Embed Size (px)
Citation preview

© Pittsburgh Regional Health Initiative 2011 1
From Repair to Transformation: The Healthcare Quality Revolution
Karen Wolk Feinstein,PhDPres ident & Chief Executi ve Offi cer
I nve s ti n g i n H e a l t h C a re Q u a l i t y a n d Pa ti e n t S a fe t y
G ra n t m a ke rs I n H e a l t hJ u n e 1 3 , 2 0 1 1
Spreading Quality, Containing Costs.

© Pittsburgh Regional Health Initiative 2011 2
“A Think, Do, Train and Give Tank”
A public charity with two supporting organizations• Pittsburgh Regional Health Initiative (PRHI)• Health Careers Futures (HCF)

© Pittsburgh Regional Health Initiative 2011 3
Staff and Functions
Think Researchers Data analysts Communications,
media, writers Policy analysts Evaluators
Give Program officers Grant managers Fiscal agents for
HIV/AIDS funds Accounting
Do Program directors Event planners Trainers Grant writers Web designers Public relations
Train Curriculum developers Coaches and trainers
40+ Staff

© Pittsburgh Regional Health Initiative 2011 4
Phase One:1997 to 2001 Pre-IOM Reports

© Pittsburgh Regional Health Initiative 2011 5
What and Why: PRHI
Pittsburgh Regional Health Initiative (PRHI) A not-for-profit, regional, multi-stakeholder coalition
formed in 1997 An initiative of a business group, the Allegheny
Conference on Community Development
PRHI’s message Dramatic quality improvement (approaching zero
deficiencies) is the best cost-containment strategy for health care

© Pittsburgh Regional Health Initiative 2011 6
The Persistence ofMedical Errors in U.S.
Adapted from Milliman: The Economic Measurement of Medical Errors, June 2010
Error Type% of
Injuries that are Errors
Count of Errors (2008)
Total Cost per
Error
Total Cost of Error
(millions)
Pressure Ulcer (Medicare Never Event) >90% 374,964 $10,288 $3,858
Postoperative Infection >90% 252,695 $14,548 $3,676
Infection due to Central Venous Catheter >90% 7,062 $83,365 $589
Catheter - Associated Urinary Tract Infection (Medicare Never Event)
>90% 12,839 $26,793 $344
Object Left in Body (Medicare Never Event) >90% 11,690 $8,031 $94
Blood-Type Incompatibility (Medicare Never Event) >90% 6,350 $11,738 $75
Total Cost of all errors = $19.5 Billion per year

© Pittsburgh Regional Health Initiative 2011 7
Toyota/Lean Production Thinking: The Basics
Problems identified and solved Rapid root cause analysis Organized work areas Concise communication Active involvement of managers
“Go and see” On the floor
Intense respect for the employee: Every employee has what they need,
when they need it to succeed Career development
Team problem solving to meet customer need

© Pittsburgh Regional Health Initiative 2011 8
What We Observe in Health Care
W. Edwards Deming, PhD: “Where Art Thou?”
Chaos Uncertainty Random Behaviors Work-Arounds Confusion Disorder Errors High Turnover Secrecy

© Pittsburgh Regional Health Initiative 2011 9
PRHI’s Prescription for Transformation
Services That Add Value All Services Add Value
Preventable Complications
Unnecessary Treatments
Inefficiencies
Errors
100% Value
60% Value
40% Waste
NOW FUTURE

© Pittsburgh Regional Health Initiative 2011 10
The Journey: From Vision to Innovation
PPC for Systems Transformation
PPC for Organizational Transformation
PPC for Repairs
An Early Vision for Perfecting Care
A Method for Perfecting Patient CareSM (PPC)
Incr
easin
g Valu
e with
Each
Step
PPC in New Technologies and New Models

© Pittsburgh Regional Health Initiative 2011 11
Where Value Derives
THE PATIENT
• Outcomes of Care
• Efficiency of Care
• Zero Defects
Value begins at the front linewhere patients receive care

© Pittsburgh Regional Health Initiative 2011 12
Our Method: Perfecting Patient CareSM PRHI’s Unique Brand of Quality Improvement
Adapted from Lean Patient-focused systems redesign Can be applied in the
course of everyday work The ultimate goal is perfection
© Pittsburgh Regional Health Initiative 2011 13
Phase 2:2001 to 2008 QI in Acute Care

© Pittsburgh Regional Health Initiative 2011 14
A Defining Initiative:Reducing Hospital-Acquired Infections
30+ hospitals participating in PRHI’s community-wide infection control project reported an average 68 percent reduction in CLABs over four years Results varied among institutions The Power of Perfecting Patient CareSM:
one hospital virtually eradicated CLABs from its main intensive care units

© Pittsburgh Regional Health Initiative 2011 15
The Champion Role in Transformation
PPC empowers frontline staff…and more
Nurse Navigators
Nurse Managers
Team LeadersSalk Fellows
Patient Safety Fellows
Physician Champions
Clinical Pharmacists
Long-term Care Workers
Librarians
Hospital Trustees
Emergency Medical Technicians
Caregivers

