Embed Size (px)
Citation preview

Title: Variation in the position of the Conus Medullaris and Dural Sac in adult dogs
Authors: Zohra Khan1, Elizabeth Munro1, Darren Shaw1, Kiterie M E Faller1*
Authors’ affiliation: 1The Royal (Dick) School of Veterinary Studies. The University of
Edinburgh, Easter Bush Campus, Midlothian, EH25 9RG.
Qualifications:
Zohra Khan BVMS MRCVS
Elizabeth Munro VetMB MA DVR MRCVS
Darren Shaw BSc PhD
Kiterie Faller DVM DPhil DipECVN MRCVS
* Corresponding author: Kiterie M E Faller. [email protected]
Word Count: 3174 (excluding title page, abstract, references, figures and tables.)
1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16

ABSTRACT:
Although it has long been stated that the level of spinal cord termination varies depending on the
size of the dog, the evidence for this remains limited. The aim of this study is to investigate the
position of the conus medullaris and dural sac in a population of dogs of varying size.
Magnetic resonance images of the thoraco-lumbo-sacral spine of one hundred and one dogs were
included. The location of conus medullaris and dural sac was determined on sagittal T2-weighted
magnetic resonance images and T1-weighted images respectively by three independent
observers. The body weight and the back length were used as markers of size.
Regression analysis showed that the termination point of the conus medullaris had a statistically
significant relationship with bodyweight (R2=0.23, p<0.05). Although not statistically significant
(p=0.058), a similar relationship was found between conus medullaris and back length (R2=0.21).
No statistically significant relationship was found between the termination point of the dural sac
and bodyweight (p=0.24) or back length (p=0.19).
The study confirms the terminal position of the conus medullaris is dependent on size, with a
more cranial position with increasing size; however, the termination point of dural sac remains
constant irrespective of dog size.
Keywords:
Conus medullaris, dural sac, dog, MRI, spinal cord anatomy, tethered cord syndrome
2
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37

INTRODUCTION:
In mammals, the spinal cord tapers to a point caudal to the lumbar intumescence known as the
conus medullaris (CM). At the CM, the central canal dilates to form the ventriculus terminalis
(terminal ventricle), the parenchyma narrows to form a layer of columnar ciliated ependymal
cells lining the terminal ventricle and a very thin glia layer and thicker pia layer; this is
collectively known as the filum terminale (terminal filament). The dura mater and arachnoid
mater extend beyond the CM forming the lumbar cistern containing cerebrospinal fluid (CSF).
Caudal to the lumbar cistern the dural sac (DS) constricts around the filum terminale forming the
spinal dura mater filament, which anchors at one or two sites on a sacral or coccygeal vertebrae.
(1-3)
During early embryological development, the spinal cord extends along the full length of the
vertebral column. The spinal nerves pass out of the corresponding intervertebral foramina, which
at this stage are directly opposite their point of origin. As the embryo and later the neonate
develop, the vertebral column continues to extend as spinal cord growth slows; this continues to
maturity meaning in the adult animal the spinal cord does not occupy the whole length of
vertebral canal.(1)
It is known that the position of the conus medullaris relative to the vertebrae varies between
species.(4) It has long been thought that in larger dogs the cord terminates more cranially when
compared to smaller breed dogs; however this is only based on a single cadaveric study from
1966 involving thirty-eight dogs, most of them being medium sized.(5)
3
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60

Knowing the position of termination for the CM and DS has clinical applications in terms of site
of CSF sampling or epidural local anaesthesia. Additionally it would help with the identification
of pathological variations in the position of the CM such as tethered cord syndrome: a congenital
disorder described in both humans and dogs characterised by an abnormal caudal traction of the
CM.(6-11)
The aim of the study is to determine the position of the CM and DS termination in a population
of dogs of various sizes and evaluate whether these termination points depend on the size of the
dog. Our hypotheses were that the CM position depends on the size of the dog whilst the end
point of the DS is a species constant.
MATERIALS AND METHODS:
Study design:
This is a retrospective, single-centre study performed at the Hospital for Small Animals of the
University of Edinburgh. All patients were client owned dogs and were scanned as part of
diagnostic investigations. Ethical approval was obtained from the ethics board of the University
(VERC 116.17). The clinical database was searched for dogs which required magnetic resonance
imaging (MRI) of the vertebral column between January 2017 and May 2018. The MR images
were acquired with the patients positioned in dorsal recumbency with the pelvic limbs in a
relaxed “frog-legged” position, achieving a neutral view of the lumbosacral vertebral column.
The images were acquired using a 1.5 Tesla field strength MRI scanner (Philips Achieva™,
Philips Medical Systems, Reigate, UK).
4
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83

