Embed Size (px)
Citation preview

Aetiology Of Bacteraemia Among Adult Aids Patients Attending Lagos University Teaching
Hospital (LUTH), Lagos, Nigeria
Ogunsola F. T, Arewa D. G, Akinsete I. E, Oduyebo 0. 0, 'Akanmu A. S. and Odugbemi T. 0
Department of Medical Microbiology 'Department of Haematology
College of Medicine, University of Lagos, P.M.B 12003, Lagos Nigeria
' Correspondence to
F. T. Ogunsola
Abstract
Background: Bacteraemia is a relatively common event in HIV-infected patients, especially in late infection. Studies in Africa have shown that more than 23% of AIDS patients have bacteraemia but there is paucity of data from Nigeria. Methods: Blood samples from 67 consecutive patients with A/OS attending the Lagos University Teaching Hospitafbetween April and August 2000 were cultured. Temperature, ESR, Full blood count, and where possible C04 counts were obtained. Socio-demographic details were also recorded. Thirty apparently healthy people were randomly selected from a low-risk population to act as non-AIDS controls. The Oxoid Signal Blood Culture System was used to investigate bacteraemia. Antibiotic sensitivity tests were carried out on all isolates. Results: Twenty-two (33%) of the 67 AIDS patients were culture positive. Non typhoidal Salmonella spp (45.5%), coagulase-negative staphylococci (22. 7%) and Staphylococcus aureus (18.2%) were most commonly isolated. One isolate each of Klebsie/la pneumoniae, Pseudomonas eeruqtnose and Bacillus spp were identified. All bacteraemic patients had temperatures above 3B°C and white blood cell counts ranged between 2, 700 - 13, 500/mm'. There was a high rate of antibiotic resistance particularly to ch/oramphenicol, tetracyclines, cotrimoxazole and b lactam antibiotics. However, most isolates were still susceptible to gentamicin and the fluoroquinolones. There was no significant difference in the socio-demographics of the bacteraemic AIDS and non-bacteraemic AIDS patients. Conclusion: Salmonella spp. were the most common aetiological agent of bacteraemia among AIDS patients seen at the Lagos University Teaching Hospital (LUTH), Niqerie. A high temperature was a pointer to the presence of bactaeraemia while total white blood cell counts were not useful. It is recommended that blood culture should be done for AIDS patients with elevated temperature irrespective of the total white blood cell count.
Key words: bacteraemia, human immunodeflency virus, AIDS, blood culture
Introduction
Al OS is a global pandemic which has killed more people than all the wot st war history and natural disasters put together and the sub-Saharan Africa is the region of the world most affected. An
estimated 26.6 rnil!ion people were living with HIV/AIDS and approximately 32.2 million new infections occurred in sub-Saharan Africa in 2002, while the prevalence rates as at 2003 ranged from about 1% in Somalia to over 37.5o/o in Botswana 1. The epidemic has in the past years, claimed the lives of an estimated 2.3 million Africans. Ten million young people(aged 15-24 years) and almost
3 million children have been orphaned by AIDS in sub-saharan Africa ( 1-4 ). AIDS cases were not reported in Nigeria until 1987. and till 1990, less than 200 cases were reported to the \Vorld Health Organization 1. However, by 1992, 552 HIV I AIDS cases were documented2 while in 1998 over 3 million Nigerians were already living with the human immunodeficiency virus' 7
. This made Nigeria fourth after Kenya, Congo Republic and Coted' lvoire in the prevalence of AIDS cases. Increases in the rate of new cases by 1999 made Nigeria second only to South Africa in the rating for number of people living with HIV I AIDSH9. As at December 2003, an estimated 5.8o/o of Nigeria populace were already suffering
The Nigerian Postgraduate Medical Journal. Vol. 16, No 3 Sept., 2009 186

Aetiology Of Bacteraemia Among Adult Aids, F. T. Ogunsola et al
from HIV infection with infection rates ranging from 0.5o/o in Gerdam. Yobe state to 21% in Otukpo, Benue State 1 .
The profound impairment of cellular immunity associated with HIV infection predisposes to bacterial infections with recurrent bacteraemia as well as other opportunistic infections in patients with AIDSl().n. Bacteraernia is a relatively common event in HIV-infected patients, especially under particular conditions such as intravenous drug abuse (IOU), use of central venous catheters, indwel l ing venous catheters, neutropenia. and hypogamrnaglobuhnaemia consequent on low CD4 � T-lymphocyte count!':" While it has been noted that as many as 50% of HIV
posiuve patients with bacteraemia may be asymptomatic". it can also present as a complication of other bacterial infections such as cndocarditis. pulmonary infection. urinary tract infection, gastrointestinal infection, soft tissue infection and many others 1,1 18 I'! 22-H
Studies in Africa revealed that between 16 and 30°/o of AIDS patients have bacteraemia; and that the most common pathogens are Salmonella spp. Staphylococcus aureus, coagulase negative staphylococci, K!ebsiella spp, Enterobacter spp. Streptococcus pneumoncae, Shigel!a spp, Pseudomonos aeruginosa and Mycobactenum spp'"" 2(,-JI. AIDS·associatcd bacteraemia due to species of Lactobacillus":": Gonococcus3\ -Campylobacter": J(,.
