Embed Size (px)
Citation preview


Problem of Pediatric Pain Myths/Misconceptions: Fact or Fallacy? Pain In Children’s Lives Assessment of Pain Pain Management Principles Procedural Pain Special Challenges: Neonates, Chronic
Pain, End of Life Leadership and Advocacy

Pain part of growing up Pain part of exploring the world Preschoolers during play experience an average on one
“owie” every 3 hours Children frequently fall in playgrounds, riding bikes Children often experience pain as a result of dental care Some children and adolescents struggle for years with
painful diseases and hospital treatments

Perpetuation of myths Lack of knowledge –pre professional,
professional, Lack of interprofessional collaboration Knowledge transfer challenges Challenge of pain assessment in
children Institutional barriers Everyone’s Problem Yet Nobody’s
Problem

Infants and young children do not experience pain like adults
Infants and young children will not have memory of painful experiences
Neonates do not feel pain like older children and adults due to immature nervous systems
Self report is always accurate in pediatric pain assessment
Narcotics (opioids) should be avoided in infants and children due to risk factors such as respiratory depression and addictions

Opioids should be avoided in adolescents due to the problem in society with substance abuse
The harmful effects of analgesics are more serious than the harmful effects of unrelieved pain
PRN (as needed) analgesics are more effective than scheduled analgesics
Parental presence usually results in a lack of cooperation by the child
Topical anesthetics such as EMLA or Ametopp make it more difficult to draw blood and perform procedures, such as IV insertion

Infants do not have the capacity to experience or remember pain
Infants are neurologically immature and therefore cannot conduct pain impulses.
Infants do not remember pain, because of cortical immaturity.
Sleeping infants are not experiencing pain
(Kuttner,2010; Twycross, A., Dowden, S., & Bruce, E. 2009)

Self report is gold standard in pain assessment“Pain is what the experiencing person says it
is, when and where it is…”Challenges with non-verbal individuals * rely on
physiological and behavioural measures (and the belief there is a reason for the pain!)
A number of validated and reliable non-verbal pain scales based on these measures: PIPP, NIPP, FLACC
(Kuttner, 2010; Twycross, A., Dowden, S., & Bruce, E. 2009)

Unrelieved pain in infants can result in long term developmental problems
Unrelieved pain in infants can permanently change their nervous system and may “prime” them for having chronic pain
(Kuttner,2010; Twycross, A., Dowden, S., & Bruce, E. 2009)


The anatomical, physiological and biochemical prerequisites for pain perception are present in early part of intrauterine life
Infants have larger receptive fields and possibly a higher concentration of substance P receptors (neurotransmitter related to sensation of pain)
Nonmyelinated transmission: lack of inhibitory neurotransmitters(Mathew & Mathew, 2003)

Respiratory (lungs)compromise Cardiovascular (heart) compromise Increased stress hormones Increased glucose secretion Slowing of gastrointestinal/genitourinary systems Poor nutritional state Muscle tension, spasm and fatigue Behavioural and psychological disturbances, PTSD Long term neurological effects Chronic pain syndromes(Kuttner,2010; Twycross, A., Dowden, S., & Bruce, E. 2009)

Acute illness Chronic Illness Unintentional injuries ex trauma Child abuse
*These children experience pain d/t disease, injury, treatments and procedures

Average 10-16 painful procedures per day and in some infants up to 300/week
40-90% receive no effective treatment
(Stevens et al., 2003)

Affects 15 -20 % of children and adolescents Reported as young as 3 years of age, however most
prevalent in early teens Can be part of a chronic medical condition, develop
following surgery, illness or injury or have no obvious cause
Despite the significant physical, psychological, social and economic impact on children and families, chronic pain is often under-recognized and undertreatedPhysical and psychological impact of chronic pain in school age children can impact overall health and persist throughout adolescents and adulthood
Children and teens with chronic pain have an increased incidence of anxiety and depression
(Stinson & Bruce, 2009; Kuttner, 2010)

“Chronic pain in children is the result of a dynamic integration of biological processes, psychological factors and socio-cultural context, considered within a developmental trajectory”(American Pain society Position Statement on Chronic Pain in Children, 2006)
Has no apparent protective purpose and often the consequence of damaged, abnormally functioning nerves
Despite the significant physical, psychological, social and economic impact on children and families, chronic pain is often under-recognized and undertreated(Stinson, 2009).