Inclusion and exclusion criteria:
We searched for dogs, for which a sagittal T2-weighted and where available a sagittal T1-
weighted MR scan had been acquired of the thoraco-lumbo-sacral vertebral column including at
least the second thoracic vertebrae and part of the sacrum. Only dogs aged greater than 12
months and for which a body weight was available on the patient records were included. Cases
were excluded if a mid-sagittal image was not available, there was a deviation from the normal
canine vertebral formula or presence of vertebral malformations or finally, if a caudal lumbar or
lumbosacral myelopathy was found.
Size of dog was determined by two methods: the bodyweight, and the distance between the
second thoracic vertebrae and the seventh lumbar vertebrae was used as a surrogate of the dog
size, independent of body condition. This distance was measured on a single mid-sagittal image
if available or sequential images in larger patients. This length was considered equivalent to the
distance between the most dorsal points of the scapula and the wing of the ilium in the standing
patient,(12) which can easily be measured on the live animal, and was referred to as back length.
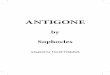
The termination of the CM was determined from a mid-sagittal T2-weighted image in which the
hyperintense CSF highlights the comparatively hypointense spinal cord. The termination of the
DS was determined from a mid-sagittal T1-weighted image in which the hypointense CSF within
the dural sac is delineated by the comparatively hyperintense epidural fat. The measured level of
termination for both structures was then attributed to the corresponding half of the vertebral body
by drawing a perpendicular line to the long axis of the spinal cord or dural sac (Figure 1). This
was performed by three observers (ZK, KF and EM), a neurology resident, a board-certified
5
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106

neurologist and a board-certified radiologist; each observer was blinded to the patient size and
the other observers’ results. Individual termination points for each patient were based on two or
three observers agreeing or where there was no agreement, the mean of the three observers’
results. Finally, to assess intra-observer reproducibility, one observer (ZK) graded all images on
a second occasion three months later. Before statistical analyses, the sequential halves of the
vertebral bodies were assigned a numerical value from one (cranial half of fifth lumbar vertebra)
to eight (caudal half of the sacrum).
Statistical analysis:
All statistical analyses were performed using R Statistical Software (R Foundation for Statistical
Computing, Vienna, Austria). The termination points of the CM and DS were assigned a
numerical value between one and eight according to the corresponding vertebral bodies; this
conversion assumed a linear relationship for vertebral body length. To determine the effect of
bodyweight and back length on the termination points of the CM, Poisson regressions were
performed with the residuals being normally distributed. For the termination points of the DS, no
such normality of residuals was observed, and instead ordinal logistic regressions were
performed. Percentage agreement and Fleiss’s Kappa were used to assess the inter-observer
agreement between the three observers for the termination points of the CM and the DS,(13) and
the intra-observer agreement was evaluated using percentage agreement and Cohen’s Kappa. The
guidelines recommended by Landis and Koch were used to interpret the Kappa coefficients.(14)
RESULTS:
6
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128

