Embed Size (px)
Citation preview

Hands only Energy Healing: A review of the recent literature.
Donna Bass
06/22/2012
Year 2 final paper
John Elfers

Abstract:
Ten scholarly articles were reviewed to determine the state of Energy Medicine research.
Hands only modalities are covered in this review in order to keep variables low, and to isolate
the energy involved in this type of therapy. Also covered in this review are the questions of
whether the phenomenon of Energy Medicine has been adequately observed, defined, researched
and how research may proceed from here. The definition of wellness is discussed, along with the
possible implications of the existence of energy healing.
Possible mechanisms discussed include electromagnetic fields, biofield hypothesis,
quantum physics, classical and non-classical fields, as is cortical reshaping.
The findings suggest that indeed there is an energy phenomenon, and that it does
facilitate healing. However, the mechanism is unknown. More rigorous studies and much larger
studies need to be conducted.
Suggestions are made in regard to further research, more rigorous research, defining
energy medicine further, and the future of Energy medicine research.
Keywords: “energy medicine” “energy healing”, “touch healing”,“hands on energy
healing”, “biofields”, “bioenergy”, “wellness”.

During the past 20 years an increasing number of people are turning to alternative energy
therapies. Of the research reviewed for this paper, dementia, stress, pain, post-operative patients,
anxiety, and cancer patients with fatigue, pain and nausea were the conditions treated. While
there is no conclusive research to prove that there is any beneficial effect, more and more people
continue to seek these alternative therapies (National Center for Complementary and Alternative
Medicine (NCCAM) website). These alternative therapies include but are not limited to:
acupuncture, herbalism, yoga, massage, Ayurveda, and meditation. This review will explore the
current literature to determine the effects, if any, of human energy healing, and what those
effects may be. In order to focus on healing energy, this paper will only review research
conducted on Reiki, Therapeutic Touch, Johrei, and Qigong. The reason for this is these
modalities use no tools, and move no bones, tendons, fascia, or muscle to get a result;
practitioners use the laying on of hands exclusively.
Have studies observed the energy of healing clearly and rigorously enough to ask
questions or make assertions about this healing energy? According to Dossey (2008) much
more work needs to be done to have cohesive research on energy and healing. Dossey poses the
important point of: “not how large the effects [of energy healing] are, but whether they exist at
all” (Dossey, 2008, p. 343). Dossey cites Jonas and Crawford [Jonas is the former director of the
NIH National Center for Complementary and Alternative Medicine] as stating:
“There is evidence to suggest that mind and matter interact in a way that is consistent with the assumptions of distant healing. Mental intention has effects on nonliving random systems (such as random number generators) and may have effects on living systems. While conclusive evidence that these mental interactions result in healing of specific illness is lacking, further quality research should be pursued.” (Dossey, 2008, p. 343)

The very idea that non local consciousness can have an effect on a living system could
have a major impact on the way our universe is understood. The entire field of modern medicine
would be dwarfed by this concept. Form following function would no longer be the basis of
medicine. Consciousness would have to become a significant factor in healing, wellness, and
chronic wellbeing; this would also mean that the spirituality of an individual would have to be
taken into account when diagnosing illness.
This review makes the assumption that healing energy is a causal phenomenon and work
within that paradigm. To begin, there are two critical questions: what is wellness, and what is
energy and healing?
First, what is wellness? Fahlberg and Fahlberg (1997) explicate the difference between
Eastern awareness of optimal wellness and the awareness of wellness that is part of the current
Western lexicon.
The World Health Organization defines wellness as: “the optimal state of health of
individuals and groups. There are two focal concerns: the realization of the fullest potential of
an individual physically, psychologically, socially, spiritually, and economically, and the
fulfillment of one’s role expectations in the family, community, place of worship, workplace and
other settings.”(Health Promotion Glossary update WHO website)
Fahlberg and Fahlberg take this idea further to describe wellness in terms of expanding
consciousness beyond culture-bound biases (fulfillment of one’s role expectations). In the West
the perceived prevailing cultural norm of wellness is the absence of pathology. Pathology is
often determined by the “fashion of the day” (Fahlberg & Fahlberg, 1997, p. 3); this phrase alone
reveals the spurious nature of what wellness means in this culture. The Western paradigm of
wellness is primarily behavior and culture based.

