Embed Size (px)
Citation preview


Preface
Neurosurgical anesthesia
P.H. Petrozza
Guest Editor
Not long ago, discussions about neurosurgical anesthesia were dominated by
prerequisites of hyperventilation, a proscription concerning the use of inhaled
anesthetics, surgery guided by crude CT examinations and cerebral arteriography,
and patients placed in unusual positions. In reviewing many superb articles
submitted for this issue of the Anesthesiology Clinics of North America, I was
impressed by the great progress that has been made in both neurosurgery and the
anesthetic management of patients who require complex and technically difficult
procedures. As editor of this issue, my aim is to provide readers with practical
discussions of issues that are clearly relevant to the daily practice of neuro-
anesthesia. I solicited manuscripts from recognized leaders in the field who are
excellent lecturers and clinicians, and who have conducted much of their research
within their own laboratories.
Many topics are covered in this issue. Innovative monitoring technology
allows insight into the basics of cerebral blood flow and the effects of anesthetics
on the brain, while monitors of cerebral oxygenation allow characterization of the
physiologic milieu of cerebral tissue in individual patients during complex
anesthetics. Important issues in anesthetic practice are emphasized in discussions
on fluids, brain protection, and pediatric neurosurgery. The increasing scope of
neurosurgery is explored in articles on interventional neuroradiology, minimally
invasive neurosurgery, and spine surgery. Finally, vitally important elements of
perioperative critical care are explored in the articles on traumatic brain injury
and neurointensive care.
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (02 )00002 -0
Anesthesiology Clin N Am
20 (2002) xi–xii

I believe that readers of this issue of the Anesthesiology Clinics of North
America will not only be greatly enriched by the thoughtful discussions in this
issue, but will also become excited about recent developments within a field that
offers highly gratifying experiences to anesthesiologists, surgeons, and patients.
P.H. Petrozza
Department of Anesthesiology
Wake Forest University School of Medicine
Medical Center Boulevard
Winston-Salem, NC 27157-1009, USA
E-mail address: [email protected]
Preface / Anesthesiology Clin N Am 20 (2002) xi–xiixii

Cerebral blood flow and vascular physiology
Monica S. Vavilala, MD, Lorri A. Lee, MD,Arthur M. Lam, MD, FRCPC*
Department of Anesthesiology, Harborview Medical Center, Box 359724,
325 Ninth Avenue, Seattle, WA 98104, USA
Cerebrovascular anatomy
Arterial supply
The two common carotid arteries (anterior circulation) and the two vertebral
arteries (posterior circulation) supply blood to the anterior and posterior parts of
the brain respectively. In general (65–70% of patients), the common carotid
arteries originate from the innominate artery on the right side and from the aorta on
the left side. In adults, bifurcation of the common carotid artery into the internal
and external carotid arteries occurs usually at C4,5 compared to children in whom
bifurcation occurs one to two cervical levels rostral [1]. The internal carotid artery
(ICA) supplies the brain and the ipsilateral eye. There are four segments of the
ICA: cervical, petrous, cavernous, and supraclinoid, describing its course as it
enters the cranium. In general, the size of the area supplied by the artery
determines the diameter of the cerebral artery [2]. The ophthalmic, posterior
communicating, anterior choroidal, anterior cerebral, middle cerebral, and anterior
perforating arteries are all branches of the ICA, and provide most of the blood
supply to the cerebrum. All areas of the brain supplied by the main branches of the
ICA have good collateral circulation except the area supplied by the middle
cerebral artery (MCA). As a result, the MCA territory is prone to ischemia.
The two vertebral arteries and the basilar artery comprise the posterior
circulation. The vertebral arteries are the largest branches of the subclavian
artery, and before merging to form the basilar artery, the verterbral arteries give
rise to the anterior spinal and posterior inferior cerebellar arteries. Each anterior
spinal ramus originating from the vertebral artery merges with the opposite spinal
ramus to form the anterior spinal artery. The posterior inferior cerebellar artery is
the largest branch of the vertebral artery, and supplies the cerebellum and lower
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00012 -8
* Corresponding author.
E-mail address: [email protected] (A.M. Lam).
Anesthesiology Clin N Am
20 (2002) 247–264

brainstem. The basilar artery ascends ventral to the pons and terminates in the
pontomesencephalic junction. It gives rise to the anterior inferior cerebellar,
superior cerebellar, and posterior cerebral arteries. The posterior communicating
arteries (Pcom) connect the basilar artery to the carotid circulation.
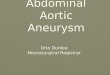
The Circle of Willis represents an anastomosis of the basal cerebral arteries
and the potential collateral circulation. (Fig. 1) This polygonal-shaped ring is
composed of the anterior communicating segments (Acom) of the anterior cere-
bral artery, and the ICA anteriorly. The posterior portion of the circle of Willis is
composed of the two Pcoms, and the two posterior cerebral arteries. However,
this classic pattern is found in less than 50% of the people; the Acom and Pcom
are frequently hypoplastic. While the main function of the Circle of Willis is to
provide collateral flow to the part of the brain with insufficient blood flow,
hypoplasia of the Acom or Pcom can be a limiting factor.
Venous drainage
The venous system of the brain consists of superficial and deep cerebral veins.
The superficial veins drain from the surface and the cortex of the cerebral
hemispheres, whereas the deep veins drain from the deep white matter, the basal
ganglia, the diencephalons, the cerebellum, and the brainstem. Large subepen-
dymal veins empty into the basal veins to form the great vein of Galen, which is
part of the deep venous system. Both superficial and deep veins including the
Fig. 1. The Circle of Willis showing the potential collaterals via the communicating arteries.
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264248

vein of Galen drain into the major dural venous sinuses, which, in addition to
receiving blood from the brain, also reabsorb cerebrospinal fluid from the
subarachnoid space. The walls of the cerebral veins are very thin while the walls
of the dural sinuses are fibrous. Both the veins and sinuses lack valves. The dural
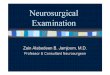
sinuses eventually drain into one of the two internal jugular veins. In most
individuals one of the internal jugular veins is dominant, usually the right one
[3] (Fig. 2).
Dural venous sinuses
The major venous sinuses are the superior sagittal sinus, inferior sagittal sinus,
sigmoid sinus, transverse sinus, straight sinus and cavernous sinus.
Superior sagittal sinus—this sinus lies in the attached margin of the falx
cerebri and receives numerous superficial cerebral veins. Where the falx joins the
tentorium cerebelli, the sinus turns laterally to become one of the transverse
sinuses, usually the right one.
Inferior sagittal sinus—this lies in the free margin of the falx cerebri and runs
posteriorly to join the straight sinus in the midline of the tentorium cerebelli.
Straight sinus—this sinus receives blood from the inferior sagittal sinus and
great cerebral vein that drains from deep parts of the brain. The straight sinus
usually turns left to become the left transverse sinus.
Fig. 2. Venous angiogram demonstrating the drainage from sagittal sinus into the two transverse
sinuses, which became the sigmoid sinuses. The final drainage is into the two internal jugular veins.
The jugular bulb is situated at the junction between the internal jugular vein and the sigmoid sinus.
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 249

Sigmoid sinuses—each sigmoid sinus lies in an S-shaped groove in the
petrous part of the temporal bone and in the occipital bone. The groove carries
the sinus downward to the posterior part of the jugular foramen, where it becomes
the internal jugular vein.
Cavernous sinuses—each cavernous sinus runs on either side of the sphenoid
bone between the dura of the middle cranial fossa and the periosteum covering
the bone. The two sinuses communicate with each other across the midline near
the pituitary where it is joined by the ophthalmic veins and the central retinal
veins. The superficial cerebral vein also drains into the roof of the sinus. Through
the foramen ovale, the sinuses communicate with the petrous sinuses. The
cavernous sinuses also communicate with the facial veins. Various nerves and
arteries also traverse through the cavernous sinus.
Basilar venous plexus—this plexus of veins lies on the clivus and provides
communication between the internal verterbral venous plexus and the veins and
venous sinuses in the cranial cavity.
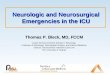
Normal cerebral blood flow and metabolism
Normal cerebral blood flow (CBF) is approximately 50 mL/100 g/min (see
Fig. 3). This represents the average blood flow for thewhole brain; blood flow to the
graymatter is higher at 80mL/100 g/min, whereas flow to thewhitematter averages
20 mL/100 g/min. The average brain receives about 14% of the cardiac output.
Cerebral metabolic rate for oxygen (CMRO2) averages about 3.2 mL/100 g/min,
Fig. 3. The major factors affecting the control of the cerebral circulation. The response of the change in
CBF to change in viscosity is not shown.
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264250

with the gray matter consuming approximately 6 mL/100 g/min and white matter
consuming about 2mL/100 g/min. Consequently, the normal arteriovenous oxygen
content difference is about 6.4 vol %, corresponding to a jugular bulb oxygen
saturation of between 65–70% in an individual with a normal hemoglobin
concentration. Glucose is the main energy substrate used by the brain except
during periods of starvation or hyperglycemia where ketones are used as an
alternative energy source. At rest, up to 92% of the adenosine triphosphate
(ATP) in the brain comes from oxidative metabolism of glucose. Lactate is also
consumed in very small quantities by the brain under normal circumstances.
However, there is little storage capacity for energy substrate in the brain, as
demonstrated by the fall in ATP levels to zero within 7 minutes after termination of
the oxygen supply. Therefore, the brain is dependent upon a constant supply of
oxygen (aerobic metabolism) and glucose (glycolysis) by the blood (perfusion).
The energy requirements for the brain can be compartmentalized to basal and
functional needs. Basal energy is required for maintenance of cell integrity with
electrochemical gradients; cellular transport of molecules; synthesis of proteins,
lipids, and carbohydrates; and the production, storage, release, and reuptake of
transmitters. Functional energy is expended in neuronal functioning including
generation of electrical activity by the pyramidal cells. About 40% of the energy
is used for basal needs, whereas functional activity consumes about 60%.
Measurement of cerebral blood flow
Numerous techniques are now available for monitoring of CBF, although most
are expensive, time-consuming, and seldom practical for routine clinical uses.
These methods can measure global, regional, or local CBF.
Global CBF
The Kety-Schmidt technique of nitrous oxide washing is considered to be the
gold standard for measurement of hemispheric blood flow [4]. Modifications and
adaptations of this technique include argon washing and 133xenon clearance. Re-
cently, a double indicator method to measure hemispheric CBF was introduced [5].
Regional CBF
Regional CBF can be determined using multiple detectors with 133xenon
clearance. Regional CBF can also be mapped with xenon CT. Single photon
emission CT provides relative qualitative information but not absolute CBF,
whereas positron emission tomography will measure absolute regional CBF.
Transcranial Doppler sonography
Transcranial Doppler (TCD) sonography measures CBF velocity in the basal
cerebral arteries. Although TCD is not a direct measure of CBF, changes in flow
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 251

velocity generally correlate well with changes in CBF, except under specific
circumstances such as vasospasm. Because it is noninvasive, it allows repetitive,
bedside measurement of relative changes in regional CBF. It is particularly suited
for the repetitive assessment of cerebral autoregulation [6].
Local CBF
The Laser Doppler measures local CBF in a tissue volume of 1 mm3.
Experimental methods include hydrogen clearance, radioactive or fluorescent
microspheres, and autoradiographic measurements, which are only applicable in
animal models.
Control of the cerebral circulation
The cerebral circulation is tightly regulated with a number of homeostatic
mechanisms (see Fig. 4). The major influence of the cerebral circulation are (1)
metabolism, (2) partial pressure of carbon dioxide (PaCO2), (3) partial pressure of
oxygen (PaO2,) (4) viscosity, and (5) blood pressure/cerebral perfusion pressure.
Fig. 4. (A) An autoregulatory test demonstrating absent cerebral autoregulation. (B) A similar test in a
patient with preserved cerebral autoregulation. MABP = mean arteriala blood pressure. Vmca = mean
middle cerebral artery flow velocity. Lt/Rt = left/right.
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264252

Flow–metabolism coupling
In the absence of pathology, CBF flow is tightly coupled to cerebral
metabolism. This occurs both at a global and regional level. During periods of
central nervous system activation, CBF increases to accommodate the rapid
increase in CMRO2 necessitated by the increased energy requirements for
synaptic transmission. Thus, activation of the occipital cortex with light stimu-
lation of the retina is immediately followed with an increase in flow in the
posterior cerebral arteries. Epileptic seizures are accompanied by an almost
instant increase in global CBF. Flow–metabolism coupling is perhaps the most
important control of the cerebral circulation. It is a robust mechanism that is
preserved during sleep [7–9] as well as during general anesthesia [10]. It can be
observed during the different stages of sleep where light or deep sleep is
associated with a 10% decline in CBF, and rapid-eye-movement (REM) sleep
has CBF similar to the awake state [7]. Flow–metabolism coupling can also be
observed during deep inhalation anesthesia, where regional changes in metabo-
lism are coupled with regional changes in flow [11]. Recent studies have
Fig. 4 (continued ).
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 253

demonstrated that the increase in CBF may transiently exceed the increase in
CMRO2 (luxury perfusion), and that the regulation of CBF during neuronal
activity is independent of local tissue levels of oxygen [12].
Mediators of flow–metabolism coupling
Adenosine and nitric oxide are two purported mediators of flow–metabolism
coupling. Adenosine causes increased cyclic AMP production that results in cere-
brovasodilation. Nitric oxide (NO) is an intercellular messenger in the peripheral
circulation and in the central nervous system, and causes vascular smooth muscle
relaxation and inhibition of platelet aggregation. Antagonists of both adenosine
and NO will attenuate the rise in CBF associated with neuronal activation,
although neither mediator antagonist alone, nor in combination, will completely
abolish the CBF increase in response to neuronal activation [13]. Therefore, other
mediators such as H + ions, adenine nucleotides, potassium, prostaglandins, and
vasoactive intestinal peptide, may also be involved in flow–metabolism coupling.
Both sympathetic and parasympathetic neurons may contribute to the neuro-
genic regulation of flow–metabolism coupling. In rats, stimulation of the
sympathetic system causes both increased CBF and CMRO2, while stimulation
of the parasympathetic system causes an increase in CBF only. Activation of the
central sympathetic system causes a much greater increase in CBF and CMRO2
than activation of the extrinsic sympathetic system that originates extracranially.
The role of the sympathetic system in regulation of CBF in humans remains
unknown, although it is thought that sympathetic stimulation shifts the autore-
gulatory curve to the right.
Temperature effects on flow–metabolism coupling
Hypothermia causes a reduction in CMRO2, thereby decreasing CBF via
flow–metabolism coupling. CBF decreases approximately 5% to 7% per degree
Centigrade. Reduction of the brain temperature to 15�C will reduce CMRO2 to
10% of normothermic values. Hypothermia causes a reduction in both the basal
metabolism required for maintenance of cellular integrity and the functional
metabolism of the CNS. Anesthetic agents affect only the functional component
of the CMRO2.
CO2 vasoreactivity
The cerebral circulation is exquisitely sensitive to changes in PaCO2. In
normal subjects CBF increases linearly by 2% to 4% per mmHg PaCO2 within
the range of 25 to 75 mmHg. This makes PaCO2 the most potent physiologic
cerebral vasodilator. The change in CBF occurs within seconds after PaCO2 is
changed, and complete equilibration occurs within 2 minutes [14]. The brisk
response of the cerebral vasculature to carbon dioxide (CO2) is caused by the
rapid diffusion of arterial CO2 across the blood–brain barrier (BBB) and into the
perivascular fluid and cerebral vascular smooth muscle cell. CO2 causes a
reduction in the perivascular pH, which leads to cerebral vasodilation and
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264254

increased CBF. Both CO2 and bicarbonate ions exert their effects on the
cerebrovasculature via changes in the extracellular fluid pH, and not by direct
action [15]. Although CO2 is a potent cerebral vasodilator, arterial H + ions do
not affect the cerebrovasculature because they do not readily diffuse across the
intact BBB, and therefore, cannot lower the perivascular pH of the cerebral
vessels. Consequently, metabolic acidosis and alkalosis do not affect cerebral
vascular tone, as do respiratory acidosis and alkalosis [16].
The changes in CBF associated with alterations of arterial CO2 are not
maintained for prolonged periods. During chronic hypercapnia maintained for
6 hours in dogs, Warner et al. [17] demonstrated an adaptive increase in the
cerebrospinal fluid (CSF) pH that was associated with a decrease in CBF. The pH
change was accompanied by an increase in the CSF bicarbonate ion. Similarly,
during chronic hypocapnia, the CSF pH gradually decreases toward baseline as
CSF bicarbonate concentration decreases and CBF increases [18].
Mechanism of CO2 vasoreactivity
The mechanism for CO2 vasoreactivity appears to be regulated by local
mediators, rather than by chemoreceptors in the periphery because their denerva-
tion does not alter the CBF response to changes in arterial CO2. The molecular
pathway by which perivascular pH influences cerebral vascular tone has not been
clearly defined. Frommice to humans, it has been demonstrated that NO is partially
responsible for CO2-mediated cerebral vasodilation. Schmetterer et al. [19]
demonstrated a significant reduction in mean flow velocity of the middle cerebral
artery to hypercapnia in healthy human volunteers after administration of an NO
synthase (NOS) inhibitor. However, NOS inhibitors do not completely ablate CO2
vasoreactivity, and NO may be more important in regional rather than global
regulation of vasoreactivity. The cerebral cortex in primates was the only site in
which NOS inhibitor attenuated the CBF response to increasing arterial CO2
concentration [20]. Site-specific responses indicate either the existence of more
than one pathway of CO2-mediated vasodilation, or that different regulatory
mechanisms occur at different locations. Moreover, CO2 vasoreactivity in neuronal
NOS knockout mice was found to be the same as in wild-type mice [21]. Other
putative mediators of CO2 vasoreactivity include prostaglandin E2 (PGE2) and
cyclic guanosine monophosphate. Indomethacin, an inhibitor of prostaglandin
production, causes potent attenuation of CO2 vasoreactivity, which is restored
upon addition of PGE2 [22].
Conditions that alter CO2 vasoreactivity
Global CO2 vasoreactivity is relatively robust, and is only abolished in brain-
damaged patients in terminal conditions. However, there are many conditions in
which it may be attenuated. Patients with severe carotid stenosis, head injury,
subarachnoid hemorrhage (SAH), cardiac failure, or severe hypotension, in which
the compensatory cerebral vascular response is already exhausted, may have a
decreased response to changes in CO2 compared to healthy subjects. Local loss or
decrease in response to CO2 in carotid stenosis has been demonstrated, and can
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 255

be used to predict the need for intraoperative shunting, and to predict which
patients with asymptomatic disease might benefit from surgery [23]. Similarly,
impaired CO2 vasoreactivity can be used to prognosticate in severe head-injury
patients [24]. Patients with aneurysmal SAH frequently demonstrate a reduced
response to hypocapnia, and may have absent response to hypercapnia when
vasospasm is present [25,26]. Cardiac failure patients demonstrated reduced CO2
vasoreactivity that was associated with reduced left ventricular ejection fraction
[27]. Hypercapnia, under these pathologic conditions, may induce cerebral
ischemia by causing vasodilation of unaffected regions of the brain and vessels,
and diverting blood flow away from the maximally dilated, diseased regions. This
phenomenon is known as cerebrovascular ‘‘steal.’’ Severe hypotension would
also maximally vasodilate the cerebral vasculature, and results in a temporary
loss of CO2 vasoreactivity [28]. The extent of attenuation of CO2 vasoreactivity is
probably influenced by the choice of hypotensive agent, because different
hypotensive agents demonstrate different reductions in CO2 vasoreactivity [29].
Hypothermia does not seem to affect CO2 vasoreactivity [30,31], but advancing
age ( > fourth decade) in the female gender is associated with a decline in CO2
responsiveness unless subjects are on hormone replacement therapy [32].
Hypoxemia-induced cerebral vasodilation
Compared to PaCO2, the influence of PaO2 on the cerebral circulation is mild
and of much less clinical significance. CBF generally does not increase appreciably
until PaO2 decreases below 60 mmHg, although one study reported a 23% increase
in CBF in humans when PaO2 was decreased from 100 to 65 mmHg [33]. The
response to hypoxemia is not as brisk as the response to changes in PaCO2, because
equilibration of CBF takes approximately 6 minutes after the establishment of
hypoxemia. On the other hand, the effect of hyperoxemia is less certain, as studies
have shown either a slight decrease in CBF velocity or no change at all [19,33].
Traystman et al. [34] demonstrated that the mechanism of hypoxemia-induced
vasoreactivity is not dependent upon baroreceptors or chemoreceptors in dogs.
Hypoxemia may induce cerebral vasodilation via anaerobic glycolysis and lactic
acid production causing decreased extracellular pH and subsequent vasodilation.
However, Koehler et al. [35] demonstrated that pH changes during hypoxemia
are only partially responsible for the increased CBF. Many studies have demon-
strated that release of adenosine is necessary for the vasodilatory response to
hypoxemia [36,37]. In animal models, adenosine activates large conductance cal-
cium-activated potassium channels and ATP-sensitive potassium channels that
contribute to vasodilation [38]. NO has also been implicated as a mediator, because
NOS inhibitors will reduce the increase in CBF, which occurs during hypoxemia
[39,40].
Effects of viscosity on CBF
Viscosity of blood is primarily a function of the hematocrit. Decrease in
viscosity is usually secondary to hemodilution, and CBF increases as a result of
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264256

the improved rheology of the blood flow in the cerebral vessels, as well as a
compensatory response to decreased oxygen delivery [41].
Blood pressure or cerebral perfusion pressure (cerebral autoregulation)
Normal flow, pressure, and resistance relationships
The relationship between flow and pressure can be simplistically described by
the equation
F ¼ P=R
where F = flow, P = pressure, and R = resistance. However, the cerebral
vascular bed is not rigid. Resistance to flow is dependent on the length of the
blood vessel, the viscosity of the fluid going through it, and the caliber of the
vessels. Thus, laminar flow through a cerebral vascular bed can be described by
the Poiseuille’s equation:
F ¼ ðpr4DPÞ=8gL
where F = flow, r = vessel radius, DP = pressure gradient, h = viscosity, and L =
length. Thus, resistance = (8 hL)/(pr) [4].However, the brain and its blood vessels are encased in the rigid cranium and,
therefore, subjected to the surrounding pressure (intracranial pressure—ICP). The
net cerebral perfusion pressure (CPP) is generally defined as the difference
between mean arterial blood pressure (MAP) and ICP. It should be noted that the
cerebral venous pressure at the junction between the cerebral veins and the dural
sinuses is usually slightly greater than ICP (necessary to allow venous flow).
When ICP is low but jugular venous pressure (JVP) is high, (e.g., when there is
venous obstruction at the neck), then CPP = MAP � JVP.
Under normal physiologic conditions, changes in MAP between 60 and
160 mmHg in the average individual produces little or no change in CBF [42].
This homeostatic mechanism of cerebral autoregulation with in vivo vaso-
constriction and vasodilation in response to changes in blood pressure was first
observed by Fog [43]. Cerebral autoregulation ensures that as MAP increases
there is increased resistance from a reduction in the caliber of the small cerebral
arteries and arterioles. This protects the cerebral arterioles and the brain from
elevation in MAP. This adaptive mechanism also maintains adequate CBF when
MAP or CPP decreases. Thus, cerebral arterioles dilate as MAP decreases, and
constrict as MAP increases. Beyond these limits of autoregulation, CBF is
directly proportional to MAP and can be described as pressure-dependent or
pressure-passive. There are some areas of the brain that are more at risk for
ischemia than others. The watershed areas between the anterior, middle, and
posterior cerebral arteries, as well as the areas between the superior and inferior
cerebellar arteries are particularly susceptible to ischemia as MAP decreases.
These regions have resting MAP that is lower compared to more proximal
territories supplied by the major arteries and are, therefore, the first ones to
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 257

reach a critical threshold when systemic MAP decreases. When MAP exceeds
150–160 mmHg, CBF begins to increase, and vessels may begin to leak with
extravasation of blood into the extravascular space. The MAP at which CBF
increases is termed ‘‘breakthrough’’ or the upper limit of cerebral autoregulation
[44]. Sudden decrease in CBF occurs at the other inflection point, or the lower
limit of autoregulation.
Mechanisms of autoregulation
The precise physiologic process accounting for cerebral autoregulation is
unknown, and may represent a combination of metabolic, myogenic, and neuro-
genic mechanisms.
The metabolic mechanism
This stipulates that autoregulation is mediated by the release of vasodilator
substance that regulates the cerebrovascular resistance to maintain CBF constant.
Although no specific substance fits all experimental observations, adenosine, a
potent cerebral vasodilator, formed from breakdown of ATP when neuronal
demand of oxygen exceeds supply is a prime candidate [45]. Adenosine can be
found in increased concentration in cerebral tissue as systemic blood pressure
falls towards the lower limit of autoregulation. In fact, brain adenosine concen-
tration doubles within 5 seconds of decreasing blood pressure [46]. Cortical
activation via contralateral peripheral stimulation is also immediately followed by
adenosine release and regional vasodilation [47]. It has been suggested that NO
exerts an influence on basal and stimuli-mediated cerebrovascular tone. The
mechanism of NO-induced cerebral vasodilation probably involves cyclic gua-
nosine monophosphate and a decrease in intracellular calcium. It is unclear to
what extent NO affects cerebral autoregulation in both healthy patients and in
patients with traumatic brain injury. Although earlier studies suggest that NO has
no influence on cerebral autoregulation, Jones et al. [48] recently described an
increase in the lower limit of autoregulation with NOS inhibitors. Other trans-
mitters/substances that have been proposed as mediators of autoregulation
include protein kinase C [48], melatonin [49], prostacyclin, activated potassium
channels, and intracellular second messengers [50].
The myogenic mechanism
This theory of pressure-dependent myogenic tone, first proposed by Bayliss in
1902, was not experimentally verified until approximately 50 years later. The
myogenic theory states that the basal tone of the vascular smooth muscle is
affected by change in perfusion or transmural pressure, and the muscle contracts
with increased MAP and relaxes with decreased MAP. Studies suggest that there
may be two myogenic mechanisms involved in cerebral autoregulation: a rapid
fast reaction to pressure pulsations, and a slower reaction to change in MAP. This
adaptive process appears to be initiated within the first 400 milliseconds (rapid
and rate-dependent response), and is probably completed in a few minutes by the
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264258

slower and rate independent component of the autoregulatory process. The
slower secondary component appears to be the dominant force in regulating
CBF. Autoregulation might also be invoked by incremental and nonpalatial
pressure. However, constant pressure elevation is probably not a sufficient stim-
ulus to maintain sustained vascular contraction. Some investigators believe the
myogenic mechanism sets the limits of autoregulation, whereas the metabolic
mediators are responsible for cerebral autoregulation itself.
The neurogenic mechanism
Perivascular innervation of the cerebral resistance vessels and the specific
neurotransmitter contained within the perivascular nerve fibers may also modu-
late vascular response to changes in blood pressure. However, the specific
mechanisms by which the central nervous system exerts control on the cerebral
vasculature are poorly understood. Although acetylcholine is the most abundant
perivascular neurotransmitter, the list of neurotransmitters involved in this neural
response includes norepinephrine, neuropeptide Y, cholecystokinin, acetylcho-
line, vasoactive intestinal peptide, and calcitonin gene-related peptide [51].
Experimentally sympathetic stimulation can shift the autoregulatory curve to
the right, thus protecting the brain against severe elevation of MAP.
Abnormal autoregulation
Autoregulation can become impaired or abolished by a variety of causes
including trauma, hypoxemia, hypercapnia, and high-dose volatile anesthetics.
Physiologically, hypercapnia (PaCO2>60 mmHg) will consistently impair cere-
bral autoregulation [52]. Clinically, the neurologic disorders where autoregulatory
impairment may contribute to the pathophysiology include ischemic cerebrovas-
cular disease, subarachnoid hemorrhage, and traumatic brain injury (TBI).
Abnormal autoregulation can range from minimal impairment to complete loss
and can be classified as ‘‘intact,’’ ‘‘impaired,’’ or ‘‘abolished.’’ However, auto-
regulation is not an all-or-none phenomenon, but rather represents a continuous
spectrum of adaptive response in cerebrovascular resistance to a change in
perfusion pressure. In patients with absent autoregulation, systemic hypertension
may lead to cerebral hemorrhage and edema formation, whereas a decrease in
blood pressure may turns areas with ischemia into areas of infarction. In patients
with subarachnoid hemorrhage with impaired autoregulation, induced hyperten-
sion may ameliorate ischemic deficits and improve outcome; thus, the risk of
increased cerebral edema and hemorrhage must be balanced against the benefits
of improved perfusion. Patients with TBI frequently suffer from cerebral
ischemia and loss of autoregulation, and a relatively high-maintenance MAP
may be indicated. Because the compensatory vasoconstriction mediated by the
autoregulatory response would result in a decrease in ICP, elevation of MAP may
be beneficial even in patients with preserved cerebral autoregulation. Moreover,
some TBI patients may have a rightward shift of the lower limit of autoregu-
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 259

lation, necessitating the maintenance of a higher MAP than normal (see below).
Documentation of the cerebral autoregulatory capacity would often facilitate
clinical management of these patients.
Limits of autoregulation
Although the limits of cerebral autoregulation are often stated as 60 and
160 mmHg, there is considerable variation in the limits among normal individ-
uals. Pathologically, these limits can be affected by a number of conditions. The
classic examples are chronic hypertension and traumatic brain injury. In chroni-
cally hypertensive adults, the autoregulatory curve is shifted to the right, and a
MAP >160 mmHg may not cause any increase in CBF. In patients with traumatic
brain injury, cerebral autoregulation may be impaired or abolished, or similarly
shifted to the right [53,54].
Autoregulation testing
Determination of autoregulation requires monitoring of CBF (see above) with
simultaneous change in MAP effected either spontaneously or provocatively, and
in the latter category, either pharmacologically or nonpharmacologically. The gold
standard is static testing, with measurement of CBF at two different levels of
steady-state MAP. With the advent of TCD monitoring, it is now possible to test
static autoregulation repetitively in the bedside. Because of the high temporal
resolution of TCD, it is also possible to test dynamic as well as static cerebral
autoregulation. Dynamic autoregulation is performed by monitoring the change in
CBF velocity in response to a transient decrease in MAP from sudden deflation of
bilateral thigh cuffs that have been inflated for a duration of 3 minutes [55]. The
autoregulatory index (ARI) is derived from a mathematical model, and reflects
how quickly middle cerebral artery flow velocity (Vmca) returns to baseline while
the MAP remains low (Appendix 1). An abnormal ARI reflects either a decreased
capacity of the autoregulatory response or an increased latency in the response. An
ARI derived from static autoregulation measurements quantifies the change in
cerebrovascular resistance (CVR) in response to change in MAP during steady
state without regard to latency (Appendix 2) [6]. The autoregulatory stimulus
during static testing often necessitates pharmacologic manipulation of blood
pressure. On the other hand, dynamic testing offers the advantage of quantifying
the speed of the response without use of any pharmacologic agents and tests the
response to hypotension instead of hypertension. Despite the fact that each testing
method may assess different aspects of the cerebral autoregulatory response, good
correlation between them have been demonstration under conditions of both intact
and impaired autoregulation [56].
Recently, the transient hyperemic response (monitored by TCD) from unilate-
ral carotid compression has been proposed as a test of cerebral autoregulation
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264260

[57]. However, the uncontrolled nature of the provocative stimulus makes this
unreliable, and is at best a semiquantitative test.
Conclusion
Remarkable progress has been made in the understanding of the control of the
cerebral circulation in health and disease states during the last 20 years. This is in
part due to the multidisciplinary basic science research and clinical research into
the mechanisms of regulation of CBF. In this article we have attempted to
describe aspects of CBF physiology relevant to the practicing anesthesiologist.
Anesthesiologists, in their daily practice, knowingly and unknowingly manipulate
and modulate the cerebral circulation. A thorough understanding should improve
patient care and outcome in those with neurologic disease.
Appendix 1
Dynamic cerebral autoregulation was calculated by the computer using the
following algorithm. The Autoregulation Index (ARI) is scaled 0–9.
DP = (MAP� cMAP)/cMAP�CCP)�x2 = x2 + (x1� 2D�x2)/f�T)x1 = x1+(dP� x2)/(f�T)mV = cVmca�(1 + dP� k�x2)dP = change in MAP due to cuff release
cMAP = baseline MAP value before cuff release
CCP = critical closing pressure (calculated by the computer)
x1 and x2 = variables that were assumed to be zero during the control period
D = damping factor
f = sampling rate
T = time constant
mV = mean velocity
cVmca = mean middle flow velocity before cuff deflation
K = autoregulatory dynamic gain
Appendix 2
The ARI scaled 0–1 using the static method of testing is calculated as follows:
ARI = % DeCVR/% DMAP
And e CVR = MAP/Vmca
ARI = Autoregulation Index
e CVR = estimated cerebrovascular resistance
MAP = mean arterial pressure
Vmca = middle cerebral artery flow velocity
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 261