One hundred and one dogs met the inclusion criteria. One hundred dogs had T2- weighted
images of the thoraco-lumbo-sacral spine. One dog was included in the DS analysis but excluded
from CM analysis as all three observers independently agreed that the quality of the T2-weighted
images was too poor to reliably assess the position of the CM. Twenty-four dogs were excluded
for the DS position evaluation (for twenty-three patients, T1-weighted images had not been
acquired, and for one patient, the full length of the sacrum had not been included), leaving 77
dogs for DS analysis. The median bodyweight of the patients was 13.0 kilograms (range and
interquartile range 4.1-67.5; 6.9-28.2 kg) (Figure 2).
The inter-observer percentage agreement for two or more observers was 93.0% and 96.1% for
CM and DS termination points respectively. The intra-observer percentage agreement was 88.0%
and 90.0% for CM and DS termination points respectively. When evaluating the inter-observer
agreement, Fleiss’s Kappa gave a value of 0.54 (confidence interval (CI): 0.47-0.60) for the CM
and 0.37 (CI: 0.28-0.46) for the DS, leading to moderate and fair level of inter-observer
agreement respectively. When evaluating the intra-observer agreement, Cohen’s Kappa gave a
value of 0.83 (CI: 0.74-0.92) for the CM and 0.79 (CI: 0.66-0.93) for the DS, leading to almost
perfect and strong level of intra-observer agreement respectively (Table 1).(14)
Table 1: Inter- and Intra-observer variability in assessing the termination points for both the
conus medullaris and dural sac.
Conus medullaristermination point
Dural sactermination point
Number(n = 100)
Percentage (%)
Number (n=77)
Percentage (%)
Inter- Number of 3 54 54.0 40 51.9
7
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148

observer variability
observers in agreement
2 39 39.0 34 44.2
0 7 7.0 3 3.9Fleiss’s Kappa (95% Confidence interval) 0.54 (0.47-0.60) 0.37 (0.28-0.46)
Intra-observer
variability
Number of observations in
agreement
2 88 88.0 69 90.0
0 12 12.0 8 10.0Cohen’s Kappa (95% Confidence interval) 0.83 (0.74-0.92) 0.79 (0.66-0.93)
We evaluated the relationship between the size of the dog and the position of the CM and DS
respectively. The size was determined by two methods: the body weight and the back length.
Using a Poisson regression, there was a statistically significant relationship between the
termination point of the CM and bodyweight (McFadden pseudo-R2 = 0.23, p<0.05) (Figure 3
A). Although not statistically significant (p=0.058), a similar relationship was found between
CM and back length (McFadden pseudo-R2 = 0.21) (Figure 3 C). Using an ordinal logistic
regression, no statistically significant relationship was found for the termination point of the DS
and bodyweight (p=0.24) or back length (p=0.19) (Figure 3 B and D).
To further highlight the difference in position of the conus medullaris depending on body size
and to give the reader the expected/most frequent position of CM and DS for a dog of a specific
size, we split dogs into bodyweight categories of less than 5 kilograms (kg), between 5 and 10
kg, between 10 and 25 kg, between 25 and 40 kg and greater than 40 kg; these categories were
chosen according to Hawthorne et al.(15) In the less than 5 kg group the most commonly
observed termination points for the CM were the cranial and caudal halves of the seventh lumbar
vertebra found in 33.3% and 44.4% of dogs respectively. In the 5 to 10 kg group, the most
commonly observed CM termination point was the cranial half of the seventh lumbar vertebrae
8
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166

found in 40.0% of dogs. In the 10 to 25 kg group, the most commonly observed CM termination
points were the caudal half of the sixth and cranial half of the seventh lumbar vertebrae found in
36.7% and 40.0% of dogs respectively. In the 25 to 40 kg group, the most commonly observed
CM termination point was the caudal half of the sixth lumbar vertebrae found in 62.5% of dogs.
Finally, in the over 40 kg group the most commonly observed CM termination point was the
caudal half of the sixth lumbar vertebra, which was found in 85.7% of dogs. Using the regression
equation (Figure 3 A), predicted terminations points for the CM were calculated using the mid-
point for each of the above-mentioned weight categories. The predicted termination points of the
CM aligned accurately with the most commonly observed termination points for this population
of dogs (Table 2). Furthermore, the most commonly observed DS termination points was the
cranial half of the sacrum irrespective of body weight, further confirming the absence of
relationship between body weight and the DS termination point.
Table 2: Most commonly observed conus medullaris and dural sac termination points in our
population. Predicted termination points of CM were calculated using the regression equation.
The number 4-7 in italic refers to our grading system where the sequential halves of vertebral
bodies have been assigned to a number from the caudal half of the sixth lumbar vertebrae to the
cranial half of the sacrum: e.g. 4 represents the caudal half of L6, 5 the cranial half of L7, 6 the
caudal half of L7 and 7 the cranial half of the sacrum).
Conus medullaris Dural sac
9
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186