The Eastern characterization of wellness is consciousness centered. According to
Fahlberg and Fahlberg (1997), “for the West the medium for adaptation to society has been
behavior, for the East the medium for progression beyond normality has been human
consciousness” (Fahlberg & Fahlberg, 1997, p.4) in fact, both can be true. A change in
consciousness can cause a change in wellness, which would also cause a cessation of symptoms.
Fahlberg & Fahlberg also discuss the dangers of misinterpreting expanded consciousness for
pathology. There are a number of key points presented by this paper on the dangers of
misinterpreted normal development being mislabeled as illness. Those points are: the
pathologizing of optimal development because it is not “normal”, and that people who go beyond
the normal are ill and need to be “corrected”; therefore the development must be suppressed.
This point is an eerie warning from the past in light of the rampant use of brain altering drugs on
children who are regularly diagnosed with behavior disorders (Emery & Bass, 2012). Expanded
consciousness behaviors could very well be normal optimal development.
The second point Fahlberg and Fahlberg make concerns self-transformation and how
self-transformation can positively affect the community as well as the individual; “inner work for
growth and the outer work of enhanced human relationships and community”(Fahlberg &
Fahlberg, 1997, p.6), in other words, the inner work strengthens the individual which in turn
strengthens the entire community. “As inner identity expands and transcends the isolated and
separate ego self, more of the world that was previously other or separate from the ego self, is
now identified with a new expanded self. This expansion has tremendous implications for
community and social responsibility as well as the transformation from a sociocentric view to a
worldcentric view” (Fahlberg & Fahlberg, 1997, p.6), this outlook provides a much expanded

viewpoint of wellness. This article successfully invites and induces new pathways of thought
and points of view about the definition of wellness on a personal level and on a global level.
Next we will examine practitioners and healers who use alternative healing modalities.
Levin (2011) separates the traditions into: East Asian tradition such as Reiki and Qigong;
Western professional tradition which is widely used among nurses, Healing Touch and
Therapeutic Touch; a bioenergy tradition originating in Eastern Europe (Wirkus Method); and
contemporary metaphysical traditions such as Barbara Brennan, Donna Eden, and Rosalyn
Bruyere, who are well known healers who certify healers in their perspective methods.
Levin (2011) asks if there are core (common) concepts for healing. He then poses
fundamental questions critical to the healing community. These questions are: “ what is the
source of healing and the pathway by which it is transmitted to the client, what exactly is being
transmitted, what exactly healers do when they perform healing, the state of consciousness
required by the healer in order for healing work to take place, what is required of the client to
receive healing?” (Levin, 2011, pp. 17-18). Levin concludes “it is difficult to identify a single
underlying belief or practice that unites all energy healers” (Levin, 2011, p. 18). Levin then
goes on to contradict himself by listing salient (common) themes in healing (Levin, 2011, p. 19).
Does technique matter? Levin asserts that technique does not matter, and there are many
different forms and methods of healing. Each approach is valid in its own way and is not
important for healing.
Levin’s (2011) ideas are confusing, and contradictory. In summary, there are many ways
and numerous beliefs and techniques of healing, but technique and belief are not the important
part of healing. On the one hand Levin finds that there is no unifying concept (pg. 6) then lists
unifying concepts of healers.

Another study that attempts to define energy healing is the study by Warber, Cornelio,
Straughn and Kile, (2004). “The primary objective of this paper is to explore relevant unifying
concepts about the nature of energy healing that may underlie the different modalities through
qualitative interviews with practicing biofield energy therapists” (Warber et al., 2004, p.1108).
Participants (n=19) with general knowledge of energy healing modalities: Reiki, Healing
touch, Barbara Brennan School, Sufi advanced energy healing, therapeutic touch, polarity
therapy, esoteric healing and qigong were interviewed for this study. Each practitioner was
interviewed; interviews were then transcribed and coded by a single investigator, which may
have introduced bias into the analysis. Survey questions were not included in the article. Videos
were also viewed by researchers and the responses were coded as well, though the coding lacks a
clear description. Seven dimensions of energy were gleaned from practitioners’ responses by
Warber et al. Those dimensions were: sources of energy, entities with energy, human energy
anatomy, descriptions of energy, movement of energy, action of energy, and perception of
energy. Each category is described and summarized. The article goes on to describe healer
client relationships, healing facilitation, compatibility, collaboration, communication, trust, and
ethics.
The authors conclude that there is a coherent worldview held by energy healers that describes the
world in energetic terms (the seven dimensions of energy). This worldview goes beyond only
electromagnetic nature. The researchers felt that they had attained the goal of exploring unifying
concepts about the nature of energy healing that may underlie the different modalities. This was
achieved by conducting qualitative interviews with practicing biofield energy therapists. One
limitation of this study is that the information is one sided; clients were not interviewed about
their relationship with the practitioner or about the healing encounter. Also, the failure to bring