17: Hencobacrer":" liaemophilus rnjluenzae2'1303
�. Rhodococcus equi/C orynebacterium equr?": Mycobacterium tubercutosts":" have also been reported. There are however only a few studies done in Nigeria. Considering the rising epidemic profile of HIV I
AIDS and the importance of opportunistic infections in overall mortality and morbidity rates of AIDS patients in Nigeria, there is need for baseline data on ;\IDS associated bacteraemia. This study was therefore conducted to establish the prevalence ofbacteraemia and bacterial agents common with AIDS �ssociated bacteraemia.
i\'laterials and Methods
Sampling: A total of97 cases were studied. Blood samples were collected from 67 adults of both sexes with confirmed clinical AIDS attending gastroenterology and the two haematology out patient clinics in the Lagos University Teaching Hospital between April and August 2000 while the remaining samples were collected From 30 randomiy selected individuals of the population with low- nsk for HIV/AiDS as non-AIDS controls. Ethical clearance was obtained trorn the research ethic committee before the commencement of the study. Every participant recruited for this study voluntarily gave an oral consent before the questionnaire was administered and blood samples subsequently collected for blood culture.
PaJients' information: Information on socio-economic and demographic status of patients and controls as well as temperature and history of antibiotic therapy were obtained with questionnaires confidentially administered with the assistance of medical practitioners
Blood collection and culture: Ten milliliter (IOml) of venous blood aseptically collected with strict adherence to standard aseptic technique was immediately inoculated into Oxoid Signal Blood Culture System (Code BC 102) without allowing the blood to clot 1233 Bottles were incubated aerobically at 37'"C with daily visual exarmnation for evidence of growth as described in the manual (Oxoid signal culture s)'stem manual). Bottles with evidence of growth were subcultured on to Blood Agar Base medium (Oxoid) aseptically supplemented with 10% sterile sheep blood ''BA",
Chocolate Agar medium (heated Blood agar) "CA·· and MacConkey Agar medium (Oxoid) ·'MC''. Bottles without evidence of growth were terminally gram-stained and subcultured on .. BA··. ··cA··
and .. MC'" after 7 days of incubation before discarding. fhe ··sA .. and .. MC" plates were incubated aerobically at 37"C while ··cA··
plates were incubated in 5-JOo/o C02 at 37"C. All plates were incubated continuously for 5 days before discarding. Colonies from primary plates were subcultured appropriately to obtain pure isolates for standard characterisation and identification 43.
Haematology parameters: All haematology parameters including
CD4+ "l-Iyrnphocyte cell counts were obtained from patients' medical records.
Characterisation and identification of bacterial isolates: Isolates were characterised and subsequently identified on the basis of their cultural. colonial and ceil morphoiogy, and brcchcmica! characteristics including diagnostic enzymes and sugar fermentation
tests.
Antibiotic susceptibility testing: This was done to measure the bacterial susceptibility to some antibiotics 1n vitro. based on the principle of comparative disk diffusion using Mueller-H inton Agar. All the tests were performed in a single batch and all procedures were standardised both for test and controls strains and perforrned according to the National Committee for Clinical Laboratory Standards. Standard strains of E coli ATCC 25922 and ATCC'
35218, Staphylococcus aureus ATCC 25923 and Pseudomonas aeruginosa ATCC 27853 were used as controls. Results were interpreted by comparing the zone of inhibition of test strains with that of control strains. Zone of inhibition greater than or equal to that of control was interpreted as sensitive while those Jess than the zone of inhibition of the control were interpreted as resistant".
Data analysis: EPi info 2004 {version 3.2.2) was used for darn. entry. validation and analysis. Statistical methods were by ANOVA and chi square analysis.
Results
Of the 67 AIDS patients. there were 29 (43.2%) males and 38 (56.72°/o) females with a male to female ratio of I : 1 .3 . All the AIDS patients were between age of 2 1 and 58 years with mean. median and mode of 37. 35 and 32 years respectively. Non-AIDS controls had age range between 24 and 47 years.
The socio-demograhic parameters of the 67 AIDS patients are represented in figure I . Thirty six (54o/o) of the AIDS patients had formal education up to secondary level. Nineteen 19 (28%) were"single" while 22 (33%) were married. At least 1 1 (30o/o) had a history of blood transfusion either alone or during surgery while IO (26%) had a previous history of major surgery. All the non AIDS controls had tertiary education while only 4( 13 .33%) and 3( 10°/o) had a history of major surgery (with blood transfusion) and blood transfusion respectively.
