Embed Size (px)
Citation preview

1

2

3

4

5
6
7

The Delta Center For a Thriving Safety Net will provide technical assistance to state primary care associations and behavioral health state associations to build a stronger safety net with a focus on ambulatory care settings in both rural and urban areas. We also aim to inspire innovation and change in the value‐based care and payment space through both policy and practice. We selected the name, The Delta Center, for a reason. Delta connotes the idea of change. It also connotes the idea of confluence: confluence of ideas, confluence of both payment and care, and confluence of behavioral health and primary care in some ways in this unique collaboration.
Finally, it also has a connotation of a river delta where things come together, oftentimes in rural areas. We really are trying to make sure that all of our efforts are equally tailored and targeting PCAs and behavioral health state associations that are surveying both rural and urban settings.
8

We have three key areas of focus. Care delivery transformation is one. Ultimately we are trying to promote excellence and care and outcomes for patients. The second is payment reform, which increasingly is being seen as a way to sustain new models of care, especially in ambulatory care settings. The third focus is to acknowledge that change doesn't just happen. Both state organizations and provider organizations can benefit from cultivating and fostering the practices of learning organizations from leadership styles, to having change management built in to their leadership and organizational culture, to having cultures of continuous improvement including using human‐centered design principles to make sure that change is designed around the ultimate end users.
9

The Robert Wood Johnson Foundation is ultimately the funder behind Delta Center, and we are very grateful for their innovative investment in this initiative. We are also joined by National Action Partners at the National Council and the National Association for Community Health Centers. This is a first in terms of a large scale collaboration between these two national associations.
There are also three entities that came together in a unique partnership to serve you as Delta Center staff. First, JSI Research and Training, or JSI has long worked with hundreds of community health centers, community behavioral health centers, health departments, and primary care programs in both rural and urban areas. We have over the years done work in technical assistance, in research and evaluation at both state and national levels, in policy development, as well as working on the ground with safety‐net clients. We will also have active research efforts to understand and articulate the challenges and opportunities for safety‐net providers participating in value‐based payment and accountable care models.
The second partner is the Center for Care Innovations, or CCI, that has long been supporting care delivery change in safety‐net organizations over the past 18 years. CCI works to design, develop, and implement programs that build capacity, capability, catalyze innovation, and spread solutions that ultimately work in healthcare safety net organizations across the country. CCI's programs are built on a foundation of improvement, innovation, and peer learning. They will bring to bear these experiences and their experience leading
10

efforts to prepare safety net providers to deliver value‐based care and population health under alternative payment models.
The third partner is the MacColl Center for Healthcare Innovation at Kaiser Permanente. Since 1992, MacColl has been an internationally recognized center for health services research and translation, and they design interventions, develop and administer evaluation tools, convene national meetings and regional learning collaboratives, and have developed many white papers and tools, as well as conducted Train the Trainer programs to support quality improvement efforts in the safety net. Perhaps best known for their development of the Chronic Care Model, MacColl has also been deeply involved in patient‐centered medical home implementation efforts in the safety net, and in regional collaborations to improve delivery of care for the chronically ill. They'll also be bringing to bear recent expertise in leading the National Program Office for the RWJF LEAP project.
10

The Delta’s Center main initiative is a Learning & Action collaborative that will bring together a total of five primary care associations and five behavioral health state associations over the course of two years. The Learning & Action collaborative is ultimately meant to build capacity at the state levels for delivering TA and training to providers within those states. Through the course of the Learning & Action collaborative, we will also develop and source high quality materials that can be widely spread and disseminated to the field at large, even for those not participating actively as one of the 10 grantees.
We will also develop policy insight papers based on best practices and learnings along the way; these can be shared widely with safety net providers, as well as state and national policy makers.
We will also engage with national experts and faculty for the Learning & Action collaborative convenings, and be advised by a national strategy board in addition to our national partners at the Foundation and NACHC and National Council.
11