References
[1] Day AL. Arterial distributions and variants in cerebral blood flow. In: Wood James H, editor.
Physiological and Clinical Aspects. New York: McGraw-Hill, Inc; 1987. p. 19–36.
[2] Lehrer HZ. Relative calibre of the cervical internal carotid artery. Normal variation with the
circle of Willis. Brain 1968;91:339–48.
[3] Streeter GL. The development of the venous sinuses of the dura mater in the human embryo. Am
J Anat 1915;18:145–78.
[4] Kety SS. Recent approaches to the measurement of cerebral blood flow and their underlying
principles. Res Publ Assoc Res Nerv Ment Dis 1966;41:226–36.
[5] Wietasch GJ, Mielck F, Scholz M, von Spiegel T, Stephan H, Hoeft A. Bedside assessment of
cerebral blood flow by double-indicator dilution technique. Anesthesiology 2000;92:367–75.
[6] Strebel S, Lam AM, Matta B, Mayberg TS, Aaslid R, Newell DW. Dynamic and static cerebral
autoregulation during isoflurane, desflurane, and propofol anesthesia. Anesthesiology 1995;83:
66–76.
[7] Madsen PL, Schmidt JF, Wildschiodtz G, Friberg L, Holm S, Vorstrup S, et al. Cerebral O2
metabolism and cerebral blood flow in humans during deep and rapid-eye-movement sleep. J
Appl Physiol 1991;70:2597–601.
[8] Lenzi P, Zoccoli G, Walker AM, Franzini C. Cerebral blood flow regulation in REM sleep: a
model for flow-metabolism coupling. Arch Ital Biol 1999;137:165–79.
[9] Lenzi P, Zoccoli G, Walker AM, Franzini C. Cerebral circulation in rem sleep: is oxygen a main
regulating factor? Sleep Res Online 2000;3:77–85.
[10] Lam AM, Matta BF, Mayberg TS, Strebel S. Change in cerebral blood flow velocity with onset
of EEG silence during inhalation anesthesia in humans: evidence of flow-metabolism coupling?
J Cereb Blood Flow Metab 1995;15:714–7.
[11] Hansen TD, Warner DS, Todd MM, Vust LJ. The role of cerebral metabolism in determining the
local cerebral blood flow effects of volatile anesthetics: evidence for persistent flow-metabolism
coupling. J Cereb Blood Flow Metab 1989;9:323–8.
[12] Mintun MA, Lundstrom BN, Snyder AZ, Viassenko AG, Shulman GL, Raichle ME. Blood flow
and oxygen delivery to human brain during functional activity: theoretical modeling and exper-
imental data. Proc Natl Acad Sci USA 2001;98:6859–64.
[13] Gotoh J, Kuang TY, Nakao Y, Cohen DM, Melzer P, Itoh Y, et al. Regional differences in
mechanisms of cerebral circulatory response to neuronal activation. Am J Physiol Heart Circ
Physiol 2001;280:H821–9.
[14] Severinghaus JW, Lassen N. Step hypocapnia to separate arterial from tissue PCO2 in the
regulation of cerebral blood flow. Circ Res 1967;20:272–8.
[15] Kontos HA, Raper AJ, Patterson JL. Analysis of vasoactivity of local pH, PCO2 and bicarbonate
on pial vessels. Stroke 1977;8:358–60.
[16] Harper A, Bell R. The effect of metabolic acidosis and alkalosis on the blood flow through the
cerebral cortex. J Neurol Neurosurg Psychiatry 1963;26:341–4.
[17] Warner DS, Turner DM, Kassell NF. Time-dependent effects of prolonged hypercapnia on
cerebrovascular parameters in dogs: acid-base chemistry. Stroke 1987;18:142–9.
[18] Muizelaar JP, van der Poel HG, Li ZC, Kontos HA, Levasseur JE. Pial arteriolar vessel diam-
eter and CO2 reactivity during prolonged hyperventilation in the rabbit. J Neurosurg 1988;69:
923–7.
[19] Schmetterer L, Findl O, Strenn K, Graselli U, Kastner J, Elchler HG, et al. Role of NO in the O2
and CO2 responsiveness of cerebral and ocular circulation in humans. Am J Physiol 1997;273:
R2005–12.
[20] McPherson RW, Kirsch JR, Ghaly RF, Traystman RJ. Effect of nitric oxide synthase inhibition
on the cerebral vascular response to hypercapnia in primates. Stroke 1995;26:682–7.
[21] Irikura K, Huang PL, Ma J, Lee WS, Dalkara T, Fishman MC, et al. Cerebrovascular alterations
in mice lacking neuronal nitric oxide synthase gene expression. Proc Natl Acad Sci USA 1995;
92:6823–7.
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264262

[22] Wagerle LC, Degiulio PA. Indomethacin-sensitive CO2 reactivity of cerebral arterioles is restored
by vasodilator prostaglandin. Am J Physiol 1994;266:H1332–8.
[23] Lam JM, Smielewski P, al-Rawi P, Griffiths P, Yu AL, Pickord JD, et al. Prediction of cerebral
ischaemia during carotid endarterectomy with preoperative CO2-reactivity studies and angiog-
raphy. Br J Neurosurg 2000;14:441–8.
[24] Schalen W, Messeter K, Nordstrom CH. Cerebral vasoreactivity and the prediction of outcome in
severe traumatic brain lesions. Acta Anaesthesiol Scand 1991;35:113–22.
[25] Dernbach PD, Little JR, Jones SC, Ebrahim ZY. Altered cerebral autoregulation and CO2
reactivity after aneurysmal subarachnoid hemorrhage. Neurosurgery 1988;22:822–6.
[26] Hassler W, Chioffi F. CO2 reactivity of cerebral vasospasm after aneurysmal subarachnoid
haemorrhage. Acta Neurochir 1989;98:167–75.
[27] Georgiadis D, Sievert M, Cencetti S, Unlmann F, Krivokuca M, Zierz S, et al. Cerebrovascular
reactivity is impaired in patients with cardiac failure. Eur Heart J 2000;21:407–13.
[28] Harper AM, Glass HI. Effect of alterations in the arterial carbon dioxide tension on the blood
flow through the cerebral cortex at normal and low arterial blood pressures. J Neurol Neurosurg
Psychiatry 1965;28:449–52.
[29] Matta BF, Lam AM, Mayberg TS, Eng CC, Strebel S. Cerebrovascular response to carbon diox-
ide during sodium nitroprusside- and isoflurane-induced hypotension. Br J Anaesth 1995;74:
296–300.
[30] Johnsson P, Messeter K, Ryding E, Kugelberg J, Stahl E. Cerebral vasoreactivity to carbon
dioxide during cardiopulmonary perfusion at normothermia and hypothermia. Ann Thorac Surg
1989;48:769–75.
[31] Irikura K, Miyasaka Y, Nagai S, Yuzawa I, Morii S, Fujii K. Moderate hypothermia reduces
hypotensive, but not hypercapnic vasodilation of pial arterioles in rats. J Cereb Blood Flow
Metab 1998;18:1294–7.
[32] Kastrup A, Dichgans J, Niemeier M, Schabet M. Changes of cerebrovascular CO2 reactivity
during normal aging. Stroke 1998;29:1311–4.
[33] Ellingsen I, Hauge A, Nicolaysen G, Thoresen M, Walloe L. Changes in human cerebral blood
flow due to step changes in PAO2 and PACO2. Acta Physiol Scand 1987;129:157–63.
[34] Traystman RJ, Fitzgerald RS. Cerebrovascular response to hypoxia in baroreceptor- and chemo-
receptor-denervated dogs. Am J Physiol 1981;241:H724–31.
[35] Koehler RC, Traystman RJ. Bicarbonate ion modulation of cerebral blood flow during hypoxia
and hypercapnia. Am J Physiol 1982;243:H33–40.
[36] DiGeronimo RJ, Gegg CA, Zuckerman SL. Adenosine depletion alters postictal hypoxic cerebral
vasodilation in the newborn pig. Am J Physiol 1998;274:H1495–501.
[37] Morii S, Ngai AC, Ko KR, Winn HR. Role of adenosine in regulation of cerebral blood flow:
effects of theophylline during normoxia and hypoxia. Am J Physiol 1987;253:H165–75.
[38] Brian JE Jr, Faraci FM, Heistad DD. Recent insights into the regulation of cerebral circulation.
Clin Exp Pharmacol Physiol 1996;23:449–57.
[39] Hudetz AG, Shen H, Kampine JP. Nitric oxide from neuronal NOS plays critical role in cerebral
capillary flow response to hypoxia. Am J Physiol 1998;274:H982–9.
[40] Berger C, von Kummer R. Does NO regulate the cerebral blood flow response in hypoxia? Acta
Neurol Scand 1998;97:118–25.
[41] Tomiyama Y, Jansen K, Brian JE Jr, Todd MM. Hemodilution, cerebral O2 delivery, and cerebral
blood flow: a study using hyperbaric oxygenation. Am J Physiol 1999;276:H1190–6.
[42] Paulson OB, Strandgaard S, Edvinsson L. Cerebral autoregulation. Cerebrovasc Brain Metab
Rev 1990;2:161–92.
[43] Fog M. Cerebral circulation: the reaction of the pial arteries to a fall in blood pressure. Arch
Neurol Psychiatry 1937;37:351–64.
[44] Strandgaard S, MacKenzie ET, Sengupta D, Rowan JO, Lassen NA, Harper AM. Upper limit of
autoregulation of cerebral blood flow in the baboon. Circ Res 1974;34:435–40.
[45] Winn HR, Morii S, Berne RM. The role of adenosine in autoregulation of cerebral blood flow.
Ann Biomed Eng 1985;13:321–8.
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264 263

[46] Winn HR, Welsh JE, Rubio R, Berne RM. Brain adenosine production in rat during sustained
alteration in systemic blood pressure. Am J Physiol 1980;239:H636–41.
[47] Ngai AC, Meno JR, Ko KR, Winn HR. Role of adenosine in cerebral vasodilator responses to
sciatic nerve stimulation. J Cereb Blood Flow Metab 1998;18:580–1.
[48] Jones SC, Radinsky CR, Furlan AJ, Chyatte D, Perez-Trepichio AD. Cortical NOS inhibition
raises the lower limit of cerebral blood flow-arterial pressure autoregulation. Am J Physiol 1999;
276:H1253–62.
[49] Regrigny O, Delagrange P, Scalbert E, Lartaud-Idjouadiene I, Atkinson J, Chillan JM. Effects of
melatonin on rat pial arteriolar diameter in vivo. Br J Pharmacol 1999;127:1666–70.
[50] Faraci FM, Heistad DD. Regulation of the cerebral circulation: role of endothelium and potas-
sium channels. Physiol Rev 1998;78:53–97.
[51] Morillo CA, Ellenbogen KA, Fernando Pava L. Pathophysiologic basis for vasodepressor syn-
cope. Cardiol Clin 1997;15:233–49.
[52] McCulloch TJ, Visco E, Lam AM. Graded hypercapnia and cerebral autoregulation during
sevoflurane or propofol anesthesia. Anesthesiology 2000;93:1205–9.
[53] Junger EC, Newell DW, Grant GA, Avellino AM, Ghatan S, Douville CM, et al. Cerebral
autoregulation following minor head injury. J Neurosurg 1997;86:425–32.
[54] Sahuquillo J, Munar F, Baguena M, Poca MA, Pedraza S, Rodriguez-Baeza A. Evaluation of
cerebrovascular CO2-reactivity and autoregulation in patients with post-traumatic diffuse brain
swelling (diffuse injury III). Acta Neurochir 1998;(vol. 71):233–6.
[55] Aaslid R, Lindegaard KF, Sorteberg W, Nornes H. Cerebral autoregulation dynamics in humans.
Stroke 1989;20:45–52.
[56] Tiecks FP, Lam AM, Aaslid R, Newell DW. Comparison of static and dynamic cerebral autor-
egulation measurements. Stroke 1995;26:1014–9.
[57] Tibble RK, Girling KJ, Mahajan RP. A comparison of the transient hyperemic response test and
the static autoregulation test to assess graded impairment in cerebral autoregulation during
propofol, desflurane, and nitrous oxide anesthesia. Anesth Analg 2001;93:171–6.
M.S. Vavilala et al / Anesthesiology Clin N Am 20 (2002) 247–264264

Anesthetics and the brain
Tod B. Sloan, MD, PhD, MBADepartment of Anesthesiology, 7838 University of Texas Health Science Center,
7703 Floyd Curl Dr., San Antonio, TX 78229, USA
Site of action of anesthetic agents
The method by which general anesthesia is produced remains unclear.
Obscuring the search for a common method for production of anesthesia is the
observation that anesthetics comprise a wide variety of chemical structures
without any apparent common mechanism of action. The common trait of these
drugs, lipophilicity, and the lack of a specific antagonist for general anesthesia
further suggest that no one specific receptor is involved in the process. However,
all of the drugs do appear to produce an alteration of neuronal excitability either
through depression of synaptic function or axonal conduction. Because synaptic
function appears more sensitive to anesthetics than does axonal conduction, a
strong focus of research has examined the effects of anesthetic agents on the key
determinants of synaptic function [1].
Because of the importance of ion channels in synaptic transmission, they have
been considered a potential target for anesthetic-induced depression of synaptic
function. These channels can be opened or closed by direct action of drugs at
receptors, by action on the molecule through changes in the protein–lipid milieu
around it in the cell membrane, or secondarily through intermediary messengers
from other receptors affected by the anesthetics (such as guanosine nucleotide
binding protein–G-protein) [2,3].
Because of the lipophility of anesthetic drugs, substantial research has focused
on anesthetic-induced changes in the fluidity of the plasma membrane that may
alter receptor and ion channel function. This mechanism may be particularly
important for the inhalational anesthetic agents where specific receptor inter-
actions are lacking (unlike the intravenous anesthetic agents, where many
receptor interactions are known). Such changes in membrane fluidity leading
to membrane protein changes have been demonstrated in the Na/K ATP’ase
membrane protein [4] and the nicotinic acetylcholine receptor [5], supporting the
possibility for this mechanism of anesthetic action. However, as a sole mech-
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00002 -5
E-mail address: [email protected] (T.B. Sloan).
Anesthesiology Clin N Am
20 (2002) 265–292

anism of anesthetic action, this effect may not be sufficient to explain all the
effects leading to anesthesia.
Evidence suggests that the inhalational agents may exert effects by more
specific mechanisms than changes in membrane fluidity. Inhalational agents have
low-affinity binding sites on some proteins, and these may contribute to conforma-
tional or functional shifts in protein action. It is also possible that these agents
occupy pockets, patches, or cavities that result from folding or interfacial (protein–
protein or lipid–protein) contacts and alter the normal noncovalent binding sites,
resulting in a conformational shift that changes function. If these proteins control
the electrochemical functioning of a neuron, then depression or enhancement of
function could result. In contrast to the inhalational agents, the intravenous
anesthetic agents appear to have specific interactions with membrane receptors.
Molecular action of anesthetics
Studies have examined the interactions of anesthetic agents with several
receptors and ion channels. In general, differences between inhalational and
intravenous agents have been observed. Perhaps the best evidence for specific
mechanisms of anesthetic action comes from the study of the major inhibitory
(gama amino butyric acid) and major excitatory (glutamate) synaptic systems in
the central nervous system (CNS).
Gama amino butyric acid (GABA) receptors
As the main inhibitory neurotransmitter in the CNS, GABA is a prime candidate
for participating in anesthetic-induced neuronal depression. Two major receptor
types are known. The ionotropic GABAa receptor is expressed in virtually every
neuron in the CNS and gates an ion channel. The GABAb receptor is a
metabotropic receptor that activates a series of intracellular events when activated.
Several anesthetic agents have prominent effects at the GABAa receptor.
When this receptor is activated, a chloride channel is opened, resulting in an
inhibitory effect on the cell. Receptor activation also causes enhancement of
potassium conductance and depression of calcium conductance via a G-protein
coupling system. Because specific binding sites have been shown on the GABAa
receptor for barbiturates, etomidate, althesin, propofol, and benzodiazepines, the
GABA receptor may play an important role in anesthesia produced by these
agents (Fig. 1) [6]. Although specific binding sites have not been identified,
volatile anesthetic agents do appear to modulate GABAa receptor function,
specifically enhancing GABA and benzodiazepine binding [7], resulting in
neuronal depression.
The glutamate receptor
The synaptic receptors that respond to glutamate are the principle fast ex-
citatory neurotransmitter system of the CNS and may also participate in the an-
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292266

esthetic state. These receptors are divided into three classes based on the binding
of N-methyl-D-aspartate (NMDA), a-amino-3-hydroxy-5-methyl-isoxazole pro-
pionic acid (AMPA), and kainate. These receptors are also believed to be
involved in learning, memory, motor coordination, neurotoxicity, and neuro-
degenerative disorders. The NMDA class has been studied extensively, and is
strongly voltage dependent due to a block by Mg2 + ions at negative membrane
potential [8]. When stimulated, calcium enters into the cell setting off a cascade
of events. AMPA and kainate receptors are believed to mediate the majority of
fast excitatory synaptic transmission in the brain, and inhibition would likely
cause profound changes in excitability of the brain.
The NMDA receptor probably plays a role in anesthesia because its antago-
nists (e.g., ketamine) produces a state of dissociative anesthesia (Fig. 2) [9,10].
When the receptor is at normal resting membrane potential, magnesium blocks
the calcium channel. When activated, the cell is depolarized, the magnesium
block is relieved, and calcium entry is permitted. This may be the predominant
site of action for ketamine in producing anesthesia. The evidence suggests a use-
dependent blockade; the anesthetic molecule enters the open channel, binds, and
then is trapped as the channel closes. Studies have shown that ketamine inhibits
NMDA receptor-mediated neurotransmitter release (e.g., regional effects involv-
ing acetylcholine, dopamine, GABA, norepinephrine [11–13]), as well as affect-
ing sodium flux and intracellular calcium levels [14].
Fig. 1. Depiction of GABAa receptor and hypothetical binding sites for several anesthetic agents.
(Reprinted from DeLorey TM, Olsen RW. GABA and glycine. In: Siegel GJ, et al, editors. Basic
neurochemistry: molecular, cellular, and medical aspects. 5th ed. New York: Raven Press; 1994.
p. 389–99; with permission.)
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 267

Ketamine may be unique among intravenous anesthetics in that it produces its
anesthetic effect by a mechanism not involving the GABA receptor. This may
account for the production of the anesthetic state called ‘‘dissociative’’ anesthesia
where, rather than general electroencephalographic (EEG) depression, there is
EEG evidence of dissociation between the thalamocortical and limbic systems
[15]. In this state, the thalamus and cortex exhibit synchronous delta bursts while
the ventral hippocampus and amygdala exhibit theta waves characteristic of
arousal. The anesthetic state produced, rather than an unresponsive sleep state, is
a cataleptic-like state of unresponsiveness with occasional purposeful move-
ments. There is intense analgesia, amnesia, and occasional hallucinations. Keta-
mine also appears to interact with mu and kappa opioid receptors, but because the
anesthetic state is not reversed by naloxone, the primary anesthetic effect is
probably via the NMDA mechanism.
A variety of evidence suggests that barbiturates also interact with the NMDA
receptor. Evidence suggests that they upregulate the receptor [16], and that they
may interact competitively with some of the binding sites [17]. However, the
exact role of this receptor in the production of anesthesia from barbiturates
remains unclear. With respect to inhalational agents, modulation of the NMDA
receptor is known to alter the potency of inhalational agents [18]. Studies have
also shown that inhalational agents inhibit the NMDA and AMPA/kainate
receptors [19–21]. Evidence suggests that the site of action may be near the
Fig. 2. Depiction of NMDA receptor and hypothetical binding sites for several anesthetic agents
including ketamine (Ket). (Reprinted with permission in adapted form from Peoples and Weight,
1998 [10]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292268

hydrophobic regions of the receptor near or in the plasma membrane. Alcohol
may play a role in NMDA receptor changes in a similar way.
Other receptors and ion channels
We have seen that anesthetic agents interact with the GABA and glutamate
receptors, thereby altering the balance of inhibitory and excitatory influences in
the nervous system. However, anesthetic agents also have effects on other ion
pores and receptor types, suggesting that other systems may play a role in the
neural state characteristic of anesthesia.
In the neural system, calcium channels play a role in the release of synaptic
transmitters via excitation–secretion coupling. Anesthetics could participate in
the depression of presynaptic release of neurotransmitters, thereby depressing
synaptic function through these calcium dependant processes. The effect of
anesthetic agents (volatile as well as intravenous) leading to the depression of
calcium channels in cardiac tissue is well described [22]. Similar effects have
been shown in sensory neurons. However, a clear connection with production of
the anesthetic state has yet to be proven.
The potassium channels represent a diverse set of channels involved in
maintenance of the resting membrane potential, repolarization after depolariza-
tion, reduction of the frequency of spikes during repetitive firing, and termination
of firing after a period of marked activity. Within the nervous system an increase
in potassium conductance has been associated with central a2 agonists, and with
m and d opioid receptor agonists [23–25]. This change is said to ‘‘stabilize’’ the
neuronal membrane because it hyperpolarizes it, making it less excitable. This
system could play a role in the anesthetic effects of opioids and central a2
agonists; however, further study will be needed to characterize the specific role
fully. The role of inhalational agents with potassium channels is still unclear.
The nicotinic acetylcholine receptor is a ligand-gated ion channel on the
postsynaptic membrane. It is found at the neuromuscular junction and in the
peripheral and CNS. Acetylcholine is released at the presynaptic membrane and
activates the synapse to receptors on the postsynaptic membrane. This action
opens sodium channels activating the postsynaptic membrane. The subsequent
depolarization then starts intracellular calcium-dependent muscle contraction.
Consistent with the known muscle relaxant properties of inhalational agents, the
volatile anesthetics interact with this receptor. Although this may occur at a
known hydrophobic site [26], it is not known whether the effect is by binding
within the channel pore or by inducing a conformational change in the receptor
by binding at a specific allerosteric site. This receptor is also the likely target for
the action of neuromuscular blocking agents.
The opioid receptors are a part of the G-protein coupling system. In this
system, the receptors (m, k, and d) are activated by their agonists, resulting in
depression of the cell by increasing the inward K + current and depressing the
outward Na + current via a G-protein mechanism linking the receptors to the ion
channels. Recetor activation also causes several other intracellular actions (Fig. 3)
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 269

[27]. Most opioid analgesics produce their effects via the m1 receptor while the
two other m receptor types mediate other effects. This mechanism is distinct from
the mechanisms of action of the volatile and other intravenous anesthetic agents.
Therefore, this may explain the fact that the net effect is different (e.g., analgesia
rather than anesthesia).
Fig. 3. Opioid receptor transduction mechansisms. Once activated by an opioid, G-proteins mediate
alterations in Na+ and K+ conductance and several intracellular processes. (Reprinted from Nestler EJ,
Aghajanian GK. Molecular and cellular basis of addiction. Science 1997;278:58–63. Copyright 1997
American Association for the Advancement of Science; with permission.)
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292270

The effect of local anesthesia on axonal conduction by interaction with
sodium channels is an excellent example of anesthetic-induced neuronal
depression. Both the charged and uncharged forms of the local anesthetic
molecule have blocking properties. Charged molecules, by virtue of their water
solubility, are restricted to blocking the channel by entering an open pore and
occluding the channel. The uncharged form, by virtue of its lipid solubility, can
enter the lipid membrane and interact with a site on the lipid–protein interface.
The interaction of lidocaine with the sodium channel is depicted in Fig. 4 [28].
The interference with the sodium channel is likely the major site of effect of
lidocaine on axonal conduction.
Fig. 4. Mechanism of Lidocaine action at binding sites within the plasma membrane. (Reprinted from
Hardman JG, Limbird LE. Goodman and Gilman’s the pharmacologic basis of therapeutics, 9th ed.
New York: McGrawHill; 1996; with permission of the McGraw-Hill Companies.)
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 271

Because of the numerous effects of anesthetic agents on various synaptic
receptors and ion channels, it is likely that general anesthesia and sedation are a
consequence of hyperpolarization of neurons and/or depression of excitatory
transmission (increasing K+ or Cl� currents or depressing Na+ or Ca+ currents).
Clearly, a large number of different mechanisms (axonal, pre- and postsynaptic)
and different CNS locations have been implicated such that one unifying
mechanism is not apparent. Studies in the hippocampus suggest several possible
mechanisms including: (1) depression of excitatory synaptic transmitter release,
(2) depression of action potential discharge in small diameter axons, (3) en-
hancement of presynaptic fiber discharge in GABA synapses, (4) depression of
postsynaptic responses to glutamate, (5) enhancement of GABA-mediated inhib-
itory transmission by presynaptic mechanisms, and (6) enhancement of postsy-
naptic responses to GABA [29]. Hence, anesthesia may be a change in the
balance of excitatory (especially glutamate), inhibitory (especially GABA), and
other neuronal or synaptic systems in brain structures with no single receptor or
ion channel playing the key role for all anesthetic drugs.
CNS site of action for anesthetic drugs
The CNS structure affected by anesthetics that has received the most
attention is the reticular activating system of the brainstem (RAS), in which
several neuronal systems interact with sensory pathways to the brain and
several mechanisms of arousal originate. However, gross lesions in this system
that result in major EEG disruptions can leave animals behaviorally awake [30].
Similarly, studies of this area show that anesthetics may or may not depress the
RAS activity [8,31,32]. Therefore, it is highly likely that general anesthesia also
involves an effect above the brainstem, such as a bilateral cerebral cortical
effect. Perhaps several types of regional disruptions can result in general
anesthesia [33], and no one neural structure plays the major role with all anes-
thetic drugs.
It is unclear from their mechanism of action whether drugs resulting in
increased depression or excitation of neurons and synapses may be advantageous
in different pathophysiological states. Given the increased cerebral blood flow
(CBF) associated with ketamine (see below) and the reduction in metabolism
associated with depressant agents, it would appear that preservation of a state of
reduced energy metabolism by depression would increase the margin of safety
during potential ischemia. Because the depressant effects may be regionally
specific (depending on the specific neural pathways involved), the possibility
exists that advancements in our knowledge will lead us to conclude that certain
pathophysiologic conditions may prompt certain anesthetics. For example, the
prominent anticonvulsant actions for the GABA related drugs (e.g., benzodiaze-
pines) suggest that these medications may be advantageous when EEG suppres-
sion is desirable (e.g., routine craniotomy with a seizure focus), but may be
detrimental when EEG activity must be preserved (e.g., electrocotigraphy).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292272

The major implications of these anesthetic drug actions is that our knowledge
remains vague about defining the specific actions of anesthetic drugs and the
anesthetic state. There is insufficient knowledge about the regional action of
drugs, making it difficult to recommend preferential agents when specific
regional pathology exists. Certainly advancements in knowledge of mechanisms
of drug action will lead to a refinement of our understanding the anesthetic state,
the specific interaction of drugs and pathophysiology, and the design of future
anesthetic agents.
Effect of anesthetic agents on cerebral physiology
The effects of anesthetic drugs on cerebral physiology can also be viewed as
effects on cerebral metabolism and blood flow. In general, CBF, cerebral
metabolic rate (CMR), and alterations in vascular tone are interdependent such
that alterations in one (by anesthesia or other effects) can alter the others. In
Fig. 5. Data of CBF showing the relationship of CBF to CPP in isoflurane anesthetized dogs.
(Reprinted with permission from McPherson and Traystman, 1988 [68]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 273

general, anesthetic agents are thought to affect cerebral vascular physiology by
(1) direct effects on the cerebral vasculature, (2) effects on cellular metabolism,
and (3) uncoupling or changing the relationship between CBF or cerebrospinal
fluid pressure (CSFP) and the normal physiological control mechanisms [34].
Because synaptic activity accounts for 40–60% of the normal resting metabolic
activity of the cells, the relationship of metabolism and anesthetic action is
dependent on the mechanism of action discussed in the previous section. In
general, it is thought that an decrease in CMR will cause a decrease in CBF
(coupling) and result in an decrease in CBV with a subsequent decrease in
intracranial pressure (ICP).
Anesthetics have a direct effect on blood vessels (e.g., vasodilation) and
autoregulation. Shown in Figs. 5 and 6 is the effect of anesthetic action on
autoregulation [35,36]. It is likely that endothelial relaxing factor (nitric oxide)
plays a role in the regulation of vascular tone and the interaction of inhalational
Fig. 6. Idealized graph of inhalational anesthetic-induced changes in autoregulation at different
dosages. (Reprinted from Donegan J. Effect of anesthesia on cerebral physiology and metabolism In:
Newfield P, et al, editors. Neuroanesthesia: handbook of clinical and physiologic essentials. 2nd ed.
Boston: Little Brown and Co; 1991. p. 17–30; with permission.)
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292274

agents. A second mechanism of action of anesthetic agents is changes in CMR,
which also affects CBF via flow–metabolism coupling [37]. The effect of
anesthesia at clinically usable doses may represent a depression of neuronal
Fig. 7. CBF as a function of CMRO2 at different levels of isoflurane. Flow and metabolism remained
coupled for both anesthetics. (Data from Maekawa et al, 1986 [38]).
Fig. 8. CBF as a function of CMRO2 in different brain regions for isoflurane and halothane. Flow and
metabolism remained coupled for both anesthetics. (Reprinted with permission from Hansen et.al,
1989 [36]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 275

and synaptic related neural function rather than a depression of basal metabolism.
The depression of CMR by anesthetics with an associated decrease in CBF is
Fig. 9. CSF pressure has been modeled as an equilibrium between CSF production flow rate and the
resistance to absorption. The ICP occurs at the pressure that is at the intersection of the horizontal
production flow rate and the resistance to absorption line which varies with ICP. (Reprinted with
permission from Artru, 1998 [39]).
Fig. 10. The net effect on ICP due to anesthetic influence on CSF dynamics is depicted for etomidate.
Etomidate lowers the production flow rate and changes the slope of the resistance to absorption curve.
The net effect is a reduction in ICP. (Reprinted with permission from Artru, 1998 [39]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292276

an important anesthetic action. However, the coupling of CMR to CBF is
preserved under anesthesia, although the degree of coupling may be different
between anesthetic agents (Fig. 7) and at different dosages of the anesthetic
agents (Fig. 8) [36,38].
It is important to note that for a given patient, regions of the brain may behave
differently depending on regional pathology. Therefore, some physiologic
maneuvers may shunt blood preferentially from areas of good flow to areas of
poor flow (reverse steal or Robin Hood effect), or shunt blood from areas of poor
flow to areas already rich with flow (steal phenomena). It appears that these
shunting phenomena can occur using pharmacologic agents, but the clinical
significance is unclear.
Finally, anesthetic actions may also alter cerebral physiology by altering
cerebrospinal fluid (CSF) dynamics. The actual mechanisms of CSF pressure and
volume regulation are rather complex. However, CSFP has been modeled as the
equilibrium defined by the production flow and the resistance to absorption
(Fig. 9) [39]. Normal physiologic mechanisms that alter CSF production or
absorption include temperature and ventilation and anesthetic agents likely
produce changes by altering the rate of production and the resistance to
absorption (Fig. 10). Table 1 shows representative data for anesthetics taken
from Artru [39].
Table 1
Effect of anesthetic agents on CSF dynamics
Low dose High dose
Vf Ra ICP Vf Ra ICP
Inhaled anesthetics
Halothane dec inc inc
Enflurane none inc inc inc none inc
Isoflurane none none/inc none/inc none dec dec
Desflurane none/inc none/inc none/inc
Sevoflurane dec inc ?
Nitrous Oxide none none none
Opiods
Fentanyl none dec dec dec none/inc dec/?
Alfentanil none dec dec none none none
Sufentanil none dec dec none inc/none inc/none
Sedative-hypnotics
Thiopental none inc/none none dec none/dec none
Midazolam none inc/none inc/none dec none/inc dec/?
Etomidate none none none dec none/dec none/dec
Propofol none none none
Ketamine none inc inc
Abbreviations: Vf = Production rate of CSF flow; Ra = resistance to absorption; ICP = predicted effect
on ICP.
Data from Artu AA. Cerebral fluid dynamics. In: Cucchiara RF et al, editors. Clinical neuroanesthesia,
2nd ed. New York: Churchile-Livingstone; 1998. p. 41–72.
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 277