practitioners of various disciplines together to compare and contrast efficacy, methodology, and
agreed upon principles and descriptions.
The second key question is: What is this energy? There are a number of theories in the
literature about the substance and function of this energy. An early theory is presented in a
seminal work written by Rubik (2002). This article sets forth the scientific foundation of the
biofield using the theories of linear and nonlinear systems, self-organizing systems, chaos theory,
and classical physics; electromagnetic (EM). Rubik (2002) does not go into quantum physics as
do other theories of biofield therapies (Rein, 2004, Feinstein & Eden, 2008, Miles & True,
2003), but limits her definitions to the fields of bioelectromagnetics and biophysical systems
theory (p.709).
The biofield hypothesis is defined by Rubik as “the endogenous complex dynamic
electromagnetic field resulting from the superposition of component EM fields of the organism
that is proposed to be involved in self-organization and bioregulation of the organism” (Rubik,
2002, p. 709). This biofield could be a very complex dynamic standing wave (standing waves do
not propogate). Standing waves are non-classical waves. The way that the biofield mediates
healing with hands on biofield therapies could be” mediated by means of electromagnetic
bioinformation” (p. 714). In other words low level electromagnetic waves from the practitioner
could interact or resonate with the EM of the client, causing a shift in the biofield of the client
toward wellness. A similar theory has been proposed by others in the field (Gulman, 2004;
Miles & True, 2003; Warber, et al., 2004); that one person can affect another person’s biofield.
Rubik (2002) presents a well thought out theory and definition of biofields. This theory
is grounded in classical physics and what is known about information systems. However, Rubik
runs the risk of oversimplification. There are complex systems at work that are weaving together

not in a summation, but in a synergy of energies and fields yet to be described. Electromagnetic
fields are a part of this complex system to be sure, as are electrical systems, magnetic systems,
linear and nonlinear systems. This article fails to address the efficacy of this mode of healing,
and offers only a limited definition of biofields. For a more comprehensive addition to this
theory Rein (2007) introduces theories of quantum physics to the definition of the biofield and
adds non classical and quantum forms of energy (Rein, 2007, p. 59). The intent is to broaden the
definition of the biofield introduced by Rubik (2002) to give it a more comprehensive definition.
Rein (2007) begins with classical electromagnetic (EM) by explaining that there is an
altered DC (direct current) resistance and conductance at accupoints on the body. He discusses
electroencephalograph, electromyography, and electrocardiograph which all measure
fluctuations of the human EM fields, and introduces the biophoton.
“Biophotons are associated with cell growth and differentiation, and mediate intercellular
communication” (Rein, 2007, p.60). Biophotons, then, would be the biological particle as the
photon is to the light wave. While this is fascinating, no connection with healing and biophotons
is ever made. However, this is a familiar theory as the author has often wondered if there are
bioquanta that would unify physics and biology. Instruments to diagnose and assess the biofield
are then discussed.
The instruments measure and record the natural biofield information of the patient and
play it back to the body in order to balance the biofield. This method is reminiscent of resonance
at work.
Rein elaborates on these ideas by explaining that, “Under healthy conditions there is a
periodic fluctuation in a meridians frequency whereas no fluctuations are observed in illness”
(Rein 2007, p.61). Rein then goes on to explain that “externally applied frequencies can alter

