Embed Size (px)
Citation preview

Title Page:
1. Title: Decision modelling in donation after circulatory death (DCD) liver transplantation.
2. Authors: McLean KA 1, Camilleri-Brennan J 1, Knight SR 1, Drake T 1, Ots R 1, Shaw CA 1,
Wigmore SJ 1, Harrison EM 1.
1 Clinical Surgery, University of Edinburgh, Royal Infirmary of Edinburgh.
3. Keywords:
Outcomes.
Quality of life.
Markov.

Footnote Page:
1. Abbreviations: Donation after brain death (DBD)
Donation after circulatory death (DCD)
Health-related quality of life (HR-QoL)
Model of end-stage liver disease (MELD)
Quality-adjusted life years (QALYs)
Short form of liver disease quality of life (SF-LDQOL).
2. Grants and Financial support: None.
3. Conflicts of interest: None.
4. Correspondence Author:
Mr Ewen Harrison.
Royal Infirmary of Edinburgh
51 Little France Crescent
Edinburgh EH16 4SA
E-mail: [email protected]
Phone Number: 0131 242 3614.

Abstract: Word count: 274/275.
Introduction: Donation after circulatory death (DCD) liver allografts are increasingly used for
transplantation. However, the post-transplantation clinical and quality of life outcomes of DCD
recipients are traditionally considered to be inferior compared with donation after brain death (DBD)
allograft recipients. Decision making for such marginal organs can be difficult. This study investigated
the optimal decision to accept or decline a DCD liver allograft for a patient based on their current
health.
Methods: A Markov decision process model was constructed to predict the 5 year clinical course of
patients on the liver transplant waiting list. Clinical outcomes were determined from the UK Transplant
registry or appropriate literature. Quality-adjusted life years (QALYs) were determined using the
condition-specific “Short form of liver disease quality of life” (SF-LDQOL) questionnaire.
Results: There were 293 / 374 (78.3%) eligible patients who completed the SF-LDQOL
questionnaire. Seventy-three respondents (24.9%) were pre-transplant and 220 were post-transplant
(DBD-recipient, 57.0%; DCD-recipient, 10.2%; re-transplant recipient, 7.9%). Predictive modelling
indicated that quality-adjusted life years (QALYs) gained at 5 years were significantly higher in DCD-
recipients (3.77, 95% CI=3.44–4.10) compared to those who remained on the waiting list for a DBD
transplant with model of end-stage liver disease (MELD) scores of 15-20 (3.36, 95% CI=3.28–3.43),
or >20 (3.07, 95% CI=3.00–3.14). There was no significant advantage for individuals with MELD
scores <15 (3.55, 95% CI=3.47–3.63).
Conclusion: This model predicts that patients on the UK liver transplant waiting list with MELD
scores >15 should receive an offered DCD allograft based on the QALYs gained at 5 years. This
analysis only accounts for donor-recipient risk pairings seen in current practice. The optimal decision
for patients with MELD scores <15 remains unclear, however a survival benefit was observed when a
DCD organ was accepted.

1. Introduction:First performed in humans in 1963 1, liver transplantation remains the sole intervention with curative
potential for end-stage liver disease 2. In the UK, the active waiting list for liver transplantation has
more than doubled in the past decade (264 in 2004/5 to 549 in 2013/4) 3, highlighting a growing
discrepancy between organ demand and availability. In combination with sustained improvements in
surgical expertise and post-transplantation care, there has been renewed interest in live-donor 4 and
split-liver transplantation 5. Furthermore, expansion of the liver allograft criteria to include previously
unconsidered ‘marginal donors’ has involved donor livers from older patients, and from those with
underlying pathologies or prolonged ischaemic periods 6.
Despite this renewed interest, cadaveric donations comprise over 98% of liver transplantations in the
UK 7. These are classified as either being donated after brain death (DBD), or donated after
circulatory death (DCD). DCD liver transplantations have become increasingly prevalent in recent
years, constituting 17% of all transplantations in 2013/14 3. However, due to the prolonged warm
ischaemic period, these allografts are far more susceptible to severe reperfusion injury than DBD
livers 8. As a result, DCD-recipients often experience inferior outcomes in terms of survival, graft
rejection rates, post-transplant complications 9-12, and health-related quality of life (HR-QoL)13, 14.
Ischaemic cholangiopathy is a particular concern in DCD-recipients 15, 16 and is associated with further
increased morbidity, reduced HR-QoL, and often necessitates re-transplantation. However, it should
be noted that with rigorous organ selection and a sufficiently skilled transplantation team, DCD
outcomes can be comparable to DBD patients 17-19.
Consequently, there is uncertainty with regards to the optimal pathway for those on the liver transplant
waiting list. When a liver transplant becomes available, a surgeon can decline a transplant to wait for
a potentially ‘higher quality’ DBD liver for their patient, accepting the risk of clinical deterioration and
removal from the list or death 20. Conversely, they may choose to proceed with transplantation,
irrespective of the organ type, with potentially inferior post-transplantation outcomes. Markov decision
process models can be utilised to model these complex choices 21, and they might therefore be able
to provide crucial clarification in these situations. The aim of this study was to determine the optimal
decision for a patient when a DCD liver allograft becomes available based on the current health of the
patient.