Effects of specific anesthetic agents on cerebral physiology
Potent inhalational agents
The potent inhalational agents (halothane, enflurane, isoflurane, sevoflurane,
desflurane) produce a multitude of changes in the normal brain, which suggest
that they should have adverse effects on patients with intracranial pathology (i.e.,
increase ICP). These agents produce at least three different effects that together
result in a dose-related change in cerebral physiology. First, they produce a dose-
dependent depression of metabolism that tends to reduce CBF through coupling.
Second, the inhalational agents change the coupling so that CBF is reset to a
higher level for each CMR (Fig. 8). Finally, the inhalational agents are direct
vasodilators producing a dose-dependent increase in CBF. Hence, at low doses
CBF is not elevated, but at higher doses it increases. The balance of these effects
is different between agents and determines the net effect at any given anesthetic
level. Depicted in Fig. 11 is the effect of three agents on CBF, suggesting above a
certain threshold (e.g., 1 minimal alveolar concentration [MAC] for isoflurane),
the net effect is vasodilation [40]. CBF increase appears as a consequence of
arterial dilation as well as increase in venous capacitance [41]. Nitric oxide likely
Fig. 11. CBF as a function of relative MAC value in volunteers for isoflurane, enflurane, and
halothane. Flow and metabolism remained coupled for both anesthetics. (Reprinted with permission
from Eger, 1981 [40]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292278

plays a role in the vasodilation effect that appears to decrease over time [22,42].
CBF responsiveness to carbon dioxide also appears to decrease over time [43].
Halothane is a potent cerebral vasodilator that can produce a marked increase
in ICP clinically. This has been attributed to increases in arterial blood volume
producing an increase in pressure in a cranial cavity rendered noncompliant by
pathology. This observation in 1969 resulted in an editorial condemning volatile
agents for neurosurgical procedures [44]. Fortunately, if hyperventilation (e.g.,
arterial carbon dioxide [PaCO2] 25 mmHg) is instituted prior to introduction of
halothane, the rise in ICP can be prevented. Halothane appears to enhance
vascular reactivity to PaCO2 and changes the relationship of mean arterial
pressure (MAP) and CBF (autoregulation). These reactivities appear to be lost
above 2 MAC.
Finally, although CMR is decreased, CBF increases, suggesting an uncoupling
of CBF and CMR [45]. The effect is not uniform, as the most prominent
vasodilation occurs in the cerebral cortex. In fact, there is a positive correlation
of MAC multiples and the CBF/CMR ratio for all volatile inhalational agents. Of
interest, the decrease in CMR does not appear to be linear, with a major shift to
lower metabolism at 0.5–0.6%. High doses of halothane (above 2.3%) appear to
be associated with toxicity apparently due to interference with mitochondrial
electron transport.
Halothane appears to be a direct vasodilator through an effect on vascular
smooth muscle. This effect occurs faster than metabolic suppression, explaining
why hyperventilation needs to be instituted prior to introduction of the drug. This
effect may be potent enough to overcome beneficial vasoconstriction associated
with decreases in CMR. The net effect is that at low doses (less than 0.5 MAC)
the reduction in CBF offsets the vasodilation effect, resulting in no major cerebral
vascular effect. However, at higher doses the vasodilation is prominent, resulting
in a rise in ICP. It is also of interest that the effect on CBF is time dependent so
that the effects may be different for longer duration exposure. Halothane appears
to increase the resistance to CSF resorption decreases in production. Studies with
cerebral injury show that brain protrusion is worse with halothane than some
other agents. These effects may also contribute to increases in ICP.
Enflurane has similar effects to halothane but appears to be a less potent
cerebral vasodilator and a more potent depressant of CMR. Whereas halothane
has marked effects on cerebral dynamics above 0.5 MAC, enflurane does not
have marked effects until values above 1 MAC. Higher doses of enflurane (over
1.5 MAC) combined with hypocarbia (PaCO2 less than 30 mmHg) produce
cerebral seizure activity with an increase in CMR that is associated with increases
in CBF and ICP. Enflurane increases ICP by mechanisms affecting CSFP. At low
doses, resistance to absorption is increased (with flow unchanged), and at high
doses there is increased production (with normal resistance).
Isoflurane is the least potent cerebral vasodilator and the most potent
metabolic suppressant. It produces a decline in CMR until 2 MAC, when an
isoelectric EEG occurs. Further increases do not decrease CMR further. Like
halothane, ICP increases with the use of isoflurane. However, the effects are
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 279

minimal if hyperventilation is used. Unlike halothane, the hyperventilation need
not be introduced prior to the agent. The net effect appears to be a reduction in
CBF below 0.5% with increased CBF above 0.95%. Also, unlike halothane, high
doses of isoflurane do not appear to be toxic.
Because of these favorable properties, isoflurane has been recommended as a
better choice for patients with intracranial pathology. The regional effects of
isoflurane are not uniform. CBF is affected in deeper structures more than in the
superficial cortex. The metabolic effects of isoflurane appear disproportionately
greater in the neocortex. As with halothane, reactivity to PaCO2 is maintained
below 2 MAC. This reactivity appears to be more prominent with isoflurane than
with halothane. In studies of brain surface protrusion, isoflurane produced less
effect than halothane. However, following cryoinjury edema formation was
worse. Isoflurane appears to have no adverse effect on CSFP. Production is
unchanged at all doses, and resistance to absorption is decreased at high doses
(some questionable increases at low doses).
Desflurane is similar to isoflurane in many respects [46]. It produces a steady
decrease in CMR with increases in CBF and ICP with the production of EEG
burst suppression at 2 MAC. Reactivity to PaCO2 remains intact at least to 1.5
MAC, and hyperventilation appears to minimize the ICP consequences of its use.
Also, like isoflurane, it appears to be nontoxic at doses associated with burst
suppression. Desflurane appears to produce no change in resistance to CSF
absorption but may increase production, raising the possibility of some contri-
bution to a rise in ICP [47]. The lower blood-gas solubility of desflurane does
offer some potential advantages over isoflurane for more prompt awakening.
Sevoflurane also appears to have properties similar to isoflurane, with minimal
impact on cerebral dynamics below 1.5 MAC [48]. The effects on CBF and CMR
are similar to that of isoflurane, with burst suppression at about 2 MAC.
Response to PaCO2 and autoregulation appear intact up to 1 MAC. Studies have
shown that ICP can be increased even without CBF changes indicating dilation of
cerebral capacitance vessels. This suggests that the relationship of CBF and
cerebral blood volume (CBV) is nonlinear.
Sevoflurane appears to produce offsetting effects on CSFP, with decreases in
production and increases in resistance to absorption. The net effect of this is
unclear. Sevoflurane is metabolized to inorganic fluoride, and this metabolism is
increased in patients treated with pentobarbitol and phenytoin [49]. The clinical
significance of this in neurosurgical patients is unclear. Sevoflurane is similar to
desflurane, in that the lower blood-gas solubility may have some advantages for
faster awakening.
Nitrous oxide
The impact of nitrous oxide on cerebral dynamics has been controversial for
some time, because studies in humans and animals have produced conflicting
results. For example, it has little to no effect in the rat, but major adverse changes
are seen in other species. Some of these differences are species specific, but they
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292280

may also be related to the background physiologic state and the presence of other
anesthetics. In contrast to the other inhalational agents, nitrous oxide appears to
stimulate cerebral metabolism, which increases CBF and ICP. Without other
agents, nitrous oxide also appears to be a potent cerebral vasodilator (by
mechanisms other than by stimulation of metabolism) with the potential to
increase ICP. Increases in ICP in humans have been demonstrated [50–52].
Fortunately, when combined with barbiturates, narcotics, and hypocarbia, the
potential effects of nitrous oxide on CBF and ICP appear to be minimal.
However, when added to volatile agents, nitrous oxide may increase ICP. Nitrous
oxide does not appear to alter CSF dynamics.
Intravenous agents
Opioid agents have also shown conflicting results in studies depending on the
background anesthetic and physiologic state. For example, in the presence of vas-
Fig. 12. Mean arterial blood pressure (MABP) and ICP following an intravenous dose of sufentanil.
As shown in group 1, ICP did not rise when MABP did not fall, but a transient rise in ICP was seen
with a transient fall in MABP (group 2). (Reprinted with permission from Werner et al., 1995 [53]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 281

odilating agents (e.g., halothane), opioids produce a decrease in CBF and CMR.
However, in the presence of vasoconstricting agents, or no other agents, opioids
had no effect or were associated with an increase in CBF and CMR (Fig. 12) [53].
These effects have led to some reports that opioids have increased CBF and ICP
[54]. However, there is presently no clinical evidence that opioids increase ICP
significantly if ventilation is maintained [55]. Fortunately, opioids do not appear to
alter the CBF changes with PaCO2. Seizures have been reported in some cir-
cumstances with opioid agents. When these occur, CBF and CMR increase. The
opioid agents appear to either decrease CSFP or produce no change through a
variety of effects lowering resistance to absorption or lowering production. How-
ever, sufentanil at high doses may increase resistance to absorption, raising the
possibility of a contribution to increased ICP.
The barbiturates (thiopental, methohexitol, pentobarbitol) have been charac-
terized as cerebral vasoconstrictors. This is because increasing doses cause
decreasing CBF. This is likely due to a steady decrease in CMR until burst
suppression is produced by reduction in synaptic function (Fig. 13) [56]. Unlike the
inhalational agents, the barbiturates do not appear to uncouple or change the
relationship of CBF and CMR. Reactivity to PaCO2 is maintained, and hyper-
ventilation appears to decrease CBF further in the presence of barbiturates. Large
doses do not appear to be toxic. However, as with the inhalational agents, maximal
CMR depression occurs at doses that produce burst suppression on the EEG. Doses
beyond those producing maximal CMR reduction may produce vasodilation. The
metabolic depression of the barbiturates is uniform throughout the brain except for
the habenulo-interpeduncular system, which is unchanged on increased [57]. The
barbiturates appear to produce no major effects on CSFP except at high doses,
when thiopental may decrease production and resistance to flow.
Fig. 13. Reduction in resting cerebral metabolism following a massive dose of thiopental in a dog. The
CMRO2 is progressively decreased until the EEG becomes isoelectric. (Reprinted with permission
from Michenfelder, 1974 [56]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292282

Etomidate resembles thiopental in its effects on CBF and CMR. Increasing
doses produce depression of CMR until burst suppression, when further doses do
not decrease metabolism. In dogs, etomidate reduces CBFmore rapidly than CMR,
suggesting an intrinsic vasoconstricting property. The depression of metabolism is
not uniform, with the major effect in the forebrain. As with the barbiturates,
toxicity at higher doses was not seen. One caveat with etomidate is that myoclonic
activity on induction might be misinterpreted as seizure activity. Etomidate in low
doses does appear to activate seizure foci in epileptic patients. Toxicity when used
for prolonged periods appears to be related to the propylene glycol solvent [58].
Reactivity to PaCO2 is preserved. Etomidate appears to produce no change in
CSFP at low doses with a decrease in CSFP at high doses caused by decreased
production and possibly by decreased resistance to absorption.
Propofol, also like the barbiturates, produces a dose-related decrease in CBF
and CMR. The metabolic depression appears to be more prominent in cortical
tissue. Also, similar to the barbiturates, propofol does not appear to alter
autoregulation or reactivity to PaCO2. Some case reports have suggested that
propofol can induce seizures; however, it appears to be safe in epileptic patients
[59]. Concerns have also been raised about reductions in MAP with induction
causing reductions in cerebral perfusion pressure, which can be mitigated by
proper dose and application of the agent. Propofol appears to produce no major
Fig. 14. CBF, CMRO2, and mean arterial pressure (MAP) following ketamine (2 mg/kg). (Reprinted
with permission from Dawson et al, 1972 [62]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 283

changes in CSFP. Prolonged infusions in intensive care setting have resulted in
lactic acidemia and death [60].
The benzodiazepines also resemble the barbiturates, but the effect on CMR
has a limitation of 25% decrease in metabolism rather than the 50–60% decrease
seen at burst suppression with the barbiturates [61]. Midazolam may increase
CSFP at low doses by an increase in resistance to absorption. At high doses it
reduces production and may increase resistance, with a net reduction in CSFP.
Ketamine is unusual in that it produces an increase in CBF with little or no
effect on overall CMR (Fig. 14) [62]. The rise in CBF may be related to
cholinergic mechanisms. In the presence of cerebral vasodilators like halothane or
nitrous oxide, ketamine reduces CBF. Some effects on metabolism have been
seen, particularly in the hippocampus and extrapyramidal systems with decreases
in somatosensory and auditory systems. Reports have shown that ICP is increased
in patients with intracranial pathology. However, the rises in ICP may be related
to inadequate ventilation, because they were prevented with mechanical ventila-
tion. These changes also appear to be blocked or attenuated with prior use of
barbiturates or benzodiazepines [62]. Ketamine appears to produce an increase in
CSFP by increasing resistance to absorption.
Other drugs also have some important effects. Local anesthetics have a
biphasic effect, with low doses producing sedation and reductions of CBF and
CMR. Larger doses produce seizures, severe CNS sedation, and ultimately death.
Succinylcholine produces a transient increase in ICP (Fig. 15) [63]. This appears
to be attenuated or blocked by defasciculating doses of nondepolarizing neuro-
muscular blockers, suggesting that the cerebral afferent effects from muscle
spindles may mediate the effect. The rise can also be attenuated by pretreatment
Fig. 15. The observed increase in CBF following 1.0 mg/kg succinylcholine. Also shown is the
calculated rise in CBF for the rise in PaCO2 in these dogs. (Reprinted with permission from Lanier
et al., 1989 [63]).
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292284

with thiopental. It is important to recall the excessive potassium release in
denervated muscle (e.g., stroke or spinal cord injury). Muscle relaxants, which
produce histamine release, can cause an increase in CBF associated with the
consequent vasodilation. This effect can be blocked by pretreatment with
diphenhydramine. Atracurium is metabolized to laudanosine, which can cause
seizures in animals. There is presently no evidence for this effect in clinically
relevant doses in humans. Chronic use of anticonvulsants (especially phenytoin
and possibly carbamazine) increases the dose requirements of nondepolarizers
(with the possible exception of atracurium) by changes in protein binding and the
number of acetylcholine receptors [64].
Choice of anesthetic—does it matter?
This understanding of probable mechanisms of anesthetic action leads to a
better understanding of the anesthetic state. Because general anesthesia appears to
be mediated by synaptic mechanisms, then the measurement of inhalational
anesthetic effect (MAC) by looking at peripheral reflex activity may be a
measurement of the anesthetic effect at the spinal level and not by the cerebral
effects that likely control wakefulness and memory. This sets the stage for a
dissociation of these two systems and awareness under anesthesia, which has been
observed. Further, because the action of the opioids is by receptor mechanisms that
do not involve the traditional GABA or NMDA systems, the possibility also exists
that awareness may be produced if only opioids are used during surgery.
In terms of anesthetic choice for specific procedures in patients with
intracranial pathology, some drugs appear to have specific advantages, however,
but few drugs are contraindicated.
Anesthesia in patients where ICP is an issue
In general, we have traditionally thought that anesthetic agents that increase
CMR or CBF result in increased CBV and ICP. However, the relationship
between these agents and ICP is complex, and adjuvant techniques (e.g., hyper-
ventilation) and medications (mannitol) often mitigate the possible adverse
effects. In addition, the actual effect of short-term drug-induced ICP increases
on outcome in the operating room is not clear.
Because of the propensity to induce seizures with hypocapnea, enflurane has
largely been abandoned from anesthesia protocols during intracranial surgery.
Based on the effects of the volatile agents in the normal brain, isoflurane,
sevoflurane, and desflurane would appear to be a better choice than halothane
for patients with intracranial pathology. However, neither drug appears to have
adverse effects when hypocapnea is present. Any ICP rises seen with either drug
(both raise ICP during normocapnea) have not been shown to produce adverse
outcomes. Further, studies in rabbits with raised ICP have shown that the two
drugs were identical [65]. This raises the possibility that the differences described
for the drugs in the normal brain are not as clinically significant in the pathologic
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 285

brain. Sevoflurane and desflurane would appear to have advantages in intracranial
neurosurgery because of the possibility of faster awakening. At present, these
effects aside, clinical differences between these drugs and halothane or isoflurane
are not clear [19]. It is possible that all of the inhalational agents are actually
similar in patients with intracranial pathology who are at risk for raises in ICP, and
that it is more important how the drugs are used than the specific drug chosen.
The situation with nitrous oxide is probably different. A growing appreciation
of the ability of nitrous oxide to increase CBF and ICP, and the fact that hypo-
capnea does not appear to reduce the effect, has suggested that it may be a poor
choice in patients at risk for high ICP. Certainly, nitrous oxide is a poor choice
when closed air-filled cavities are present (e.g., pneumothorax, air embolism, and
pneumocephalus). At present, ketamine also remains controversial because of
CBF increases and the observation of ICP increases in some patients. However,
contradictory and even beneficial observations have been made suggesting a
possible role for ketamine. At present, ketamine is probably not appropriate as a
sole drug in intracranial neurosurgery.
The issue of the significance of the transient rise in ICP with succinylcholine
in emergency patients remains controversial. Studies in acute head-injured
patients suggest that the advantages for rapid intubation offered by succinylcho-
line may offset the potential disadvantages on the ICP rise (especially when the
magnitude of the rise can be reduced by pretreatment and other techniques which
lower ICP). Another area of controversy with head trauma revolves around the
appropriateness of hyperventilation. With CBF reduced from the trauma, it is
possible that concurrent hyperventilation may produce regional ischemia.
Because the actual circumstance in any given patient is difficult to discern, no
recommendations can be made.
Anesthesia when brain protection is desired
Discussion of anesthetic choice during procedures in which brain ischemia
and stroke can occur has revolved around the possible use of anesthetic agents for
brain protection. The possibility of protection appears to be related, in part, to the
depression of metabolism of the synapse by the anesthetic agents. Barbiturates
have a clear track record for protection during focal ischemia. However, they may
produce delayed awakening from anesthesia. The results of studies with other
agents that can lower CMR by producing burst suppression (e.g., isoflurane,
etomidate, propofol) are less clear. Lidocaine, ketamine, and certain other agents
has been shown to be protective in some models but clinical significance as not
yet been established in humans. Of interest is one study with halothane, in which
CMR depression was associated with better cellular energy stores during
ischemia, but a worse infarct resulted.
These observations suggest that the protective effects of anesthetics are
probably related to mechanisms other than CMR depression. For example,
barbiturates have been associated with free radical scavenging, reduced calcium
flux, reduced cerebral edema, enhancing cyclic AMP production, blocked Na
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292286

channels, and other potentially advantageous effects. Because hypothermia also
protects by some of these mechanisms, there is a growing appreciation that
metabolic rate reduction may not be as protective as once thought. Thus,
anesthetic choice in these circumstances probably relates to the other effects of
anesthesia aside from brain protection.
In this context, it should be remembered that ketamine has the property of
increasing CBF. Although this may cause detrimental elevations in ICP when
pathology is present, when the ICP is not an issue the increase in blood flow
might be helpful with ischemia in the same way nitroglycerine is useful in cardiac
ischemia. Theoretically, an increase in flow might also be detrimental by a
‘‘steal’’ of blood from ischemic areas by increasing flow to nonischemic areas.
Sufficient studies are not available at present to determine if or when this property
of ketamine is advantageous when a rise in ICP is not a problem.
Also of interest is anesthetic choice for carotid endarterectomy. EEG monitor-
ing has shown that the mean CBF at which 50% of patients show EEG
abnormalities (so-called critical blood flow) is lower with isoflurane than with
halothane. This has suggested to some that isoflurane may reduce the possibility
of cerebral ischemia. However, no improvement in outcome has been shown.
Anesthetic choice for general anesthesia in these patients probably still remains
focused on cerebral perfusion and considerations for cardiac disease.
Anesthesia where neurophysiological monitoring is conducted
There are clear differences in anesthetic effects on neurophysiologic monitor-
ing. The anesthetic choice depends on the modality of monitoring chosen for the
patient and the other anesthetic considerations applicable to the patient and
surgery [66]. When the choice of anesthetic is not constricted by the pathology
and physiology, the specific effects of the medications on cerebral neurophysi-
ology should be considered.
Because the major target of anesthetic action appears to be synaptic function,
electrophysiological recordings that depend on these structures will be most
susceptible to depressant agents. Hence, monitoring which does not record or
stimulate the cortex and does not record muscle activity has little influence on
anesthetic choice. On the other hand, if recordings are to be taken from the
cerebral cortex (e.g., somatosensory-evoked potentials: SSEP, visual-evoked
potentials), then inhalational agents need to be used in restricted concentrations
(less than 0.5 MAC) unless monitoring suggests larger concentrations are
tolerated and intravenous agents have been titrated to acceptable levels. Opioids
appear to have minimal effects on these recordings, possible because of their
unique mechanism of action.
Etomidate or ketamine may be used to enhance cortical SSEP recordings,
possibly because of an altered balance of effects on the depressant and excitatory
neural pathways. The beneficial effect appears to be restricted to the cortical
recordings of sensory modalities, suggesting that the shift in synaptic balance is
primarily in the cortex.
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 287

Routine EEG recording can usually be done with most anesthetics as long as
the doses are not excessive (e.g., where the depressant effects stop the synaptically
produced EEG) (Fig. 16) [67]. However, if the EEG is being recorded for seizure
focus detection, all medications that depress seizure activity must be avoided.
Muscle relaxants are preferred when there is recording from the epidural space
or peripheral nerves, but should be controlled carefully when monitoring record-
ings from muscles (and not used when recording spontaneous or mechanically
elicited muscle responses). Transcranial stimulated motor-evoked potentials
severely restrict anesthetic choice to largely intravenous agents probably due to
the combined anesthetic effects in the cerebral motor cortex and the synapses of the
anterior horn cell of the spinal cord. The anesthetic choice is further complicated by
the need to restrict muscle relaxation so as to record muscle responses. As with the
cerebral cortical responses, etomidate and ketamine appear to make the neuro-
Fig. 16. Stages of EEG for various anesthetics at various doses. Two basic types of anesthetic action are
noted (e.g., EEG activation and EEG depression). (Reprinted fromWinters WD. Effects of drugs on the
electrical activity of the brain: anesthestics. AnnuRev Pharm Toxicol 1976;16:413–26; with permission
from the Annual Review of Pharmacology and Toxicology, volume 16 D 1976 by Annual Reviews
www.AnnualReviews.org. <http://www.AnnualReviews.org>
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292288

physiologic environment more favorable for recording these responses. Finally, the
newer multipulse stimulation techniques appear to overcome some of the depress-
ant effects, and that inhalational agents may be usable in some patients at low
concentrations. Clearly, examining the actual monitoring and then holding steady
during periods of neural risk should evaluate the choice of anesthetic.
Summary
The action of anesthetics on the nervous system can be understood by
considering their possible interactions with neuronal function. Anesthesia may
be produced by a change in the balance of inhibitory synapses (notable via
GABAa receptors) and excitatory synapses (notably glutamate receptors). Our
knowledge of the specific mechanisms of anesthetic drugs and the structures in
the CNS remains inadequate to explain the anesthetic state by one mechanism.
The action of anesthetics can also be considered based on the action of the drugs
on cerebral physiology, notably CMR, CBF, metabolic coupling, and autoregu-
lation. Some specific anesthetic recommendations can be made for certain
neurosurgical procedures and pathology based on the effects on physiology.
References
[1] Larabee MG, Posternak J. Selective action of anesthetics on synapses and axons in mammalian
sympathetic ganglia. J Neurophysiol 1952;15:91–114.
[2] Brown MF. Modulation of rhodopsin function by properties of the membrane bilayer. Chem
Phys Lipids 1994;73:159–80.
[3] Sunshine C, McNamee MG. Lipid modulation of nicotinic acetylcholine receptor function: the
role of membrane lipid composition and fluidity. Biochem Biophys Acta 1994;1191:59–64.
[4] Sinensky M, Pinkerton F, Sutherland E, et al. Rate limitation of (Na+ +K+ )-stimulated ad-
enosinetriphosphatase by membrane acyl chain ordering. Proc Natl Acad Sci USA 1979;76:
4893–7.
[5] Firestone LL, Alifimoff JK, Miller KW. Does general anesthetic-induced desensitization of the
Torpedo acetylcholine receptor correlate with lipid disordering? Mol Pharmacol 1994;46:508–15.
[6] DeLorey TM, Olsen RW. GABA and glycine. In: Siegel GJ, et al, editors. Basic neurochemistry:
molecular, cellular, and medical aspects. 5th ed. New York: Raven Press; 1994. p. 389–99.
[7] Cheng SC, Brunner EA. Anesthetic effects on GABA binding. Anesthesiology 1984;61:A326.
[8] Mayer ML, Westbrook GL, Guthrie PB. Voltage-dependent block by Mg2+ of NMDA responses
in spinal cord neurons. Nature 1984;309:261–3.
[9] France CP, Winger GD, Woods JH. Analgesic, anesthetic, and respiratory effects of the com-
petitive N-methyl-D-aspartate (NMDA) antagonist CGS 19755 in rhesus monkeys. Brain Res
1990;526:355–8.
[10] Peoples RW, Weight FF. Anesthetic actions on excitatory amino acid receptors. In: Yaksh TL,
et al, editors. Anesthesia: biologic foundations. New York: Lippincott-Raven; 1998. p. 239–58.
[11] Lodge D, Johnston GA. Effect of ketamine on amino acid-evoked release of acetylcholine from
rat cerebral cortex in vitro. Neurosci Lett 1985;56:371–5.
[12] Schmidt CJ, Taylor VL. Release of [3H} norepinephrine from rat hippocampal slices by
N-methyl-D-aspartate comparison of the inhibitory effects of Mg2 + and MK-801. Eur J Pharma-
col 1988;156:111–20.
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 289

[13] Snell LD, Johnson KM. Characterization of the inhibition of excitatory amino acid-induced
neurotransmitter release in the rat striatum by phencyclidine-like drugs. J Pharmacol Exp Ther
1986;238:938–46.
[14] O’Shaughnessy CT, Lodge D. N-Methyl-D-aspartate receptor-mediated increase in intracellular
calcium is reduced by ketamine and phencyclidine. Eur J Pharmacol 1988;153:201–9.
[15] Hemmings HC Jr, Hopkins PM. Intravenous anesthetic agents. In: Hemmings HC Jr, et al, editors.
Foundations of anesthesia basic and clinical sciences. St. Louis: Mosby; 2000. p. 241–52.
[16] Cai Z, McCaslin PP. Acute, chronic and differential effects of several anesthetic barbiturates on
glutamate receptor activation in neuronal culture. Brain Res 1993;611:181–6.
[17] Martin DC, Dennison RL, Aronstam RS. Barbiturate interactions with N-methyl-D-aspartate
(NMDA) receptors in rat brain. Mol Neuropharmacol 1992;2:255–9.
[18] Raja SN, Moscicki JC, Woodside JR Jr, et al. The effect of acute phencyclidine administration on
cyclopropane requirement (MAC) in rats. Anesthesiology 1982;56:275–9.
[19] Carla V, Moroni F. General anesthetics inhibit the responses induced by glutamate receptor
agonists in the mouse cortex. Neurosci Lett 1992;146:21–4.
[20] Lin L-H, Chen LL, Harris RA. Enflurane inhibits NMDA, AMPA, and kainate-induced currents
in Xenopus oocytes expressing mouse and human brain mRNA. FASEB J 1993;7:479–85.
[21] Puil E, El-Beheiry H. Anaesthetic suppression of transmitter actions in neocortex. Br J Pharma-
col 1990;101:323–6.
[22] Werz MA, Macdonald RL. Barbiturates decrease voltage-dependent calcium conductance of
mouse neurons in dissociated cell culture. Mol Pharmacol 1985;28:269–77.
[23] Aghajanian GK, Wang Y-Y. Common alpha-2 and opiate effector mechanisms in the rat locus
coeruleus: intracellular studies in brain slices. Neuropharmacology 1987;26:789–800.
[24] Morita K, North RA. Clonidine activates membrane potassium conductance in myenteric neu-
rons. Br J Pharmacol 1981;74:419–28.
[25] North RA, Wiliams JT, Suprenant A, MacDonald JC. Mu and delta receptors belong to a
family of receptors that are coupled tp potassium channels. Proc Natl Acad Sci USA 1987;
84:5487–91.
[26] White BH, Cohen JB. Agonist-induced changes in the structure of the acetylcholine receptor
M2 regions revealed by photoincorporation of an uncharged nicotinic noncompetitive antagonist.
J Biol Chem 1992;267:15770–83.
[27] Nestler EJ, Aghajanian GK. Molecular and cellular basis of addiction. Science 1997;278:58–63.
[28] Hardman JG, Limbird LE. Goodman and Gilman’s the pharmacologic basis of therapeutics,
9th ed. New York: McGrawHill; 1996.
[29] Maciver MB. General anesthetic actions on transmission at glutamate and GABA synapses. In:
Yaksh TL, et al, editors. Anesthesia: biologic foundations. New York: Lippincott-Raven; 1998.
p. 277–86.
[30] Feldman SM, Waller HJ. Dissociation of electrocortical activation and behavior arousal. Nature
1962;196:1320–2.
[31] Angel A. The G.L. Brown lecture. Adventures in anaesthesia. Exp Physiol 1991;76:1–38.
[32] Darbinjan TM, Golovchinsky VB, Plehotkina SI. The effects of anesthetics on reticular and
cortical activity. Anesthesiology 1971;34:219–29.
[33] Richards CD. In search of the mechanisms of anesthesia. Trends Neurosci 1980;3:9–13.
[34] ToddMM,Warner DS, Maktabi MA. Neuroanesthesia: a critical review. In: Longnecker DE, et al,
editors. Principles and practice of anesthesiology. 2nd ed. New York: Mosby; 1988. p. 1607–58.
[35] Donegan J. Effect of anesthesia on cerebral physiology and metabolism In: Newfield P, et al,
editors. Neuroanesthesia: handbook of clinical and physiologic essentials. 2nd ed. Boston: Little
Brown and Co; 1991. p. 17–30.
[36] Maekawa T, Tommasino C, Shapiro HM, et al. Local cerebral blood flow and glucose utilization
during isoflurane anesthesia in the rat. Anesthesiology 1986;65:144–51.
[37] Lebrun-Gandie P, Baron JC, Soussaline F, et al. Coupling between regional blood flow and
oxygen utilization in the normal human brain. Arch Neurol 1983;40:230–6.
[38] Hansen TD, Warner DS, Todd MM, et al. The role of cerebral metabolism in determining the
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292290

local cerebral blood flow effects of volatile anesthetics: evidence for persistent flow-metabolism
coupling. J Cereb Blood Flow Metab 1989;9:323–8.
[39] Artu AA. Cerebral fluid dynamics. In: Cucchiara RF, et al, editors. Clinical neuroanesthesia,
2nd ed. New York: Churchill-Livingstone; 1998. p. 41–72.
[40] Eger EI. Isoflurane: a review. Anesthesiology 1981;55:559–76.
[41] Koenig HM, Pelligrino DA, Albrecht RF. Halothane vasodilation and nitric oxide in rat pial
vessels. J Neurosurg Anesthesiol 1993;5:264–71.
[42] Brian JE Jr, Traystman RJ, McPherson RW. Changes in cerebral blood flow over time during
isoflurane anesthesia in dogs. J Neurosurg Anesthes 1990;2:122.
[43] McPherson RW, Tratysman RJ. Effect of time on cerebral vascular responsivity to PaCO2 during
isoflurane anesthesia. Anesthesiology 1989;71:A105.
[44] Anonymous. Halothane and neurosurgery [editorial]. Br J Anaesth 1969;41:277.
[45] Smith AL. Dependence of cerebral venous oxygen tension on anesthetic depth. Anesthesiology
1973;39:291–8.
[46] Ornstein E, Young WL, Fleischer LH, et al. Desflurane and isoflurane have similar effects on
cerebral blood flow in patients with intracranial mass lesions. Anesthesiology 1993;79:498–502.
[47] Muzzi DA, Losasso TJ, Dietz NM, et al. The effect of desflurane and isoflurane on cerebral spi-
nal fluid pressure in humans with supratentorial mass lesions. Anesthesiology 1992;76:720–4.
[48] Scheller MS, Nakakimura K, Fleischer JE, et al. Cerebral effects of sevoflurane in the dog:
comparison with isoflurane and enflurane. Br J Anaesth 1990;65:388–92.
[49] Hoffman J, Konopka K, Buckhorn C, et al. Ethanol-inducible cytochrome P450 in rabbits
metabolizes enflurane. Br J Anaesth 1989;63:103–8.
[50] Drummond JC, Scheller MS, Todd MM. The effect of nitrous oxide on cortical cerebral blood
flow during anesthesia with halothane and isoflurane with and without morphine in the rabbit.
Anesth Analg 1987;66:1083–9.
[51] Moss E, McDowall DG. ICP increases with 50 per cent nitrous oxide in oxygen in severe head
injuries during controlled ventilation. Br J Anaesth 1979;51:757–61.
[52] Pelligrino DA, Miletich DJ, Hoffman WE, Albrecht RF. Nitrous oxide markedly increases
cerebral cortical metabolic rate and blood flow in the goat. Anesthesiology 1984;60:405–12.
[53] Werner C, Kochs E, Bause H, et al. Effects of sufentanil on cerebral hemodynamics and intra-
cranial pressure in patients with brain injury. Anesthesiology 1995;83:721–6.
[54] Albanese J, Durbec O, Viviand X, et al. Sufentanil increases intracranial pressure in patients with
head trauma. Anesthesiology 1993;79:493–7.
[55] Todd MM, Warner DS, Sokoll MD, et al. A prospective comparative trial of three anesthetics for
elective supratentorial craniotomy. Anesthesiology 1993;78:1005–20.
[56] Michenfelder JD. The in-vivo effects of massive concentrations of anesthetics on canine cerebral
metabolism. In: Fink BR, editor. Molecular mechanisms of anesthetics. New York: Raven Press;
1974. p. 537–43.
[57] Hodes JE, Soncrant TT, Larson DM, et al. Selective changes in local cerebral glucose utilization
induced by Phenobarbital I the rat. Anesthesiology 1985;63:633–9.
[58] Levy ML, Aranda M, Zelman V, et al. Propylene glycol toxicity following continuous etomidate
infusion for the control of refractory cerebral edema. Neurosurgery 1995;37:363–9.
[59] Ebrahim ZY, Schubert A, Van Ness P, et al. The effect of propofol on the electroencephalogram
of patients with epilepsy. Anesth Analg 1994;78:275–9.
[60] Cray SH, Robinson BH, Cox PN. Lactic acidemia and bradyarrhythmia in a child sedated with
propofol. Crit Care Med 1998;26:2087–92.
[61] Fleischer JE, Milde JH, Moyer TP, et al. Cerebral effects of high-dose midazolam and subsequent
reversal with RO 15-1788 in dogs. Anesthesiology 1988;68:234–42.
[62] Dawson B, Michenfelder JD, Theye RA. Effects of ketamine on canine cerebral blood flow and
metabolism: modification by prior administration of thiopental. Anesth Analg 1971;50:443–7.
[63] Lanier WL, Iaizzo PA, Milde JH. Cerebral function and muscle afferent activity following
intravenous succinylcholine in dogs anesthetized with halothane: the effects of pretreatment with
a defasciculating dose of pancuronium. Anesthesiology 1989;71:87–95.
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292 291

