Embed Size (px)
Citation preview
Organization: The Johns Hopkins Hospital
Solution title: Hopkins NINJA: Nephrotoxic Injury Negated by Just-in-Time Action
Program/Project Description and Goals:
Most hospitalized children receive nephrotoxic medications (NTMx), and NTMx exposure is one of the most common causes of acute kidney injury (AKI) in non-critically ill, hospitalized children. AKI results in significant morbidity, including prolonged hospitalization and risk for developing chronic kidney disease. AKI is under-recognized in children due to a lack of monitoring of kidney function (serum creatinine) and a failure to recognize small, but clinically significant, changes in serum creatinine.
In 2011-2012, more than 160 children hospitalized in the Johns Hopkins Bloomberg Children’s Center were recognized as having AKI severe enough to prompt a pediatric nephrology consult and more than 700 acute dialysis treatments were required for children with AKI in 2012 alone. These rates are higher than many other prominent Children’s hospitals. AKI rates and length of hospital stay among those exposed to NTMx’s was examined over a three month period in 2014. The AKI rate among NTMx-exposed hospitalized children was 14.5%. The average length of stay among exposed children with AKI was significantly longer (54 days with AKI vs 30 days without AKI).
A team from Cincinnati Children’s Hospital first reported on the ability to mitigate the risk of NTMx exposure to children (Pediatrics 2013; 132; e756). A multicenter collaborative of children’s hospitals called NINJA: Nephrotoxic Injury Negated by Just-in-Time Action was established to work together to help prevent AKI in hospitalized children. The Johns Hopkins Children’s Center joined the collaborative in 2015.
Working within this collaborative Hopkins NINJA evaluates non-critically ill children hospitalized in the Bloomberg Children’s Center and exposed to NTMx and aims to: 1) decrease exposure to NTMx when clinically appropriate, 2) improve monitoring of kidney function, 3) decrease incidence of AKI, and 4) decrease intensity of (days with) AKI.
Process:
Reducing AKI requires identification of at-risk patients At Hopkins, NINJA is executed by a multidisciplinary team including a pediatric nephrologist, nurse, pharmacist, research assistant, and technical experts from JHHS Clinical and Quality Analytics within the Armstrong Institute of Patient Safety and Quality. The team built NINJA’s complex NTMx exposure and AKI detection algorithms into a proprietary QlikView dashboard. Using demographic, laboratory, and medication administration data obtained from Epic Clarity, the dashboard updates daily.
Solution:
Since September 2016, the Hopkins NINJA team has used the data obtained from the dashboard to provide daily outreach and education to primary clinical teams. During these face-to-face interactions the NINJA team alerts providers to NTMx exposures and AKI risk among their patient and recommends appropriate monitoring of kidney function with daily serum creatinine
while the exposure persists or, if a patient is injured, until the injury resolves. The dashboard also enables routine assessment of metrics and permits data queries to enhance the surveillance system. Using the dashboard, the team reviews two primary metrics, NTMx exposure and AKI.
1) NTMx Exposure: A child is flagged as “exposed” if the child received: ≥ 3 consecutive days of an aminoglycoside or ≥ 3 NTMx in a day. NTMx with longer lasting effects (intravenous radiographic contrast, cidofovir, amphotericin) count as an exposure for 7 days after the administration. The NINJA NTMx list was determined by a literature review and consensus among centers in the national NINJA collaborative.
2) AKI: AKI is defined using a standard international definition based on serum creatinine levels (2). A child is identified as “injured” if a creatinine value: A) is at least 150% of the patient’s minimum value from the past 6 months, provided that the current value is >0.5 mg/dL, or B) is 0.3 mg/dL higher than any prior value in the past 48 hours.