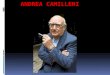
2. Methods:2.1. Markov Model:A Markov decision process model was constructed to reflect the clinical course of patients currently
on the UK liver transplant waiting list (Figure 1). The model is a necessary simplification of the clinical
process. When a DCD liver becomes available (the start of the model), the on-call transplant team
together with the patient must decide to either accept or decline this allograft. The latter choice entails
the patient remaining on the waiting list until a DBD transplant is available, or until there is significant
clinical deterioration.
Patients could exist within four pre-transplantation health states: three based on MELD score (<15,
15–20, >20), and death (an aggregate measure of death on the waiting list and delisting).
Furthermore, there are four post-transplantation health states defined as survival without ischaemic
cholangiopathy (T), survival with ischaemic cholangiopathy (IC), survival after re-transplantation (RT),
or death. Each state has a defined number of actions possible which allows transition from one state
to another during a cycle, and the probability of this transition is based solely upon their current state.
Each cycle lasted 1 month (30 days), with a limit of 5 years (60 cycles) due to the limited clinical data
available beyond this point. Each patient remained within the model until the final cycle (cycle 60) or
their death, which acted as an ‘exit state’ (the probability of further transition being 0). The 30-day
transition probabilities used in the model are presented in Supplement A.
The model depends on several fundamental assumptions; there can only be one state transition per
cycle, the transition probabilities are independent of the underlying cause of end-stage liver disease
(ESLD), patients could only receive one re-transplantation (which could with a DBD organ only), and
the type of transplantation would not affect the clinical course of ischaemic cholangiopathy.
2.2. Clinical outcomes:Clinical outcomes within the model were primarily derived from data routinely collected for patients
who underwent liver transplantation at the seven UK Liver Transplant Units (extracted from the UK
Transplant Registry on 30 August 2012). This database included all deceased donor liver
transplantations performed in adult patients (aged ≥18 years at the time of transplant) in the UK
between 1st January 2001 and 31st December 2011. It excluded all transplants involving DCD livers
out-with Maastricht category 3 (an expected circulatory arrest 22); any performed outside the seven UK
Liver Transplant Units; and all procedures including multi-organ, heterotopic, split, or reduced liver
transplants. Patients designated as having fulminant liver failure were further excluded as DCD
organs are rarely used in this context. All MELD scores referenced are biological MELD scores.
The probabilities of being transplanted or dying on the waiting list (transition probabilities) were
determined from United States Scientific Registry of Transplant Recipients data, adjusted to the

median wait period as determined using UK NHS Blood and Transplant registry data 3. Similarly, the
clinical outcomes for patients with ischaemic cholangiopathy were derived from the literature 15, 23.
Ischaemic cholangiopathy was defined as strictures, irregularities, or dilatations of the intrahepatic or
extra-hepatic bile ducts of the liver graft excluding isolated strictures at the bile-duct anastomosis, as
determined by clinical imaging 15, 23.
2.3. Health-related quality of life:
Quality-adjusted life years (QALYs) were used to quantify the effectiveness of each decision. The
previously validated ‘Short form of liver disease quality of life’ (SF-LDQOL) questionnaire 24 was used
to assess the health-related quality of life (HR-QoL) in pre- and post-transplantation patients. This
questionnaire was administered to all patients who attended the Scottish Liver Transplantation Unit for
an outpatient clinic or wait list assessment during the study period (16th July 2015 to 3rd September
2015), after verbal consent was obtained. The electronic patient record was subsequently accessed to
obtain additional sociodemographic and clinical information. Formal institutional ethical approval was
not required as this study was considered a service evaluation, otherwise involving routinely collected
data.
2.4. Statistical Analyses:
Continuous data were summarised as a mean or median and analysed using parametric or non-
parametric tests, as appropriate. Categorical data were cross-tabulated and differences in proportions
were tested using chi-square (Χ2) or Fisher’s exact tests. Survival analyses were performed using
Kaplan-Meier estimation and log-rank tests. Where appropriate, clinical outcomes were adjusted
using backwards stepwise elimination multivariate logistic regression analyses.
To minimise the impact of missing quality of life data, questionnaires and variables with a substantial
number of missing responses were excluded from the analysis and multiple imputation using chained
equations (MICE) 25 was subsequently performed. This method of multiple imputation involves
sequential regression of each variable with missing data to provide more credible complete datasets.
All questionnaire responses were assigned a value based upon the original Likert scale 24, and all
domains were equally weighted before being summated into an overall score. Five complete data sets
were imputed and an overall pooled estimate was generated (in accordance with Rubin's rules 26).
This was used to assign an average QALY value for each pre- and post-transplantation patient group.
‘Perfect’ health was accorded a value of 1 QALY whereas death was assigned a value of 0, with
intermediate values for all other patient groups.
Probabilistic sensitivity analyses (Monte-Carlo simulation, n=10,000) and one-way sensitivity analyses
were conducted to account for uncertainties in model parameters, including the length of time on the
waiting list. In the base-cases of these analyses, the estimated clinical and quality of life outcomes for
a patient who received a DCD liver transplant was compared (in turn) to a patient who remained on
the waiting list at a MELD score of <15, 15-20, and > 20. This allowed simulation of the optimal

decision for an individual within each MELD category. These base-case values are listed in Table 2
and Supplementary Tables 1a-c (Supplement A) and Table 2.
All analyses were performed in R v2.1 (R Foundation for Statistical Computing, Austria) and Markov
models were constructed using TreeAge Pro 2011 software (Treeage Software Inc., Williamstown,
MA, USA). Two-tailed statistical significance was set at the level p <0.05.