[64] Ornstein E, Matteo RS, Schwartz AE, et al. The effect of phenytoin on the magnitude and
duration of neuromuscular block following atracurium or vecuronium. Anesthesiology 1987;
67:191–6.
[65] Scheller MS, Todd MM, Drummond JC, et al. The intracranial pressure effects of isoflurane and
halothane administered followed cryogenic brain injury in rabbits. Anesthesiol 1987;67:507–12.
[66] Sloan T. Anesthetic effects on electrophysiologic recordings. J Clin Neurophysiol 1998;15:
217–26.
[67] Winters WD. Effects of drugs on the electrical activity of the brain: anesthestics. Annu Rev
Pharm Toxicol 1976;16:413–26.
[68] McPherson RW, Traystman RJ. Effects of isoflurane on cerebral autoregulation in dogs. Anes-
thesiology 1988;69:493–9.
T.B. Sloan / Anesthesiology Clin N Am 20 (2002) 265–292292

Monitors of cerebral oxygenation
Paul R. Smythe, MD, DDS*, Satwant K. Samra, MBBS, MDDepartment of Anesthesiology, University of Michigan Medical Center, 1500 E. Medical Center Drive,
1H247-UH, Box 0048, Ann Arbor, MI 48109, USA
The central nervous system (CNS) differs from other organ systems in that it is
both the intended target of anesthesia and, at the same time, it is the organ system
that is least monitored in anesthetized patients. Intraoperative monitoring is well
recognized as the ‘‘anesthesiologist’s domain.’’ We are able monitor the function
of the cardiovascular, pulmonary, hepatic, and renal systems with varying degrees
of accuracy, but we are not able to know with certainty the neurological status
of the unconscious patient. There are several reasons why CNS monitoring has
not gained popularity among anesthesiologists. CNS monitoring is technically
difficult and demanding, anesthetics interfere with electrophysiological monitor-
ing (adding to the difficulties in interpretation), and there is only limited data to
support the contention that CNS monitoring improves outcome. On the contrary,
there is ample data suggesting that CNS monitoring frequently gives ‘‘false-
positive’’ alarms; that is, the monitor indicates impending CNS injury while the
patients awaken without a neurological deficit even if no intervention is made
based on the abnormalities observed. The pathophysiologic basis that can easily
explain this dichotomy is that neurological deficit results from infarction of
neuronal tissue while alterations in electrical activity of CNS are observed in the
presence of ischemia. Neuronal ischemia does not always lead to infarction.
Cerebral infarction results from a combination of both the severity and duration
of ischemia. Mild ischemia (enough to result in alteration of electrical activity) of
variable duration can be present without cerebral infarction. Fortunately, neuro-
logical complications of anesthesia are rare, unless the surgical procedure itself is
accompanied by significant changes in blood supply of CNS (e.g., cardiovas-
cular, major orthopedic, and neurosurgical procedures). However, neurological
complications, when they do occur, are devastating for the patients and family,
and costly for the society. It is for this reason that there will always be an interest
in the development of user-friendly, reliable, CNS monitoring systems.
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00003 -7
* Corresponding author.
E-mail address: [email protected] (P.R. Smythe).
Anesthesiology Clin N Am
20 (2002) 293–313

Most CNSmonitors are designed to monitor cerebral hemodynamics or cerebral
electrical activity. Monitors of cerebral hemodynamics include the measurement of
intracranial pressure (ICP), cerebral perfusion pressure (CPP), and cerebral blood
flow (CBF) or cerebral blood flow velocity (TCD). Monitors of CNS electrical
activity include electroencephalography (EEG), sensory-evoked potentials (SEPs),
and motor-evoked potentials (MEPs). These monitors give a warning of lack of
blood (and hence oxygen) supply to CNS and its impact on electrical activity. None
of these monitors are meant to directly measure the presence of oxygen within the
brain tissue. Direct monitoring of brain oxygenation, representing the balance
between cerebral oxygen consumption and supply, may be of greater clinical
utility. There are three monitors of cerebral oxygenation currently in clinical use:
(1) monitoring of jugular venous oxygen saturation (SjvO2), (2) transcranial
cerebral oximetry measuring regional cerebrovascular oxygen saturation (rSO2),
and (3) monitoring of the brain tissue oxygen tension (PbtO2). This manuscript is
devoted to a review of historic developments, underlying technology, limitations,
and clinical use of three monitors of cere-bral oxygenation.
Jugular venous bulb oxygen saturation
History and methodology
The measurement of SjvO2 of hemoglobin was first performed by insertion of
a needle into the jugular bulb located about 1 centimeter anterior and inferior to
the mastoid process. Blood was then analyzed for oxygen saturation of hemo-
globin. A reading of saturation < 50% was deemed ‘‘critical,’’ indicating cerebral
hypoxia. Generally, the technique was used either to calculate arteriovenous
oxygen difference in neurosurgical intensive care units (NICUs) or during carotid
endarterectomy (CEA). A single sample of blood was drawn after occlusion of
internal carotid artery as a monitor to determine the adequacy of collateral blood
flow, and hence, the need for placement of an intravascular shunt. Later, it was
appreciated that taking a single sample was not adequate because cerebral
hypoxia could develop at a variable interval after carotid occlusion. Central
venous catheters were thus placed in the jugular bulb by insertion into the internal
jugular vein and advancement of the catheter in a cephalad direction. Placement
was confirmed radiographycally. This method allowed repeated sampling of
jugular bulb venous blood without repeated needle punctures, and increased the
use of this monitoring both during CEA as well as in patients in NICUs.
Development of in vivo reflectance oximetry (using fiber optic bundles) has
allowed continuous monitoring of SjvO2 without sampling blood except for
initial calibration. Each catheter has at least two optical bundles. One bundle
transmits light into the bloodstream, and second transmits the reflected light to a
photo sensor that is able to distinguish the intensity of the light at various
wavelengths. A computer algorithm uses the relative intensities of appropriate
wavelengths to determine the saturation of hemoglobin in the jugular bulb.
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313294

Catheters with three fiberoptic bundles are able to estimate hemoglobin concen-
tration in addition to determining the relative concentrations of oxy- and reduced
hemoglobin. Catheters with only two fiberoptic bundles must have hemoglobin
concentration values entered into the algorithm. The value of SjvO2 is then
continuously displayed as a percentage of saturated hemoglobin. These techno-
logic advances in development of catheters have made continuous monitoring of
SjvO2 possible, resulting in a rejuvenation of interest in this monitoring in
patients in NICU [1–3].
Hemoglobin saturation in the jugular venous bulb is primarily dependent on
the relative balance of oxygen consumption and oxygen supply to the cerebrum.
The absolute values for cerebral metabolic rate of oxygen consumption (CMRO2)
are impossible to measure directly, and are estimated only indirectly. The absolute
value for oxygen supply is somewhat easier to estimate, but, like oxygen demand,
is remarkably heterogeneous and in a constant state of flux. SjvO2 theoretically
reflects the relationship between global cerebral oxygen supply and global
cerebral oxygen demand. It is therefore possible to miss regional cerebral hypoxia
with this monitoring tool.
In patients with normal CMRO2–CBF coupling, changes in cerebral blood
flow will initially compensate for changes in CMRO2. When changes in CBF can
no longer compensate for increased CMRO2, decrease in SjvO2 will be seen. The
changes in SjvO2 are also different in cases of anemia versus hypoxia. With a fall
in hemoglobin, SjvO2 remains relatively constant until CBF can no longer
compensate for lower oxygen content of arterial blood (CaO2). SjvO2 will then
fall linearly with falling hemoglobin values. With hypoxia, SjvO2 decreases more
linearly immediately after a decrease in CaO2. In brain-injured patients, CMRO2
is approximately half of that of the normal patients [4]. CBF is uncoupled from
CMRO2 in many such patients to an unpredictable degree. CBF can increase or
decrease in response to a decrease in CMRO2. Thus, the CMRO2/CBF ratio may
increase or decrease and, therefore, SjvO2 may increase or decrease in the
presence of decreased CMRO2. As a result, SjVO2 readings in brain-injured
patients become difficult to interpret. Despite the possibility for inaccuracies,
some recommendations are made for interpretation of SjvO2 values. Normal
values range from 55% to 71% (mean 61.8%) in healthy individuals, and any
SjvO2 greater than 50% is considered to be within normal limits [5,6]. An SjvO2
between 45% and 50% is suggestive of mild cerebral hypoxia, while SjvO2
< 45% indicates severe cerebral hypoxia [2,3,7,8]. Jugular venous PO2 equivalent
of an SjvO2 of 40% has been shown to be associated with EEG changes in
humans [9]. Mental confusion has been found to occur when SjvO2 has decreased
below 45%, and loss of consciousness has occurred when SjvO2 has decreased
below 24% [10].
Clinical use
Lack of a ‘‘gold standard’’ with which the accuracy of SjvO2 monitors can be
compared is well recognized. Clinical utility of SjvO2 has therefore been
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 295

determined either by association with clinical findings in patients in the ICU and
during surgery or SjvO2 readings have been compared with measurements from
other monitors, like transcranial cerebral oximeters and brain tissue oxygen
probes. It is difficult to draw definitive conclusions from these comparisons
because SjVO2 is a monitor of global hypoxia while cerebral oximetry and PbtO2
are monitors of regional hypoxia. Further, it should be emphasized that other
monitors have their own limitations and their own lack of proven validity. There
have been no randomized, prospective clinical trials correlating the use of SjvO2
monitoring with improved clinical outcome. Despite these limitations, availabil-
ity of oximetric catheters has led to a renewed interest in SjvO2 monitoring, and
several clinical studies have been recently published. SjvO2 monitoring has been
used in NICUs in patients with traumatic brain injury and for intraoperative
monitoring during neurosurgical and cardiovascular surgical procedures
Head-injury patients
In patients with traumatic brain injury with a Glasgow Coma Scale (GCS) < 8,
even a single episode of SjvO2 < 50% lasting more than 10 minutes was
associated with doubling of mortality [11]. One episode of desaturation increased
the risk of poor outcome from 55% to 70%.
During anesthesia for neurosurgical procedures
Matta et al [12] have examined the feasibility and usefulness of SjvO2
monitoring during neurosurgical procedures. One hundred patients having
craniotomy for variety of indications were studied. Episodes of desaturation
were discovered in 50–72% of these patients, which would not have otherwise
been detected. This study only reported observations and did not address
differences in outcomes.
During anesthesia for cardiovascular surgical procedures
Intraoperative monitoring of SjvO2 in patients undergoing cardiopulmonary
bypass has undergone extensive study [13–15]. SjvO2 remains normal (or may
increase) during the hypothermic phase of extracorporeal circulation, but desatu-
ration ( < 50%) occurs with rewarming, and is associated with more neurologic
deficits. Desaturation during rewarming is likely to be associated with mean
arterial pressure < 60 mmHg, low hematocrit and rapid rate of rewarming.
Limitations
There are several limitations that make routine use of SjvO2 catheters
less attractive:
1. SjvO2 monitoring is an invasive procedure, and has inherent risks
associated with central catheter placement and maintenance; that is, carotid
artery puncture, bleeding, nerve damage, and infection. SjvO2 catheters are
directed away from the lungs and heart; therefore, there is less risk of
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313296

pneumothorax and cardiac arrhythmias when compared to central venous
catheters for hemodynamic monitoring.
2. There can be damage to catheters during continuous use that gives
inaccurate readings.
3. Migration of a catheter is a problem. The catheter may get displaced and
sample blood proximal to opening of the facial vein into the internal
jugular vein. This will result ‘‘false’’ high values of SjvO2, and cerebral
hypoxia may be missed.
4. There is extracerebral contribution to jugular venous blood, which means
that blood from the jugular bulb at least partially represents drainage from
areas other than just the brain. Sources of extracranial contamination in-
clude blood from emissary and frontal veins (via sagittal sinus), ophthalmic
vein, and pterygoid plexus (via cavernous sinus). Facial and retromandib-
ular veins open directly into jugular veins, usually below the jugular bulb.
But they may have an aberrant course with an opening at the level of the
jugular bulb.
5. Rate of aspiration of the blood sample may effect SjvO2 readings. Matta
et al [7] found that the faster the blood was withdrawn from the bulb, the
higher the reading for SjvO2. It is possible that, with the faster withdrawal
rate, more extracerebral blood was incorporated into the sample, but the
reason is not known with certainty.
6. The SjvO2 is a monitor of global oxygenation and not a monitor of regional
ischemia or hypoxia.This means that there may be focal areas of ischemia
that are not detected with a global monitor.
All these limitations have prevented clinical studies that are necessary to
validate the use of SjvO2 as a means of altering treatment in a way that would
improve clinical outcome. Although SjvO2 may be a useful monitor in a limited
set of circumstances, the search for a better monitor will continue.
Transcranial cerebral oximetry
Like pulse oximeters and mixed venous oximeters, development of cerebral
oximeters is based on principles of transmission and absorption of light in a near-
infrared (NIR) spectrum. Cerebral oximetry theoretically offers a technique for
continuous, noninvasive, bedside monitoring that reflects a balance between
cerebral oxygen consumption and supply. These attributes make near-infrared
spectroscopy (NIRS) almost the ideal monitor for monitoring cerebral oxygena-
tion. In addition to differentiation between oxygenated and deoxygenated
hemoglobin based on their light absorption characteristics, NIRS can also
measure the oxidation state of Cytochrome aa3 (Cyt aa3), the terminal cyto-
chrome of the electron transport chain. Indeed, when Jobsis [16] first described a
spectroscopic technique for measuring oxygenation in a tissue bed, he did so by
measuring, in the rat heart and cat brain, the oxidation state not of hemoglobin
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 297

but of Cyt aa3. However, transforming the spectroscopic technique developed by
Jobsis into an everyday, easy-to-use bedside instrument has proven to be a
difficult task. Nearly 2.5 decades after Jobsis’s original experiments, there is only
one Federal Drug Administration (FDA)-approved device commercially available
for clinical use in United States, and there is a fair amount of criticism regarding
the performance of that device. As a result, there is some degree of skepticism
surrounding the utility of cerebral oximetry in clinical practice.
Methodology
NIR spectroscopy is based on few relatively simple physical principles:
1. Light in the NIR range readily penetrates skin and bone. A small amount
of light absorption by skin pigments, that is, melanin and bilirubin, is
independent of the tissue oxygenation status, and hence, represents a
source of fixed scattering of light only. However, in cases of severe jaun-
dice, serum bilirubin concentrations can reach levels that will interfere with
NIRS [17].
2. Very few biological substances absorb NIR.
3. Hemoglobin and Cyt aa3 are the only absorbers (chromophores) that show
a detectable change in NIR absorption in response to hypoxia or ischemia.
These, therefore, are the chromophores of interest.
4. Each chromophore has a characteristic and unique (although somewhat
overlapping) absorbance spectrum. For example, oxygenated hemoglobin
(HbO2) absorbs less red light (600–750 nm) and more infrared light (850–
1000 nm) than does deoxygenated hemoglobin (Hb). As a result, Hb has an
absorption peak at 740 nm while HbO2 does not. HbO2 and Hb absorb NIR
of a 810-nm wavelength in equal amounts, and this wavelength of NIR is
referred to as the isobestic point. Similarly, Cyt aa3 has a broad band of
light absorption with a peak at 840 nm. There are also other pigments, such
as cerebrocuprein and erythrocuprein, that change their absorption spectra
when they are bound to oxygen, but these do not have significant ab-
sorption in the NIR range [18,19]. Some other pigments that can absorb
NIR (like nitrosyl hemoglobin, glucose, and indocyanine green) either do
not normally exist in the body or their absorbance is too limited to affect
NIRS spectrometry [20,21].
The basic components of an NIR oximeter are: (1) a light source that can
generate known wavelengths and intensities of NIR light; (2) optical bundles
(optodes) to transmit the light from the source across the tissue site; (3) a light
detector (photo diode or photomultiplier); (4) a computer with proper algorithms
to process the information obtained from the recovered light and translate it into
useful information (i.e., hemoglobin saturation). It should be noted that NIRS
technology can and has been applied to the study of skeletal muscle, heart, and
other organs, and that NIRS can be used for other purposes, such as the
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313298

calculation of cerebral blood flow. We shall limit our discussion in this chapter to
the use of NIRS in cerebral oximetry.
Cerebral oximeters can be divided in to two main groups: (a) saturation
monitors, and (b) concentration monitors. Saturation monitors, like pulse oxim-
eters, measure the ratio of hemoglobin and oxyhemoglobin. These monitors do
not include path length in the algorithm used for calculation of rSO2. Concen-
tration monitors measure the amount of oxy- and reduced hemoglobin, as well as
Cyt aa3, and some monitors even incorporate blood volume measurement.
Concentration monitors are further subdivided into relative and absolute concen-
tration monitors. Relative concentration monitors measure a ratio of substrates,
and do not require exact knowledge of the path length.
Two cerebral oximeters have been frequently used in the majority of
published clinical studies: the INVOS series (Somanetics, Troy, MI), and NIRO
500/1000 (Hamamatsu Photonics, UK). These two types of cerebral oximeters
differ in the types of light emitters and light detectors used. The INVOS is a
saturation monitor. It uses a light-emitting diode that transmits NIR at two
wavelengths (735 and 810 nm) as the light source and two silicon photodiodes
(SiPDs) as light detectors. Both the light source and detectors are enclosed in a
common adhesive strip assembly, which is applied to the patient’s forehead.
Two light detectors are placed at a distance of 3 cm and 4 cm from the light
source. The light detected by the closer sensor reads light that has traveled
a shorter distance and is reflected primarily from extracranial tissues like skin
and bone. The light detected by the farther sensor has travelled through both
superficial structures and the cerebrum. Information from the former is ‘‘sub-
tracted’’ from information gained from the latter to exclude extracranial con-
tamination. The light source of the NIRO 500, a relative concentration monitor,
is comprised of four pulsed laser diodes that produce NIR in the range of 775,
825, 850, and 905 nm. The advantage of laser diodes is that the intensity and
wavelength of NIR delivered is more precise. Disadvantage is that laser diodes
are more expensive and add to the cost of the instrument. The light detector
used in the NIRO series of cerebral oximeters is a photomultiplier tube (PMT).
Once again, the PMT amplifies the reflected NIR making the measurements
more accurate than SiPDs. The disadvantage is that PMT requires an additional
connection to the patient, and it must be precisely spaced from the light source;
greater separation allows a reading of deeper tissue but also results in greater
scatter and less accuracy. Because of its high sensitivity, the PMT is more
vulnerable to contamination by ambient light. The advantages of the SiPDs
over PMT are their small size and high efficiency, which allows it to be
mounted as part of the forehead sensor assembly.
Two cerebral oximeters (INVOS and NIRO) measure different things and
provide different outputs for interpretation by the clinicians. INVOS presents a
single numerical value for regional rSO2, persumably of the cerebrovascular
tissue bed under the sensor applied to the forehead. A trend of changes over time
is continuously displayed on the oscilloscope. NIRO-oximeters continuously
display values for reduced oxygenated and total hemoglobin and Cyt aa3. It
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 299

should be emphasized that with both types of instruments, monitoring of trends
(changes over time) are more important than absolute values.
Despite the greater sophistication of the NIRO 500, Cho et al [22] found the
INVOS (in its earlier version, INVOS 3100A) to be as accurate as the NIRO,
and Grubhofer et al [23] found the INVOS 3100 to be the more accurate of
the two.
Jobsis used transmitted light, shown across the greatest length of the tissue
beds, in his original experiments. To decrease the path length (to minimize light
attenuation), commercially available instruments use reflected light, measured a
shorter distance from the source of the light. In the reflective method, light passes
across a parabolic path, which can be made longer (deeper) or shorter (shallower),
depending on the distance between the light source and detector. Regional
monitoring of cerebral oxygenation thus becomes possible [24].
There is no gold standard against which to measure the accuracy and validity
of NIRS. There has been much work to best quantify what is being measured by
NIRS and how valid NIRS is. The major difference between pulse oximeters and
cerebral oximeters is that transmission of NIR is ‘‘gated’’ by the arterial pulse in
pulse oximeters but is more or less continuous in cerebral oximeters. Therefore,
pulse oximeters measure oxygen saturation of hemoglobin in arterial blood while
cerebral oximeters measure hemoglobin in the entire tissue bed, which includes a
mixture of brain tissue, arterial, and venous blood. Because the ratio of arterial
and venous blood is about 16:84 and, because this ratio stays the same during
normoxia, hypoxia, and hypocapnia [25,26], NIRS primarily measures cerebral
venous saturation.
Clinical use
Even before cerebral oximeters became commercially available for clinical
use, the first publication of the NIR absorption spectrum of Cyt aa3 by Jobsis in
1977 had stimulated a keen interest of clinicians in this technology, resulting in
quite a few laboratory and clinical studies. In the last decade, the INVOS cerebral
oximeter became commercially available in the United States, and has been more
frequently used in clinical studies from the United States, while NIRO 500 or
NIRO 1000 oximeters have been more frequently used in England and other
European countries. A large body of literature dealing with transcranial oximetry
has thus accumulated in the last 2 decades. However, the majority of publications
are in the form of case reports or a small series of a few patients and number of
well-designed prospective clinical studies clearly showing clinical utility is rel-
atively small. For the sake of brevity, we will review only the pertinent clinical
studies here instead of burdening the readership with an exhaustive review of the
literature on this subject.
Early studies used concentration monitors, which were prototypes instru-
ments, for validation of technology in small animals, and were quickly followed
by clinical studies in pediatric patients in the 1980s. These studies established that
concentration monitors (which used the NIR technology similar to that used in
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313300

NIRO 500) were successful in tracking changes in the concentration of Hb,
HbO2, and oxidized Cyt aa3. These instruments used a variety of algorithms and
reported results in arbitrary units, such that it is not possible to compare the
results obtained in different investigations. In these investigations each subject
(patient) acted as its own control. Therefore, one could only track changes in Hb,
HbO2, and Cyt aa3, and it was not possible to define normative data for the entire
patient population. However, combined results of several clinical investigations
[27–33] established that cerebral oximetry, using concentration monitors based
on NIR technology, can track changes in the cerebral oxygen supply and
utilization as well as changes in the intracranial blood volume secondary to
changes in PaCO2, hypoxemia, drug therapy, mental work [34,35], cardiopulmo-
nary bypass, induction of anesthesia, and extracorporeal membrane oxygenation.
Cerebral oxygenation determined by these instruments has been shown to
correlate with cerebral blood flow changes produced by acetazolamide injection
or carotid occlusion [36–38] as well as with PaO2.
More recently, it has been shown that cerebral oximetry with an NIRO 500
type of instrument (NIRO 1000) can register changes in cerebral oxygenation due
to carotid cross-clamping and shunt insertion (during carotid endarterectomy)
without significant contamination from extracranial circulation [39]. A decrease
in HbO2 corresponded with a decrease in middle cerebral artery blood flow
velocity measured by a transcranial Doppler. However, an association (or lack
thereof ) between the decrease in HbO2 and changes in sensorium was not
studied, as the operations were performed under general anesthesia. In patients
with closed-head injury [40], admitted to the neurointensive care unit, it has been
shown that cerebral oximetry (using NIR 1000) successfully detected 97%
episodes of brain hypoperfusion (related to changes in cerebral perfusion
pressure, accompanied by changes in middle cerebral artery blood flow velocity),
while only 53% of the episodes were detected by continuous monitoring of
jugular venous saturation. Although this finding emphasized the potential use of
cerebral oximetry in the neurointensive care unit, it also pointed out the potential
for contamination by electronic artifacts in the ICU setting. In this study, after
886 hours of continuous monitoring, data for only 376 hours (42.4%) could be
considered artifact free. Once again, this investigation did not comment on the
findings of cerebral oximetry and clinical outcome. From a brief review of the
literature it can be seen that lack of outcome studies and the cost and FDA
approval remained major hurdles for widespread clinical use of these instruments
in the United States.
In 1991, Somanetics1 developed a saturation monitor (INVOS series) based
on technology similar to that used in pulse oximeters. Prototype instruments
based on the technology used in the development of INVOS 3100 were validated
first in animals and then in clinical studies [41]. At that time this technology was
different then previously used spectroscopy techniques in that it used a
reflectance mode rather than a transillumination mode of spectroscopy. Since
then, prototypes of NIRO 500 have also been developed to work in the
reflectance mode. It should be emphasized that instruments which use reflect-
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 301

ance spectroscopy provide a measure of ‘‘regional’’ rather than ‘‘global’’ cerebral
oxygenation. The second major difference in this category of instruments is that
mathematical modeling used avoids any attempt to generate a definitive value for
the tissue content of a given chromophore, and generates a ratio of two
chromophores, Hb and HbO2. The algorithm used in the calculation of cere-
brovascular saturation (rSO2) measured by INVOS instruments is based on the
assumption that path length is not dependent on wavelength, and remains
relatively constant over a narrow range of NIR wavelengths (between 650 and
850 nm) used in this instrument. Simplification of technology used in the
development of saturation monitors may result in some potential sources of
error. As mentioned before, and common to all instruments, the effect of light
reflection and scattering is unknown. Another potential limitation of the
measurement obtained is the validity of using a molar extinction in vivo that
is inferred from in vitro work. The assumption that path length remains constant
for NIR in wavelengths used may not be absolutely correct. The potential
influence of contamination by extracranial blood flow and changes in cerebral
blood flow and intracranial blood volume secondary to head injury or surgical
trauma remains unknown. These limitations in technology were somewhat off set
by the small size suitable for bedside use, low cost, user friendliness, and easy
availability in the United States. A fair number of clinical studies have been
conducted in recent years using INVOS monitors, with controversial results.
These investigations have also been conducted during a time when the monitors
and the sensors used with those monitors were being constantly upgraded. It is,
therefore, difficult to compare the results reported in different studies even
though the same equipment was used. One can say that, in a sense, the FDA
approval of this instrument was somewhat premature, as became evident by the
fact that in 1994 FDA rescinded the approval and required further data
collection, and has only very recently (June 1996) approved this device again
for clinical use in adult patients only. The clinical studies using this device
between 1991 and 1994 have reported mixed results regarding the efficacy of
prototypes of this device. Results of these studies are briefly reviewed below.
McCormick and associates [42] demonstrated the sensitivity of rSO2, measured
by INVOS, to transient cerebral hypoxia produced by inhalation of a hypoxic gas
mixture in humans. Ausman and associates [43] used INVOS to monitor rSO2 in
seven patients undergoing intracranial aneurysm surgery facilitated by deep
hypothermic circulatory arrest. They observed that circulatory arrest at 18�C was
associated with a significant progressive decrease in rSO2. In five patients with
no neurological damage, rSO2 remained above 35%, and in one who had rSO2
less than 35% there was postmortem evidence of global cerebral hypoxia. They
suggested that a value of rSO2 of 35% may be critical, and values below that
may be used to predict poor neurological injury. We [44] have reported a patient
in whom an rSO2 reading of 32% was observed for 15 minutes during 30 minutes
of induced deep hypothermic circulatory arrest, without development of any
neurological deficit. Williams and associates [45] have reported a significant
correlation among SjvO2, rSO2, and middle cerebral artery blood flow velocity
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313302

during carotid cross-clamping in patients undergoing carotid endarterectomy
under general anesthesia.
Carotid endarterectomy (CEA) is potentially a human model of regional
cerebral ischemia, and hence, provides an ideal opportunity for validation of
rSO2 as a monitor of cerebral ischemia. It is therefore not surprising that cerebral
oximetry has been used in multiple studies in patients undergoing CEA. Un-
fortunately, most of these investigations have been done in patients under general
anesthesia, and performance of cerebral oximeters has been compared to other
monitors (SjvO2 EEG, SEPs, and TCD) that have their own limitations and
pitfalls. We have recently studied rSO2 changes in patients undergoing carotid
endarterectomy under regional anesthesia in two separate investigations [44,46],
and attempted to determine if there is an association between a decrease in rSO2
and development of a clinically detectable neurological deficit. In the first
investigation we observed a + 2.6% to � 28.6% change in ipsilateral rSO2
following carotid occlusion, but we were unable to identify a critical change that
may be associated with a clinically identifiable neurologic deficit. In a larger
series we determined that a mean ipsilateral decrease in rSO2 after carotid
occlusion was significantly greater (12.2 versus 4.8 units) in patients who
developed clinical signs suggestive of cerebral ischemia than in those who did
not. A 20% decrease (from preclamp value) after carotid occlusion provided the
best sensitivity (80%) and specificity (82.2%) for predicting cerebral ischemia.
The false-positive rate of this cutoff point was 66.7% and false-negative rate was
2.3%, thus providing a positive predictive value of 33.3% and a negative
predictive value of 97.4%.
Several investigators [47,48] have reported a lack of correlation between rSO2
readings recorded by INVOS and jugular bulb oxygen saturation (SjvO2)
measured by indwelling oximetric catheters. Such a lack of correlation is not
entirely surprising when one considers the fact that rSO2 reflects a regional value
while SjvO2 is a global measurement. In other words, the two are measuring
similar but not the same phenomenon. Lack of correlation between rSO2 and
SjvO2 may also suggest a limitation of the current algorithm used, which has
been recently validated by Pollard and associates [49,50]. rSO2 measured by
INVOS has also been reported to change with a change in PaCO2 as well as a
change in position (Trendelenburg) of the subject [51]. Some investigators
[48,52] have proposed that rSO2 readings recorded by INVOS-3100 are signifi-
cantly affected by changes in extracranial blood flow. Germon et al produced
changes in extracranial blood flow either by application of a tourniquet around
the forehead or by constant exercise of the temporalis muscle. Both these
maneuvers are capable of adding potential sources of error either by venous
congestion of the scalp or by movement artifact due to repeated muscle con-
tractions. We have assessed the contribution by extracranial blood flow to rSO2
recorded by INVOS by studying the changes in rSO2 in response to selective
clamping of external and internal carotid arteries. A mean decrease in rSO2 (from
67.4 ± 8.5 to 65.6 ± 8.3) after external carotid artery occlusion was not
statistically significant, while that following internal carotid artery (65.6 ± 8.3 to
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 303

