Embed Size (px)
Citation preview
+
VA HEALTHCARE: SCANDAL, GREATNESS AND BACK AGAIN
Key lessons learned, and relevance to the NHS
Ashish K. Jha, MD, MPHDecember 2, 2014Twitter: @ashishkjha
+Goals
Basic background on the VA
The VA story for change
VA as a model for improvement Decentralization of decision making Performance measurement Health Information Technology Visionary leadership
What went wrong?
How the VA can turn things around
+History of the VA
Continental Congress of 1776 Authorizes pensions for disability in the
revolutionary war
Veterans Administration established 1930
Department of Veterans Affairs in 1989 Achieves cabinet level status
+The VA
6 million patients receive at least some care in the VA
Out of 26 million living veterans in the U.S.
Who is eligible for VA care? Service-connected (service-related health
conditions) Prisoners of War or recipients of the Purple Heart Poor (for a family of 4, <$35K in annual income)
+Who receives care in the VA system?
They are old: 40% are > 65 years old
They are poor: 70% have annual incomes <$26,000 Median family income in US is $51,000
They are generally sick: Compared to age-matched Americans, they have
3 additional non-Mental Health Diagnoses 1 additional Mental Health Diagnosis
+VA Facilities: Some Basics
1400 Sites of Care 153 Medical Centers 768 Community-based outpatient clinics 135 Nursing Homes
254,000 employees 19,000 doctors (about 3% of all physicians) 50,000 nurses
+VA Background
Perceptions of poor quality Widely depicted as having poor quality doctors,
nurses Long wait times High mortality rates
Congress considered closing VA hospitals
Mid-1990s: Transformation is launched Decentralization Data collection and feedback Performance measurement Accountability Electronic Information Systems
+VA Transformation: Element #1
Decentralization
Nation split into 22 regions based on referral
patterns
Each region had a director who was given a budget
All major clinical decisions were to be made locally
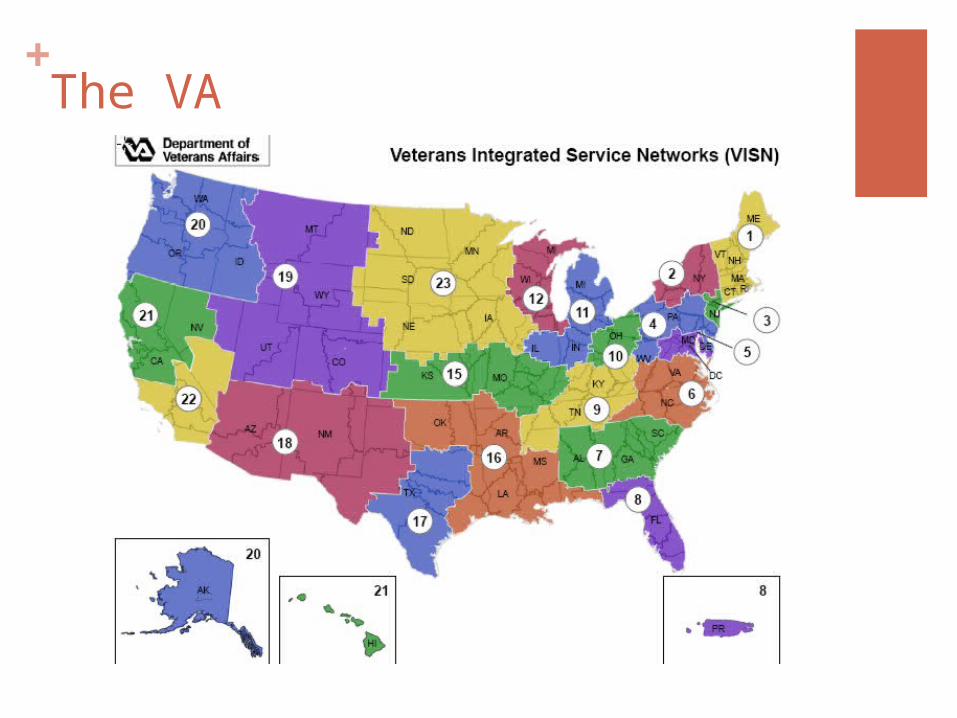
+The VA
+VA Transformation: Element #2
Performance measurement & accountability
Key quality metrics chosen based on clinical priority
Targets set in Washington DC with input from clinicians
Contracts with local leadership, salary tied to performance
Peer-pressure and competition
+VA Transformation: Element #3
Data collection / feedback
Independent outside entity collects quality data
Data reported back to facility every 3 months
Opportunities for review, correction of errors, etc.