3. Results:
3.1. Post-transplantation clinical outcomes:A total of 488 DCD and 4340 DBD liver transplantations were performed in the UK between the 1st
January 2001 and 31st December 2011. The baseline characteristics of donors and recipients were
investigated after stratification by type of transplantation (Table 1). There were numerous prominent
differences between these groups, most notable being significantly lower donor ages (p<0.001);
MELD scores (p=0.03); cold ischaemic times (p<0.001); and reperfusion times (p<0.001) in DCD-
recipients.
Over the 11 year period, there were 4465 primary liver transplantations and 962 (21.5%) post-
transplantation deaths, with 158 (16.4%) of these deaths occurring in the first 30 days after
transplantation. Those who received a DCD transplantation had significantly lower probability of
survival post-transplantation over the 11 year period (p=0.02). In comparison, there were just 375 re-
transplantations in the UK and 129 post-transplantation deaths (34.4%), with 37 of these deaths
(28.7%) in first 30 days.
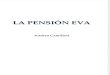
3.2. Health-related quality of life:There were 374 patients eligible for inclusion during the study period (Figure 2). Of these, 306
(81.8%) completed the questionnaire, while 46 (12.3%) declined participation, and 22 (5.9%) were not
encountered. A further 13 (3.5%) were subsequently excluded due to questionnaire incompleteness,
therefore 293 patients (78.3%) were included in the final analyses. Seventy-three respondents
(24.9%) were pre-transplantation, and 220 were post-transplantation – either DBD (56.3%), DCD
(8.5%), patients with ischaemic cholangiopathy (2.4%), or re-transplant (7.9%) recipients.
The level of missingness was <5% for all questions used in the multiple imputation model with the
exception of questions 2a (20%), 2b (18%), 2c (16%) and 7 (10%). Three questions (9a, 9b, 10)
related to sexual function were excluded due to levels of missingness >20%.
The average overall score for each patient group was used to attribute QALY values to each (Table 2). The post-transplant group reported a significantly higher overall HR-QoL than the pre-transplant
groups (mean score difference 13.7, 95% CI 9.7 - 17.6, p<0.001). There was no significant difference
in the QALYs associated with different MELD scores in the pre-transplant groups. However, the DBD-
liver recipients reported a significantly higher overall HR-QoL compared to DCD-liver recipients (mean
score difference 5.9, 95% CI 0.02 - 11.8, p=0.049).
3.3. Model Findings:The model provided a quantification of the predicated outcome for patients over time for either
decision, and across different initial MELD scores (Figure 3, Table 3). Declining an available DCD
transplant was associated with substantially higher mortality at the model end-point (60 months) in all
cases, which increased with higher MELD categories. In contrast, the decision to offer DCD
transplantation was associated with the highest 5 year survival without complications (81.6%).

However, those patients had a considerably higher predicted probability of ischaemic cholangiopathy
(5.3%).
The base analyses (Table 4) indicate that DCD transplantation would be associated with the highest
QALYs gained at the model end-point. Furthermore, that the QALYs gained though waiting for DBD
transplantation would reduce as the MELD score increased. Subsequent probabilistic sensitivity
analyses indicated that proceeding with DCD transplantation remained the optimal choice (3.77
QALYs, 95% CI = 3.44-4.10) for a patient with a MELD score ≥15. However, for patients with MELD
scores <15, there is no significant difference in the QALYs gained, and so the optimal decision (in
terms of quality of life) for these patients remains unclear.
One-way sensitivity analyses were also conducted to assess the validity of this conclusion across the
minimum (0.000) to maximum (0.083) QALYs per month range (Figure 4). Proceeding with
transplantation remained the optimal decision for patients in all MELD categories when the QALYs in
pre-transplantation patients and post-transplant patients with ischaemic cholangiopathy were
investigated. However, when the QALYs gained after DCD transplantation were varied, there were
thresholds observed at 0.057, 0.053, or 0.048 for patients with respective MELD scores of <15, 15–
20, or >20. Below these thresholds, the optimal choice would be to decline and wait for a DBD
allograft or further clinical deterioration.
4. Discussion:The demand for liver transplantation continues to rise, as does utilisation of DCD allografts 3, and in
the UK the National Health Service (NHS) is implementing strategies to further expand the proportion
of DCD organs available 27. Therefore, it is increasingly important to improve the understanding of
which patients would gain most benefit from DCD allografts. This study aimed to determine the
optimal decision for a patient when a DCD liver transplant becomes available – for the surgeon to
either accept or refuse this allograft – based on the current health of their patient. As such, this
represents the first assessment of the comparative effectiveness of liver allograft acceptance
strategies for the UK. In particular, this model adopts a patient-centred perspective, quantified as
QALYs gained after 5 years, under the rationale that “the ultimate measure by which to judge the
quality of a medical effort is whether it helps patients (and their families) as they see it” 28. This is an
important difference from models which assume a health-system perspective 29, 30, quantifying the
decision in terms of the cost–effectiveness to enable policy makers to allocate limited resources most
appropriately 31. It must be noted that cost–effectiveness was not assessed within the current model,
and that as DCD allografts are associated with increased morbidity, re-transplantation rates, and
mortality 9-12, these entail substantially higher post-transplantation costs 32. Although the cost-
effectiveness of DCD liver transplantation has not been formally evaluated in the UK 33, waiting list
strategies involving these organs have been identified as cost-effective in comparison to DBD-only
strategies 29. This can be attributed to reductions in the burden of disease (and associated costs) in
end-stage liver disease patients.