61.4 ± 9.6) was significant [53]. These data suggest that although the algorithm
used in INVOS does not entirely eliminate extracranial contamination, the rSO2
readings provided by this oximeter are predominantly derived from the intracra-
nial compartment. Lam and associates [54] have reported similar findings using
NIRO 500.
Recent case reports have suggested that cerebral oximetry may be useful in
monitoring response to therapy in patients with intracranial vasospasm [55,56].
However, more rigorous investigations are required before any firm conclusions
can be drawn.
An investigation by Schwarz et al has supplied data that is interesting and also
disturbing [78]. These investigators used INVOS 3100 to measure rSO2 in
18 dead subjects and 15 healthy volunteers. The mean value for rSO2 in dead
subjects was 51 ± 26.8% compared to 68.4 ± 5.2% in volunteers. Six of the
dead subjects had values above the lowest values observed in healthy volunteers.
In five dead subjects, after removal of the brain at autopsy, a mean rSO2 reading
of 73.4 ± 13.3% was noted. This is an unusual use of transcranial cerebral
oximetry, and one for which this technology is not designed.
Based on the review of published literature, a few general statements can be
made regarding clinical use of cerebral oximeters:
1. Cerebral oximeters are only trend monitors where each patient acts as his/
her own control and no normative or comparative data applicable across
the entire patient population are available. Basically, these monitors
provide a number (or set of numbers) that still awaits accurate inter-
pretation and utility in clinical practice.
2. The use of prototype instruments and changing technology as the instru-
ments are being constantly upgraded adds to the difficulty in interpreting
results and in comparing the results of different studies. Instrumentation
used in many studies is not commercially available.
3. Only a few studies [43,46] have attempted to study the role of cerebral
oxygen saturation monitoring in predicting neurologic outcome in small
numbers of patients, and the data are far from conclusive. It is fair to
conclude that, at present, there are very few sizable prospective studies
evaluating the place of cerebral oximetry in either predicting or improving
the clinical outcome.
Limitations
Limitations of NIRS are the limitations of the technology itself. The most
important limitation may be the lack of definition of the boundaries of the brain
tissue being monitored. Superficial tissues will give the most accurate readings,
yet those tissues are usually of the least interest. Constructing an algorithm to
compensate for all the variables is a formidable task. The lack of a gold standard
against which to test such an algorithm makes validation difficult. More
prospective outcome studies involving sufficient numbers of patients are needed.
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313304

Lactate is the byproductof anaerobic glucose metabolism, and its accumula-
tion in cerobrospinal fluid is an indication that oxygen availability to the brain has
decreased to a level that cannot support aerobic mitochondrial respiration.
Menzel et al [76] used a Neurotrend probe in severe head-injury patients to
study, among other things, the effects of increased FiO2 and increased CBF on
PbtO2 and lactate levels in dialysate. Oxygen reactivity was calculated by a
change in PbtO2 in response to increased FiO2. Oxygen reactivity was then
related to clinical outcome 3 months later. Under normoxic conditions, there was
significant correlation between CBF and PbtO2, while FiO2 had an inverse
correlation with CBF. Under hyperoxic (FiO2=100%) conditions PbtO2 increased
and lactate in dialysate decreased, but the increase in PbtO2 was more
pronounced (87%) than the decreased in lactate (38%). Surprisingly, PbtO2
response to hyperoxia was also inversely related to the outcome at 3 months.
Taking that study a step further, Valadka also used intracerebral microdialysis as
well as PbtO2 and cerebral concentrations of lactate, glucose, glutamate, and
aspartate in five patients with refractory intracranial hypertension after severe
head injury. Glutamate and aspartate are intracellular amino acids that are
released with cellular necrosis. Lactate/glucose ratios correlated well with PbtO2
[77]. The group also noted that
Cerebral oxygen tension monitors
Monitors of PbtO2 have been developed as a modification of small intra-
vascular electrodes that were originally designed for continuous arterial blood gas
monitoring in patients with severe pulmonary disease, who required prolonged
mechanical ventilation. These monitors place a miniaturized oxygen detector
directly over or into brain parenchyma. The readings are direct, focal, and
accurate. For the measurement of oxygen tension within the brain matter
surrounding the oxygen probe, this is as close to a gold standard as we now
have [57].
Methodology
Currently, probes made by two manufacturers are available for PbtO2
monitoring. The Licox probe (G.MS. Kiel-Mielkendorf, Germany) consists of
a miniaturized Clark-type polarized amperometric (also known as ‘‘polaro-
graphic’’) circuit separated from brain tissue by a membrane across which only
oxygen can diffuse. The oxygen sensor is at the very tip of the catheter. The
catheter is 0.8 mm in diameter. The probe monitors oxygen tension in 7.9 sq mm
of brain tissue. The catheter is normally placed into the frontal cortex and held in
place by a screw in the frontal bone. The Neurotrend probe (Diametrics, St. Paul,
MN) has been developed as a modification of the multiple electrode system
(paratrend) that was originally designed for intra-arterial insertion for continuous
monitoring of arterial blood gasses. The Neurotrend probe combines fiber optics,
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 305

a modified Clark-type oxygen sensor, as well as carbon dioxide and hydrogen ion
concentration sensors (spectrophotometry), and a thermocouple temperature
sensor. The oxygen sensor on the Neurotrend is about 2.5 mm from the catheter
tip, which means the catheter must be placed at a greater depth in to the brain
parenchyma (than the Licox probe) to measure oxygen tension. This makes it
difficult to know (with certainty) whether the oxygen sensor is in gray or white
matter of the cerebral cortex. The catheter width is 0.5 mm, and is placed in a
manner similar to the Licox catheter [58].
Validation and clinical use
Dings et al [59,60] have extensively studied the Licox probes (one series of
118 probes in 101 patients and another in a series of 73 probes in 70 patients).
They found only two iatrogenic hematomas and no infections after an average of
6.7 days of monitoring. After 7 days of monitoring, a drift was found to occur in
the readings (a sensitivity drift of � 10.3 ± 17.3% in the first 1–4 days of use to
� 6.8 ± 13.4% after a week). No infections were seen, and the only complica-
tions noted were four clinically insignificant hematomas. In the larger study,
dislocation of or defect in the catheter occurred 13.6% of the time.
Sarrafzadeh et al [61] did a side-by-side comparison of the Licox and
Paratrend probes in seven severely head-injured patients (GCS < 8). Probes were
placed in various combinations into nonlesioned, pericontusional, or contusioned
brain tissue, and catheter position was checked with a CT scan. In similar tissue,
there was a close correlation of readings obtained by the two probes (mean
difference of < 5 mmHg after 20 hours of monitoring). A similar decrease in
readings was observed during periods of significant reductions of mean arterial
blood pressure and CPP. They noted that the contusioned and pericontusional
regions had the lowest oxygen readings and were, therefore, most at risk for
reinjury. However, they also noted that these injured areas were less reactive to a
significant decreases in CPP than areas of noninjured brain. Their conclusion was
that probes should be placed in nonlesioned areas because those areas were most
responsive to changes in oxygen delivery.
Critical values of PbtO2
Most of the clinical studies with PbtO2 have involved the patients in NICU,
and have attempted to correlate the observations of PbtO2 with clinical outcome.
Valadka et al [62] used either a Licox (n = 39) or Paratrend (n = 4) probe in 43
severely head-injured patients. PbtO2 data were analyzed by comparing average
time duration for which PbtO2 was < 2, 4, 6, 8, 15, or 20 Torr, and its association
with outcome as determined by survival, 3 months after initial head injury. It was
concluded that the likelihood of death increased with increasing duration of
PbtO2 < 15 Torr or with any occurence of PbtO2 < 6 Torr.
Bardt et al [63] studied 35 patients with severe head injury and found that
56% of the patients with more than 300 minutes of PbtO2 < 10 mmHg died,
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313306

22% had an unfavorable outcome, and 22% had a favorable outcome. In a
study of 22 patients with severe head injury van Santbrink et al [64] found that
PbtO2 values of � 5 mmHg within 24 hours after trauma were associated with
poor outcome.
Doppenberg et al [65,66] have attempted to determine a ‘‘critical’’ value of
PbtO2 that will be associated either with cerebral infarction (in cats) or cerebral
ischemia or poor clinical outcome in humans. Cerebral infarction was produced
by occlusion of middle cerebral artery in cats. In humans, regional CBF was
measured using a stable Xenon-CT.CBF technique. In the model of cerebral
infarction (after 4–6 hours of MCA occlusion), observed values of PbtO2 were
between 19–23 Torr. CBF decrease to ischemic threshold (18 mL/100 g/min) in
humans was also accompanied by PbtO2 reading of 22 Torr. They, therefore,
suggested that PbtO2 values between 19–23 should be considered critical, and
are likely to be associated with cerebral ischemia.
Critical values for cerebral perfusion pressure/CCP to maintain PbtO2
Several authors have used PbtO2 probes to study the effect of raising
cerebral perfusion pressure either by increasing mean arterial pressure or
lowering intracranial pressure [67–71]. The conclusions were strikingly similar.
PbtO2 was best maintained with a CPP of 60 mmHg. Raising it above that
figure did not improve oxygenation. Further, the best way of raising CPP was
by increasing mean arterial pressure. Using hyperventilation or mannitol
successfully raised CPP by lowering ICP, but the use of those modalities
caused a decrease in PbtO2.
Effect of inhaled anesthetics on PbtO2
Hoffman et al [72–75] have performed a series of studies comparing the effect
of an intravenous anesthetic with that of an inhaled anesthetic on PbtO2. In each
case, the i.v. anesthetic (Pentothal, etomidate, or propofol), in a dose sufficient to
produce EEG burst suppression, produced a lowering of PbtO2. This is to be
expected, because these agents lower cerebral metabolic rate, decrease cerebral
blood flow, and, therefore, decrease oxygen delivery to the brain. When the
inhaled anesthetic was used at a high dose (i.e., 3% isoflurane), PbtO2 was found
to rise from baseline in each case. The conclusion was that high-dose isoflurane
(or desflurane) had an attenuating effect on CMRO2–CBF coupling. This is not
surprising, and is in keeping with known effects of inhalation anesthetics on CBF
and CMRO2. The importance of cerebral CMRO2–CBF coupling was also
emphasized in a study by van Santbrink et al [64] using PbtO2 in patients with
severe head injury, who found that a significant rise in PbtO2 following an increase
of FiO2 to 100% was associated with a bad outcome. The authors suggested that
the loss of CMRO2–CBF coupling may reflect severity of cerebral injury.
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 307

Effect of change of PBTO2 on lactate levels
Lactate is the byproduct of anaerobic glucose metabolism, and its accumula-
tion in cerebrospinal fluid is an indication that oxygen availability to the brain has
decreased to a level that cannot support aerobic mitochondrial respiration.
Menzel et al [76] used a Neurotrend probe in severe head-injury patients to
study, among other things, the effects of increased FiO2 and increased CBF on
PbtO2 and lactate levels in dialysate. Oxygen reactivity was calculated by a
change in PbtO2 in response to increased FiO2. Oxygen reactivity was then
related to clinical outcome 3 months later. Under normoxic conditions, there was
significant correlation between CBF and PbtO2, while FiO2 had an inverse
correlation with CBF. Under hyperoxic (FiO2 = 100%) conditions PbtO2 in-
creased and lactate in dialysate decreased, but the increase in PbtO2 was more
pronounced (87%) than the decrease in lactate (38%). Surprisingly, PbtO2
response to hyperoxia was also inversely related to the outcome at 3 months.
Taking that study a step further, Valadka also used intracerebral microdialysis as
well as PbtO2 to study the relationship between PbtO2 and cerebral concen-
trations of lactate, glucose, glutamate, and aspartate in five patients with re-
fractory intracranial hypertension after severe head injury. Glutamate and
aspartate are intracellular amino acids that are released with cellular necrosis.
Lactate/glucose ratios correlated well with PbtO2 [77]. The group also noted that
glutamate and aspartate concentrations both correlated with PbtO2, and did not
rise until PbtO2 reached zero in these fatally injured patients. Glucose concen-
trations lagged behind PbtO2, and continued to decline for a short time after
PbtO2 reached zero. An increases in extracellular glutamate and aspartate were
not observed until both oxygen and glucose concentrations reached zero, sug-
gesting that glucose is used by the cells anaerobically once oxygen is depleted so
as to maintain structural integrity.
Limitations
The main limitation of PbtO2 monitoring is the fact that it is an invasive
procedure involving puncture of the brain parenchyma. It is, therefore, reserved
for patients who have either had severe traumatic injuries or are undergoing
neurosurgical procedures. Once the probe is properly in place, complications
have proven to be few. The Licox probe appears to be less likely to cause
complications because it is applied less deeply into brain tissue, while Neurotrend
probes will have to be inserted to a depth of at least 3 mm.
Summary
None of the monitors of cerebral oxygenation discussed above has proven to
be effective enough to have become a standard of care in any given area of
medical treatment. As described above, each has specific and well-defined
shortcomings that prevent its widespread use. These shortcomings may not be
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313308

so much a failure of technology as an acknowledgement of the complexity of our
goal: a monitor that can divide the entire brain into small, focal, and discrete areas
and accurately measure the oxygen tension in each one. Because we are asking
for the functional equivalent of 30 or 40 simultaneous PbtO2 probes, it is small
wonder that we are not yet satisfied.
Of the three monitors discussed here, the greatest potential may lie with the
transcranial cerebral oximetry. The cerebral oximeter has the biggest potential for
improvement because it holds the most potential for technical advancement.
Although, for instance, jugular venous bulb oximetric catheters may become
somewhat more accurate, the biggest drawbacks in that monitor’s usefulness lie in
human anatomy and intracerebral blood mixing, not catheter accuracy. PbtO2
probes, also, have little room for improvement. Although every technology can be
refined, the PbtO2 probes are already accurate. The fact that they are an invasive
monitor, and a regional one at that, will relegate them to a limited number of cases.
Cerebral oximeters hold more potential. Their greatest limitations lie in technical
aspects that can be, and hopefully will be, improved upon in terms of computer
technology as well as algorithm accuracy. The fact that cerebral oximeters can be
used on any patient, at any time, on almost any case, makes it, potentially, truly an
ideal monitor for anesthesiologists and intensivists alike. There is no certainty that
any of these limitations will be surmounted, at least to the degree necessary to
achieve desired accuracy. But there is much to anticipate.
References
[1] Andrews PJ, Dearden NM, Miller JD. Jugular bulb cannulation: description of a cannulation
technique and validation of a new continuous monitor. Br J Anaesth 1991;67:553–8.
[2] Cruz J. Cerebral oxygenation monitoring. Crit Care Med 1993;21:1242–6.
[3] Sheinberg M. Continuous monitoring of jugular venous oxygen saturation in head-injured pa-
tients. J Neurosurg 1992;76:212–7.
[4] Obrist W. Cerebral blood flow and metabolism in comatose patients with acute head injury:
relationship to intracranial hypertension. J Neurosurg 1988;68:241–53.
[5] Albin M. Testbook of neuroanesthesia with neurosurgical and neuroscience perspectives. New
York: McGraw-Hill Companies; 1977.
[6] Gibbs E, Lennox W, Nims L. Arterial and cerebral venous blood: arterial-venous differences in
man. J Bio Chem 1942;144:324.
[7] Matta BF, Lam AM. The rate of blood withdrawal affects the accuracy of jugular venous bulb.
oxygen saturation measurements. Anesthesiology 1997;86:806–8.
[8] Lyons C. Cerebral venous oxygen content during carotid thrombintimectomy. Ann Surg 1964;
160:561.
[9] Meyer JS, Gotoh F, Ebihara S, Tomita M. Effects of anoxia on cerebral metabolism and electro-
lytes in man. Neurology 1965;15:892–901.
[10] Lennox W, Gibbs F, Gibbs E. Relationship of unconsciousness to cerebral blood flow and to
anoxemia. Arch Neurol Psychiatry 1935;34:1001.
[11] Feldman Z. Monitoring of cerebral hemodynamics with jugular bulb catheters. Crit Care Clin
1997;13:51–77.
[12] Matta B. A critique of the intraoperative use of jugular venous bulb catheters during neuro-
surgical procedure. Anesth Analg 1994;79:745–50.
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 309

[13] Croughwell N. Warming during cardiopulmonary bypass. Ann Thorac Surg 1992;53:827–32.
[14] Nakajima T, Kuro M, Hayashi Y, Kitaguchi K, Uchida O, Takaki O. Clinical evaluation of
cerebral oxygen balance during cardiopulmonary bypass: on-line continuous monitoring of
jugular venous oxyhemoglobin saturation. Anesth Analg 1992;74:630–5.
[15] Nakajima T, Ohsumi H, Kuro M. Accuracy of continuous jugular bulb venous oximetry during
cardiopulmonary bypass. Anesth Analg 1993;77:1111–5.
[16] Jobsis FF. Noninvasive, infrared monitoring of cerebral and myocardial oxygen sufficiency and
circulatory parameters. Science 1977;198:1264–7.
[17] Madsen PL, Skak C, Rasmussen A, Secher NH. Interference of cerebral near-infrared oximetry
in patients with icterus. Anesth Analg 2000;90:489–93.
[18] Porter H. Mitochondrocupein. In: Peisach J, editor. The biochemistry of copper. New York:
Academic Press; 1996. p. 159–72.
[19] Giltvedt J, Sira A, Helme P. Pulsed multifrequency photoplethysmograph. Med Biol Eng Com-
put 1984;22:212–5.
[20] Cooper CE, Springett RJ, Panagiotopoulou A, Penrice J. Near infrared spectroscopy of nitrosyl
haemoglobin—relevance to in vivo detection of nitric oxide. Biochem Soc Trans 1996;24:448S.
[21] Roberts I, Fallon P, Kirkham FJ, Lloyd-Thomas A, Cooper C, Maynard R, et al. Estimation of
cerebral blood flow with near infrared spectroscopy and indocyanine green. Lancet 1993;
342:1425.
[22] Cho H, Nemoto EM, Sanders M, Fernandez K, Yonas H. Comparison of two commercially
available near-infrared spectroscopy instruments for cerebral oximetry. Technical note. J Neuro-
surg 2000;93:351–4.
[23] Grubhofer G, Tonninger W, Keznickl P, Skyllouriotis P, Ehrlich M, Hiesmayr M, et al. A
comparison of the monitors INVOS 3100 and NIRO 500 in detecting changes in cerebral oxy-
genation. Acta Anaesthesiol Scand 1999;43:470–5.
[24] Williams I. Recent developments in cerebral monitoring—near infrared light spectroscopy. An
pverview. Eur J Vasc Endovasc Surg 1996;12:263–71.
[25] Mehedlishvili G. Cerebral arterial behavior providing constant cerebral blood flow, pressure, and
volume. In: Bevan JA, editor. Arterial behavior and blood circulation in the brain. New York:
Plenum Press; 1986. p. 42–95.
[26] Watzman HM, Kurth CD, Montenegro LM, Rome J, Steven JM, Nicolson SC. Arterial and
venous contributions to near-infrared cerebral oximetry. Anesthesiology 2000;93:947–53.
[27] Ferrari M, De Marchis C, Giannini I, Di Nicola A, Agostino R, Nodari S, et al. Cerebral blood
volume and hemoglobin oxygen saturation monitoring in neonatal brain by near IR spectroscopy.
Adv Exp Med Biol 1986;200:203–11.
[28] Wyatt JS, Cope M, Delpy DT, Wray S, Reynolds EO. Quantification of cerebral oxygenation and
haemodynamics in sick newborn infants by near infrared spectrophotometry. Lancet 1986;
2:1063–6.
[29] Hampson NB, Camporesi EM, Stolp BW, Moon RE, Shook JE, Griebel JA, et al. Cerebral
oxygen availability by NIR spectroscopy during transient hypoxia in humans. J Appl Physiol
1990;69:907–13.
[30] Liem KD, Hopman JC, Kollee LA, Oeseburg B. Assessment of cerebral oxygenation and
hemodynamics by near infrared spectrophotometry during induction of ECMO: preliminary
results. The ECMO Research Group. Adv Exp Med Biol 1992;317:841–6.
[31] Skov L, Pryds O, Greisen G, Lou H. Estimation of cerebral venous saturation in newborn infants
by near infrared spectroscopy. Pediatr Res 1993;33:52–5.
[32] van Bel F, Dorrepaal CA, Benders MJ, Zeeuwe PE, van de Bor M, Berger HM. Changes in
cerebral hemodynamics and oxygenation in the first 24 hours after birth asphyxia. Pediatrics
1993;92:365–72.
[33] Hock C, Muller-Spahn F, Schuh-Hofer S, Hofmann M, Dirnagl U, Villringer A. Age dependency
of changes in cerebral hemoglobin oxygenation during brain activation: a near-infrared spectro-
scopy study. J Cereb Blood Flow Metab 1995;15:1103–8.
[34] Villringer A, Planck J, Hock C, Schleinkofer L, Dirnagl U. Near infrared spectroscopy (NIRS): a
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313310

new tool to study hemodynamic changes during activation of brain function in human adults.
Neurosci Lett 1993;154:101–4.
[35] Villringer A, Planck J, Stodieck S, Botzel K, Schleinkofer L, Dirnagl U. Noninvasive assessment
of cerebral hemodynamics and tissue oxygenation during activation of brain cell function in
human adults using near infrared spectroscopy. Adv Exp Med Biol 1994;345:559–65.
[36] Kaminogo M. Effect of acetazolamide on regional cerebral oxygen saturation and regional
cerebral blood flow. Stroke 1995;26:2358–60.
[37] Piepgras A, Guckel F, Lammler B, Weigel R, Schmiedek P. Non-invasive diagnosis of cerebral
ischemia with nuclear magnetic resonance tomography and near-infrared spectroscopy. Radiol-
ogy 1994;34:627–31.
[38] Kuroda S, Houkin K, Abe H, Tamura M. Cerebral hemodynamic changes during carotid artery
balloon occlusion monitored by near-infrared spectroscopy. Neurol Med Chir (Tokyo) 1996;
36:78–86.
[39] Kirkpatrick PJ, Smielewski P, Whitfield PC, Czosnyka M, Menon D, Pickard JD. An obser-
vational study of near-infrared spectroscopy during carotid endarterectomy [see comments].
J Neurosurg 1995;82:756–63.
[40] Kirkpatrick PJ, Smielewski P, Czosnyka M, Menon DK, Pickard JD. Near-infrared spectroscopy
use in patients with head injury [see comments]. J Neurosurg 1995;83:963–70.
[41] McCormick PW, Stewart M, Goetting MG, Dujovny M, Lewis G, Ausman JI. Noninvasive
cerebral optical spectroscopy for monitoring cerebral oxygen delivery and hemodynamics. Crit
Care Med 1991;19:89–97.
[42] McCormick PW, Stewart M, Goetting MG, Balakrishnan G. Regional cerebrovascular oxygen
saturation measured by optical spectroscopy in humans. Stroke 1991;22:596–602.
[43] Ausman JI, McCormick PW, Stewart M, Lewis G, Dujovny M, Balakrishnan G, et al. Cerebral
oxygen metabolism during hypothermic circulatory arrest in humans. J Neurosurg 1993;79:
810–5.
[44] Samra SK, Dorje P, Zelenock GB, Stanley JC. Cerebral oximetry in patients undergoing carotid
endarterectomy under regional anesthesia. Stroke 1996;27:49–55.
[45] Williams I. Light-reflective cerebral oximetry and jugular bulb venous oxygen saturation during
carotid endarterectomy. Br J Surg 1994;81:1291–5.
[46] Samra SK, Dy EA, Welch K, Dorje P, Zelenock GB, Stanley JC. Evaluation of a cerebral
oximeter as a monitor of cerebral ischemia during carotid endarterectomy. Anesthesiology
2000;93:964–70.
[47] Brown R, Wright G, Royston D. A comparison of two systems for assessing cerebral venous
oxyhaemoglobin saturation during cardiopulmonary bypass in humans. Anaesthesia 1993;
48:697–700.
[48] Harris DN, Bailey SM. Near infrared spectroscopy in adults. Does the Invos 3100 really measure
intracerebral oxygenation? Anaesthesia 1993;48:694–6.
[49] Pollard V, Prough DS, DeMelo AE, Deyo DJ, Uchida T, Stoddart HF. Validation in volunteers
of a near-infrared spectroscope for monitoring brain oxygenation in vivo. Anesth Analg 1996;
82:269–77.
[50] Pollard V, Prough DS. Cerebral near-infrared spectroscopy: a plea for modest expectations
[editorial; comment]. Anesth Analg 1996;83:673–4.
[51] Pollard V, Prough DS, DeMelo AE, Deyo DJ, Uchida T, Widman R. The influence of carbon
dioxide and body position on near-infrared spectroscopic assessment of cerebral hemoglobin
oxygen saturation. Anesth Analg 1996;82:278–87.
[52] Germon TJ, Kane NM, Manara AR, Nelson RJ. Near-infrared spectroscopy in adults: effects of
extracranial ischaemia and intracranial hypoxia on estimation of cerebral oxygenation. Br J
Anaesth 1994;73:503–6.
[53] Samra SK, Stanley JC, Zelenock GB, Dorje P. An assessment of contributions made by ex-
tracranial tissues during cerebral oximetry [in process citation]. J Neurosurg Anesthesiol 1999;
11:1–5.
[54] Lam JM, Smielewski P, al-Rawi P, Griffiths P, Pickard JD, Kirkpatrick PJ. Internal and external
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 311

carotid contributions to near-infrared spectroscopy during carotid endarterectomy. Stroke
1997;28:906–11.
[55] Luer MS, Dujovny M, Slavin KV, Hernandez-Avila G, Ausman JI. Regional cerebral oxygen
saturation during intra-arterial papaverine therapy for vasospasm: case report. Neurosurgery
1995;36:1033–6.
[56] Ekelund A, Kongstad P, Saveland H, Romner B, Reinstrup P, Kristiansson KA, et al. Trans-
cranial cerebral oximetry related to transcranial Doppler after aneurysmal subarachnoid haemor-
rhage. Acta Neurochir 1998;140:1029–35.
[57] Dings J, Meixensberger J, Roosen K. Brain tissue pO2-monitoring: catheterstability and com-
plications. Neurol Res 1997;19:241–5.
[58] Hutchinson PJ, Al-Rawi PG, O’Connell MT, Gupta AK, Maskell LB, Hutchinson DB, et al.
Monitoring of brain metabolism during aneurysm surgery using microdialysis and brain multi-
parameter sensors. Neurol Res 1999;21:352–8.
[59] Dings J, Meixensberger J, Jager A, Roosen K. Clinical experience with 118 brain tissue oxygen
partial pressure catheter probes. Neurosurgery 1998;43:1082–95.
[60] Dings J, Meixensberger J, Amschler J, Hamelbeck B, Roosen K. Brain tissue pO2 in relation to
cerebral perfusion pressure, TCD findings and TCD-CO2-reactivity after severe head injury.
Acta Neurochir 1996;138:425–34.
[61] Sarrafzadeh AS, Kiening KL, Bardt TF, Schneider GH, Unterberg AW, Lanksch WR. Cerebral
oxygenation in contusioned vs. nonlesioned brain tissue: monitoring of PtiO2 with Licox and
Paratrend. Acta Neurochir 1998;71:186–9.
[62] Valadka AB, Gopinath SP, Contant CF, Uzura M, Robertson CS. Relationship of brain tissue
PO2 to outcome after severe head injury. Crit Care Med 1998;26:1576–81.
[63] Bardt T, Uterberg A, Hartl R. Monitoring of brain tissue PO2 in traumatic brain injury: effect of
cerebral hypoxia on outcome. Acta Neurochir 1998;(Suppl 71):153–6.
[64] van Santbrink H, Maas AI, Avezaat CJ. Continuous monitoring of partial pressure of brain tissue
oxygen in patients with severe head injury. Neurosurgery 1996;38:21–31.
[65] Doppenberg EM, Zauner A, Bullock R, Ward JD, Fatouros PP, Young HF. Correlations between
brain tissue oxygen tension, carbon dioxide tension, pH, and cerebral blood flow—a better way
of monitoring the severely injured brain? Surg Neurol 1998;49:650–4.
[66] Doppenberg EM, Zauner A, Watson JC, Bullock R. Determination of the ischemic threshold for
brain oxygen tension. Acta Neurochir 1998;(Suppl 71):166–9.
[67] Kiening KL, Hartl R, Unterberg AW, Schneider GH, Bardt T, Lanksch WR. Brain tissue pO2-
monitoring in comatose patients: implications for therapy. Neurol Res 1997;19:233–40.
[68] Kiening KL, Unterberg AW, Bardt TF, Schneider GH, Lanksch WR. Monitoring of cerebral
oxygenation in patients with severe head injuries: brain tissue PO2 versus jugular vein oxygen
saturation. J Neurosurg 1996;85:751–7.
[69] Unterberg AW, Kiening KL, Hartl R, Bardt T, Sarrafzadeh AS, Lanksch WR. Multimodal
monitoring in patients with head injury: evaluation of the effects of treatment on cerebral oxy-
genation. J Trauma 1997;42:S32–7.
[70] al-Rawi PG, Hutchinson PJ, Gupta AK, Piechnik SK, Pickard JD, Kirkpatrick PJ. Multiparam-
eter brain tissue monitoring—correlation between parameters and identification of CPP thresh-
olds. Zentralbl Neurochir 2000;61:74–9.
[71] Schneider GH, Sarrafzadeh AS, Kiening KL, Bardt TF, Unterberg AW, Lanksch WR. Influence
of hyperventilation on brain tissue-PO2, PCO2, and pH in patients with intracranial hyper-
tension. Acta Neurochir Suppl (Wein); 1998;71:62–5.
[72] Hoffman WE, Charbel FT, Edelman G, Ausman JI. Thiopental and desflurane treatment for brain
protection. Neurosurgery 1998;43:1050–3.
[73] Hoffman WE, Charbel FT, Edelman G, Misra M, Ausman JI. Comparison of the effect of
etomidate and desflurane on brain tissue gases and pH during prolonged middle cerebral artery
occlusion. Anesthesiology 1998;88:1188–91.
[74] Hoffman WE, Edelman G. Enhancement of brain tissue oxygenation during high dose isoflurane
anesthesia in the dog. J Neurosurg Anesthesiol 2000;12:95–8.
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313312

[75] Hoffman WE, Edelman G. Isoflurane increases brain oxygen reactivity in dogs. Anesth Analg
2000;91:637–41.
[76] Menzel M, Rieger A, Roth S, Soukup J, Peuse C, Hennig C, et al. Simultaneous continuous
measurement of pO2, pCO2, pH and temperature in brain tissue and sagittal sinus in a porcine
model. Acta Neurochir 1998;(Suppl 71):183–5.
[77] Valadka AB, Goodman JC, Gopinath SP, Uzura M, Robertson CS. Comparison of brain tissue
oxygen tension to microdialysis-based measures of cerebral ischemia in fatally head-injured
humans. J Neurotrauma 1998;15:509–14.
[78] Schwarz G. J Neurosurg Anesthesiol. 1996;8:189–93.
P.R. Smythe, S.K. Samra / Anesthesiology Clin N Am 20 (2002) 293–313 313

