Embed Size (px)
Citation preview
www.APACRS.org
Licensed Publication
APACRS meeting highlights — P. 5, 7, 31Surgical blades — P. 51 OVD cheat sheet — P. 53
Table of Contents P. 4 & P. 6
Feature: Astigmatism
Getting the cornea
into shape — Page 8
Management of
corneal astigmatism — Page 12
Experts on astigmatism
correction — Page 15
Impact of posterior
corneal astigmatism — Page 17
Meeting reporterThe 28th APAO
Congress — Page 55
Vol.9 No.1
March 2013 The Asia-Pacifi c Association of Cataract and Refractive Surgeons
001_COVER_EWAP Mar13_VER 1 No9.indd 1001_COVER_EWAP Mar13_VER 1 No9.indd 1 22/03/2013 08:0922/03/2013 08:09
04,06_Table Of Contents_EW Mar13.indd 2 21/03/2013 13:33

3EWAPMarch 2013 3
Letter from the Guest EditorDear Friends
Cataract surgeons are now, more than ever, aware that preexisting corneal astigmatism needs to be corrected in
order for patients to gain the full visual benefi ts of cataract surgery, especially in those having multifocal or
accommodating intraocular lenses implanted. Just simply correcting the spherical refractive error without
addressing the corneal astigmatism will not deliver the optimal results that our cataract patients demand today. How
many of us at present, as cataract surgeons would be satisfi ed that an unaided vision of 6/12 or 6/9 due to residual
astigmatism is considered a surgical success? I would say none. Our patients would also agree.
Astigmatism has always been diffi cult to treat. Following presbyopia, which remains the most enigmatic and diffi cult refractive error to correct,
astigmatism is the most diffi cult refractive error to treat. This is because astigmatism not only has a magnitude, it also has an axis (direction). It is a vector.
In order to treat astigmatism fully, one has to not only correct the magnitude but also take into account the axis of the astigmatism. In the human eye,
measurements of the magnitude and axis of astigmatism have reached high levels of accuracy and reproducibility, but the treatment of it can be confounded
by issues of visual fi xation and cyclotorsion of the eye from the usual measurement position (seated) to the usual treatment position (reclined) of the patient.
In this issue, we have several excellent articles on the measurement and treatment of astigmatism in cataract patients. There have been huge improvements
in the way we measure astigmatism which have progressed beyond the manual keratometer to multipoint Placido, Scheimpfl ug and wavefront-based
techniques that deliver outstanding accuracy and precision. Intraoperative methods of astigmatism correction have also progressed in leaps and bounds
with limbal relaxing incisions, femtosecond laser arcuate keratotomy and toric IOLs being the preferred methods of intraoperative correction today.
One article of particular signifi cance is on the work of Douglas Koch, MD, and Li Wang, MD, on the role that posterior corneal astigmatism plays in the
surgical management of astigmatism. It provides a lot of illumination on how we should think of the cornea as a structure that has not only a front surface
that we can surgically manipulate, but also a posterior surface that affects the results of our treatment that we cannot manipulate as yet. To me, it does
explain why sometimes we do not get the surgical outcome expected when treating low levels of corneal astigmatism in cataract patients with a toric IOL. I
strongly recommend that interested colleagues read the full paper in the Journal of Cataract & Refractive Surgery referenced in the article. It will change how
you use toric IOLs.
It would appear that we as clinicians and surgeons view astigmatism as an always debilitating optical aberration that must be relentlessly pursued and
corrected to oblivion. Is this always true? I do not think so. I feel that there is a role for small magnitudes of corneal astigmatism in the appropriate axis
that might provide the eye with an IOL an increased depth of fi eld without signifi cant visual degradation and loss of contrast sensitivity. We all remember
cases of patients with pseudoaccommodation demonstrating excellent vision for distance and near before the days of multifocal and accommodating IOLs.
Perhaps we should not always view astigmatism as an evil refractive error. We could harness it to the benefi t of our patients. Food for thought and after
dinner conversation with our colleagues!
Finally, we have several comments from our Asia-Pacifi c surgeons on some of these articles. This gives a very special and unique perspective that is the
hallmark of our publication and I am sure readers will fi nd this edition informative and benefi cial to their clinical practice.
I wish all of our readers and supporters the very best for 2013.
Warmest regards
Chan Wing Kwong, MDGuest Medical Editor and Editorial Board Member, EyeWorld Asia-Pacifi c
EYEWORLD ASIA-PACIFIC EDITORIAL BOARD
CHIEF MEDICAL EDITORGraham BARRETT, Australia
MEMBERS
Abhay VASAVADA, India
ANG Chong Lye, Singapore
CHAN Wing Kwong, Singapore
CHEE Soon Phaik, Singapore
Choun-Ki JOO, Korea
Hiroko BISSEN-MIYAJIMA, Japan
ASIA-PACIFIC CHINA EDITION
Editors-in-ChiefZHAO Jialiang
ZHAO Kan Xing
Deputy EditorHE Shouzhi
Assistant EditorZHOU Qi
ASIA-PACIFIC INDIA EDITION
Regional Managing EditorS. NATARAJAN
ASIA-PACIFIC KOREA EDITION
Regional Editor-in-ChiefHungwon TCHAH
Regional Managing EditorChul Young CHOI
Hungwon TCHAH, Korea
John CHANG, Hong Kong
Johan HUTAURUK, Indonesia
Kimiya SHIMIZU, Japan
Pannet PANGPUTHIPONG, Thailand
Prin ROJANAPONGPUN, Thailand
Ronald YEOH, Singapore
S. NATARAJAN, India
YAO Ke, China
YC LEE, Malaysia
003_Editorial_EWAP Mar13.indd 3003_Editorial_EWAP Mar13.indd 3 22/03/2013 08:1322/03/2013 08:13

March 20134 EWAP TABLE OF CONTENTS
Feature March 2013Astigmatism 8 - 18
Letter from the Guest Editor 3
30
Getting astigmatic cataract patients into corneal shape 8Beefi ng up your astigmatic measurement and treatment routineby Maxine Lipner
Modalities for correcting total corneal astigmatism 12With several now available, surgeons weigh in on the pros and cons of eachby Michelle Dalton
Experts differ on corneal astigmatism correction in cataract surgery 15Total corneal astigmatism correction during cataract surgery could be either by eliminating it or by leaving slight with-the-rule astigmatismby Erin L. Boyle
Posterior corneal astigmatism vital to calculating correct total astigmatism 17Researchers highlight the signifi cance of posterior corneal astigmatism in estimating total corneal astigmatismby Erin L. Boyle
CATARACT/IOL
A new complication after endothelial keratoplasty procedures 19 Opacifi cation, calcifi cation linked to a certain type of IOL materialby Vanessa Caceres
REFRACTIVE
Mysterious infection after LASIK has lessons for all 33A recent case in the Middle East highlighting the need for refractive surgeons to be aware of serious corneal problemsby Matt Young
19
33
38
44
Preventing the Argentinian Flag Sign: Phaco capsulotomy 22 An overview of the phaco capsulotomy technique for preventing complications with white and intumescent cataractsby Christopher C. Teng, MD
Taking the spin out of toric rotation: Part 1 25 A two-part case-based examination of toric IOL rotationby Steven G. Safran, MD
Taking the spin out of toric rotation: Part 2 28 by Steven G. Safran, MD
The business side of femto for cataract 30How to integrate a femtosecond laser into your practice, and when to use itby Michelle Dalton
Presbyond Laser Blended Vision: Another approach to presbyopia 34A laser-based approach that takes advantage of natural mechanisms within the optical systemby Dan Z. Reinstein, MD
A scleral approach to presbyopia 38Procedure in phase III U.S. FDA trial targets plano presbyopesby Vanessa Caceres
Strengthening corneas in Singapore 40Surgeon explains why and how he performs crosslinking during many LASIK proceduresby Matt Young
CORNEA
Cornea surgeons compare thin DSAEK and DMEK as options for endothelial keratoplasty procedures 44 Looking beyond the obviousby Ellen Stodola
Expanding corneal tissue availability 47 Largest cornea clinical trial today compares preservation timeby Vanessa Caceres
DMEK gaining ground on
04,06_Table Of Contents_EW Mar13.indd 4 25/03/2013 17:02

5
g
n
04,06_Table Of Contents_EW Mar13.indd 504,06_Table Of Contents_EW Mar13.indd 5 22/03/2013 17:0022/03/2013 17:00
March 20136 EWAP TABLE OF CONTENTS
APACRS Secretariat11 Third Hospital Avenue, Singapore 168751
Fax: (65) 6327 8630 Email: [email protected]: www.apacrs.org
50 51
51
GLAUCOMA
Can diet influence the risk of glaucoma? 49Studies highlight the relationship between diet and glaucomaby Tony Realini, MD
New technology could improve eye drop delivery 50New delivery system seeks to address need for more effective administration of medicationby Ellen Stodola
DEVICES
Not all blades serve all purposes 51When it comes to choosing instrumentation to make incisions, variables between disposable and reusable blades make a differenceby Michelle Dalton
PHARMA FOCUS
Experts provide OVD cheat sheet 53 Rigging the game to win in challenging cataract casesby Maxine Lipner
NEWS & OPINION
Meeting Reporter 55 Reporting live from the 28th APAO-AIOS Congress
56
55
P U B L I S H I N G S TA F F
Publisher APACRSCharity Wai [email protected]
Donald R. Long
APACRS EditorialKathy [email protected]
Summer [email protected]
Christine ShimmonSenior Staff WriterChiles Aedam R. Samaniego
ASCRS Editorial
EditorJena Passut
Managing EditorStacy Majewics
Senior Staff WriterErin Boyle
Staff WriterEllen Stodola
ProductionGraphic DesignerJulio Guerrero
Production AssistantDaniela Galeano
Contributing EditorsVanessa Caceres – Lakeland, Florida
Michelle Dalton – Reading, Pennsylvania
Rich Daly – Arlington, Virginia
March 2013 Volume 9 • No.1
Enette Ngoei – Singapore
Matt Young – Malaysia
Senior Contributing EditorMaxine Lipner – Nyack, New York
Advertising SalesASCRSMedia
4000 Legato Road
Suite 700, Fairfax, VA 22033
(1-703) 591-2220 • fax: (1-703) [email protected] • www.eyeworld.org
DirectorDonald R. [email protected]
Advertising Sales Manager Jeff [email protected]
(1-703) 788-5745
Paul [email protected]
(1-703) 383-5729
Classifi ed Sales, Production ManagerCathy [email protected]
(1-703) 591-2220
EyeWorld Special Projects and EventsJessica [email protected]
(1-703) 591-2220g
APACRS Publisher: EyeWorld Asia-Pacifi c Edition (ISSN 1793-1835) is published quarterly by the Asia-Pacifi c Association of Cataract & Refractive Surgeons (APACRS), c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, telephone (65) 6322-7469, fax (65) 6327-8630, email [email protected]. Printed in Singapore.
EyeWorld Asia-Pacifi c Chinese Edition (ISSN 1521-7566) is jointly published quarterly by the Asia-Pacifi c Association of Cataract & Refractive Surgeons (APACRS), c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, telephone (65) 6322-7469, fax (65) 6327-8630, email [email protected]; and the Chinese Ophthalmological Society (COS), c/o Chinese Medical Association, 42 Dongsi Xidajie, Beijing 100710, PR China, telephone (86-10) 6524-9989 ext 2456, fax (86-10) 6512-3754. Printed in Beijing, PR China.
Editorial Offi ces: EyeWorld Asia-Pacifi c Edition: Asia-Pacifi c Association of Cataract & Refractive Surgeons (APACRS), c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, telephone (65) 6322-7469, fax (65) 6327-8630, email [email protected].
EyeWorld Asia-Pacifi c Chinese Edition: Chinese Ophthalmological Society (COS), c/o Chinese Medical Association, 42 Dongsi Xidajie, Beijing 100710, PR China; telephone (86-10) 6524-9989 ext 2456; fax (86-10) 6512-3754.
EyeWorld News Service: 4000 Legato Road, Suite 700, Fairfax, VA 22033-4003, USA, toll-free (1-800) 451-1339, telephone(1-703) 591-2220, fax (1-703) 273-2963, email [email protected].
Advertising Offi ces: ASCRSMedia, 4000 Legato Road, Suite 700, Fairfax, VA 22033-4003, USA, telephone (1-703) 591-2220, fax (1-703) 273-2963, email [email protected].
Copyright 2005, Asia-Pacifi c Association of Cataract & Refractive Surgeons (APACRS), c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, telephone (65) 6322-7469, fax (65) 6327-8630, email [email protected].
Licensed through the American Society of Cataract & Refractive Surgery (ASCRS), 4000 Legato Road, Suite 700, Fairfax, VA 22033-4003, USA. All rights reserved. No part of this publication may be reproduced without written permission from the publisher. Letters to the editor and other unsolicited material are assumed intended for publication and are subject to editorial review and acceptance. The ideas and opinions expressed in EyeWorld Asia-Pacifi c do not necessarily refl ect those of the editors, publishers or its advertisers.
Subscriptions: Requests should be addressed to the APACRS publisher, c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, telephone (65) 6322-7469, fax (65) 6327-8630, email [email protected].
Back copies: Subject to availability. Contact the APACRS publisher, c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, telephone (65) 6322-7469, fax (65) 6327-8630, email [email protected].
Requests to reprint, use or republish: Requests to reprint or use material published herein should be made in writing only to the APACRS publisher, c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, telephone (65) 6322-7469, fax (65) 6327-8630, email [email protected].
Change of address: Notice should be sent to the APACRS publisher, c/o Singapore National Eye Centre, 11 Third Hospital Avenue, Singapore 168751, six weeks in advance of effective date. Include old and new addresses and label from a recent issue. The APACRS publisher cannot accept responsibility for undelivered copies.
KDN number: PPS1766/07/2013(022955) MCI (P) 160/02/2013
04,06_Table Of Contents_EW Mar13.indd 6 25/03/2013 18:48
March 2013 EWAP TABLE OF CONTENTS 7
e
04,06_Table Of Contents_EW Mar13.indd 704,06_Table Of Contents_EW Mar13.indd 7 22/03/2013 17:0022/03/2013 17:00
March 20138 EWAP FEATURE
Getting astigmatic cataract patients into corneal shapeby Maxine Lipner Senior EyeWorld Contributing Writer
Beefi ng up your astigmatic measurement and treatment routine
While for decades
practitioners neglected
residual astigmatism
when removing
cataracts, many wouldn’t dream
of it now, according to Stephen
S. Lane, MD, adjunct professor
of ophthalmology, University of
Minnesota, Minneapolis, Minn.,
USA. “The way that I look at
astigmatism in cataract surgery
is the same way I’ve looked at
it my entire career: You would
never want to give patients glasses
without the astigmatism correction
in the glasses,” Dr. Lane said. “So
why with cataract surgery would
we essentially ignore astigmatism
and just treat the spherical
correction?”
Evolving equipmentPractitioners today have
their pick of equipment for
measuring astigmatism. Jack T.
Holladay, MD, clinical professor
of ophthalmology, Baylor College
of Medicine, Houston, Texas, USA,
noted that technology to measure
astigmatism has been evolving
for years, beginning with original
manual keratometers. “Those
devices used a circle and measured
the principal meridians of the
refl ected image,” Dr. Holladay
said. “If the refl ected image was
an oval that meant that you had
astigmatism.” With this method,
usually four points, located
about 3.2 mm apart, were used to
measure the principal radii.
As automated keratometers
emerged, the size of the ring
was reduced, changing the area
that was actually measured.
Since the magnitude and axis of
astigmatism is not always constant
as one moves peripherally from
the center, signifi cant differences
would result. Even today, the
IOLMaster (Carl Zeiss Meditec,
Jena, Germany) measures points
that are 2.5 mm apart on a 44 D
cornea, while the Lenstar (Haag-
Streit, Mason, Ohio, USA) measures
two rings, one with points 1.65
mm apart and the other with
points 2.35 mm apart, and arrives
at an average of the two.
Meanwhile, topographers
would measure a zone from 1-9
mm in diameter. They would
measure thousands of points
within this zone. “That’s when we
began to fi nd with topography that
as you moved out from the center
of the cornea, the magnitude
and axis of astigmatism was not
constant on many patients,” Dr.
Holladay said.
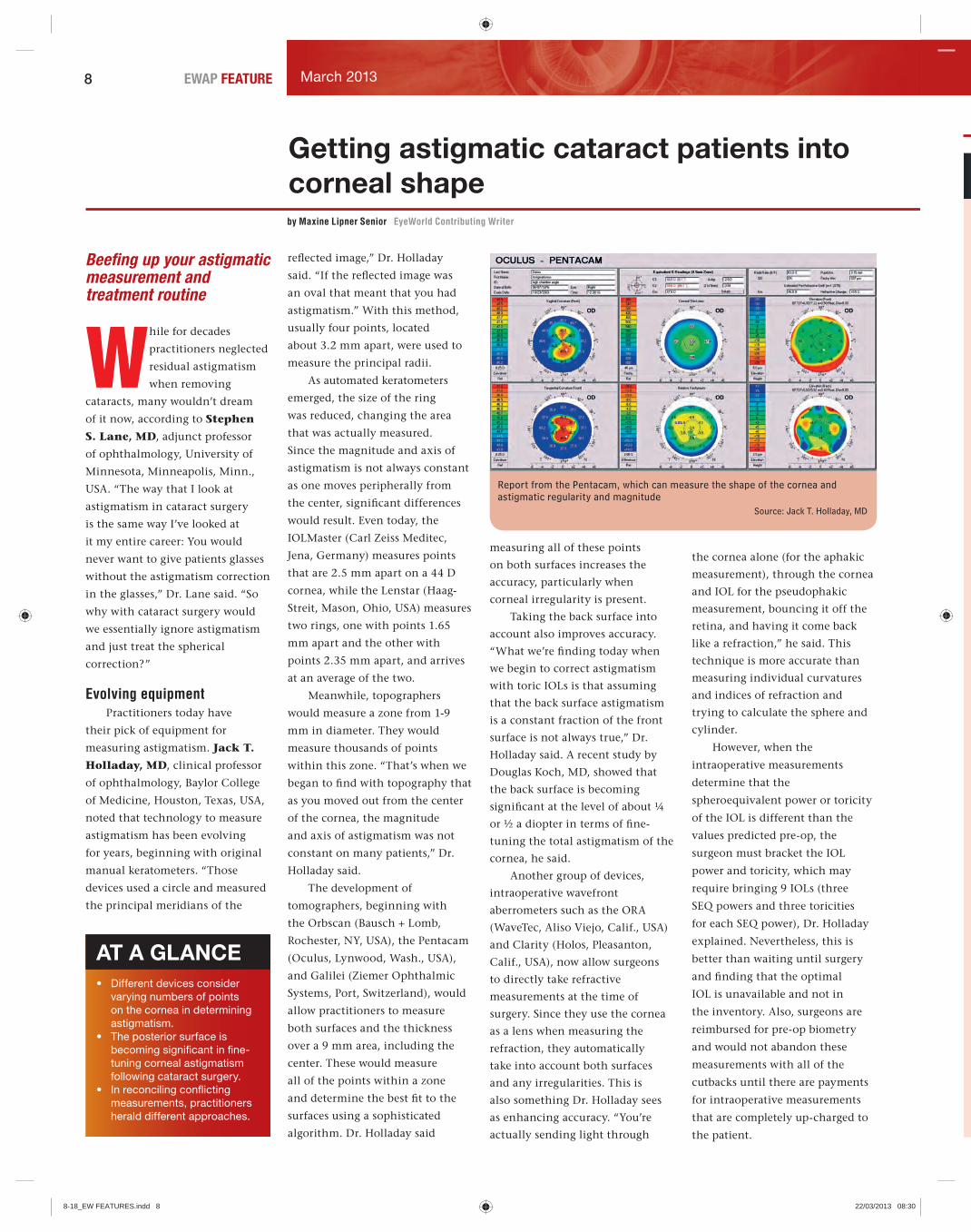
The development of
tomographers, beginning with
the Orbscan (Bausch + Lomb,
Rochester, NY, USA), the Pentacam
(Oculus, Lynwood, Wash., USA),
and Galilei (Ziemer Ophthalmic
Systems, Port, Switzerland), would
allow practitioners to measure
both surfaces and the thickness
over a 9 mm area, including the
center. These would measure
all of the points within a zone
and determine the best fi t to the
surfaces using a sophisticated
algorithm. Dr. Holladay said
measuring all of these points
on both surfaces increases the
accuracy, particularly when
corneal irregularity is present.
Taking the back surface into
account also improves accuracy.
“What we’re fi nding today when
we begin to correct astigmatism
with toric IOLs is that assuming
that the back surface astigmatism
is a constant fraction of the front
surface is not always true,” Dr.
Holladay said. A recent study by
Douglas Koch, MD, showed that
the back surface is becoming
signifi cant at the level of about ¼
or ½ a diopter in terms of fi ne-
tuning the total astigmatism of the
cornea, he said.
Another group of devices,
intraoperative wavefront
aberrometers such as the ORA
(WaveTec, Aliso Viejo, Calif., USA)
and Clarity (Holos, Pleasanton,
Calif., USA), now allow surgeons
to directly take refractive
measurements at the time of
surgery. Since they use the cornea
as a lens when measuring the
refraction, they automatically
take into account both surfaces
and any irregularities. This is
also something Dr. Holladay sees
as enhancing accuracy. “You’re
actually sending light through
the cornea alone (for the aphakic
measurement), through the cornea
and IOL for the pseudophakic
measurement, bouncing it off the
retina, and having it come back
like a refraction,” he said. This
technique is more accurate than
measuring individual curvatures
and indices of refraction and
trying to calculate the sphere and
cylinder.
However, when the
intraoperative measurements
determine that the
spheroequivalent power or toricity
of the IOL is different than the
values predicted pre-op, the
surgeon must bracket the IOL
power and toricity, which may
require bringing 9 IOLs (three
SEQ powers and three toricities
for each SEQ power), Dr. Holladay
explained. Nevertheless, this is
better than waiting until surgery
and fi nding that the optimal
IOL is unavailable and not in
the inventory. Also, surgeons are
reimbursed for pre-op biometry
and would not abandon these
measurements with all of the
cutbacks until there are payments
for intraoperative measurements
that are completely up-charged to
the patient.
AT A GLANCE• Different devices consider
varying numbers of points
on the cornea in determining
astigmatism.
• The posterior surface is
becoming signifi cant in fi ne-
tuning corneal astigmatism
following cataract surgery.
• In reconciling confl icting
measurements, practitioners
herald different approaches.
Report from the Pentacam, which can measure the shape of the cornea and astigmatic regularity and magnitude
Source: Jack T. Holladay, MD
8-18_EW FEATURES.indd 88-18_EW FEATURES.indd 8 22/03/2013 08:3022/03/2013 08:30

March 2013 9EWAP FEATURE
a
y
Views from Asia-Pacifi cArup CHAKRABARTI, MDSenior Consultant, Cataract and Glaucoma Services, Chakrabarti Eye Care CentreNo. 102, Kochulloor, Trivandrum 695011, Kerala, IndiaTel. no. +91-471-2555530Fax no. [email protected]
In this era of refractive cataract surgery, our goal is to reduce the patient’s dependence on glasses in the postoperative period, if not eliminate it altogether. This has come about due to our ability to more accurately
determine IOL power (Optical Biometry: IOLMaster and Lenstar) and to the incorporation of steps to reduce the quantum of postoperative astigmatism. Accurate determination of the preoperative astigmatism, knowledge of the SIA and an appropriate astigmatism reduction strategy play an important role. Preoperative astigmatism is traditionally measured using: 1. Manual keratometry, 2. Automated keratometry, 3. Corneal topography, 4. Optical Biometry. In an ideal situation the K-readings from all the devices will give similar readings, which, unfortunately, is hardly ever the case because devices don’t always measure the same areas of the cornea.
The various methods to reduce postoperative astigmatism in cataract patients have been limbal relaxing incisions, paired opposite clear corneal incisions, toric IOLs and laser. However, toric IOLs have been increasing in popularity for various reasons. Satisfactory results with these lenses require proper work up of preoperative astigmatism, a good surgical technique and proper IOL handling/alignment. Toric IOLs are not used in patients with irregular astigmatism. Topography is a tool that may detect astigmatic irregularity which may go undetected in conventional keratometry. In case of major disagreement between the various devices it may be a good idea to perhaps not employ a toric IOL after proper explanations to the patient. In case of a minor disagreement, the axis of the astigmatism may be assessed using manual or automated keratometry and the actual magnitude may be taken from topography according to Dr Lane. Some surgeons would like to average the measurements after repeating them to ensure consistency in the values for each device. These devices don’t put due importance to the back surface of the cornea. Dr. Douglas Koch has shown in his recent study that the corneal back surface plays a signifi cant role in terms of “fi ne-tuning the total astigmatism of the corneas”. The back surface is taken into account by tomographers, e.g. Orbscan (Bausch + Lomb), Pentacam (Oculus) and Galilei (Ziemer). These limitations may perhaps be answered by a group of devices—intraoperative wavefront aberrometers such as the ORA (Wavetec) or Clarity (Holos)—which allow surgeons to directly detect accurate refraction including astigmatism at the time of surgery after the cataract is removed. However, the surgeon should be ready with a wider inventory of toric IOLs in case the intraoperative measurements differ from the predicted preoperative values.
The surgeon should also have a clear idea of his SIA and the various factors impacting it to optimize his astigmatic outcomes. Neglect of this component often leads to suboptimal results with toric IOLs.
Intraoperative lens positioning along the proper axis is of paramount importance. The standard technique of marking with ink is considered to be inadequate. The emerging guidance systems play an increasingly important role for proper intraoperative lens placement.Guidance devices such as the SMI (Alcon, Fort Worth, Texas, USA/Hünenberg, Switzerland) take a photograph of the eye and match this intraoperatively so that landmarks are identifi ed, ensuring proper lens positioning.
The bottomline is no single device currently serves all functions with regard to corneal measurements and many believe that intraoperative aberrometry will become the standard of care in the future enabling practitioners to better achieve the target of emmetropia without astigmatism and possibly other higher aberrations such as spherical aberration and coma.
Editors’ note: Dr. Chakrabarti is a consultant for Allergan (Irvine, Calif., USA) but has no fi nancial interests related to his comments.
How devices measure upHow devices measure up
Practitioners today are fortunate to have a variety of devices for measuring astigmatism at the ready. Here’s what’s available:
Manual keratometry determines the quantity of astigmatism and the axis, according to Dr. Trattler. “It’s good for planning cataract surgery, but it doesn’t help us to fi gure out whether the cornea is regular or irregular,” he said.
The IOLMaster considers corneal shape, using three measurements for astigmatism. “It’s a very rudimentary method, but it’s very accurate as far as helping us plan for the right intraocular lens power,” Dr. Trattler said. This will tell if astigmatism is present, how steep the cornea is, and help with surgical planning but will not identify irregular astigmatism.
Corneal topography uses imaging technology to get a sense of the magnitude of the astigmatism and the shape of the cornea, Dr. Trattler explained. It can tell if the cornea is regular or irregular and if the patient has a condition such as keratoconus.
The Pentacam measures the shape of the cornea and the magnitude and regularity of the astigmatism. “You press it back and can determine the shape of the cornea and if there’s any regularity or irregularity,” Dr. Trattler said.
The Galilei gives measurements for both anterior and posterior corneal curvatures. This can be helpful in considering what posterior astigmatism contributes, which has gained importance thanks to Dr. Koch’s new nomogram for implanting toric IOLs, which uses both measurements, Dr. Trattler explained.
The Clarity and the ORA offer intraoperative wavefront measurements of astigmatism. These allow practitioners during surgery to measure the cornea through the power of the astigmatism. “It helps you to fi ne-tune your planning,” Dr. Trattler said.
Devices such as the iDesign (Abbott Medical Optics, AMO, Santa Ana, Calif., USA), the iTrace (Tracey Technologies, Houston, Texas, USA), and the OPD (Marco, Jacksonville, Fla., USA) can analyze a combination of topography and wavefront measurements at the same time. These units can give corneal shape and also determine whether the astigmatism is symmetrical or asymmetrical.
Optimizing outcomesHow can practitioners best
use devices to optimize results for
astigmatic cataract patients?
Dr. Lane stressed that
it’s important to begin by
distinguishing lenticular from
corneal astigmatism. “Obviously
the astigmatism associated with
the lens will be absent following
the removal of the cataract,” he
said. “So you need to have an idea
of what the post-operative corneal
astigmatism will be.”
He fi nds that’s best
accomplished pre-op with the aid
of different available tools. “Some
of them are automated like the
measurements that you would
take with an IOLMaster or with
the Lenstar,” he said. “Some of
them have been around for many
decades like manual keratometry,
and some of them are looked at
in terms of corneal topography or
even OCT.”
Intraoperatively, Dr. Lane sees
systems such as the ORA and the
Holos as serving an important
function. “With the WaveTec
aberrometry and in the future with
Clarity aberrometry, that will help
us to determine what the amount
of astigmatism is after we’ve
removed the cataract on the table,
real-time,” he said.
He also stressed the importance
of using a guidance system
for proper intraoperative lens
placement. “We have guidance
systems because with astigmatism
not only is there an amount,
there’s also a direction,” he said.
“So you can choose the correct
power implant, but if you put it
in the wrong position you’ll be
inaccurate in your correction of
the astigmatism.” Guidance devices
such as the SMI (Alcon, Fort
Worth, Texas, USA/Hünenberg,
Switzerland) take a photograph
of the eye and match this
continued on page 10
8-18_EW FEATURES.indd 98-18_EW FEATURES.indd 9 22/03/2013 08:3022/03/2013 08:30

10 March 2013EWAP FEATURE
Views from Asia-Pacifi cTim ROBERTS, MBBS, MMed, FRANZCO, FRACSConsultant Ophthalmologist and Clinical Senior Lecturer, Department of Ophthalmology, Royal North Shore Hospital, University of SydneyConsultant Eye Surgeon, Vision Eye InstituteLevel 3 270 Victoria Ave, Chatswood,Sydney, Australia 2067 Tel. no. +61-2-9424-9999Fax no. +61-2-9415-4220 [email protected]
After myopia and hypermetropia, astigmatism remains the major optical aberration causing reduced vision. A signifi cant number of patients presenting for cataract surgery have coexisting astigmatism, which if left uncorrected, is likely to result in reduced postoperative visual quality.1 Assessing cataract surgery success by only looking at best-corrected
visual acuity or spherical equivalent targets will result in suboptimal refractive outcomes and dissatisfi ed patients. Improvements in cataract surgery and intraocular lenses (IOLs), combined with a generational change in patient expectations, have resulted in a paradigm shift with spectacle independence now regarded by most ophthalmologists and patients as the expected and desired outcome following surgery.
Accurately measuring preoperative keratometric cylinder and planning for spherical and astigmatic emmetropia should be the target for all patients when removing cataracts. Various techniques have been used in combination with non-toric IOLs to reduce or eliminate astigmatism; however, these techniques have been limited by induced higher-order aberrations, the amount of astigmatism that can be treated and the long-term mechanical stability of the cornea following relaxing incisions. Options to treat astigmatism include incision placement on the steep corneal meridian, paired opposite clear corneal incisions, corneal relaxing incisions and laser refractive surgery.
The availability of toric IOLs based on widely used non-toric IOL platforms, combined with improved rotational stability, has made toric IOLs a viable option for many surgeons. They produce accurate and predictable refractive results and do not require additional expensive instrumentation or special surgical skills and training.
The construction of a circular, consistently-sized capsulorhexis which overlaps the IOL throughout 360° is important in maximizing IOL stability and reducing the onset of posterior capsular opacifi cation.2 The recent introduction of femtosecond lasers to cataract surgery has shown promising results with reports of greater precision and accuracy of the anterior capsulotomy and more stable and predictable positioning of the intraocular lens.3,4,5 The FS laser can also create extremely accurate corneal incisions for both the main wound and astigmatic relaxing incisions in the steep corneal meridian.
Key factors in achieving successful results with toric IOLs are thorough education of offi ce, anesthetic and nursing staff, proper patient selection, accurate measurement of corneal cylinder, and accurate IOL alignment intraoperatively. The cardinal meridians are marked on the cornea with the patient in the upright position prior to commencing surgery. These reference marks can be made with commercial instruments or by the surgeon aligning the horizontal meridian with the horizon. Correct alignment of the toric IOL axis can be confi rmed under the operating microscope by using a fi xation ring (Mendez marker, Mastel Inc., Rapid City, SD, USA) after wound hydration and reformation of the anterior chamber.
Key Points• After myopia and hypermetropia, astigmatism remains the major optical aberration causing reduced vision• A signifi cant number of patients presenting for cataract surgery have coexisting astigmatism, which if left uncorrected, is likely to result in reduced postoperative visual quality• Best-corrected visual acuity and spherical equivalent refraction should not be used as indicators of good refractive outcomes• Calculations should not be based on the subjective refraction as progressive lenticular astigmatism may either mask corneal astigmatism or give a falsely high estimate of cylinder• Manual and automated keratometry measurements are reliable with comparable results• Topography should be performed if astigmatism >1.5 D to exclude corneal pathology
References
1. Ferrer-Blasco T, Montés-Micó R, Peixoto-de-Matos SC, Gonzá-les-Méijome JM, Cerviño A. prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35:70-75.2. Ravalico G, Tognetto D, Palomba M, et al. Capsulorhexis size and posterior capsule opacifi cation. J Cataract Refract Surg. 1996;22:98-103.3. Kránitz K, Miháltz K, Sándor GL, et al. Intraocular lens tilt and decentration measured By Scheimpfl ug camera following manual or femtosecond laser-created continuous circular capsulotomy. J Refract Surg. 2012;28:259-63.4. Roberts TV, Lawless M, Chan CC, et al. Femtosecond laser cataract surgery: technology and clinical practice. Clin Experiment Ophthalmol. 2012 Jul 12. doi: 10.1111/j.1442-9071.2012.02851.x. [Epub ahead of print]5. Kránitz K, Takacs A, Miháltz K, et al. Femtosecond laser capsulotomy and manual continuous curvilinear capsulorrhexis parameters and their effects on intraocular lens centration. J Refract Surg. 2011;27:558-63.Editors’ note: Dr. Hwang and Prof. Joo have no fi nancial interests related to their comments.
Editors’ note: Dr. Roberts has no fi nancial interests related to his comments.
intraoperatively so that landmarks
are identifi ed, ensuring proper lens
positioning.
Meanwhile, William B. Trattler, MD, director, Cornea,
Center for Excellence in Eye Care,
Miami, Fla., USA, emphasized
the need for topography on all
astigmatic patients. “You need a
topography because you can be
surprised if the astigmatism is
quite irregular,” he said. “It could
be keratoconus or it could be other
irregularities, and unless you use
the topography, you’ll have no
idea.”
This could lead to trouble
in a case in which, for example,
the IOLMaster identifi es 1 D of
astigmatism. If the practitioner
assumes that this is regular and
implants a toric lens, if it turns
out to be irregular that will make
things worse, Dr. Trattler warned.
He uses the IOLMaster on every
patient to help measure the axial
length and determine the right
intraocular lens power, pairing
this with Placido disk topography.
In unusual cases he also employs
the Pentacam, which measures the
shape of the cornea. “They’re very
complementary and can be helpful
in fi guring things out,” Dr. Trattler
said.
Dr. Holladay stressed that
no single device currently serves
all functions. “The topography
wavefront devices don’t measure
the back surface or the thickness
of the cornea, and the tomography
devices measure the front and
the back surface of the cornea but
don’t measure the wavefront,”
he said. “So you don’t get
everything from any one of
them.” What is needed, he thinks,
is a tomographer that measures
wavefront.With no single device available,
this may mean reconciling confl icting measurements. In cases of discrepancies, Dr. Trattler recommended averaging measurements or repeating the tests. Dr. Lane advised trusting your own experience. He pointed out that while manual keratotomy remains the gold standard, accuracy somewhat depends on operator experience. However, with
au
of
re
of
to
th
ty
au
to
us
di
be
ab
st
en
Getting - from page 9
8-18_EW FEATURES.indd 108-18_EW FEATURES.indd 10 22/03/2013 08:3022/03/2013 08:30