Body- weight
(kg)
Most commonly observed
termination point (value
from our grading system)
Percentage % (n)
Predicted termination
point
Body-weight used
for predicted
termination point (kg)
Most commonly observed
termination point (value
from our grading system)
Percentage % (n)
<5Cranial and caudal L7
(5/6)77.7 (7) 5.1 2.5 Cranial
Sacrum (7) 50.0 (4)
5-10 Cranial L7 (5) 40.0 (12) 4.9 7.5 Cranial
Sacrum (7) 68.0 (17)
10-25Caudal L6 and cranial L7 (4/5)
76.7 (23) 4.6 17.5 Cranial Sacrum (7) 81.0 (17)
25-40 Caudal L6 (4) 62.5 (15) 4.1 32.5 Cranial
Sacrum (7) 52.9 (9)
>40 Caudal L6 (4) 85.7 (6) 3.7 50 Cranial
Sacrum (7) 83.8 (5)
DISCUSSION:
In this study, we have shown that the CM position varies between dogs and a relationship exists
between CM position and bodyweight. However, the position of the DS remains constant
independent of dog’s size.
In both humans and canines during embryological development, the spinal cord initially occupies
the full length of the vertebral column; ultrasonographical studies have shown in foetuses of both
species the termination of the conus medullaris migrates cranially in the vertebral column
through gestation.(16, 17) During postnatal development, the vertebral column continues to
elongate and the caudal lumbar, sacral and coccygeal spinal segments progressively become
10
187
188
189
190
191
192
193
194
195
196
197
198

more cranial to their respective vertebrae.(3) To avoid dogs for which further CM migration
could occur, dogs less than twelve months old were excluded from the study population.
However, for some large and giant breed dogs, adult bodyweight and skeletal maturity is
achieved beyond 12 months of age. One study showed that toy, small, and medium breed dogs
reached 99% of their adult weight at approximately 9 or 10 months old, whereas large and giant
breed dogs reached this point at approximately 11 to 15 months old.(15) In our study population
there were only four dogs, which were between 12 and 24 months of age, these were all small
breed dogs weighing between 4.1 and 9.8 kg, consequently the age at MR imaging, and potential
for further growth are unlikely to have affected the results.
In larger dogs, growth and the vertebral column elongation occurs for a longer period than in
smaller dogs; therefore, it is not surprising that the CM ends up being located more cranially in
larger dogs. Conversely to the relatively mobile CM, the spinal dura mater filament attaches at
one or two points to a sacral or coccygeal vertebrae,(2) this anchoring of the DS may provide an
explanation to why the position of the CM varies with bodyweight and the DS termination does
not.
To assess non-invasively the position of the CM and DS on a large population of dogs, we used
MR images. MRI has been extensively used in people to study variation of spinal cord length
with gender, age and race. A human literature review revealed most of these studies use sagittal
T2-weighted and/or T1-weighted images to identify the CM, whilst sagittal T1-weighted images
are most often used to assess DS position. Occasionally, dorsal or transverse views or MR
myelography were analysed.(18-25) Based on this information, we opted to use T2-weighted
11
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221