+VA Transformation: Element #4
Health Information Technology
Electronic Health Record rolled out across the VA
Computerized physician order entry a priority
Clinical Decision Support such as clinical
reminders
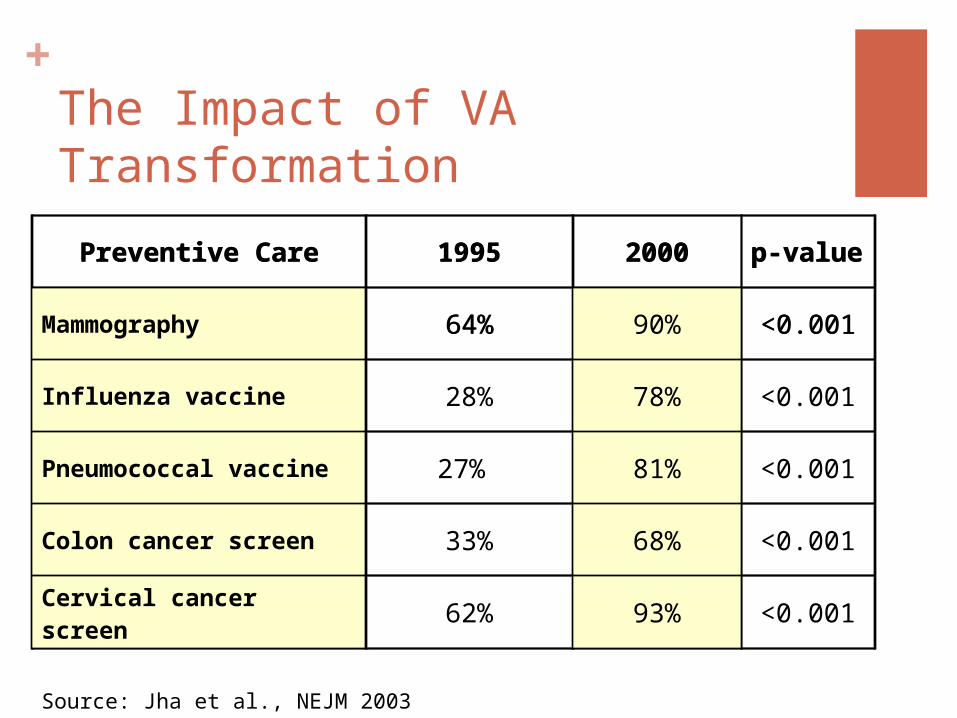
+The Impact of VA Transformation
Source: Jha et al., NEJM 2003
Preventive Care 1995 2000 p-value
Mammography 64% 90% <0.001
Influenza vaccine 28% 78% <0.001
Pneumococcal vaccine 27% 81% <0.001
Colon cancer screen 33% 68% <0.001
Cervical cancer screen 62% 93% <0.001
Preventive Care 1995 2000 p-value
Mammography 64% 90% <0.001
Influenza vaccine 28% 78% <0.001
Pneumococcal vaccine 27% 81% <0.001
Colon cancer screen 33% 68% <0.001