A child’s pain is to be believed and acknowledged
Pain is real, and children and adolescents are the true authorities on their pain
Treating children in pain requires a thorough understanding of the interaction of biological, psychological and social systems impacting the pain experience
(Kuttner, 2010)

“First do no harm” Understand developmental influences Be honest! Give choices when possible Involve parents and caregivers Take a pain history

Respect “safe places”ex. child’s bed, playroom
Choose the most appropriate analgesic, route and schedule
Observe and prevent side effects of analgesics
Use non-pharmacological methods Use a team approach

Studies show that children can give a reliable self report of pain as early as age 3 (Twycross, 2009; Kuttner, 2010)
Self report of pain is most reliable if the child is not overly distressed (Ibid.)
Self report of pain is more reliable when parental support is present (Ibid.)
A number of reliable and valid self report tools have been tested in children based on their developmental age and stages (Stinson, 2009; Kuttner, 2010)


Pain as the “5th Vital Sign”Pain scores: the concept of interpretability Clinical meaning must also be assessed: mild, mod or severe -treatment threshold, satisfaction with analgesia
(Stinson et al., 2006)

Practice in advance Use same tool for same child Evaluate at rest and with activity Document , including response to
interventions

Numerical Rating Scale (NRS) 0-10 Faces Pain Scale – Revised (FPS-R) 0 -
10 FLACC behavioural scale

Reprinted with permission

*reprinted with permission

Developmental stage Believe the pain is punishment Influence of parent/health care professional
(HCP) Adolescent sense of “imaginary audience” Longer hospital stay Fears of unknown, worsening pathology,
death, addictions, ‘drugs are bad’ Challenge of chronic pain – not identified by
child
(Kuttner,2010; Twycross, A., Dowden, S., & Bruce, E. 2009)

Variable Facial expression, body posture,
vocalization Child may sleep in presence of pain Children use distraction well Judgments can lead to poor pain
control

Face Legs Arms Cry Consolability (FLACC) 0-10
Neonatal/Infant Pain Scale (NIPS) Premature Infant Pain Scale (PIPP) Non-Communication Children’s Pain
Checklist (NCCPC) Parent’s Post-operative Pain Measure Pediatric Pain Profile


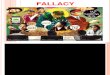
NASO-LABIAL FOLDdeepened

Facial expression of pain.

Cry of infant in pain is higher pitched, less melodious and more harsh
Only relevant in infants that vocalize cryNeonates and infants with ‘silent crying’ are not
taken into consideration(Wong et al, 2009)

When children are Limited English proficient (LEP), pain assessments must be conducted in the language the child is most familiar (Boyd, Bee & Johnson, 2009; Dowden, S., & Bruce, E. 2009
Twycross, 2010).
Children with developmental or communication disabilities are often under assessed and under treated for pain (Kuttner, 2010).

Children with neurological disorders such as cerebral palsy or autism may have difficulty expressing their pain in a way that others understand
In addition to communication barriers, these children often have multiple medical problems and often undergo multiple medical procedures(Stinson, 2009)

Behavioural cues:facial expression, moaning, screaming, sweating or flushing, changes in posture and movement,changes in sleep and eating, changes in mood and sociability
(Stinson, 2009)

Children in pain may regress to an earlier stage of development
A child’s experience of illness and hospitalization may change their perception of and ability to cope with pain
(Kuttner, 2010)

In summary, assessment of a child’s pain can be very challenging. Even with a multidimensional approach, there may be uncertainty about the presence and severity of pain, particularly in infants and young children.
When a child cannot or will not report pain, a high index of suspicion may be the most helpful assessment and a trial of analgesics is usually helpful for diagnosis
(McCaffery, 1996)

“The presences of a known and trusted adult makes the experience bearable for both children and adolescents in a myriad of obvious and subtle ways, and enables them to cope” (Kuttner, 2010, p. 75).
Both children and adolescents have reported that what has counted the most when having pain is having parents with them (Kuttner, 2010)
Teens may say they can handle it on their own but it is important to offer support until they are coping (Kuttner, 2010)

Prn (as need) versus scheduled analgesia Pre-emptive analgesia (in advance of
painful procedure) Choice of analgesic, dose range and
frequency Route of choice: considerations Proper dosing Prevention and management of side
effects

Acetaminophen –dosing, alternating, adjunctive
NSAIDS: Ibuprofen, Naprosyn, Ketorolac Codeine concern Meperidine (Demerol) not recommended Morphine “gold standard” Hydromorphone Other: ketamine, methadone, fentanyl
Twycross, A., Dowden, S., & Bruce, E. 2009