Only 3 of the 67 AIDS patients, with ages � 40 years had HIV I and II dual infection while 64 (95.So/o) had HIV I alone. There was no case of infection with HIV II alone. A significant percentage was on various antimicrobial agents. About 30 (44.0°/o)
were on antibacterial drugs, 25 (37 .0%) were on antiviral drugs. 29 {40.0%) on antiparasitic drugs and J 1(16.5%) were on anti-TB drugs. However, only five of the controls were on antibiotic and
The Nigerian Postgraduate Medical Journal. Voi. i 6, No 3 Sept , 2009 i87
Aetiology Of Bacteraemia Among Adult Aids, F. T. Ogunsola et al
anliparasilic drugs. Fhe prevalence of bacteraernia among AIDS patients was
33°/o (22 of the 67 casesjstudied. T\VO of the three patients with HIV I and II dual infection had bacteraemia while there was no case ofbacteraernia among non-AIDS controls. There was no case of polyrnicrobial bacteraemia in the study. Non-typhoidal Sahnonetla spp were the most prevalent accounting for IO
('15.45%) of all isolates. These were followed by coagulase - negativc Staphylococcus spp 5 (22. 73o/o) and Staphylococcus
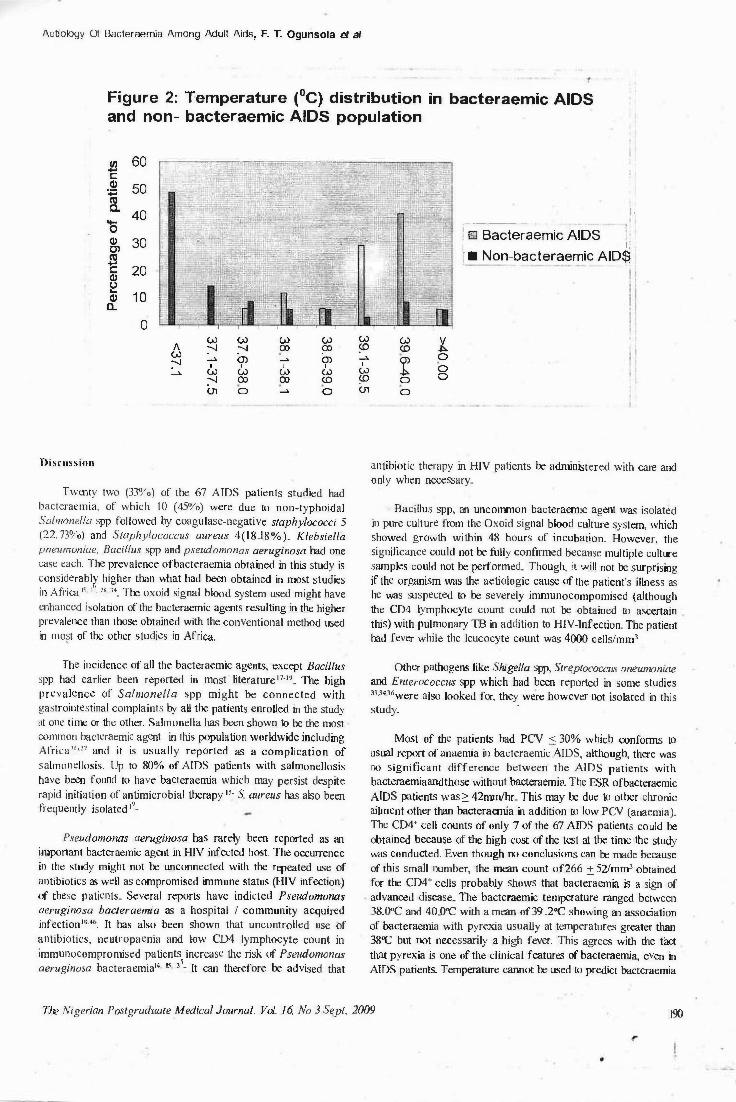
aureus 4 ( 18.18°/o) while there was only one isolate for each of Klebsie/la pneumoniae. Pseudomonas aeruginosa and Bacillus spp. Figure 2 shows the temperature distribution in the general AIDS population and the bacteraernic AIDS patients. For the non bacteraernic AIDS, the minimum temperature was 35.8°C while the maximum temperature was 40(C. The mean,·mode and median were 37 .5°C. 36.6°C and 37 .211C respectively. For the bacteraemic AIDS patients. the minimum temperature was 38°C while the maximum was 4011C. The rnean, mode and median temperatures were 39.J°C. 39.8°( and 39.3°C. Non-AIDS controls had temperature range between 36.5"C and 38.0•,C. The bacteraemic AIDS cases had higher temperatures than the non-bacteraernic AIDS (p < 0.05)
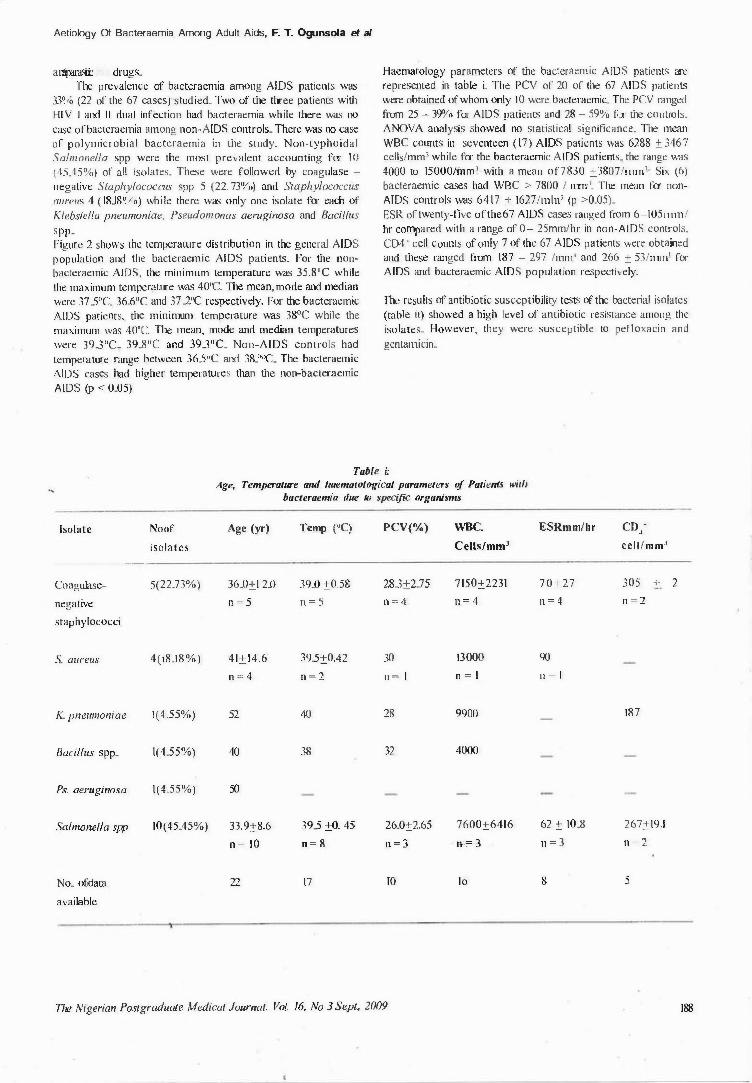
Haematology parameters of the bacteraernic AIDS patients are represented in table i. The PCV or 20 of the 67 AIDS patients were obtained of whom only IO were bacteraemic. The PCV ranged from 25 - 39o/o for AIDS patients and 28 - 59% for the controls. ANOVA analysis showed no statistical significance. The mean
WBC counts in seventeen ( 17) AIDS patients was 6288 ± 346 7 cells/mm' while for the bacteraemic AIDS patients. the range was 4000 to 15000Hnm3 with a mean of7830 ±3807/1111n1. Six (6)
bacteraemic cases had WBC > 7800 / 111111.1. Fhe mean for non AIDS controls was 6417 ± 1627/t111113 (p >0.05). ESR of twenty-five ofthe67 AIDS cases ranged from 6-105111,n/ hr compared with a range of 0- 25mm/hr in non-AIDS controls. C04 ... cell counts of only 7 of the 67 AIDS patients were obtained and these ranged from 187 - 297 /mn13 and 266 ± 53/1111111 for AIDS and bacteraemic AIDS population respectively.