Cervical cancer screen 62% 93% <0.001
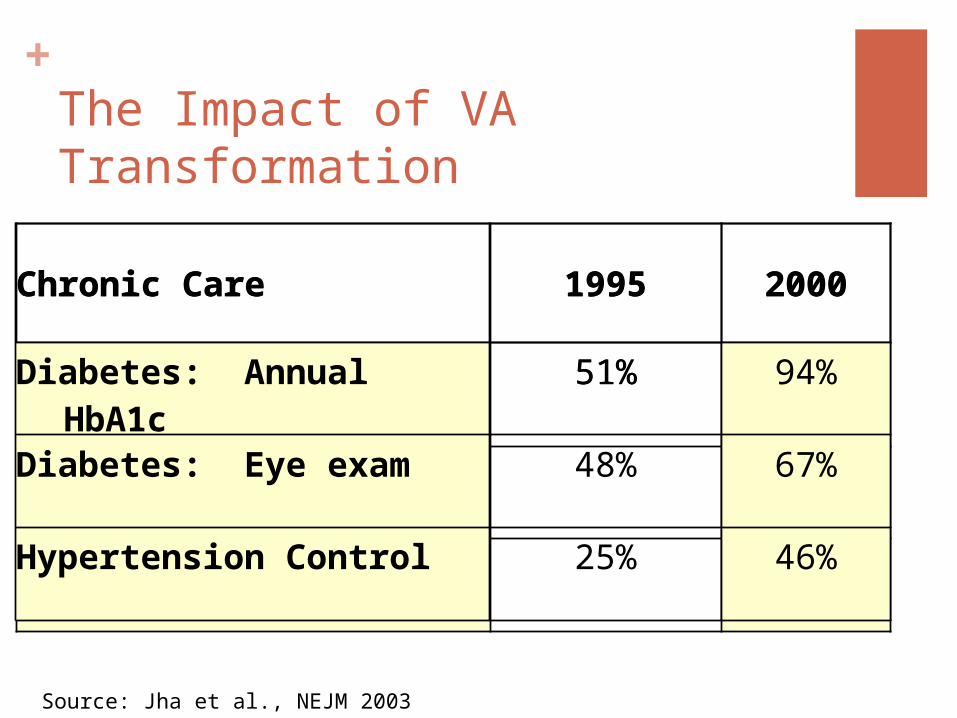
+The Impact of VA Transformation
Chronic Care 1995 2000
Diabetes: Annual HbA1c
51% 94%
Diabetes: Eye exam 48% 67%
Hypertension Control 25% 46%
Source: Jha et al., NEJM 2003
Chronic Care 1995 2000
Diabetes: Annual HbA1c
51% 94%
Diabetes: Eye exam 48% 67%
Hypertension Control 25% 46%
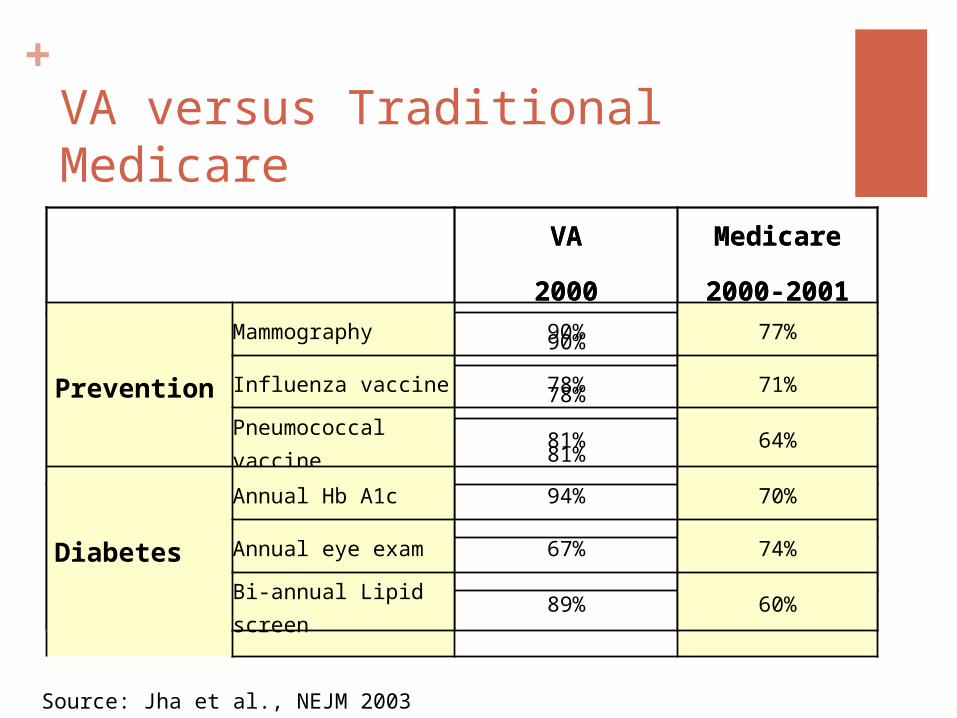
+VA versus Traditional Medicare
VA
2000
Medicare
2000-2001
Prevention
Mammography 90% 77%
Influenza vaccine 78% 71%
Pneumococcal vaccine
81% 64%
Diabetes
Annual Hb A1c 94% 70%
Annual eye exam 67% 74%
Bi-annual Lipid screen
89% 60%
Source: Jha et al., NEJM 2003
VA
2000