these endogenous frequencies by shifting their fundamental value or modulating their
fluctuations” (Rein 2007, pg. 61).
Rein then discusses anomalies in the human system that cannot be explained by classical
physics. These anomalies include: extreme sensitivity to ultra-low intensity EM fields, long
distance healing of Reiki and prayer, biologic effects of plasma waves, biologic effects of
potential fields. These would all suggest that there is a non-classical mechanism at work in the
human biofield.
Rein presents a convincing argument that includes non-classical fields in the definition of
biofields. However, jumping to quantum physics may be a bit premature. Quantum physics has
become the universal explanation for many scientific conundrums. Each thread of information
must be disentangled from the whole one piece at a time. A more pragmatic route of discovery
would be to just continue to observe the energy, allowing it to reveal itself. Labeling this energy
prematurely is taking the risk of oversimplifying this complex human energy system.
Another perspective on human energy fields is illuminated by Miles and True (2003).
Their study focuses on Reiki, a biofield therapy. They “evaluate and synthesize the history,
theory, and practice of Reiki and the state of Reiki research” (Miles & True, 2003, p. 62). They
start with the five precepts of Reiki which are “Just for today do not anger. Just for today do not
worry. Be humble. Be honest in your work. Be compassionate with yourself and others”
(Miles & True, 2003, p. 63). These are similar values with every modality discussed in this
paper. Miles and True continue to describe the session itself, history and training of Reiki.
Miles and True (2003) discuss possible theories or models of mechanism of action being
consistent with bioelectromagnetism, quantum physics, and superstring theory, “which are
consistent with Asian scripture (Miles & True, 2003, p. 65) Reiki vibration [or the universal Chi

energy] is understood to be drawn through the practitioner by the client according to the client’s
needs. The client often feels vibrational flow, sometimes heat or coolness or waves of relaxation
throughout their body. These observations are consistent with Gulman (2004). Miles & True
(2003) postulate that these feelings may be a “subtle entrainment effect similar to that of sound
healing, whereby Reiki vibrations attune the recipient’s biofield to greater harmony. “The
reason for this attunement [is that it] could have a strengthening effect on the biofield thereby
influence the body’s ability to heal” (Miles & True, p. 65). This article then goes on to discuss
clinical practices and programs, and then delves into the state of Reiki research.
Miles and True (2003) discuss seven randomized controlled studies. Many of them find
Reiki to a be statistically significant treatment for pain, reduction of blood urea nitrogen and a
trend toward normalization of blood glucose, statistically significant reduction in sEMG activity
at thoracic and lumbar sites associated with autonomic system and relaxation response (Miles &
True, 2003, p. 70). There were also inconclusive or negative findings with accelerated healing,
and detection of “real” or “sham” Reiki practitioners.
Miles and True (2003) also found that these trials also had a number of limitations and
flaws in methodology (p. 70).
Feinstein & Eden (2008) in a very dense article propose six pillars of energy medicine
and describe them in detail. The biofield as defined in this paper : “The biofield is comprised of
an extremely weak but measurable electromagnetic field (EM)—with its own waveform,
intensity, polarity, and modulation patterns—that surrounds and permeates all living systems “
(p.46) along with more localized energy fields in different parts of the body or the chakras.
According to this article these chakras have been measured “up to 1600 cycles per second, as
compared to 0-100 cycles per second in the brain, 225 cycles per second in the muscles, and 250

cycles per second in the heart" and that these local energy domains corresponded with ancient
descriptions of the body's "chakras" (Feinstein & Eden, p. 46).
The next energetic system discussed is energy pathways. According to Feinstein and
Eden (2008) there is a possible energetic pathway that interacts with and acts upon the lymph,
nervous and circulatory system that is capable of reading coding and transmitting information
from one part of the body to another. With this begins a discussion of what possible energies are
at work in the body. The energies discussed are: chemical-electrical-chemical interactions of ion
pumps and polarization/depolarization of cells in the body, and: “electromagnetic energy travels
as a wave but is absorbed as a particle [photon]” (Feinstein & Eden, 2008, p. 48).
The six pillars of energy medicine are then introduced and explained at length. The
pillars are: 1. Reach, or that EM can address biological processes at their energetic foundations
thereby able to address all physical conditions 2. Efficiency regulates all biological processes
with precision speed and flexibility, 3. Practicality, EM fosters healing and prevents illness with
methods that can be readily, economically, and non-invasively applied. 4. Patient empowerment,
EM includes methods that can be used on an at-home, self-help basis, fostering a stronger patient
and practitioner partnership in the healing process. 5. Quantum compatibility, EM adopts non-
linear concepts consistent with distant healing, the healing impact of prayer, and the role of
intention in healing 6. Holistic orientation EM strengthens the integration of body, mind, and
spirit, leading not only to a focus on healing but to achieving greater well-being peace, and
passion for life (Feinstein & Eden, 2008, p. 49). These claims are largely speculative as there is
no research to substantiate these claims, and a more comprehensive definition of what they mean
by quantum physics is in order as non-classical physics is not necessarily quantum.