This model predicts that patients who receive the DCD transplant have significantly higher 5 year
post-transplant survivals, ischaemic cholangiopathy rates, and QALYs gained compared to patients
with MELD scores >15 where the offered allograft is declined. Therefore, the optimal decision for
these patients is for the DCD liver transplant to be accepted when it becomes available. It is important
to recognise that this analysis is only valid for the DCD donor-recipient pairings currently seen in
actual practice. It says nothing of the outcomes if higher risk donor-recipient pairings are undertaken.
Moreover, this choice remains unclear in patients with MELD scores <15 given the absence of a
significant QALY-difference. This contrasts with a similar Markov model 30 that predicted only patients
with MELD scores >20 would gain significant benefit from accepting DCD allografts. One-way
sensitivity analysis indicated that these conclusions persist over a range of QALY values for pre-
transplant patients and post-transplant patients with ischemiac cholangiopathy at different MELD
score categories (Figure 4), and there is evidence to suggest that MELD score correlates poorly with
HR-QoL measures 34. In addition, the thresholds observed during sensitivity analysis of the QALYs
after DCD transplantation (Figure 4) lay out-with the 95% CI (Table 2), and so this further increases
confidence in the robustness of the model. Furthermore, the model demonstrated that the decision to
accept a DCD organ was associated with the highest 5 year survival without complications at the
model end-point (Table 3, Figure 3).
One of the foremost strengths of this study is the use of the UK Transplant Registry to allow
calculation and adjustment of clinical outcomes. This large patient database provided high quality
longitudinal clinical data, which allows the model results to be generalised to all UK units. Although
there were significant differences observed in the baseline characteristics of the DBD and DCD
transplantation groups, this is undoubtedly an artefact of the highly selective criteria for DCD liver
transplantation allografts and recipients 35. Furthermore, as the large sample size provides substantial
statistical power, significant differences should be interpreted in the context of clinical importance.
These differences were accounted for in the multivariate regression analyses to produce
independent predictions of patient survival. However, the database does possess several limitations.
Firstly, the data needed for the waiting list and ischaemic cholangiopathy patient clinical outcomes
were not included, and so these were derived from published literature 36, 37. These studies were within
US populations, and so may not accurately reflect the clinical situation in the UK. However,
In 2014, the majority (56%) of liver transplant recipients in the US had MELD scores of less than 30 6.
These patients composed just 34% of liver transplant recipients in the 2001-2011 NHSBT database
(at the time of transplant, based on the biochemical results). On balance, it was concluded that the
practical benefits of further nuance within the model outweighed the theoretical concerns of
generalisability. Secondly, the survival curves (Figure 2) indicate the majority of liver transplant
patients survive beyond the 11 year period the database covers. However, as all surviving patients
were censored on the 31st December 2011, patients varied in post-transplantation follow-up period. As
a result of limited long-term data, the model results were based on the first 5 years post-
transplantation only. Therefore, it is important to recognise that the conclusions of the model could
alter if individual patient follow-up was extended.

A further advantage of this study is the incorporation of population-specific quality of life data into the
model, in contrast to literature-derived values 29, 30, or complete omission 38, 39, seen in other Markov
models of liver transplantation. However, our model assumes that the responses from Scottish Liver
Transplant Unit patients are generalisable to the UK cohort as a whole. This is a reasonable
assumption given the demographic make-up of the UK. Furthermore, it is important to recognise the
impact patient experience and non-health related factors can have on patient-reported outcome
measures 40 and these may differ between the UK units. In addition, an excellent questionnaire
response rate (81.8%) was obtained, which compares favourably to other HR-QoL studies in these
populations 14, 41, 42, therefore volunteer and selection biases were minimised. Nevertheless, due to the
limited data collection period it must be recognised that clinic attendees are more likely to have higher
MELD scores, shorter post-operative periods, or higher complication rates and/or severities.
Therefore, these factors could have led to an underestimation of the HR-QoL observed in
respondents. Alternately, patients with the worst post-transplantation health may have died or been
re-transplanted, thus these results have inherent positive bias. This would be of greatest concern in
the ischaemic cholangiopathy group, particularly given the low sample size, and so may explain the
high HR-QoL observed. Nevertheless, when the QALYs for ischaemic cholangiopathy patients were
explored, this did not alter the conclusions of the model. We are planning a condition–specific HR-
QoL questionnaire extended into a UK-wide longitudinal study of routine clinical practice within the
liver transplant units which will confirm or refute the assumptions implicit in this analysis. .
There are also several limitations, and necessary assumptions implicit within the Markov model that
should be considered. Firstly, the model only compares outcomes after DCD and DBD
transplantation, and so the conclusions must be interpreted in view of alternative forms of liver
transplantation, including split or reduced livers, live liver donation, and multi-organ transplantation. In
addition, the clinical and HR-QoL outcomes presented in this paper are generalisations. Therefore, it
is essential that there is consideration of the specific organ and patient-related factors (including
aetiology of liver disease), and the anticipated local waiting time for DBD transplantation in the
decision to accept a DCD organ. Furthermore, the MELD score utilised here does not include
exception points utilised in some organ transplant jurisdictions for patients with HCC. However, as
these patients are expected to have a higher mortality risk on the waiting list compared to their
biological MELD 43, the model results could represent a conservative estimate of the benefits of DCD
transplantation. Finally, this model assumed that all re-transplantations were performed with a DBD
organ, and so the conclusions regarding the use of DCD can only be applied to the patients’ first
transplantation.
Future work will focus on improving the model reliability including: obtaining UK-specific clinical data
on waiting list and ischaemic cholangiopathy epidemiology; expansion of a condition–specific HR-QoL
questionnaire into a UK-wide longitudinal study or routine clinical practice; direct comparison of the
outcomes from different primary liver diseases, including the presence of HCC; and extension of the
UK Transplant Registry database to allow determination of longer-term patient outcomes.
Furthermore, with appropriate input from medical informatics specialists, this model could be

developed into an application that medical staff could utilise to help inform the optimal decision for
individual patients at the point of being offered DCD liver transplantation. As the clinical outcomes are
derived from routinely available data, these could be regularly updated to reflect changes in clinical
practice.
5. Conclusion:
In conclusion, this Markov model predicted that DCD liver transplantation would provide significantly
higher QALYs gained by 5 years for average patients on the waiting list with MELD scores >15.
Therefore, from a quality of life perspective, an offered DCD liver transplantation should be accepted
in this patient cohort. The optimal decision for average patients with MELD scores <15 remains
unclear, however the model also demonstrated a survival benefit in patients when a DCD organ was
accepted. Nonetheless, it is essential that there is consideration of the specific organ and patient-
related risk factors (including aetiology of liver disease, and prior liver transplantation), and the
anticipated local waiting time for DBD transplantation in the decision to accept a DCD organ.