11March 2013 EWAP FEATURE
s
ns
r
ry
e
y
ul
r
y
,
e,
y
h
automated keratometry, there’s
often greater ability to duplicate
results. For looking at the direction
of the astigmatism, however,
topography tends to be best. “If
there is a lot of disagreement
typically what I’ll do is use
automated or manual keratometry
to determine magnitude and then
use the topography to look at the
direction of the cylinder,” he said.
Going forward, Dr. Holladay
believes that intraoperative
aberrometry will become the
standard of care in the future
enabling practitioners to better
achieve the target of emmetropia
without astigmatism and possibly
other higher aberrations such
as spherical aberration and
coma. Ultimately this will
enable practitioners to put
patients within 1/8 of a diopter
of spheroequivalent target, the
limit of IOLs available in 0.50
D increments, without any
residual astigmatism or higher-
order aberrations. “When we do
that we’ll have a large number
of patients, more than 70%,
that are much better than 20/20
because the studies show that
approximately 90% of the cataract
age group has the neurological and
retinal function that is as good as
the vision as when they were 19
years old,” he said. EWAP
Editors’ note: Dr. Holladay has
fi nancial interests with Alcon, AMO,
WaveTec, and Oculus. Dr. Lane has
fi nancial interests with Alcon and
WaveTec. Dr. Trattler has fi nancial
interests with AMO and Oculus.
Contact information
Holladay: 713-669-8977, [email protected]: 651-275-3000, [email protected]: 305-598-2020, [email protected]
OCULUS Asia Ltd. Hong KongTel. +852 2987 1050 • Fax +852 2987 1090 www.oculus.de • [email protected]
OCULUS Pentacam® HR
The new Belin/Ambrosio Display III:
Unique for Keratoconus and Ectasia Detection Based on Corneal Tomography
Combination of 5 corneal elevation and pachy-metry parameters into one fi nal overall index
for quick visual inspectionfor quick decision makingcomprehensive but intuitive
ONLY available for Pentacam®!
database for hyperopic patientsnovel pachymetric parameter ARTmax
•
•
•
•
•
Views from Asia-Pacifi cYi LU, MDDirector, Department of Ophthalmology, Eye & ENT Hospital of Fudan University83 Fenyang Road, Shanghai 200031, ChinaTel. no. +86-21-64377134-407Fax no. [email protected]
Nowadays, I agree that attention should be paid to astigmatism correction for cataract surgery in a more comprehensive way, such as taking the posterior surface of the cornea into consideration. Actually, for the
eye as a whole, astigmatism, as a lower-order aberration, has a much greater impact on the visual function than higher-order aberrations such as spherical aberration, so that the correction of spherical aberration should be based on the full correction of astigmatism.
To correct astigmatism accurately, precise measurement is the prerequisite. However, regarding the selection of instruments, there is no gold standard for the evaluation of preoperative astigmatism in cataract patients at this moment. Since each instrument possesses its pros and cons, establishing the optimal measuring approach still requires the support of rigorous randomized controlled trials. And these approaches will constantly be improved in subsequent practice. In fact, if simply considering correcting corneal astigmatism in cataract surgery, Pentacam is better than either the OPDscan or IOLMaster because it measures more corneal points, and it can measure both anterior and posterior corneal surfaces, as well as recognize irregular astigmatism and keratoconus; if both astigmatism and spherical aberration are aimed to be corrected during the surgery, devices that can analyze a combination of topography and wavefront measurements at the same time might be a better choice, such as OPDscan. However, as for those intraoperative measuring equipment mentioned in this article, such as the ORA or Clarity, I am worried that although they can provide timely monitoring of astigmatism, they neglect the importance of surgically induced astigmatism (SIA). If the surgical design is based on these data, one would expect error in the fi nal result due to postoperative corneal incision reconstruction.
Therefore, before the gold standard is established, I suggest that every practitioner evaluate his or her personal SIA precisely, and assess preoperative astigmatism carefully using advanced equipment such as the Pentacam in order to establish a rational surgical plan.
Editors’ note: Dr. Lu has no fi nancial interests related to his comments.
8-18_EW FEATURES.indd 118-18_EW FEATURES.indd 11 22/03/2013 08:3022/03/2013 08:30

March 201312 EWAP FEATURE
Modalities for correcting total corneal astigmatismby Michelle Dalton EyeWorld Contributing Writer
With several now available, surgeons weigh in on the pros and cons of each
Visually signifi cant
astigmatism (generally
considered 0.50 D or
greater) affects almost
70% of patients presenting for
cataract surgery, and most patients
expect surgeons to correct the
astigmatism along with the
cataract surgery.
Eric D. Donnenfeld, MD,
partner, Ophthalmic Consultants
of Long Island, Rockville Centre,
NY, USA, and clinical professor
of ophthalmology, NYU Medical
School, New York, NY, USA,
believes that even smaller amounts
of astigmatism—perhaps even less
than 0.5 D—can be signifi cant.
Surgeons need to manage and treat
not only pre-op astigmatism, but
surgically induced astigmatism
(SIA) as well, he said.
“The most common mistake
that I see doctors make on
a routine basis in treating
astigmatism is treating the pre-op
astigmatism and not treating the
SIA,” Dr. Donnenfeld said, but
noted there are two websites in
particular that can help surgeons
determine what IOL to use and
what the SIA is (www.acrysoftoric.
com [Alcon, Fort Worth, Texas,
USA/Hünenberg, Switzerland] for
the former and www.lricalculator.
com [Abbott Medical Optics, AMO,
Santa Ana, Calif., USA] for the
latter).
For Louis D. “Skip”
Nichamin, MD, in private
practice, Laurel Eye Clinic,
Brookville, Pa., USA, limbal
relaxing incisions (LRIs) “work
quite well if you treat them
with respect and pay regard
to the surgical technique and
instrumentation used.” If surgeons
measure the patients’ astigmatism
carefully, plan an equally careful
surgery, and execute the LRI with a
“great deal of precision, the results
can be fabulous,” Dr. Nichamin
said. Although there are “defi nitely
studies out there indicating better
results with a toric lens than with
an LRI,” using a premier diamond
blade and paying exquisite
attention to the execution levels
the fi eld with regard to outcomes,
he said.
Incisional techniquesAdvantages of incisional
keratotomy over other methods of
correcting corneal astigmatism are
its lower cost and ease to perform,
said Richard Tipperman, MD,
attending surgeon, Wills Eye
Institute, Philadelphia, Pa., USA.
“But what you’re really after are
predictability, reproducibility,
AT A GLANCE• 70% of patients presenting
with cataract also have
visually signifi cant
astigmatism.
• LRIs can produce exquisite
results, but surgeons need to
execute them with incredible
precision.
• The variable outcomes with
incisional keratotomy may be
unacceptable.
• Femtosecond lasers can
create arcuate incisions so
precise SIA is minimized.
• Toric IOLs remain the “go-to”
choice for higher levels of
astigmatism.
Views from Asia-Pacifi cJohan A. HUTAURUK, MDDirector, Jakarta Eye CenterJl. Cik Ditiro 46, Menteng, Jakarta – 10310 IndonesiaTel. no. +62-21-2922-1000Fax no. [email protected]
Cataract surgery has now become cataract refractive surgery, because the
target is not only visual rehabilitation by removing the cloudy lens but also
to optimize the visual acuity postoperatively, so our patients can expect to
be free of glasses.
Almost 70% of patients presenting with cataract also have astigmatism, this is a
huge number but fortunately, most of them have less than 1.0 D of astigmatism.
Hoffer reported 23% of eyes exhibited more than 1.5 D of astigmatism in a series
of 7500 patients undergoing cataract surgery and others reported that only 8%
exhibited >2.0 D of corneal astigmatism and 2.6% exhibited >3.0 D. Peripheral
corneal relaxing incisions are still the most cost effective modalities to treat
preexisting astigmatism, and the nice thing about this procedure is that we don’t
have to be so accurate but results will almost always reduce the astigmatism. For
example, most patients with <1.0 D astigmatism can be treated by placing the
phacoemulsifi cation on the steep corneal meridian. This is the simplest method
to take advantage of SIA (surgically induced astigmatism) to neutralize the
preexisting astigmatism.
Limbal relaxing incisions (LRI) are the low-cost approach for correction of corneal
astigmatism between 1 and 3 D, but I still prefer to opt for toric IOLs for better
reliability if the patient can afford premium IOLs. Toric IOLs are easier to adopt
since they do not need any additional procedures other than marking the axis and
rotating the toric lens at the end of surgery.
We are aware that the precision of refractive outcome after cataract surgery is
only half compared with LASIK. Only 45% of cataract surgeries are within 0.5 D of
targeted refraction with current biometry compared with 90% in LASIK. Patients
with high corneal astigmatism of >3 D, which is less than 2.5% of the cataract
population, might benefi t from LASIK touch up to reduce the corneal astigmatism
as well as any residual refractive errors.
In my opinion, the best way to correct corneal astigmatism in cataract patients
is to correct the cause of astigmatism, which is in the cornea, rather than to
compensate it with a toric lens. LRI fi ts with this idea and femtosecond laser
cataract surgery has an added value of creating precise arcuate corneal incisions.
Corneal topography should help to detect asymmetric corneal astigmatism and if
there is an irregular astigmatism then topography guided LASIK would be the best
option.
Editors’ note: Dr. Hutauruk has no fi nancial interests related to his comments.
an
ha
fo
qu
m
th
sa
Ri
LR
ta
2.
in
th
PL
vi
of
sh
ru
sh
18
yo
Bu
an
ef
th
ke
ge
go
to
te
us
th
in
po
su
pe
“g
to
sy
tr
th
to
re
L
Le
co
8-18_EW FEATURES.indd 128-18_EW FEATURES.indd 12 22/03/2013 08:3022/03/2013 08:30
March 2013 13EWAP FEATURE
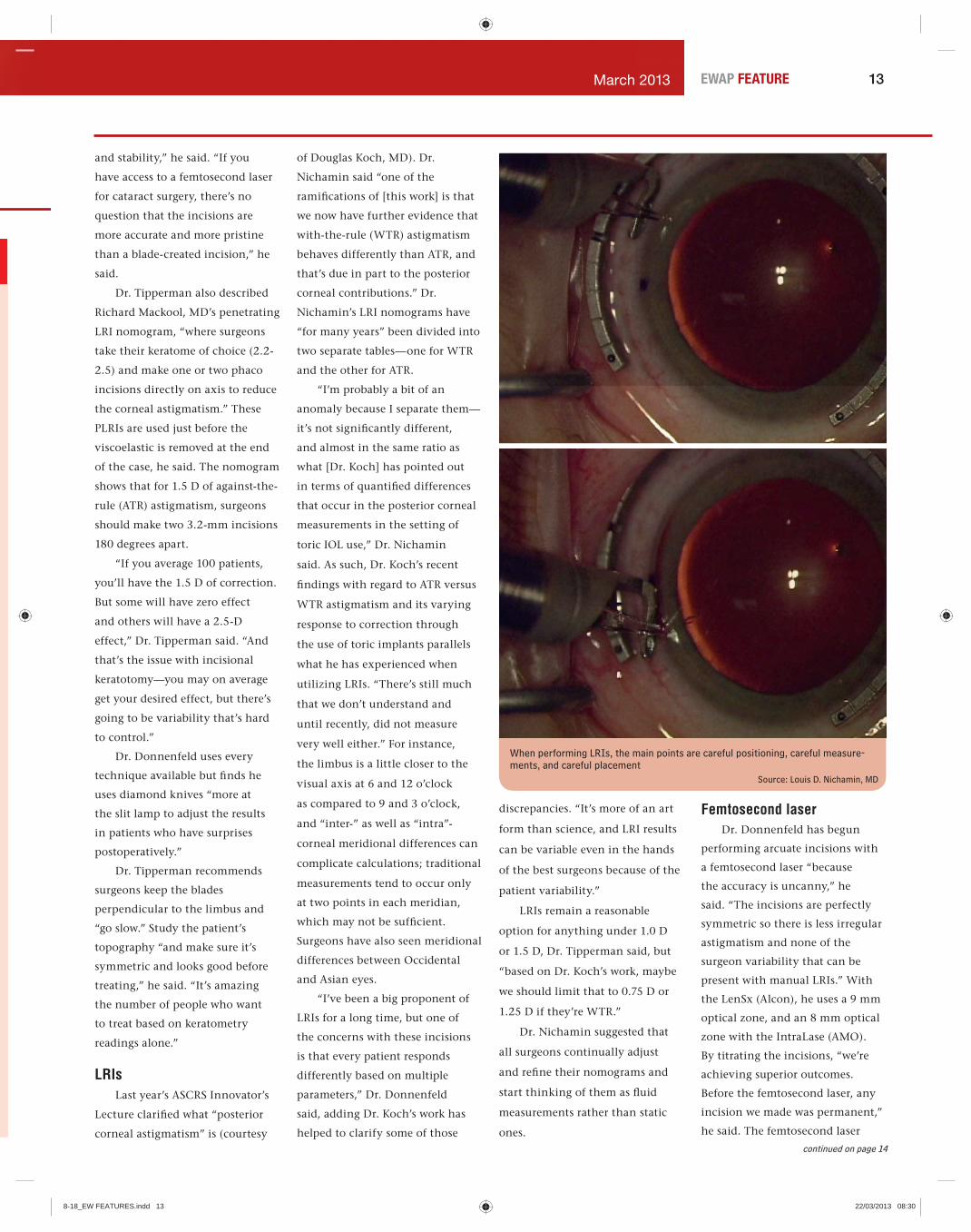
When performing LRIs, the main points are careful positioning, careful measure-ments, and careful placement
Source: Louis D. Nichamin, MD
and stability,” he said. “If you
have access to a femtosecond laser
for cataract surgery, there’s no
question that the incisions are
more accurate and more pristine
than a blade-created incision,” he
said.
Dr. Tipperman also described
Richard Mackool, MD’s penetrating
LRI nomogram, “where surgeons
take their keratome of choice (2.2-
2.5) and make one or two phaco
incisions directly on axis to reduce
the corneal astigmatism.” These
PLRIs are used just before the
viscoelastic is removed at the end
of the case, he said. The nomogram
shows that for 1.5 D of against-the-
rule (ATR) astigmatism, surgeons
should make two 3.2-mm incisions
180 degrees apart.
“If you average 100 patients,
you’ll have the 1.5 D of correction.
But some will have zero effect
and others will have a 2.5-D
effect,” Dr. Tipperman said. “And
that’s the issue with incisional
keratotomy—you may on average
get your desired effect, but there’s
going to be variability that’s hard
to control.”
Dr. Donnenfeld uses every
technique available but fi nds he
uses diamond knives “more at
the slit lamp to adjust the results
in patients who have surprises
postoperatively.”
Dr. Tipperman recommends
surgeons keep the blades
perpendicular to the limbus and
“go slow.” Study the patient’s
topography “and make sure it’s
symmetric and looks good before
treating,” he said. “It’s amazing
the number of people who want
to treat based on keratometry
readings alone.”
LRIsLast year’s ASCRS Innovator’s
Lecture clarifi ed what “posterior
corneal astigmatism” is (courtesy
of Douglas Koch, MD). Dr.
Nichamin said “one of the
ramifi cations of [this work] is that
we now have further evidence that
with-the-rule (WTR) astigmatism
behaves differently than ATR, and
that’s due in part to the posterior
corneal contributions.” Dr.
Nichamin’s LRI nomograms have
“for many years” been divided into
two separate tables—one for WTR
and the other for ATR.
“I’m probably a bit of an
anomaly because I separate them—
it’s not signifi cantly different,
and almost in the same ratio as
what [Dr. Koch] has pointed out
in terms of quantifi ed differences
that occur in the posterior corneal
measurements in the setting of
toric IOL use,” Dr. Nichamin
said. As such, Dr. Koch’s recent
fi ndings with regard to ATR versus
WTR astigmatism and its varying
response to correction through
the use of toric implants parallels
what he has experienced when
utilizing LRIs. “There’s still much
that we don’t understand and
until recently, did not measure
very well either.” For instance,
the limbus is a little closer to the
visual axis at 6 and 12 o’clock
as compared to 9 and 3 o’clock,
and “inter-” as well as “intra”-
corneal meridional differences can
complicate calculations; traditional
measurements tend to occur only
at two points in each meridian,
which may not be suffi cient.
Surgeons have also seen meridional
differences between Occidental
and Asian eyes.
“I’ve been a big proponent of
LRIs for a long time, but one of
the concerns with these incisions
is that every patient responds
differently based on multiple
parameters,” Dr. Donnenfeld
said, adding Dr. Koch’s work has
helped to clarify some of those
discrepancies. “It’s more of an art
form than science, and LRI results
can be variable even in the hands
of the best surgeons because of the
patient variability.”
LRIs remain a reasonable
option for anything under 1.0 D
or 1.5 D, Dr. Tipperman said, but
“based on Dr. Koch’s work, maybe
we should limit that to 0.75 D or
1.25 D if they’re WTR.”
Dr. Nichamin suggested that
all surgeons continually adjust
and refi ne their nomograms and
start thinking of them as fl uid
measurements rather than static
ones.
Femtosecond laserDr. Donnenfeld has begun
performing arcuate incisions with
a femtosecond laser “because
the accuracy is uncanny,” he
said. “The incisions are perfectly
symmetric so there is less irregular
astigmatism and none of the
surgeon variability that can be
present with manual LRIs.” With
the LenSx (Alcon), he uses a 9 mm
optical zone, and an 8 mm optical
zone with the IntraLase (AMO).
By titrating the incisions, “we’re
achieving superior outcomes.
Before the femtosecond laser, any
incision we made was permanent,”
he said. The femtosecond laser
continued on page 14
8-18_EW FEATURES.indd 138-18_EW FEATURES.indd 13 22/03/2013 08:3022/03/2013 08:30
14 March 2013EWAP FEATURE
T
c
s
e
s
m
Cso
al
be
ha
as
ru
cl
Ba
H
go
co
co
a
th
fr
15
“I
is
Modalities - from page 13
*SUPRACOR is CEmarked. SUPRACOR for myopic, emmetropic, and post-LASIK patients is currently in clinical evaluation.
SUPRACOR is NOT approved for use in the US. Technolas Excimer 217P is NOT approved for use in the US. Some of the products and/or specific features as well as the procedures
featured in this document may not be approved in your country and thus may not be available there. Design and specifications are subject to change without prior notice as a result of
ongoing techncal development. Please contact our regional representative regarding individual availability in your respective market.
SURPACOR is a trademark of Bausch & Lomb Incorporated or its affiliate. kbcomunicacion. BLT-007/02-2013
©2013 Bausch & Lomb Incorporated. All rights reserved.
Varifocal excimer treatment for presbyopia
Excellent far, intermediate, and near vision*
Treats a wide range of patients
As simple as a LASIK procedure
Expanding LASIK to the presbyopia market
TECHNOLAS Perfect VisionGmbH –A Bausch + LombCompany
Messerschmittstr. 1+3, Munich, Germany
Regional Office Asia-PacificTechnolas Singapore Pte Ltd
101 Thomson Road, #27-03AUnited Square
Singapore 307591
Tel: +65-6592-0792
www.technolas.com – www.bausch.com
allows surgeons to create the
incision but not fully open it
until deemed necessary, either
intraoperatively or post-op,
allowing the surgeon to adjust the
results.
“You don’t have to open the
incisions at the time of surgery,”
Dr. Tipperman said. “One of the
biggest advantages of the femto
incision is that it’s adjustable and
titratable.” He treats at 9 mm, and
“I use 90% of the nomogram and
about 85% depth.”
Dr. Nichamin has worked
with the LensAR (Orlando, Fla.,
USA) laser and although FDA
approval for relaxing incisions is
still pending, in the laboratory
“we have been able to create near
perfect incisions all the way out to
the limbus in most cases.”
ASCRS is working on
developing nomograms for the
different femtosecond lasers/
arcuate incisions.
Toric IOLsToric IOLs are still the
preferred treatment if patients
have undergone previous refractive
surgery, have higher levels of
astigmatism, or have thin corneas,
Dr. Nichamin said.
“Toric IOLs have been our
game changer in astigmatism
management” because of their
stability and predictability, Dr.
Tipperman said.
“I like toric lenses,” Dr.
Donnenfeld said. “They don’t have
the incisions, they don’t induce dry
eye, and they’re more accurate for
higher amounts of astigmatism.”
He routinely combines arcuate
incisions with toric IOLs and uses
the former as a template for where
to place the lens; he opens the
incisions post-op “if I need to do
any fi ne-tuning.”
Dr. Tipperman suggests
marking at 6 o’clock using a
circular marker and ensuring the
viscoelastic is removed at the end
of the procedure to avoid post-op
rotation.
“For surgeons to achieve
optimal results, they need to be
familiar with all of these treatment
modalities,” Dr. Nichamin said.
“You can’t hang your hat on
just one.” The decision of which
technique to use “is quite complex,
and there’s not one quick, simple
answer. It depends on the surgeon’s
comfort level, what technologies
are readily available, cost, and
perhaps most importantly, specifi c
patient characteristics.” EWAP
Editors’ note: Dr. Donnenfeld has fi nancial interests with Alcon and AMO. Dr. Nichamin has fi nancial
interests with LensAR. Dr. Tipperman has fi nancial interests with Alcon and Marco (Jacksonville, Fla., USA).
Contact informationDonnenfeld: 516-766-2519, [email protected]: 814-849-6547, [email protected]: 484-434-2716, [email protected]
8-18_EW FEATURES.indd 148-18_EW FEATURES.indd 14 22/03/2013 08:3022/03/2013 08:30
15March 2013 EWAP FEATURE
Experts differ on corneal astigmatism correction in cataract surgeryby Erin L. Boyle EyeWorld Senior Staff Writer
Total corneal astigmatism
correction during cataract
surgery could be either by
eliminating it or leaving
slight with-the-rule astig-
matism
Corneal astigmatism
correction in cataract
surgery should achieve
zero residual astigmatism,
some experts say, but there is
also a theory that patients might
benefi t from one quarter to one
half a diopter (D) of with-the-rule
astigmatism because of against-the-
rule drift.
Jack T. Holladay, MD,
clinical professor of ophthalmology,
Baylor College of Medicine,
Houston, Texas, USA, said the
goal in corneal astigmatism
correction should be to eliminate it
completely.
“The idea that you should leave
a little with-the-rule and against-
the-rule are old myths that come
from articles written about 10 or
15 years ago,” said Dr. Holladay.
“It’s not true. Residual astigmatism
is like any other aberration. The
best vision and the best result are
with zero residual astigmatism and
with- or against-the-rule are not
benefi cial. They blur the image,
particularly if you don’t wear
glasses.”
The ultimate goal in patient
management for total corneal
astigmatism correction in cataract
surgery is both short-term and
long-term patient satisfaction, said
Douglas D. Koch, MD, professor
and the Allen, Mosbacher, and Law
Chair in ophthalmology, Cullen
Eye Institute, Baylor College of
Medicine. He said a key step in
achieving that goal is determining
patients’ needs.
“If we go to the assumption
that most patients want to see
clearly at some distance without
glasses, and therefore have a
signifi cant reduction of their
astigmatism, the goal in my mind
would be a small amount of with-
the-rule astigmatism, around 0.25
D or at most 0.5 D, the reason
for that being there’s a long-term
against-the-rule shift that takes
place. If you leave patients with
just a little bit of with-the-rule
astigmatism, that will enable them
to maintain a relatively small
amount of astigmatism over a long
period of time,” Dr. Koch said.
“We should also recognize that
occasionally patients do well with
myopic astigmatism, which gives
them greater depth of focus, but at
the expense of clear vision at any
distance. It is diffi cult to predict
those who might like this, so I
rarely recommend it,” he said.
Patient ageDr. Koch has been researching
corneal astigmatism and toric IOL
selection in cataract surgery cases.
He has developed a nomogram that
incorporates the mean posterior
corneal astigmatism in eyes with
either with-the-rule astigmatism
or against-the-rule astigmatism
and the effect of against-the-rule
drift that happens with aging.
Warren E. Hill, MD, East Valley
Ophthalmology, Mesa, Ariz., USA,
said that he follows Dr. Koch’s
recommendation of leaving patients
with one quarter to one half a D of
with-the-rule astigmatism as the
fi nal operative goal.
“I think that’s a very good
strategy. Typically what happens
for the older patients is that they
may gain a little against-the-rule
astigmatism over time, so if you
leave them with some with-the-
rule astigmatism, they’ll always be
changing toward something better
[rather] than away from what it
is that they want,” said Dr. Hill.
AT A GLANCE• Some experts say the goal
in total corneal astigmatism
correction is eliminating it.
• Theory postulates that one
quarter to one half D of with-
the-rule astigmatism could
be effective.
• Against-the-rule drift that
happens with age could play
a role in effectiveness.
• With-the-rule astigmatism
cases are easier to treat,
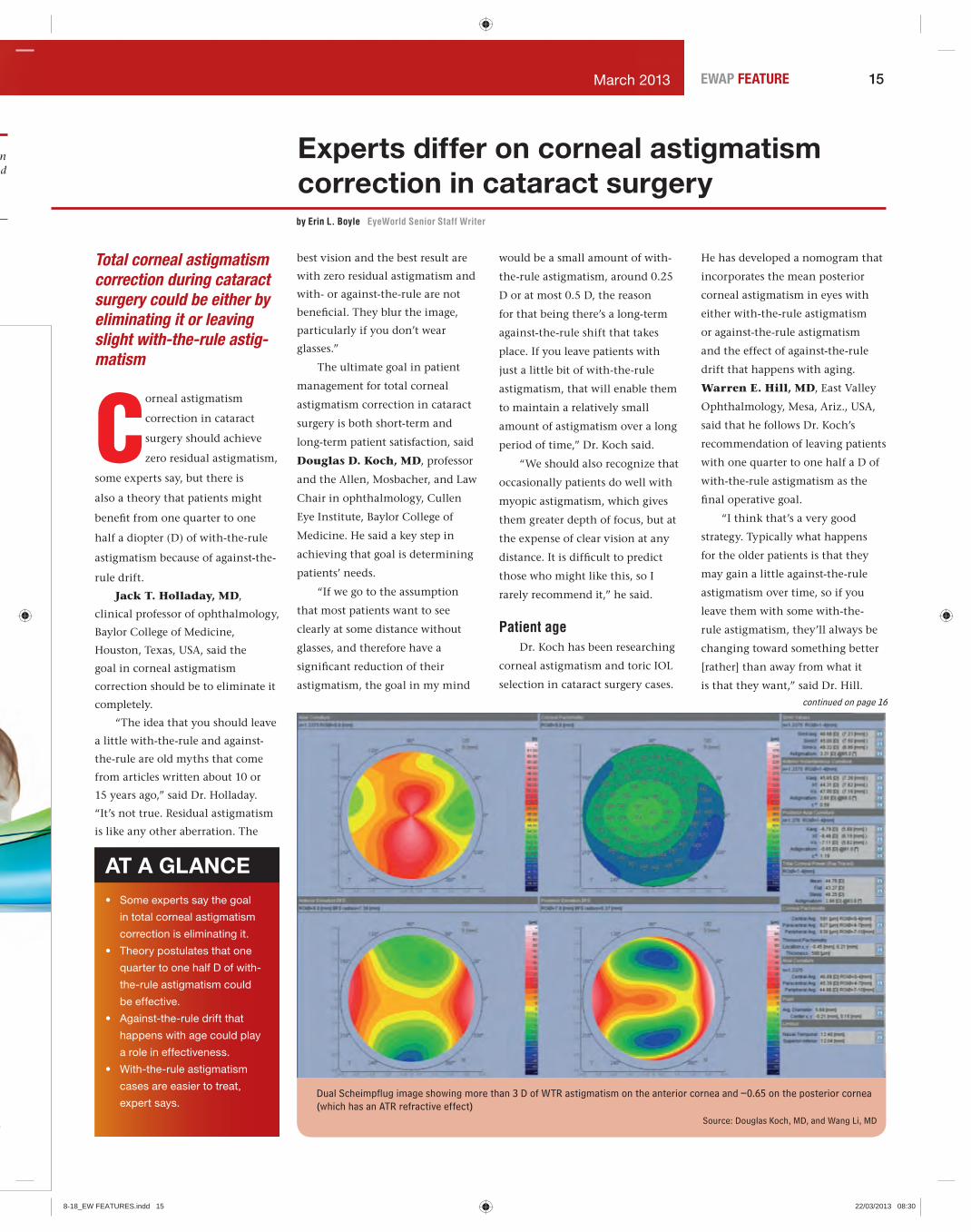
expert says. Dual Scheimpfl ug image showing more than 3 D of WTR astigmatism on the anterior cornea and –0.65 on the posterior cornea (which has an ATR refractive effect)
Source: Douglas Koch, MD, and Wang Li, MD
n nd
continued on page 16
8-18_EW FEATURES.indd 158-18_EW FEATURES.indd 15 22/03/2013 08:3022/03/2013 08:30

16 March 2013EWAP FEATURE
“Younger patients are completely
different. They’re going to drift
toward against-the-rule over time,
but it may take decades. We’re very
good at taking care of the older
patients, but the younger patients
still have some questions that need
to be answered.”
Dr. Koch said that it could be
argued that with an 85-year-old
patient, with-the-rule astigmatism
is not needed, as there is not likely
to be signifi cant change over the
course of the patient’s life. “On the
other hand, an 85-year-old could
live to 95, and you could argue
that a 50-year-old will have a much
greater chance of against-the-rule
shift, so you might leave them more
with-the-rule,” he said.
“My philosophy is, most of
these folks, if they want their
astigmatism corrected, they want it
corrected so they have good vision
now,” Dr. Koch said. “So the goal
in my mind is to leave them with
just a little bit, just enough that
they will have great uncorrected
vision, and then you can deal with
the against-the-rule shift as it takes
place in a 50-year-old—if it takes
place in 15 years, then you can
treat it at that time. But I think the
50-year-old would be disappointed
if you left him or her at 1 D of with-
the-rule astigmatism with blurry
vision planning that far ahead,
unless that patient’s a special kind
of patient and really understands
that concept.”
With-the-rule astigmatismDr. Koch said that he fi nds
with-the-rule astigmatism cases (as
measured on the anterior corneal
surface) require lower amounts
of correction per unit diopter of
astigmatism because of the against-
the-rule refractive effect on the
back of the eye. He bases this on
data from a recently published
study in which posterior corneal
astigmatism was measured with a
dual Scheimpfl ug device1 and from
analysis of clinical results with toric
IOLs.
“These patients often don’t
need much, and they need a lot less
than we used to think. That applies
to relaxing incisions and it applies
to toric lenses,” he said.
Dr. Holladay said that Dr. Koch
and others have found that those
with-the-rule astigmatism cases
need a different amount of cylinder
than against-the-rule cases.
“[Dr. Koch’s] observation has
been that whether it’s with-the-rule
or against-the-rule astigmatism,
for some reason, they end up with
more or less residual,” Dr. Holladay
said.
“The question is, why?” he said.
“What I’ve told [Dr. Koch] is, we’ve
got to pin down what the reason
for that is, if it’s to make sense. …
it’s possible that it may be due to
the fact that the with- and against-
the-rule astigmatism have different
posterior corneal astigmatisms,
and if that’s true, we should be
able to see that with Scheimpfl ug
devices like the Pentacam [Oculus,
Lynnwood, Wash., USA] and the
Galilei [Dual Scheimpfl ug Analyzer,
Ziemer, Port, Switzerland] and be
able to show that it’s a result of
the posterior surface. That’s one
possibility—that the posterior
cornea might have an effect, and
that’s what he believes. But we’ve
looked at the Pentacam and Galilei
and that’s not supported yet.”
Other reasons could exist,
Dr. Holladay said, including the
fact that, regardless of whether
a horizontal or vertical cataract
incision is made in what location,
patients drift in the direction of
against-the-rule with age.
“The other possibility is that
when you put an implant in,
that implant is never parallel
or perpendicular to the visual
axis; it may be tilted a little bit
and that tilt induces a small
amount of astigmatism. That’s
under investigation right now.
In other words, that’s [Dr.
Koch’s] observation, but there’s
no mechanism yet that’s been
confi rming that that observation
may be correct. The reason for that
observation is still up in the air,”
Dr. Holladay said.
Against-the-rule astigmatismAccording to Dr. Koch, against-
the-rule astigmatism cases need
more adjustment than with-the-rule
cases because the posterior cornea
“increases the amount of against-
the-rule astigmatism.”
“So in using a toric IOL, you
want to go up at least one half D of
increased correction for the against-
the-rule patient, and in terms of
relaxing incisions for the against-
the-rule patient, yes, they are more
likely to need it, even if there’s a
small amount of against-the-rule,”
he said.
The diffi cult part of against-
the-rule astigmatism cases is that
relaxing incisions must not be
made too long, he said. If they are,
they can create dryness and foreign
body sensation because of incised
corneal nerves.
“That astigmatism, in my mind,
is more challenging to treat,” Dr.
Koch said. “I more often will go to a
toric lens and do a relaxing incision
in those, whereas more often in
with-the-rules, for amounts up to 1
D, I do nothing and will not use a
1 D toric IOL until anterior corneal
with-the-rule astigmatism is 1.7 D.”
Dr. Holladay said in some
cases, despite the best planning,
the outcome is still not as desired.
In those cases, his Holladay IOL
Consultant has a Toric Back
Calculator tab that provides
physicians with a second chance.
“It allows the surgeon to take
the observed axis of the lens and
the refraction and by observed
axis, you look in with the slit lamp,
you line up the slit beam and you
say, that lens is at 45 degrees. And
then, if you refract the patient, with
those two bits of information, I can
calculate for you exactly how much
you need to rotate that lens to the
perfect position,” he said.
He also recommended that
physicians look at the post-op
refraction and observed axis or
post-op refraction and K reading.
“When you do end up with
an outcome that’s not on the
button, you use that Toric Back
Calculator to fi nd out how much
you need to rotate it to get it to
the right position. That helps a lot,
and it tells you what the residual
astigmatism is,” he said. EWAP
Reference1. Koch D, Ali SF, Weikert MP,
Shirayama M, Jenkins R, and
Wang L. Contribution of posterior
corneal astigmatism to total
corneal astigmatism. J Refract Surg.
2012;38:2080-2087.
Editors’ note: Dr. Hill has fi nancial
interests with Alcon (Fort Worth,
Texas, USA/Hünenberg, Switzerland).
Dr. Holladay is the developer of the
Holladay IOL Consultant programs.
Dr. Koch has fi nancial interests
with Alcon, Abbott Medical Optics
(Santa Ana, Calif., USA), OptiMedica
(Sunnyvale, Calif., USA), and Ziemer.
Contact information
Hill: 480-981-6111, [email protected]
Holladay: [email protected]
Koch: 713-798-6443,
Nas
se
in
un
as
pr
an
C
of
an
pr
Ba
H
of
an
su
an
m
ca
po
sa
co
pr
an
th
m
as
th
m
co
on
C
ev
co
to
tr
si
co
co
se
m
pr
Experts - from page 15
8-18_EW FEATURES.indd 168-18_EW FEATURES.indd 16 22/03/2013 08:3022/03/2013 08:30