This article has some good arguments about electricity being a mechanism of healing,
and the six pillars are a good place to begin. However much more work needs to be done to
quantify these pillars and these precepts. Feinstein and Eden (2008) propose a number of
experiments to validate these pillars. This article is definitely a well thought out place to start the
quest for the mechanism of energy medicine.
Jain & Mills (2010) reviewed 66 clinical studies of 9 different biofield therapies
(Therapeutic touch, Qigong, Reiki, spiritual healing, healing touch, Johrei, laying on of hands,
Johnson bioenergy and polarity therapy) that summarize “the state of the science on biofield-
based techniques as they are practiced proximately” (Jain & Mills, 2010, p. 12)
The studies included: peer reviewed journals, practitioner and client were in same room
(proximal), quantitative studies with randomized controlled trials (clinical).
This was in pain-related disorders (n=15); cancer patients; (n=11); postoperative or rehab (n=6);
with dementia (n=4), cardiovascular (n=4); students (n=9); healthy participants (n=13) The
results were, of 66 studies reviewed 85% reported physiological or self- report outcomes, 54%
reported biological or objective functional outcomes, and 9% examined qualitative reports. The
findings suggest strong evidence for effects of biofield therapies in decreasing pain intensity,
moderate evidence for reducing pain in cancer populations, moderate evidence behaviors
associated with dementia, limited findings for quality of life in pain patients (Jain & Mills, 2010,
p. 12). Proximal biofield therapies suggest: they are promising for reducing pain, anxiety, and
reducing agitation of dementia (Jain & Mills, 2010, p. 13).
The limitations of this study were: no quantitative only quantitative data, reliance on p
(probability not Pearson) values and not effect sizes, not meta-analysis, area of study is in its
infancy. The n values were small giving low power to findings. Only proximal treatments no

long distance data was taken. This article recommended for future studies: cardiovascular,
neuroendocrine and immune variables; comparison of biofield interventions with empirically
supported treatments to determine benefits of energy based treatment.
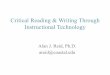
Kerr, Wasserman & Moore (2007) postulate that a somatosensory plasticity and
perceptual learning mechanism modulate touch healing. This theory is based upon
“somatosensory hand maps from musicians and braille readers that have specific differences
from those of normal controls” (Kerr et al., 2007, p. 60). The somatosensory homunculus is
provided below (image 1). Each section of the somatosensory cortex corresponds to a portion of
the body and is labeled with a drawing of that body part. The hypothesis is: “that touch healing
modalities work to renormalize somatotropic maps. This prediction is supported by the
observation that factors facilitating map reorganization are also cardinal features of touch healing
treatments and this cardinal features act in opposition to the conditions that initiate and maintain
chronic pain” (Kerr et al., 2007, p. 61).
To support this hypothesis Kerr et al. (2007) present some interesting correlations.
Cardinal factors in persistent chronic pain are listed as: repeated sensory input (chronic nature of
pain), somatosensory attentional modulation (pain draws attention), behavioral relevance
(sensory inputs cause behaviors, if these behaviors modulate pain, the behaviors continue) and
stress. The cardinal factors of inducing cortical plasticity (or change in somatosensory cortex),
along with the cardinal factors of pain, makes the case for the optimal induction of cortical
plasticity.
Repeated sensory input (repeated tactile stimulus such as pain), somatosensory
attentional modulation (shifts of attention can reorganize sensory cortical maps.), behavioral
relevance; “context and expectation associated with a stimulus are central to its efficacy in