images to determine the position of CM as the surrounding CSF is markedly hyperintense
compared to the spinal cord parenchyma, allowing easier identification of the CM. A T1-
weighted image was used for identification of the DS as it gives good contrast between the
hypointense CSF and the hyperintense epidural fat.
Before analysing the relationship between dog size and spinal cord terminations, we had to
evaluate the reproducibility of our grading system, both in terms of intra and inter-observer
agreement. The percentage of agreement are high, however some kappa (κ) values only show fair
agreement. Both percentage agreement and κ coefficients can be used to assess both inter-
observer and intra-observer variability. κ coefficients take into account the agreement may have
occurred by chance, so often the values are less than those achieved by measuring percentage
agreement. In addition, weighted κ index can be used for ordinal or ordered categorical variables
and lead to a stronger agreement in cases where observers choose adjacent categories.(13)
However, a weighted κ indices is not available for more than two observers, so could not be used
to assess inter-observer variability in this study. This may explain why only a fair agreement
between the three observers is obtained for the position of the dural sac despite a high inter-
observer percentage agreement and the fact that even if all observers disagreed, it was never by
more than two grades. It has been suggested that both percentage agreement and κ coefficients
should be used to assess inter-observer agreement in studies where the observers are well trained
and unlikely to guess, whereas when there is higher likelihood of guessing, κ coefficients are
likely to be a more accurate assessment of true agreement.(26)
12
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244

Being able to more accurately estimate the position of the termination of the spinal cord and its
relationship to the termination of the DS is of great importance when sampling CSF from the
lumbar cisterna and also when considering anaesthesia or analgesia in this region. CSF collection
is most often performed from the lumbar subarachnoid space at the junction between the fifth
and sixth or sixth and seventh lumbar vertebrae; however, the junction between the fourth and
fifth lumbar vertebrae or the lumbosacral junction can also be used.(27, 28) Inaccuracy could
lead to damage of the terminal segment of the spinal cord or failure to obtain a sample. Epidural
injections are commonly performed at the lumbosacral junction as it provides the largest access
to the epidural space. Inaccurate needle placement can lead to subarachnoid or intrathecal
injections, which can be hazardous as the dose of anaesthetic or analgesic agents are much lower
when used intrathecally compared to epidural placement.(29)
The results show there is a statistically significant variation in termination point of the conus
medullaris between small and large breed dogs, however there is variability between individuals
of similar weights. This makes ascertaining the termination point of the spinal cord for a specific
dog difficult. The authors would still always recommend attempting lumbar CSF sampling as
caudal as possible even in very large breed dogs and only if the tap is “dry” should you try more
cranially, therefore as much as possible avoiding iatrogenic trauma to the spinal cord.
A further clinical application is during the diagnosis of tethered cord syndrome, a congenital
disorder described in humans, which is characterised by an abnormal caudal traction of the conus
medullaris. In humans, it can be found in association with ventral positioning of the conus
medullaris within the vertebral canal, lipid infiltration of the filum terminale,
13
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267

lipomyelomeningocoele, myelomeningocoele, myelocystocoele, meningocoele, split cord
malformations, dermal sinus, anorectal malformations and intramedullary tumours.(10) Tethered
cord syndrome has been reported in dogs in association with congenital vertebral and spinal cord
malformations such as spina bifida, myeloschisis, meningocoele and myelomeningocoele.(6, 7,
9, 11) More recently tethered cord syndrome has been identified as a sole finding in a canine
patient causing progressive pelvic limb lameness.(8) Currently, diagnosis in dogs remains
challenging considering the lack of data of normal anatomical position of the conus medullaris,
therefore being able to estimate the expected position of the CM would further aid diagnosis of
this condition.
This study has the limitations of a retrospective study including the distribution of the body sizes
in the study population and using images not specifically acquired for their purpose.
The median bodyweight of the patients was 13.0 kg, with a range 4.1 to 67.5 kg. The majority of
the study population were less than 25 kg of bodyweight, with 69% of dogs less than 25 kg of
bodyweight, 24% between 25 and 40 kg and 7% greater than 40 kg. This distribution of
bodyweight suggests the conclusions drawn from this study are more applicable to toy, small,
medium and large breed dogs, than for giant breed dogs.
During investigations of thoracolumbar myelopathy, commonly obtained MR images include the
thoracic, lumbar and sacral segments and T1-weighted and T2-weighted sequences. In two
human studies assessing the relationship between CM, body mass and age, the use of tranverse
and dorsal sequences helped better identify the termination points of the caudal spinal cord.(19,
14
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290