Medicare
2000-2001
Prevention
Mammography 90% 77%
Influenza vaccine 78% 71%
Pneumococcal vaccine
81% 64%
Diabetes
Annual Hb A1c 94% 70%
Annual eye exam 67% 74%
Bi-annual Lipid screen
89% 60%
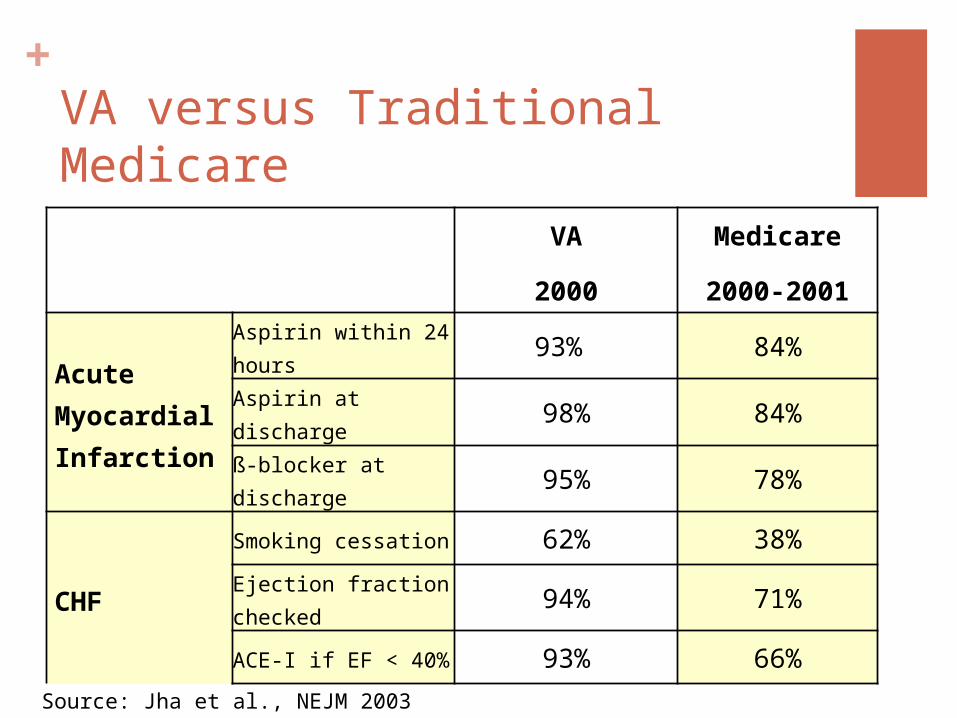
+VA versus Traditional Medicare
VA
2000
Medicare
2000-2001
Acute Myocardial Infarction
Aspirin within 24 hours
93% 84%
Aspirin at discharge 98% 84%
ß-blocker at discharge
95% 78%
CHF
Smoking cessation 62% 38%
Ejection fraction checked
94% 71%
ACE-I if EF < 40% 93% 66%
Source: Jha et al., NEJM 2003
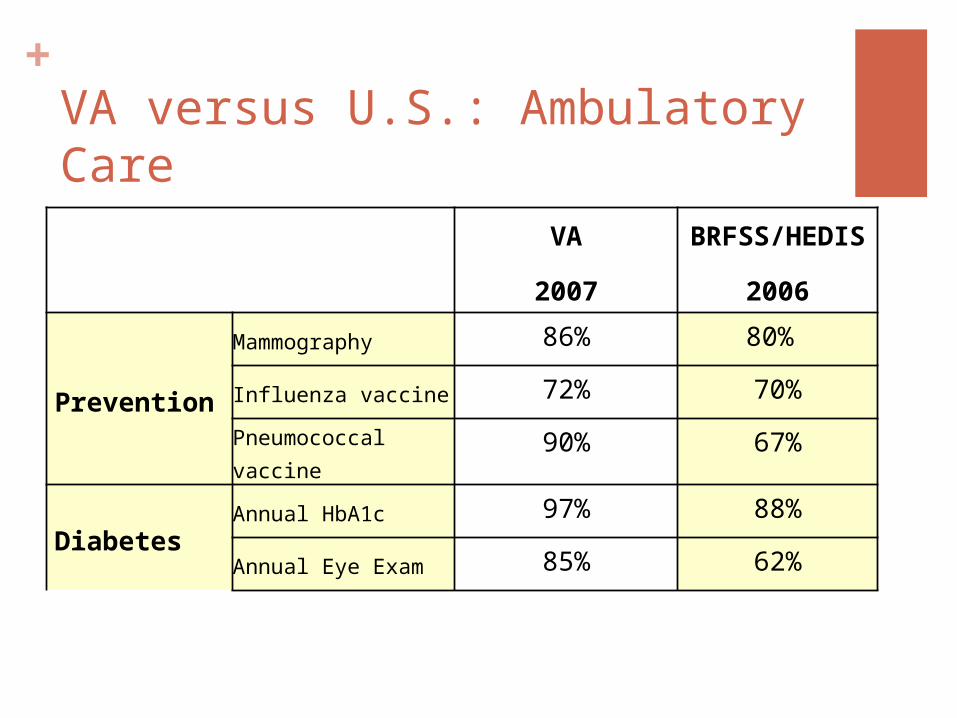
+VA versus U.S.: Ambulatory Care
VA
2007
BRFSS/HEDIS
2006
Prevention
Mammography 86% 80%
Influenza vaccine 72% 70%