References:
1. Starzl T, Marchioro TL, Vonkaulla KN, Hermann G, Brittain RS, Waddell WR.
Homotransplantation of the liver in humans. Surg Gynecol Obstet. 1963; 117: 659-76.
2. National Health Service. Liver transplant, 2015. Available from:
http://www.nhs.uk/conditions/Liver-transplant. [Accessed: 30/05/15].
3. National Health Service Blood and Transplant. Organ donation and transplantation activity
report 2013/14, 2014. Available from:
http://www.organdonation.nhs.uk/statistics/transplant_activity_report/. [Accessed: 16/05/15].
4. Fisher R, Cotterell AH, Maluf DG, Stravitz RT, Ashworth A, Nakatsuka M, Sterling RK, Luketic
VA, Behnke MK, Posner MP. Adult living donor versus deceased donor liver transplantation: a 10-
year prospective single center experience. Ann Hepatol. 2009; 8 (4): 298-307.
5. Clavien P, Petrowsky H, DeOliveira ML, Graf R. Strategies for safer liver surgery and partial
liver transplantation. N Engl J Med. 2007; 356 (15): 1545-59.
6. Busuttil R, Tanaka K. The utility of marginal donors in liver transplantation. Liver Transpl.
2003; 9 (7): 651-63.
7. Charman S, Copley L, Tovikkai C, van der Meulen J, Counter C, Rushton S, Collett D. UK
Liver Transplant Audit in patients who received a liver transplant between 1st March 1994 and 31st
March 2012. London: The Royal College of Surgeons of England, 2012.
8. Zhai Y, Petrowsky H, Hong JC, Busuttil RW, Kupiec-Weglinski JW. Ischaemia–reperfusion
injury in liver transplantation—from bench to bedside. Nat Rev Gastroenterol Hepatol. 2013; 10 (2):
79-89.
9. Foley D, Fernandez LA, Leverson G, Chin LT, Krieger N, Cooper JT, Shames BD, Becker YT,
Odorico JS, Knechtle SJ, Sollinger HW, Kalayoglu M, D'Alessandro AM. Donation after cardiac death:
the University of Wisconsin experience with liver transplantation. Ann Surg. 2005; 242 (5): 724-31.
10. Jay C, Lyuksemburg V, Ladner DP, Wang E, Caicedo JC, Holl JL, Abecassis MM, Skaro AI.
Ischemic cholangiopathy after controlled donation after cardiac death liver transplantation: a meta-
analysis. Ann Surg. 2011; 253 (2): 259-64.
11. Callaghan C, Charman SC, Muiesan P, Powell JJ, Gimson AE, van der Meulen JH.
Outcomes of transplantation of livers from donation after circulatory death donors in the UK: a cohort
study. BMJ Open [Online]. 2013; 3 (9): e003287. Available from:
http://bmjopen.bmj.com/content/3/9/e003287.full?rss=1. [Accessed: 16/09/15].
12. de Vera M, Lopez-Solis R, Dvorchik I, Campos S, Morris W, Demetris AJ, Fontes P, Marsh
JW. Liver transplantation using donation after cardiac death donors: long-term follow-up from a single
center. Am J Transplant. 2009; 9 (4): 773-81.
13. Dubbeld J, van Hoek B, Ringers J. Use of a liver from donor after cardiac death: is it
appropriate for the sick or the stable? Curr Opin Organ Transplant. 2011; 16 (2): 239-42.
14. Parikh N, Skaro AI, Ladner DP, Lyuksemburg V, Cahan JG, Daud A, Butt Z. Clinical
outcomes and quality of life in recipients of livers donated after cardiac death. Gastroenterol Res
Pract [Online]. 2015; 2015: 680316. [Accessed: 16/09/15].