25) However, in our hospital, transverse images of the caudal spinal cord do not tend to be
acquired in absence of pathology in that area. A study in human subjects assessing the impact of
age and gender on the CM and DS terminations also used an MR myelography sequence to
identify the endpoint of the dural sac. This sequence accurately differentiates the epidural fat
from the cerebrospinal fluid;(24) however, currently we limit the use of this specific technique
for investigation for spinal arachnoid diverticula. A true mid-sagittal image is required for
accurate identification of the terminations points of both the CM and DS. However, when
reviewing the retrospective images, the area of interest, which prompted the MRI acquisition, is
often not the lumbosacral region so positioning for this region may have not be optimal. A
prospective study including equal proportions of dogs of various sizes, with fine slice sagittal,
tranverse T1-weighted and T2-weighted MR sequences and an MR myelography sequence
between the fifth lumbar and first coccygeal vertebrae with optimal positioning of this region
would allow more accurate identification of the conus medullaris and termination of the dural
sac.
In conclusion, the results of the study confirm the widespread belief that the position of the
conus medullaris is dependent on bodyweight, with a more cranial position with increasing
bodyweight. However, the termination of dural sac remains similar despite increasing
bodyweight.
Competing interests:
None declared.
15
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313

16
314
315
316
317

REFERENCES:
1. Uemura EE. Spinal Cord. In: Fundamentals of canine neuroanatomy and
neurophysiology. Ames, Iowa: Wiley Blackwell; 2015:99-119.
2. Marin-Garcia P, Gonzalez-Soriano J, Martinez-Sainz P et al. Spinal cord central canal of
the German shepherd dog: morphological, histological, and ultrastructural considerations.
J Morphol. 1995;224:205-12.
3. Fletcher TF. Spinal Cord and Meninges. In: Evans HE, Miller ME, De Lahunta A,
editors. Miller's anatomy of the dog. Fourth ed. St. Louis, Missouri: Elsevier Saunders;
2013:589-610.
4. De Lahunta A, Habel RE. Vertebral Column and Spinal Cord. In: Applied veterinary
anatomy. Philadelphia: Saunders; 1986:202-21.
5. Fletcher TF, Kitchell RL. Anatomical studies on the spinal cord segments of the dog. Am
J Vet Res. 1966;27:1759-67.
6. Acevedo Naranjo CM, Martínez MdP, Ruíz Sierra IC et al. Tethered spinal cord
syndrome in an english bulldog puppy. A case report. Revista Colombiana de Ciencias
Pecuarias. 2008;21:87-96.
7. Cloquell A, Mateo I, Munoz A. Spina bifida, myelomeningocele and tethered cord as the
cause of incontinence and paraphimosis in a dog. Diagnosis by Computed Tomography
and myelography. Clinica Veterinaria de Pequenos Animales. 2012;32:81-6.
8. De Decker S, Gregori T, Kenny P et al. Tethered cord syndrome associated with a
thickened filum terminale in a dog. J Vet Intern Med. 2015;29:405-9.
17
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338