Brain protection during neurosurgery
Verna L. Baughman, MDDivision of Neuroanesthesiology, Departments of Anesthesiology and Neurosurgery,
University of Illinois at Chicago, Suite 3200, 1740 W. Taylor Street (M/C 515),
Chicago, IL 60612, USA
Protecting the brain from ischemia during neurosurgery is one of the most im-
portant concerns for anesthesiologists. It is amazing that, to my knowledge, there
is a paucity of prospective randomized controlled clinical trials comparing
different treatments upon which to base cerebral protectant therapy. However,
there is a wealth of laboratory research, both in vivo and in vitro, which supply the
neuroanesthesiologist with theories that guide the management of patients at risk
for cerebral ischemia.
There are three major themes to this chapter. The first section reviews the
research that led to the establishment of barbiturates as the gold standard for
cerebral protection. The second discusses current methods of providing intra-
operative cerebral protection. The third examines new and exciting possibilities
regarding therapy/drugs that may become important tools in the future for
cerebral protection.
The past: the development of barbiturates as the gold standard for
cerebral protection
A brief examination of the historical sequence of barbiturate use for cerebral
protection provides insight into not only the choice of this drug category but also
the proposed mechanisms of ischemia. The classic theory of cerebral protection is
based on the concept that by decreasing cerebral metabolic demand, the neuronal
survival will improve during periods of inadequate cerebral blood flow (CBF).
Because barbiturates decrease cerebral metabolism, it was the first drug group to
be considered as a potential cerebral protectant.
In the 1970s Michenfelder demonstrated that barbiturates decreased cerebral
metabolic activity in a dose-dependent manner, which produced a progressive
decrease in EEG activity, a reduction in the rate of ATP depletion, and protection
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00004 -9
E-mail address: [email protected] (V.L. Baughman).
Anesthesiology Clin N Am
20 (2002) 315–327

from incomplete cerebral ischemia [1–3]. Elimination of the metabolic require-
ment for EEG activity permitted this energy to be available for neuronal basal
metabolic needs. Current clinical practices of providing cerebral protection are
based on this concept. When the EEG is isoelectric, neuronal energy consumption
is decreased by approximately 50%. Therefore, with barbiturate treatment to an
isoelectric EEG during ischemia, all metabolic energy is used for maintenance of
cellular integrity. Additional barbiturate dosing produces no further reduction in
cerebral metabolism.
An early study by Bleyaert [4] supported the use of barbiturates as a
cerebral protectant. Using a neck tourniquet to completely eliminate blood
flow to the brain, the authors reported good neurologic outcome in barbiturate-
pretreated (thiopental, 90 mg/kg) monkeys compared to control animals. How-
ever, when Gisvold [5] repeated this experiment he was unable to reproduce
the positive results. This difference is probably due not to the drug treatment
but rather to the postoperative care. In the first study the barbiturate-treated
monkeys remained intubated and ventilated following reperfusion due to the
large barbiturate dose, whereas the control animals were extubated early and
returned to their cages without additional oxygen or intravenous fluids. In
the second study both barbiturate and control animals received similar post-
ischemia care. The difference in outcome disappeared when both groups
received identical ICU supportive treatment. In both studies EEG activity
disappeared with the initiation of complete cerebral ischemia (neck tourniquet
inflation), so it is reasonable to conclude that the drug-induced suppression of
EEG metabolic activity was immaterial because the EEG was abolished by the
study design.
The Brain Resuscitation Clinical Trial [6] confirmed the lack of barbiturate
protection in humans following complete absence of CBF. After resuscitation from
cardiac arrest patients were randomized to receive either thiopental (30 mg/kg,
infusion over time as blood pressure would permit) or saline. Mortality was high in
both groups (77% versus 80%). This human experiment confirmed that barbitu-
rates were ineffective in preventing or ameliorating cerebral ischemic damage that
occurred in the setting of complete ischemia (ie, no blood flow to the brain). With
cessation of CBF, the EEG becomes isoelectric within 1–2 minutes. Therefore,
any drug that suppresses EEG activity will be ineffective because the EEG is
already isoelectric.
Following up on the theory that barbiturates work only during incomplete
ischemia (ie, when EEG activity is still present during the ischemic period),
Nussmeier examined the protective potential of barbiturates when CBF was
substantially decreased but not completely interrupted [7]. She randomized
normothermic cardiac surgery patients to either thiopental 39.5 mg/kg infusion
or placebo. Neurologic outcome was improved in thiopental-treated patients
having valve replacement operations (in which the left ventricle was open, which
presumably resulted in cerebral air emboli with the reestablishment of circula-
tion). Zaidan [8] replicated Neussmeier’s study; however, he used hypothermic
cardiopulmonary bypass and found no difference between the two groups. The
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327316

most logical explanation for the difference in outcome between these two cardiac
surgery studies is that the barbiturate protective effect was invisible in the face of
the hypothermia treatment.
Summary
The conclusions derived from this research have shaped our clinical approach
to cerebral protection. Barbiturates decrease cerebral metabolism in a dose-
dependent manner until the EEG becomes isoelectric. Additional drug doses after
an isoelectric EEG provide no additional metabolic depression. Barbiturates
provide cerebral protection in the face of incomplete ischemia, but not with
complete cessation of CBF (complete ischemia). In situations where CBF is
completely arrested, EEG activity disappears within 90 seconds, so the admin-
istration of a drug to depress EEG metabolic activity would be irrelevant.
The present: current cerebral protection treatments
One would expect any anesthetic that depresses cerebral metabolism and EEG
activity to be similar to barbiturates in providing cerebral protection from
ischemia. The following section reviews current anesthetic drugs and evaluates
their potential for cerebral protection.
Etomidate
Etomidate, an intravenous sedative-hypnotic, is similar to barbiturates in
decreasing cerebral metabolism progressively until an isoelectric EEG appears
[9]. Unlike barbiturates, etomidate has very little effect on blood pressure, and a
short duration of action. For these reasons it was frequently used as a cerebral
protectant because it produced approximately 50% reduction in cerebral oxygen
demand while preserving cerebral perfusion pressure. Etomidate has demonstrat-
ed protection in some laboratory research models [10–12]; however, the results
are not universally positive [13,14], suggesting that etomidate might provide
protection only during mild to moderate ischemia. In some animal models,
etomidate initially decreases CBF to a greater degree than cerebral metabolism,
potentially putting the brain at risk of inadequate substrate delivery [15]. It
must also be remembered that etomidate produces adrenal depression (inhibition
of 11-B-hydroxylase), which caused increased mortality when it was used as a
continuous infusion for sedation in the ICU [16]. This inhibition lasts 4–6 hours
with a single dose, but is prolonged with continuous infusion or in elderly
critically ill patients [17].
Propofol
Propofol, introduced into clinical practice in the late 1980s, depresses cerebral
metabolism in a dose dependent manner, similar to barbiturates, producing
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327 317

isoelectric EEG at clinically relevant doses [18]. Rapid emergence from burst
suppression EEG may permit more accurate postanesthesia neurologic evalu-
ation. It has been used to provide brain protection in multiple laboratory studies;
however, no clinical studies compare its cerebral protection potency to barbitu-
rates. Because propofol has significant negative inotropic activity in addition
to vasodilatory properties, it can decrease cerebral perfusion pressure when
a large dose is administered over a short period of time. Propofol has been
shown to be superior to fentanyl–nitrous oxide anesthesia in a rat model of
incomplete ischemia [19] and equal to halothane in a regional cerebral ischemic
rat model [20]. Additionally, propofol may afford cerebral protection by its
antioxidant potential [21] or by acting as a glutamate antagonist at the N-methyl-
D-asparate (NMDA) receptor [22].
Opioids
Narcotic-based anesthesia has been a foundation for neuroanesthesia because
opioids have little effect on cerebral metabolism and blood flow while supporting
the cardiovascular system and cerebral perfusion pressure. Some literature ques-
tions the safety of narcotics (increased intracarnial pressuse—ICP) [23]. These
changes are small, and appear to be due to cerebral vasodilation in response to a
decrease in blood pressure [24]. Maintenance of blood pressure appears to reduce
or eliminate the mild increase in ICP. It has been reported that large doses of
opioids can produce seizure activity in animals [25]. However, the wide-spread
use of opioids in neuroanesthesia without evidence of seizure activity speaks to
the safety of this class of drugs. Evidence as to whether opioids produce neuro-
protection and the possible mechanism of this action is lacking.
Benzodiazepines
Benzodiazepines also depress cerebral metabolism in a dose-response manner;
however, they are not as potent as barbiturates (maximal decrease in cerebral
metabolism is 25–30%), and do not produce isoelectricity [13,26]. Because they
are unable to maximally suppress EEG activity, they have not been seriously
considered for cerebral protection.
Ketamine
Ketamine is a controversial drug in neuroanesthesia because it has been shown
to increase both cerebral metabolism and blood flow [27]. Animal studies re-
garding the effectiveness of ketamine as a cerebral protectant are both supportive
[28,29] and contradictory [30]. Recently, however, ketamine has been proposed
as an anesthetic drug that may provide cerebral protection because it blocks the
NMDA receptor, which is highly activated via enhanced excitatory neurotrans-
mitter release during ischemia [31]. In vitro studies show ketamine can also
interfere with transmembrane calcium influx [32]. Initial concern that ketamine
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327318

increases intracranial pressure in spontaneously breathing subjects has been
eliminated by demonstrating no increase in pressure when administered to
anesthetized, ventilated patients [33]. Ketamine’s place as a neuroprotectant is
still debatable.
Nitrous oxide
Nitrous oxide has been used in neuroanesthesia for many years. Its rapid on/
off action makes it a useful addition to the anesthetic plan. Despite its track
record, nitrous oxide possesses undesirable characteristics. Nitrous oxide
increases CBF, which could cause problems in patients with increased intracra-
nial pressure [34,35]. When used alone, nitrous oxide can increase CBF by 37%
and cerebral metabolism [36]. When used in combination with inhalational
anesthetics, the CBF increase persists, but to a lesser degree [37]. Whether these
vascular effects translate into ischemic injury is debatable, with some animal data
demonstrating worse outcome [38] while other studies show no effect [39].
Because it readily diffuses into air containing spaces, and because pneumo-
cephalus is evident in computerized tomography (CT scans) for up to 2 weeks
postcraniotomy, nitrous oxide should not be used during this time frame. Whether
or not the use of nitrous oxide is harmful has not been established in clini-
cal studies.
Inhalation anesthetics
Almost all of the inhalational anesthetic agents are similar to barbiturates in
producing progressive EEG depression in a dose-dependent manner until
obtaining electrical silence. This occurs at approximately 1.5–2 MAC. Concur-
rent with EEG suppression is a reduction in cerebral metabolism by approx-
imately 50% when the EEG is isoelectric. Because of this similarity to
barbiturates, inhalational anesthetics are frequently used for cerebral protection.
They produce less cardiovascular depression than the barbiturates, and are more
rapidly eliminated at the end of surgery. The exceptions are halothane and
enflurane. Halothane requires about 4 MAC for isoelectricity, which is clinically
impractical. Halothane also increases intracranial pressure by cerebral vaso-
dilation unless hyperventilation is initiated prior to the introduction of halothane.
Enflurane has been reported to produce seizure like activity on EEG, especially
when paired with hyperventilation.
Are there differences among the inhalational anesthetics in brain protection?
Laboratory and clinical studies suggest that they all provide cerebral protection,
but a direct comparison among all of the agents is lacking. Are they as good or
better than barbiturates? Multiple experiments have compared inhalational
anesthetics to barbiturates and other intravenous drugs. The results are variable.
A comparison between desflurane and thiopental in neurosurgical patients
showed an increase in brain oxygen (using a brain probe) with desflurane
when both were administered to EEG burst suppression [40]. Blood pressure
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327 319

was supported to maintain adequate CBF due to a loss of autoregulation. Are
these results drug specific or do they reflect the cerebral vascular effects of
these drug categories? A recent isoflurane study reported on its ability to mod-
ulate release of excitatory neurotransmitters and delay apoptosis (programmed
cell death), which may provide a window of opportunity for the administration
of other protective agents [41]. Detailed neuropsychiatric outcome studies are
needed to determine if there is a difference in neuroprotection among the
inhalational agents.
Temperature
The beneficial effect of hypothermia is well known. Hypothermia has long
been used during cardiopulmonary bypass and circulatory arrest surgery to
provide protection from cerebral ischemia. Initially it was felt that hypothermic
protection was based on a significant decrease in cerebral metabolism, allowing
the neurons to exist in almost a suspended energy consumption state. However, it
has subsequently been shown that profound hypothermia is not required to
protect the brain. Even mild levels have proven to be protective [42–44]. For
example, with rat global ischemia studies, marked hippocampal injury was seen
in 100% of rat brains following 20 minutes of ischemia when tested at 36�C.The injury decreased to 20% when studied at 34�C and 0% at 33�C [45]. This
protective effect, which has been reproduced by many investigators, cannot be
explained by changes in energy consumption during ischemia. For every degree
Centigrade decrease in temperature, cerebral metabolism is reduced by 5–7%.
Therefore, a reduction in temperature from 37�C to 34�C produces a 15–20%
reduction in cerebral metabolism, which is far less than the 50% decrease seen
with EEG silence. Obviously hypothermia’s protective effect is not mediated
solely by metabolic depression. Proposed mechanisms include suppression of
glutamate release [46,47], blunted nitric oxide production [48] which is involved
in producing oxygen free radicals, formation of free fatty acids [46], reduced
calcium influx [49], and increased gamma-aminobutyric acid (GABA) release
during ischemia. Glutamate release is increased 10-fold when temperature is
increased to 39�C during ischemia [45,50].
Unfortunately, intraoperative cerebral temperature is usually not monitored.
Instead, temperature is measured with esophageal, bladder, rectal, or tympanic
membrane probes. Even pulmonary artery catheter measurement may not be
reflective of cerebral temperature. To compound this problem, brain temper-
ature during surgery varies from cortical surface to deep intracerebral. It is
frustrating that a brain protectant therapy with few side effects is so difficult
to correctly implement because of our inability to measure the temperature of
the brain region at risk for ischemia. If this were possible, the local cooling
methodologies could be used instead of subjecting the entire body to hypo-
thermia. Currently, a multicenter study evaluating the effect of normothermic or
mild hypothermic management during cerebral aneurysmal clipping is under-
way [51]. This is the first time that a study sufficiently large enough to
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327320

evaluate a single intraoperative manipulation on neurologic outcome in humans
has been initiated.
Blood pressure
Control of blood pressure is possibly one of the most important aspects of
preventing brain injury and promoting cerebral protection. The direction and
extent of this control depends on the surgical procedure. For example, if an-
eurysm clipping includes trapping the aneurysm, maintenance of normal or
slightly increased blood pressure is indicated to increase collateral perfusion to
the area of brain transiently robbed of it blood supply due to the temporary clip.
Conversely, a reduction of blood pressure during direct aneurysm clipping may
reduce the intra-aneurysm pressure and decrease its potential for rupture during
surgical manipulation. Similarly, maintenance or increasing blood pressure
during carotid endarterectomy or the anastomosis of an extracranial-intracranial
(ECIC) bypass may also improve collateral perfusion to the tissue bed distal to
the occluded cerebral blood vessel. The effectiveness of these manipulations
depends on the state of vascular patency. For example, if the angiogram shows a
complete Circle of Willis, then increasing blood pressure during carotid
endarterectomy is appropriate; on the other hand, if the flow through the carotid
artery is minimal or the surgeon places a shunt, blood pressure need not be
elevated. Increasing blood pressure risks producing myocardial ischemia or
vasogenic edema in previously poorly perfused brain tissue because these
vessels are not governed by cerebral pressure autoregulation.
The amount and direction of blood pressure control depends upon knowledge of
the preoperative flow pattern (it is essential to review the angiogram preoper-
atively) and the surgical approach, rather than a cookbook methodology. Post-
operative management also requires a consideration of the surgical procedure.
Glucose
Serum glucose concentration at the time of ischemia contributes substantially
to the ischemic injury. The deleterious effects of hyperglycemia have been well
reported in both clinical and laboratory reports [52,53]. Hyperglycemia markedly
increases damage in both global and focal ischemia [54,55]. Even moderately
elevated serum glucose worsens outcome. During incomplete ischemia the
continuous delivery of glucose with an inadequate oxygen supply converts aerobic
to anaerobic metabolism, increasing brain lactic acid, which decreases brain pH.
Buffering capacity is overwhelmed, free oxygen radicals are generated, neuronal
pH decreases, and cell membrane rupture occurs, producing tissue necrosis [56].
There are several specific situations where elevated glucose concentrations
may be beneficial. First, in a rat model of cardiac arrest, administration of glucose
plus insulin (to moderate hyperglycemia) improved functional and histologic
outcome [57]. Second, abrupt normalization of hyperglycemia in patients with
chronically elevated glucose worsens ischemic damage.
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327 321

The future
The concept of providing cerebral protection in the future will probably not
focus on decreasing cerebral metabolism, but rather on blocking the cascade of
events that occur during ischemia (see boxed text).
The ischemic cascade
During cerebral ischemia large amounts of excitatory neurotransmitters (glu-
tamate and aspartate) are released by presynaptic neurons. The amount released
correlates with the severity of the ischemic insult and subsequent neuronal
damage. Glutamate and aspartate activate postsynaptic receptors (NMDA,
amino-3-hydroxy-5-methyl-4-isoxazol-propionic acid [AMPA], kainate), result-
ing in an increase in intracellular calcium and stimulation of enzyme systems that
produce ischemic damage and ultimately neuronal death. Nitric oxide synthase is
stimulated, producing large amounts of neuronal nitric oxide. Lipid peroxidases,
proteases, and phospholipases are activated, increasing intracellular free fatty
acids and free radicals. Capsase, translocase, and endonuclease activity results in
DNA fragmentation. Cell membranes become permeable, leading to edema and
additional calcium influx. ATP stores are depleted, energy-dependent membrane
pumps fail, and neuronal death occurs.
New concepts
Current philosophies of cerebral protection are focusing on these excitatory
neurotransmitters and their receptors with the hopes of finding ways to interrupt
the cascade of neuronal damage. This section briefly outlines some of the areas
and drugs under consideration and currently being evaluated (see boxed text).
Potential cerebral protective mechanisms
Decrease cerebral metabolismIncrease cerebral blood flowMild hypothermiaPrevent hyperthermiaMaintain normoglycemiaInhibit release of excitatory neurotransmitters (eg, glutamate,
aspartate)Enhance release of inhibitory neurotransmitters (eg, GABA)Block neuronal calcium influxDecrease nitric oxide formationDecrease Neuronal free radical formationPrevent apoptosisScavenge free radicalsPrevent Ca++ and Na+ influx
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327322

Some of the drugs that block glutamate release include inhalation anesthetics
(70% reduction), adenosine A1 blockers, and a2 agonists. Inhalational anestheticsmay also increase reuptake of neurotransmitters from the synaptic space. Drugs
that competitively block postsynaptic receptors include barbiturates (primarily
AMPA and kainate receptors) and possibly inhalation anesthetics. Noncompetitive
receptor antagonists include MK801 (dizoclipine), phencyclidine, dextromethor-
phan, ketamine, and magnesium. Recently, sodium channel inhibition has been
reported to decrease both potassium-evoked and spontaneous glutamate release.
Methods to block the ischemic cascade
Inhibit glutmate releaseInhalational anestheticsAdenosine A1 receptor blockersa2 agonistsHypothermiaSodium channel inhibitorsLamotrigenEtomidate
NMDA, AMPA, and kainate receptor blockersBarbiturates (mainly AMPA, Kainate)? Inhalational anesthetics
Noncompetative receptor blockersDizoclipine (MK801)PhencyclidineDextromethorphanKetamineMagnesiumPropofol
Block calcium influxPropofolKetamineInhalational anestheticsLidocaineHypothermia
Prevent apoptosisIsofluranceHalothane
Inhibit lipid peroxidationLazariods (21 aminosteroids)Hypothermia
Reduce inflammatory cytokinesStatinsAnti-inflammatory drugs
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327 323

Examples of other interesting approaches include aspirin, statins, and free
radical scavengers. Aspirin has shown laboratory evidence of neuronal protection
(delay in energy depletion and functional recovery), probably due to its antiin-
flammatory action [58]. Development of COX-2 inhibitors may make this
approach feasible. Recent work suggests that the statins, in addition to decreasing
atheromatous plaque, may also posses beneficial effects during ischemic stroke
and reperfusion [59]. The proposed mechanisms include upregulation of endo-
thelial nitric oxide synthase (which promotes vasodilation) while inhibiting
inducible nitric oxide synthase (which increases ischemic damage). They also
attenuate the inflammatory cytokine response to ischemia, possess antioxidant
properties, and reduce ischemic oxidative stress.
Drugs that decrease free radical formation or enhance free radical scavenging
are currently being evaluated as cerebral protectants. These include many well-
known drugs such as mannitol and steroids in addition to some new ones. Although
laboratory studies are promising, the human studies have not been very encour-
aging. Because cerebral ischemia is a complex event, a multifocal approach will
probably be necessary, focusing at different steps in the pathway of ischemia.
Outlook
The future for developing methodologies to protect the brain from ischemia is
bright. The scope and range of potential interventions appears unending. As
understanding of the cellular and molecular mechanisms that promote ischemic
damage or provide neuronal protection increases, research will become even more
exciting. The focus will not be on a single method or drug, but rather a cocktail of
options will be used to inhibit the harmful effects of the ischemic cascade.
References
[1] Michenfelder JD, Milde JH, Sundt TM. Cerebral protection by barbiturate anesthesia. Use of
middle cerebral artery occlusion in Java Monkeys. Arch Neurol 1976;33:345–50.
[2] Michenfelder JD, Theye R. Cerebral protection by thiopental during hypoxia. Anesthesiology
1973;39:510–7.
[3] Michenfelder JD. The interdependency of cerebral function and metabolic effects following
massive doses of thiopental in the dog. Anesthesiology 1974;41:231–6.
[4] Bleyaert A, Nemoto EM, Safar P, et al. Thiopental amelioration of brain damage after global
ischemia in monkeys. Anesthesiology 1978;49:390–8.
EstrogenHeparin
Decrease free radicalsMannitolStatinsHypothermia
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327324

[5] Gisvold S, Safar P, Hendrickx HHL, et al. Thiopental treatment after global brain ischemia in
pigtailed monkeys. Anesthesiology 1984;60:88–96.
[6] Brain Resuscitation Clinical Trial I Study Group. Randomized clinical study of thiopental load-
ing in comatose survivors of cardiac arrest. N Eng J Med 1986;314:397–403.
[7] Nussmeier NA, Arlund C, Slogoff S. Neuropsychiatric complications after cardiopulmonary
bypass: cerebral protection by a barbiturate. Anesthsiologoy 1986;64:165–70.
[8] Zaidan J, Klochany A, Martin WM, et al. Effect of thiopental on neurologic outcome following
coronary artery bypass grafting. Anesthesiology 1991;74:406–11.
[9] Milde LN, Milde JH, Michenfelder JD. Cerebral functional, metabolic, and hemodynamic effects
of etomidate in dogs. Anesthesiology 1985;63:371–7.
[10] Milde LN, Milde JH. Preservation of cerebral metabolites by etomidate during incomplete
cerebral ischemia in dogs. Anesthesiology 1986;65:272–7.
[11] Patel PM, Goskowicz RL, Drummond JC, et al. Etomidate reduces ischemia-induced glutamate
release in the hippocampus in rats subjected to incomplete forebrain ischemia. Anesth Analg
1995;80:933–9.
[12] Smith DS, Keykhah MM, ONeill JJ, et al. The effect of etomidate pretreatment on cerebral high
energy metabolites, lactate, and glucose during severe hypoxia in the rat. Anesthesiology
1989;71:438–42.
[13] Baughman VL, Hoffman WE, Miletich DJ, et al. Cerebral metabolic depression and brain
protection produced by midazolam and etomidate in the rat. J Neurosurg Anesthesiol 1989;1:
22–8.
[14] Edelman G, Hoffman WE, Charbel FT. Cerebral hypoxia following etomidate administration and
temporary cerebral artery occlusion. Anesth Analg 1997;85:521–825.
[15] Frizzell RT, Meyer YJ, Borchers DJ, et al. The effects of etomidate on cerebral metabolism and
blood flow in a canine model for hypoperfusion. J Neurosurg 1991;74:263–9.
[16] Fellows IW, Bastow MD, Byrne AJ, et al. Adrenocortical suppression in multiply injured
patients: a complication of etomidate treatment. Fr Med J 1983;287(6408):1835–7.
[17] Absalom A, Plodger D, Kong A. Adrenocortical function in critically ill patients 24 hours after a
single dose of etomidate. Anaesthesia 1999;54:861–7.
[18] Vandesteene A, Trempont V, Engelman E, et al. Effect of propofol on cerebral blood flow and
metabolism in man. Anaesthesia 1988;43(Suppl):42–3.
[19] Kochs E, Hoffman WE, Werner C, et al. The effects of propofol on brain electrical activity,
neurologic outcome, and neuronal damage following incomplete ischemia in rats. Anesthesiol-
ogy 1992;76:245–52.
[20] Ridenour TR, Warner DS, Todd MM, et al. Comparative effects of propofol and halothane on
outcome from temporary middle cerebral artery occlusion in the rat. Anesthesiology 1992;76:
807–12.
[21] Murphy PG, Myers DS, Davies MJ, et al. The antioxidant potential of propofol (2,6-diisopro-
pylphenol). Br J Anaesth 1992;8:613–8.
[22] Orser BA, Bertlik M, Wang LY, et al. Inhibition by propofol (2,6 di-isopropylphenol) of the
N-methyl-D-aspartate subtype of glutamate receptor in cultured hippocampal neurons. Br J
Pharmacol 1995;116:1761–8.
[23] Marx W, Shah N, Long D, et al. Sufentanil, alfentanil, and fentanyl: impact on cerebrospinal
fluid pressure in patients with brain tumors. J Neurosurg Anesthesiol 1989;1:3–7.
[24] Werner C, Kochs E, Bause H, et al. Effects of sufentanil on cerebral hemodynamics and intra-
cranial pressure in patients with brain injury. Anesthesiology 1995;83:721–6.
[25] Kofke WA, Garman RH, Tom WC, et al. Alfentanil-induced hypermetabolism, seizure, and
histopathology in rat brain. Anesth Analg 1992;75:953–64.
[26] Hoffman WE, Miletich DJ, Albrecht RF. The effects of midazolam on cerebral blood flow and
oxygen consumption and its interaction with nitrous oxide. Anesth Analg 1986;65:729–33.
[27] Dawson B, Michenfelder JD, Theye RA. Effect of ketamine on canine cerebral blood flow
and metabolism: modification by prior administration of thiopental. Anesth Analg 1971;50:
443–7.
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327 325

[28] Church J, Zeman S, Lodge D. The neuroprotective effect of ketamine and MK801 after transient
cerebral ischemia in rats. Anesthesiology 1988;69:702–9.
[29] Hoffman WE, Pelligrino D, Werner C, et al. Ketamine decreases plasma catecholamines and
improves outcome from incomplete cerebral ischemia in rats. Anesthesiology 1992;76:755–62.
[30] Jensen ML, Auer RN. Ketamine fails to protect against ischemia neuronal necrosis in the rat. Br J
Anaesth 1988;61:206–10.
[31] Thompson A, et al. An N-methylaspartate receptor-mediated synapse in rat cerebral cortex: a site
of action of ketamine? Nature 1985;313:479–81.
[32] Fukuda S, Murakawa T, Takeshita H, et al. Direct effects of ketamine on isolated canine cerebral
and mesenteric arteries. Anesth Analg 1983;62:553–8.
[33] Mayberg TS, Lam AM, Matta BF, et al. Ketamine does not increase cerebral blood flow velocity
or intracranial pressure during isoflurane/nitrous oxide anesthesia in patients undergoing craniot-
omy. Anesth Analg 1995;81:84–9.
[34] Henriksen HT, Jorgensen PB. The effect of nitrous oxide on intracranial pressure in patients with
intracranial disorders. Br J Anaesth 1973;45:486–92.
[35] Pelligrino DA, Miletich DJ, Hoffman WE, et al. Nitrous oxide markedly increases cerebral
cortical metabolic rate and blood flow in the goat. Anesthesiology 1984;60:405–12.
[36] Deutsch G, Samra SA. Effects of nitrous oxide on global and regional cortical blood flow. Stroke
1990;21:1293–8.
[37] Lam AM, Mayberg TS, Eng CC, et al. Nitrous oxide-isoflurane anesthesia causes more cerebral
vasodilation than an equipotent dose of isoflurane in humans. Anesth Analg 1994;78:462–8.
[38] Baughman VL, Hoffman WE, Thomas C, et al. The interaction of nitrous oxide and isoflurane
with incomplete cerebral ischemia in the rat. Anesthesiology 1989;70:767–74.
[39] Warner DS, Zhou JG, Ramani R, et al. Nitrous oxide does not alter infarct volume in rats
undergoing reversible middle cerebral artery occlusion. Anesthesiology 1990;73:686–93.
[40] Hoffman WE, Charbel FT, Edelman G, et al. Thiopental and desflurane for brain protection.
Neurosurgery 1998;43:1050–3.
[41] Faberowski LW, Raizada MK, Sumners C. Hypoxia- and ischemia-induced neuronal apoptosis is
decreased by halothane and isoflurane (Abstract). J Neurosurg Anesthesiol 1999;11(4):307.
[42] Ginsberg MD, Sternau LL, Globus MY, et al. Therapeutic modulation of brain temperature:
relevance to ischemic brain injury. Cerebrovasc Brain Metab Rev 1992;4(3):189–225.
[43] Minamisawa H, Nordstrom CH, Smith ML, et al. The influence of mild body and brain hypo-
thermia on ischemic brain damage. J Cereb Blood Flow Metab 1990;10(3):365–74.
[44] Sano T, Drummond JC, Patel PM, et al. A comparison of the cerebral protective effects of
isoflurane and mild hypothermia in a model of incomplete forebrain ischemia in the rat. Anes-
thesiology 1992;76:221–8.
[45] Busto R, Dietrich WD, Globus MY, et al. Small differences in intraischemic brain temperature
critically determine the extent of neuronal injury. J Cereb Blood Flow Metabol 1987;7:729–38.
[46] Busto R, Globus MY, Dietrich WD, et al. Effect of mild hypothermia on ischemia-induced
release of neurotransmitters and free fatty acids in rat brain. Stroke 1989;20:904–10.
[47] Patel P, Drummond JC, Cole DJ, et al. Differential temperature sensitivity of ischemia-induced
glutamate release and eicosanoid production in rats. Brain Res 1994;650:205–11.
[48] Kader A, Frazzini VI, Baker CJ, et al. Effect of mild hypothermia on nitric oxide synthesis
during focal cerebral ischemia. Neurosurgery 1994;35:272–7.
[49] Bickler P, Buck LT, Hansen BM. Effects of isoflurane and hypothermia on glutamate receptor-
mediated calcium influx in brain slices. Anesthesiology 1994;81:1461–9.
[50] Takagi E, Ginsberg MD, Globus MY, et al. Effect of hyperthermia on glutamate release in ische-
mia penumbra after middle cerebral artery occlusion in rats. Am J Physiol 1994;266:H1770–6.
[51] Hindman BJ, Todd MM, Geld AW, et al. Mild hypothermia as a protective therapy during
intercranial aneurysm surgery: a randomized prospective pilot trial. Neurosurgery 1999;44(1):
23–32.
[52] Longstreth WT Jr, Inui TS. High blood glucose level on hospital admission and poor neuro-
logical recovery after cardiac arrest. Ann Neurol 1984;15:59–63.
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327326