15. O'Neill S, Roebuck A, Khoo E, Wigmore SJ, Harrison EM. A meta-analysis and meta-
regression of outcomes including biliary complications in donation after cardiac death liver
transplantation. Transpl Int 2014; 27 (11): 1159-74.
16. Mourad M, Algarni A, Liossis C, Bramhall SR. Aetiology and risk factors of ischaemic
cholangiopathy after liver transplantation. . World J Gastroenterol. 2014; 20 (20): 6159-69.
17. Mathur A, Heimbach J, Steffick DE, Sonnenday CJ, Goodrich NP, Merion RM. Donation after
cardiac death liver transplantation: predictors of outcome. Am J Transplant. 2010; 10 (11): 2512-9.
18. Taner C, Bulatao IG, Willingham DL, Perry DK, Sibulesky L, Pungpapong S, Aranda-Michel J,
Keaveny AP, Kramer DJ, Nguyen JH. Events in procurement as risk factors for ischaemic
cholangiopathy in liver transplantation using donation after cardiac death donors. Liver Transpl. 2012;
18 (1): 100-11.
19. Dubbeld J, Hoekstra H, Farid W, Ringers J, Porte RJ, Metselaar HJ, Baranski AG, Kazemier
G, van den Berg AP, van Hoek B. Similar liver transplantation survival with selected cardiac death
donors and brain death donors. Br J Surg. 2010; 97 (5): 744-53.
20. Merion R. When Is a Patient Too Well and When Is a Patient Too Sick For a Liver
Transplant? Liver Transpl. 2004; 10 (10): S69-73.
21. Alagoz O, Hsu H, Schaefer AJ, Roberts MS. Markov decision processes: a tool for sequential
decision making under uncertainty. Med Decis Making 2010; 30 (4): 474-83.
22. Kootstra G, Daemen JH, Oomen AP. Categories of non-heart-beating donors. Transplant
Proc. 1995; 27 (5): 2893-4.
23. Guichelaar M, Benson JT, Malinchoc M, Krom RA, Wiesner RH, Charlton MR. Risk Factors
for and Clinical Course of Non-Anastomotic Biliary Strictures After Liver Transplantation. Am J
Transplant. 2003; 3 (7): 885-90.
24. Kanwal F, Spiegel BM, Hays RD, Durazo F, Han SB, Saab S, Bolus R, Kim SJ, Gralnek IM.
Prospective validation of the short form liver disease quality of life instrument. Aliment Pharmacol
Ther. 2008; 28 (9): 1088-101.
25. van Buuren S, Groothuis-Oudshoon K. MICE: Multivariate Imputation by Chained Equations
in R. J Stat Softw. 2011; 45 (3): 1-67.
26. Rubin DB. Multiple Imputation for Nonresponse in Surveys. 1st ed. New York: John Wiley &
Sons; 1987. 75–240 p.
27. National Health Service Blood and Transplant. Taking Organ Transplantation to 2020: A
detailed strategy, 2013. Available from:
http://www.nhsbt.nhs.uk/to2020/resources/nhsbt_organ_donor_strategy_long.pdf. [Accessed:
16/05/15].
28. Berwick D. Medical associations: guilds or leaders? BMJ. 1997; 314 (7094): 1564-5.
29. Dageforde L, Feurer ID, Pinson CW, Moore DE. Is liver transplantation using organs donated
after cardiac death cost-effective or does it decrease waitlist death by increasing recipient death?
HPB. 2013; 15 (3): 182-9.
30. Jay C, Skaro AI, Ladner DP, Wang E, Lyuksemburg V, Chang Y, Xu H, Talakokkla S, Parikh
N, Holl JL, Hazen GB, Abecassis MM. Comparative effectiveness of donation after cardiac death

versus donation after brain death liver transplantation: Recognizing who can benefit. Liver Transpl.
2012; 18 (6): 630-40.
31. National Institute for Health and Care Excellence. NICE local government briefings: How
NICE measures value for money in relation to public health interventions (NICE advice LGB10B),
2013. Available from: http://publications.nice.org.uk/lgb10b. [Accessed: 16/05/15].
32. Jay C, Lyuksemburg V, Kang R, Preczewski L, Stroupe K, Holl JL, Abecassis MM, Skaro AI.
The increased costs of donation after cardiac death liver transplantation: caveat emptor. Ann Surg.
2010; 251 (4): 743-8.
33. National Institute for Health and Care Excellence. Organ donation for transplantation: Costing
report, 2011. Available from: http://guidance.nice.org.uk/CG135. [Accessed: 16/05/15].
34. Saab S, Ibrahim AB, Shpaner A, Younossi ZM, Lee C, Durazo F, Han S, Esrason K, Wu V,
Hiatt J, Farmer DG, Ghobrial RM, Holt C, Yersiz H, Goldstein LI, Tong MJ, Busuttil RW. MELD fails to
measure quality of life in liver transplant candidates. Liver Transpl. 2005; 11 (2): 218-23.
35. British Transplantation Society. United Kingdom Guidelines: Transplantation from donors
after deceased circulatory death., 2013. Available from: https://www.bts.org.uk. [Accessed:
36. Scientific Registry of Transplant Recipients. 2011 Annual Report of the US Organ
Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients:
Transplant Data 2001–2010. Rockville, MD: Health Resources and Services Administration,
Healthcare Systems Bureau, Division of Transplantation, 2011.
37. Chan E, Olson LC, Kisthard JA, Perkins JD, Bakthavatsalam R, Halldorson JB, Reyes JD,
Larson AM, Levy AE. Ischemic cholangiopathy following liver transplantation from donation after
cardiac death donors. Liver Transpl 2008; 14 (5): 604-10.
38. Alagoz O, Maillart LM, Schaefer AJ, Roberts MS. The Optimal Timing of Living-Donor Liver
Transplantation. Manag Sci. 2004; 50 (10): 1420–30.
39. Alagoz O, Maillart LM, Schaefer AJ, Roberts MS. Determining the Acceptance of Cadaveric
Livers Using an Implicit Model of the Waiting List. Operations Research. 2007; 55 (1): 24–36.
40. Devlin N, Appleby J. Getting the most out of PROMs. Putting health outcomes at the heart of
NHS decision-making. London: The Kings Fund, 2010.
41. Yang L, Shan LL, Saxena A, Morris DL. Liver transplantation: a systematic review of long-
term quality of life. Liver Int. 2014; 34 (9): 1298-313.
42. Aberg F, Rissanen AM, Sintonen H, Roine RP, Höckerstedt K, Isoniemi H. Health-related
quality of life and employment status of liver transplant patients. Liver Transpl. 2009; 15 (1): 64-72.
43. Massie A, Caffo B, Gentry S, Hall E, Axelrod D, Lentine K, et al. MELD Exceptions and Rates
of Waiting List Outcomes. Am J Transplant. 2011; 11 (11): 2362-71.