9. Fingeroth J, Johnson G, Burt J et al. Neuroradiographic diagnosis and surgical repair of
tethered cord syndrome in an English bulldog with spina bifida and myeloschisis. J Am
Vet Med Assoc. 1989;194:1300-2.
10. Hertzler DA, DePowell JJ, Stevenson CB et al. Tethered cord syndrome: a review of the
literature from embryology to adult presentation. Neurosurgical focus. 2010;29:E1.
11. Shamir M, Johnston D, Rochkind S. Surgical treatment of tethered spinal cord syndrome
in a dog with myelomeningocele. Vet Rec. 2001;148:755–6.
12. Evans HE, De Lahunta A, Miller ME. Skeleton. In: Miller's anatomy of the dog. Fourth
ed. St. Louis, Missouri: Elsevier Saunders; 2013:589-610.
13. Hallgren KA. Computing inter-rater reliability for observational data: an overview and
tutorial. Tutorials in quantitative methods for psychology. 2012;8:23-34.
14. Landis JR, Koch GG. The measurement of observer agreement for categorical data.
Biometrics. 1977;33:159-74.
15. Hawthorne AJ, Booles D, Nugent PA et al. Body-weight changes during growth in
puppies of different breeds. J Nutr. 2004;134:2027S-30S.
16. Zalel Y, Lehavi O, Aizenstein O et al. Development of the fetal spinal cord: time of
ascendance of the normal conus medullaris as detected by sonography. J Ultrasound
Med. 2006;25:1397-401.
17. Amer MS, Hassan EA, Torad FA et al. Sequential Canine Neonatal Spinal
Ultrasonography from Birth till Spinal Ossification. Pakistan Veterinary Journal.
2015;36:6-10.
18. Saifuddin A, Burnett SJ, White J. The variation of position of the conus medullaris in an
adult population: a magnetic resonance imaging study. Spine. 1998;23:1452-6.
18
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361

19. Binokay F, Seydaoğlu G, Erman T et al. Relationship between the levels of normal conus
medullaris and body mass index in the Turkish adult population. Neurosurgery
Quarterly. 2013;23:81-4.
20. Demiryürek D, Aydingöz Ü, Akşit MD et al. MR imaging determination of the normal
level of conus medullaris. Clin imaging. 2002;26:375-7.
21. Kim J-T, Bahk J-H, Sung J. Influence of age and sex on the position of the conus
medullaris and Tuffier's line in adults. Anesthesiology. 2003;99:1359-63.
22. Malas M, Seker M, Salbacak A et al. The relationship between the lumbosacral
enlargement and the conus medullaris during the period of fetal development and
adulthood. Surgical and Radiologic Anatomy. 2000;22:163-8.
23. Macdonald A, Chatrath P, Spector T et al. Level of termination of the spinal cord and the
dural sac: a magnetic resonance study. Clin Anat. 1999;12:149-52.
24. Soleiman J, Demaerel P, Rocher S et al. Magnetic resonance imaging study of the level
of termination of the conus medullaris and the thecal sac: influence of age and gender.
Spine. 2005;30:1875-80.
25. Wilson DA, Prince JR. MR imaging determination of the location of the normal conus
medullaris throughout childhood. Am J Roentgenol. 1989;152:1029-32.
26. McHugh ML. Interrater reliability: the kappa statistic. Biochemia medica. 2012;22:276-
82.
27. Chrisman CL. Cerebrospinal Fluid Analysis. Vet Clin North Am Small Anim Pract.
1992;22:781-810.
28. Lorenz MD, Coates JR, Kent M. Confirming a Diagnosis. In: Handbook of veterinary
neurology. 5th ed. St Louis, Missouri: Elsevier Saunders; 201:75-92.
19
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384

29. Valverde A. Epidural analgesia and anesthesia in dogs and cats. Vet Clin North Am Small
Anim Pract. 2008;38:1205-30.
20
385
386
387
388

FIGURE LEGENDS
Figure 1: Sagittal (A) T2-weighted and (B) T1-weighted magnetic resonance images of the
lumbo-sacral vertebral column. The termination points of (A) the conus medullaris and (B) the
dural sac were attributed to the corresponding half of the vertebral body by drawing a line
perpendicular to the long axis of the spinal cord. In this example the CM ends in the cranial
portion of L7 and the DS in the cranial part of the sacrum; all observers independently agreed to
this.
Figure 2: Histogram representing the distribution of the bodyweight within the study population.
Figure 3: Relationship between (A) the termination of the conus medullaris and bodyweight, (a
statistically significant relationship was found using Poisson regression,
y=exp(1.65−0.007*BW)); (B) the termination of the dural sac and bodyweight (no relationship
was found using an ordinal logistic regression); (C) the termination of the conus medullaris and
back length, (a statistically significant relationship was found using Poisson regression,
y=exp(1.87−0.01*(T2−L7 length))) and (D) the termination of the dural sac and back length (no
relationship was found using an ordinal logistic regression).
21
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406