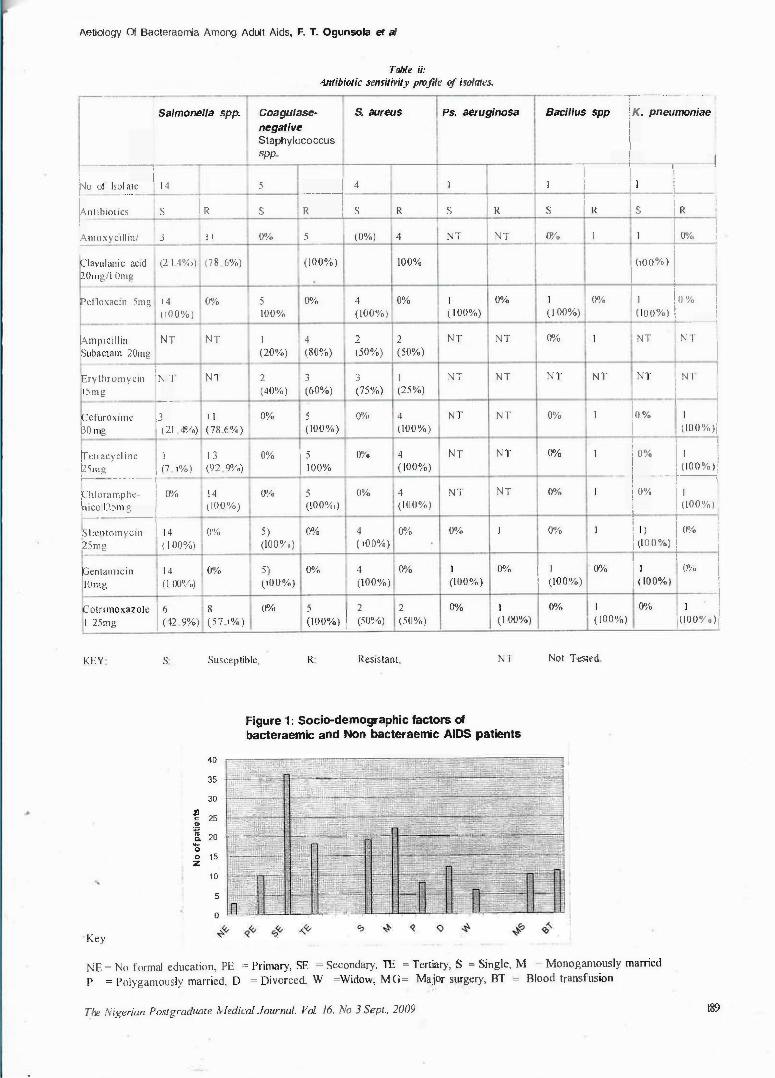
The results of antibiotic susceptibility tests of the bacterial isolates (table ii) showed a high level of antibiotic resistance among the
isolates. However. they were susceptible to pefloxacin and
gentarmcin.
·Table i:
Age, Temperature and ltaematological parameters of Patients willt bacteraemia due to specific organisms
Isolate Noof Age (yr) Temp ("C) PCV(%) WBC. ESRmm/hr CD/
isolates Cells/mm3 cc ll/mm1
---------
Coagulase- 5(22.73%) 36.0:+:I 2.0 39.0 ±0.58 28.3±2.75 7150±2231 70±27 305 + 2
negative n = 5 n = 5 n = 4 n = 4 n = 4 n = 2
staphylococci
S. aureus 4(18. 18%) 41±14.6 39.5±0.42 30 13000 90
n = 4 n = 2 n = I n = 1 n = l
K. pneumoniae 1(4.55%) 52 40 28 9900 187
Bacillus spp. 1(4.55%) 40 38 32 4000
Ps. aeruginosa 1(4.55%) 50
Salmonella spp 10(45.45%) 33.9:+:8.6 39.5 ±0. 45 26.0±2.65 7600±6416 62 :+: 10.8 267±19.I
n = 10 n - 8 n - 3 rr= 3 n = 3 n = 2
No. ofdata 22 17 IO IO 8 5
available
The Nigerian Postgraduate Medical Journal. Vol. 16, No 3 Sept., 2009 188
Aetiology Of Bacteraemia Among Adult Aids, F. T. Ogunsola et al
Table ii:
Autibiotic sensitivity profile of isolates.