[53] Pulsinelli WA, Levy DE, Sigsbee B, et al. Increased damage after ischemic stroke in patients
with hyperglycemia with or without established diabetes mellitus. Am J Med 1983;74:540–4.
[54] Siemkowicz E, Gjedde A. Post-ischemic coma in rat: effect of different pre-ischemic blood
glucose levels on cerebral metabolic recovery after ischemia. Acta Physiol Scand 1980;110:
225–32.
[55] Warner DS, Gionet TX, Todd MM, et al. Insulin-induced normoglycemia improves ischemic
coutcome in hyperglycenic rats. Stroke 1992;23:1775–80.
[56] Dietrich WD, Busto R, Globus MY, et al. Brain damage and temperature: cellular and molecular
mechanisms. Adv Neruol 1996;71:177–99.
[57] Katz L, Ebmeyer U, Safar P, et al. Outcome model of asphyxial cardiac arrest in rats. J Cereb
Blood Flow Metab 1995;15:1032–9.
[58] Riepe MW, Kasischke K. Raupach: acetylsalicylic acid increases tolerance against hypoxic and
chemical hypoxia. Stroke 1997;28(10):2006–11.
[59] Vaughan DJ, Delanty N. Neuroprotective properties of statins in cerebral ischemia and stroke.
Stroke 1999;30:1969–73.
V.L. Baughman / Anesthesiology Clin N Am 20 (2002) 315–327 327

Fluids and the neurosurgical patient
Concezione Tommasino, MD*
Institute of Anesthesiology and Intensive Care, University of Milano,
Department of Anesthesia and Intensive Care, San Raffaele Hospital, Via Olgettina,
60 20132, Milano, Italy
The fluid management of neurosurgical patients presents special challenges for
anesthesiologists and intensivists [1]. Neurosurgical patients often receive diu-
retics (eg, mannitol, furosemide) to treat cerebral edema and/or to reduce
intracranial hypertension. Conversely, they may also require large amounts of
intravenous fluids to correct preoperative dehydration and/or to maintain intra-
operative and postoperative hemodynamic stability as part of therapy for vaso-
spasm, for blood replacement, or for resuscitation.
For a long time restrictive fluid management has been the treatment of choice
in patients with brain pathology, growing from fear that fluid administration
could enhance cerebral edema [2]. It is well known that fluid restriction, if
pursued to excess (hypovolemia), may result in episodes of hypotension, which
can increase intracranial pressure (ICP) and reduce cerebral perfusion pressure,
and the consequences can be devastating [3].
It is unfortunate that little substantial human data exist concerning the impact of
fluids on the brain, or which can guide rational fluid management in neurosurgical
patients. However, it is possible to examine those factors that influence water
movement into the brain, and to make some reasonable recommendations.
This review will address some of the physical determinants of water move-
ment between the intravascular space and the central nervous system (CNS).
Subsequent sections will address specific clinical situations with suggestions for
the types and volume of fluids to be administered.
Osmolality/osmolarity, osmotic and oncotic pressure, hemodilution
With intravenous fluid therapy, three properties of the blood can be manipu-
lated: osmolality (owing to concentrations of large and small molecules), colloid
oncotic pressure (COP; owing to large molecules only), and hematocrit.
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00013 -X
* Department of Anesthesia and Intensive Care, San Raffaele Hospital, Via Olgettina, 60 20132,
Milano, Italy.
E-mail address: [email protected] (C. Tommasino).
Anesthesiology Clin N Am
20 (2002) 329–346

Osmotic pressure
This is the hydrostatic force acting to equalize the concentration of water on
both sides of the membrane that is impermeable to substances dissolved in that
water. Water will move along its concentration gradient. Osmolarity describes the
molar number of osmotically active particles per liter of solution. In practice, the
osmolarity of a solution can be ‘‘calculated’’ by adding up the mEq concen-
trations of the various ions in the solution. Osmolality describes the molar
number of osmotically active particles per kilogram of solvent. This value is
directly ‘‘measured’’ by determining either the freezing point or the vapor
pressure of the solution. For most dilute salt solutions, osmolality is equal to
or slightly less than osmolarity.
Colloid oncotic pressure
Osmolarity/osmolality is determined by the total number of dissolved ‘‘par-
ticles’’ in a solution, regardless of their size. COP is nothing more that the
osmotic pressure generated by large molecules (eg, albumin, hetastarch, dextran).
The COP becomes particularly important in biological systems where vascular
membranes are often permeable to small ions, but not to large molecules.
Fluid movement between capillaries and tissues
As defined by the Starling equation [4], the major factors that control the
movement of fluids between the intravascular and extravascular spaces are the
transcapillary hydrostatic gradient, the osmotic and oncotic gradients, and
the relative permeability of the capillary membranes that separate these spaces.
The Starling equation is as follows:
FM ¼ kðPc þ pi � Pi � pcÞ
where FM = fluid movement, k = the filtration coefficient of the capillary wall
(= how leaky it is), Pc = hydrostatic pressure in the capillaries, Pi = hydrostatic
pressure (usually negative) in the interstitial space, and pi and pc are interstitial
and capillary osmotic pressures, respectively. In a simplified fashion, fluid
movement is proportional to the hydrostatic pressure gradient minus the osmotic
gradient across a vessel wall. The magnitude of the osmotic gradient will depend
on the relative permeability of the membrane.
In the periphery (muscle, lung, and other areas), the capillary endothelium has
a pore size of 65 A, and is freely permeable to small molecules and ions (Na+,
Cl�), but not to large molecules, such as proteins [5] (Fig. 1A). Thus, in the
periphery, movement of water is governed by the plasma concentration of large
molecules (oncotic gradient). If COP is reduced, fluid will begin to accumulate in
the interstitium, producing edema. In the cerebral capillaries, Fenstermacher [5]
calculated the effective pore size to be only 7 to 9 A. This small pore size of the
blood–brain barrier (BBB) prevents not only the movement of proteins, but also
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346330

sodium, chloride, and potassium ions [5] (Fig. 1B). The fluid movement across
the BBB is determined by the ‘‘total’’ osmotic gradient, generated both by large
molecules and small ions. Because there are so few protein molecules compared
with the number of inorganic ions, their effect on total osmolality is minimal
(normal COP � 20 mmHg � 1 mOsm/kg). Clearly, the influence of changes in
osmolality on cerebral water distribution dwarfs the effects of alteration in COP.
These differences explain why the administration of large volumes of isotonic
crystalloids, with dilutional reduction of COP, results in peripheral edema, but
does not increase brain water content and/or ICP [6–8].
When plasma osmolality decreases, the osmotic gradient drives water into the
brain tissue. Even small changes in plasma osmolality ( < 5%) increase brain
water content and ICP [7].
The above scenario describes the situation in conditions of normal BBB. After
a brain lesion, according to the severity of the damage (head trauma, tumor,
seizure, abscess, or other damage), there can be varying degrees of BBB integrity,
which can respond differently to the osmotic/oncotic changes. With complete
breakdown of the BBB, no osmotic gradient can be established [9–11]. It is
possible that with a less severe injury to the BBB, the barrier may function
similarly to the peripheral tissue [12]. Finally, there is usually a significant
Fig. 1. Schematic diagram of capillary membrane in the periphery. (A) The vessel wall is permeable to
both water (H2O) and small ions, but not to proteins (P), in the brain. (B) The blood–brain barrier is
permeable only to water.
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 331

portion of the brain where the BBB is normal. The presence of a functionally
intact BBB is essential if osmotherapy is to be successful [13].
Hematocrit and hemodilution
One common accompaniment of fluid infusion is a reduction in hemoglobin/
hematocrit. This hemodilution is typically accompanied by an increase in cerebral
blood flow (CBF) [7,14,15]. In the normal brain, the increase in CBF produced
by hemodilution is an active compensatory response to a decrease in arterial
oxygen content, and this response is essentially identical to that seen with
hypoxia [16–18]. However, it should be stressed that in the face of brain injury,
the normal CBF responses to hypoxia and to hemodilution are attenuated, and
both changes may contribute to secondary tissue damage [19].
A hematocrit level of 30–33% gives the optimal combination of viscosity and
O2 carrying capacity, and may improve neurologic outcome [6,20,21]. However,
marked hemodilution (Hct < 30%) exacerbates neurologic injury [20,22].
Fluids for intravenous administration
The anesthesiologists and the intensivists can choose among a variety of fluids
suitable for intravenous administration, commonly categorized as crystalloids
and colloids.
Crystalloids and cerebral effects of plasma osmolality
Crystalloid solutions do not contain any high molecular weight compound,
and have an oncotic pressure of zero. Crystalloids may be hypo-osmolar, iso-
osmolar or hyperosmolar, and may or may not contain glucose. Commonly used
crystalloid solutions are illustrated in Table 1.
Hypo-osmolar crystalloids
Since the early years of the last century, scientists have known that fluid
regimens provide free water (eg, 0.45% saline or 5% glucose in water, D5W), and
cause a concomitant reduction in plasma osmolality, can cause cerebral edema.
One of the first animal studies on the cerebral effects of fluid administration
showed that hypotonic solutions expanded the brain [23]. The osmotic gradient
drives water across the BBB into the cerebral tissue, increasing brain water
content (= edema) and ICP. As a consequence, the use of fluid therapy that avoids
excess free water has been a standard element of management in patients with
brain and spinal cord damage.
Iso-osmolar crystalloids
Although some clinicians have long believed that iso-osmolar crystalloids
induce and/or aggravate brain edema, the many attempts to demonstrate experi-
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346332

mentally this phenomenon have not yielded scientifically convincing proof or
have generated negative results [7–11,24–27]. Iso-osmolar solutions, with an
osmolality � 300 mOsm/L, such as plasmalyte, 0.9% saline, do not change
plasma osmolality, and do not increase brain water content. The same does not
apply to solutions that are not truly iso-osmolar with respect to plasma. For
example, commercial lactated Ringer’s solution has a calculated osmolarity of
� 275 mOsm/L, but a measured osmolality of � 254 mOsm/kg, indicating
incomplete dissociation [7]. The administration of large volumes of this solution
(> 3 l in humans) can reduce plasma osmolality and increase brain water content
and ICP [7,28], as approximately 114 mL of free water is given for each liter of
lactated Ringer’s solution.
Hyperosmolar crystalloids
Crystalloids may be made hyperosmolar by the inclusion of electrolytes (eg,
Na+ and Cl�, as in hypertonic saline), or low molecular weight solutes, such as
mannitol (molecular weight 182), or glucose (molecular weight 180). Hyper-
osmolar solutions exert their beneficial effects by osmotically shifting water
from the nervous tissue (intracellular and interstitial space) to the intravascular
space. This effect has been demonstrated in brain tissue with normal a BBB
[13,28–31], and is the cornerstone treatment of intracranial hypertension. Fur-
thermore, the increased serum osmolality reduces cerebrospinal fluid (CSF)
secretion rate, and this effect can contribute to improve the intracranial com-
pliance [32–34].
Table 1
Composition of commonly used intravenous fluids: Crystalloids
mEq/l
g/l
Intravenous fluids MOsm/la Na+ Cl� K Ca Mg Lactate
Dextrose
(g/l)
5% Dextrose in water (D5W) 278 50
5% Dextrose in 0.45% NaCl 405 77 77 50
5% Dextrose in 0.9% NaCl 561 154 154 50
5% Dextrose in Ringer’s solution 525 130 109 4 3 50
Ringer’s solution 309 147 156 4 4–4.5
Lactated Ringer’s solution 275 130 109 4 3 28
5% Dextrose in Lactated
Ringer’s solution
525 130 109 4 3 28 50
Plasmalyteb 298 140 98 5 3
0.45% NaCl 154 77 77
0.9% NaCl 308 154 154
3.0% Saline 1026 513 513
5.0% Saline 1710 855 855
7.5% Saline 2566 1283 1283
20% Mannitol 1098
a osmolarity = calculated value (osm/l = mg�molecular weigh � 10 � valence).b Acetate 27 mEq/l and gluconate 23 mEq/l.
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 333

Colloids and cerebral effects of colloid oncotic pressure
Colloid is the term used to denote solutions that have an oncotic pressure
similar to that of plasma. Colloidal solutions share the presence of large
molecules that are relatively impermeable to the capillary membranes. Frequently
used colloids are illustrated in Table 2. Colloids include albumin, plasma,
hetastarch (hydroxyethylstarch, molecular weight 450), pentastarch (a low
molecular weight, 264, hydroxyethylstarch), and the dextrans (molecular weights
40 and 70). Dextran and hetastarch are dissolved in normal saline, so the
osmolarity of the solution is approximately 290 to 310 mOsm/L, with a sodium
and chloride content of about 154 mEq/L each.
Although it is accepted that a reduction in serum osmolality will cause
cerebral edema [7,12,23], there is not uniform agreement about the potential
effect of reduction in COP. Carefully conducted investigations have system-
atically sought a cerebral edema effect of COP reduction but have failed to
identify one [6,8–11]. Only a recent and elegant study by Drummond et al.
[12] has reported that COP reduction has the potential to aggravate brain
edema. The different results can be explained by the nature and severity of the
brain injury. In the study of Drummond et al. [12], the injury was deliberately
mild. It seem reasonable to suspect that this type of mechanical injury made the
BBB permeable to low molecular weight solutes while remaining impermeable
to colloids.
From the above-mentioned studies we can postulate that, depending on the
severity of the BBB damage, we will have brain areas where the osmotic/
oncotic gradient is totally effective (normal BBB), areas where only the colloid
oncotic gradient is effective (mild opening of the BBB, with pore size similar to
the periphery), and areas where there is no osmotic/oncotic gradient effect
(BBB breakdown).
The message is to avoid and/or correct, in patients with brain or spinal cord
injury, a decrease in ‘‘both’’ serum osmolality and COP. This message, however,
is part of the ‘‘common clinical sense.’’ As anesthesiologists and intensivists, we
treat not only brains but patients, and a COP reduction, even if it could not
directly affect brain water content, affects other organs and perfusion (eg,
pulmonary edema) [35], which in turn, can influence brain homeostasis.
Table 2
Composition of commonly used intravenous fluids: Colloids
mEq/lOsmolaritya Oncotic pressure
Intravenous fluids Na + Cl � K Ca (mOsm/l) (mm Hg)
Fresh-frozen plasma 168 76 3.2 8.2 � 300 21
5% Albumin 290 19
Dextran (10%) 40 in 0.9% saline 154 154 � 310 61
Dextran (6%) 70 in 0.9% saline 154 154 � 310 19
Hetastarch (6%) in 0.9% saline 154 154 31
Hetastarch (10%) in 0.9% saline 154 154 � 310 82
a Osmolarity = calculated value (osm/l = mg�molecular weigh � 10 � valence).
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346334

Glucose-containing solutions
Intravenous salt-free solutions containing glucose should be avoided in
patients with brain and spinal cord pathology. Once glucose is metabolized, only
free water remains only free water, which reduces serum osmolality and increases
brain water content. Furthermore, several studies in animals as well as in humans
have demonstrated that glucose administration increases neurologic damage and
can worsen outcome from both focal and global ischemia [36–40], presumably
because in ischemic areas glucose metabolism enhances tissue acidosis [40,41].
Glucose-containing solutions should be withheld in adult neurosurgical patients,
with the exception of neonates and patients with diabetes, in whom hypoglycemia
can occur very rapidly and be detrimental. It should be noted that this caveat does
not appear to apply to the use of hyperalimentation fluids in neurosurgical
patients, perhaps because these hyperglycemic fluids are typically started several
days after the primary insult, and/or because concomitant insulin is used. In
humans, it has not been carefully studied whether aggressive control of hyper-
glycemia with insulin will improve outcome, but laboratory evidence supports
the concept that preischemic correction of hyperglycemia with insulin im-
proves outcome.
In neurosurgical patients blood sugar level should be controlled frequently,
and the goal should be to avoid either hypo-and hyperglycemia, and maintain
sugar levels between 100 and 150 mg/dL.
Fluids to control ICP and brain swelling
Diuretics: mannitol and furosemide
Both mannitol and furosemide are extensively used to control ICP and brain
swelling. Mannitol accomplishes this goal by establishing an osmotic gradient
between the intravascular compartment and the cerebral parenchyma, in the
presence of a relatively intact BBB. The increased plasma osmolality promotes
removal of water from areas of normal brain [29,33]. Several issues related to
mannitol have also been clarified in recent years. Mannitol can transiently elevate
ICP. The mechanism of this effect is clearly due to the vasodilator effects of
hyperosmolality, with a resultant increase in cerebral blood volume (CBV)
[42,43]. However, it has been shown in both dogs and humans that this is a
phenomenon that does not occur in the presence of intracranial hypertension, or
when mannitol is given at moderate rates [42,43]. Thus, there is no important
reason to avoid mannitol in most neurosurgical patients, other than in patients
with significant cardiovascular disease, in whom the transient volume expansion
might precipitate congestive heart failure.
The other important concern is the excessive and/or repeated use of the drug,
because excessive hyperosmolality can be detrimental. In addition, mannitol does
progressively accumulate in the interstitium with repeated doses, and may even
aggravate brain edema [44,45]. If interstitial osmolality rises excessively, it is
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 335

possible that the normal brain–blood gradient might be reversed, with resultant
worsened edema. Furthermore, if brain osmolality is increased, there is a risk of
enhancing edema by subsequent normalization of serum osmolality.
Although mannitol is extensively used in patients with intracranial hyperten-
sion, a larger dose-finding study in humans has not been performed, and single
doses of mannitol from 0.25 up to 2.27 g/kg have been reported in the literature.
Marchall et al. [46] studied the effect of different mannitol doses in patients, and
concluded that small doses (0.25 g/kg) were as effective as larger doses. At our
institution mannitol is used at a dose range of 0.25–1.0 g/kg, and we always
choose the smallest possible dose, which is infused in at least in 10–15 min.
The mechanism of furosemide’s action remains controversial (although it
certainly is related to the drug’s ability to block Cl� transport) [47]. Furosemide
and similar drugs may also act primarily by reducing cell swelling, rather than by
changing extracellular fluid volume. In several studies it has been demonstrated
that furosemide decreases CSF production, and this effect can explain the
synergism between mannitol and furosemide on intracranial compliance [48].
Furosemide’s maximal effect is delayed compared with mannitol [49,50]. For this
reason, mannitol probably remains the agent of choice for rapid ICP control.
Hypertonic saline solutions
Hypertonic salt solutions have been primarily used for small-volume resus-
citation in patients with hemorrhagic shock. Because hyperosmolality is known
to reduce brain volume [23], hypertonic saline may become part of standard
resuscitation in patients with concomitant head injury. Laboratory and clinical
data suggest that hypertonic solutions are effective for volume resuscitation, and
result in a lesser degree of cerebral edema [51,52]. In humans, acute resuscitation
from hemorrhagic shock with 7.5% hypertonic saline is associated with improved
outcome in traumatized head-injured patients, and clinical studies suggest that
hypertonic saline may be efficacious in hypotensive, brain-injured patients during
transport to the hospital [53,54].
Various animal experiments have indicated that hypertonic saline solutions
lower ICP and improve cerebral perfusion pressure [3,30,31,51]. The CNS effects
of hypertonic saline are similar to mannitol [30,55]; however, the fact that
hypertonic saline does not produce an osmotic diuresis simplifies perioperative
fluid management. There are a number of case reports and a few controlled trials
that suggest that hypertonic saline may produce significant and sustained
reductions in ICP where mannitol has failed [56,57]. The mechanism by which
hypertonic saline succeeded when mannitol failed, however, remains unclear.
The principal disadvantage of hypertonic saline is related to the possible
danger of hypernatremia. In a recent study in neurosurgical patients during
elective procedures, we have shown that equal volumes of 20% mannitol and
7.5% hypertonic saline reduce brain bulk and cerebrospinal fluid pressure to the
same extent [55]. Serum sodium levels increased during the administration of
hypertonic saline, and peaked at over 150 mEq/L at the end of the infusion [55].
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346336

However, initial concerns regarding the adverse nurologic sequelae of hypertonic
saline appear to have been premature. First, the increment in serum sodium in
response to addition of concentrated sodium is less than would be predicted [55].
Second, patients tolerate acute increases in serum sodium to 155–160 mEq/L,
without apparent harm [53–55,58]. Third, central pontine myelolysis has not
been observed in a clinical trial of hypertonic resuscitation [53]. One concern is
that hypertonic saline solutions have the potential to cause rebound intracranial
hypertension, similar to other osmotic agents [59,60].
Hypertonic/hyperoncotic solutions
More recent attention has been directed at hypertonic/hyperoncotic solutions
(typically hypertonic hetastarch or dextran solutions). Because of the powerful
hemodynamic properties of these fluids in circulatory shock, administration in
patients with multiple traumas and head injury might be particularly advantage-
ous for the prevention of secondary ischemic brain damage [58]. Small volumes
of such solutions can restore normovolemia rapidly, without increasing ICP
[28,61]. They have been successfully used to treat intracranial hypertension in
head-injured patients and in patients with stroke [53,54,62,63].
Implications for patient care
The available information can be used to make a series of ‘‘reason-
able’’ suggestions, useful either in the perioperative period as well as for
fluid resuscitation.
Fluid restriction
Despite a lack of convincing experimental evidence that iso-osmolar crystal-
loids are detrimental, fluid restriction is still widely practiced in patients with
mass lesions, cerebral edema, and/or at risk for intracranial hypertension. The
only directly applicable data indicate that clinically acceptable fluid restriction
has little effect on edema formation; however, there is some ‘‘logic’’ behind
modest fluid restriction. One of the few human studies on fluid therapy in
neurosurgical patients demonstrated that patients given standard ‘‘maintenance’’
amounts of intravenous fluids (eg, 2000 mL/day) in the postoperative period
developed a progressive reduction in serum osmolality [2]. On the other hand,
patients given half this volume over a period of about 1 week showed a
progressive increase in serum osmolality, which could account for dehydration
of the brain (Fig. 2) [55]. Although no CNS-related parameters were measured in
this study, the results suggest that the maintenance fluids used (0.45% NaCl in
5% dextrose) contain excess-free water for the typical postoperative craniotomy
patient. In this light, fluid restriction can be viewed as ‘‘preventing’’ hypo-
osmotically driven edema. This does not imply that even greater degrees of fluid
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 337

restriction are beneficial, or that the administration of a fluid mixture that does
not reduce osmolality is detrimental.
Intraoperative volume replacement/resuscitation
As a general rule, intraoperative fluid administration should be given at a rate
sufficient to replace the urinary output and insensible losses. Table 3 illustrates
the intravascular volume expansion obtained with different types of fluids.
The available data indicate that volume replacement/expansion will have no
effect on cerebral edema as long as normal serum osmolality and oncotic pressure
are maintained, and as long as cerebral hydrostatic pressures are not markedly
increased (eg, due to true volume overload and elevated right heart pressures).
Whether this is achieved with crystalloids or colloids seems irrelevant. Serum
osmolality should be checked repeatedly, with the goal being to maintain this
value either as constant or slightly increased.
Table 3
Fluid replacement and intravascular volume
Fluid infused Intravascular volume increase
1 liter isotonic crystalloid � 250 ml
1 liter 5% albumin � 500 ml
1 liter hetastarch � 750 ml
Fig. 2. Effect of fluid restriction (1 L/day) on serum osmolality in neurosurgical patients. (From Shenkin
HA, Benzier HO, BouzarthW. Restricted fluid intake: rational management of the neurosurgical patient.
J Neurosurg 1976;45:432–6; with permission by Lippincott Williams & Wilkins D.)
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346338

Fluid administration that results in a reduction in osmolality should be
avoided. Small volumes of Lactated Ringer’s (not strictly iso-osmotic, measured
osmolality 252–255 mOsm/kg) are unlikely to be detrimental, and can be safely
used. If large volumes are needed (blood loss or other source of volume loss), a
change to a more isotonic fluid is advisable. It is also important to remember that
large and rapid infusion of 0.9% NaCl can induce a dose-dependent hyper-
chloremic metabolic acidosis [64,65]. Whether this acid-base abnormality is, in
fact, harmful remains unclear, although animal studies suggest that hyperchlore-
mia causes renal vasoconstriction [66]. If large volumes are needed, a combina-
tion of isotonic crystalloids and colloids may be the best choice. The combined
use of these fluids can avoid reductions both is serum osmolality and COP.
Hetastarch should be used with caution due to coagulation factor VIII depletion
and possible coagulation difficulties encountered with volumes >1000 mL
[67,68]. Pentastarch, a new formulation of hydrolyzed amylopectin, causes fewer
effects on coagulation than hetastarch; it does not prolong the bleeding time, and
has little effect on factor VIII [69]. Dextran 40 interferes with normal platelet
function, and therefore is not advisable for patients with intracranial pathology,
other than to improve rheology, such as in ischemic brain diseases.
These recommendations should not be interpreted as ‘‘give all the isotonic–
iso-oncotic fluid you like.’’ Volume overload can have detrimental effects on ICP,
via increasing CBV or via hydrostatically driven edema formation.
Postoperative period
In the postoperative period, large fluid requirements should cease. In such
cases, the recommendations of Shenkin et al. [2] are probably reasonable, and we
recommend periodic measurements of serum osmolality, particular if neurologic
status deteriorates. If cerebral edema does develop, further restriction is unlikely
to be of value, and can result in hypovolemia. Specific treatment with mannitol,
furosemide, and other drugs, combined with normovolemia achieved with fluids
that will maintain the increased osmolality, appears to be reasonable.
Head injury
Prompt restoration of systemic pressure is essential in head-injuried patients.
In patients in whom multiple trauma complicates head injury, no resuscitation
fluid has proven ideal [70]. Hypotonic solutions (including Lactated Ringer’s
solutions) should be avoided, and therapy should rely on fluids with osmolalities
around 300 mOsm/L. In cases of large-volume fluid administration, oncotic
pressure should be checked, and colloid solutions administered as needed.
Hypertonic saline solutions have been used successfully to treat hypovolemia
and intracranial hypertension in these patients [51–54,62]. Glucose-containing
solutions should be avoided, because hyperglycemia is associated with poorer
neurologic outcome in head-injured patients [37,39].
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 339

Subarachnoid hemorrhage
When treating patients with subarachnoid hemorrhage two problems should be
kept in mind: hyponatremia and hypovolemia.
In these patients, relative hypovolemia develops very often. The cause is
multifactorial, and includes bed rest, negative nitrogen balance, decreased
erythropoiesis, iatrogenic blood loss, and dysregulation of the autonomic nervous
system. Hyponatremia appears to develop as the result of a central salt-wasting
syndrome, and the causative factor seems to be an increased release of a
natriuretic factor from the brain [71]. Excessive renal excretion of sodium
precedes the development of ischemic symptoms [72], and patients appear to
be at increased risk for delayed cerebral infarction [73]. Hyponatremia should not
be a serious concern if electrolytes and type of fluids administered are carefully
monitored. With the administration of a large volume of isotonic crystalloids and
restriction of free water (hypotonic intravenous fluids and oral fluids) the severity
of the fall in serum sodium concentration is ameliorated, and usually does not
require further intervention. If hyponatremia is more severe or significant cere-
bral edema exists, the use of mild hypertonic fluids (1.25 or 1.5% saline) and
strict avoidance of free water administration are usually successful in reversing
the hyponatremia.
Fluid restriction should be abandoned, as it worsens volume contraction and
exacerbates symptoms from vasospasm. Hypertensive/hypervolemic therapy is
widely accepted to prevent/treat symptomatic cerebral vasospasm [74]. This
therapeutic treatment, however, has never been carefully studied (control group
with no therapy, or other treatments), and it is not clear whether hypertension and/
or hypervolemia is the critical factor. Volume loading is usually performed with
colloids, and great care is required to avoid reduction in serum osmolality,
because this will increase brain water content in ischemic as well as normal
cerebral regions [75].
Ischemic injury
The one situation where hemodilution may be beneficial is in the period
immediately during/after a focal cerebral ischemic event. Several studies have
shown that regional O2 delivery in this situation may be increased (or at least
better maintained) in the face of modest hemodilution (Hct � 30%), and animal
studies demonstrate improvement in CBF and some reductions in infarction
volumes [20,76]. Unfortunately, several trials have failed to demonstrate any
benefit of hemodilution in stroke, except in polycythemic patients [77–80].
Spinal cord injury
Although the literature lacks specific studies on the spinal cord effects of fluid
therapy, in patients with acute spinal cord injury, a prevalence of hyponatremia
much higher than in the general medical or surgical patient population has been
reported [81]. This study did not elucidate the ethiology of hyponatremia, and did
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346340

not consider type and amount of fluids administered. However, the occurrence of
hyponatremia after acute spinal cord injury stresses the importance of appropriate
fluid management in these patients, mostly to prevent the consequences of
reduced plasma osmolality, which might exacerbate spinal cord edema. Labo-
ratory researches have demonstrated that hypertonic saline decreases spinal cord
water content [13], and may provide protection after mechanical injury [82].
Water and electrolytes disturbances
Diabetes insipidus
Diabetes insipidus (DI) is a common sequelae of pituitary and hypothalamic
lesions, but it can also occur after head trauma or intracranial surgery. Patients
with brain death also commonly develop DI, and it should be remembered that
DI may also occur during phenytoin use, in alcohol intoxication, and bacte-
rial meningitis.
DI is a metabolic disorder due to a decreased secretion of antidiuretic hormone
(ADH), resulting in failure of tubular reabsorbtion of water. Polyuria (>30 mL/
kg/h or, in an adult, >200 mL/h), progressive dehydration, and hypernatremia
subsequently occur. Diabetes insipidus is present when the urine output is
excessive, the urine osmolality is inappropriately low relative to serum osmolality
(above normal because of water loss), and the urine specific gravity is lower than
1.002 (Table 4).
Management of DI requires careful balancing of intake and output, mostly to
avoid fluid overload
Each hour the patient should receive maintenance fluids plus three quarters
of the previous hour’s urine output, or plus the previous hour’s urine output minus
50 mL. Half-normal saline and D5W are commonly used as replacement fluids,
Table 4
Principal water-electrolytes disorders
DI SIADH CSWS
Etiology Reduced secretion
of ADH
Excessive release
of ADH
Release of brain
natriuretic factor
Urine Output > 30 ml/kg/h
specific gravity < 1.002
Sodium < 15 mEq/l > 20 mEq/l > 50 mEq/l
Osmolality vs.
serum osmolality
Lower Higher Higher
Serum Sodium Hypernatremia Hyponatremia Hyponatremia
Osmolality Hyperosmolality Hypoosmolality
Intravascular
volume
Reduced Normal or increased Reduced
Abbreviations: ADH, antidiuretic hormone; CSWS, celebral salt-wasting syndrome; DI, Diabetes
insipidus; SIADH, syndrome of inappropriate antidiuretic hormone secretion.
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 341

with appropriate potassium supplementation. Serum sodium, potassium, and gly-
cemic values should be checked frequently. In the presence of urine output higher
than 300 mL/h, at least for 2 hours, it is now standard practice to administer
aqueous vasopressin [5-10 IU, intramuscularly (i.m.), or subcutaneously (s.c.),
q 6 h] or the synthetic analog of ADH, desmopressin acetate (DDAVP: 0.5–2 mg,
intravenously (i.v.), q 8 h; or by nasal inhalation, 10–20 mg).
Syndrome of inappropriate antidiuretic hormone secretion
Various cerebral pathologic processes (mostly head trauma) can result in
excessive release of ADH, which causes continued renal excretion of sodium,
despite hyponatremia and associated hypo-osmolality. Urine osmolality is there-
fore high, relative to serum osmolality (Table 4). It should be remembered that
the syndrome of inappropriate antidiuretic hormone secretion (SIADH) can also
be the result of overadministration of free water (D5W) in patients who cannot
excrete free water, because of excess of ADH.
Management
The mainstay of treatment of SIADH is fluid restriction, usually to about
1000 mL/24 h of an iso-osmolar solution. If hyponatremia is severe (lower than
110–115 mEq/L) administration of hypertonic (3–5%) saline and furosemide
may be appropriate. Great care is required to avoid rapid correction of severe
hyponatremia. A good rule is to restore serum sodium levels at a rate of about
2 mEq/L/h.
Cerebral salt-wasting syndrome
Cerebral salt-wasting syndrome (CSWS) is frequently seen in patients with
subarachnoid hemorrhage, and is characterized by hyponatremia, volume con-
traction, and high urine sodium concentration (Table 4).
Management
The therapy is to reestablish normovolemia with the administration of sodium-
containing solutions.
The distinction between SIADH and CSWS is very important, because fluid
treatment of theses two syndromes is quite different (fluid restriction versus fluid
infusion). It should be stressed that in patients with SAH, in whom normo/
hypervolemia is advocated, fluid restriction (that is, further volume contraction)
may be especially deleterious.
Conclusion
Fluid management has progressed rapidly in the last 3 decades. Current
regimens are sufficient to restore systemic perfusion in the majority of pa-
tients undergoing surgery. However, important questions still remain to be
answered regarding the frequency of complications of current fluid therapy
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346342

and the comparative advantages of different fluid formulations in a variety of
clinical circumstances.
As neuroanesthesiologists/intensivists, we should always remember that we
treat patients and not only brains. Thus, with the exception of patients with
SIADH, the old dogma that states that patients with intracranial pathology should
be kept ‘‘dry’’ (‘‘run them dry’’) should be abandoned, and be replaced by ‘‘run
them isovolemic, isotonic, and isooncotic.’’
References
[1] Tommasino C. Fluid management. In: Newfield P, Cottrell JE, editors. Handbook of neuro-
anesthesia. 2nd edition. New York: Lippincott-Williams and Wilkins; 1999. p. 368–84.
[2] Shenkin HA, Benzier HO, Bouzarth W. Restricted fluid intake: rational management of the
neurosurgical patient. J Neurosurg 1976;45:432–6.
[3] Chestnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining
outcome from severe head injury. J Trauma 1993;34:216–22.
[4] Starling EH. In: Schaefer E, editor. Textbook of physiology. London: Caxton; 1898. p. 285–311.
[5] Fenstermacher JD, Johnson JA. Filtration and reflection coefficients of the rabbit blood–brain
barrier. Am J Physiol 1966;211:341–6.
[6] Hindman BJ, Funatsu N, Cheng DCH, et al. Differential effect of oncotic pressure on cerebral
and extracerebral water content during cardiopulmonary bypass in rabbits. Anesthesiology
1990;73:951–7.
[7] Tommasino C, Moore S, Todd MM. Cerebral effects of isovolemic hemodilution with crystalloid
or colloid solutions in normal rabbits. Crit Care Med 1988;16:862–8.
[8] Zornow MH, Todd MM, Moore SS. The acute cerebral effects of changes in plasma osmolality
and oncotic pressure. Anesthesiology 1987;67:936–41.
[9] Kaieda R, Todd MM, Cook LN, et al. Acute effects of changing plasma osmolality and colloid
oncotic pressure on the formation of brain edema after cryogenic injury. Neurosurgery 1989;
24:671–8.
[10] Kaieda R, Todd MM, Warner DS. Prolonged reduction in colloid oncotic pressure does not
increase brain edema following cryogenic injury in rabbits. Anesthesiology 1989;71:554–60.
[11] Zornow MH, Scheller M, Todd MM, et al. Acute cerebral effects of isotonic crystalloid
and colloid solutions following cryogenic brain injury in the rabbit. Anesthesiology 1988;69:
185–91.
[12] Drummond JC, Patel PM, Cole DJ, et al. The effect of the reduction of colloid reduction of
oncotic pressure, with and without reduction of osmolality, on post-traumatic cerebral edema.
Anesthesiology 1998;88:993–1002.
[13] Todd MM, Tommasino C, Moore S. Cerebral effects of isovolemic hemodilution with a hyper-
tonic saline solution. J Neurosurg 1985;63:944–8.
[14] Harrison MJG. Influence of haematocrit in the cerebral circulation. Cerebrovasc Brain Metabol
Rev 1989;1:55–67.
[15] Hudak ML, Koehler RC, Rosenberg AA, et al. Effect of hematocrit on cerebral blood flow. Am J
Physiol 1986;251:H63–70.
[16] Brown MM, Wade JPH, Marshall J. Fundamental importance of arterial oxygen content in the
regulation of cerebral blood flow in man. Brain 1985;108:81–93.
[17] Jones MD, Traystman RJ, Simmons MA, et al. Effects of changes in arterial O2 content on
cerebral blood flow in the lamb. Am J Physiol 1981;240:H209–15.
[18] Todd MM, Wu B, Maktabi M, et al. Cerebral blood flow and oxygen delivery during hypoxemia
and hemodilution: role of oxygen content. Am J Physiol 1994;267:H2025–31.
[19] Todd MM, Wu B, Warner DS. The hemispheric cerebrovascular response to hemodilution is
attenuated by a focal cryogenic brain injury. J Neurotrauma 1994;11:149–60.
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 343