17March 2013 EWAP FEATURE
p,
h
n
h
m
Posterior corneal astigmatism vital to calculating correct total astigmatismby Erin L. Boyle EyeWorld Senior Staff Writer
Not measuring the posterior
corneal astigmatism
could result in incorrect
estimation of total corneal
astigmatism, hindering toric IOL
selection through overcorrection
in with-the-rule astigmatism and
undercorrection in against-the-rule
astigmatism, researchers found.
Douglas D. Koch, MD,
professor and the Allen, Mosbacher,
and Law Chair in ophthalmology,
Cullen Eye Institute, Baylor College
of Medicine, Houston, Texas, USA,
and Li Wang, MD, associate
professor, Cullen Eye Institute,
Baylor College of Medicine,
Houston, are researching the effect
of posterior corneal astigmatism
and toric IOL selection in cataract
surgery cases.
Dr. Wang said both posterior
and anterior corneal astigmatism
measurements are important to all
cases undergoing cataract surgery.
“It would be best to measure
posterior corneal astigmatism,” she
said. “The magnitude of posterior
corneal astigmatism cannot be
predicted based on the amount of
anterior corneal astigmatism. If
there is no access to a device that
measures the posterior corneal
astigmatism, the average value of
the posterior corneal astigmatism
may be used.”
Drs. Koch and Wang and
colleagues published study results
on the topic in the Journal of
Cataract & Refractive Surgery. They
evaluated 715 corneas of 435
consecutive patients, calculating
total corneal astigmatism using ray
tracing, corneal astigmatism from
simulated keratometry, anterior
corneal astigmatism, and posterior
corneal astigmatism.
They found that toric IOL
selection based on anterior corneal
measurements only could lead to
problems.
“Patients who have anterior
Posterior corneal astigmatism
Baylor toric IOL nomogramSource (all): Douglas D. Koch, MD, and Li Wang, MD
with-the-rule astigmatism—in
other words, the cornea is steep
at 90 degrees anteriorly—tend to
have, on average, 0.5 diopter (D)
of steepness vertically along the
posterior cornea, and because the
posterior cornea is a minus lens,
steepness vertically translates into
power horizontally or against-
the-rule effect refractive power at
180,” Dr. Koch said. “So you might
measure a patient who has 2 D on
the anterior cornea. And when all
is said and done, that patient may
only have 1.3 or 1.4 D on the total
corneal power because the posterior
cornea throws in about 0.5 or 0.6 D
in the other direction.”
Measuring devicesMeasuring posterior corneal
astigmatism is a challenge, Dr. Koch
said. Two devices on the market,
the Galilei Dual Scheimpfl ug
Analyzer (Ziemer, Port, Switzerland)
and the Pentacam (Oculus,
Lynnwood, Wash., USA), measure it
“moderately accurately,” he said.
continued on page 18
8-18_EW FEATURES.indd 178-18_EW FEATURES.indd 17 22/03/2013 08:3022/03/2013 08:30

18 March 2013EWAP FEATURE
Views from Asia-Pacifi cSri GANESH, MDChairman and Managing Director, Nethradhama Hospitals Pvt. Ltd.26/14, Kanakapura Main Road, 7th Block Jayanagar Bangalore 560082 IndiaTel. no. +91-80-26088000/+91-98451294740Fax no. [email protected]
As cataract and refractive surgeons, we are constantly in pursuit of ensuring that our patients attain maximum uncorrected visual acuity after our interventions. Residual refractive astigmatism contributes signifi cantly
to the refractive outcomes of the surgery. Not measuring posterior corneal astigmatism may be one of the reasons for unexpected postoperative astigmatism, especially after toric IOLs.
Despite correct IOL calculation with the standard parameters, IOL placement and alignment, surgeons encounter a refractive surprise. There may be overcorrection of with-the-rule astigmatism and undercorrection of against-the-rule astigmatism. This can be attributed to the posterior corneal astigmatism. Anterior corneal astigmatism in younger individuals is with-the-rule and in older individuals it is against-the-rule. In contrast, the posterior cornea has a steeper vertical axis which effectively causes against-the-rule astigmatism, since the posterior cornea tends to act as a minus lens. Therefore, the anterior with-the-rule astigmatism is reduced and the anterior against-the-rule astigmatism is enhanced due to the posterior corneal astigmatism in most cases.
As pointed out by the authors, estimation of posterior corneal astigmatism should be done routinely in toric IOL patients in addition to the standard parameters. If there is no access to the available devices to estimate the posterior astigmatism, then the data available in Dr. Koch’s nomogram or the Baylor’s nomogram can be used to estimate the mean posterior corneal astigmatism to calculate the toric IOL power and axis. One more important fact pointed out by the authors is that it is essential to keep in mind the effect of against-the-rule drift that occurs with age. Hence, it is always better to leave the toric IOL patient with some amount of residual with-the-rule astigmatism to compensate for the against-the-rule drift which occurs with aging. Imaging the posterior corneal astigmatism can be done on all patients posted for refractive cataract procedures in particular toric IOLs and toric multifocal IOLs thereby enhance the outcome.
The posterior corneal surface acts like a negative lens due to the relative change in the corneal thickness from periphery to center. This may be the reason that some eyes having with-the-rule astigmatism may have a higher overcorrection than others following toric IOL implantation. It would probably be a good idea to assess the effect of posterior corneal astigmatism in relation to the relative change in corneal thickness or progression of corneal thickness from periphery to center. Depending upon the central corneal thickness an average correction factor could be derived to compensate for the posterior corneal astigmatism and this could be incorporated into the formula for calculating the power of the toric IOL. This could help practices
that do not have Scheimpfl ug devices to measure the posterior corneal astigmatism.
Editors’ note: Dr. Ganesh is a consultant for Abbott Medical Optics (Santa Ana, Calif., USA), Carl Zeiss (Jena, Germany), Hoya Surgical Optics (Chino Hills, Calif., USA), Bausch + Lomb (Rochester, NY, USA), and Schwind eye-tech-solutions (Kleinostheim, Germany), but has no fi nancial interests related to his comments.
“I think that our measurements
could improve,” Dr. Koch said. “We
do fi nd that even the Galilei, which
has a wonderful dual Scheimpfl ug
with against-the-rule astigmatism,”
he said.
He cited a long-term study
by K. Hayashi and colleagues
that followed patients’ astigmatic
change after undergoing 3-mm
clear corneal temporal incisions.
The study also had a control group
that did not undergo cataract
surgery.
Researchers found that both
groups had a comparable change
of against-the-rule shift after more
than 10 years.
“You would think that a
corneal incision temporarily might
weaken the cornea such that the
cornea would not steepen along
the horizontal meridian over time.
But in fact it does,” Dr. Koch said.
“So in planning for our patients, I
believe that we need to leave our
patients a little bit on the with-the-
rule side in order to compensate
for the fact that they’re going to
drift to against-the-rule over time.
This will provide them with better
uncorrected acuity over a much
longer period of time and perhaps
serve them well for 20 or more
years.” EWAP
References1. Hayashi K, Hirata A, Manabe S,
Hayashi H. Long-term change in
corneal astigmatism after sutureless
cataract surgery. Am J Ophthalmol.
2011 May;151(5):858-65.
2. Koch DD, Ali SF, Weikert MP,
Shirayama M, Jenkins R, Wang L.
Contribution of posterior corneal
astigmatism to total corneal
astigmatism. J Cataract Refract Surg.
2012 Oct 12. [Epub ahead of print]
Editors’ note: Dr. Wang has fi nancial
interests with Ziemer. Dr. Koch has
fi nancial interests with Ziemer, Alcon
(Fort Worth, Texas, USA/Hünenberg,
Switzerland), Abbott Medical Optics
(Santa Ana, Calif., USA), and
OptiMedica (Sunnyvale, Calif., USA).
Contact information
Wang: 713-798-7946, [email protected]
Koch: 713-798-6443, [email protected]
mechanism for measuring the
back, does not always seem to
capture all of the posterior corneal
astigmatism, and especially in
patients [who have] with-the-
rule astigmatism, it still seems
to underestimate the amount of
posterior corneal astigmatism based
on our actual refractive outcomes.”
Dr. Koch has created a
nomogram that incorporates: 1) the
mean posterior corneal astigmatism
in eyes having either with-the-rule
or against-the-rule astigmatism
and 2) the effect of against-the-rule
drift that occurs with age. He said
that their data indicate that the
new nomogram greatly improves
accuracy with toric IOLs.
In addition, manufacturers are
interested in providing clinicians
with this information because
they are fi nding similar results
retrospectively in their data, he
said.
However, to disseminate a new
nomogram themselves, they would
have to validate it in a clinical trial
with the U.S. FDA, which could
slow the approval process.
Toric IOLsDr. Koch began examining
posterior corneal astigmatism
when he noticed that some patients
had unexpected results with toric
IOLs. Patients who had with-
the-rule astigmatism were being
overcorrected, while patients who
had against-the-rule astigmatism
were undercorrected.
“It has a huge impact on my
decision making now in patients
who are seeking astigmatic
correction during cataract surgery,”
Dr. Koch said. “It’s completely
changed everything I’m doing with
regard to both relaxing incisions
and with regard to the selection of
toric IOLs.
“I have backed off on toric IOL
power in patients who have with-
the-rule astigmatism and conversely
ramped it up for those patients with
against-the-rule. For example, for
someone who has 1 diopter with-
the-rule astigmatism, I will not put
a toric IOL in because I am likely
to overcorrect him and leave him
Posterior - from page 17
8-18_EW FEATURES.indd 188-18_EW FEATURES.indd 18 22/03/2013 08:3022/03/2013 08:30

19EWAP CATARACT/IOLMarch 2013
A new complication after endothelial keratoplasty proceduresby Vanessa Caceres EyeWorld Contributing Writer
Opacifi cation, calcifi cation
linked to a certain type of
IOL material
Surgeons may want to
avoid hydrophilic acrylic
lenses when performing
cataract surgery either
concurrently or in a patient at risk
for an endothelial keratoplasty
procedure, a number of fellow
surgeons are reporting.
That’s because these surgeons
are fi nding they have to explant
the IOLs after IOL calcifi cation
forms right where the visual axis
and air bubble were in contact,
causing opacifi cation and
essentially decreasing a patient’s
vision, said W. Barry Lee, MD,
Cornea, External Disease, &
Refractive Surgery, Eye Consultants
of Atlanta/Piedmont Hospital,
Atlanta, Ga., USA.
“It’s clear that the air bubble is
reacting to the hydrophilic acrylic
lens material and causing a buildup
of hydroxyapatite. Over time it
gets more opacifi ed and eventually
leads to a drop in vision,” Dr. Lee
said. “The problem is its directly
in the patient’s central vision so
we very likely have to do a lens
explant, which is risky for the
endothelial transplant survival.”
Tracking the problemThis is a new problem related
to endothelial keratoplasty
procedures as this kind of surgery
has only been around a few years,
Dr. Lee said. However, calcifi cation
of some hydrophilic IOLs
previously occurred one to two
years after cataract surgery, said
Nick Mamalis, MD, professor
of ophthalmology, John A.
Moran Eye Center, Department of
Ophthalmology & Visual Sciences,
University of Utah, Salt Lake City,
Utah, USA. The calcifi cation in
those cases occurred in different
locations and for different reasons.
Surgeons rarely if ever have seen
that kind of calcifi cation with
modern hydrophilic IOLs until
the localized calcifi cation after
Descemet’s stripping endothelial
keratoplasty (DSEK) or Descemet’s
stripping automated endothelial
keratoplasty (DSAEK) began to
occur, he said.
Although Dr. Lee said there
are few published reports on this
problem right now, he said there
is even more word-of-mouth
evidence from surgeons that this
problem is occurring more often.
Additionally, a report of three cases
in the October 2012 issue of Cornea
by Patryn et al. as well as a letter in
the April 2012 issue of the Journal
of Cataract & Refractive Surgery
(JCRS) from Werner et al. have
addressed the problem.
“We have recently published
a letter calling attention to a
phenomenon of calcifi cation
of intraocular lenses following
procedures using intracameral
injections of air or gas, including
posterior lamellar keratoplasty
techniques,” said Liliana
Werner, MD, associate professor
and co-director, Intermountain
Opacifi ed Memory Lens after DSAEK
Opacifi ed Rayner IOL after DSAEK. After dilation, the hydroxyapatite respects the visual axis and only coats the anterior surface of the IOL where the previously undilated pupil was present. The iris protected the remainder of the IOL from opacifi ca-tion.
Source (all): W. Barry Lee, MD
Ocular Research Center,
Department of Ophthalmology
and Visual Sciences, John A. Moran
Eye Center, referring to the JCRS
letter. “Since that publication,
we have received new specimens
in our laboratory at the John A.
Moran Eye Center represented
by lenses calcifi ed after DSEK or
DSAEK.”
The exact cause and how
often the problem is occurring are
not yet clear, Dr. Mamalis said.
“Something is changing on the
anterior surface of the IOL. We’re
trying to fi gure out what it is,” he
said.
The problem does not seem
to be linked with IOLs from a
particular manufacturer, Dr.
Werner said. All lenses studied by
Dr. Werner and co-investigators
have a distinctive pattern of
calcifi cation localized to the
anterior surface/subsurface of the
lens and within the pupillary or
the capsulorhexis area.
“The calcifi cation was very
dense and could not be removed
by Nd:YAG laser applications or
surgical means, and the lenses had
to be explanted due to decrease in
visual function,” Dr. Werner said.
Dr. Werner’s letter discusses
the circumstances surrounding
the handful of reported cases
where this problem has occurred.
One such case analyzed at her lab
had localized IOL calcifi cation
after DSAEK. In June 2010, the
patient had Fuchs’ dystrophy and
phacoemulsifi cation, followed by continued on page 21
19-32 EW CARARACT.indd 1919-32 EW CARARACT.indd 19 22/03/2013 11:5222/03/2013 11:52

20 EWAP CATARACT/IOL March 2013
F A M I L Y O F I O L S
Multifocal Monofocal
The TECNIS® Family of IOLs: Proven performance and outcomes. Invaluable peace-of-mind.
You deserve some inner peace. And that’s what you get with the broad portfolio of TECNIS® aspheric IOLs. The proven combination of optics, material, and design associated with TECNIS® IOLs continues to help you provide patients with predictable, high-quality outcomes.
When it comes to peace-of-mind, the choice is clear.
Please contact your local Abbott Medical Optics Inc. sales representative to learn which lens options are available.
TECNIS is a trademark owned by or licensed to Abbott Laboratories, its subsidiaries or affiliates. ©2013 Abbott
Medical Optics Inc.
www.AbbottMedicalOptics.com / 2013.02.05-CT6339
19-32 EW CARARACT.indd 2019-32 EW CARARACT.indd 20 22/03/2013 11:5322/03/2013 11:53
21EWAP CATARACT/IOLMarch 2013
hydrophilic IOL implantation. The
DSAEK procedure was performed
with intracameral injections of
air in October 2010. “Two months
later, the patient complained
of ‘foggy’ vision,” Dr. Werner
and co-investigators reported.
“Opacifi cation of the anterior
surface of the IOL within the
pupillary area was observed. As
Nd:YAG laser disruption of the
opacifi cation was not successful,
surgeons exchanged the IOL in
October 2011.”
ImplicationsThe easiest way to prevent this
problem is to avoid hydrophilic
acrylic lenses in patients where
cataract surgery is needed
concurrently or prior to DSEK or
DSAEK. Surgeons should instead
use hydrophobic lenses in those
patients.
“For the moment, surgeons
should consider avoiding
hydrophilic acrylic IOLs when
procedures using intracameral air
or gas are anticipated, particularly
in DSEK or DSAEK,” Dr. Werner
said.
Generally speaking, surgeons
in Europe use hydrophilic lenses
more often, said Dr. Mamalis.
However, even surgeons in the
U.S. may have their personal
preferences for the material,
Dr. Lee said. In Dr. Lee’s offi ce,
some surgeons favor the use of
hydrophilic acrylic lenses in
routine cataract cases, and they
work great in most cases—except
for in two patients in whom the
hydrophilic acrylic IOLs had to
be explanted after endothelial
keratoplasty procedures due to
severe opacifi cation and vision
decline. In both cases the DSAEK
was performed for advanced Fuchs’
dystrophy following prior cataract
surgery. The IOL explantation
occurred with the fi rst year
after the DSAEK procedures. IOL
explantation under an endothelial
graft carries a high risk for
potential endothelial graft damage.
“If a patient is going to have
combined DSAEK and cataract
removal, or if it is a patient with
Fuchs’ dystrophy and you see
moderate to advanced guttata,
avoid hydrophilic acrylic lenses in
those cases,” Dr. Lee said. “This
is another thing to think about
when you see patients with Fuchs’
dystrophy to avoid a potential
serious complication.”
However, this area requires
further research, Dr. Werner
believes.
“Further investigation in
this phenomenon is necessary
to ascertain if the localized
calcifi cation is a result of direct
contact between the IOL surface
and the exogenous gas and air, of
a metabolic change in the anterior
chamber due to the presence of the
exogenous gas and air, or the result
of an exacerbated infl ammatory
reaction after multiple surgical
procedures,” said Dr. Werner. EWAP
Editors’ note: The physicians have
no fi nancial interests related to this
article.
Contact information
Lee: 404-351-2220, [email protected]
Mamalis: 801-581-6586,
Werner: 801-581-8136,
A new - from page 19
TECNIS® Monofocal Intraocular Lens (IOL)Warnings: Physicians considering lens implantation under any of the conditions described in the Directions for Use labeling should
Precautionsirrigating solutions such as balanced salt solution or sterile normal
Adverse Events: The most frequently reported adverse event that occurred during the clinical trial of the 1-Piece lens was
surgical intervention (pars plana vitrectomy with membrane peel)
TECNIS® Multifocal 1-Piece Intraocular Lens (IOL)Warnings: Physicians considering lens implantation under any of the conditions described in the Directions for Use labeling
expected because of the superposition of focused and unfocused
percentage of patients, the observation of such phenomena will be annoying and may be perceived as a hindrance, particularly
contrast sensitivity is reduced with a multifocal lens compared
should exercise caution when driving at night or in poor-visibility
be taken to achieve centration, as lens decentration may result in patients experiencing visual disturbances, particularly in patients
Precautions: The central one millimeter area of the lens creates a far image focus; therefore, patients with abnormally small pupils (~1mm) should achieve, at a minimum, the prescribed distance vision under photopic conditions; however, because this multifocal design has not been tested in patients with abnormally small pupils, it is
Autorefractors may not provide optimal postoperative refraction of
contact lens wearers, surgeons should establish corneal stability
should be taken when performing wavefront measurements, as two different wavefronts are produced (one will be in focus [either far or near], and the other will be out of focus); therefore, incorrect
therefore, implant patients should be monitored postoperatively
occasionally in patients with controlled glaucoma who received
targeted, as this lens is designed for optimum visual performance Adverse Events: The most
frequently reported adverse event that occurred during the clinical ®
retinal repair, iris prolapse/wound repair, trabeculectomy, lens
The second most frequent adverse event was macular edema,
Caution: Federal law restricts these devices to sale by or on the
Attention: Reference the Directions for Use labeling for a
Important Safety Information
19-32 EW CARARACT.indd 2119-32 EW CARARACT.indd 21 22/03/2013 11:5322/03/2013 11:53

22 EWAP CATARACT/IOL March 2013
Preventing the Argentinian Flag Sign: Phaco capsulotomyby Christopher C. Teng, MD
The Argentinian
Flag Sign occurs
during capsulorhexis
construction. Due to
the overbearing pressure of the
cataract, the anterior capsule tears
and extends to the periphery.
Once this occurs, the remainder
of the cataract extraction can
become extremely difficult and
can lead to many complications,
such as posterior capsule rupture,
vitreous loss, retained nucleus,
and endothelial damage due to
prolonged surgery time.
Phaco capsulotomy is
a technique in which the
phacoemulsification tip is
used to simultaneously create
the initial tear in the anterior
capsule and remove a portion of
the intumescent lens, thereby
debulking and relieving pressure
from the lens and capsule, and
preventing the Argentinian Flag
Sign.
IntroductionWhite cataracts and
intumescent cataracts are
challenging cases for most
surgeons. In these eyes,
during capsulorhexis creation,
the pressure created by the
hyperhydration of lens fibers can
cause spontaneous tears in the
capsulorhexis that extend to the
periphery.
When this occurs, the
appearance of the stained
blue anterior capsule beside
the white cataract mimics the
blue-white-blue pattern of the
Argentinian flag and was named
the Argentinian Flag Sign (Figure
1). Daniel Mario Perrone, MD,
coined the term, and his video
won awards at the 2000 American
Society of Cataract & Refractive
Surgery and the European Society
of Cataract & Refractive Surgeons
annual meetings.
One method for preventing
the Argentinian Flag Sign is by
introducing a 27-gauge needle
on a syringe into an intact
anterior capsule. The needle is
used to aspirate the liquefied
cortex, thereby depressurizing
the nucleus, which facilitates
a controlled capsulorhexis.1
Additionally, a highly cohesive
ophthalmic viscosurgical device
(OVD) can be used to pressurize
the anterior chamber against the
pressure of the intumescent lens,
which can facilitate continuous
curvilinear capsulorhexis (CCC)
completion.2 Alternatively, a
CCC can be created using a two-
stage technique, which can help
prevent unexpected radial tears.3
The phaco capsulotomy
technique, which likely first
originated in India, introduces the
phacoemulsification tip through
the center of an intact anterior
capsule and aspirates a portion
of the lens. This simultaneously
creates the initial anterior capsule
puncture and removes some of
the liquefied cortex and nucleus.
Phaco capsulotomy debulks and
depressurizes the entire lens/
capsule apparatus, and removes
the impetus for the capsule to
tear outward. Once enough of
the cortex is aspirated, OVD
is injected and a leaflet of the
capsule can be grasped with a
forceps, and the capsulorhexis
can be completed without
complication.
TechniqueThe initial steps are identical
to a cataract extraction in which
capsular stain is used. This includes
creating a paracentesis, using a
capsular stain, injecting highly
cohesive and/or dispersive OVD,
and creating a main wound.
After the main wound is created,
the phacoemulsifi cation tip is
introduced into the eye. The
handpiece should not be irrigating
upon entry, as there is OVD
present in the anterior chamber
that maintains anterior chamber
form. The bevel of the tip should
be positioned facing up, as this
best facilitates removal of liquefi ed
cortex and underlying nucleus.
Next, the phacoemulsifi cation tip
should be directed at a downward
angle and situated over the center
of the anterior capsule.
The settings on a torsional
phacoemulsifi cation machine
should be in the sculpting mode,
with no phacoemulsifi cation
power but high phaco handpiece
Figure 1. Argentinian Flag Sign. Arrow indicates tear of the anterior capsule, which extends to the periphery.
Figure 2B. Ophthalmic viscosurgical device injected into the anterior chamber, with good visualization of the capsular tear
Figure 2C. Completion of a continuous curvilinear capsulorhexis
Source (all): Christopher C. Teng, MD
Figure 2A. Phaco tip puncturing an intact anterior capsule and aspirating and debulk-ing the nucleus
continued on page 24
19-32 EW CARARACT.indd 2219-32 EW CARARACT.indd 22 22/03/2013 11:5322/03/2013 11:53

23EWAP CATARACT/IOLMarch 2013
s
D
CHEE Soon Phaik, MDSenior Consultant and Head, Cataract Subspecialty Service and Ocular Infl ammation & Immunology,Singapore National Eye CentreAssociate Professor, Department of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, and Duke-National University of Singapore Post Graduate Medical School, Singapore, Singapore Eye Research Institute
11 Third Hospital Avenue, Singapore 168751Tel. no. +65-62277255Fax no. [email protected]
Creating an intact continuous curvilinear capsulorhexis (CCC) for the intumescent cataract always poses a challenge for the cataract surgeon. This step is crucial for phacoemulsifi cation especially when dealing with a dense
nucleus. In eyes with shallow anterior chamber, the intumescent lens may present as phacomorphic glaucoma, complicating the surgery further.
There are various ways of avoiding the Argentinian Flag Sign. This article describes the “phaco capsulotomy”, which I have had no personal experience with. I am reluctant to use this technique for fear of creating a leading edge (as seen in Figure 2B) which may extend in an uncontrolled fashion during the initial maneuver. If the phaco tip becomes occluded, resulting in impaling of the nucleus, further aspiration of the liquefi ed cortex will cease, allowing the tear to propagate.
I routinely use the needle aspiration method, which has rarely failed in my hands. Here are some tips for a successful outcome:
1. Run intravenous mannitol to shrink the vitreous and swollen lens a half hour prior to surgery even in the absence of raised intraocular pressure.
2. Avoid speculums that exert pressure on the globe.
3. Have a low threshold for giving regional anesthetic block in an uncooperative squeezing patient.
4. Always use capsular dye to ensure visibility of the anterior capsule. Apply the dye directly onto the capsule under viscoelastic to avoid staining of the endothelium of a swollen cornea.
5. Fill the eye with Healon 5 (Abbott Medical Optics, Santa Ana, Calif., USA) in the presence of signifi cant positive pressure until the anterior capsule is fl attened.
6. Enter the eye only partially with the keratome in order to keep the main incision small, thus minimizing viscoelastic loss and maintaining a deep anterior chamber. Enlarge the incision once lens decompression is successful.
7. Perform trans pars plana 23-gauge limited anterior vitrectomy to decompress the eye if the anterior chamber is still extremely shallow and the anterior capsule is bulging.
8. While holding a 1-cc syringe fi tted with a 27-gauge needle bevel up, simultaneously puncture the anterior capsule and aspirate liquefi ed cortex, pressing down on the nucleus. Rotate the bevel sideways without extending the breach in the anterior. Ballot the nucleus and continue aspiration as liquefi ed cortex from behind the nucleus is displaced anteriorly.
9. Fill the anterior chamber with retentive viscoelastic and complete the CCC. Use intraocular capsulorhexis forceps if the lens is still swollen.
Editors’ note: Prof. Chee is a consultant for Bausch + Lomb/Technolas Perfect Vision (Rochester, NY, USA/Munich, Germany), and Hoya Surgical Optics Pte. Ltd. (Chino Hills, Calif., USA), but has no fi nancial interests in the content of her comments.2007;33:47-52.
Views from Asia-Pacifi cYAO Ke, MDProfessor, Eye Center, Second Affi liated Hospital, College of Medicine, Zhejiang University88 Jiefang Road, Hangzhou 310009, Zhejiang Province, ChinaTel. no. +86-571-87783897Fax no. [email protected]
When a highly intumescent, bulging white lens is seen under the surgical
microscope, the surgeon will usually pause and hope that a rapid tear
of the anterior capsule to the lens equator would not happen. White and
intumescent cataracts are common in China, especially in the remote countryside.
The incidence of white cataracts is 5 to 10% in our Eye Center, Second Affi liated
Hospital of Zhejiang University. Fortunately, the Argentinian Flag Sign occurs in only
10% or less of these cases. It is a kind of challenge for the cataract surgeon to
perform the remaining surgery.
When I meet a white and intumescent cataract, it is necessary to evaluate the
possibility of the Argentinian Flag Sign before capsulorhexis. For the white cataract
without a liquefi ed cortex, capsulorhexis would be performed directly after the
capsular staining and OVD injection. If the injection of OVD can change the shape
of the lens surface due to the liquefi ed cortex, there is a risk of the Argentinian
Flag Sign developing. In these cases, I would inject a highly cohesive OVD from the
anterior chamber central and fl at the central anterior capsule as much as possible.
Adequate anterior chamber formation facilitates the following steps although it
requires more OVD. Then, a 27-guage needle on a syringe is introduced into the
center of the anterior capsule with a downward angle and the liquefi ed cortex is
aspirated simultaneously to depressurize the underlying nucleus, which is defi nitely
an effective method to prevent the Argentinian Flag Sign. As long as the anterior
capsule does not tear and extend to the periphery when punctured, the risk will
be reduced greatly with the aspiration of the liquefi ed cortex. Additionally, once
enough liquefi ed cortex is aspirated, OVD can be used to pressurize the anterior
capsule, followed by capsulorhexis. A leafl et of the capsule should be grasped and
torn concentrically with forceps during capsulorhexis. Any outward force can easily
tear the capsule to the lens equator because of the brittle anterior capsule.
I have not performed the phaco capsulotomy presented by Dr. Teng for dealing
with white and intumescent cataracts. According to the introduction, I think it is a
nice method worth being popularized. The point of my comments is that regardless
of which method you use, if the Argentinian Flag Sign does occur, be cautious
in deciding whether to continue phacoemulsifi cation. Meeting a hard and large
nucleus, switching to ECCE and circling out the nucleus by widening the incision
can avoid many serious complications such as rupture of the posterior capsule and
nucleus dislocation into the vitreous.
Editors’ note: Prof. Yao has no fi nancial interests related to his comments.
24
19-32 EW CARARACT.indd 2319-32 EW CARARACT.indd 23 22/03/2013 11:5322/03/2013 11:53

24 EWAP CATARACT/IOL March 2013
torsion, low vacuum, and moderate
aspiration. When the foot pedal
of the phacoemulsifi cation unit is
depressed, irrigation and aspiration
is introduced at a fi xed rate. Various
settings can be used depending on
the phacoemulsifi cation machine
used.
The next sequence of events
occurs simultaneously. The foot
pedal is depressed and the anterior
capsule is punctured with the
phaco tip. This creates the initial
anterior capsule puncture, and
the phaco tip is introduced into
the lens (Figure 2A). Milky cortex
will become visible and is quickly
aspirated into the handpiece. The
phaco tip is further embedded into
the nucleus to sculpt the nucleus
and further remove the milky
cortex. This sculpting motion can
be made repeatedly, with each
successive motion removing more
of the lens.
Once the surgeon determines
that enough of the cortex and fl uid
is removed, the phaco handpiece
is removed from the eye. OVD is
then injected to refi ll the anterior
chamber and the nonuniform
tear of the anterior capsule can be
visualized (Figure 2B). Next, using
a capsulorhexis forceps, a leafl et of
the anterior capsule can be grasped,
and the capsulorhexis can be
completed in a curvilinear fashion
(Figure 2C).
Hydrodissection can then be
performed and nucleus removal can
be performed in the usual fashion.
DiscussionPhaco capsulotomy is an
effective technique to debulk the
lens and remove the impetus for
the Argentinian Flag Sign to occur.
The main complication that I have
encountered using this technique is
wound burn. This occurs when the
phaco tip embeds immediately into
the nucleus and occludes, leading
to an interruption of aspiration.
Wound burn can be effectively
countered by pulsing the foot pedal
upon entry of the phaco tip or by
using burst mode.
Pearls to performing this
technique include using a second
instrument and using a 2.75-mm
wound and larger phaco tip. Eyes
with mature intumescent lenses
frequently have shallow anterior
chambers, and when the phaco
tip is introduced, the eye will
be pushed to a nasal position. A
second instrument can be placed
into the paracentesis to pull the eye
back to an ortho position before the
phaco capsulotomy is performed. A
larger wound and phaco tip are also
advantageous because there is less
chance of the handpiece becoming
occluded, thereby decreasing the
risk of wound burn and facilitating
removal of the dense lens
fragments.
In conclusion, phaco
capsulotomy is a safe and effective
technique for preventing the
Argentinian Flag Sign. By using
the phaco tip to simultaneously
create an anterior capsular puncture
and remove the liquefi ed cortex
and nucleus, the lens/capsule
apparatus is decompressed and
the impetus for the capsulorhexis
to spontaneously tear outward is
eliminated. EWAP
References1. Rao SK, Padmanabhan P.
Capsulorhexis in eyes with phacomorphic glaucoma. J Cataract Refract Surg. 1998;24:882-4.
2. Kara-Junior N, de Santhiago MR, Kawakami A, Carricondo P, Hida WT. Mini-rhexis for white intumescent cataracts. Clinics (Sao Paulo). 2009;64:309-12
2. Bissen-Miyajima H. Ophthalmic viscosurgical devices. Curr Opin Ophthalmol. 2008;19:50-4.
Editors’ note: Dr. Teng is affi liated with the Einhorn Clinical Research Center, New York Eye and Ear Infi rmary, New York, NY, USA; New York Medical College, Valhalla, NY, USA; and New York University School of Medicine, New York, NY, USA. He has no fi nancial interests related to this article.
Contact informationTeng: [email protected]
Preventing - from page 22
The new generation of ophthalmic instruments
Come and discover this innovative reusable range of instruments
at ASCRS San Francisco Booth #2417
19-32 EW CARARACT.indd 2419-32 EW CARARACT.indd 24 22/03/2013 11:5322/03/2013 11:53