Table 1 – Recipient and donor characteristics, and operative outcomes for DBD or DCD liver
allograft recipients from 2001-11 at all UK liver transplant units. Data are n (%) unless otherwise
stated.
Type of liver allograft receivedDBD Group
n =4340DCD Group
n = 488 p-value
Recipient Characteristics:Age (years) Mean (sd) 51.6 (11.1) 53.4 (10.0) <0.001Sex Male 2811 (64.8%) 334 (68.4%) 0.85
Female 1529 (35.2%) 154 (31.6%) Ethnicity White 3757 (86.6%) 383 (78.6%) <0.001
Non-White 582 (13.4%) 104 (21.4%)Primary Liver Disease Alcoholic 1019 (23.5%) 125 (25.6%) <0.001
Cholestatic 1004 (23.1%) 78 (16.0%)HCV 727 (16.8%) 107 (21.9%)HCC 235 (5.4%) 44 (9.0%)Other 1355 (31.2%) 134 (27.5%)
MELD Score * Mean (sd) 32.1 (6.4) 31.4 (5.8) 0.03Donor Characteristics:Age (years) Mean (sd) 47.7 (14.7) 43.4 (15.9) <0.001BMI (kg/m2) Mean (sd) 26 (4.7) 25.3 (4.3) <0.001Ethnicity White 4125 (96.5%) 456 (95.4%) 0.20
Non-White 148 (3.5%) 22 (4.6%)Cause of Death ICH 2852 (66.0%) 213 (43.6%) <0.001
Hypoxic brain injury 329 (7.6%) 84 (17.2%)RTA (any) 188 (4.4%) 31 (6.4%)Other Accident 152 (3.5%) 19 (3.9%)Other Causes 800 (18.5%) 141 (28.9%)
Operative Outcomes:CIT (mins) Mean (sd) 593 (166) 427 (120) <0.001Reperfusion time (mins) Mean (sd) 49 (34) 44 (24) <0.001
Abbreviations: sd = standard deviation; DCD = Donation after circulatory death; DBD =
Donation after brain death; HCV = Hepatitis C virus; HCC = Hepatocellular Carcinoma; MELD =
Model for End-Stage Liver Disease; ICH = Intracerebral haemorrhage; CIT = Cold ischaemic
time. * At time of transplant.

Table 2: The mean QALYs attributable to pre- and post-transplant groups, derived from Scottish Liver
Transplant Unit patients.
n
Mean quality adjusted life years (QALYs) gained
Per year (95% CI) Per monthly cycle (95% CI)
Pre-transplant patients 73 0.659 (0.639 – 0.679) 0.055 (0.053 – 0.057)MELD score < 15 35 0.638 (0.610 – 0.666) 0.053 (0.051 – 0.055)
MELD score 15 – 20 15 0.667 (0.624 – 0.710) 0.056 (0.052 – 0.059)
MELD score > 20 23 0.690 (0.649 – 0.730) 0.057 (0.054 – 0.061)
Post-transplant patients 220 0.795 (0.786 – 0.805) 0.066 (0.065 – 0.067)DBD-liver recipients 165 0.805 (0.794 – 0.815) 0.067 (0.066 – 0.068)
DCD-liver recipients 25 0.744 (0.710 – 0.779) 0.062 (0.059 – 0.065)
IC patients 7 0.844 (0.780 – 0.909) 0.070 (0.065 – 0.076)
Re-transplant recipients 23 0.767 (0.737 – 0.796) 0.064 (0.061 – 0.066)
Abbreviations: MELD = Model of End-stage liver disease; DBD = Donation after brain death; DCD =
Donation after circulatory death; IC = Ischaemic cholangiopathy; QALYs = quality-adjusted life years.

Table 3 – The predicated outcome for patients at the model end-point (60 months), by the decision and MELD
score at the time.
Predicated outcome the model end-point
Pre-transplant
Post-transplant
DeathDecision Transplanted IC patient Re-transplanted
Accept DCD liver allograft - 81.6% 5.3% 1.1% 12.3%
Decline MELD < 15 0.0% 72.3% 1.5% 2.2% 24.0%
MELD 15-20 0.0% 67.5% 1.4% 2.1% 29.0%
MELD > 20 0.0% 60.9% 1.3% 2.0% 35.8%
Abbreviations: MELD = Model of End-stage liver disease; DBD = Donation after brain death; DCD =
Donation after circulatory death; IC = Ischaemic cholangiopathy.

Table 4 – Base analyses and probabilistic sensitivity analyses of the modelled QALYs gained by the model end-point (60 months).
Accept the offered Decline the offered DCD allograft
DCD allograft MELD < 15 MELD 15 - 20 MELD > 20
QALYs gainedby 60 months
Base-case analysis 3.56 3.26 3.08 2.79
Probabilistic sensitivity
analysis (95% CI)
3.77(3.44 – 4.10)
3.55(3.47 – 3.63)
3.36(3.28 – 3.43)
3.07(3.00 – 3.14)
Abbreviations: MELD = Model of End-stage liver disease; DCD = Donation after circulatory death; IC = Ischaemic cholangiopathy;
QALYs = quality-adjusted life years.

Figure 1: Structure of the Markov model of the clinical course of patients on the UK liver transplant waiting list when a DCD liver transplant becomes available.
Abbreviations: DBD = donated after brain death; DCD = donated after circulatory death; T = Transplanted (no ischaemic cholangiopathy); IC = Transplanted with ischaemic cholangiopathy; RT = Re-transplantated; MELD = Model of End-stage liver disease.