--
I Salmonella spp. -f .-;,,�um�ni�e Coagulase- S. aureus Ps. aeruginosa Bacillus spp
negative
:--�-� Staphylococcus spp. I i
·----+--,-----1 I I ' I �o of lsnlmc 1 4 5 -� 4 I I I ' I I !
' ' I I
i I R ' ' I nnbroucs s I R s s R s s R s \ R
rmoxyc1ll1n/ 3 1 1 0% 5 (0%) 4 NT I NT Oo/o I I i 0%, I '
\100%) I Clavulamc acid (2 J.4%J) (78 6%) (100%) 100% 20mg/l Omg I . i ' ' I Pcfloxecm 5mg 1 4 0% 5 0% 4 0% I 0% I 0% I l o % (100%) 100% (100%) ( I 00%) ( I 00%) 1100%> I I
I �50%) ----I
lA..mpicillin NT NT I 4 2 NT NT 0%, I NT . N f I Subactam 20mg (20%) (80%) (50%) !
IErythromycin I�, NT 2 J J I NT NT NT NT NT ! N"l I
1.'img (40%) (60%) (75%) (25%) ' ' ' Cefuroxunc 1 1 0% 5 0%, 4 NT NT 0% I l o % I I GO mg l21 4°/o) (78.6%) (100%) (100%) i (\00%)j
I ' ! [Ietracycfme I I 3 0%
I ioo% Oo/o 4 NT NT 0%, I
r J 1 ' t2.'img I (7 1%) (92 9o/o) ( 100%) ! ( 100%):
f---- - - - · - · " - r . - 1--�, I f"hloramphe- ' 0% 1 4 ()O/o 5 0% 4 NT NT 0% I OO/o ' I
�-12.'im�t (100%) (100%,) (100%) '
I (100%) - ' I 1 4 I ' f)t1eptornyc111 O'Yo 5) 0% 4 0% 0% I 0% I l I ) l O�'o
t2Smg ( l OO'Yo) (IOOo/o) ( 100%) I ,100%) 1
' ' ..
l ' I Dentanucin 1 4 0% 5) 0% 4 0% I 0% I I 0%
I !100%) Oo/o ! IOmg ( I Q()O/o) (100%) (100%) (100%) I (100%)
- I
Cotnmoxazolc I �42 9%) 8 0%, 5 I 2 2 0% 1 0% I O�'o I I
! I 25mg (57. 1%) (100%) I (50°/o) (50%) (I 00%) ( 100%) j(lOOo/o):
KEY s Susceptible, R Resistant, NT Not Tested.
Key
40
35
30
� 25 c
� 20 �
0 0 15 z
10
5
Figure 1 : SocilHlemographic factors of bacteraemic and Non bacteraemic AIDS patients
NE= No formal education, PE = Primary, SE = Secondary, TE = Tertiary, S = Single, M = Monogamously married p = Polygamously married, D = Divorced, W =Widow, MG= Major surgery, BT = Blood transfusion
The Nigerian Postgraduate Nledical Journal. Vol. 16, No 3 Sept., 2009 189
Actrology Of Bacteraemla Among Adult Aids, F. T. Ogunsola et al
Figure 2: Temperature (°C) distribution in bacteraemic AIDS and non- bacteraemic AIDS population
.l'J 60
c: Q)
50 .a
a 40
0 Q) 30 Ol
s c 20 Q) o ..
1 0 Q)
0..
0 (,.) (,.) (,.) (,.) cc s» v
A :--J :--J a, a, c.o co .ls (,.)
� CJ) � Cl) � CJ) 0
:--J ' ' ' ' ' !.. 0
� i» (,.) co w w 0
:--J co a, co c.o 0
"' 0 � 0 "' 0
�------
I ,
,·--·-- --- -
' Kl Bacter aemic A I D S I ,
j • No n - bact e raem ic A I D $
Discussion
Twenty two (33o/o) of the 67 AIDS patients studied had bactcraemia, of which IO ( 450/o) were due to non-typhoidal Salmonefla spp followed by coagulase-negative staphylococci 5 (22. 73o/o) and Staphylococcus aureus 4(18.18%). Klebsiella pneumontae, Bacillus spp and pseudomonas aeruginosa had one case each. The prevalence ofbacteraemia obtained in this study is considerably higher than what had been obtained in most studies in Africa 15 1"· u, 14. The oxoid signal blood system used might have enhanced isolation of the bacteraemic agents resulting in the higher prevalence than those obtained with the conventional method used in n1o�t of the other studies in Africa.
The incidence of all the bacteraemic agents, except Bacillus spp had earlier been reported in most literature"-". The high prevalence of Salmonella spp might be connected with gastrointestinal complaints by all the patients enrolled in the study at one tirne or the other. Salmonella has been shown to be the most common bacteraemic agent in this population worldwide including Africau>27 and it is usually reported as a complication of salmonellosis. Up to 80% of AIDS patients with salmonellosis have been found to have bacteraemia which may persist despite rapid initiation of antimicrobial therapy 11• S. aureus has also been frequently isolated 1').