25EWAP CATARACT/IOLMarch 2013
Taking the spin out of toric rotation: Part 1by Steven G. Safran, MD
I consulted a panel of
Stephen Lane, MD,
Michael Wong, MD,
Jeff Horn, MD, and Lisa
Arbisser, MD, to ask what they
would do for this patient’s left eye
given the problems he had with
toric IOL rotation twice in his right
eye after cataract surgery.
Figure 3 is an image of the OD
that had cataract surgery 4 years
ago. Note the advanced glistenings
and the rhexis that extends beyond
the optic nasally.
Dr. Wong (Princeton Eye
Group, Princeton, NJ, USA) said,
“In this case, high myopia is
a predisposing factor for toric
malrotation. The history of the fi rst
eye does not make clear whether
the malrotation went to the same
axis each time. Nevertheless, a large
bag diameter that is greater than
the IOL diameter is the likely cause.
Some surgeons have suggested
inserting capsular tension rings
(CTRs) in these cases as it evenly
distributes the forces at the equator,
to make the bag taut so the capsular
leaves come in closer proximity,
and to simply put material in the
fornices to increase rotational
friction. On the other hand, if
the effect of the CTR is to further
stretch the edge of the bag beyond
the haptics, it is conceivable to
make matters worse. I am not aware
of a study that has tackled this
issue. I would be less aggressive
than usual in vacuuming the
underside of the anterior capsule
during surgery. In choosing the
toric IOL axis goal, I would give
greater weight to the axis of the
bigger bowtie.”
Dr. Arbisser (adjunct clinical
associate professor, John A. Moran
Eye Center, University of Utah,
Salt Lake City, Utah, USA, and
in private practice, Eye Surgeons
Associates, Iowa and Illinois Quad
Cities) agreed with Dr. Wong
completely but was committed to
Figure 1. Topography, OD, s/p cataract surgery with toric IOL
Figure 2. Topography, OS
the use of a CTR in the second eye.
Like Dr. Wong, she would be less
aggressive with polishing of the
anterior capsule to remove lens
epithelial cells.
“CTR is the only thing to be
done differently, in my opinion.
The CTR should be placed this time
with the toric, and he should be
told that no matter what is done,
short of a two-staged procedure
where the astigmatism is fi xed on
the cornea, there is always a small
chance of required repositioning.
I would be certain to remove all
OVD from the posterior chamber
under the lens, and I would not
aggressively polish LECs off the
anterior capsule to promote an
early sandwich effect for IOL
stability,” Dr. Arbisser said.
Dr. Lane (Associated Eye Care,
St. Paul, Minn., USA) would also
use a toric lens in this case but take
a different approach altogether.
He said, “This patient, in my
opinion, should receive a toric
IOL. … I would perform standard
phacoemulsifi cation, being sure
that the capsulorhexis was well
centered and no larger than
5.0–5.5 mm in diameter. Perhaps
this would be a good indication
for the use of the femtosecond
laser to achieve this. I would then
place the toric IOL in the bag,
prolapse the optic out of the bag
(keeping the haptics in the bag,
i.e., reverse capsule capture) and
then rotate the IOL to the proper
position using either previously
placed ink marks or preferably the
SMI [SensoMotoric Instruments,
Teltow, Germany]. By capturing the
IOL in this way I believe you have
assurance the lens will not rotate
or come out of position; it has
essentially been locked in place and
return visits to the OR are avoided.
Depending upon the power of the
IOL (I assume it will be a relatively
low power IOL due to the axial
length), it could be adjusted 0.2-0.5
D (or not at all if a low enough
power) to account for the slightly
anterior position of the IOL.”
Dr. Lane’s novel approach of
anterior optic capture would likely
be successful but may make some
surgeons who have seen pigment
Figure 3 Figure 4Source (all): Steven G. Safran, MD
In the next two columns I’d like
to examine the topic of toric IOL
rotation. We will examine two
patients who had this problem starting
with the presentation of this month’s
case.
The patient is a 48-year-old male
engineer who was a high myope (27
mm eye). He had cataract surgery in
the OD 4 years earlier with a toric IOL
by a highly respected, expert cataract
surgeon. The 11.0 D AcrySof SN60T5
toric lens (Alcon, Fort Worth, Texas,
USA/Hünenberg, Switzerland) that
was placed at that time rotated on its
axis twice in the post-op period and
had to be repositioned two times.
The fi rst repositioning was done
14 days after his cataract surgery,
but the lens rotated again, and the
second repositioning was done 23
days later and ended up with a stable
outcome at the proper axis.
The patient contacted me by email
asking if I’d be willing to see him for
a consultation and to perform cataract
surgery in the second eye. He lived
3,000 miles away but was willing
to travel. His goal was to avoid the
repositionings that were required after
his fi rst eye surgery, as he found these
to be more stressful than the initial
cataract surgery.
The right eye (dominant eye) has
an AcrySof toric in proper position,
3-4+ glistenings, and a best corrected
vision of 20/20 with a –0.75–0.75X
107 refraction. Uncorrected vision was
20/50.
The non-dominant left eye had a dense
NS cataract with 20/200 best corrected
vision. This eye was also 27 mm and, like
the fi rst eye, had 2.37 D of topographic
astigmatism with a corneal topography
that was a bit “funny” with slightly
non-orthogonal astigmatism that
made me nervous about doing LRIs or
LASIK (Figures 1 and 2).
continued on page 26
ts
19-32 EW CARARACT.indd 2519-32 EW CARARACT.indd 25 22/03/2013 11:5322/03/2013 11:53

26 EWAP CATARACT/IOL March 2013
Haike GUO, MD, PhDGuangdong Provincial People’s HospitalZhongshan 2 Road, Guangzhou, ChinaTel. no. +86-020-83844380Fax no. [email protected]
Continuously developing IOL technologies allow surgeons to consider corneal astigmatism in planning the cataract postoperative refraction. In recent years, toric IOLs have proved effective in the correction of corneal
astigmatism following cataract surgery. But toric rotation postoperatively has been found frequently, and it is a serious problem especially in high myopes.
At the Guangdong Eye Institute, we usually use toric IOLs and capsular tension ring (CTR) implantation for the correction of corneal astigmatism in high myopia.
In-the-bag IOL dislocation is thought to depend upon zonular instability, for example in eyes with traumatic injuries or pseudoexfoliation syndrome, after vitrectomy, in patients with Marfan syndrome, and in eyes with high myopia. The CTR has been found to provide stabilization of the capsular bag and IOL during and after cataract surgery in cases of zonular instability and large capsular bag.
In our clinical observation, the use of toric IOLs and CTRs could provide rotational stability and IOL centration in large capsular bags because of the fi nal refractive effect.
As discussed, reverse optic capture (ROC) is another way of preventing toric rotation for high myopes. The optic capture was fi rst described by Neuhann as rhexis-fi xation lens in 1991 (a three-piece posterior chamber IOL was placed in the ciliary sulcus and then the optic was depressed posteriorly beneath the rim of the anterior continuous curvilinear capsulorhexis to achieve IOL stability). In contrast, ROC is achieved by capture of the optic anteriorly through the anterior capsulorhexis opening (haptics in the bag, optic anterior to rhexis). Now, it is often used in cases of incomplete or insuffi cient capsule support. Although ROC has been used for many other purposes and its technique is detailed, including the use of three-piece or one-piece IOLs, it has not been proved that ROC for toric fi xtion in high myopia is stable and accurate through a precise clinical outcome.
Prevention is more important than treatment for dealing with toric rotation. But for patients having toric rotation, waiting 4-6 weeks for capsular contraction and then performing the repositioning is a good way to solve the problem.
In a word, I think toric IOL with CTR implantation is an effective method for correcting corneal astigmatism in the course of cataract surgery for patients with high myopia, and technical diffi culties associated with it should not cause problems for an experienced surgeon. In addition, although creating individually adjusted IOLs is associated with the cost of the procedure, it is another way to solve the problem and may come true easily in the future.
Editors’ note: Prof. Guo is a consultant for Alcon, but has no fi nancial interests related to his comments.
Views from Asia-Pacifi cHadi PRAKOSO, MDKlinik Mata NusantaraJl. Paus Dalam C-16, Rawamangun, Jakarta 13220 IndonesiaTel. no. [email protected]
Looking at Dr Safran’s cases, I would like to share my personal experience. I
have had four post-op rotation cases (one was a high myope) out of my over
350 toric patients. All these cases occurred in the fi rst week after surgery.
When I reexamined the videos of those surgeries, I noticed that I had not removed
the OVD meticulously from behind the IOL and the equator of the capsular bag.
So, it is clear for me that residual OVD in the bag makes the bag so slippery that it
prevents the IOL from staying in its proper position.
When I repositioned my cases, I used cohesive OVD to release the capsular bag
from its attachment to the IOL because it is easier to remove all OVD from the bag
without leaving any residual OVD compared to using dispersive OVD such as Viscoat
after repositioning is completed. All repositions were performed 2-5 weeks after
the fi rst surgery, and all IOLs remained stable after surgery in the desired position.
I do not agree that leaving the LECs on the anterior capsule may facilitate adhesion
of the IOL to the capsular back since all post-op rotation always occurs within the
fi rst post-op week before LECs undergo fi broblastic transformation. Also, I do
not think that it is necessary to perform ROC when you restore the IOL position,
because this is not an easy procedure on single-piece IOLs and on the other hand
the potential risk of pigment dispersion and glaucoma may persist.
A CTR with a 14-mm diameter in a large capsular bag as in high myopic eyes seems
a rational way to avoid post-op rotation. The CTR will stretch the capsular bag and
makes both the anterior and posterior capsule stay much closer to each other,
which will clamp the haptics of the lens. Especially in a post-vitrectomy eye, the
CTR will keep the capsular bag in its normal shape and secure the position of the
IOL. Unfortunately, I do not have any experience with CTRs in such a case.
Finally, I believe that the most important thing to prevent post-op rotation of a toric
IOL is a thorough OVD wash from behind the IOL and equator of the capsular bag.
Editors’ note: Dr. Prakoso has no fi nancial interests related to his comments.
dispersion due to interaction of the
iris and one-piece AcrySof lenses
a bit nervous, whether or not they
have actual cause to be in this
proposed situation.
Dr. Horn (Vision for Life,
Nashville, Tenn., USA) would take a
more conventional approach.
“Anecdotally, there does seem
to be a higher incidence of rotation
in long eyes with presumably
large capsular bags,” he said. “In
these cases, the lens has been
reported to rotate again even after
repositioning, and in at least some
of these cases, the lens seems
to rotate to the same position,
implying that there is a ‘home’ in
these particular eyes, which would
suggest the bags are not round,
but oval. So there may be place for
a CTR, which would presumably
‘round out’ the capsular bag,
reducing rotation if the lens were
initially oriented in the long axis or
diameter of the bag. Other things
regarding surgical technique may
be important to prevent rotation,
continued on page 32
Taking - from page 25
19-32 EW CARARACT.indd 2619-32 EW CARARACT.indd 26 22/03/2013 11:5322/03/2013 11:53
27EWAP CATARACT/IOLMarch 2013
or
32
19-32 EW CARARACT.indd 2719-32 EW CARARACT.indd 27 22/03/2013 11:5322/03/2013 11:53
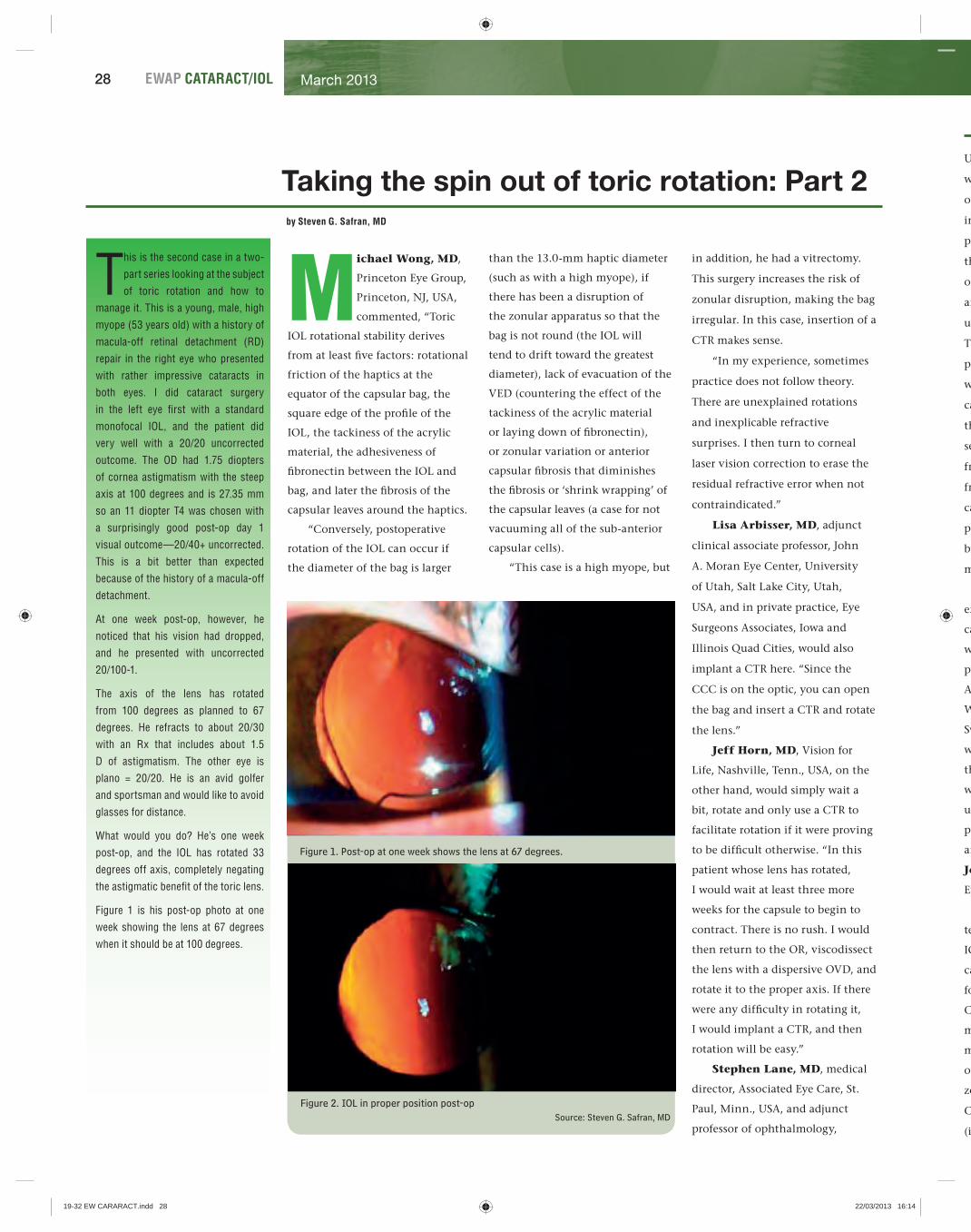
28 EWAP CATARACT/IOL March 2013
Taking the spin out of toric rotation: Part 2by Steven G. Safran, MD
than the 13.0-mm haptic diameter
(such as with a high myope), if
there has been a disruption of
the zonular apparatus so that the
bag is not round (the IOL will
tend to drift toward the greatest
diameter), lack of evacuation of the
VED (countering the effect of the
tackiness of the acrylic material
or laying down of fi bronectin),
or zonular variation or anterior
capsular fi brosis that diminishes
the fi brosis or ‘shrink wrapping’ of
the capsular leaves (a case for not
vacuuming all of the sub-anterior
capsular cells).
“This case is a high myope, but
in addition, he had a vitrectomy.
This surgery increases the risk of
zonular disruption, making the bag
irregular. In this case, insertion of a
CTR makes sense.
“In my experience, sometimes
practice does not follow theory.
There are unexplained rotations
and inexplicable refractive
surprises. I then turn to corneal
laser vision correction to erase the
residual refractive error when not
contraindicated.”
Lisa Arbisser, MD, adjunct
clinical associate professor, John
A. Moran Eye Center, University
of Utah, Salt Lake City, Utah,
USA, and in private practice, Eye
Surgeons Associates, Iowa and
Illinois Quad Cities, would also
implant a CTR here. “Since the
CCC is on the optic, you can open
the bag and insert a CTR and rotate
the lens.”
Jeff Horn, MD, Vision for
Life, Nashville, Tenn., USA, on the
other hand, would simply wait a
bit, rotate and only use a CTR to
facilitate rotation if it were proving
to be diffi cult otherwise. “In this
patient whose lens has rotated,
I would wait at least three more
weeks for the capsule to begin to
contract. There is no rush. I would
then return to the OR, viscodissect
the lens with a dispersive OVD, and
rotate it to the proper axis. If there
were any diffi culty in rotating it,
I would implant a CTR, and then
rotation will be easy.”
Stephen Lane, MD, medical
director, Associated Eye Care, St.
Paul, Minn., USA, and adjunct
professor of ophthalmology,
Michael Wong, MD,
Princeton Eye Group,
Princeton, NJ, USA,
commented, “Toric
IOL rotational stability derives
from at least fi ve factors: rotational
friction of the haptics at the
equator of the capsular bag, the
square edge of the profi le of the
IOL, the tackiness of the acrylic
material, the adhesiveness of
fi bronectin between the IOL and
bag, and later the fi brosis of the
capsular leaves around the haptics.
“Conversely, postoperative
rotation of the IOL can occur if
the diameter of the bag is larger
Figure 1. Post-op at one week shows the lens at 67 degrees.
Figure 2. IOL in proper position post-opSource: Steven G. Safran, MD
This is the second case in a two-
part series looking at the subject
of toric rotation and how to
manage it. This is a young, male, high
myope (53 years old) with a history of
macula-off retinal detachment (RD)
repair in the right eye who presented
with rather impressive cataracts in
both eyes. I did cataract surgery
in the left eye fi rst with a standard
monofocal IOL, and the patient did
very well with a 20/20 uncorrected
outcome. The OD had 1.75 diopters
of cornea astigmatism with the steep
axis at 100 degrees and is 27.35 mm
so an 11 diopter T4 was chosen with
a surprisingly good post-op day 1
visual outcome—20/40+ uncorrected.
This is a bit better than expected
because of the history of a macula-off
detachment.
At one week post-op, however, he
noticed that his vision had dropped,
and he presented with uncorrected
20/100-1.
The axis of the lens has rotated
from 100 degrees as planned to 67
degrees. He refracts to about 20/30
with an Rx that includes about 1.5
D of astigmatism. The other eye is
plano = 20/20. He is an avid golfer
and sportsman and would like to avoid
glasses for distance.
What would you do? He’s one week
post-op, and the IOL has rotated 33
degrees off axis, completely negating
the astigmatic benefi t of the toric lens.
Figure 1 is his post-op photo at one
week showing the lens at 67 degrees
when it should be at 100 degrees.
U
w
op
in
pr
th
of
an
un
Th
po
w
ca
th
se
fr
fr
ca
po
be
m
ex
ca
w
pu
A
W
Sw
w
th
w
us
pl
an
Jo
Ey
te
IO
ca
fo
C
m
m
op
zo
C
(i
19-32 EW CARARACT.indd 2819-32 EW CARARACT.indd 28 22/03/2013 16:1422/03/2013 16:14

29EWAP CATARACT/IOLMarch 2013
g
a
n
te
g
d
t
nd
e
University of Minnesota, Minn.,
would choose the option of anterior
optic capture to “lock” the lens
in place. “While keratorefractive
procedures could be considered,
they do not solve the basic problem
of the lens being out of position,
and the lens may continue to be
unstable and rotate down the line.
The photograph shows a well-
positioned toric IOL in the bag
with good overlap of the anterior
capsule over the optic (at least for
the 270 degrees or so that I can
see). After viscodissecting the IOL
free, I would prolapse the optic in
front of the rhexis (reverse capsule
capture) and rotate it to the proper
position on the steep axis. This can
be done quite atraumatically with
minimal risk.”
Because I have no personal
experience with anterior optic
capture, I was a bit uncomfortable
with the idea of purposefully
putting part of a single-piece
AcrySof implant (Alcon, Fort
Worth, Texas, USA/Hünenberg,
Switzerland) anterior to the rhexis
where it could potentially contact
the iris. I asked about experience
with reverse optic capture (ROC)
using the single-piece AcrySof
platform on the ASCRS chat board
and got this response from Jason
Jones, MD, medical director, Jones
Eye Clinic, Sioux City, Iowa.
“ROC is a capsule fi xation
technique where the haptics of the
IOL are posterior to the anterior
capsule and the optic is brought
forward (captured) by the intact
CCC. Several anatomic elements
must be respected here. The CCC
must be intact, smaller than the
optic, and well centered. The
zonules must be stable. And the
CCC must be free of any vitreous
(if the PC has been breached).
Ideally the confi guration of the iris
relative to the capsule should be
assessed; I don’t have any numbers
to recommend here, but there
should be good clearance to avoid
iris-optic contact. Given that the
cataract has been removed and the
IOL occupies much less space, I feel
it is reasonable to assume most (not
all) eyes will avoid such contact.
In the case of repositioning a toric
with ROC, this can and should
be considered. Once the lens is
rotated into position then the
optic can be brought forward to
obtain capture. … Now, I have
not had an opportunity to use
ROC for a misbehaving toric lens.
But I have implanted a series of
AcrySof single-piece acrylic IOLs
using ROC. In these cases the
PC was damaged during primary
surgery, and I elected to use this
technique. All of my patients have
done very well with clear visual
pathways, no UGH syndrome, no
RD, no decentration, and with
up to four years or more follow-
up in select cases. This is not
sulcus fi xation, and the issues that
AcrySof SPA IOLs in the sulcus
have encountered should not be
confl ated with ROC.”
Dr. Jones’ experience with this
technique should be comforting
to those who may consider it. In a
follow-up email, Dr. Lane did add
that he has done ROC “twice with
good results and no iris chafe.” I
do have the personal experience
of having treated six cases of
pseudophakic reverse pupillary
block that caused contact between
the iris and IOL leading to iris
chafi ng and pigment dispersion.
I reported and discussed this
phenomenon in the ASGR column
of the January 2012 issue of
EyeWorld, “Reversal of misfortune.”
All patients were vitrectomized
high myopes (as is the case here)
so I believe that if one wishes to
consider ROC in a vitrectomized
high myope, one should also
consider placing a peripheral
iridotomy to prevent the possibility
of reverse pupillary block
occurring, which could lead to the
iris being pushed back against the
optic, leading to chafi ng.
In this case I chose to simply
wait fi ve weeks and reposition
the lens. My own experience is
that if you reposition the lens
immediately, it is very likely to
rotate again. If, on the other hand,
you wait a few weeks for some
fi brosis to occur, the bag will shrink
wrap a bit around the lens, and
the lens will not rotate a second
time. Although a CTR could have
been used, I discussed the option
with the patient who wished not to
have one placed unless I felt it was
absolutely necessary. In this case I
did not feel that it was so we chose
not to use it. The patient ended up
with a 20/30 fi nal outcome and no
repeat rotation (Figure 2). One does
not want to wait so long that the
haptics become so strongly fi brosed
in place that they are impossible to
free up but long enough that there
is some shrink wrapping of the bag
around the lens so that the lens is
not likely to rotate a second time.
Although we don’t know the exact
timeframe for this, it is likely that
waiting fi ve to six weeks post-op
from the original cataract surgery is
a pretty safe play.
One tip is that if you know
the axis the lens is at, you don’t
need to mark the patient sitting
up. For example, in this case the
lens was measured at an axis of 67
degrees at the slit lamp, so I simply
made a mark 33 degrees in the
counterclockwise direction under
the surgical microscope knowing
that this would be exactly 100
degrees and then I rotated the lens
to this point. I like to use a fl at tip
LASIK cannula (Katena K7-5106,
Denville, NJ, USA) to get under
the edge of the anterior capsule
and initiate viscoelastic dissection.
When you reopen the bag there
is no need to “hyperinfl ate” with
viscoelastic but rather to reopen
just enough to easily facilitate
rotation. The capsular bag exhibits
a slightly different stiffer feel at
six weeks out then it does at the
time of initial cataract surgery
due to fi brosis, and I believe this
is what prevents the lens from
rotating again. After rotation the
viscoelastic is removed and the case
is completed.
Again, the CTR turned out not
to be necessary. If I were to treat
a patient who was not willing to
consider waiting 4 to 6 weeks for
a rotation then I would defi nitely
use a CTR, but if you can wait a
bit to do the repositioning, a CTR
is probably not needed. If this
lens were to rotate again, I would
consider adding a CTR, and fi nally
if it rotated a third time, reverse
optic capture with a laser iridotomy
could be considered as a fi nal
option. EWAP
Editors’ note: Drs. Arbisser, Jones, Lane, and Wong have no fi nancial interests related to this article. Dr. Safran has fi nancial interests with Bausch + Lomb.
Contact information
Arbisser: [email protected]
Horn: [email protected]
Jones: [email protected]
Lane: [email protected]
Safran: [email protected]
Wong: [email protected]
19-32 EW CARARACT.indd 2919-32 EW CARARACT.indd 29 22/03/2013 11:5322/03/2013 11:53

30 EWAP CATARACT/IOL March 2013
The business side of femto for cataractby Michelle Dalton EyeWorld Contributing Writer
Effi cacy and safety issues
aside, practices debating
how to integrate a femto-
second laser and when to
use it should read on
When evaluating
whether or not
to purchase a
femtosecond
laser for refractive cataract surgery,
the question is not whether or not
the technology is viable, but how to
bring a very expensive and space-
consuming piece of equipment into
the surgical area without disrupting
patient workfl ow. Leading
authorities tell EyeWorld how they
went about it.
Physical placementPhysically smaller practices—those
with one or two ORs—that have
dedicated refractive and cataract
suites have an advantage over a
general teaching hospital where the
OR is used by various specialties,
said Kevin M. Miller, MD,
Kolokotrones Professor of Clinical
Ophthalmology, Jules Stein Eye
Institute, Los Angeles, Calif., USA.
Ambulatory surgery centers (ASCs)
with three or four rooms, however,
have a harder situation “because
you might have two doctors doing
cataract surgery on a given day,
and you’re probably not going to
buy one femto laser for each room,”
Dr. Miller said, adding some bigger
facilities are “just fi nding a closet
where they can place it.”
The dilemma for ASCs is that
most haven’t been built with
enough physical space to house
the laser and may end up placing
it on another fl oor altogether,
said Robert P. Rivera, MD, in
private practice, Hoopes Vision,
Draper, Utah, USA. His group was
already scheduled to move into a
new facility at the end of last year,
so they reconfi gured the space to
accommodate the two femtosecond
lasers the ASC uses into their own
dedicated room.
For Robert J. Weinstock, MD, in
private practice, the Eye Institute
of West Florida, Largo, Fla., USA,
there were already four ORs and a
good amount of pre-op and post-op
space, “but what we didn’t have is
a lot of ‘extra procedures’ room. In
one small room we have a YAG laser
and an argon laser, but no room to
house more.” The group weighed
several options, including “stealing”
a conference room, or taking some
space away from the kitchen and
other administrative areas. They
decided to place the laser in one of
the ORs and drop down to three
rooms for intraocular surgery.
At the Center for Sight, Sarasota,
Fla., William Soscia, MD, said
four of the surgeons are cataract
specialists, and the entire ASC
is “very high volume”. The
group spent almost two years
evaluating how to incorporate the
technology into the available space
and ultimately opted to build a
separate room, complete with an
observation area for family to watch
while staff members narrate the
entire femtosecond aspect of the
procedure.
Dr. Miller said “moving 80- and
90-year-olds around is no simple
matter,” but at Jules Stein the only
place to put the femto laser was on
a different fl oor from the surgical
suite, and that with 10 surgeons
vying to use the laser, “it’s going to
be a total nightmare.”
Impacting the workfl owThe Catalys (OptiMedica,
Sunnyvale, Calif., USA) is the only
one of the devices where patients
can have the femto portion done
on the same bed as their cataract
removal, Dr. Rivera said. From a
patient perspective, that’s the least
disruptive, he said, but not all
machines are capable of that just
yet.
“Ergonomically, we had to decide
what would make the most sense,”
Dr. Rivera said. “The downside to
that scenario is that it does commit
that room to only the surgeons
who are going to use the Catalys.
That only works in a situation
with dedicated anterior segment
surgeons.”
The logistics of scheduling several
surgeons when the femto resides
alongside a phaco machine is
daunting, Dr. Miller said, but it’s
equally diffi cult when the femto is
in a separate location.
“It’s now going to take a procedure
that takes, say, 20 to 25 minutes in
an average person’s hands, or 10
minutes for somebody who’s really
fast, and make it at least twice as
long, if not three times as long, if
the laser is outside the room,” Dr.
Miller said. With reimbursement
rates declining, losing time on one
patient because of logistics can be
economically devastating.
Workfl ow can be diffi cult in very
high volume practices, Dr. Soscia
said. “Before we had the LensAR
[Orlando, Fla.] in our practice, we
analyzed how to incorporate it—we
started focus groups from patients
to gauge interest, we evaluated
where to physically place it, we
looked at staffi ng issues, and then
we tackled how we were going to
market this to our patient base.”
Dr. Weinstock’s group, “a relatively
high-effi ciency, high-volume center,
where we like to do somewhere
At Hoopes Vision, two different femtosecond lasers reside in a previously underused OR.
Source: Robert Rivera, MD
continued on page 32
19-32 EW CARARACT.indd 3019-32 EW CARARACT.indd 30 22/03/2013 11:5322/03/2013 11:53
31EWAP CATARACT/IOLMarch 2013
e
y
e
y
er,
32
19-32 EW CARARACT.indd 3119-32 EW CARARACT.indd 31 22/03/2013 11:5322/03/2013 11:53