Figure 2 – Questionnaire completion by patients attending the Scottish Liver Transplant Unit (SLTU) from 16 th July
2015 to 3rd September 2015.
Scheduled appointments
n = 548
Ineligible patients n = 174
Repeat attendances n = 119
Eligible patients Did not attend n = 52
n = 374 Live liver donor n = 3
Excluded patients n = 86
Refused participation n = 46
Complete questionnaires Not encountered n = 22
n = 293 Incomplete questionnaire n = 13
Pre-transplant Post-transplant
n = 73 n = 220

Figure 3 – The predicated outcome for patients over time, by
the decision (accept or decline a DCD organ) and the MELD
score of the patient at the time.
a) Percentage of patients who remain alive pre-transplant.
0 5 10 15 20 25 30 35 40 45 50 55 600%
10%20%30%40%50%60%70%80%90%
100%Decline DCD (MELD <15)Decline DCD (MELD 15-20)Decline DCD (MELD>20)Accept DCD organ
Time in the model (months)
Perc
enta
ge o
f pat
ient
s w
hore
mai
n pr
e-tr
ansp
lant
b) Percentage of patients who are alive post-transplant.
0 5 10 15 20 25 30 35 40 45 50 55 600%
10%20%30%40%50%60%70%80%90%
100%
Decline DCD (MELD <15)Decline DCD (MELD 15-20)Decline DCD (MELD>20)Accept DCD organ
Time in the model (months)
Perc
enta
ge o
f pat
ient
sar
e po
st-tr
ansp
lant
c) Percentage of patients who have died (overall).
0 5 10 15 20 25 30 35 40 45 50 55 600%
10%20%30%40%50%60%70%80%90%
100%Decline DCD (MELD < 15)Decline DCD (MELD 15 - 20)Decline DCD (MELD > 20)Accept DCD organ
Time in the model (months)
Perc
enta
ge o
f pat
ient
s w
ho h
ave
died
(ove
rall)

Figure 4 – One-way sensitivity analysis of quality adjusted life
year (QALY) parameters.
a) QALYs per month on the waiting list (by MELD score).
0.000 0.021 0.042 0.063 0.0830.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
Accept DCD organDecline DCD (MELD <15)Decline DCD (MELD 15-20)Decline DCD (MELD >20)
QALYs per month on the waiting list
QAL
Ys g
aine
d by
60
mon
ths
b) QALYs per month with after DCD transplantation
0 0.021 0.042 0.063 0.0830.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00Accept DCD organDecline DCD (MELD <15)Decline DCD (MELD 15-20)Decline DCD (MELD >20)
QALYs per month with DCD transplant
QAL
Ys g
aine
d by
60
mon
ths

Figure 4 – One-way sensitivity analysis of quality adjusted life
year (QALY) parameters.
c) QALYs per month with IC after transplantation
0 0.021 0.042 0.063 0.083330.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
Accept DCD organDecline DCD (MELD <15)Decline DCD (MELD 15-20)Decline DCD (MELD >20)
QALYs per month IC post-transplant
QAL
Ys g
aine
d by
60
mon
ths

Supplement A – Supplementary Tables Supplementary Table 1a - Transition probabilities (95% CI) for patients on the liver transplant waiting list (after a DCD
liver is declined), derived from the 2001-2011 Scientific Registry of Transplant Recipients (SRTR) report 36.
End State
MELD < 15 MELD 15-20 MELD >20 DBD transplant Death
Start State MELD < 15 0.950
(0.944-0.954)
0.032
(0. 028-0.036)
0.003
(0.002-0.005)
0.006
(0.004-0.008)
0.010
(0.008-0.012)
MELD 15-20 0.085
(0.075-0.096)
0.806
(0.790-0.820)
0.064
(0.055-0.073)
0.024
(0.019-0.031)
0.022
(0.017-0.028)
MELD >20 0.011
(0.005-0.020)
0.144
(0.121-0.169)
0.605
(0.571-0.638)
0.155
(0.131-0.180)
0.087
(0.069-0.107)
Abbreviations: DBD = Donation after brain death; MELD = Model of End-Stage Liver Disease.

Supplementary Table 1b-Transition probabilities (95% CI) for patients who receive DBD liver transplantation.
Data are from the UK Transplant Registry unless otherwise indicated.
End State
TH TIC 15, 23 TR Death
Start State Cycle 1 TX 0.964
(0.955-0.971)
0.001
(0.001-0.002)
0.003
(0.002-0.005)
0.032 *
(0.027-0.038)
Cycle 2-60 TH 0.997
(0.996-0.997)
0.000
(0.000-0.000)
0.000
(0.000-0.000)
0.003 *
(0.002-0.003)
TIC 23 0.001
(0.000-0.002)
0.990
(0.985-0.994)
0.005
(0.003-0.007)
0.004 *
(0.002-0.006)
TR 0.996
(0.995-0.997)- -
0.004 *
(0.003-0.005)
Dead - - - 1
Abbreviations: TX = Transplantation; TH / TIC = survival without / with ischaemic cholangiopathy; TR = survival
after re-transplant. * Multivariate logistic regression was conducted with baseline characteristics (Table 2) using
backwards stepwise elimination.

Supplementary Table 1c-Transition probabilities (95% CI) for patients who receive DCD liver transplantation.
Data are from the UK Transplant Registry unless otherwise indicated.
End State
TH TIC 15, 23 TR Death
Start State Cycle 1 TX 0.932
(0.902-0.955)
0.006
(0.005-0.007)
0.000
(0.000-0.008)
0.062 *
(0.041-0.083)
Cycle 2-60 TH 0.997
(0.996-0.997)
0.001
(0.001-0.002)
0.000
(0.000-0.000)
0.002 *
(0.002-0.003)
TIC 23 0.001
(0.000-0.002)
0.990
(0.985-0.994)
0.005
(0.003-0.007)
0.004
(0.002-0.006)
TR 0.996
(0.995-0.997)- -
0.004 *
(0.003-0.005)
Dead - - - 1
Abbreviations: TX = Transplantation; TH / TIC = survival without / with ischaemic cholangiopathy; TR = survival
after re-transplant. * Multivariate logistic regression was conducted with baseline characteristics (Table 2) using
backwards stepwise elimination.