changing the somatosensory cortical body map” (Kerr, et al., 2007, p. 61), stress; high stress or
high concentration of stress hormones with a stimulus are central to this change. Interestingly,
Dossey (2008), Feinstein & Eden, (2008) and Warber et al. (2004) also discussed repeated
sensory input of repeated sessions with a practitioner and the importance of at home self-
treatment for optimum effect.
Finally the cardinal factors of touch healing treatment are discussed. Repeated sensory
input (repeated sessions); somatosensory attentional modulation (implied touch stimuli may
serve the function of guiding subject’s somatosensory attention (Kerr et al., 2007 p. 62). This
may engage tactile induced changes. The behavioral relevance according to this model is
patients who believe in “vibrational power” may endow touch healing with greater behavioral
relevance which may facilitate therapeutic cortical remodeling. Lack of stress (soothing
environment, lying down, evocative music, etc.) may block stress hormones and stress
neurochemistry that could cause a therapeutic cortical remodeling.
To summarize, touch healing, with repeated use can actually remodel the brain to a
healthier, less stressful form and function. This theory does make sense, however much work
including bench research needs to be done to quantify this theory more completely.
Image 1: http://www.orble.com/images/ns312.jpg

Processes that are discussed in any study require rigorous definition. The research
reviewed in this paper define Energy and Healing as: Touch Healing (Kerr et al., 2007), Biofield
Healing (Feinstein & Eden, 2008; Jain & Mills, 2010; Miles & True, 2003, Rein, 2004; Rubik,
2002) and Energy medicine (Dossey, 2008; Feinstein & Eden, 2008). These three terms describe
the same healing modalities. In order to clarify precisely what group of modalities that are being
discussed Biofield Healing originally described by Rubik (2002) would be the most logical term
to describe hands on energy and healing. This modality group would include Reiki, Therapeutic
Touch, Johrei, healing Qigong, or any proximal hands only healing modality.

The processes themselves also require clear and concise definitions. In the reviews there
were few explanations of what Johrei, Reiki, or Qigong or their history, however Miles and True
(2003) did an excellent job defining the Reiki process and training. The history of a modality
may shed light on how this energy is tapped into and how it works for healing.
Search keywords used were: “energy medicine” “energy healing”, “touch healing”, and
“hands on energy healing”. Most of the articles included other modes of healing such as herbs,
new age dogma, religious dogma and belief et al., acupuncture and food, which are variables
surrounding hands on energy healing, not about the healing energy itself. This fact contributes to
the lack of clarity.
Vilifying the current way of doing medicine is not going to advance the cause for any
modality. Many of the papers reviewed had a very harsh tone in regard to Western Medicine.
Western medicine is not the enemy. Thanks to Western medicine many diseases have been
eradicated and the quality of life has been made better for many with life threatening diseases in
ways that biofield healing cannot. A biofield healer cannot do a heart or kidney transplant that
can save a life, or a hip replacement that will greatly enhance the quality of life. Research must
stop “Western bashing” because it gives the entire profession of Bioenergy research an
unprofessional and biased presence, and completely discounts the strides made by Western
science. This is the opposite of what Transpersonal and Humanistic Psychology holds up as core
values, which are to value and seriously consider all points of view, and to be humble enough to
diligently add to the knowledge base with respect for all. Dossey (2008) states; to “simply to do
our work patiently and take the long view” (Dossey, 2008, p. 351). Working together with
Western medicine synergistically combining and researching together for the greater good would
accelerate our understanding of this biofield and how it works for healing.

Miles and True (2003), Jain and Mills (2010), and Dossey (2008) found the quality of
research studies to be lacking. As long as there is critical thinking and critique of the research it
will only get better and better.
Researchers must decrease the number of variables, to reduce bioenergy to the specific
issue of energy for healing. For example, energy and modes to access that energy (ritual, belief)
are two very different things. Dogma and spirituality are not the energy that is used; the ball of
twine needs to be unraveled more finely. Many assumptions have to be set aside. These
assumptions are that healing is a spiritual experience, along with the assumption that everyone
knows what spiritual is or means. For example, according to Dossey (2008), the STEP
intercessory prayer study found that the group who got intercessory prayer during recovery from
coronary bypass had the greatest number of postoperative complications. The researchers
reported this “may have been a chance finding” (Dossey 2008). The assumption was that prayer
could not be bad for a person. Assumptions must be eliminated or clearly stated to get a clear
view of the results of studies.
Dossey’s (2008) paper suggests a number of considerations for future research, and
future directions for healing research. Many of these considerations are extremely pragmatic and
seem effective. He suggests: a healing summit that would bring together key healing researchers
in order to confront some of the questions about healing research, a moratorium be enacted in
order to sort out exactly where we are and what to do next. Some of the issues to be addressed:
study the actual techniques of healing, single case reports should be encouraged, determine what
conditions are most susceptible to this methodology. Importantly, this paper recommends more
bench science and proof of principal studies.