32 EWAP CATARACT/IOL March 2013
between seven to eight cases per
hour at least,” realized positioning
the femto in its own room “would
improve the effi ciency of patient
fl ow and keep the surgeon from
being idle.” With almost 50% of
their patients undergoing limbal
relaxing incisions, toric lenses,
or premium IOLs, the center has
turned one OR into an advanced
cataract room complete with
intraoperative aberrometry and 3D
guidance software. The patients
move directly into this room after
their femtosecond laser treatment
in another room. There is also a
standard OR for traditional cataract
surgery.
“We made the decision to take
one of our remaining two ORs and
put both the LenSx [Alcon, Fort
Worth, Texas, USA/Hünenberg,
Switzerland] and the Catalyst in
there,” Dr. Rivera said.
Sharing responsibilitiesSurgical centers will need to
evaluate not only patient workfl ow,
but also surgeon workfl ow. Dr.
Soscia said in the previous three
months, he’s probably performed
“over 600 femtosecond cases.” He
volunteered to be the ASC’s femto
expert and has reorganized his
schedule so that three days a week
he’s doing femto for his partners,
and one day a week he’s doing the
femto for his own patients.
“With this setup, I can do about
eight laser cases an hour, therefore
allowing the cataract surgeons
to perform the same number of
cases as they were prior to the
femtosecond laser,” Dr. Soscia said.
Dr. Miller will likely have each
surgeon do his or her own femto
cases initially, “and then we’ll have
to fi gure out what makes the most
sense. We’ll have a technician be
the femto laser technician just like
we have in our laser practice center.
It may even be the same person.”
Eventually, he predicts fellows will
do part of the procedure.
Dr. Weinstock split the
responsibilities with his partners—
one day they each do only the
femto, the next they do only the
cataract surgery aspects. Dr. Rivera
has not transitioned into this model
yet, but his new facility will allow
them to do so.
“If I have 20 patients scheduled for
cataract surgery on an afternoon,
at least 50% of those are getting
femto,” Dr. Weinstock said. “So
that’s the equivalent of doing 30
procedures, not 20. [You have
to] take into account bringing
the patient into the room,
programming the laser, getting
the patient in position, doing the
procedure, and on and on. This
takes just as long as the cataract
surgery itself. So far, it’s working
great to divide the tasks with two
surgeons. We can each keep our
focus. And if you’re the guy who’s
just doing lasers, you’re 100%
focused on just doing the laser.”
For the other surgeons? “They’ve
got 50% of the procedure already
done,” Dr. Soscia said. “Me? I’m just
in the zone.” EWAP
Editors’ note: Drs. Miller, Rivera, and
Soscia have no fi nancial interests
related to this article. Dr. Weinstock
has fi nancial interests with Alcon and
Bausch + Lomb (Rochester, NY, USA).
Contact information
Miller: 310-206-9951, [email protected]
Rivera: 801-568-0200, [email protected]
Soscia: 941-806-9784, [email protected]
Weinstock: 727-244-1958, [email protected]
such as evacuating all the OVD
from behind the lens. Some have
suggested that not polishing or
vacuuming the underside of the
anterior capsule increases the
‘stickiness’ of the lens. I don’t
believe this to be true.
“This patient is highly sensitive
to a less-than-spectacular result
and is willing to travel great
distances to achieve that. First, his
astigmatism clearly needs to be
managed surgically. Because of the
slight skewing of the astigmatism
on topography, and because of
my confi dence in the toric lens,
I would still implant the toric.
But in order to reduce the odds
the lens rotated, I would implant
a CTR prophylactically prior to
implantation of the lens.”
I agree with Dr. Horn here, and
this is basically the approach that
I took. I have seen or consulted in
a handful of cases of toric rotation,
and all have been in high myopes
who rotated within the fi rst
week or so. Since rotation occurs
before the LECs remaining on the
anterior capsule have undergone
any fi broblastic transformation
and prior to any resultant bag
contracture, I see no benefi t to
purposefully leaving LECs behind.
They will not be able to prevent
the early rotation that we typically
see in these cases, although later
on they will certainly cause fi brotic
changes that will “lock things in
place.” Within the fi rst week or
so, I don’t believe the presence
of LECs helps and, in fact, may
prevent some of the tacky adhesion
between the optic and the capsule
that we typically see with the
AcrySof material. Anyone who
has tried to rotate a toric lens
after removing all the viscoelastic
knows that there is an immediate
adhesion between the tacky
AcrySof material and the capsule
that is somewhat unique to this
material. To rotate the lens without
stressing the capsule, one often
needs either additional viscoelastic
or an infusion line to dilate the
bag. As Dr. Horn stated, I believe
that in high myopes the bag may
be a bit too large for the lens and it
may not be perfectly round, which
creates a “preferred axis” that the
lens may gravitate toward. I believe
that the use of a CTR will both
round out the bag and make the
equator of the bag slightly smaller,
creating a frictional resistance to
early rotation. If the lens does not
rotate immediately (within the fi rst
10 days or so), then it is extremely
unlikely to rotate at all.
In this case I did choose to use
an 11 D T5 toric lens (Alcon) to
correct astigmatism and targeted
a –0.25 spherical outcome for
better distance vision as per the
patient’s request. I used my normal
surgical approach, creating a
centered round rhexis (effectively
achieved without the benefi t of a
femtosecond laser) that covered
the optic 360 degrees followed by
meticulous removal of LECs with
a Singer Sweep (Epsilon Surgical,
Ontario, Calif., USA). I did choose
to place a CTR with the hope that
this would prevent rotation and
then removed all viscoelastic from
behind the lens and took extra
precaution to press the optic
down against the posterior
capsule at the end of the case
to create adhesion against the
posterior capsule. The patient did
very well with no IOL rotation
post-op and a –0.25 refractive
outcome with 20/20 uncorrected
distance vision. He was very happy
with this. Figure 4 is an image of
the eye 1 month post-op.
It does appear that the use of
the CTR inhibited the rotation of
the lens in this patient. I do think
that it is reasonable to consider the
primary use of a CTR for toric IOL
cases at high risk for rotation. All of
the cases of rotation I’ve seen so far
have been relatively young, highly
myopic males, so in a patient fi tting
this demographic, especially with a
history of rotation in the fi rst eye, I
would certainly consider using this
approach again. EWAP
Contact informationArbisser: [email protected]: [email protected]: [email protected]: [email protected]
Taking - from page 26The business - from page 30
19-32 EW CARARACT.indd 3219-32 EW CARARACT.indd 32 22/03/2013 11:5322/03/2013 11:53
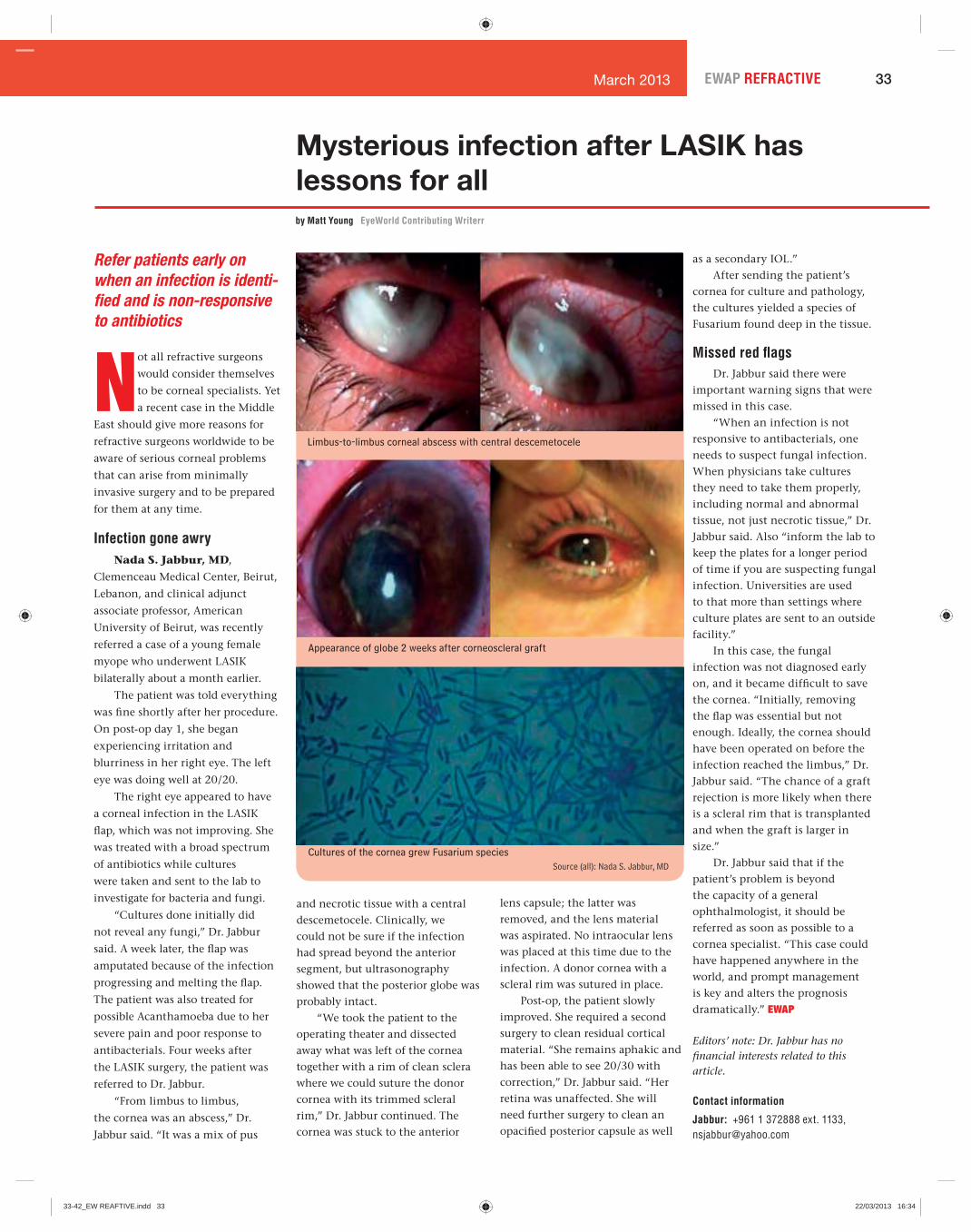
33EWAP REFRACTIVE March 2013
Mysterious infection after LASIK has lessons for allby Matt Young EyeWorld Contributing Writerr
Refer patients early on
when an infection is identi-
fi ed and is non-responsive
to antibiotics
Not all refractive surgeons
would consider themselves
to be corneal specialists. Yet
a recent case in the Middle
East should give more reasons for
refractive surgeons worldwide to be
aware of serious corneal problems
that can arise from minimally
invasive surgery and to be prepared
for them at any time.
Infection gone awryNada S. Jabbur, MD,
Clemenceau Medical Center, Beirut,
Lebanon, and clinical adjunct
associate professor, American
University of Beirut, was recently
referred a case of a young female
myope who underwent LASIK
bilaterally about a month earlier.
The patient was told everything
was fi ne shortly after her procedure.
On post-op day 1, she began
experiencing irritation and
blurriness in her right eye. The left
eye was doing well at 20/20.
The right eye appeared to have
a corneal infection in the LASIK
fl ap, which was not improving. She
was treated with a broad spectrum
of antibiotics while cultures
were taken and sent to the lab to
investigate for bacteria and fungi.
“Cultures done initially did
not reveal any fungi,” Dr. Jabbur
said. A week later, the fl ap was
amputated because of the infection
progressing and melting the fl ap.
The patient was also treated for
possible Acanthamoeba due to her
severe pain and poor response to
antibacterials. Four weeks after
the LASIK surgery, the patient was
referred to Dr. Jabbur.
“From limbus to limbus,
the cornea was an abscess,” Dr.
Jabbur said. “It was a mix of pus
and necrotic tissue with a central
descemetocele. Clinically, we
could not be sure if the infection
had spread beyond the anterior
segment, but ultrasonography
showed that the posterior globe was
probably intact.
“We took the patient to the
operating theater and dissected
away what was left of the cornea
together with a rim of clean sclera
where we could suture the donor
cornea with its trimmed scleral
rim,” Dr. Jabbur continued. The
cornea was stuck to the anterior
lens capsule; the latter was
removed, and the lens material
was aspirated. No intraocular lens
was placed at this time due to the
infection. A donor cornea with a
scleral rim was sutured in place.
Post-op, the patient slowly
improved. She required a second
surgery to clean residual cortical
material. “She remains aphakic and
has been able to see 20/30 with
correction,” Dr. Jabbur said. “Her
retina was unaffected. She will
need further surgery to clean an
opacifi ed posterior capsule as well
as a secondary IOL.”
After sending the patient’s
cornea for culture and pathology,
the cultures yielded a species of
Fusarium found deep in the tissue.
Missed red fl agsDr. Jabbur said there were
important warning signs that were
missed in this case.
“When an infection is not
responsive to antibacterials, one
needs to suspect fungal infection.
When physicians take cultures
they need to take them properly,
including normal and abnormal
tissue, not just necrotic tissue,” Dr.
Jabbur said. Also “inform the lab to
keep the plates for a longer period
of time if you are suspecting fungal
infection. Universities are used
to that more than settings where
culture plates are sent to an outside
facility.”
In this case, the fungal
infection was not diagnosed early
on, and it became diffi cult to save
the cornea. “Initially, removing
the fl ap was essential but not
enough. Ideally, the cornea should
have been operated on before the
infection reached the limbus,” Dr.
Jabbur said. “The chance of a graft
rejection is more likely when there
is a scleral rim that is transplanted
and when the graft is larger in
size.”
Dr. Jabbur said that if the
patient’s problem is beyond
the capacity of a general
ophthalmologist, it should be
referred as soon as possible to a
cornea specialist. “This case could
have happened anywhere in the
world, and prompt management
is key and alters the prognosis
dramatically.” EWAP
Editors’ note: Dr. Jabbur has no fi nancial interests related to this article.
Contact information
Jabbur: +961 1 372888 ext. 1133, [email protected]
Limbus-to-limbus corneal abscess with central descemetocele
Appearance of globe 2 weeks after corneoscleral graft
Cultures of the cornea grew Fusarium speciesSource (all): Nada S. Jabbur, MD
33-42_EW REAFTIVE.indd 3333-42_EW REAFTIVE.indd 33 22/03/2013 16:3422/03/2013 16:34

34 EWAP REFRACTIVE March 2013
Presbyond Laser Blended Vision: Another approach to presbyopiaby Dan Z. Reinstein, MD
The ideal solution for
correcting presbyopia
would be to restore
accommodation, however,
no procedure up to now has been
proven to reverse presbyopia
and restore the natural focusing
mechanism of the eye. While there
is ongoing research on techniques
to achieve this, clinical applications
of these techniques will probably
not be available for another 10-20
years. Because of our inability to
restore accommodation, current
treatments for presbyopia rely on
splitting the refractive power for
distance and near either within
the same eye (multifocality)
or between eyes (monovision),
but all treatments require some
compromise from the patient.
The challenge for such
treatment options is to achieve
good binocular vision at far,
intermediate, and near distances
while also maintaining optical
quality, contrast sensitivity, night
vision, stereo acuity, and as a bonus
the procedure should be reversible.
This was the goal that we set
when developing Presbyond Laser
Blended Vision with Carl Zeiss
Meditec (Jena, Germany), and our
approach was to take advantage of
the natural mechanisms within our
optical system and minimize the
need for the patient to adapt.
All multifocal approaches
require the patient to adjust to the
unnatural situation of having to
differentiate between two images
in the same eye, so it is no surprise
that these procedures are associated
with loss of CDVA, contrast
sensitivity, and night vision
disturbances. There have been
signifi cant improvements over the
years; however, multifocality will
always rely on the patient’s ability
to adapt to this new and unnatural
intraocular rivalry. Multifocal
treatments are also usually limited
to a small range of refractive error
(usually low hyperopic patients).
The well-established principles
of contact lens monovision have
been used in laser refractive
surgery; however, many of
the limitations of contact lens
monovision also affected laser
Spherical aberration diagramSource: Dan Z. Reinstein, MD
Views from Asia-Pacifi cPOR Yong Ming, MBBS, FRCS, MMed, MRCOphthConsultant Eye Surgeon, Jerry Tan Eye Surgery& Jerry TAN, MBBS, FRCS, FRCOphth, FAMSConsultant Eye Surgeon, Jerry Tan Eye SurgeryCamden Medical Centre,1 Orchard Boulevard #10-06Singapore 248649Tel. no. +65-6738-8122Fax no. [email protected]
Presbyond as a concept is attractive in potentially
enhancing the benefi ts while moderating the
cons of standard monovision. However, a number
of aspects of this treatment bear consideration.
Theoretically, there is no doubt that spherical aberration
(SA) or even coma and astigmatism can improve an
eye’s depth of fi eld, but at the expense of some loss of visual quality. Indeed,
as Dr. Reinstein mentions, beyond a certain amount of SA the visual cortex no
longer compensates and considerable disturbances such as haloes and loss of
contrast surface. In real life, we have all seen changes of corneal topography
as an eye heals after laser refractive surgery, originating from factors such as
epithelial remodeling. As such, attempting to maximize depth of fi eld to 1.50 D by
fi ltering SA while avoiding side effects involves negotiating a fi ne line which can
easily be crossed by individual healing responses.
Presbyopic patients are also older than the average LASIK patient, and lenticular
changes are not insignifi cant. The aging lens is associated with increasing
SA with time, so even if Presbyond manages to hit the target on the cornea, one
cannot be certain how long it will be before the combined corneal and lenticular
aberrations cause noticeable visual disturbances.
The effects of any optical aberration depend greatly on pupil size, and it is intriguing
that pupillometry is not mentioned as a factor considered in the generation of the
ablation profi le. Unless Presbyond can tailor the SA to suit the range of pupil sizes
seen in different patients, the hoped for effects may not materialize. It is also
possible that a patient has large scotopic pupils in the dark which magnify the
visual disturbance caused by the induced SA.
According to the diagram accompanying this article, it appears that positive
spherical aberration is induced by the Presbyond ablation profi le, causing
peripheral rays of light striking the lens periphery to be focused before more
central rays. This is reminiscent of night myopia, resulting from scotopic mydriasis
in the presence of positive SA. It would be the opposite of what is required for
presbyopia, since during close work the pupil becomes miotic. Perhaps a small
amount of negative, rather than positive, SA may be helpful in the presence of a
bias toward slightly more myopic undercorrection.
We look forward to studies comparing standard monovision and Presbyond Laser
Blended Vision, to quantify its benefi ts as well as potential for visual side effects.
Editors’ note: Drs. Por and Tan have no fi nancial interests related to their comments.
continued on page 36
33-42_EW REAFTIVE.indd 3433-42_EW REAFTIVE.indd 34 22/03/2013 16:3422/03/2013 16:34
35EWAP REFRACTIVE March 2013
// ReLEx MADE BY CARL ZEISS
The moment flapless surgery becomes clearly visible: in a smile.This is the moment we work for.
Flapless. All-femto. Single-step. For the first time ever, advanced femtosecond technology and highly precise lenticule extraction are combined to perform minimally invasive corrections – with a single system: the VisuMax® from Carl Zeiss. Thereby, a refractive lenticule is created within the intact cornea and extracted through a small incision. The new flapless procedure offers clear advantages: minimal surgical impact on the corneal stability and excellent predictability of the refractive outcomes.
www.meditec.zeiss.com/ReLEx
ReLE
x is
not a
ppro
ved
for s
ales
in th
e U.
S.
33-42_EW REAFTIVE.indd 3533-42_EW REAFTIVE.indd 35 22/03/2013 16:3422/03/2013 16:34

36 EWAP REFRACTIVE March 2013
Michael LAWLESS, MDMedical Director, Vision Eye Institute4/270 Victoria Ave., Chatswood, NSW 2067 AustraliaTel. no. [email protected]
Dr. Reinstein is to be congratulated for exploring the use of spherical aberration
to enhance depth of focus in presbyopic patients. The same thoughts have
occurred to those using an IOL approach to presbyopia with lenses now
being trialled which increase spherical aberration to provide a similar effect.
The problem with analyzing the data provided is that the age of the patients would
have signifi cant bearing on the results presented, but it is not clear from the article
how age would have impacted Dr. Reinstein’s excellent results.
All good things come at a cost. Generally, in the normal untouched eye, the cornea has
positive spherical aberration which is matched by the negative spherical aberration of
the lens, resulting in a more or less neutral state. Of course there is a range through
the population in both the degree of corneal and lens spherical aberration. We also
know that the natural lens changes from negative to positive spherical aberration
with age and this is the very population in which a presbyopia treatment would be
required. This is one reason why the quality of vision under mesopic and scotopic
conditions declines with age. The impact of spherical aberration on visual function is
pupil dependent. So there are many variables to consider when attempting to change
the spherical aberration profi le of an individual patient.
To induce more spherical aberration on the cornea to enhance depth of focus has to
unquestionably alter the quality of vision, particularly night vision, which is one of
the reasons that LASIK excimer laser profi les moved from conventional to optimized
and wavefront guided, based on a knowledge of higher order aberrations and their
effect on the visual system.
This is an interesting approach and is likely to be helpful in a small way to enhance
presbyopic treatments, but I think we need data to support these optimistic fi rst
conclusions and perhaps better targeted treatments based on an individual eye’s
aberration profi le, as Dr. Reinstein rightly points out.
Editors’ note: Dr. Lawless is a consultant for Alcon/LenSx (Fort Worth, Texas, USA/Hünenberg, Switzerland) but has no fi nancial interests related to his comments.
refractive surgery-induced
monovision. These limitations
include loss of fusion due to the
anisometropia between the two
eyes, poor intermediate vision,
poor distance vision in the near
eye, reduced binocular contrast
sensitivity, and reduced (or even
broken) stereoacuity. However,
monovision is based on the
John S. M. CHANG, MDDirector, Guy Hugh Chan Refractive Surgery CentreHong Kong Sanatorium and Hospital8/F Li Shu Pui Block, Phase II2 Village Road, Happy Valley, Hong KongTel. no. +852-2835-8885Fax no. [email protected]
There have been many approaches in corneal refractive surgery to create a
multifocal eye, in order for the eye to see distance, intermediate and near.
Some create a central myopic region, so that when we read and the pupil
constricts, the induced myopia will compensate for the lack of accommodation.
However, if the patient is not satisfi ed with the result, whether this can be safely and
completely reversed is still a matter of discussion and more research. Monovision
works very well in patients who live in a city and do not drive. In our experience,
the success rate is over 95%. However, in countries where patients have to do a
lot of driving, the success rate drops signifi cantly. Recently, Presbyond (Carl Zeiss
Meditec), F-Cat (Allegretto, Alcon), Supracor (Baush+Lomb) all involve some form of
micro-monovision. In Presbyond and F-Cat, negative spherical aberration is induced,
thus increasing the depth of focus. We have had over 5 years of experiences with
the Allegretto F-Cat and have found that it works quite well in myopes below –6
to –7 D and, like the Presbyond, when the patient does not like the monovision or
micro-monovision, it can be easily removed without any loss of vision. Night vision
does not seem to be compromised, however, when the adjustment is pushed too far,
or when the patient’s pupil is too small there tends to be an under-correction. The
disadvantage is that it is still monovision (although the loss of stereovision should
be less) and its effect may not be long lasting because of possible epithelial fi lling
with time.
Editors’ note: Dr. Chang has no fi nancial interests related to his comments.
natural process of binocular fusion
(interocular rivalry as opposed
to the unnatural intraocular
rivalry experienced in multifocal
procedures), and recent studies
have demonstrated that many of
these limitations could be avoided
by limiting the anisometropia to
1.25 D or 1.50 D. But this level of
anisometropia does not always give
Views from Asia-Pacifi c
Presbyond - from page 34
33-42_EW REAFTIVE.indd 3633-42_EW REAFTIVE.indd 36 22/03/2013 16:3422/03/2013 16:34
37EWAP REFRACTIVE March 2013
e
ACS and the Cornea Society launch CorneaEd
IKS is massive undertaking for ACSIKS is massive undertaking for ACSThe Asia Cornea Society’s Infectious Keratitis Study (ACSIKS) is set to be
a major game changer for the region. “Corneal blindness is big in Asia,”
said Donald Tan, MD, Singapore, current president of the Cornea Society
and the Asia Cornea Society (ACS).
It’s a fair statement, summarizing the signifi cance of the most important
cause of blindness in the region second only to cataract, but it barely
scratches the surface, given the full scope and many nuances of the
problem.
Most corneal disease in the world occurs in Asia, said Prof. Tan. Here, he
said, corneal ulceration is a “silent epidemic.”
But the challenge of corneal blindness in Asia isn’t confi ned to magnitude;
unsurprisingly for the region, huge variations exist from country to country,
such that the problem runs the gamut of the entire spectrum of corneal
infections.
Epidemiological patterns, for one, differ signifi cantly, said Prashant Garg, MD, Hyderabad, India. For instance, whereas studies have identifi ed
contact lens use and ocular surface disease as the major risk factors for
microbial keratitis in a developed region like Hong Kong, trauma is the
most prevalent cause of infection in India, affecting a correspondingly
different age group: Most patients in India, said Dr. Garg, fall in the range
of 20-50 years—the economically productive age group.
Wide variations also exist from country to country in terms of pathogen,
environmental risk factors, the availability of drugs, antibiotic resistance
patterns, access to treatment, and any number of other variables that
have yet to be adequately quantifi ed.
To this end, the ACS has embarked on the ACSIKS, a multicenter,
prospective observational study in 11 study centers in eight major
locations (China, India, Japan, Korea, Philippines, Taiwan, Thailand, and
Singapore).
The study is intended to document the clinical management practices of
doctors all over the region, while also collecting microbiological samples
from recruited cases.
To date, said Prof. Tan, the study has recruited 2,118 cases, with
preliminary data analysis of 1,544 of these cases. Preliminary analysis, he
said, has identifi ed fungal and bacterial pathogens to be the main causes
of infectious keratitis in the region.
Editors’ note: ACSIKS is made possible by the support of Alcon (Fort
Worth, Texas, USA/Hünenberg, Switzerland), Allergan (Irvine, Calif., USA),
Bausch + Lomb (Rochester, NY, USA), and Santen (Napa, Calif., USA).
The Asia Cornea Society (ACS) and Cornea Society have created an
initiative to reach out to young ophthalmologists looking for opportunities
to train in the cornea subspecialty.
“CorneaEd is, quite simply, ‘cornea education,’” said Donald Tan, MD,
Singapore, president of both societies, which, he said, have always had
strong missions for education.
The website is a joint educational initiative of the sister societies,
essentially a registry with links to fellowship programs in the Asia-Pacifi c
and the U.S.
The idea, said Michael Belin, MD, vice president for international
relations, Cornea Society, is to give young ophthalmologists the
opportunity to fi nd programs that will present them with experiences they
might not otherwise have.
This in mind, the two societies hope to select two young ophthalmologists
in the corneal fellowship program of their choice.
Applications will be available on the website in the fi rst quarter of 2013.
For more information and to access the registry, visit www.CorneaEd.org.
the patient enough near vision.
Therefore, with Presbyond Laser
Blended Vision, we incorporated
another natural visual process—
fi ltering of spherical aberration—to
increase the depth of fi eld in each
eye and achieve good binocular
vision at all distances. In an eye
with no spherical aberration, light
is focused to a point, so any forward
or backward movement of the
object will make it instantly go out
of focus. However, if we introduce
some spherical aberration into the
system, there is dissemination of
the focal point, meaning that there
is a wider range of distances where
the focus is equivalent, although
slightly reduced. This of course
applies to the retinal image, but the
image is still perceived as sharply
as if there were no aberrations
due to the natural ability of the
visual cortex to “process” spherical
aberration. This range is the depth
of fi eld and can be demonstrated by
the better-than-expected distance
vision in the near eye (the mean
visual acuity is about 20/45 whereas
20/80 would be expected for a –1.50
D refraction).
This concept is simply an
extension of the eye’s natural state
as everyone has some naturally
occurring spherical aberration, and
the brain is already preprogrammed
to do this fi ltering. If there is
too much spherical aberration,
however, the visual cortex is no
longer able to fully “process” the
spherical aberration and will result
in loss of contrast sensitivity and
other aberration-related quality of
vision symptoms, similar to those
seen after multifocal ablations.
The ideal depth of fi eld in each eye
is 3.00 D, but we have found that
the maximum depth of fi eld that
can be safely induced is 1.50 D.
Therefore, this spherical aberration
method cannot be used to correct
presbyopia by itself but can be
combined with monovision to
improve the range of vision in each
eye.
The increased depth of fi eld in
each eye enables good near vision
to be achieved with a lower degree
of anisometropia than in traditional
monovision, which we refer to as
micromonovision. With Presbyond
Laser Blended Vision, it is possible
to displace the foci between the
eyes and create continuous vision,
from near to intermediate to far.
In essence, this strategy creates
a blend zone of vision between
the two eyes at intermediate
distances meaning that much less
suppression is required and there
is no dissociation between the
eyes. In fact, patients even retain
a functional level of uncorrected
stereoacuity—proving that they
have binocular function.
In Presbyond Laser Blended
Vision, a number of factors
are considered including age,
accommodative amplitude,
pre-op wavefront, tolerance to
anisometropia, and the amount
of refractive error. The software
then combines these factors to
generate an ablation profi le with
the aim of leaving the patient with
an appropriate level of spherical
aberration in order to maximize
the depth of fi eld without
compromising contrast sensitivity,
stereoacuity, or night vision.
At one year after Presbyond
Laser Blended Vision, binocular
UDVA was 20/20 or better and
UNVA was J2 or better in 95% of
136 myopic patients (≤–8.50 D),
77% of 111 hyperopic patients
(≤+5.75 D), and 95% of 148
emmetropic patients (within ±0.88
D). The safety in terms of contrast
sensitivity was the same as for continued on page 43
33-42_EW REAFTIVE.indd 3733-42_EW REAFTIVE.indd 37 22/03/2013 16:3422/03/2013 16:34
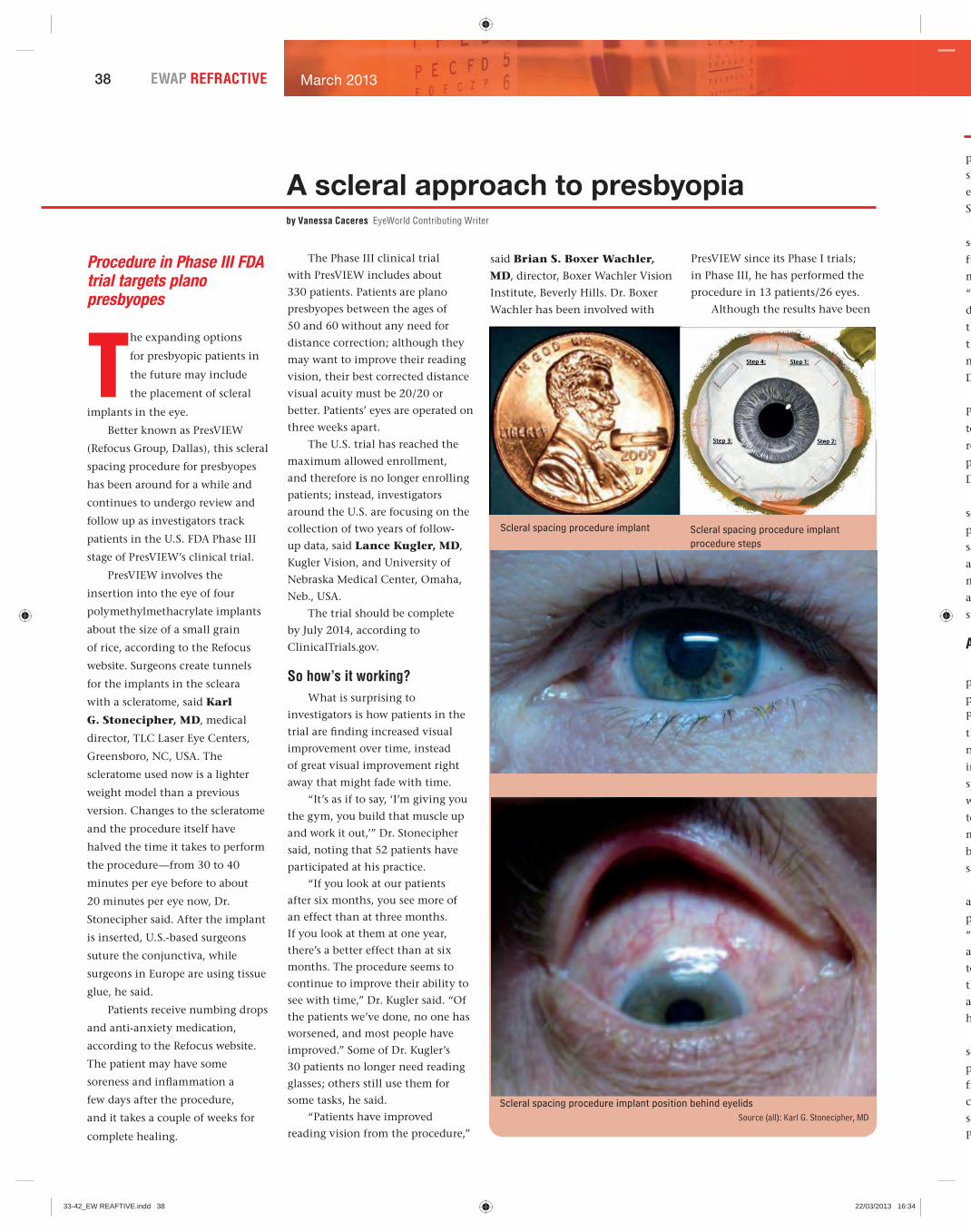
38 EWAP REFRACTIVE March 2013
A scleral approach to presbyopiaby Vanessa Caceres EyeWorld Contributing Writer
Procedure in Phase III FDA trial targets plano presbyopes
The expanding options
for presbyopic patients in
the future may include
the placement of scleral
implants in the eye.
Better known as PresVIEW
(Refocus Group, Dallas), this scleral
spacing procedure for presbyopes
has been around for a while and
continues to undergo review and
follow up as investigators track
patients in the U.S. FDA Phase III
stage of PresVIEW’s clinical trial.
PresVIEW involves the
insertion into the eye of four
polymethylmethacrylate implants
about the size of a small grain
of rice, according to the Refocus
website. Surgeons create tunnels
for the implants in the scleara
with a scleratome, said Karl
G. Stonecipher, MD, medical
director, TLC Laser Eye Centers,
Greensboro, NC, USA. The
scleratome used now is a lighter
weight model than a previous
version. Changes to the scleratome
and the procedure itself have
halved the time it takes to perform
the procedure—from 30 to 40
minutes per eye before to about
20 minutes per eye now, Dr.
Stonecipher said. After the implant
is inserted, U.S.-based surgeons
suture the conjunctiva, while
surgeons in Europe are using tissue
glue, he said.
Patients receive numbing drops
and anti-anxiety medication,
according to the Refocus website.
The patient may have some
soreness and infl ammation a
few days after the procedure,
and it takes a couple of weeks for
complete healing.
The Phase III clinical trial
with PresVIEW includes about
330 patients. Patients are plano
presbyopes between the ages of
50 and 60 without any need for
distance correction; although they
may want to improve their reading
vision, their best corrected distance
visual acuity must be 20/20 or
better. Patients’ eyes are operated on
three weeks apart.
The U.S. trial has reached the
maximum allowed enrollment,
and therefore is no longer enrolling
patients; instead, investigators
around the U.S. are focusing on the
collection of two years of follow-
up data, said Lance Kugler, MD,
Kugler Vision, and University of
Nebraska Medical Center, Omaha,
Neb., USA.
The trial should be complete
by July 2014, according to
ClinicalTrials.gov.
So how’s it working?What is surprising to
investigators is how patients in the
trial are fi nding increased visual
improvement over time, instead
of great visual improvement right
away that might fade with time.
“It’s as if to say, ‘I’m giving you
the gym, you build that muscle up
and work it out,’” Dr. Stonecipher
said, noting that 52 patients have
participated at his practice.
“If you look at our patients
after six months, you see more of
an effect than at three months.
If you look at them at one year,
there’s a better effect than at six
months. The procedure seems to
continue to improve their ability to
see with time,” Dr. Kugler said. “Of
the patients we’ve done, no one has
worsened, and most people have
improved.” Some of Dr. Kugler’s
30 patients no longer need reading
glasses; others still use them for
some tasks, he said.
“Patients have improved
reading vision from the procedure,”
Scleral spacing procedure implant
Scleral spacing procedure implant position behind eyelidsSource (all): Karl G. Stonecipher, MD
Scleral spacing procedure implant procedure steps
p
sh
ef
St
so
fu
m
“T
d
th
th
m
D
P
te
re
p
D
se
p
sa
a
m
a
su
A
p
p
F
th
n
in
sp
w
to
m
b
sa
a
p
“Y
a
te
th
a
h
se
p
fr
co
so
P
said Brian S. Boxer Wachler,
MD, director, Boxer Wachler Vision
Institute, Beverly Hills. Dr. Boxer
Wachler has been involved with
PresVIEW since its Phase I trials;
in Phase III, he has performed the
procedure in 13 patients/26 eyes.
Although the results have been
33-42_EW REAFTIVE.indd 3833-42_EW REAFTIVE.indd 38 22/03/2013 16:3422/03/2013 16:34

39EWAP REFRACTIVE March 2013
positive, the research still needs to
show exactly what makes PresVIEW
effective in target patients, Dr.
Stonecipher said.
The procedure itself will have
some improvements in the near
future, including the previously
mentioned faster surgical speed.
“The company is working on the
device that will make creating
the tunnels a faster process
than it currently is. This will
make it easier for surgeons,”
Dr. Boxer Wachler said.
Some refi nements to
PresVIEW that are undergoing
tests overseas may soon
reach the U.S. and make the
procedure more predictable,
Dr. Kugler said.
There is a risk of anterior
segment ischemia with the
procedure, Dr. Stonecipher
said. However, with the use of
a pupillometer, surgeons can
measure the pupil as needed
and eliminate the chance of
such a problem occurring.
A marketplace fi tIf PresVIEW’s trials have
positive results and the
procedure is approved by the
FDA, investigators envision
the surgery targeting the large
number of plano presbyopes
in the population—and
specifi cally, patients who
want to avoid or cannot
tolerate monovision and who
may need particularly strong
binocular vision, Dr. Kugler
said.
“Right now, we don’t have
a great solution for plano
presbyopes,” Dr. Kugler said.
“You look at scleral spacing
and corneal inlays and other
technology that’s emerging. I
think there will be a role for
all of them, and the demand is
huge.”
Dr. Stonecipher also
sees a role for the various
presbyopic solutions, ranging
from modifi ed monovision to
corneal inlays to lens-based
solutions to a procedure like
PresVIEW.
“I think the market will allow
us to treat different factions of
patients with different options,” he
said.
PresVIEW also fi ts into the
ever-growing presbyopic market
due to both the large population
of plano presbyopes ideal for this
treatment and because patients
who have had previous refractive
surgery are requesting presbyopic
options as they age into their
naturally occurring presbyopia, Dr.
Stonecipher said. EWAP
Editors’ note: Dr. Stonecipher has
fi nancial interests with Refocus Group.
Drs. Boxer Wachler and Kugler have
no fi nancial interests related to this article.
Contact information
Boxer Wachler: 310-860-1900, [email protected]: 400-558-2211, [email protected]: 336-288-8523, [email protected]
n
33-42_EW REAFTIVE.indd 3933-42_EW REAFTIVE.indd 39 22/03/2013 16:3422/03/2013 16:34