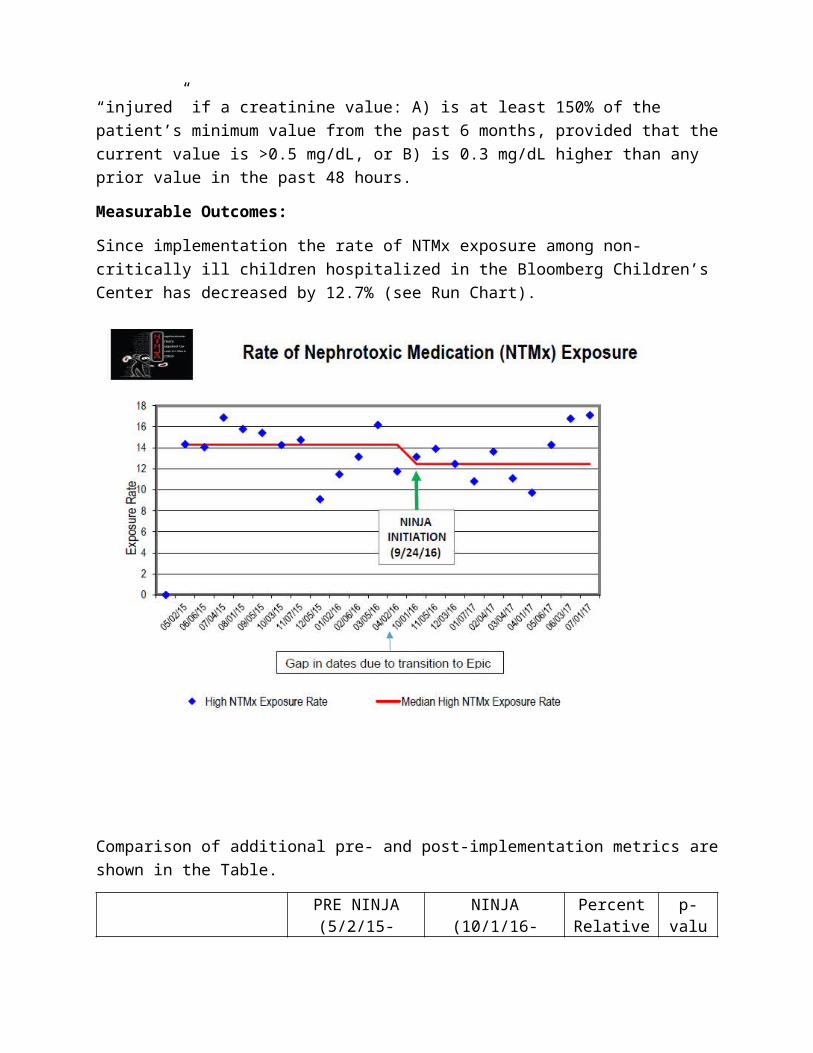
Measurable Outcomes:
Since implementation the rate of NTMx exposure among non-critically ill children hospitalized in the Bloomberg Children’s Center has decreased by 12.7% (see Run Chart).
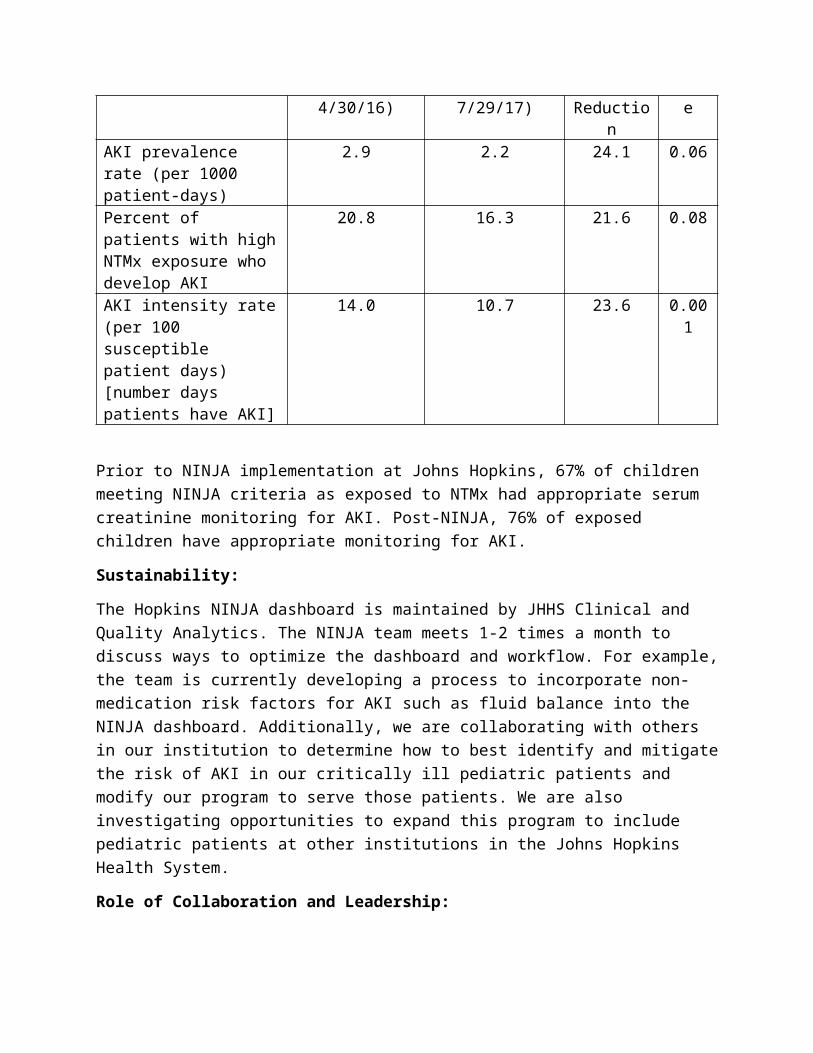
Comparison of additional pre- and post-implementation metrics are shown in the Table.
PRE NINJA (5/2/15-4/30/16)
NINJA (10/1/16-7/29/17)
Percent Relative
Reduction
p-value
AKI prevalence rate (per 1000 patient-days)
2.9 2.2 24.1 0.06
Percent of patients with high NTMx exposure who develop AKI
20.8 16.3 21.6 0.08
AKI intensity rate (per 100 susceptible patient days) [number days patients have AKI]
14.0 10.7 23.6 0.001
Prior to NINJA implementation at Johns Hopkins, 67% of children meeting NINJA criteria as exposed to NTMx had appropriate serum creatinine monitoring for AKI. Post-NINJA, 76% of exposed children have appropriate monitoring for AKI.
Sustainability:
The Hopkins NINJA dashboard is maintained by JHHS Clinical and Quality Analytics. The NINJA team meets 1-2 times a month to discuss ways to optimize the dashboard and workflow. For example, the team is currently developing a process to incorporate non-medication risk factors for AKI such as fluid balance into the NINJA dashboard. Additionally, we are collaborating with others in our institution to determine how to best identify and mitigate the risk of AKI in our critically ill pediatric patients and modify our program to serve those patients. We are also investigating opportunities to expand this program to include pediatric patients at other institutions in the Johns Hopkins Health System.
Role of Collaboration and Leadership:
Collaboration has been essential to this program from the beginning. As Hopkins NINJA is part of a multicenter collaborative, the team works together with experts from other pediatric institutions to address the problem of NTMx-related AKI in children. The collaborative holds monthly calls to share best practices and ideas for improving and expanding the NINJA program.
Within Hopkins, there has been a great deal of multidisciplinary collaboration. Within the NINJA team itself, a physician, pharmacist, and nurse work together to provide the clinical services for NINJA. Each member brings expertise to help the provider teams with different aspects of clinical care such as diagnosing and treating AKI, monitoring medication levels and making medication dose adjustments in the setting of AKI, selecting alternative medications to help avoid nephrotoxic medications when clinically appropriate, and assisting bedside nurses with implementing the recommended monitoring plans. Additionally, the collaboration of technical experts from JHHS Clinical and Quality Analytics within the Armstrong Institute of Patient Safety and Quality has been vital to the development of the dashboard, which allows at-
risk patients to be identified accurately, and clinical services to be provided efficiently. The ability to query this data retrospectively is also key as we continue to work within the collaborative to optimize the exposure algorithm. Many of the other collaborating institutions’ process for implementing the NINJA program do not allow for such robust retrospective data analysis.
