma.
What might be the first suspicions of the GP relating to
possible diagnosis during the patients visit? Explain your
reasoning, based on the initial history.
First suspicions might have been diabetes due to her being
overweight and thirsty
Or too much GH as she has lateral growth
her feet and hands have gotten biggerHow does the presence of
glucose in the urine fit in with the GPs initial provisional
diagnosis?
Glycosuria is a classic presentation of diabetes insufficient
glucose reabsorption
What other signs and symptoms could be present (if latent) if
the initial diagnosis is correct?
Diabetic neuropathy, retinopathy, nephropathy and other micro-
or macrovascular disease
Which signs and symptoms are explained by the presence of a
suprasellar extension of the pituitary tumour?
Her bitemporal hemianopia
Describe and explain the results of the patients GTT.
Increased glucose and maintained greater than 7.0 = T2DM. Caused
by increased growth hormone in the
body causing increased glucose
What is the diagnosis of thispatients condition?Acromegaly
secondary to a pituitary adenoma secreting excess GH
What treatment(s) would be appropriate?
Surgery, drugs (such as bromocriptine or octreotide, maybe
tumour will shrink?), and radiotherapy are
options