40 EWAP REFRACTIVE March 2013
Strengthening corneas in Singaporeby Matt Young EyeWorld Contributing Writer
Surgeon explains why
and how he performs
crosslinking during many
LASIK procedures
While there are
known risk
factors for
ectasia after
LASIK, analysis of such factors
continues to remain controversial.
Scoring systems can lead to
incorrect predictions of risk factors
that—let’s face it—still aren’t
entirely understood.
Even as surgeons attempt
to screen out bad LASIK
candidates from good ones,
corneal crosslinking is—in some
countries—allowing surgeons to
stabilize many more corneas during
the LASIK procedure.
At least that’s what Jerry Tan,
FRCS, believes.
Dr. Tan, consultant eye
surgeon, Jerry Tan Eye Surgery,
Singapore, has been performing
follow-up for patients who have
undergone corneal crosslinking
during LASIK for the last nine
months.
He is among a select group
of surgeons performing this
procedure outside of the U.S.,
where the procedure has yet to
gain approval from the FDA.
Dr. Tan performs Lasik
Xtra (Avedro, Waltham, Mass.,
USA), which involves corneal
crosslinking, on corneas
potentially at risk for ectasia, on
hyperopic LASIK patients as well as
on very high myopes.
“At present, there is no major
complication we see,” Dr. Tan said.
Dr. Tan explained step by step
how the procedure compares to
a normal LASIK procedure and
his reasons for taking such steps
toward more stable corneas and
ones that do not regress visually.
Risks vs. benefi ts
Despite practicing Lasik Xtra
over the course of the past year, Dr.
Tan readily admits that the body of
scientifi c literature supporting the
procedure could be stronger.
“At the present moment, there
are few papers that have been
written on Lasik Xtra regarding
hyperopia,” Dr. Tan said.
Several peer-review articles
have favorably discussed Lasik
Xtra for high myopia, many just
appearing in the later half of 2012.
Meanwhile, discussion of Lasik
Xtra for hyperopia appears more
prevalently not in peer-reviewed
literature, but at ophthalmic
meetings and in trade articles.
That said, in Dr. Tan’s hands,
the procedure seems to be working
well for hyperopic patients.
“Nobody knows why hyperopic
LASIK seems to be more stable
[with Lasik Xtra],” Dr. Tan said.
“The cornea profi le seems to be
better.”
For its part, Avedro says that
Lasik Xtra preserves “corneal
biomechanical integrity” in
company literature. Essentially,
a ribofl avin formula is applied to
the cornea during LASIK along
with UVA illumination in order
to bring about crosslinking with
the intention of strengthening the
cornea.
Using topography, Dr. Tan
said these hyperopic corneas
post-surgery with Lasik Xtra
look better—i.e., “shapes are
beautiful”—compared to non-Lasik
Xtra procedures. He also feels there
is less regression occurring among
Lasik Xtra cases—a notorious
occurrence among standard
hyperopic LASIK cases.
High myopes also tend to
experience signifi cant regression
after LASIK, but not with Lasik
Xtra, Dr. Tan said.
Performing Lasik XtraSource: Jerry Tan, FRCS
Jerry Tan, FRCS
continued on page 43
33-42_EW REAFTIVE.indd 4033-42_EW REAFTIVE.indd 40 22/03/2013 16:3422/03/2013 16:34