Pseudomonas aeruginosa has rarely been reported as an important bacteraemic agent in HIV infected host. The occurrence in the study might not be unconnected with the repeated use of antibiotics as well as compromised immune status (l·HV infection) of these patients. Several reports have indicted Pseudomonas aeruginosa bacteraemia as a hospital I community acquired iufection'v'". It has also been shown that uncontrolled use of antibiotics. neutropaenia and low CD4 lymphocyte count in immunocompromised patients increase the risk of Pseudomonas aeruginosa bacteracmia14 is 3�. It can therefore be advised that
antibiotic therapy in HIV patients be administered with care and only when necessary.
Bacillus spp, an uncommon bacteraemic agent was isolated in pure culture from the Oxoid signal blood culture system, which showed growth within 48 hours of incubation. However. the significance could not be fully confirmed because multiple culture samples could not be performed. Though, it ·.viii not be surprising if the organism was the aetiologic cause of the patient's illness as he was suspected to be severely immunocompomised (although the CD4 lymphocyte count could not be obtained to ascertain this) with pulmonary TB in addition to HIV-Infection. The patient had fever while the leucocyte count was 4000 cells/mm3
Other pathogens like Shigella spp, Streptococcus oneumon1ae and Enterococcus spp which had been reported in some studies 33
.3436were also looked for, they were however not isolated in this
study. -
Most of the patients had PCV .S 30% which conforms to usual report of anaemia in bacteraemic A.IDS, although, there was no significant difference between the AIDS patients with bacteraemiaandthose without bacteraemia, The ESR ofbacteraemic AIDS patients was� 42mm/hr. This may be due to other chronic ailment other than bacteraemia in addition to low PCV (anaemia). The CD4+ cell counts of only 7 of the 67 AJDS patients could be obtained because of the high cost of the test at the time the study was conducted. Even though no conclusions can be made because of this small number, the mean count of266 ± 52/mm3 obtained for the CD4+ cells probably shows that bacteraemia is a sign of advanced disease. The bacteraemic temperature ranged between 38.0"C and 40.0<'C with a mean of39 .. 2°C showing an association of bacteraemia with pyrexia usually at temperatures greater than 38<C but not necessarily a high fever. This agrees with the tact that pyrexia is one of the clinical features of bacteraemia, even in AIDS patients. Temperature cannot be used to predict bactcraemia
The Nigerian Postgraduate Medical Journal. Vol. I 6, No 3 Sept., 2009 190

Aetiology Of Bacteraemia Among Adult Aids, F. T. Ogunsola et al
in AIDS patients since most of the AIDS patients observed had pyrexia without a positive blood culture. However temperatures above 39°C was significantly associated with bacteraemia inAJDS patients (p < 0.05)
The bacterial isolates showed a high rate of resistance to most antibiotics, particularly those commonly used for empiric therapy. All the staphylococci were resistant to penicillin, tlucloxacillin, oxacillin, azithromycin and cefuroxime. This further _confirms the rising trend of multiple resistance to b-lactam antibiotics, particularly cephalosporins and anti-staphylococcal drugs as earlier reported 47. A significant percentage of Sabnonella spp were resistant to chloramphenicol (100°/o), a,noxycillin I
clavulanic acid (78.6°/o). cefuroxime (78.6%), tetracycline (92.9%) and cotrimoxazole (57.1 %). This may explain the reason why rnany of the patients still had bacteraenua despite the antibiotics used (mainly only for other reasons). All the bacterial isolates were susceptible to pefloxacin and gentamicin. The fact that quinolones (among which pefloxacin is one) are very expensive drugs while gentamicin is only available in parenteral formulation and thus are not as easily abused as most other cheap-orally administered drugs may explain their relative efficacy.
As it has been previously reported, a large percentage (up to 50°/o) of HIV-positive patients with bacteraemia may be asymptomatic. Since bacteraemia is a life-threatening condition and a common event in patients with acquired immunodeficiency syndrome (A[DS), blood culture and susceptibility test should be made a compulsory investigation for effective management of opportunistic infections in HIV-infected patients. Considering the high rate of resistance to most commonly prescribed antibiotics, it is thus necessary to raise an audible alarm to medical professionals 1nanagingAIDS patients in Nigeria to strongly discourage the use of cotrimoxazole, chloramphenicol, Amoxycillin or Atnoxycillin/ Clavulanic acid for the treatment of salmonella infections. Quinolones and aminoglycosides should be considered very important in formulating an empiric antibiotic therapy for AIDS patients. Larger studies with extensive haematological data are needed to establish some Of the relationship reported amongAIDS patients in this study, including ESR, full blood count, WBC differentials and GD4 .. cell count.
References
I. Willia,ns E. E., Mohammed I., Chikwen J. et al. HIV - I and HIV -2 in Nigerian Population with high-risk and low-risk behaviour patterns (letter). AIDS 1990i4: 1041 �1042.
2. Federal Ministry of Health. Hand book on HIV infection and AIDS for health workers. FMOH, Lagos, Nigeria. 1992; !06.
3. Okonofua T. Editorial comment. Women S Health Form 1999� 4(2)
4. World Health Organization. Global HIV, AIDS and STD Surveillance. WHO, Geneva. 1997
5. World Health Organization. The state of health in the world health reports. Life in 21st century: a vision for all. WHO, Geneva 1998; 57-58.
6. UN AIDS. Report of the Global HIV /AIDS epidemic in Africa 2002.
7. Federal Ministry of Health, Nigeria. 2003 National HIV sero-prevalence sentinel survey. Technical Report. Federal Ministry of Health, Abuja. 2004.