Pneumococcal vaccine
90% 67%
DiabetesAnnual HbA1c 97% 88%
Annual Eye Exam 85% 62%
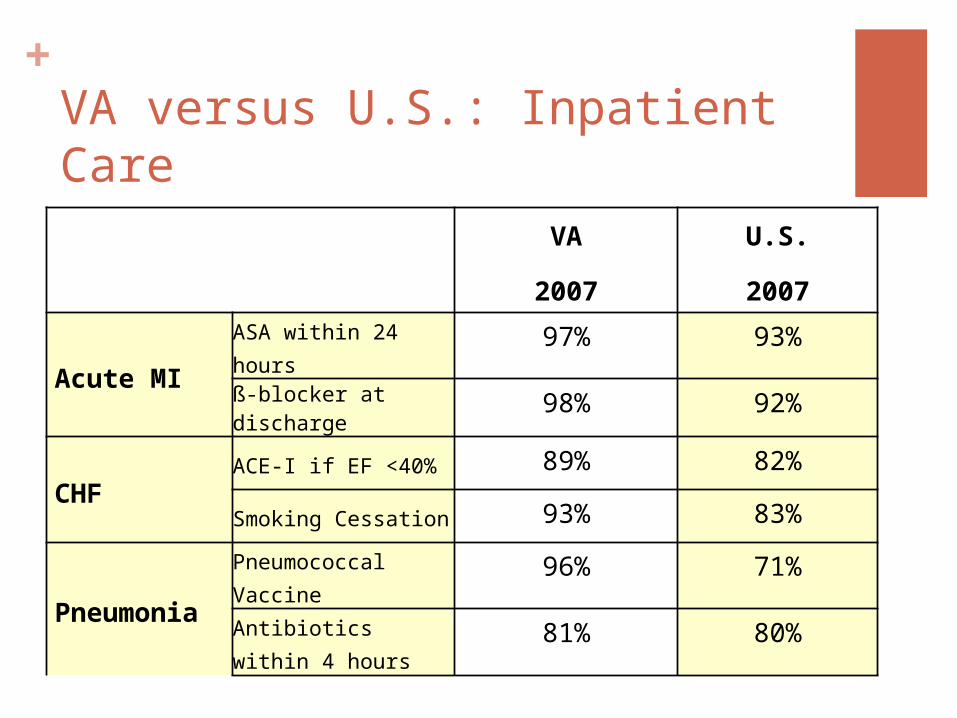
+VA versus U.S.: Inpatient Care
VA
2007
U.S.
2007
Acute MIASA within 24 hours 97% 93%
ß-blocker at discharge
98% 92%
CHFACE-I if EF <40% 89% 82%
Smoking Cessation 93% 83%
Pneumonia
Pneumococcal Vaccine
96% 71%
Antibiotics within 4 hours
81% 80%
+Lessons from the VA
Reform must encompass multiple actions at once
Any single activity likely inadequate
Focus on high value conditions, prevention, safety
Critical for ensuring patient trust in the system
Hold senior managers accountable
Focus on a robust information system
+And the VA declared victory….