41EWAP REFRACTIVE March 2013
e
ik
re
g
Views from Asia-Pacifi cColin CHAN, MD, MBBS(Hons), FRANZCOConjoint Associate Professor, SOVS, Faculty of Sci-ence, UNSWClinical Senior Lecturer, Central Clinical School, University of SydneyVision Eye InsititueLevel 4, 270 Victoria Ave., Chatswood, NSW 2067 AustraliaTel. no. +61-9424-9999Fax no. [email protected]
Post-LASIK ectasia is a devastating complication for both the patient and
the refractive surgeon, hence the desperate search for either a screening
or treatment method to reduce the incidence of ectasia. Current screening
methods do not identify all patients with abnormal corneas. For example, the
Randleman Ectasia Risk Factor score1,2, while probably one of the better screening
scales, in our retrospective review would have only identifi ed 56% of ectasia patients
preoperatively as high risk.3
There are too many unknowns about accelerated crosslinking after LASIK or LASIK
Xtra to conclude whether it can reduce the incidence of post-LASIK ectasia. Firstly,
there are no peer-reviewed publications to confi rm that accelerated crosslinking
actually works like conventional crosslinking. Secondly, even if there was evidence
that accelerated crosslinking worked in keratoconus, the parameters used when it is
applied in LASIK Xtra are different again (45 seconds UV exposure versus 3 minutes).
Therefore, no conclusions can be made about its safety and effi cacy with this set
of parameters. Thirdly, crosslinking as a prevention modality is quite a different
proposition from crosslinking as a treatment modality. Ectasia takes a median time
of 4 years to occur and is rare; so suffi cient longitudinal data and signifi cant numbers
are needed to prove LASIK Xtra works.4
My opinion is that there needs to be prospective data on LASIK Xtra before it can be
embraced as preventative treatment for ectasia in high risk corneas. Until then, the
best prevention is in careful case selection. Abnormal corneal topography seems to
be consistently the best predictor of post-LASIK ectasia and if a cornea is potentially
at risk for ectasia, my advice would be simple: don’t operate.
References
1. Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for
ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):
37-50. Epub 2007 Jul 12.
2. Randleman JB, Trattler WB, Stulting RD.Validation of the Ectasia Risk Score
System for preoperative laser in situ keratomileusis screening. Am J Ophthalmol. 2008 May;145(5):813-8. doi: 10.1016/j.ajo.2007.12.033. Epub
2008 Mar 10.
3. Chan CC, Hodge C, Sutton GExternal analysis of the Randleman Ectasia Risk
Factor Score System: a review of 36 cases of post LASIK ectasia. Clin Experiment Ophthalmol. 2010 May;38(4):335-40.
4. Raj R, Sutton G, Hodge C. “Incidence of Keratectasia after LASIK.” Under
review J Refract Surg.
Editors’ note: Prof. Chan has no fi nancial interests related to his comments.
Lim Li, MBBS, FRCS(Ed), MMed(Ophth), FAMSHead (Clinical Service and Education) and Senior Consultant, Corneal & External Eye Disease ServiceSingapore National Eye Centre11 Third Hospital Ave., Singapore 168751Tel. no. [email protected]
Corneal collagen crosslinking treatment has been shown to be effective in stabilizing corneal ectatic conditions such as keratoconus and post-LASIK keratectasia.1-3 The creation of a LASIK fl ap reduces the biomechanical strength
of the cornea. The structural integrity of the cornea can be weakened especially in high myopia treatment. In recent years, post-LASIK iatrogenic keratectasia has become a signifi cant problem for many refractive surgeons and LASIK patients. Over time, with the increasing number of eyes treated with LASIK, more and more corneas are likely to suffer mechanical fatigue resulting in ectasia. The incidence of post-refractive corneal ectasia is unknown, but it has been estimated by some to be as high as 1 in 1000 cases after LASIK surgery.
Traditionally, corneal collagen crosslinking is generally performed by removing the corneal epithelium and then pretreating the cornea for 30 minutes with 0.1% Ribofl avin Ophthalmic Solution to saturate the corneal tissue with the ribofl avin photosensitizer. The cornea is then irradiated with UVA (365 nm) at 3 mW/cm2 for 30 minutes. The whole procedure takes an hour to perform.
By using higher UVA irradiance, the Avedro corneal crosslinking system signifi cantly reduces crosslinking time from one hour to a few minutes. There are currently two indications for this system: KXL procedure for the treatment of keratoconus and LASIK ectasia and the Lasik Xtra procedure for prophylactically crosslinking during LASIK surgery. Both procedures have received the CE mark approval for use in Europe and are currently undergoing FDA trials in the USA. However, prophylactic crosslinking in LASIK is a new emerging technique with few published results todate. Celik4 reported in a case series of 8 eyes (fellow eye as control) that the LASIK – CXL group had equal or better visual outcome than the LASIK only group. Further long term follow-up and clinical evaluations are required.
References
1. Wollensak G, Spoerl E, Seiler T. Ribofl avin/Ultraviolet-A-induced collagen cross-linking for the treatment of keratoconus. Am J Ophthalmol. 2003; 135:620-627.
2. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long term results of ribofl avin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eye cross study. Am J Ophthalmol. 2010 Apr;149(4):585-93.
3. Vinciguerra P, Albe E, Trazza S, Seiler T, Epstein D. Intraoperative and postoperative effects of corneal collagen cross-linking on progressive keratoconus. Arch Ophthalmol. 209 Oct;127(10):1258-65.
4. Celik HU, Alagöz N, Yildirim Y, et al. Accelerated corneal crosslinking concurrent with laser in situ keratomileusis. J Cataract Refract Surg. 2012 Aug;38(8):1424-31.
Editors’ note: Dr. Lim has no fi nancial interests related to her comments.
43
33-42_EW REAFTIVE.indd 4133-42_EW REAFTIVE.indd 41 22/03/2013 16:3422/03/2013 16:34
42 EWAP rEfrActivE March 2013
ORGANISED BY:
AND
```
CIC04: Optimizing Outcomes in Toric IOLsTetsuro OSHIKA, GUO Haike, Ronald YEOH
MC06: Flawless Femto LASIK Flaps
MC01: Mastering Femto Phaco Cataract Surgery
MC02: Glued IOL
MC03: From FLEx to SMILE
WL01: Basic Phaco hands-on Wetlab with KITARO Wetlab System
Core Instructional Courses & Masterclasses
CIC01: Phaco Fundamentals
CIC02: Retinal Updates for Anterior Segment Surgeons
CIC03: Ocular Trauma
1100 - 1300 hrs
1330 - 1500 hrs
1530 - 1700 hrs
0830 - 1000 hrs
- All Core Instructional Courses and MasterClasses will be held at SUNTEC Singapore (included in meeting registration) - All Hands-on Wetlab sessions will be held at the Singapore National Eye Centre (separate charge applies)
CIC05: Tips & Tricks for Successful Pterygium Surgery
CIC06: What the Refractive Surgeon Needs to Know about Glaucoma
1045 - 1215 hrsMC04: Finer Points in IOL Fixation
WL02: Basic Phaco with KITARO Wetlab System
WL03: Basic Phaco with KITARO Wetlab System
Hands-on Wetlabs
Log on to www.2013apacrs.org for registration
1345 - 1545 hrs
1600 - 1800 hrs
Learn expert techniques from the best practitioners with our new series of Core Instructional Courses, MasterClasses and Hands-on Wetlabs!
11 July 2013 (Thursday)
11 July 2013 (Thursday)
Ronald YEOH, CHEE Soon Phaik, Gerard SUTTON, Michael KNORZ, Zoltan NAGY
Amar AGARWAL, Athiya AGARWAL, Roger STEINERT, Keiki MEHTA
Johan HUTAURUK, CHEE Soon Phaik, Hadi PRAKOSO, TI Seng Ei
ANG Chong Lye, Manish NAGPAL, LEE Shu Yen, ONG Sze Guan, Ian YEO, Doric WONG, Edmund WONG
Gangadhara SUNDAR, Hunter YUEN, Paul CHEW, S. NATARAJAN
Donald TAN, Jodhbir S. MEHTA, Kimiya SHIMIZU
Cordelia CHAN, Gerard SUTTON, Donald TAN
CHEE Soon Phaik, Ronald YEOH, Roger STEINERT
Shamira PERERA, John CHANG, Prin ROJANAPONGPUN, ZHOU Qi
MC05: Advanced BiometryFAM Han Bor, Wolfgang HAIGIS, John SHAMMAS
CHAN Wing Kwong, Cordelia CHAN, Choun-Ki JOO, WANG Zheng
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
12 July 2013 (Friday)
WL04: DSAEK Hands-on Wetlab 1600 - 1800 hrs
Hands-on Wetlab
Donald TAN, LIM Li, Jodhbir S. MEHTA(Limit to 8 participants only)
Hosted by the Asia Cornea Society and the Cornea Society
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
ORGANISED BY:
AND
```
CIC04: Optimizing Outcomes in Toric IOLsTetsuro OSHIKA, GUO Haike, Ronald YEOH
MC06: Flawless Femto LASIK Flaps
MC01: Mastering Femto Phaco Cataract Surgery
MC02: Glued IOL
MC03: From FLEx to SMILE
WL01: Basic Phaco hands-on Wetlab with KITARO Wetlab System
Core Instructional Courses & Masterclasses
CIC01: Phaco Fundamentals
CIC02: Retinal Updates for Anterior Segment Surgeons
CIC03: Ocular Trauma
1100 - 1300 hrs
1330 - 1500 hrs
1530 - 1700 hrs
0830 - 1000 hrs
- All Core Instructional Courses and MasterClasses will be held at SUNTEC Singapore (included in meeting registration) - All Hands-on Wetlab sessions will be held at the Singapore National Eye Centre (separate charge applies)
CIC05: Tips & Tricks for Successful Pterygium Surgery
CIC06: What the Refractive Surgeon Needs to Know about Glaucoma
1045 - 1215 hrsMC04: Finer Points in IOL Fixation
WL02: Basic Phaco with KITARO Wetlab System
WL03: Basic Phaco with KITARO Wetlab System
Hands-on Wetlabs
Log on to www.2013apacrs.org for registration
1345 - 1545 hrs
1600 - 1800 hrs
Learn expert techniques from the best practitioners with our new series of Core Instructional Courses, MasterClasses and Hands-on Wetlabs!
11 July 2013 (Thursday)
11 July 2013 (Thursday)
Ronald YEOH, CHEE Soon Phaik, Gerard SUTTON, Michael KNORZ, Zoltan NAGY
Amar AGARWAL, Athiya AGARWAL, Roger STEINERT, Keiki MEHTA
Johan HUTAURUK, CHEE Soon Phaik, Hadi PRAKOSO, TI Seng Ei
ANG Chong Lye, Manish NAGPAL, LEE Shu Yen, ONG Sze Guan, Ian YEO, Doric WONG, Edmund WONG
Gangadhara SUNDAR, Hunter YUEN, Paul CHEW, S. NATARAJAN
Donald TAN, Jodhbir S. MEHTA, Kimiya SHIMIZU
Cordelia CHAN, Gerard SUTTON, Donald TAN
CHEE Soon Phaik, Ronald YEOH, Roger STEINERT
Shamira PERERA, John CHANG, Prin ROJANAPONGPUN, ZHOU Qi
MC05: Advanced BiometryFAM Han Bor, Wolfgang HAIGIS, John SHAMMAS
CHAN Wing Kwong, Cordelia CHAN, Choun-Ki JOO, WANG Zheng
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
12 July 2013 (Friday)
WL04: DSAEK Hands-on Wetlab1600 - 1800 hrs
Hands-on Wetlab
Donald TAN, LIM Li, Jodhbir S. MEHTA(Limit to 8 participants only)
Hosted by the Asia Cornea Society and the Cornea Society
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
In fact, while standard LASIK
patients experience a “wow”
factor almost immediately post-
op, that effect tends to diminish
with regression over the course
of weeks and months in high
myopes. With Lasik Xtra, it’s just
the opposite, Dr. Tan said. A small
amount of myopia tends to remain
immediately post-op, and vision
continues to improve to plano until
about the three-month follow-up
period, he said.
“The patients tell me they see
better and better,” Dr. Tan said. “So
I am getting late-onset ‘wows.’”
Dr. Tan much prefers late-
onset “wows” to regression, and so
do his patients, he said. Patients
potentially at risk for ectasia (i.e.,
young patients, those with thinner
corneas, etc.) also appreciate
the added potential safety that
crosslinking allows.
in my hands
Normally, corneal ectasia
develops anywhere from two to
four years after LASIK and even as
late as 10 years post-op, Dr. Tan
said.
“This is something very
difficult to predict in normal eyes,”
Dr. Tan said. “So I do [Lasik Xtra]
on all high myopes, and all patients
who have a residual corneal
thickness of 250-300 microns in
the stromal bed underneath the
flap. I tell the patient, ‘I think you
need Lasik Xtra just in case I make
the cornea too weak.’ Most of them
say, ‘If it’s no risk to me, I just get a
bit of insurance.’”
As noted earlier, Dr. Tan also
performs Lasik Xtra on hyperopes.
Normally, Dr. Tan starts out
the LASIK procedure with IntraLase
(Abbott Medical Optics, Santa Ana,
Calif., USA). He makes a 100- to
Strengthening - from page 40
ORGANISED BY:
AND
```
CIC04: Optimizing Outcomes in Toric IOLsTetsuro OSHIKA, GUO Haike, Ronald YEOH
MC06: Flawless Femto LASIK Flaps
MC01: Mastering Femto Phaco Cataract Surgery
MC02: Glued IOL
MC03: From FLEx to SMILE
WL01: Basic Phaco hands-on Wetlab with KITARO Wetlab System
Core Instructional Courses & Masterclasses
CIC01: Phaco Fundamentals
CIC02: Retinal Updates for Anterior Segment Surgeons
CIC03: Ocular Trauma
1100 - 1300 hrs
1330 - 1500 hrs
1530 - 1700 hrs
0830 - 1000 hrs
- All Core Instructional Courses and MasterClasses will be held at SUNTEC Singapore (included in meeting registration) - All Hands-on Wetlab sessions will be held at the Singapore National Eye Centre (separate charge applies)
CIC05: Tips & Tricks for Successful Pterygium Surgery
CIC06: What the Refractive Surgeon Needs to Know about Glaucoma
1045 - 1215 hrsMC04: Finer Points in IOL Fixation
WL02: Basic Phaco with KITARO Wetlab System
WL03: Basic Phaco with KITARO Wetlab System
Hands-on Wetlabs
Log on to www.2013apacrs.org for registration
1345 - 1545 hrs
1600 - 1800 hrs
Learn expert techniques from the best practitioners with our new series of Core Instructional Courses, MasterClasses and Hands-on Wetlabs!
11 July 2013 (Thursday)
11 July 2013 (Thursday)
Ronald YEOH, CHEE Soon Phaik, Gerard SUTTON, Michael KNORZ, Zoltan NAGY
Amar AGARWAL, Athiya AGARWAL, Roger STEINERT, Keiki MEHTA
Johan HUTAURUK, CHEE Soon Phaik, Hadi PRAKOSO, TI Seng Ei
ANG Chong Lye, Manish NAGPAL, LEE Shu Yen, ONG Sze Guan, Ian YEO, Doric WONG, Edmund WONG
Gangadhara SUNDAR, Hunter YUEN, Paul CHEW, S. NATARAJAN
Donald TAN, Jodhbir S. MEHTA, Kimiya SHIMIZU
Cordelia CHAN, Gerard SUTTON, Donald TAN
CHEE Soon Phaik, Ronald YEOH, Roger STEINERT
Shamira PERERA, John CHANG, Prin ROJANAPONGPUN, ZHOU Qi
MC05: Advanced BiometryFAM Han Bor, Wolfgang HAIGIS, John SHAMMAS
CHAN Wing Kwong, Cordelia CHAN, Choun-Ki JOO, WANG Zheng
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
12 July 2013 (Friday)
WL04: DSAEK Hands-on Wetlab1600 - 1800 hrs
Hands-on Wetlab
Donald TAN, LIM Li, Jodhbir S. MEHTA(Limit to 8 participants only)
Hosted by the Asia Cornea Society and the Cornea Society
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
TI Seng Ei, Johan HUTAURUK, Akura JUNSUKE, YC Lee
33-42_EW REAFTIVE.indd 42 25/03/2013 17:13
43EWAP REFRACTIVE March 2013
In fact, while standard LASIK
patients experience a “wow”
factor almost immediately post-
op, that effect tends to diminish
with regression over the course
of weeks and months in high
myopes. With Lasik Xtra, it’s just
the opposite, Dr. Tan said. A small
amount of myopia tends to remain
immediately post-op, and vision
continues to improve to plano until
about the three-month follow-up
period, he said.
“The patients tell me they see
better and better,” Dr. Tan said. “So
I am getting late-onset ‘wows.’”
Dr. Tan much prefers late-
onset “wows” to regression, and so
do his patients, he said. Patients
potentially at risk for ectasia (i.e.,
young patients, those with thinner
corneas, etc.) also appreciate
the added potential safety that
crosslinking allows.
In my hands
Normally, corneal ectasia
develops anywhere from two to
four years after LASIK and even as
late as 10 years post-op, Dr. Tan
said.
“This is something very
diffi cult to predict in normal eyes,”
Dr. Tan said. “So I do [Lasik Xtra]
on all high myopes, and all patients
who have a residual corneal
thickness of 250-300 microns in
the stromal bed underneath the
fl ap. I tell the patient, ‘I think you
need Lasik Xtra just in case I make
the cornea too weak.’ Most of them
say, ‘If it’s no risk to me, I just get a
bit of insurance.’”
As noted earlier, Dr. Tan also
performs Lasik Xtra on hyperopes.
Normally, Dr. Tan starts out
the LASIK procedure with IntraLase
(Abbott Medical Optics, Santa Ana,
Calif., USA). He makes a 100- to
110-micron fl ap.
Dr. Tan applies the ribofl avin
(without dextran) for 45 seconds to
the stroma, rinsing any excess from
the fl ap. Then he puts the fl ap back.
Dr. Tan applies UV light (30
mW/cm2) to the cornea for 45
seconds. Afterward, he waits an
additional minute. That’s it. These
are the only procedural differences
compared to standard LASIK.
For Dr. Tan, this means no
additional time to the LASIK
procedure required.
Normally when Dr. Tan doesn’t
perform Lasik Xtra, after putting
the fl ap back, he waits three
minutes and then fi nishes the
procedure.
“I like to wait three minutes
for my fl ap to really stick on well
so there are no fl ap shifts [during
standard LASIK],” Dr. Tan said. “I
used to wait one minute but then
would occasionally get a few fl ap
shifts. Then I waited two minutes
and rarely would get fl ap shifts.
When I wait three minutes I get
no fl ap shifts. For the last few
thousand cases I have never had a
fl ap shift. So I wait three minutes.
It seems to be a nice magic fi gure
for me.”
Now instead of waiting
three minutes, he performs the
crosslinking component during
this time. With the ribofl avin
component, UVA illumination
component, and added machines
moving about during crosslinking,
the time involved is identical to Dr.
Tan’s standard LASIK procedure.
“It doesn’t increase my time
for surgery at all, at least for my
technique,” Dr. Tan said.
Drawbacks vs. drawbacks
Initially, Dr. Tan said he was
standard LASIK with the MEL 80
excimer laser (Carl Zeiss Meditec)
with no eyes losing more than one
line CDVA. Mean post-op mesopic
contrast sensitivity was either the
same or slightly better than pre-op
at 3, 6, 12, and 18 cpd for all three
populations, using the CSV-1000.
In summary, Presbyond Laser
Blended Vision is a solution for
presbyopia that meets all the
goals of good binocular vision
at all distances, no compromise
in safety, contrast sensitivity,
or night vision, and retention
of functional stereo acuity. The
procedure is immediately reversible
by wearing spectacles, or a simple
retreatment can be done using a
standard excimer laser ablation
with the advantage of keeping the
depth of fi eld. All this is achieved
while simultaneously correcting a
wide range of refractive errors and
astigmatism levels.
he key to this approach
was to base it on the natural
mechanisms of spherical aberration
processing and binocular fusion,
unlike multifocal approaches that
require the patient to adjust to the
unnatural situation of having to
differentiate between two images in
the same eye. EWAP
Editors’ note: Dr. Reinstein practices
at the London Vision Clinic, London,
England, UK, and is affi liated with
the Department of Ophthalmology,
Columbia University Medical College,
New York, NY, USA, and the Centre
Hospitalier National d’Ophtalmologie,
Paris, France. He has fi nancial
interests with Carl Zeiss Meditec and
ArcScan Inc. (Morrison, Colo., USA).
Contact information
Reinstein: +44 020 7224 1005,
Presbyond - from page 37Strengthening - from page 40
using a ribofl avin formula that
included dextran during the Lasik
Xtra procedure.
“When you leave dextran
underneath the fl ap, it causes a
little bit of DLK,” Dr. Tan said.
“With the new formulation of
ribofl avin without dextran—with
just normal saline—there is no
DLK.”
The DLK experienced
previously was mild, grade 1 DLK,
he said.
While the jury is still out
on the long-term effects of
crosslinking, Dr. Tan is convinced
that it is safer than performing
PRK with mitomycin-C, another
refractive surgery option for higher
myopia that reduces the risk of
ectasia.
“If you have a choice between
crosslinking and mitomycin-C,
mitomycin-C is more dangerous,”
he said.
Meanwhile, Lasik Xtra is a
better option than the Visian ICL
(STAAR Surgical, Monrovia, Calif.,
USA) for many cases in Singapore,
he said.
Dr. Tan described the typical
Singaporean myope as having
“long eyeballs and anterior
chambers that are too shallow for
the Visian ICL.
If I try to [implant a Visian ICL]
in Singapore, the anterior chamber
is going to be too small.”
Referring to Lasik Xtra, Dr. Tan
said, “If there is no downside, why
not do it?” EWAP
Editors’ note: Dr. Tan has no fi nancial
interests related to this article.
Contact information
Tan: +65 6738 8122,
,
33-42_EW REAFTIVE.indd 4333-42_EW REAFTIVE.indd 43 22/03/2013 16:3422/03/2013 16:34
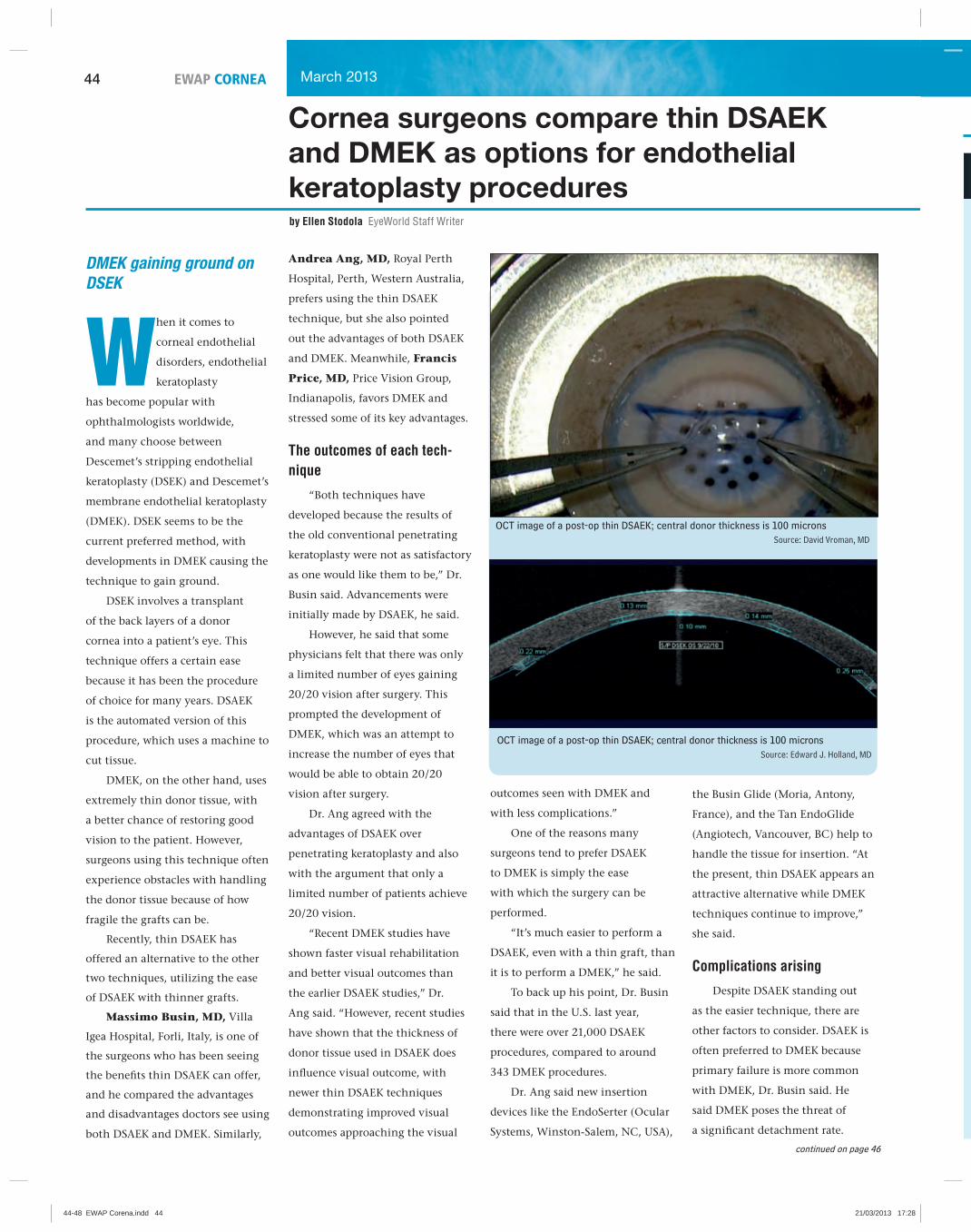
44 EWAP CORNEA March 2013
Cornea surgeons compare thin DSAEK and DMEK as options for endothelial keratoplasty procedures by Ellen Stodola EyeWorld Staff Writer
DMEK gaining ground on
DSEK
When it comes to
corneal endothelial
disorders, endothelial
keratoplasty
has become popular with
ophthalmologists worldwide,
and many choose between
Descemet’s stripping endothelial
keratoplasty (DSEK) and Descemet’s
membrane endothelial keratoplasty
(DMEK). DSEK seems to be the
current preferred method, with
developments in DMEK causing the
technique to gain ground.
DSEK involves a transplant
of the back layers of a donor
cornea into a patient’s eye. This
technique offers a certain ease
because it has been the procedure
of choice for many years. DSAEK
is the automated version of this
procedure, which uses a machine to
cut tissue.
DMEK, on the other hand, uses
extremely thin donor tissue, with
a better chance of restoring good
vision to the patient. However,
surgeons using this technique often
experience obstacles with handling
the donor tissue because of how
fragile the grafts can be.
Recently, thin DSAEK has
offered an alternative to the other
two techniques, utilizing the ease
of DSAEK with thinner grafts.
Massimo Busin, MD, Villa
Igea Hospital, Forli, Italy, is one of
the surgeons who has been seeing
the benefi ts thin DSAEK can offer,
and he compared the advantages
and disadvantages doctors see using
both DSAEK and DMEK. Similarly,
Andrea Ang, MD, Royal Perth
Hospital, Perth, Western Australia,
prefers using the thin DSAEK
technique, but she also pointed
out the advantages of both DSAEK
and DMEK. Meanwhile, Francis
Price, MD, Price Vision Group,
Indianapolis, favors DMEK and
stressed some of its key advantages.
The outcomes of each tech-nique
“Both techniques have
developed because the results of
the old conventional penetrating
keratoplasty were not as satisfactory
as one would like them to be,” Dr.
Busin said. Advancements were
initially made by DSAEK, he said.
However, he said that some
physicians felt that there was only
a limited number of eyes gaining
20/20 vision after surgery. This
prompted the development of
DMEK, which was an attempt to
increase the number of eyes that
would be able to obtain 20/20
vision after surgery.
Dr. Ang agreed with the
advantages of DSAEK over
penetrating keratoplasty and also
with the argument that only a
limited number of patients achieve
20/20 vision.
“Recent DMEK studies have
shown faster visual rehabilitation
and better visual outcomes than
the earlier DSAEK studies,” Dr.
Ang said. “However, recent studies
have shown that the thickness of
donor tissue used in DSAEK does
infl uence visual outcome, with
newer thin DSAEK techniques
demonstrating improved visual
outcomes approaching the visual
OCT image of a post-op thin DSAEK; central donor thickness is 100 micronsSource: Edward J. Holland, MD
OCT image of a post-op thin DSAEK; central donor thickness is 100 micronsSource: David Vroman, MD
outcomes seen with DMEK and
with less complications.”
One of the reasons many
surgeons tend to prefer DSAEK
to DMEK is simply the ease
with which the surgery can be
performed.
“It’s much easier to perform a
DSAEK, even with a thin graft, than
it is to perform a DMEK,” he said.
To back up his point, Dr. Busin
said that in the U.S. last year,
there were over 21,000 DSAEK
procedures, compared to around
343 DMEK procedures.
Dr. Ang said new insertion
devices like the EndoSerter (Ocular
Systems, Winston-Salem, NC, USA),
the Busin Glide (Moria, Antony,
France), and the Tan EndoGlide
(Angiotech, Vancouver, BC) help to
handle the tissue for insertion. “At
the present, thin DSAEK appears an
attractive alternative while DMEK
techniques continue to improve,”
she said.
Complications arising
Despite DSAEK standing out
as the easier technique, there are
other factors to consider. DSAEK is
often preferred to DMEK because
primary failure is more common
with DMEK, Dr. Busin said. He
said DMEK poses the threat of
a signifi cant detachment rate.
continued on page 46
44-48 EWAP Corena.indd 4444-48 EWAP Corena.indd 44 21/03/2013 17:2821/03/2013 17:28

45EWAP CORNEAMarch 2013
D
D
o
n
Views from Asia-Pacifi cAlvin Lerrmann YOUNG, MDChief of Service, Department of Ophthalmology & Visual Sciences, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong SARTel. no. +852-26322878Fax no. [email protected]
There has been a major paradigm shift in the fi eld of corneal transplantation since the advent of modern endothelial keratoplasty. The popularity of the technique has been widespread. One of the main reasons for this immense positive response about this surgery is the relative ease of performing the whole procedure. In the earlier days, DLEK (deep lamellar endothelial keratoplasty) surgery was technically more demanding and diffi cult hence subsequently replaced by DSEK. Most corneal surgeons are now using DSEK or DSAEK depending upon the availability of an automated micokeratome or precut tissue in their set up. More recently, the focus of discussion has shifted to the use of thin donor lenticules, consequently bringing ultra-thin DSAEK and DMEK to the forefront. However, there are certain pertinent issues that need to be considered before these relatively new surgeries can be adopted. Obtaining a thin-cut donor lenticule or only the Descemet’s membrane (in DMEK) can be a diffi cult proposition resulting in inadvertent wastage of human tissue, which certainly is not affordable in countries where there is an obvious dearth of donor corneas. In addition, using two microkeratome heads for ultra-thin DSAEK lenticules would impose extra fi nancial burden in less affl uent economies and especially when these heads are disposable. Furthermore, Asian eyes are commonly found to have shallow anterior chambers, limiting the freedom of movement inside the eye when the surgeon in trying to “center” or orientate a very thin donor lenticule. The situation becomes worse if another intervention, such as refl oating the graft, is required.
At the moment, there is still a relative scarcity of reports on excellent visual outcomes after thin lenticule DSAEK or DMEK. In the absence of any long-term comparative clinical trials, one needs to weigh the benefi ts and risks that are local in terms of graft availability, preparation, wastage rate, patient factors and surgeons’ expertise in deciding whether or not to adopt thin lenticule DSAEK, DMEK, or to ‘settle with’ a fairly confi dently attainable visual acuity of 20/30 with conventional DSEK/DSAEK. As mentioned earlier, the ease of performing a conventional DSEK/DSAEK is one of the highlights of this surgery. Further research and refi nement towards innovation of better technology and techniques aiming toward the better and safer preparation of donor material (perhaps best served by an eye bank), surgical handling of donor and its insertion are warranted.
Editors’ note: Dr. Young acknowledges the kind assistance of Dr. Vishal Jhanji in writing his comments. Dr. Young has no fi nancial interests related to his comments.
Tae-Im KIM, MDAssociate Professor, Yonsei University, Dept. of Ophthalmology, 50 Yonsei-ro, Seodaemun-gu, Seoul, KoreaTel. no. +82-2-2228-3570Fax no. [email protected]
Over the years, keratoplasty has been developed and has recently diversifi ed from penetrating keratoplasty (PK) to refi ned lamellar keratoplasty. Anterior stromal corneal abnormality was corrected by lamellar keratoplasty or deep lamellar keratoplasty using various techniques. The posterior part of the cornea abnormality, mainly related with endothelial dysfunction, was treated by selective replacement of diseased recipient endothelium via Descemet’s stripping endothelial keratoplasty (DSEK) or Descemet’s membrane endothelial keratoplasty (DMEK).
In Descemet’s stripping automated endothelial keratoplasty (DSAEK), the outer layers of the cornea are skimmed off using a mechanical microkeratome, leaving a very thin layer of stromal fi bers supporting the inner Descemet’s membrane and the endothelial cells. The bottom 20% of divided cornea is used for DSAEK and the top 80% can be used as donor tissue for anterior lamellar transplants. Automated cutting improves the donor preparation procedure with smooth cut surfaces and predictable thickness. The quality of the visual recovery after DSAEK is generally better than that achieved by a penetrating graft. The stability of the refraction and rapid visual rehabilitation are major advantages of all endothelial keratoplasty techniques. However, because of the remaining stromal tissue and the interface, DSAEK still shows suboptimal visual acuity and relatively slow visual rehabilitation. Also, expensive equipment and a drop in donor endothelial cell density in the early postoperative period remain drawbacks. In an attempt to overcome these limitations, pioneering corneal surgeons have invented the donor preparation surgical procedure to minimize the remaining stromal tissue. The donor Descemet’s membrane is scored and trephined from the endothelial side without any donor corneal stroma. Also, there is no need for an artifi cial anterior chamber or a microkeratome in the donor tissue preparation. This DMEK procedure can accelerate the recovery and increase the chance of obtaining 20/20 vision postoperatively. Moreover, the rate of rejection with DSAEK can be successfully reduced by minimizing antigen exposure. However, DMEK is a more challenging procedure than established DSAEK surgery. DMEK has the potential of infl icting damage to the donor endothelium and Descemet’s membrane during the surgical preparation and introduction into the anterior chamber.
The pros and cons of each advanced posterior lamellar replacement procedure have been proven. However, apart from the results of each procedure, an important factor in selecting particular surgical technique is the experience of the operating surgeon. Even though the surgical outcome of DMEK is superior in many aspects, the surgeon with lack of surgical experience and limited skills may elect not to choose DMEK. Too aggressive trial of a diffi cult procedure may induce signifi cant added cost to this surgery.
In the near future, better surgical techniques and instruments will be introduced to facilitate DMEK procedure without jeopardizing the surgical outcome. Until then, DSAEK will account for a great part of posterior lamellar procedures.
Editors’ note: Dr. Kim has no fi nancial interests related to her comments.
46
44-48 EWAP Corena.indd 4544-48 EWAP Corena.indd 45 21/03/2013 17:2821/03/2013 17:28

46 EWAP CORNEA March 2013
However, he also said DMEK
typically has a lower rejection rate.
Dr. Ang said “safety in
donor preparation and easier
manipulation of the tissue in the
anterior chamber” is a factor that
continues to make the DSAEK
technique more popular. “The
challenge for thin DSAEK is for
the eye banks to come up with
techniques to provide reproducible
and accurate thin tissue,” she said.
Tissue loss and possibility
of endothelial cell loss because
of diffi culties manipulating the
delicate tissue were two possible
risks with DMEK that Dr. Ang
cited. “Solutions to these problems
need to be found in order to make
DMEK the procedure of choice for
endothelial replacement,” she said.
Technique preferences
Dr. Busin said he is currently
seeing a trend toward thin
DSAEK, his preferred method.
This allows for thinner grafts and
thinner incisions with the DSAEK
procedure. However, he said that
some people may not trust this
method yet, which could be why
some are leaning toward DMEK. He
said in the future he expects to see
people favoring thin DSAEK.
“The ease of surgery and the
outcome, which is more or less
the same, would convince them
to move from DMEK back to thin
DSAEK grafts,” Dr. Busin said.
Likewise, Dr. Ang also said thin
DSAEK is presently her procedure
of choice. “This technique results
in excellent visual outcomes, is
technically less demanding than
DMEK, and has fewer complications
than DMEK at present,” she said.
Dr. Price said he prefers the
DMEK technique, although he
still sometimes uses DSAEK. “If
it’s a non-complicated case, we
recommend DMEK,” he said. After
nearly fi ve years using DMEK,
there are a number of reasons
he favors it. He said better vision
results are evident with DMEK.
Another reason is rejection rates are
signifi cantly lower with DMEK. He
said in a cumulative look at DMEK
for a two-year period, the rejection
rate was less than 1%, compared to
about 12% for DSAEK.
He said thin DSAEK does offer
some similarities to DMEK. “I think
the thinner it gets, the closer you’re
going to get to DMEK,” he said. But
the question, he said, is how close
you can get and how reliable the
thin DSAEK would be. Dr. Price
said he stopped using thin DSAEK
because of signifi cant tissue loss
in donor preparation. Currently
DMEK donor loss rates are less
than 1%; it will be interesting
to see if donor loss rates will be
that low if all donor preparations
for DSAEK are for thin cuts, as
there is always some irregularity
and unpredictability with
microkeratome cuts.
Endothelial replacement future
Endothelial keratoplasty has
evolved over the years, Dr. Ang said.
“The next phase will be cultured
donor endothelial cell seeding of
diseased corneas,” she said. “The
ability to culture and expand donor
endothelial cells will increase
the donor supply, especially in
countries with limited supply.
These cells could be transplanted
either as an injection-based therapy
or on a carrier.” EWAP
Editors’ note: Dr. Busin has fi nancial interests with Moria. Drs. Ang and Price have no fi nancial interests related to this article.
Contact informationAng: [email protected]: [email protected]: [email protected]
L
tr
p
Tm
gr
Th
St
tr
en
co
at
da
in
da
“R
ar
Cornea - from page 44
LASIKSurgery
• Thin, 100-micron, planar flaps
• Accuracy and predictability equivalent to Femto-SBK
• Smoother stromal bed
• No femto-complications
• … At a fraction of the cost
Think Thin
SBK without femto-furrow
James Lewis, MD(Elkins Park, PA, USA)
44-48 EWAP Corena.indd 4644-48 EWAP Corena.indd 46 21/03/2013 17:2821/03/2013 17:28
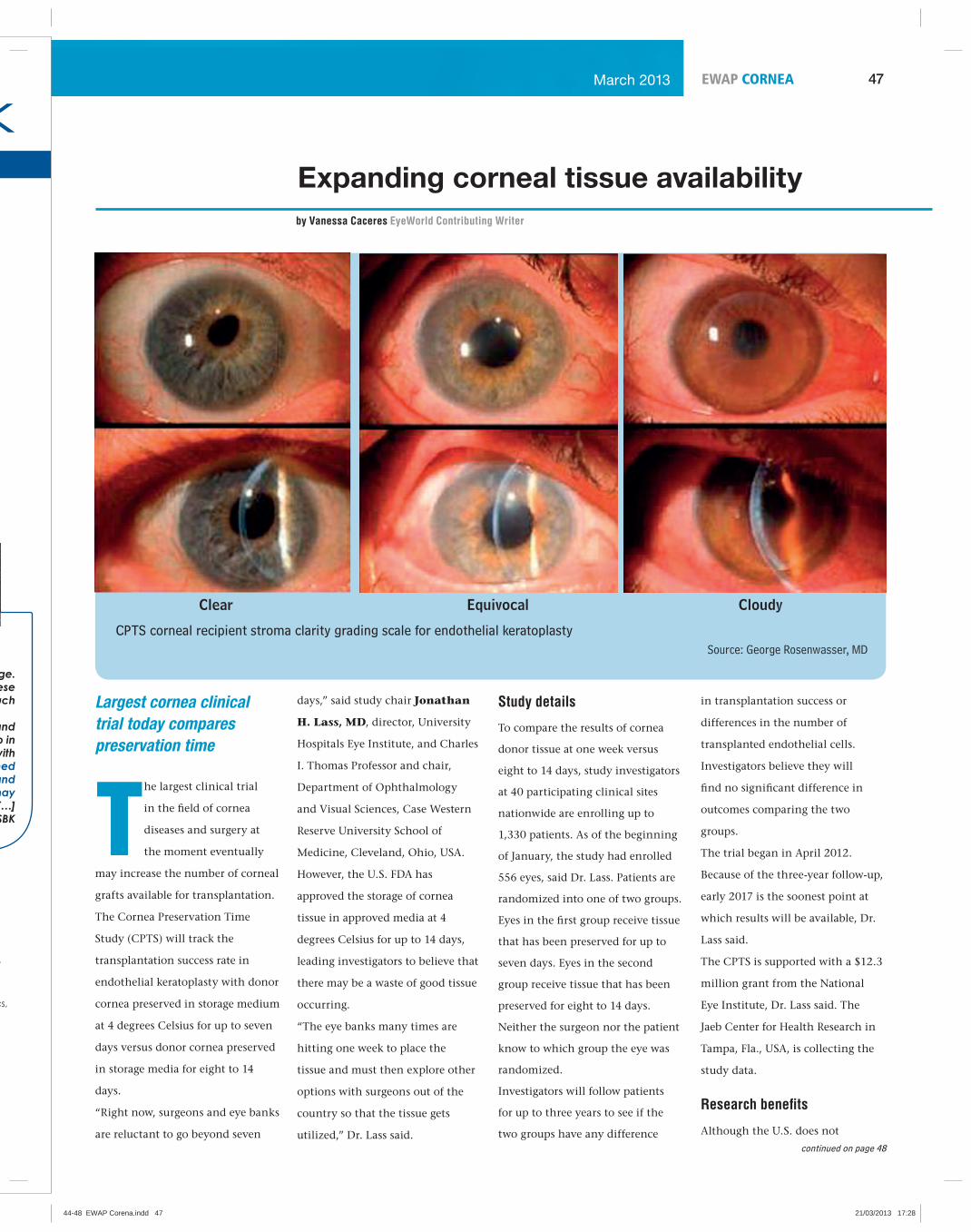
47EWAP CORNEAMarch 2013
Expanding corneal tissue availability
Largest cornea clinical
trial today compares
preservation time
The largest clinical trial
in the fi eld of cornea
diseases and surgery at
the moment eventually
may increase the number of corneal
grafts available for transplantation.
The Cornea Preservation Time
Study (CPTS) will track the
transplantation success rate in
endothelial keratoplasty with donor
cornea preserved in storage medium
at 4 degrees Celsius for up to seven
days versus donor cornea preserved
in storage media for eight to 14
days.
“Right now, surgeons and eye banks
are reluctant to go beyond seven
by Vanessa Caceres EyeWorld Contributing Writer
days,” said study chair Jonathan
H. Lass, MD, director, University
Hospitals Eye Institute, and Charles
I. Thomas Professor and chair,
Department of Ophthalmology
and Visual Sciences, Case Western
Reserve University School of
Medicine, Cleveland, Ohio, USA.
However, the U.S. FDA has
approved the storage of cornea
tissue in approved media at 4
degrees Celsius for up to 14 days,
leading investigators to believe that
there may be a waste of good tissue
occurring.
“The eye banks many times are
hitting one week to place the
tissue and must then explore other
options with surgeons out of the
country so that the tissue gets
utilized,” Dr. Lass said.
Study details
To compare the results of cornea
donor tissue at one week versus
eight to 14 days, study investigators
at 40 participating clinical sites
nationwide are enrolling up to
1,330 patients. As of the beginning
of January, the study had enrolled
556 eyes, said Dr. Lass. Patients are
randomized into one of two groups.
Eyes in the fi rst group receive tissue
that has been preserved for up to
seven days. Eyes in the second
group receive tissue that has been
preserved for eight to 14 days.
Neither the surgeon nor the patient
know to which group the eye was
randomized.
Investigators will follow patients
for up to three years to see if the
two groups have any difference
in transplantation success or
differences in the number of
transplanted endothelial cells.
Investigators believe they will
fi nd no signifi cant difference in
outcomes comparing the two
groups.
The trial began in April 2012.
Because of the three-year follow-up,
early 2017 is the soonest point at
which results will be available, Dr.
Lass said.
The CPTS is supported with a $12.3
million grant from the National
Eye Institute, Dr. Lass said. The
Jaeb Center for Health Research in
Tampa, Fla., USA, is collecting the
study data.
Research benefi ts
Although the U.S. does not
Clear Equivocal Cloudy
CPTS corneal recipient stroma clarity grading scale for endothelial keratoplastySource: George Rosenwasser, MD
continued on page 48
44-48 EWAP Corena.indd 4744-48 EWAP Corena.indd 47 21/03/2013 17:2821/03/2013 17:28

48 EWAP CORNEA March 2013
currently have a shortage of donor
corneas, there could be numerous
benefi ts if the study shows that
the longer storage time is just as
effective as the shorter storage time.
First, there’s an expected increase
in demand for corneal tissue as
the U.S. population ages, Dr. Lass
said. “If we can show preservation
time doesn’t make a difference, we
could double the supply that people
would be willing to use,” he said.
In addition, the donor pool is
at a greater risk from emerging
infections like the West Nile virus,
and the eye banks need more
time to screen donors because
of the concerns about infections
surrounding drug addiction,
including hepatitis B.
This kind of research will provide
actual evidence regarding best
practices for corneal preservation
timing and usage, Dr. Lass said.
“We want to have an evidence-
based approach to deal with
perceptions surrounding the
donor cornea and provide greater
fl exibility for eye banks in placing
tissue,” he explained.
George Rosenwasser, MD,
Central Pennsylvania Eye Institute,
Hershey, Pa., USA, whose practice
is participating in the trial, is eager
to see if the results provide proof
that the longer preservation time
is just as clinically acceptable as
the shorter preservation time. He
routinely has used tissue that has
been preserved for 10 to 11 days
and has found no difference in
outcomes or quality compared with
tissue preserved for a shorter time.
Currently, the U.S. has the most
organized eye banking process
in the world and often shares its
excess supply around the world,
said Kevin Ross, president and
CEO, Midwest Eye-Banks, Ann
Arbor, Mich., USA. There were
about 46,000 corneal transplants
performed in the U.S. in 2011,
according to Eye Bank Association
of America statistics, Mr. Ross said.
However, there were 67,590 donor
tissues available in 2011. The tissue
that are not used—for 2011, that
was a little over 30%—are typically
shipped overseas.
Although the U.S. does not have a
shortage of donor tissue, there’s a
“tremendous shortage” elsewhere,
Mr. Ross said. “There are about
100,000 to 150,000 corneal grafts
in the world each year,” Mr. Ross
said. “The number needed is closer
to a million.”
The CPTS results may help close
that gap. “We could provide a major
benefi t for the restoration of sight
in many places, fi rst and foremost
in the U.S. This could also give us
the opportunity to support corneal
surgery programs around the
world,” Mr. Ross said, noting that
many U.S. eye banks are involved
with supporting cornea surgery
programs globally.
That said, if the U.S. has an
increasing need for donor tissue,
the study results could help meet
the demand in the U.S., Dr. Lass
said.
The results will affect eye banks’
policies and procedures that guide
for how long donor tissue can be
used, Mr. Ross added. They also will
likely affect tissue criteria selection
worldwide, he said.
The study is actively recruiting
patients between the ages of 30 and
<91. Patients at participating centers
with either Fuchs’ dystrophy or
Expanding - from page 47
pseudophakic bullous keratopathy
undergoing Descemet’s stripping
endothelial keratoplasty (DSEK)
must be available for follow-ups at
one day, one week, one month, and
six months, and one, two, and three
years. The study’s website is cpts.
jaeb.org. EWAP
Editors’ note: The physicians have no fi nancial interests related to this article.
Contact informationLass: 216-844-8590, [email protected]
Rosenwasser: 717-533-5200, [email protected]
Ross: 734-780-218, [email protected]
44-48 EWAP Corena.indd 4844-48 EWAP Corena.indd 48 21/03/2013 17:2821/03/2013 17:28
49EWAP GLAUCOMA March 2013
Studies highlight the relationship between diet and glaucoma
Can what we eat increase
our risk of getting
glaucoma? A trio of
studies presented at this
year’s American Glaucoma Society
meeting suggested that the answer
might be yes.
The pathophysiology of
glaucoma is poorly understood.
The primary risk factor, IOP, has
a complex relationship with the
disease, being frequently elevated
but neither necessary nor suffi cient
to explain the majority of cases of
glaucoma. Based on the high risk
of glaucoma among fi rst-degree
relatives, a genetic basis is strongly
suspected. Major genetic studies,
however, have failed to fi nd a gene
or genes that account for more than
a small percentage of primary open-
angle glaucoma cases. This has
led many to speculate that gene-
environment interactions may be at
play. This is a two-hit mechanism
of sorts: having the gene isn’t
enough—one must also have a
specifi c environmental exposure.
To date, the nature of such an
environmental factor has been
unknown. New data suggests that it
might be diet-related.
Nutrients and oxidative stress“Oxidative stress may be an
important component of the
pathophysiology of glaucoma,”
said Sophia Wang, BA, medical
student, University of California-
San Francisco, Calif., USA. Calcium
and iron, she said, are two dietary
elements that play a role in the
formation of highly reactive oxygen
species that can damage tissues. She
proposed that high dietary intake
of these nutrients, coupled with
impaired regulation of homeostatic
regulatory processes due to aging,
could lead to damage to the
trabecular meshwork, loss of retinal
ganglion cells, and the clinical
manifestations of glaucoma.
To explore this hypothesis, Ms.
Wang conducted a cross-sectional
epidemiologic study utilizing the
National Health and Nutrition
Examination Surveys
(NHANES) database, which
contains detailed information on
the dietary intake of large numbers
of Americans as well as their
glaucoma status by self-report.
“We analyzed data from 3,833
adult Americans, of whom 248
self-reported having glaucoma,” she
said.
Ms. Wang found that people
consuming the highest levels of
calcium—more than 800 mg/
day—were 2.4 times more likely to
self-report having glaucoma than
those consuming the lowest levels
of calcium. Also, people consuming
the highest levels of iron—more
than 18 mg/day—were 3.8 times
more likely to self-report glaucoma
than those consuming the lowest
levels of iron.
People consuming the highest
levels of both calcium and iron, she
said, had a 7.2 fold higher odds of
glaucoma.
Louis Pasquale, MD,
Massachusetts Eye and Ear
Infi rmary, Boston, Mass., USA,
said, “This is the fi rst human data
in support of an oxidative stress
mechanism in glaucoma.”
Can diet infl uence the risk of glaucoma?by Tony Realini, MD
CaffeineDr. Pasquale has studied the
incidence of pseudoexfoliation
glaucoma between 1980 and 2008
and its relationship to caffeine
intake utilizing the Nurses Health
Study database. This database
included data on nutritional
intake as well as fi ndings on eye
examinations. He identifi ed 300
new cases of pseudoexfoliation
glaucoma among 1.6 million
person-years of follow-up.
“We observed a positive
association between overall caffeine
intake and pseudoexfoliation
that was not quite statistically
signifi cant,” he said. But for those
who get their caffeine specifi cally
from coffee—drinking at least
three cups a day—the risk of
pseudoexfoliation was 63% higher
than for non-coffee drinkers.
Interestingly, the effect of
caffeine intake was modifi ed by
family history. “Among those
consuming the highest levels of
caffeine, people who also had a
family history of glaucoma had a
2.9-fold higher risk of glaucoma,
compared to only a 1.2-fold
increase for those without a family
history,” he said.
This supports the concept of
a gene-environment interaction
for caffeine and pseudoexfoliation
glaucoma, he said.
Caffeine and IOPTo evaluate how caffeine might
affect glaucoma, Aliya Jiwani, in
collaboration with Dr. Pasquale and
others, conducted a randomized
trial to explore caffeine’s effect on
IOP and ocular perfusion pressure
(OPP) in healthy subjects, glaucoma
suspects, and patients with both
low-tension and high-tension
glaucoma.
In their crossover study,
patients drank an 8-oz. cup of
caffeinated coffee at one visit
and an 8-oz. cup of decaffeinated
coffee at a second visit, in a
randomized order. IOP and OPP
were determined before and 60 and
90 minutes after each beverage.
Compared to decaffeinated
coffee, caffeinated coffee raised IOP
by 1 mmHg at both time points,
and raised OPP by 1.6 mmHg and
1.3 mmHg at 60 and 90 minutes,
respectively. Although the changes
were statistically signifi cant, she
said, the effect size was quite small.
“Consuming a single 8-oz. cup
of caffeinated coffee likely does not
clinically impact IOP or OPP,” she
concluded.
Dr. Pasquale agreed. “This is the
beginning of a conversation about
the role of environmental factors
associated with the development
of glaucoma,” he said. “It is still
too early to begin recommending
lifestyle changes for our glaucoma
patients.”
But he sees the potential for
signifi cant progress in this research
area in the future. “We may be
able to prevent pseudoexfoliation
glaucoma in the decades to come,”
Dr. Pasquale said. EWAP
Editors’ note: Ms. Wang has no
fi nancial interests related to this
article.
Contact information
Jiwani: [email protected]
Pasquale:
Wang: [email protected]
49-50_ EWAP Glaucoma.indd 4949-50_ EWAP Glaucoma.indd 49 21/03/2013 17:2921/03/2013 17:29

50 EWAP GLAUCOMA March 2013
New technology could improve eye drop deliveryby Ellen Stodola EyeWorld Staff Writer
New delivery system
seeks to address the
need for more effective
administration of
medication
The eye dropper is a
technology that has
changed relatively little
over time, but many
doctors have recently seen a need
to adapt the device to make it more
effective for patients attempting to
use it to administer medications.
Sean Ianchulev, MD, clinical
associate professor, University
of California, San Francisco,
Calif., USA, recently presented on
results of a study for the new eye
droplet device being developed by
Corinthian Ophthalmic (Raleigh,
NC, USA). The new delivery system
would work to remedy some of the
obstacles to patients trying to use
eye droppers as a means to deliver
medication to the eyes. Mark
Packer, MD, clinical associate
professor of ophthalmology, Oregon
Health & Science University,
Portland, Ore., USA, also worked
on the fi ndings for the new
technology. Meanwhile, Alan L.
Robin, MD, associate professor of
ophthalmology and international
health, Johns Hopkins University,
Baltimore, Md., USA, weighed in on
what an eye drop delivery system
would need to do to be effective.
Problems with current technology
“If you look at the history
of people trying to develop