8. Dropulic L. K., Leslie J. M., Eldred L. J., Zenilman J. and Sears C. L. Clinical manifestations and risk factors of
Pseudomonas aeruginosa infection in patients with AIDS. J. Infect. Dis. 1995; 171(4): 930-937.
9. Tumbarello M., Tacconelli E., Caponera S., Cauda R., and Ortona L. The impact ofbacteraemia on HIV infection. Nine
years experience in a large Italian University Hospital. .!.
ln/ectl995.31(2): 1 2 3 - 1 3 1 . I 0. Fichtenbaum C. J ., Dunagan W. C., and Powderly V,./. G.
Bacteraemia in hospitalized patients infected with the human
immunodeficiency virus: a case control study of risk factors and out come. J. Acquir. Immune. Defic. Syndr. /{11111
Retrovirol. 1995; 8( I): 51 - 57. 1 1 . Meyer C. N., Skinhoj P., and Prag J. Bactcramia in HIV -
positive and AIDS patients; incidence, species distribution. risk factors, outcome, and influence of long - term prophylactic antibiotic treatment. Scand. J. tnfea Dis 1994: 26(6): 635 -642.
12. Krumlolz H. M., and Sande M . A . Community acquired bactcracmia in patients with acquired immunodeficiency syndrome. Clinical Presentation, bacteriology and outcome. Am�ricanJournaJ of Medicine 1989; 86: 776 -779.
13. Witt D. J., Craven D. E., and McCabe W. R. Bacterial infections in adult patients with the acquired immunodeficiency syndrome (AIDS) and AIDS - related
complex. American Journal o/A1edicine 1987; 82: 900-906. 14. Roviglione M. C., Battan R., Pablos M .A . et al. Infection
associated with catheters in patient with acquired immunodeficiency syndrome. American Journal cfMedicine
1989; 86:780-786. 15. Gilkes C. F., Brindle R. J., Oueno et al. Life threatening
bacteraemia in HIV-seropositive adults admitted to hospital in Nairobi, Kenya. lancet 1990; 336: 545 - 549.
16. Petit P. L., Haarlem J. V., Poelman M., Haverkamp M. C .. Wamola L A. Bacteraemia in patients presenting with fever. East African Medica/Journal 1995; 72(2): 1 1 6 - 1 2 0 .
17. Batchelor F., Kimar J. N., and Brindle R . .J. Microbiology of HIV associated bacteraemia and diarrhoea in adults from
Nairobi, Kenya. £pidemiol. Infect 1996: 1 1 7 : 139� 144.
18. Bonard D., Aka K., Zabhibo J .C . , You B .. Gomba P. el "al
HIV associated mycobacteraernia in West Africa (Letter]. Int. J. Tuberc. Dis. 1999; 3(6): 546.
19. Horwitch C. A., Furseth H. A., Larson A. M .. Jones T. L.,
Olliffe J. F. and Spach D. H. Lacto!:.acillaemia in three patients with AIDS. Clin. Infect. Dis. 1995 2 ! 16): 1460- 1462.
20. Owens L. J., Bradford C. A., Rhodes S. S. et al. Clinical Course and Presentation of lactobacil/us bacteraemia in AIDS patients. Clinical Infect. Dis. 1995; 63: 421 �30.
21 . lesson M. B. and Clark A. J. lactobaci/lus bacteria in HIV infected patients. Eur. J. Clin Micro. Infect. Dis. 1997; 183: 250-254.
22. Jacoby H. M., and Mady B. J .. Acute gonococcal sepsis in an HIV-infected woman. Sex. Transm. Dis. 1995; 22(6): 380 -382.
23. Peterson M. C., Fair R. W., Castiglia M. Prosthetic hip infection and bacteraemia due to Campyiobacter Jejuni in a patient with AIDS. Clin. Infect. Dis. 1993; 16: 439.
24. Pigrau C., Almirante B .. Bartolome R .• and Pahissa A. Bacteraemia due to Campylobacter spp in patients with 1 1 1 V infection. Med Clin. Bare 1994; 103(6): 239.
25. Manfredi R., Nanetti A., Ferri M., Chiodo F. Fatal Campylobacter Jejuni bacteraemia in patients with AIDS. J.
Med Microbiol.1999;48(6):601-603. 26. Kiehlbauch J. A., Tauxe R. V., BakerC. N., Wachsmith I. K.
Helicobacter cinaedi associated bacteraemia and cellulitis in immunocompromised patients Ann. Intern. Med. 1994:
The Nigerian Postgraduate Medical Journal. Vol. 16, No 3 Sept., 2009 191
Aetiology Of Bacteraemia Among Adult Aids, F. T. Ogunsola et al
\ 2 [ ( 2 ) · 9 0 - 9 3 . 27 Weir SC. Gilbert CL. Gordin, FM, Fischer SH. Gill VJ. An
uncommon Heficobacter isolate from blood: evidence of a group of 1-fehcobocter spp. pathogenic in AIDS patients. J.
Cl111 M,crob,ol 1999: 3 7(8): 2729 -2733. 28. Burman W. J , Cohn D. L .. Reves R. R., Wilson M. R.
Mu!tifocal c e l ! u l i t i s and rnonoarticylar arthritis as a manifestation of Hehcobacter cinaedi bacteraemia in AIDS patients Clin. Infect Dts. 1995; 20(3): 564-570.