12
13

14

The target audience are state primary care associations if the applicant is a primary care association, or behavioral health state associations that are members of National Council for Behavioral Health, if the applicant is a behavioral health state association. Ultimately, our goal is to award five state primary care associations and five behavioral health state associations.
We've had several questions about organizations sending in joint applications. This is something we definitely encourage. Associations can partner to submit a joint application, however only one award will be made per state and one entity needs to serve as the lead organization for the grant award.
The ideal applicant has experience and lessons to share. This opportunity is best suited for state associations that want to build on their experience by taking their work to another level, and/or exploring working in different ways, and work in new areas. These are organizations already working on care delivery transformation efforts with their providers, and they've started collaborating with their behavioral health primary care partners, depending where you stand in terms of your organization. These are also organizations that are currently working with key stakeholders and policy makers within their state, and these are organizations that are in state that have some significant value‐based payment opportunities underway or plans for those opportunities.
15

This slide lists some concrete examples of opportunities that move safety net providers towards category three or four alternative payment models.
16

With the Delta Center's aim of building and strengthening capacity in state organizations to support the providers on the ground to shift towards value‐based care and payment, we have designed a two year state Learning & Action collaborative that will provide grants in the amount of $240,000 per state association, and a range of technical assistance options. The TA options are designed to account for the differences in state association's capabilities and experience.
17

There will be a mix of in‐person types of TA support and learning through virtual modalities. In terms of the in‐person convenings, there will be seven in‐person convenings over the two‐year period. These are expected to be a day and a half long. We leverage some of the national convenings as part of this. During these in‐person convenings we will have some skill‐building workshops and learning labs. Attendees will have access to national experts addressing very specific topics. There will be peer sharing around best practices in how to support providers in making the changes that we're talking about, and there'll be joint problem solving around challenges.
The capability‐building webinars will focus on our technical content and address priority topics and areas that emerge from the grantees. Coaching will provide an opportunity for one‐on‐one customized support for grantees. Coaches can help grantees manage changes in working with provider networks, develop technical assistance plans, and help grantees problem solve around challenges.
There will also be expert consultations. These will be consultants with specific expertise in the different content areas we will be addressing. They will provide customized support and also group support to the state organizations participating on problem areas, and they will be able to do some initial assessments to help you as a state organization pinpoint your priority areas of focus and help to think through how to prioritize your resources.
18
We will also have some toolkits and support through a resource center that you could start using with your providers on the ground. This will be content designed at the provider level. It will include evidence‐based change packages, tools, and how‐to guides to help your providers make the care delivery changes that they need to and become well‐versed in some of the payment pieces.
The capability‐building workshops, or skills building workshops, will be embedded in the in‐person convenings.
You'll notice that there's two levels of TA. The technical assistance and coaching is targeted at state associations with the expectation that the state associations will then go and provide technical assistance and coaching to their provider networks to make the changes that need to happen to improve patient outcomes in these alternative payment models.
18
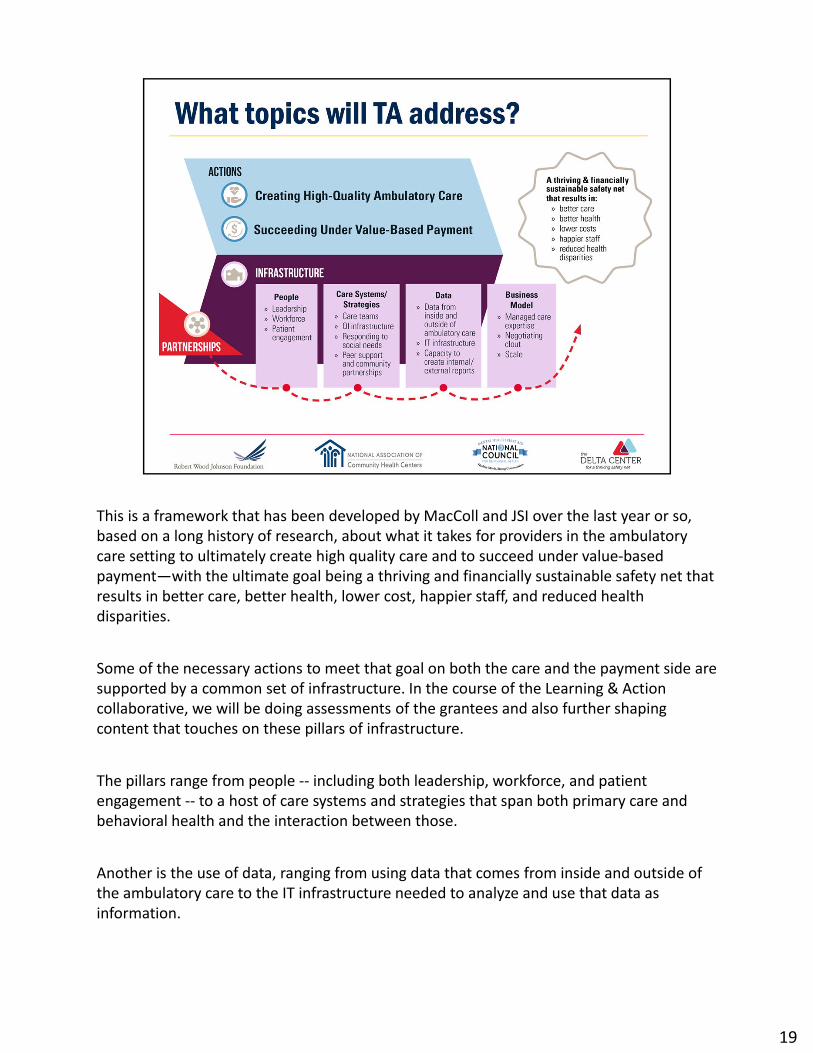
This is a framework that has been developed by MacColl and JSI over the last year or so, based on a long history of research, about what it takes for providers in the ambulatory care setting to ultimately create high quality care and to succeed under value‐based payment—with the ultimate goal being a thriving and financially sustainable safety net that results in better care, better health, lower cost, happier staff, and reduced health disparities.
Some of the necessary actions to meet that goal on both the care and the payment side are supported by a common set of infrastructure. In the course of the Learning & Action collaborative, we will be doing assessments of the grantees and also further shaping content that touches on these pillars of infrastructure.
The pillars range from people ‐‐ including both leadership, workforce, and patient engagement ‐‐ to a host of care systems and strategies that span both primary care and behavioral health and the interaction between those.
Another is the use of data, ranging from using data that comes from inside and outside of the ambulatory care to the IT infrastructure needed to analyze and use that data as information.
19