alternatives to eye drops, this is
not new,” Dr. Ianchulev said. Over
the years, people have explored
sprays and other ways to get drops
or medication inside the eye
because of the challenges associated
with the eye dropper. One of the
major issues, Dr. Ianchulev said, is
overdosing; this can cause problems
with preservative overexposure of
the ocular surface or in the case of
topical beta-blockers, systemic side
effects such as shortness of breath,
depression, fatigue, and dizziness.
Another problem is that people
often blink while trying to use
eye drops or cannot instill them
directly into the eye. Compared to
oral or intravenous drug delivery,
topical eye drops are notoriously
challenging in terms of dosing
accuracy. What physicians prescribe
is actually quite different from what
people get.
“Eye drops have been around
for hundreds of years,” Dr. Robin
said. “They are a lousy delivery
system for many reasons.” He
said eye drops pose a problem for
those who rely on caregivers to
administer eye drops for them. He
also cited problems of getting a
drop into the eye.
What a new system needsDr. Robin said there several
things a new system would need.
“It has to be relatively inexpensive,”
he said. “It has to be reusable so
that you can put any bottle in it,”
he said, referring to one system that
would take a variety of medications
and refi lls. He said the medicine
would also have to be able to be
administered to the patient without
getting contaminated.
Dr. Robin highlighted the
importance of a patient being able
to use the system with ease. “It has
to have some guidance system, a
focusing light or something that
would allow patients to aim it on
Corinthian Ophthalmic’s Whisper device spray dispenses smaller doses than a generic eyedropper, with controlled dosing and ejection for better accuracy of administration.
Corinthian Ophthalmic’s Whisper device spray dispenses smaller doses than a generic eyedropper, with con-trolled dosing and ejection for better accuracy of administration.
Sean Ianchulev, MD
their eyeball,” he said. There would
need to be a way of administering a
specifi c amount and making sure it
gets to the eye, he said, as well as a
way to keep the eye open.
The new technologyDr. Ianchulev said with the
new technology, one focus has
been improving the directionality
of the fl ow. In addition, speed is
something that was considered
with the new droplet technology.
He said the speed of delivery is
faster than the blink rate, which
would allow the medication to get
to the eye before a person has the
chance to blink.
The LED display improves
positioning and targeting. “They
solve a lot of the issues of how to
deliver medication to the eye and
improve the accuracy and effi cacy
of delivery,” he said.
Examining initial resultsThough still in research
and initial stages, Dr. Ianchulev
said results so far have been
encouraging. “I think it was
surprising to us, the results that we
saw,” he said about presenting some
of the fi rst human data.
Results from just over 100
people compared dilation between
the new technology and the current
eye drop method. Dr. Packer said
with the pupil dilation study it
was not exactly clear what size
dose would work best, so it was
tested with the microdroplets of
1.5 microliters, 6 microliters, and
two sprays of 3 microliters each. He
said all of these quantities showed
effective dilation.
Interest in the technologyDr. Ianchulev said the new
technology is not yet commercially
available anywhere; in terms of
when it will become available, he
said it will likely be different for
each country. “The company is
working on collaborations with the
different pharmaceutical companies
so they can formulate or package
their eye drops with this new
technology,” he said.
“This is the only technology
since several hundred years ago
when people invented the eye
dropper, and we know the eye
dropper has major challenges,”
Dr. Ianchulev said. “So if you’re a
pharmaceutical company, especially
in a very competitive space, that
wants to have a better technology
out there and a differentiated
technology, this could be a huge
ad
w
th
w
L
fu
te
fo
pa
pr
co
ad
bu
to
“B
an
it
in
be
ut
te
w
in
be
90
w
re
th
ph
li
w
w
bu
m
is
h
co
h
EdinDwRore
CIa
Pa
R
continued on page 52
49-50_ EWAP Glaucoma.indd 5049-50_ EWAP Glaucoma.indd 50 21/03/2013 17:2921/03/2013 17:29

51EWAP DEVICES March 2013
When it comes to choosing
instrumentation to make
incisions, variables
between disposable and
reusable blades make a
difference
Disposable or reusable?
Diamond, sapphire,
metal, or silicone?
Depending on the type
of surgery, the amount of surgical
expertise, or the physical location
of the operating room, different
blades have different advantages.
Generally speaking, diamond and
sapphire blades are reusable and
more expensive than their metal or
silicone disposable counterparts. For
some surgeons, the location of the
surgery is the determining factor
about which blade to use.
“In my own practice, I used
to use diamond blades. But at
the surgery center, where there
are multiple users of a single
diamond blade, I started noticing a
signifi cant difference in sharpness
from one day to the next,” said
Ayman Naseri, MD, chief,
Ophthalmology Surgical Service,
San Francisco Veteran’s Affairs
Medical Center, and associate
professor of clinical ophthalmology,
University of California-San
Francisco, Calif., USA. The
inconsistent quality of the diamond
tip “got frustrating,” he said, as
he was forced to change how he
constructed a wound and the
amount of pressure he would use in
a split second.
Although Uday Devgan,
MD, in private practice, Los
Not all blades serve all purposesby Michelle Dalton EyeWorld Contributing Editor
continued on page 52
Angeles, Calif., USA, and chief
of ophthalmology, Olive View–
UCLA Medical Center, uses both
a diamond blade and the newer
femtosecond lasers in his practice,
when he’s teaching residents he
prefers they use a steel blade, and
cost is not the main reason.
“With a steel blade, no matter
how sharp it is, there’s a tactile
feedback that is benefi cial to
residents,” he said. “No matter how
sharp the blade is, the incision will
be slower and have more resistance
than with a diamond blade.” Steel
blades “require more effort to enter
the eye,” Dr. Devgan said.
Deciding on blade typeDiamond blades can be too
sharp for a particular incision,
said Steven G. Safran, MD, in
private practice, Lawrenceville, NJ,
USA. He uses a diamond blade for
the paracentesis, when he needs to
use iris hooks, or when he makes
a groove incision for scleral fl aps.
For his main incision, however
(which ranges from 2.2 to 2.8 mm
depending upon which machine
This phaco incision intentionally nicks the limbal vessels to provide better long-term healing. It was created with a femtosecond laser in an anatomic pattern that is diffi cult to replicate with a manual blade.
Source: Uday Devgan, MD
A diamond keratome is used to make a corneal incision. Note the line across the tip of the blade that represents the piercing of Descemet’s membrane. The incision is nearly square with dimensions that ensure optimal sealing, minimal induced astigmatism, and adequate access to the anterior segment during surgery.
While this blade is made of a gem-quality diamond, its thinness causes it to be somewhat brittle, and care must be taken during handling. With proper care, these blades can undergo 1,000 or more uses between maintenance.
he’s using), he prefers metal blades.
“I think it’s easier to make a
well-constructed incision with a
metal blade because diamonds are
actually too sharp,” he said, and
can cut the fl ap on the side. He
prefers a technique of making a
little groove, paralleling the cornea,
and then bevelling down.
At the surgery center, the staff
are “much better at handling the
diamond blades than they are at
the hospital—in the hospital, often
break and are more likely to be
dropped,” Dr. Safran said, adding
those reasons to why he opts
for disposable blades in hospital
settings.
The variability in diamond
blade sharpness at the VA hospital
was also a problem for Dr. Naseri in
training residents. In Dr. Naseri’s
opinion, steel blades offer more
consistency with their sharpness,
and diamond blades can be
inconsistent. The last diamond
blade he used was trapezoidal,
which presented issues with side-
cutting elements in creating a
multiplanar incision.
“Uniplanar incisions that
cut in the same plane don’t pose
a problem for blades with side-
cutting features, but multiplanar
incisions change the plane of the
cut in the cornea,” Dr. Naseri said,
and this can lead to specifi c wound
fl aws.
In resident cases, he has
changed from a multiplanar
incision created with a diamond
blade to a single-plane incision
created with a metal blade. Dr.
Naseri found that the residents
were forced to push too hard with
a dull diamond blade, yet the same
amount of force was problematic
if they were using a sharp
diamond blade. Dr. Naseri said
the consistency of the metal blade
sharpness has improved resident
incision construction.
Dr. Safran typically uses
disposable blades for scleral fl aps,
but likes that a diamond blade can
be used to more easily create a fl ap
that starts at the limbus but moves
away from him. Generally, however,
51-52 EWAP Devices.indd 5151-52 EWAP Devices.indd 51 21/03/2013 17:3021/03/2013 17:30
52 EWAP DEVICES March 2013
New - from page 50Not - from page 51
advantage, particularly, since this
would not require reformulation of
the existing drugs, including those
with higher viscosity.”
Looking to the futureDr. Ianchulev said he thinks the
future looks positive for this sort of
technology. He said it’s important
for physicians to be certain that
patients are getting the medication
prescribed to them.
Dr. Packer agreed that this
could not only benefi t the
administration of drops to the eye
but also the ability for physicians
to track compliance in patients.
“Because this device is electronic
and it’s built like a microprocessor,
it can gather and communicate
information,” he said. “So it would
be possible to track patients’
utilization of their medications.”
Another advantage of the new
technology, Dr. Ianchulev said,
would be that it seems to be fairly
independent of the type of drug
being administered. So far, over
90 drugs have been tested and
worked with it. “You don’t have to
reformulate the drugs,” he said. And
this would be advantageous for the
pharmaceutical companies.
Dr. Packer added that the most
likely form for the technology
would be a cartridge-type system,
which would allow patients to
buy one system and use different
medications in it. “The main thing
is ease of use,” Dr. Packer said. It
has to be easy to use, it has to be
comfortable, and it has to be sterile,
he said. EWAP
Editors’ note: Dr. Packer has fi nancial interests with Corinthian Ophthalmic. Dr. Ianchulev has fi nancial interests with Corinthian Ophthalmic. Dr. Robin has no fi nancial interests related to this article.
Contact informationIanchulev: [email protected]
Packer: [email protected]
Robin: [email protected]
Index to Advertisers
AMO – TECHNIS Family of IOLsPage: 20, 21
www.AbottMedicalOptics.com
Carl Zeiss Meditec AGPage: 35
www.meditec.zeiss.com/ReLEx
MoriaPage: 24, 46
Phone: +33 (0) 146744674
Email: [email protected]
www.moria-surgical.com
Oculus Optikgerate GmbHPage: 11
Phone: +852-2987-1050
E-mail: [email protected]
www.oculus.de
Synergetics IncPage: 2
Phone: +636.939.5100
Fax: +636.939.6885
Email:
www.synergeticsusa.com
Technolas Perfect Vision
GmbH- A Bausch + Lomb
CompanyPage: 14
Phone: +65-6592-0792
www.technolas.com –
www.bausch.com
Topcon Singapore Medical
Pte LtdPage: 39
Phone: +65-68720606
Email: [email protected]
www.topcon.com.sg
Ziemer Ophthalmic SystemsPage: 60
www.ziemergroup.com
ASCRSPage 48, 59
www.ascrs.org
APACRSPage 5, 7, 27, 31, 42
www.2013apacrs.org
World Ophthalmology
Congress (WOC 2014)Page: 57
www.woc2014.org
Dr. Safran prefers metal blades for
lamellar work. He feels it is easier to
stay on plan with a metal blade that
is beveled on one side.
“If the blade is too sharp, it
won’t stay on the plane but will cut
across it,” Dr. Safran said. “It’s like
using a knife for the lasagna instead
of a spatula.”
Pros and consThe positives to choosing a
metal, disposable blade are cost
and tactile feedback, according to
Dr. Devgan. “They’re not nearly
as sharp as a diamond blade, and
you don’t get as clean an incision
as with diamonds. For experienced
surgeons, using a diamond blade is
like a hot knife through butter—
there’s no tactile feedback,” he
said. Diamonds don’t require
routine resharpening, but they are
expensive (running a few thousand
dollars per blade) and are “as fragile
as a potato chip because they’re so
incredibly thin,” Dr. Devgan said.
If surgeons want to change their
preferred incision size from 2.8 mm
to 2.2 mm, the diamond blade can
be rehoned, but if the surgeon opts
to go back to the larger size, a new
blade is necessary, which adds to
the cost as well.
Sapphire blades fall somewhere
between steel and diamonds, Dr.
Devgan said. They’re reusable and
cost more than steel blades, and
while they are less expensive than
diamond blades, they may not last
as long (somewhere in the tens or
hundreds of uses).
“Gem-quality diamond blades
can be used ad infi nitum unless
they’re damaged,” Dr. Devgan said.
The femtosecond lasers offer
an additional type of incision
and while they can create any
architecture design that a surgeon
can fathom, “the fl oor and the
roof of the incision aren’t quite as
smooth as you get with a diamond
blade,” Dr. Devgan said.
Number of usersNewer surgeons should
probably do their fi rst couple
hundred incisions with a metal
blade before trying a diamond.
“Part of any learning
experience is to try all the different
blades,” Dr. Naseri said. “Each
surgeon is going to make his or her
own decisions based on what he
or she likes. I provide my residents
with a rationale about why I prefer
metal blades, but in the end it’s
their decision.”
Dr. Naseri said if he’s the
only user at a surgery center, “I’d
consider the diamond blade, but
only ones without side-cutting
elements. At an institution with
multiple users and trapezoidal
blades, there is just too much
inconsistency.”
Dr. Devgan said he literally has
residents’ hands in his own during
their fi rst few uses of a diamond
blade since the feedback is reduced.
“Whatever blade you use will
ultimately depend on what you are
most comfortable having in your
hands and whether the surgery
center can process it without
breaking or damaging it,” Dr.
Safran said. EWAP
Editors’ note: Dr. Ambrosio has fi nancial interests with Oculus (Lynnwood, Wash., USA). Dr. Fontes has no fi nancial interests related to his comments.
Contact informationDevgan: 800-337-1969, [email protected]
Naseri: 415-221-4810, ext. 4707, [email protected]
Safran: 215-962 5177, [email protected]
51-52 EWAP Devices.indd 5251-52 EWAP Devices.indd 52 21/03/2013 17:3021/03/2013 17:30

53EW NEWS & OPINIONMarch 2013
Rigging the game to win in challenging cataract cases
Practitioners can only
play the cards that they
are dealt in challenging
cataract cases. But that
doesn’t mean that they can’t stack
the deck in their favor. Here’s how
the latest cohesive, dispersive, and
viscoadaptive OVDs can help do
just that.
Bonnie An Henderson,
MD, assistant clinical professor,
Harvard Medical School, Boston,
Mass., USA, believes in planning
ahead particularly in a challenging
cataract case. “I prepare for
challenging cases by thinking
through each step and what type of
viscoelastic may be the best choice
for that action,” Dr. Henderson
said.
Playing a cohesive handShe fi nds that cohesive OVDs
have unique characteristics that
can be very useful in challenging
cases. “Benefi ts of cohesive OVDs
include the ability to maintain
space, clearer visualization, and the
ability to remove the OVD quickly
and easily,” Dr. Henderson said.
One of the strengths of these
cohesive OVDs is their ability to
create space. “Cohesive OVDs,
especially higher molecular
weight OVDs, can be used as a
physical barrier to keep ocular
tissues compartmentalized,” Dr.
Henderson said. “For example,
when attempting to manipulate
the iris during IFIS (intraoperative
fl oppy iris syndrome) cases or
when suturing a PCIOL to the
iris, a high viscosity cohesive can
help compress and isolate the iris
tissue.”
Also, she emphasized, if there
is positive pressure with chamber
shallowing, a high viscosity OVD
will help maintain a formed
chamber and fl atten the anterior
surface of the lens, and this can
help when attempting to complete
a capsulotomy.
For routine cases and for fi lling
the bag, Dr. Henderson’s go-to
OVDs include ProVisc (Alcon, Fort
Worth, Texas, USA/Hünenberg,
Switzerland), AmVisc (Bausch +
Lomb, Rochester, NY, USA), or
Healon (Abbott Medical Optics,
AMO, Santa Ana, Calif., USA).
In instances requiring enhanced
stability of the anterior chamber,
however, she will use AmVisc Plus
(Bausch + Lomb) or Healon GV
(AMO).
Dealing out dispersivesLikewise, dispersive OVDs
can play an important role in
challenging cases. “Since they
adhere to surfaces like the corneal
endothelium, these agents protect
against ultrasonic or mechanical
injury,” Dr. Henderson said. She
also fi nds that because challenging
cases tend to take longer, dispersive
viscoelastics can decrease the
amount of corneal damage, as well
as resulting corneal edema.
Another key characteristic of
dispersive OVDs in challenging
cases is their ability to remain in
place. “They do not exit the eye
easily,” Dr. Henderson said. “This
ensures that the anterior chamber
does not collapse prematurely
during an inopportune moment.”
Roger F. Steinert, MD, chair,
Department of Ophthalmology,
University of California, Irvine,
Calif., USA, and director, Gavin
Herbert Eye Institute, sees
dispersives as valuable in situations
where practitioners are concerned
that they’re not going to be able
to ultimately remove all of the
OVD—something that could cause
pressure elevation. “The larger the
molecular weight on average, the
more likely you are to get higher
pressure,” Dr. Steinert said. This
makes a lighter dispersive OVD
an asset in an open capsule case,
where some viscoelastic will be left
behind.
Also in cases involving very
dense nucleus, where there is
often not much of a protective
epinucleus, he fi nds that dispersive
OVDs have a role. During the
second half of phacoemulsifi cation,
the posterior capsule starts to get
exposed and either the phaco tip
itself or a sharp piece of nucleus
can cause a rupture, he warned.
To protect against this, Dr.
Steinert uses a technique that he
dubs the “visco vault.” “As soon
as I can see some red refl ex and
I’ve got enough of the nucleus out
that I can get pretty deep behind
the nucleus, I create an artifi cial
epinucleus with a dispersive
OVD,” Dr. Steinert said. “It can do
a remarkable job in keeping the
posterior capsule back and keeping
it safe.”
Steve A. Arshinoff,
MD, clinical instructor of
ophthalmology, University of
Toronto, explains that by their very
nature, dispersive OVDs, which
demarcate spaces, are used in
more complicated cases. “A space
becomes a complicated case when
you wish to partition the space,”
he said. He pointed to protecting
the endothelium in Fuchs’
dystrophy cases. “What you’re
saying is, you want to partition the
space, the adjacent endothelium,
so that there’s no fl uid fl ow there,”
Dr. Arshinoff said. Likewise, in a
tamsulosin hydrochloride case,
Experts provide OVD cheat sheetby Maxine Lipner Senior EyeWorld Contributing Writer
he stressed, you want to partition
the iris in a way that it doesn’t get
exposed to the fl uid turbulence
and fl op all over the place. In both
cases, a dispersive OVD will remain
in place and provide the needed
buffer.
To maximize effectiveness, he
often pairs the unique properties
of a dispersive agent with those of
a cohesive. He uses the cohesive
agent to induce pressure and the
dispersive to partition space. For
example, for a case involving
a traumatic cataract with two
or three clock hours of broken
zonules, Dr. Arshinoff advised
painting the area with a dispersive
viscoelastic and then putting a
viscous cohesive in the eye to
slowly apply pressure. “Then you
do the capsulorhexis and start
your surgery,” he said. “But before
you try and induce any fl ow in the
eye, you hydrodissect gently and
try to put in a capsular tension
ring in the bag.” This broadens the
shape of the lens so this covers the
disinsertion of zonules. The only
thing in front of the ring is the
dispersive viscoelastic. “The case
then becomes a regular case,” he
said.
For his “go-to” dispersive
agent, Dr. Arshinoff prefers the
original Viscoat (Alcon) to the
others, which he terms copies. “If
it were my mother [as the patient],
I would choose Viscoat just because
we have a longer track record,” he
said. Dr. Henderson likewise favors
Viscoat.
Dr. Steinert has switched
to using the dispersive Healon
EndoCoat (AMO). “What surgeons
are observing is that EndoCoat,
because it is purely hyaluronic
acid, does not have the problem
with viability that some people
continued on page 54
53-54 PHARMACEUTICALS.indd 5353-54 PHARMACEUTICALS.indd 53 21/03/2013 17:3121/03/2013 17:31
54 March 2013EW NEWS & OPINION
experience with Viscoat,” he said.
He fi nds that Viscoat tends to be
ropey and disrupts the red refl ex,
while EndoCoat tends to be much
more uniform.
Two aces in the holeMeanwhile, because Preston
H. Blomquist, MD, professor,
Department of Ophthalmology,
University of Texas Southwestern
Medical Center, Dallas, Texas,
USA, always uses dispersive and
cohesive viscoelastics in tandem,
he favors DuoVisc (Alcon). “I am a
great believer in Steve Arshinoff’s
soft shell technique,” he said.
With this, the cohesive viscoelastic
opens up the space in the anterior
chamber while the dispersive agent
helps to protect the endothelium
during phacoemulsifi cation.
Accordingly, he pointed out with
the DuoVisc he gets the dispersive
Viscoat as well as the cohesive
ProVisc. “The DuoVisc is nice
because you have the two separate
viscoelastics that you can put
where you want and have them
function as you want them to,” he
said.
For a complex case of zonular
dehiscence, he fi nds this helps to
simplify the situation. “I want to
use my dispersive viscoelastic to
tamponade the vitreous so that it
has no way to come around the
edge of the lens in the area where
you have zonular dehiscence,”
he said. “Then I put my cohesive
viscoelastic on top of that to
open up the space to perform
the surgery.” Together these each
work to their best advantage, Dr.
Blomquist fi nds.
The viscoadaptive bridgeA fi nal category of OVDs that
can prove helpful in complex
cases is viscoadaptive agents, such
as Healon5 (AMO), which has
characteristics of cohesives and
is also pseudodispersive under
high fl ow conditions. “Healon5 is
called viscoadaptive because under
some conditions it can actually
changes its rheologic behavior,”
Dr. Arshinoff said. “Under high
fl ow conditions it behaves as a
solid, so it starts to fracture apart.”
This makes it a pseudodispersive.
Likewise, when stationary, Healon5
is exceedingly viscous, like a
cohesive, good for maintaining
anterior chamber depth.
One of the strengths of
viscoadaptives, Dr. Arshinoff
stressed, is this viscosity. “They
are so viscous they don’t allow
water to leak through them,” he
said. “So you can use balanced
salt as a second OVD because
the viscoadaptive isolates it
and does not mix with it.” The
viscoadaptive OVD can be used to
block the incision, with a solution
of lidocaine and phenylephrine
serving in place of balanced
salt in the style of the “ultimate
soft shell.” This solution causes
excellent dilation of the pupil and
makes the procedure easier.
When in need of a
viscoadaptive, Dr. Arshinoff favors
Healon5, which he terms the
prototype.
Overall, Dr. Arshinoff
encourages practitioners to look
at each case as if it were involving
physically separable spaces rather
than a single surgical space,
keeping in mind the different OVD
properties. If a practitioner keeps
three or four OVDs on hand, this
can make it easier to deal with
complex cases. “Almost all of them
end up being quite simple because
you have rigged the game for
yourself like a card player who rigs
the cards before he plays,” he said.
“If you rig the game before you
start, things that appeared very
diffi cult really aren’t hard at all.”
EWAP
Editors’ note: Dr. Arshinoff has fi nancial interests with Alcon, AMO, and Bausch + Lomb and has consulted for all of the OVD companies. Dr. Blomquist has no fi nancial interests related to this article. Dr. Henderson has fi nancial interests with Alcon and Bausch + Lomb. Dr. Steinert has fi nancial interests with AMO.
Contact informationArshinoff: 416-745-6969, ifi [email protected]
Blomquist: 214-648-3770, [email protected]
Henderson: 617-723-2015, [email protected]
Steinert: 949-824-0327, [email protected]
Experts - from page 53
DATE MEETING VENUE
April 19-23ASCRS-ASOA Symposium & Congress (ASCRS-ASOA)
www.ascrs.orgSan Francisco, USA
June 27-29
28th Annual Meeting of the Japanese Society of Cataract & Refractive Surgery
(JSCRS)
http://www.congre.co.jp/jscrs2013/english/contents/greeting.htmlTokyo, Japan
July 3-62013 AUSCRS
www.auscrsthemeetingplace.com.auUluru, Australia
July 6-82013 Indian Intraocular Implant & Refractive Surgery Convention (IIRSI)
www.iirsi.comChennai, India
July 11-14 26th APACRS Annual Meeting – A Global Focus on the Anterior Segment
www.apacrs.orgSingapore
July 14-16 An Intercontinental Perspective of Pediatric Ophthalmology & StrabismusSingapore National Eye Centre (SNEC) and AAPOS Joint Meetinghttp://www.aapos.org
Singapore
October 5-9XXXI Congress of the ESCRSwww.escrs.org
Amsterdam, Netherlands
November 16-19 Annual Meeting of American Academy of Ophthalmology (AAO) www.aao.org
Chicago, USA
CALENDAR OF MEETINGS 2013
53-54 PHARMACEUTICALS.indd 5453-54 PHARMACEUTICALS.indd 54 21/03/2013 17:3121/03/2013 17:31
March 2013 55EWAP NEWS & OPINION
MEETING REPORTER
Live reports from the 28th APAO Congress
In addition to its mind-
bogglingly comprehensive
scientifi c program, the 28th
Asia-Pacifi c Academy of
Ophthalmology (APAO) Congress
held in conjunction with the 71st
Annual Conference of the All
India Ophthalmological Society
(AIOS) featured socially relevant
sessions, human interest stories,
and an exploration of trends in
information technology.
India president speaks at Opening Ceremony
With India President Pranab Shri Mukherjee and other
attendee dignitaries lighting a lamp
in an offi cial ceremony to kick
off the 28th APAO Congress, the
meeting got off to a start with a
well-attended Opening Ceremony
that showcased the richness of
Indian culture and history.
“Ophthalmologists have a
special and important status in
society,” said President Mukherjee.
“You are the ones who, by being
doctors, are a critical human organ
that is necessary for the conduct
of human affairs and pursuit of
quality of life. According to the
ancient Indian scriptures, the eye is
the most important of senses in our
body.”
President Mukherjee was
the Chief Guest at the Opening
Ceremony, where he listened
as ICO, AAO, SAO and other
organization offi cials, including
AIOS President Rajvardhan Azad, MD, India, and Frank J. Martin, MD, Australia, discussed
the future of ophthalmology and
its need to address the rising tide
of blindness around the world.
President Mukherjee launched the
digital inauguration of the meeting,
a festival of lights and colorful
videos, with traditional Indian
music highlighting the meeting
location in Hyderabad.
Dr. Martin, outgoing president
of the APAO, said this year’s
Congress should be an excellent
place for attendees to learn.
“We come together at this
Congress from diverse nations with
different beliefs. We have one thing
in common—the preservation
of vision and the prevention of
blindness,” said Dr. Martin.
The Opening Ceremony saw
the awarding of two medals, three
lecture prizes, and three awards.
Women face challenges in ophthalmology
From gender disparities
in healthcare delivery to
potential obstacles in a career in
ophthalmology, women continue
to encounter challenges in the
medical specialty, four women said
at the 28th APAO Congress.
“The only way to change this is
to work together and to hold each
other close, men and women, to
make change over the long term,”
said Lynn Gordon, MD, Calif.,
USA, at the “APAO Women in
Ophthalmology” symposium.
She discussed unconscious bias
and schema and how it impacts
perceptions, including in the hiring
of a man or a woman.
Pearl Tamesis-Villalon, MD,
Philippines, discussed mentoring;
Ava Hossain, MD, Bangladesh,
and president of the SAARC
Academy of Ophthalmology,
discussed gender disparities in
ophthalmology healthcare delivery;
and Anita Panda, MD, Delhi,
India, and incoming president of the
AIOS, discussed potential obstacles
in a woman’s career.
Personal storyDr. Hossain told the story of
the beginning of her career in
Bangladesh. She said that in 1979,
she wanted to enroll in a residency
training program in ophthalmology.
“I went to my professor’s offi ce
and told him what I would like to
do,” she said. “He told me, being a
women, is it possible to be able to
take care of everything [involved in
such a program]? So I decided to do
a fellowship privately fi rst.”
She said that her story is
different from a man’s only because
of her gender, but the situation
in her country is changing—in
1985, there were no women
ophthalmologists, and by 2012,
there were 100. The country still has
a long way to go in gender equality
in the medical profession, she said,
but times have changed since her
professor questioned her abilities in
embarking on her chosen medical
career path.
“Most of all practicing eye
surgeons are still male. But this
will change, as in every successive
year, female ophthalmologists
are increasing, especially as the
older male surgeons are gradually
retiring,” said Dr. Hossain.
Advances neededHowever, women in
ophthalmology still have some
way to go, she said. She cited a U.S.
report that said that white female
ophthalmologists’ mean annual
income was 20% lower than white
males.
She sought to explain this
disparity in terms of how women’s
personal lives can impact their
careers.
“Women ophthalmologists
devote a substantial amount of
their career path time to families
and parenting. Some also work
part time while raising a family. It
is about seeking balance between
career and family [for women
ophthalmologists],” Dr. Hossain
said.
Prevalence of blindness is also
high among women, with women
accounting for more than 64.5%
of all visually impaired people
worldwide—the blind women to
men ratio is 1.43:1.
“In low- and middle-income
countries, men had 1.71 times more
cataract surgery than women. [A
2009 study] estimates that severe
visual impairment could be reduced
by more than 10% if women were
to receive surgery at the same rate
as men,” according to Dr. Hossain.
The women agreed that access
to healthcare is limited to women
and that sociocultural infl uences
can have a major impact on women
both receiving and giving care.
More affordable AMD treatment needed
With nearly 80% of Indians
unable to afford age-related macular
degeneration treatment, including
those who are health benefi ciaries/
government employees, a more
affordable approach to care is
needed, said AIOS President
Rajvardhan Azad, MD, India.
“The need of the hour is
by EyeWorld Staff
continued on page 56
055-060 EWAP NEWS & OPINION.indd 55055-060 EWAP NEWS & OPINION.indd 55 21/03/2013 17:3121/03/2013 17:31

March 201356 EWAP NEWS & OPINION
to propose new research by
comprehensive studies to integrate
various components of AMD-
related costs,” Dr. Azad said. “We
need to provide an easy, accessible,
affordable, and effi cacious mode
of treatment. The pricing policy
should not be only profi t-driven but
service-driven [as well].”
About AMDDr. Azad discussed vision and
economics in AMD management at the “Update on age-related macular degeneration” symposium. He outlined the story of AMD, from the epidemiology of the disease—for instance, it is a common cause of blindness in the elderly age group, and the 60+ population is the fastest growing age group in the world. The disease has serious economic ramifi cations for that rapidly growing age group, considerably lowering productivity from work absence, ability to earn a daily living, and reducing quality of life.
The most common severe vision loss in AMD is caused by choroidal neovascular membrane (CNVM), and CNVM’s primary treatment is anti-VEGF, he said.
“In the last 10, 15 years, there’s been a lot of change and a paradigm shift in AMD. For most of us sitting here, the primary treatment is anti-VEGF—others, are laser for extrafoveal CNVM and PDT for a very selective group. We have other treatment that is now historical,” he said. “Therefore, the whole treatment revolves around anti-VEGF.”
Anti-VEGFsAnti-VEGFs have changed the
“aim of therapy … to gain in vision in AMD, where previously the aim in treatment was to maintain vision
or prevent vision loss,” he said.
Therein lies the fi nancial
problem, Dr. Azad said, because
while vision is gained with
the drug, it not only has some
complications, including systemic
and others, as well as issues
involved with frequent visits for
treatments, but it also has the
burden of the cost—the treatment
is expensive.
He compared prices of two
commonly used anti-VEGFs,
Lucentis (ranibizumab, Genentech,
San Francisco, Calif., USA), U.S.
Food and Drug Administration
approved, and Avastin
(bevacizumab, Genentech) used off-
label. The two have similar profi les:
The duration of action for Lucentis
is four weeks, while the duration
of action is four to six weeks for
Avastin, and ocular and systemic
safety is comparable.
But the cost of the two drugs is
signifi cantly different.
“It is 40,000 to 60,000 rupees
per dose for ranibizumab and
2,000 to 5,000 rupees per dose for
bevacizumab,” Dr. Azad said.
The total estimated cost of
anti-VEGFs with a four to six
weeks frequency dosing at 20
expected doses for Lucentis is
800,000 to 1,200,000 rupees,
while Avastin is 40,000 to 100,000
rupees—and another anti-VEGF,
Macugen (pegaptanib sodium, OSI
Pharmaceuticals, Melville, NY,
USA), has a more initial estimated
cost, at 45,000 rupees, going up to
50,000 rupees, totaling 900,000 to
1,000,000 for 20 doses.
Cost burden, protocolAt such costs, it is not diffi cult
to understand how many patients
cannot afford their treatment for
the blinding disease, regardless of
the consequences to their vision.
In his own treatment protocol,
Dr. Azad fi rst diagnoses CNVM/
recurrence and then assigns three
monthly dose treatment of anti-
VEGF with PRN dosing based on
visual acuity, OCT, and fl uorescein
angiography eye test, as needed.
With his current protocol, for
the fi rst year, with 30% to 40%
remission, fi ve doses are expected
when using any of the three drugs,
dropping to four doses expected
in the following years, impacting
cost in a positive way by slightly
reducing the overall fi nancial
burden, he said—but still, that
cost does not account for other
coexistent costs at present, such as
OCT and fl uorescein angiography
eye test.
The future of endothelial keratoplasty
“To understand the future,
you need to understand the past,”
said Jodhbir S. Mehta, MD,
Singapore.
It has been 108 years since the
fi rst penetrating keratoplasty was
performed. Penetrating keratoplasty
became the gold standard for
endothelial replacement, but
even after more than a century
of development, it remains
problematic, including a corneal
endothelial cell loss of up to 70% at
10 years.
The trend today is increasingly
toward targeted replacement of
diseased corneal layers. Endothelial
keratoplasty represents a shift in the
paradigm that has dominated for
almost a century.
However, Dr. Mehta and his
colleagues at the Singapore National
Eye Centre (SNEC) soon found that
the typically shallow Asian eye
presented a particular challenge
to the procedure. Using the taco
folding technique for inserting
donor tissue used in countries like
the U.S., he and his colleagues
were alarmed to fi nd an initial
endothelial cell loss of 30% post-op,
going up to over 60% at one year—
results that were reinforced and
closely replicated in Japan.
They thus introduced the sheets
glide technique. Using the sheets
glide, a large incision, and a pull-
through technique, the SNEC team
was able to reduce the initial loss to
9%, with a clear cornea at day 1.
It still was not ideal—the pull-
through could damage the donor
rim, the sheets glide is open so the
donor tissue is not protected and
may slip, and requires a degree of
ambidexterity.
So the SNEC team developed
the EndoGlide. The earliest
version of the EndoGlide—the
design inspired by thumb drives—
produced double coiling of the
donor tissue, allowing surgeons to
insert larger donor tissues through
smaller incisions. More importantly,
the EndoGlide gave the surgeon full
control of the donor tissue at all
times until insertion is completed.
The EndoGlide reduced one-
year endothelial cell losses from
19% to 15.6%, then 14.9% as they
performed more cases and surgeons
grew more comfortable with the
technique.
The more recent preference for
thinner donor tissue—such as in
Descemet’s membrane endothelial
keratoplasty (DMEK)—led the SNEC
team to develop a new iteration
of the EndoGlide. The EndoGlide
Ultrathin introduces a saddle to
the design to more gently curve the
tissue while loading.
The ideal approach to
endothelial disease, however,
is to cultivate human corneal
endothelial cells.
The fi rst problem was to fi nd a
medium in which cultivated cells
Live - from page 55
w
A R
continued on page 58
055-060 EWAP NEWS & OPINION.indd 56055-060 EWAP NEWS & OPINION.indd 56 21/03/2013 17:3121/03/2013 17:31
March 2013 57EWAP NEWS & OPINION
p,
—
ts
m
o
y,
ll
s
C
e woc2014 Highlights LEARN MORE : WWW.WOC2014.ORG
www.facebook.com/woc2014 twitter.com/woc2014
Abstract Submission is Now Open http://www.woc2014.org/contents/call_for_papers.htmlRegister in April 2013 http://www.woc2014.org/contents/register.html
58
055-060 EWAP NEWS & OPINION.indd 57055-060 EWAP NEWS & OPINION.indd 57 21/03/2013 17:3121/03/2013 17:31

March 201358 EWAP NEWS & OPINION
would follow the morphology of
normal corneal tissue—with most
media, cultivated cells grow chaotic
and spindle shaped. M5 appears
to be just the medium needed for
the procedure, and now what’s
needed is a carrier—a RAFT (real
architecture for 3D tissue), made of
plastic compressed collagen.
Using cultivated endothelial
cells for treating endothelial disease
remains some years down the
road, but with Dr. Mehta and his
colleagues working on it, the future
of endothelial keratoplasty is just
over the horizon.
Dr. Mehta delivered this year’s
Nakajima Award Lecture in a
symposium on “Current trends in
posterior lamellar cornea surgery: A
revolution in evolution.”
Perspectives on diffi cult glaucoma
The International Academy of
Ophthalmology includes the world’s
senior members of ophthalmologic
academia and was established to
promote academic ophthalmology
and education. One of the strengths
of the Academy is its ability to
draw on experts from a variety of
different subspecialties to offer their
perspectives on issues on which
the discourse might otherwise be
confi ned to experts within a single
specialization.
This was exemplifi ed by the
Academy symposium on the
management of diffi cult glaucoma.
Glaucoma is an
epidemiologically signifi cant
condition in the Asia-Pacifi c region,
one that has wide-reaching effects
on and associations with a variety
of other ophthalmic conditions.
One signifi cant cause of
secondary glaucoma is iridocorneal
endothelial (ICE) syndrome. In this
condition, secondary glaucoma
develops when abnormal cells
proliferate, crossing the Schwalbe’s
line and covering the trabecular
meshwork and obstructing the
anterior chamber angles, said
Dennis S.C. Lam, MD, Hong
Kong, secretary-general of APAO.
In addition, peripheral anterior
synechiae can form.
“On one hand, you have
an open angle component,” he
said. “On the other hand, you
can actually have anatomical
changes, making this a closed angle
situation.”
The treatment options are the
same as for ordinary glaucoma,
although because the ICE syndrome
is progressive, most are only useful
at the beginning. Trabeculectomy,
for instance, is usually successful
only initially, with failure occurring
as early as six months after the fi rst
procedure, said Dr. Lam.
Trabeculectomy fails not only
because of the progressive nature
of ICE, but because of the extensive
fi brosis seen in these relatively
young patients; there can be
aggressive PAS.
“Trabeculectomy will fail
eventually,” said Dr. Lam.
While medical management
and other procedures are successful
in the beginning, Dr. Lam said
that some doctors “want to use
drainage devices as their fi rst line.”
However, the tube is at risk for tip
lumen obstruction by proliferating
abnormal cells, and tube migration
caused by this same proliferation or
PAS formation can also occur.
“If you are using this procedure,
I think it is a good idea to
communicate to your patient that
this may occur and require further
surgery,” said Dr. Lam. As a way
of minimizing or circumventing
this risk, Dr. Lam suggested using a
longer tube shunt. In pseudophakes,
the tube could be placed initially in
the sulcus or pars plana—the latter
case requiring full vitrectomy.
Indian physician sees evolution of ophthalmology in India over long career
When R. B. Jain, MD, Delhi,
India, was 10 years old, he visited
his maternal grandfather on
holiday. His grandfather needed
building materials for a house, so he
asked Dr. Jain to go with him.
His grandfather, a prominent,
well-educated postmaster in his
town in India, was 90% blind from
glaucoma.
He had to hold Dr. Jain’s hand,
and Dr. Jain led him to the shop.
Dr. Jain selected the best wood for
his grandfather. He signed forms to
ensure the wood was delivered.
He was, in essence, his
grandfather’s eyes, and the
diffi culty of the situation, and the
unfairness of it—why anyone would
go blind and be so helpless that
they could not be independent in
such every day activities as walking
or shopping—struck him hard that
day. He made his grandfather a
promise.
“I told him, ‘I’ll be an eye
surgeon,’” said Dr. Jain.
That was 1956. In 1972,
Dr. Jain became qualifi ed as an
ophthalmologist, and he went on
to an illustrious career as a retina
specialist and past president of the
Delhi Ophthalmological Society
and the All India Ophthalmological
Society.
Dr. Jain said he has never
forgotten that day when he pledged
his future career to his grandfather.
“I felt very sad,” he said. “I
thought, why should he be blind?
Why should anyone be blind?
Why should an educated person be
blind?”
He discussed his 40-year
career, and the innovations and
experiences that he has seen as
an ophthalmologist in India in an
award lecture at the Prevalence of
Visual Impairment, Training and
Education in the Asia-Pacifi c Area
symposium.
“It is fascinating to look back at
some of the radical changes during
my career of 40 years,” he said.
#1 pearlsCataract surgery, said
Hungwon Tchah, MD, Seoul, is
essentially nucleus removal—the
rate limiting step, the phase of the
surgery that takes the most time
and effort.
The hardness of cataract is
thus the main factor to determine
the technique to be used during
cataract surgery.
Soft cataracts, said Dr. Tchah,
can be managed by simple
debulking and prechopping. For
harder cataracts, there’s the divide
and conquer technique, and the
phaco chop.
The hardest cataracts, grade
5+, pose a challenge for even
experienced surgeons, but
grooving and chopping work for
these cataracts. However, for such
hard cataracts, even using these
techniques, the increased phaco
energies necessary to emulsify
the nucleus pose a risk to the
endothelium.
For these cases, Dr. Tchah
prefers his own “multichop”
technique.
The principle, he said, is similar
to eating a pizza—it’s diffi cult to eat
a whole pizza until you cut it into
radial slices.
The steps are simple: engage
the nucleus, create the fi rst chop,
rotate and chop, rotate and chop,
etc. Once the nucleus has been
“multichopped” into manageably
sized pieces, the pieces can be
emulsifi ed and removed one at a
time.
This decreases the phaco power
signifi cantly and reduces the risk of
heat damage to the incision, as well
as the potential for damage to the
corneal endothelium.
Dr. Tchah shared his pearl
with attendees at a symposium
titled “My number one pearl in
cataract surgery.” Also on hand
to share their pearls were session
chairs Shamik Bafna, MD,
Cleveland, who described ways to
improve refractive outcomes in
cataract surgery, including using
the ORA system (WaveTec Vision,
Aliso Viejo, Calif., USA); Tetsuro Oshika, MD, Tsukuba, Japan,
who described his technique for
transconjunctival single-plane
sclerocorneal cataract surgery; and
Boris Malyugin, MD, Moscow,
who described his approach
to small pupils, highlighting a
stepwise approach including but
not exclusive to the use of the
Malyugin ring (MicroSurgical
Technology, Redmond, Wash.,
USA). Dr. Malyugin also described
his technique for performing
1.8-mm C-MICS in a vitrectomized
eye. EWAP
Editors’ note: Dr. Mehta is part of the team that developed the EndoGlide, but has no fi nancial interests related to his lecture. Dr. Malyugin is the co-inventor of the Malyugin ring, which he described in one of his pearls. None of the other doctors named in this article have fi nancial interests related to their talks.
Live - from page 56
055-060 EWAP NEWS & OPINION.indd 58055-060 EWAP NEWS & OPINION.indd 58 21/03/2013 17:3121/03/2013 17:31
March 2013 59EWAP NEWS & OPINION
ar
at
r
f
ll
d
e
SYMPOSIUM & CONGRESS
2014 APRIL 25–29B O S T O N
Additional Programming
Cornea DayASCRS Glaucoma DayASOA WorkshopsTechnicians & Nurses Program
Book Early for the Best Rates
Housing OpensFriday, April 19, 2013
055-060 EWAP NEWS & OPINION.indd 59055-060 EWAP NEWS & OPINION.indd 59 21/03/2013 17:3121/03/2013 17:31

March 201360 EWAP NEWS & OPINION
The power of one
The Ziemer FEMTO LDV Z Models are FDA cleared and CE marked and available for immediate delivery. For some countries, availability may be restricted due to local regulatory requirements; please contact Ziemer for details. The creation of a corneal pocket is part of a presbyopia intervention. Availability of related corneal inlays and implants according to policy of the individual manufacturers and regulatory status in the individual countries. Cataract procedures with the FEMTO LDV Z2, Z4 and Z6 models are not cleared in the United States and in all other countries. An upgrade possibility for these devices is planned once cataract options are available and cleared by the responsible regulatory bodies.
THE ONE FEMTO PLATFORM for cornea, presbyopia and cataract.
Presenting the unparalleled Ziemer FEMTO LDV Z Models – a technical revolution in ocular surgery. No laser is more precise, more powerful or more progressive when it comes to meeting all your procedural needs in a single platform.
With Ziemer’s FEMTO LDV Z Models, now you can operate with a modular femtosecond system that is easy to configure, designed to grow with your practice – cornea and presbyopia today, cataract tomorrow.www.ziemergroup.com
EyeWorld_AsiaPacific_april-june2013_FEMTO_LDV_Z_Models_Ad_10x13i.indd 1 11.03.13 09:46055-060 EWAP NEWS & OPINION.indd 60055-060 EWAP NEWS & OPINION.indd 60 21/03/2013 17:3121/03/2013 17:31





