© Pittsburgh Regional Health Initiative 2011 16
Perfecting Patient CareSM (PPC) Training
Where We’ve Taught

© Pittsburgh Regional Health Initiative 2011 17
68% Dropin CLABs in 34 regional hospitals
50% FewerReadmissionsw/ COPD focus
86% Reductionin medication errors
180 to Zero!Lost patient hours per month due to ambulance diversions
Efficiency Increased 100%
in pathology lab
17% Dropin pediatric clinic
wait times
100% Reductionin nurse turnover
50% Reductionin pap smear
sampling defects
>20% DeclineNosocomialC. difficileinfections
35 to Zero!defective charts
100% Compliancew/guidelines & aspirinuse in a diabetes clinic
PRHI Stories of Success in Acute Care
© Pittsburgh Regional Health Initiative 2011 18
Our Methods and Successes Have Attracted Attention

© Pittsburgh Regional Health Initiative 2011 19
Phase 3: 2009 and OnPost ACA: Managing
Complex Patients

© Pittsburgh Regional Health Initiative 2011 20
The Second Systems Vision: Transforming the Care of Complex Patients
Acro
ss C
are
Setti
ngs
Essential Services System Requirements
Care Mgt
Clinical Pharmacy
Patient Engagement
Health IT
QI Training
Payment Incentives
Collaboration and
Integration
Medication Reconciliation
Informed Activated
Discerning Consumers
Data to Treat,
Measure, Evaluate
Perfect Patient
Care
Rewardsfor
Collaboration
Hospice/Palliative
Long Term Care
Rehab
Hospital
Emergency Services
Specialty Care
Primary Care
Screening and Tx
Behavioral Health
© Pittsburgh Regional Health Initiative 2011 21#21
What is essential to ourvision for reducing
readmissions?
Care Management
Clinical Pharmacy
Patient Engagement
Behavioral Health
HIT QI Training
Isn’t reimbursed

© Pittsburgh Regional Health Initiative 2011 22
The Complex Patient
Who is frequently hospitalized?
Do you know your customer?
Are you meeting their need?

© Pittsburgh Regional Health Initiative 2011 23
Let the Data Guide Work
The Complex Patient
HIV/AIDS End of Life
Skilled Nursing
Chronic Disease(COPD)
Behavioral Health and Substance Abuse
Multiple ConditionsPRHI
CurrentProject

© Pittsburgh Regional Health Initiative 2011 24
The Solution Coordinates Transition Between Hospital and Community
Improvedpatient
education and
support*in the
community
Patienteducationto addresscauses of admission
COMMUNITYHOSPITAL
Patient uses inhaler properly, leading to
improved functioning
Patient is discharged WITH training in use of inhaler
MD gives patient prescription for inhaler, but no
training
Patient gets inhaler from
pharmacy, but no training
Patient fails to use inhaler properly, leading to
hospitalization
Patient is treated with
nebulizer during hospital
stay
Patient is discharged
without training in use
of inhaler
+ + +*Care Mgt
ClinicalPharmacy
PatientEngagement
BehavioralHealth
© Pittsburgh Regional Health Initiative 2011 25
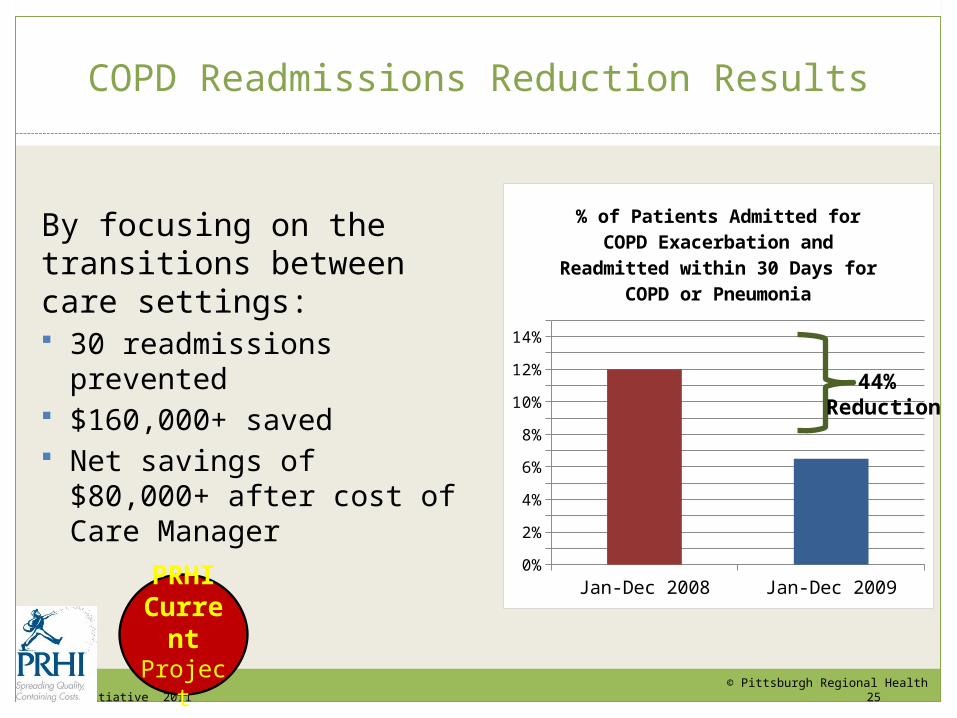
COPD Readmissions Reduction Results
By focusing on the transitions between care settings: 30 readmissions prevented $160,000+ saved Net savings of $80,000+ after
cost of Care Manager
Jan-Dec 2008 Jan-Dec 20090%1%2%3%4%5%6%7%8%9%
10%11%12%13%14%15%
% of Patients Admitted for COPD Exacerbation and Readmitted within
30 Days for COPD or Pneumonia
44% Reduction
PRHICurrentProject