Another pillar is the business model that providers use to remain sustainable. This increasingly includes reaching out and being familiar with managed care plans, negotiating with those plans, as well as sometimes size and scale in order to have the necessary economies of scale to support all of the infrastructure needed to both create high quality care and to succeed under value‐based payment.
The final pillar relates to partnerships. Partnerships can be integral to helping to ensure that providers have the necessary infrastructure and capacities to serve their patients in optimal ways and to participate in some of the value‐based payment models that require more infrastructure than an individual provider might have.
19

Here is some of the proposed content of the Learning & Action collaborative.
Payment reform and policy transformation can range from how exactly to work with a Medicaid agency or health plan to explore specific payment models, to understanding and articulating specific value‐based payment options that providers may want to pursue and how to use data to communicate provider value, especially in a managed care environment.
Care delivery transformation ranges from the details of implementing team‐based care, to how primary care and behavioral health can work more collaboratively and use data to drive clinical decision making and do panel management, population health management, and address the health, social needs and behavioral health needs of patients. This is particularly relevant for complex patients.
Cultivating practices of a learning organization gets into the how of change, including how to apply adult learning principles to trainings, how to leverage top experts in the field, how to design effective evaluation tools, and how to cultivate a culture around continuous testing, measurement, and feedback that is all part of an ongoing quality improvement cycle.
20