No longer recommended in children Weak opioid with ceiling effect Metabolized and converted to Morphine in
the body Ineffective in approximately 30% (poor
metabolizers) Approximately 5% ultra rapid
metabolizers –deaths have been reported Consider NSAID, low dose Morphine
Twycross, A., Dowden, S., & Bruce, E. 2009

Metobolite nor-meperidine accumulates in CNS and can cause neurotoxic effects (tremor, seizures, confusion, nervousness)
Can cause seizures in children after single dose
Rapidly accumulates Subsequent doses less effective Higher rates of side effects
Twycross, A., Dowden, S., & Bruce, E. 2009

Well known, well studied Mimics body’s endogenous opioids
“endorphins” Most frequently used opioid in moderate
to severe pain in pediatrics, but still underutilized
Standard by which other opioids are compared
Twycross, A., Dowden, S., & Bruce, E. 2009

Anesthetic agent with analgesic effects Uses: anesthesia, procedural sedation, analgesia In creased use as low dose infusion increasing
use in pediatric complex acute and cancer pain Opioid sparing; useful with kidney/liver
dysfunction Can be used solely or as co-analgesia Adverse effects: dysphoria , increased salivation
and agitation at higher doses
(Twycross, A., Dowden, S., & Bruce, E. 2009)

Antidepressants ex TCAs Anticonvulsants: ex. gabapentin, Clonidine, Dexmedetomidine Topicals ex lidocaine, NSAID
(Twycross, A., Dowden, S., & Bruce, E. 2009)

Addiction –psychological dependence on drugs with drug seeking and drug using behaviour
Physical dependence –physiological response to dose reduction or abrupt discontinuation of a drug leading to withdrawal symptoms
Tolerance –decreased effectiveness of a drug over time
Pseudoaddiction-drug seeking behaviour due to untreated pain
Twycross, A., Dowden, S., & Bruce, E. 2009

Do not withhold opioids Maintain patient opioid regime as baseline Opioid requirements are higher for acute
pain Often have less opioid side effects Adjuvant medications may help Assess and manage signs of withdrawal (Twycross & Dowden, 2009)

Placebos administered without patient consent are considered unethical
30 % population has placebo response “Physical “pain and “psychological “
pain cannot be separated
(Twycross, A., Dowden, S., & Bruce, E. 2009)

Parental Presence Distraction Relaxation Guided imagery TENS Biofeedback Heat/Cold Self-hypnosis
(Kuttner, 2010)

Consider conscious sedation, general anesthetic
Use topical anesthetics and/or sucrose Parental presence Positioning and restraint Respect safe places Pre and post therapeutic play –involve
parents and child life specialists Advocate!
Kuttner, 2010

Kangaroo care, Swaddling Sucrose Studies on extubation, respiratory
distress and pain Under 27 weeks gestation* work to be
done(Kuttner, 2010; Twycross, A., Dowden, S., & Bruce, E. 2009

Educate, dispel myths Evidence based practice/knowledge
translation Pain as “5th Vital Sign” Ethics /legalities Institutional strategies Unit strategies Pediatric Pain Champions Interprofessional Team work(Twycross, A., Dowden, S., & Bruce, E. 2009


Boyd, H., Bee, H. & Johnson, P. (2008). Lifespan Development. 3rd Canadian edition. Toronto: Pearson Education Dowden, S., McCarthy, M., & Chalkioadu, G. (2008). Achieving organizational change in Pediatric pain management. Pain Research Management 13 (4), 321-326.Kuttner, l. (2010). A child in pain: What Health Professionals can do to help. Bethel: Crown House PublishingStevens, B., Riahi, S., Cardoso, R., Ballantyne, M., Yamada, J., Beyere, J., Breau, L.Camfield, C., Finlay, G., Franck, L., Gibbons, S., Howlett, P., McKeever, P., O’Brien, K., & Ohlsson, A. The influence of
context on pain practices in the NICU: Perceptions of health care professionals. Qualitative Health Research 21 (6), 757 – 770.Stinson, J. (2009). Pain Assessment. In Twycross, A., Dowden, S. and Bruce, E. (eds). Managing Pain in Children: A clinical guide. West Sussex: Blackwell publishing Ltd. Taddio, A., Goldbach, M., Ipp, M., Stevens, B. (1995). Effect of neonatal circumcision on pain response during vaccination in boys. Lancet 345 (8945), 292 -292 .Twycross, A. ( 2009). Pain: a bio-psycho-social phenomenon. In Twycross, A., Dowden, S. and Bruce, E. (eds). Managing Pain in Children: A clinical guide. West Sussex: Blackwell publishing Ltd.