In recognition of the scope of the problem of hospital-acquired AKI and the potential to leverage clinical resources and the electronic medical record to mitigate this serious problem and improve patient outcomes, leadership within the Johns Hopkins Department of Pediatrics, Armstrong Institute for Patient Safety and Quality Analytics and Johns Hopkins Hospital provided significant monetary support to make this program a success. This support allowed for the development and ongoing enhancements of the dashboard to identify at-risk patients, and also supports the efforts of the nurse, physician and pharmacist on the NINJA team who interact and educate the clinical teams daily.
Innovation:
AKI is often thought of as an unavoidable harm. This collaborative has challenged that assumption and proven that harm from NTMx-related AKI can be prevented and mitigated.
Specifically, at Johns Hopkins, the use of the proprietary dashboard has permitted efficient and comprehensive implementation of the NINJA program. The dashboard also allows for easy expansion of the program to other pediatric populations within the institution and could be used to undertake similar initiatives in our adult patients.
Culture of Safety:
The Hopkins NINJA team’s daily interaction with the primary medical teams, primarily with resident physicians, has led to increased knowledge of nephrotoxic medications and AKI. Anecdotally, as the program has gone on, the NINJA team has found that the residents anticipate our daily visits and often try to predict which patients we will discuss with them and why they are at risk. We have also found that emphasizing the criteria for diagnosing AKI has made teams less likely to discount small, but clinically significant, changes in creatinine. What may have been previously unrecognized or described as an insignificant “bump” in serum creatinine is now being appropriately identified as AKI.
Patient and Family Integration:
Although this intervention has primarily involved the medical team, we are working to develop a specific AKI follow-up clinic that patients who experience AKI from NTMx exposure (or other reasons) could be referred to for long-term monitoring of kidney function after AKI. With this clinic, we plan to educate patients and families on the long-term risks of AKI, including risks of chronic kidney disease, and help them understand their diagnosis and ways to help avoid additional injury to their kidneys.
Related Tools and Resources:
See Appendices I and II.
Contact Person: Jeffrey Fadrowski, MD
Title: Associate Professor of Pediatrics, Johns Hopkins School of Medicine
Phone: (410) 955-1247
Email: [email protected]
Appendix I. Screenshots of Qlikview Dashboard Hopkins NINJA: Nephrotoxic Injury Negated by Just-in-time Action
Appendix II: Nephrotoxic Medication ListNINJA: Nephrotoxic Injury Negated by Just-in-time Action
Legend:
* = Therapeutic Monitoring Recommended
Also include combination products which include the above medications (e.g. Lisinopril/HCTZ) and formulary alternatives of the national collaborative list (e.g. candesartan)
For all medications: Systemic forms only (no topical or inhaled forms)
Blue Highlight = Medications which can trigger without another medication on
day 3 of exposure (aminoglycosides and vancomycin)
NINJA 57 Medication ListAcyclovirAmbisomeAmikacin*Amphotericin B (7days)AspirinCaptoprilCarboplatinCelecoxibCidofovir (7days)CisplatinColistimethateCyclosporine*DeferasiroxDiatrizoate meglumine (7days)Diatrizoate sodium (7days)EnalaprilEnalaprilatFoscarnetGanciclovirGentamicin*IbuprofenIfosfamideIndomethacinIodixanol (Visipaque) (7days)Iohexol (Omnipaque) (7days)Iopamidol (Isovue) (7days)Iopromide (7days)Ioversol (7days)Ioxaglate meglumine and ioxaglate sodium (7days)Ioxilan (7days)KetorolacLisinoprilLithium*LosartanMesalamineMethotrexate*MitomycinNafcillinNaproxen
Pamidronate disodiumPentamidinePiperacillinPiperacillin/TazobactamPolymixin BSirolimus*SulfasalazineTacrolimus*TenofovirTicarcillin/Clavulanic AcidTobramycin*TopiramateValacyclovirValganciclovirValsartanVancomycin* Zoledronic acidZonisamide