“Best Care Anywhere”
“High quality VA is the model for the nation”
And so on
And yet….

+

+What went wrong?
Culture of satisfaction with success“Best Care Anywhere”
InsularityMost of the leadership from within the VA
+What went wrong?
If performance measurement works, then… Mid-1990s: 20-25 measures Mid-2000s: 150+ measures 2010: 250+ measures
Bureaucratic bloat: 2000: 800 central office staff 2012: 11,000 central office staff
+And the evidence was building
Anecodotes about PMs leading to bad care
Stories about data falsification
Concerns about transparency and openness
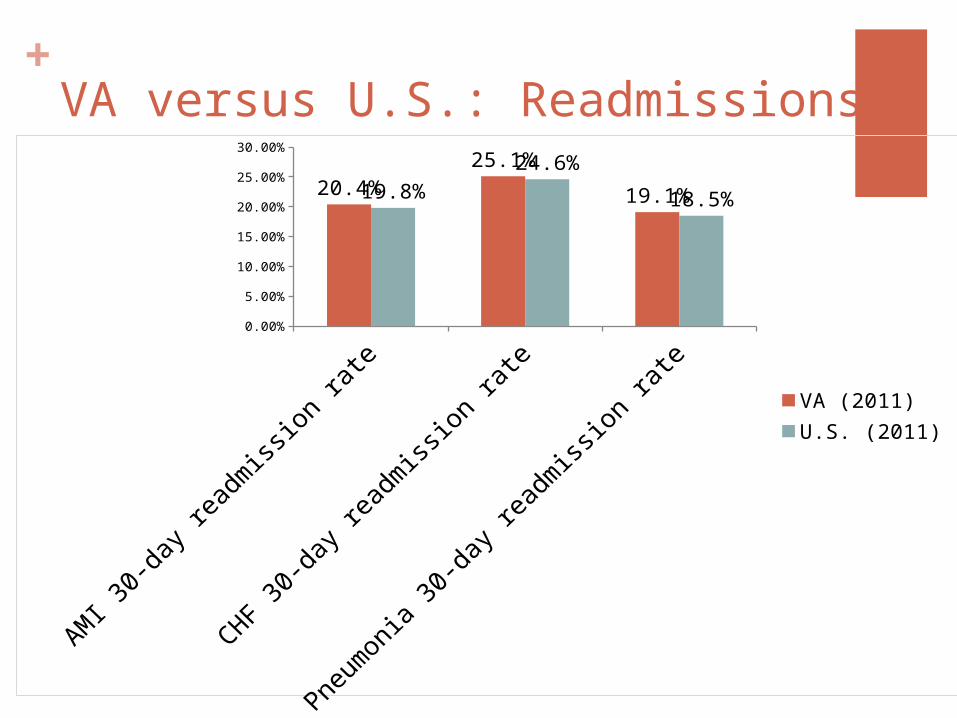
+VA versus U.S.: Readmissions
AMI 3
0-da
y re
adm
ission
rate
CHF 30
-day
read
miss
ion
rate
Pneu
mon
ia 3
0-da
y re
adm
ission
rate
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
20.4%25.1%
19.1%19.8%24.6%
18.5%
VA (2011)U.S. (2011)
+So what’s the big lesson?
+It isn’t about the what…but how
Performance measures are powerful But wrong measures can be a distraction
Incentives can change behavior, and culture critical But powerful incentives, in wrong culture, create
gaming
Information technology is an enabler IT can be manipulated and used to hide bad
actions
+How does the VA recover?
By placing competence over ideology
Focusing on what matters Limit the number of performance measures Focus on outputs, not inputs
Health of the population Be more creative with IT Focus less on # of doctors, nurses
Bring in more people from the outside
Openness and transparencySunshine is the best disinfectant
+Final thoughts
Reform is never a one step processOne is never done
Failures are part of the processIf you aren’t failing, you aren’t trying
Keep the eyes on the prize Focus on what matters And try to focus on only what matters
+The End
Thank you
Happy to take questions