29. Cross J T. (Jr), Davidson K. W., and Bradsher R. W. (Jr). Hacmophilus nuluenzae epididymo-orchitis and bacteracmia in a man infected with the human immunodeficiency virus. C/;n Infect. Dis. 1994: 19(4): 768 - 796.
30. Tierra R .. Oceja E .. Barai na E. J., Zubero Z., Munoz J., Cisterna R., Santa,naria .I. M. Bacteraemia caused by /-laemopht!us injluen:zae with special reference to its relation to HIV infection. Enferm. lnferm. lnfecc. Microbsol. C/in. 1994: 1 2 ( 1 ) : 3 4 - 3 7 .
3 1 . Archibald L. K .. den-Du[k M. 0. et al Fatal i\Jycobacterium t ubercutosis blood stream infections in febrile hospitalized adults 111 Dar es Salaam, Tanzania. Chn lnfecl. Dis 1998; 20(2)· 290- 296.
32. World Health Organization. Basic Laboratory procedures in clinical bacteriology. W.H.0 publication, Geneva Switzerland 1991 .
33. Miller J. M. Specimen collection and processing: blood collection. In A guide to specimen Management in Clinical ivticrobiology (2nd ed). American Society for Microbiology Press, Washington DC 1999; 53 -56.
34. Tietz A C .. Stonrung F. 0. et al Bacterial infection in patients with AIDS -A Review or the Literature. Hosp. Clin Fae Med Sao Paulo 1989; 5 1 ( I) : 26-33.
15 Krclhofuer M. et al Life threatening Pseudomonas aeruginosa infections in patients with human immunodeficiency virus infection. Chn Inject. Dis 1992: 14: 403 - 4 1 1 .
36 Libman H. and \Vitzburg R. A. HIV infection: A primary Cate Manual (3 cd). Little Brown and Company, Boston. 1996.
37 Pigrau C.,Almirante B., Bartolome R., PahissaA. Bacteraemia due to Campylobacter spp in patients with H[V infection. Med. C/in. Bare 1994; !03(6): 239.
38. Moxon ER. Haemophilus influenze.ln: Mandell GL. Bennett JE, Dolin R eds. Principles and Practice of Infectious Diseases. New York: Churchill Livingstone, 1995: 2039-2045
39 W.H.O. WHO Regional Office for South-East: Bacterial infections In HIV guidelines on standard operating procedures for laboratory diagnosis of Hl v-Opportunisuc infections. W.H.O publication, Geneva, Switzerland 2003
40. Drancourt M, Bonnet E, Gallais H. et al. Rhodococcus equi infection in patients with AlDS. J infect. 1992; 24 · 1 2 3 - 1 3 1
4 1 . Donisi A, Suardi MG, Casari S. et al. Rhodococcus equi infection in HIV-infected patient. AIDS 1996: 10:359-362.
42. Mc Donald LC et al. Unrecognised A1ycobaclerium tuberculosis bacteraemia among hospital inpatients in less developed countries. Lancet 1999: 354· 1 1 5 9 - 1 1 6 3 .
43. Forbes B. A., Sahm D. F., and Weissfield A. S. Diagnostic Microbiology, Tenth e d it io n . Arnertcan Society for Microbiology, Washington 1998.
44. National Committee for Clinical Laboratory Standards (NCCLS). 'Performance Standard for Antimicrobial Disk Susceptibility testing 8th ed: Approved standard NCCI..S Documents M2-A8 and M I 00-S 13 (M2) . Villanova Pa: NCCLS2003.
45. Weinstein M. P., Reller L .B . , Murphy L. R., and Lichtenstein K. A. The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes ofbacreraemia and fungemia in adult. Laboratory and epidemiology observations. Rev infect Dis 1983; 5: 35-51
46. Mendelson M. H., Gurtman A., Szabo S., Neihart E .. Meyers 8. R., Policar M., Cheung T. W., Lillienfeld D., Hammer G, Reddy S. et al Pseudomonas aeruginosa bacteraemia in patients with AIDS. Clin infect Dis 1994; 18: 886-895.
47 Ogunsolaf. T., Kesah C. N., and Odugbemi T Antimicrobial resistance in Nigeria: An overview. Nig. Qt. J. Hosp. Med 1997; 7(1 ): 57-61
The Nigerian Postgraduate Medical Journal. Vol. I 6, No 3 Sept .. 2009 192





![[XLS] Inventory... · Web view8/24/2015 4 4 4 2 1 0 0 0 0 2 2 0 0 0 0 2 0 0 3 0 0 3 0 0 1 0 0 1 0 0 2 4 0 1 4 0 1 2 0 2 4 0 2 3 0 0 0 0 2 0 0 1 0 0 0 0 0 3 3 0 3 1 0 0 1 0 2 1 0 1](https://img.pdfslide.us/doc/110x75/5af02f227f8b9ac2468db355/xls-inventoryweb-view8242015-4-4-4-2-1-0-0-0-0-2-2-0-0-0-0-2-0-0-3-0-0-3.jpg)















![[XLS]sscmpr.orgsscmpr.org/noticeboard/CEN-1/CEN-1-1.xlsx · Web view1 6000001 1 2 2 0 0 2 495001 1 1 6000001 2 2 1 0 0 2 495001 1 1 6000001 3 2 0 0 0 2 495001 1 1 6000001 4 2 0 0](https://img.pdfslide.us/doc/110x75/5aaab56b7f8b9a7c188e6bc3/xls-view1-6000001-1-2-2-0-0-2-495001-1-1-6000001-2-2-1-0-0-2-495001-1-1-6000001.jpg)