© Pittsburgh Regional Health Initiative 2011 26
AHRQ Grant: Partners in Integrating Care
$3.5 million from AHRQ to disseminate and implement behavioral health services in primary care settings
© Jewish Healthcare Foundation, et.al. 26
PRHICurrentProject

© Pittsburgh Regional Health Initiative 2011 27
PRHI’s Accountable Care Network in Pittsburgh
PARTNERS
• Pittsburgh Regional Health Initiative
• Highmark
• Jefferson Regional Medical Center
• Monongahela Valley Hospital
CLINICAL SITES
• 2 Community Hospitals
• 24 Physician Practices
• 68 Physicians
FUNDERS
• Jewish Healthcare Foundation
• Governor’s Office of Healthcare Reform
• Highmark Foundation
• Richard K. Mellon Foundation
PRHICurrentProject

© Pittsburgh Regional Health Initiative 2011 28
“Closure” is a 5-year initiative approved by the JHF Board in 2008 to change expectations for end-of-life. Our goal is to empower consumers and healthcare professionals with easy-to-access, simple-to-understand information and resources to make educated decisions about end-of-life care
Closure / End of Life
PRHICurrentProject

© Pittsburgh Regional Health Initiative 2011 29
Reducing Preventable Hospitalizations:PPC in Skilled Nursing Facilities (SNFs)
6% of seniors in SNFs = 17+% of healthcare costs
20% of hospital patients discharged to a SNF were readmitted
51% of residents have one or more ER visits
38% have a hospitalizations: 41% are readmitted
Kaiser Family Foundation data
Long Term Care
Champions PRHICurrentProject

© Pittsburgh Regional Health Initiative 2011 30
Disruptive Innovations
1. Simple, less expensive, “upstream” innovations
2. Serve more with fewer features
Do not overshoot customer need
Show better understanding of customer need
© Pittsburgh Regional Health Initiative 2011 31#31
“Training dosage had most important effect on measures of success. A combination of PPC training, additional training, and coaching were associated with improved outcomes. Social networking or on-line technology can foster a virtual PPC community.”
- Donna O. Farley, PhD RAND: Results from the
Retrospective Evaluation Effects of PPC University Training
The Technology Innovation

© Pittsburgh Regional Health Initiative 2011 32
Tomorrow’s HealthCare™ Spreading & Sustaining Change
PRHICurrentProject

© Pittsburgh Regional Health Initiative 2011 33
Summary of Good Investments
Education, training, coaching
• Building an army of champions
Research on complex patients
Consumer engagement and
empowerment
Pilots• New Models of Care
• End of Life• Behavioral Health
Workforce — new roles for new workers
Disruptive Innovations:
• New Models, New Tools

© Pittsburgh Regional Health Initiative 2011 34
The Current Agenda
For the Patient, it is care that is kind, competent, customized, comprehensive, safe and efficient; addressing the needs of vulnerable populations, including:
Seniors (Caregiver Champions) and Long Term Care Champions
The poor (Safety Net Medical Home Initiative) The chronically ill (Accountable Care Network) Those who are approaching End-of-Life (Closure) Persons living with behavioral health problems (AHRQ grant),
and persons living with HIV/AIDS (Readmissions Reduction project)

© Pittsburgh Regional Health Initiative 2011 35
The Current Agenda (cont’d)
For the Healthcare Worker, it means that care is:
Informed and supported (Regional Extension & Assistance Center for HIT)
Incentivized (Robert Wood Johnson Foundation payment reform grant and the Fine Awards)
Prepared by training and coaching (Perfecting Patient CareSM, Tomorrow’s HealthCareTM, PPC University, Fellowships and Champions Programs)

© Pittsburgh Regional Health Initiative 2011 36
For Organizations and Systems, this focus includes:
Training, coaching and leadership development (Perfecting Patient CareSM)
Comprehensive improvement and education tools (Tomorrow’s HealthCareTM)
Transformations and new models of care (Patient Centered Medical Homes, Accountable Care Networks, Primary Care Resource Centers)
Payment Reform (Robert Wood Johnson Foundation payment reform grant and the website The Center for Healthcare Quality and Payment Reform— www.chqpr.org)
The Current Agenda (cont’d)