Another useful direction would be to observe the energy indirectly. People who use this
healing energy daily would be interviewed. The people who use this energy for healing and
manipulate the biofield would be the people most intimately knowledgeable in this area. Warber
et al. began this process in the Michigan US area and noted some interesting observations that
were inspired by the participants who were bioenergy healers themselves. This interview
process could be expanded to a nationwide, then worldwide study of bioenergy healers. As
stated by Levin (2011), and Fahlberg and Fahlberg (1997) there needs to be a cross cultural
conversation about energy and healing as there are many definitions and concepts to synthesize.
This study would include standardized questions about energy and healing in order to get a
glimpse of how the bioenergy may work. Observing the energy and how it is used with no
hypothesis or agenda by the researcher will get us closer to an answer about the makeup and
behavior of the biofield. This could be followed up by a study with the clients who receive this
method of healing and how or if it worked followed by why and how it did or did not work.
Bench research could include a rat model of cortical remodeling and reshaping as
suggested by Kerr et al. (2007). Rats could be elevated maze trained which causes stress, and
then examine the brains of the stressed animals over time, as compared to non-stressed animals
to determine cortical plasticity changes.
In conclusion, the area of biofield research is rich with opportunities for the serious
researcher. There is much work to be done to design studies with power and with precision.
There is a positive consensus that something is happening, there is an effect as positive findings
keep coming forward in the areas of pain and stress. There has been no landmark study to prove
that this biofield exists, yet every day this biofield therapy is used when one soothes a child or
embraces a loved one. New ways of thinking about the biofield is in order. There must be a

separation from spirituality and the sacred, toward objective scrutiny and clear thinking in order
to move forward with finding a mechanism of action.
References
Dossey, L., (2008). Healing research: What we know and don’t know. Explore: The Journal of Science and Wellbeing. 4(6), pp. 341-352.
Emery, K. & Bass, D., (2012). Attention-seeking: Weighing old and new perspectives of ADD, ADHD. Case in Point. 10(5), pp. 22-23.
Fahlberg, L. L. & Fahlberg, L. A., (1997). Wellness re-examined: A cross cultural perspective. American Journal of Health Studies. 13(1), pp. 8-17.
Feinstein, D. & Eden, D., (2008). Six pillars of energy medicine: Clinical strengths of a complementary paradigm. Alternative Therapies in Health and Medicine. 14(1), pp. 44-54.
Jain, S. & Mills, P. J., (2010). Biofield therapies: Helpful or full of hype? International Journal of Behavioral Medicine. 17, pp.1-16. DOI 10.1007/s12529-009-9062-4
Kerr, C., Wasserman, R. H., & Moore, C. I., (2007). Cortical dynamics as a therapeutic mechanism for touch healing. The Journal of Alternative and Complementary Medicine. 13(1), pp. 59-66.
Levin, J., (2011). Energy healers: Who they are what they do. Explore: The Journal of Science and Wellbeing. 4(6), pp. 341-352.
Miles, P. & True, G., (2003). Reiki—review of a biofield therapy history, theory, practice and research. Alternative Therapies in Health and Medicine. 9(2), pp. 62-72.
National Center for Complementary and Alternative Medicine (NCCAM) website, The use of complementary and alternative medicine in the United States webpage (NA),
http://nccam.nih.gov/news/camstats/2007/camsurvey_fs1.htm
Rein, G., (2004). Bioinformation within the biofield: Beyond bioelecctromagnetics. The Journal of Alternative and Complementary Medicine. 10(1), pp. 59-68.
Rubik, B., (2002). The biofield hypothesis: Its biophysical basis and role in medicine. The Journal of Alternative and Complementary Medicine. 8(6), pp.703-717.

Warber, S.L., Cornelio, D., C, Straughn, J. & Kile, G., (2004). Biofield energy healing from the inside. The Journal of Alternative and Complementary Medicine. 10(6), pp. 1107-1113.
World Health Organization, Health promotion glossaries update PDF, retrieved from WHO website: http://www.who.int/healthpromotion/about/HPR%20Glossary_New%20Terms.pdf