Partnerships can include partnerships between providers including between primary care and behavioral health; providers within a sector like health centers collaborating with one another in the form of an IPA or an MSO; and cultivating relationships with hospitals or payers.
It is important to note that this is proposed content that will continue to be tailored and to evolve based on needs assessments with the 10 grantees. Our goal is to use some of the very learning organization principles that we will be fostering in the grantees to ensure that this Learning & Action collaborative is truly meeting the needs of the grantees and their providers on the ground.
20

Here is a timeline that outlines the convenings that all grantees will be expected to participate in. There are five convenings that will bring together the five primary care association and five behavioral health state association grantees together. There will also be two convenings that are targeted specifically towards PCAs and two convenings that will be targeted specifically toward behavioral health state associations. Those will each be aligned in terms of timing with the National Council For Behavioral Health Conference, and the NACHC conference specifically, so that we can ensure that we tailor some of the learning and some of the peer sharing to be focused within a sector while also having ample opportunity for all 10 grantees to do cross‐sector learnings and peer sharing.
There will also be a number of virtual learning opportunities, which will include check‐in calls with Delta Center staff, virtual webinars with grantees, and tailored TA hours with both Delta Center staff and expert faculty
21
22
The Delta Center will provide several things. We will provide a collaborative space for both in‐person and virtually for experts and organizations to share and learn together about transforming care and payment within provider networks. We'll also provide an opportunity for behavioral health and primary care state associations to continue their work and strengthen their work together to align and encourage providers on the ground to provide integrated whole person care for the patients they serve.
We will provide a robust array of technical assistance to support state organizations in strengthening capabilities and how they work with their providers on care delivery changes within alternative payment models. Finally, we'll provide grants in the amount of $240,000 to each state association. The funding is to enhance current efforts underway, and to encourage trying new ways of working and new changes and new types of partnerships to advance our knowledge around value‐based care and payment.
23

We're looking to fund five state primary care associations, and five behavioral health state associations. We’re looking for organizations that haven't just started their journey towards value‐based care and payment, but rather have been at it for awhile and have experience and some best practices and challenges to share.
We're looking for organizations that are trusted partners in delivering technical assistance to their providers. They're seen as leaders in providing this type of TA. These are organizations that have demonstrated leadership and taken action in pushing APMs forward in their state.
We are looking for state associations that are in a state where there are significant value‐based payment opportunities defined as in the works or there is planning underway, or these are active opportunities.
We're looking for organizations that are open to advancing partnerships that they have with their behavioral health or primary care association counterparts. It's about going beyond the status quo of what you may have in place now – about a new way to work together to really advance value‐based care and payment.
Finally, we're looking for a commitment from state associations to build these types of
24
capacities within their own organizations. That means protected time and a dedicated team to participate in all the Delta Center TA activities, and to have concrete plans for how you're going to provide TA to your provider networks.
24

The program expectations were designed to help grantees get a large enough dose to make the changes that are impactful, and that will be sustained beyond the life of the grant and TA opportunities.
We are asking grantees to be present, active learners and to share what you're learning, best practices and challenges. This collaborative is about all teaching and all learning together. You start thinking about ways to test new ideas, new partnerships, new ways of working with providers, and convene with stakeholders and policy makers, and payers to move the payment and policy forward.
We will have an external evaluator, Mathematica, that will be evaluating the overall program. We ask that you participate in the evaluation activities, and in activities that help the Delta Center learn how the program is going and how we could be more responsive to what you need.
We will also ask you to complete some assessments, put together work plans about how you're going to roll out technical assistance to your provider networks, and share your progress in quarterly reports.
25

Here is an overview of the process and timeline. We'll review the letters of intent that are submitted, and from that response pool we'll invite a select group of state associations to submit a full proposal. We will have an open Q&A for the LOI and another for those that have been asked to submit a full proposal. The full proposal deadline is April 13th. We will do some follow‐up interviews to clarify anything in the proposal and to explore questions that may come up in the review process. Acceptance emails will go out on May 16, and we’ll have our kick‐off in late June.
Note: The LOI release date has been updated to February 9.
26

27

Note: Questions and responses from the webinar will be available on the Delta Center website.
28

29