[20] Tommasino C, Ravussin P. Pressione oncotique et hemodilution. Ann Fran Anesth Reanim
1994;13:62–7.
[21] Tu KY, Heros RC, Karacostas D, et al. Isovolemic hemodilution in experimental focal cerebral
ischemia. Part 2: effects on regional cerebral blood flow and size of infarction. J Neurosurg
1988;69:82–91.
[22] Reasoner DK, Ryu KH, Hindman BJ, et al. Marked hemodilution increases neurologic injury
after focal cerebral ischemia in rabbits. Anesth Analg 1996;82:61–7.
[23] Weed LH, McKibben PS. Pressure changes in the cerebrospinal fluid following intravenous
injection of solutions of various concentrations. Am J Physiol 1919;48:512–30.
[24] Go KG, Van Woudenberg F, DeLange WE, et al. The influence of saline-loading on cold-induced
cerebral oedema in the rat. J Neurol Sci 1972;16:209–14.
[25] Korosue K, Heros RC, Ogilvy CS, et al. Comparison of crystalloids and colloids for hemodi-
lution in a model of focal cerebral ischemia. J Neurosurg 1990;73:576–84.
[26] Shapira Y, Artru AA, Qassam N, et al. Brain edema and neurologic status with rapid infusion of
0.9% saline or 5% glucose after head trauma. J Neurosurg Anesthesiol 1995;7:17–25.
[27] Tranmer BI, Iacobacci RI, Kindt GW. Effects of crystalloid and colloid infusions on intracranial
pressure and computerized electroencephalographic data in dogs with vasogenic brain edema.
Neurosurgery 1989;25:173–9.
[28] Prough DS, Johnson JC, Poole GV, et al. Effects on intracranial pressure of resuscitation from
hemorrhagic shock with hypertonic saline vs lactated Ringer’s solution. Crit Care Med
1985;13:407–11.
[29] Cascino T, Baglivo J, Conti J, et al. Quantitative CT assessment of furosemide- and mannitol-
induced changes in brain water content. Neurology 1983;33:898–903.
[30] Scheller MS, Zornow MH, Oh YS. A comparison of the cerebral and hemodynamic effects of
mannitol and hypertonic saline in a rabbit model of brain injury. J Neurosurg Anesthesiol
1991;3:291–6.
[31] Zornow MH, Scheller MS, Shackford SR. Effect of a hypertonic lactated Ringer’s solution on
intracranial pressure and cerebral water content in a model of traumatic brain injury. J Trauma
1989;29:484–8.
[32] DiMattio J, Hochwald GM, Malhan C, et al. Effects of changes in serum osmolarity on bulk flow
of fluid into cerebral ventricles and on brain water content. Pflugers Arch 1975;359:253–64.
[33] Donato T, Shapira Y, Artru A, et al. Effect of mannitol on cerebrospinal fluid dynamics and brain
tissue edema. Anesth Analg 1994;78:58–66.
[34] Hochwald GM, Wald A, DiMattio J, et al. The effects of serum osmolality on cerebrospinal fluid
volume flow. Life Sci 1974;15:1309–16.
[35] Rackow EC, Fein IA, Leppo J. Colloid osmotic pressure as a prognostic indicator of pulmonary
edema and mortality in the critically ill. Chest 1977;72:709–13.
[36] Bruno A, Biller J, Adams HP Jr, et al. Acute blood glucose level and outcome from ischemic
stroke. Trial of ORG 10172 in acute stroke treatment (TOAST) investigators. Neurology 1999;
52:280–4.
[37] Lam AM, Winn HR, Cullen BF, et al. Hyperglycemia and neurological outcome in patients with
head injury. J Neurosurg 1991;75:545–51.
[38] Longstreth WT, Inui TS. High blood glucose level on hospital admission and poor neurological
recovery after cardiac arrest. Ann Neurol 1984;15:59–63.
[39] Rovlias A, Kotsou S. The influence of hyperglycemia on neurologic outcome in patients with
severe head injury. Neurosurgery 2000;46:335–42.
[40] Wass CT, Lanier WL. Glucose modulation of ischemic brain injury: review and clinical recom-
mendations. Mayo Clin Proc 1996;71:801–12.
[41] Siesjo BK. Pathophysiology and treatment of focal cerebral ischemia. Part I: pathophysiology.
J Neurosurg 1992;77:169–84.
[42] Ravussin P, Archer DP, Meyer E, et al. The effects of rapid infusions of saline and mannitol on
cerebral blood volume and intracranial pressure in dogs. Can Anaesth Soc J 1985;32:506–15.
[43] Ravussin P, Archer DP, Tyler JL, et al. Effects of rapid mannitol infusion on cerebral blood
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346344

volume. A positron emission tomographic study in dogs and man. J Neurosurg 1986;64:
104–13.
[44] Kaufman AM, Cardoso ER. Aggravation of vasogenic cerebral edema by multiple-dose man-
nitol. J Neurosurg 1992;77:584–9.
[45] Kofke WA. Mannitol. Potential for rebound intracranial hypertension? J Neurosurg Anesthesiol
1993;5:1–3.
[46] Marchall LF, Smith RW, Rauscher LA, et al. Mannitol dose requirements in brain-injured
patients. J Neurosurg 1978;48:169–72.
[47] Garay RP, Hannaert PA, Nazaret C, et al. The significance of the relative effects of loop diuretics
and anti-brain edema agents on the Na+,K+,Cl� cotransport system and the Cl� /NaCO3�anion exchanger. Arch Pharmacol 1986;334:202–9.
[48] Pollay M, Fullenwider C, Roberts PA, et al. Effect of mannitol and furosemide on blood–brain
osmotic gradient and intracranial pressure. J Neurosurg 1983;59:945–50.
[49] Cottrell JE, Robustelli A, Post K, et al. Furosemide- and mannitol-induced changes in intra-
cranial pressure and serum osmolality and electrolytes. Anesthesiology 1977;47:28–30.
[50] Wilkinson HA, Rosenfeld S. Furosemide and mannitol in the treatment of acute experimental
intracranial hypertension. Neurosurgery 1983;12:405–10.
[51] Gunnar W, Jonasson O, Merlotti G, et al. Head injury and hemorrhagic shock: studies of the
blood brain barrier and intracranial pressure after resuscitation with normal saline solution, 3%
saline solution, and dextran-40. Surgery 1988;103:398–407.
[52] Sheikh AA, Matsuoka T, Wisner DH. Cerebral effects of resuscitation with hypertonic saline and
a new low-sodium hypertonic fluid in hemorrhagic shock and head injury. Crit Care Med 1996;
24:484–8.
[53] Vassar MJ, Fisher RP, O’Brien PE, et al. A multicenter trial for resuscitation of injured patients
with 7.5% sodium chloride. The effect of added dextran 70. The multicenter group for the study
of hypertonic saline in trauma patients. Arch Surg 1993;128:1003–11.
[54] Vassar MJ, Perry CA, Gannaway WL, Holcroft JW. 7.5% sodium chloride/dextran for resusci-
tation of trauma patients undergoing helicopter transport. Arch Surg 1991;126:1065–72.
[55] Gemma M, Cozzi S, Tommasino C, et al. 7.5% hypertonic saline versus 20% mannitol during
elective neurosurgical supratentorial procedures. J Neurosurg Anesthesiol 1997;9:329–34.
[56] Horn P, Munch E, Vajkoczy P, et al. Hypertonic saline solution for control of elevated intra-
cranial pressure in patients with exhausted response to mannitol and barbiturates. Neurol Res
1999;21:758–64.
[57] Suarez JI, Qureshi AI, Bhardwaj A, et al. Treatmernt of refractory intracranial hypertension with
23.4% saline. Crit Care Med 1998;26:1118–22.
[58] Mattox KL, Maningas PA, Moore EE, et al. Prehospital hypertonic saline/dextran infusion for
post-traumatic hypotension. The USA Multicenter Trial. Ann Surg 1991;213:482–91.
[59] Prough DS, Whitley JM, Taylor CL, et al. Rebound intracranial hypertension in dogs after
resuscitation with hypertonic solutions from hemorrhagic shock accompanied by an intracranial
mass lesion. J Neurosurg Anesthesiol 1999;11:102–11.
[60] Qureshi AI, Suarez JI, Bhardwaj A. Malignant cerebral edema in patients with hypertensive
intracerebral hemorrhage associated with hypertonic saline infusion: a rebound phenomenon?
J Neurosurg Anesthesiol 1998;10:188–92.
[61] Berger S, Schurer L, Hartl R, et al. Reduction of post-traumatic intracranial hypertension
by hypertonic/hyperoncotic saline/dextran and hypertonic mannitol. Neurosurgery 1995;37:
98–107.
[62] Hartl R, Ghajar J, Hochleuthner H, et al. Hypertonic/hyperoncotic saline reliably reduces ICP in
severely head-injuried patients with intracranial hypertension. Acta Neurochir Suppl 1997;70:
126–9.
[63] Schwarz S, Schwab S, Bertram M, et al. Effects of hypertonic saline hydroxyethyl starch solution
and mannitol in patients with increased intracranial pressure after stroke. Stroke 1998;29:1550–5.
[64] McFarlane C, Lee A. A comparison of Plasmalyte 148 and 0.9% saline for intra-operative fluid
replacement. Anaesthesia 1994;49:779–81.
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346 345

[65] Scheingraber S, Rehm M, Sehmisch C, et al. Rapid saline infusion produces hyperchloremic
acidosis in patients undergoing gynecologic surgery. Anesthesiology 1999;90:1247–9.
[66] Wilcox CS. Release of renin and angiotensin II into plasma and lymph during hyperchloremia.
Am J Physiol 1987;253:F734–41.
[67] Cully MD, Larson CP Jr, Silverberg GD. Hetastarch coagulopathy in a neurosurgical patient.
Anesthesiology 1987;66:706–7.
[68] Trumble ER, Muizelaar JP, Myseros JS, et al. Coagulopathy with the use of hetastarch in the
treatment of vasospasm. J Neurosurg 1995;82:44–7.
[69] Strauss RG, Stansfield C, Henricksen RA. Pentastarch may cause fewer effects on coagulation
than hetastarch. Transfusion 1988;28:257–60.
[70] Zornow MH, Prough DS. Fluid management in patients with traumatic brain injury. New Horiz
1995;3:488–97.
[71] Berendes E, Walter M, Cullen P, et al. Secretion of brain natriuretic peptide in patients with
aneurysmal subarachnoid haemorrhage. Lancet 1997;349:245–9.
[72] Okuchi K, Fujioka M, Fujikawa A, et al. Rapid natriuresis and preventive hypervolaemia for
symptomatic vasospasm after subarachnoid hemorrhage. Acta Neurochir 1996;138:951–6.
[73] Wijdicks EF, Ropper AH, Hunnicutt EJ, et al. Atrial natriuretic factor and salt wasting after
aneurysmal subarachnoid hemorrhage. Stroke 1991;22:1519–24.
[74] Awad IA, Carter LP, Spetzler RF, et al. Clinical vasospasm after subarachnoid hemorrhage:
response to hypervolemic hemodilution and arterial hypertension. Stroke 1987;18:365–72.
[75] Hyodo A, Heros RC, Tu YK, et al. Acute effects of isovolemic hemodilution with crystalloids in
a canine model of focal cerebral ischemia. Stroke 1989;20:534–40.
[76] Hartmann A, Rommel T, Dettmers C, et al. Hemodilution in cerebral infarcts. Arzneimittelfor-
schung 1991;41:348–51.
[77] Grotta JC. Hypervolemic hemodilution treatment of acute stroke: results of a randomized multi-
center trial using pentastarch. Stroke 1989;20:317–23.
[78] Italian Acute Stroke Study Group. Haemodilution in acute stroke: results of the Italian Haemo-
dilution Trial. Lancet 1988;1:318–21.
[79] Mast H, Marx P. Neurological deterioration under isovolemic hemodilution with hydroxyethyl
starch in acute cerebral ischemia. Stroke 1991;22:680–3.
[80] Scandinavian Stroke Study Group. Multicenter trial of hemodilution in acute ischemic stroke:
results in the total patient population. Stroke 1987;18:691–9.
[81] Peruzzi WT, Shapiro BA, Meyer PR Jr, et al. Hyponatremia in acute spinal cord injury. Crit Care
Med 1994;22:252–8.
[82] Sumas ME, Legos JJ, Nathan D, et al. Tonicity of resuscitative fluids influences outcome after
spinal cord injury. Neurosurgery 2001;48:167–72.
C. Tommasino / Anesthesiology Clin N Am 20 (2002) 329–346346

Interventional neuroradiology—anesthetic
considerations
Tomoki Hashimoto, MDa,d, Dhanesh K. Gupta, MDa,d,William L. Young, MDa,b,c,d,*
aDepartment of Anesthesia and Perioperative Care, University of California,
San Francisco, CA 94110, USAbDepartment of Neurological Surgery, University of California, San Francisco, CA 94110, USA
cDepartment of Neurology, University of California, San Francisco, CA 94110, USAdCenter for Cerebrovascular Research, University of California, San Francisco,
San Francisco General Hospital, 1001 Potrero Avenue, Room 3C-38,
San Francisco, CA 94110, USA
Interventional neuroradiology (INR) is a hybrid of traditional neurosurgery
and neuroradiology, with certain overlaps with aspects of head-and-neck
surgery. It can be broadly defined as treatment of central nervous system (CNS)
disease by endovascular access for the purpose of delivering therapeutic
agents, including both drugs and devices [1]. Because of a recent advance-
ment in the field of INR [2], more anesthesiologists are involved in care of
patients undergoing INR procedures. Anesthesiologists have several important
concerns when providing care to patients who undergo INR procedures,
including (1) maintenance of patient immobility and physiologic stability; (2)
manipulating systemic or regional blood flow; (3) managing anticoagulation;
(4) treating and managing sudden unexpected complications during the pro-
cedure; (5) guiding the medical management of critical care patients during
transport to and from the radiology suites; and (6) rapid recovery from
anesthesia and sedation during or immediately after the procedure to facilitate
neurologic examination and monitoring [3,4]. To achieve these goals, anes-
thesiologists should be familiar with specific radiological procedures and their
potential complications.
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00005 -0
This work is supported in part by National Institutes of Health, Grants K24-NS02091 (W.L.Y.).
* Corresponding author. Center for Cerebrovascular Research, University of California, San
Francisco General Hospital, 1001 Potrero Ave., Room 3C-38, San Francisco, CA 94110, USA.
E-mail address: [email protected] (W.L. Young).
Anesthesiology Clin N Am
20 (2002) 347–359

Preanesthetic considerations
The preanesthetic evaluation of a patient undergoing a potentially long
diagnostic and therapeutic procedure in the neuroradiology suite expands on
the routine preanesthetic examination of the neurosurgical patient. Airway eval-
uation should include routine evaluation of the potential ease of laryngoscopy in
an emergent situation, and also take into the account the fact that, with the head
and neck kept in a neutral position, sedation may compromise airway patency.
Further, this patient population often includes head-and-neck tumor patients with
their associated airway considerations.
Baseline blood pressure and cardiovascular reserve should be assessed care-
fully, especially when blood pressure manipulation and perturbations are antici-
pated. A careful neurologic examination should be performed to characterize any
deficits that may be present prior to the procedure, and special note should be
made of the patient’s sensorium. Furthermore, careful padding of pressure points
may assist in the patient’s ability to tolerate a long period of lying supine and
motionless and decrease the requirement for sedation, anxiolysis, and analgesia.
In addition to the issues normally considered during the preanesthetic evaluation
of the neurosurgical patient, the anesthesiologist should review the patient’s
previous experiences with angiography, noting if there were adverse reactions to
radiographic contrast agents, such as allergy or excessive dehydration. Because
of the possibility of significant radiation exposure, the possibility of pregnancy in
female patients should be explored.
Prophylaxis for cerebral ischemia is in a state of development. Some centers
use a variety of agents such as oral nimodipine for this purpose. The use of
calcium channel blockers has been suggested to decrease catheter-induced vaso-
spasm as well; transdermal nitroglycerin has also been used for this purpose.
Monitoring and vascular access
Secure intravenous (i.v.) access should be available with adequate extension
tubing to allow drug and fluid administration at maximal distance from the image
intensifier during fluoroscopy. Access to i.v. or arterial catheters can be difficult
when the patient is draped and the arms are restrained at the sides. Stopcocks and
nonlocking tubing connections under the drapes should be minimized. Prior to
covering the patient, the tightness of connections between segments of tubing
should be verified. Infusions of anticoagulant or potent medications, such as
nitroprusside and remifentanil, should be through minimal dead space, into ports
that are as proximal to the patient as possible (e.g., into a T-connector at an i.v.
catheter). This allows the infusion of medications to be relatively independent of
the rate of the i.v. carrier fluid.
Standard monitors should be applied, regardless of anesthetic technique. For
i.v. sedation, capnography sampling via the sampling port of special nasal
cannula is especially useful. A pulse oximeter probe can be placed on the great
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359348

toe of the leg that will receive the femoral introducer sheath. This may give an
early warning of femoral artery obstruction or distal thromboembolism.
For intracranial procedures and postoperative care, beat-to-beat arterial pres-
sure monitoring and blood sampling can be facilitated by an arterial line. A side
port of the femoral artery introducer sheath can be used, but most radiologists will
remove the sheath immediately after the procedure. Using a coaxial or triaxial
catheter system, arterial pressure at the carotid artery, vertebral artery, and the
distal cerebral circulation can be measured [5]. The presence of a coaxial catheter
frequently underestimates the systolic and overestimates the diastolic pressure;
however, mean pressures are reliable, and may be used to safely monitor the
induction of either hyper- or hypotension. In a patient who requires continuous
blood pressure monitoring postoperatively, it is convenient to have a separate
radial arterial blood pressure catheter. Bladder catheters are required for most of
the procedures; they assist in fluid management as well as patient comfort. A
significant volume of heparinized flush solution and radiographic contrast is
often used.
Radiation safety
There are three sources of radiation in the INR suite: direct radiation from the
x-ray tube, leakage (through the collimators’ protective shielding), and scattered
(reflected from the patients and the area surrounding the body part to be imaged).
A fundamental knowledge of radiation safety is essential for all staff members
working in an INR suite. It must be realized that the amount of exposure de-
creases proportionally to the square of the distance from the source of radiation
(inverse square law). It should also be realized that digital subtraction angiog-
raphy delivers considerably more radiation than fluoroscopy.
Optimal protection would dictate that all personnel should wear lead aprons,
thyroid shields, and radiation exposure badges. The lead aprons should be
periodically evaluated for any cracks in the lead lining that may allow accidental
radiation exposure. Movable lead glass screens may provide additional protection
for the anesthesia team. Clear communication between the INR and anesthesia
teams is crucial for limiting radiation exposure. With proper precautions, the
anesthesia team should be exposed to less than the annual recommended limit for
health care workers (see http://pdg.lbl.gov/).
Anesthetic technique
Choice of anesthetic technique is a controversial area, and varies between
centers. There are no data that support improved outcome with one technique or
another. There appears to be a trend to move more towards general endotracheal
anesthesia, but it is highly dependent on local practice and training.
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359 349

Intravenous sedation
Primary goals of anesthetic choice for i.v. sedation are to alleviate pain,
anxiety and discomfort, and to provide patient immobility. A rapid recovery from
sedation is often required for neurologic testing.
Many neuroangiographic procedures, while not painful per se, can be psycho-
logically stressful. This is especially true when there is a risk of serious stroke or
death, particularly patients who have already suffered a preoperative hemorrhage
or stroke. There may be an element of pain associated with injection of contrast
into the cerebral arteries (burning) and with distention or traction on them (head-
ache). A long period of lying can cause significant pain and discomfort.
A variety of sedation regimens are available, and specific choices are based on
the experience of the practitioner and the aforementioned goals of anesthetic
management. Common to all i.v. sedation techniques is the potential for upper
airway obstruction. Placement of nasopharyngeal airways may cause troublesome
bleeding in anticoagulated patients, and is generally avoided. Laryngeal Mask
Airways may be useful in rare emergencies in patients with difficult airway.
Endotracheal intubation, however, remains a mainstay for securing the airway
during neurological crises.
General anesthesia
The primary reason for employing general anesthesia is to reduce motion
artifacts and to improve the quality of images, especially in small children and
uncooperative adult patients. This is especially pertinent to INR treatment of
spinal pathology, in which extensive multilevel angiography may be performed.
The specific choice of anesthesia may be guided primarily by other cardio- and
cerebrovascular considerations. Total i.v. anesthetic techniques, or combinations
of inhalational and i.v. methods, may optimize rapid emergence [6]. To date,
pharmacologic protection against ischemic injury during neurosurgical proce-
dures has not been proven. A theoretical argument could be made for eschewing
the use of N2O because of the possibility of introducing air emboli into the
cerebral circulation, but there are no data to support this.
Anticoagulation
Careful management of coagulation is required to prevent thromboembolic
complications during and after the procedures. Whether heparinization should be
used for every case of intracranial catheterization is not clear to date. Generally,
after a baseline activated clotting time (ACT) is obtained, i.v. heparin (70 units/kg)
is given to a target prolongation of two to three times baseline. Heparin can then be
given continuously or as an intermittent bolus with hourly monitoring of ACT.
Occasionally, a patient may be refractory to attempts to obtain adequate anti-
coagulation. Switching from bovine to porcine heparin or vice versa should be
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359350

considered. If antithrombin III deficiency is suspected, administration of fresh-
frozen plasma may be necessary. At the end of the procedure, heparin may need to
be reversed with protamine.
Antiplatelet agents (aspirin, ticlopidine, and the glycoprotein IIb/IIIa receptor
antagonists) are used quite extensively in patients with coronary stents, and may
have great relevance for patients undergoing INR procedures. Activation of the
glycoprotein IIb/IIIa receptor is a final common pathway for platelet aggregation.
Abciximab (ReoPro), a chimeric murine–human monoclonal antibody that di-
rectly binds to the receptor, has been shown to decrease mortality and morbidity
after coronary stenting [7]. Other agents in this class include the peptide receptor
antagonists, Eptifibatide (Integrilin) and Tirofiban (Aggrastat).
These agents have various pharmacokinetic and pharmacodynamic properties.
Based on experiences in coronary stenting, several basic observations on their use
become clear. First, the effects of these agents on platelet aggregation are difficult
to monitor clinically because there is no accurate bedside test of platelet aggre-
gation. Second, the duration of the effects is approximately 12–24 hours. Rapid
reversal of antiplatelet activity can only be achieved by platelet transfusion. Final-
ly, use of these agents along with heparin may result in unexpected hemorrhage.
Therefore, reducing procedural heparin dosage and early removal of vascular
access sheaths should be carefully considered to decrease bleeding complications.
The sustained long-term reduction in morbidity and mortality of coronary throm-
bosis patients (undergoing angioplasty/stenting or thrombolysis) by an antiplatelet
agent has led to great interest for use in endovascular procedures of the CNS, but
their use is not clearly defined in the setting of cerebrovascular disease.
Superselective anesthesia functional examination (SAFE)
SAFE is carried out to determine, prior to therapeutic embolization, if the tip
of the catheter has been inadvertently placed proximal to the origin of nutritive
vessels to eloquent regions, either in the brain or spinal cord [8]. Such testing is
an extension of the Wada and Rasmussen test in which amobarbital is injected
into the internal carotid artery to determine hemispheric dominance and language
function. Its primary application is in the setting of brain arteriovenous mal-
formation (BAVM) treatment, but it may also be used for tumor or other vascular
malformation work. Prior to the testing, the patient should be fully awake from
sedation or general anesthesia. Careful selection of motivated patients and
preoperative teaching may decrease the anxiolytic requirements of these patients
and ensure ideal testing conditions. This topic is reviewed elsewhere [4].
Deliberate hypotension
The two primary indications for induced hypotension are (1) to test cerebro-
vascular reserve in patients undergoing carotid occlusion, and (2) to slow flow in
a feeding artery of BAVMs before glue injection.
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359 351

Themost important factor in choosing a hypotensive agent is the ability to safely
and expeditiously achieve the desired reduction in blood pressure while maintain-
ing the physiological stability of the patients. The choice of agent should be
determined by the experience of the practitioner, the patient’s medical condition,
and the goals of the blood pressure reduction in a particular clinical setting.
Intravenous adenosine has been used to induce transient cardiac pause, and
may be a viable method of partial flow arrest [9,10]. Further study for its safety
and efficacy is needed.
Deliberate hypertension
During acute arterial occlusion or vasospasm, the only practical way to in-
crease collateral blood flow may be an augmentation of the collateral perfusion
pressure by raising the systemic blood pressure. The Circle of Willis is a primary
collateral pathway in cerebral circulation. However, in as many as 21% of other-
wise normal subjects, the circle may not be complete. There are also secondary
collateral channels that bridge adjacent major vascular territories, most importantly
for the long circumferential arteries that supply the hemispheric convexities. These
pathways are known as the pial-to-pial collateral or leptomeningeal pathways.
The extent to which the blood pressure has to be raised depends on the condition
of the patient and the nature of the disease. Typically, during deliberate hyperten-
sion the systemic blood pressure is raised by 30–40% above the baseline or until
ischemic symptoms resolve. Phenylephrine is usually the first line agent for delib-
erate hypertension, and is titrated to achieve the desired level of blood pressure.
Management of neurologic and procedural crises
Complications during endovascular instrumentation of the cerebral vascu-
lature can be rapid and life threatening, and require a multidisciplinary collab-
oration. Having a well thought-out plan for dealing with intracranial catastrophe
may make the difference between an uneventful outcome and death. Rapid and
effective communication between the anesthesia and radiology teams is critical.
The primary responsibility of the anesthesia team is to preserve gas exchange
and, if indicated, secure the airway. Simultaneous with airway management, the
first branch in the decision-making algorithm is for the anesthesiologist to
communicate with the INR team and determine whether the problem is hemor-
rhagic or occlusive. In the setting of vascular occlusion, the goal is to increase
distal perfusion by blood pressure augmentation with or without direct throm-
bolysis. If the problem is hemorrhagic, immediate cessation of heparin and re-
versal with protamine is indicated. As an emergency reversal dose, 1 mg protamine
can be given for each 100 units heparin total dosage during the case. The ACT
can then be used to fine tune the final protamine dose.
Bleeding catastrophes are usually heralded by headache, nausea, vomiting,
and vascular pain related to the area of perforation. Sudden loss of consciousness
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359352

is not always due to intracranial hemorrhage. Seizures, as a result of contrast
reaction or transient ischemia, and the resulting post-ictal state can also result in
an obtunded patient. In the anesthetized patient, the sudden onset of bradycardia
or the radiologist’s diagnosis of extravasation of contrast may be the only clues to
a developing hemorrhage.
Postoperative management
After INR procedures, patients spend the immediate postoperative period in a
monitored setting to watch for signs of hemodynamic instability or neurologic
deterioration. Blood pressure control, either induced hypotension or induced
hypertension, may be continued during the postoperative period. Complicated
cases may go first to CT or some kind of physiologic imaging such as single
photon emission computed tomography (SPECT) scanning; only rarely is an
emergent craniotomy indicated.
Specific procedures
Brain arteriovenous malformations (BAVMs).
BAVMs are typically large, complex lesions made up of a table of abnormal
vessels (called the nidus) frequently containing several discrete fistulae [5]. They
are often called cerebral or pial arterio-venous malformations. There are usually
multiple feeding arteries and draining veins. The goal of the therapeutic embo-
lization is to obliterate as many of the fistulae and their respective feeding arteries
as possible. BAVM embolization is usually an adjunct for surgery or radiotherapy
[11]. In rare cases, embolization treatment is aimed for total obliteration. SAFE is
frequently used during BAVM embolization.
There are generally two schools of thought on how to manage anesthesia in the
patient undergoing endovascular therapy, especially with permanent agents such as
cyanoacrylate glues. One must rely on the knowledge of neuroanatomy and
vascular architecture to ascertain the likelihood of neurologic damage after
deposition of the embolic agents. The ‘‘anatomy’’ school, therefore, will prefer
to embolize under general anesthesia. Arguments for this approach include
improved visualization of structures with the absence of patient movement,
especially if temporary apnea is used. Further, it is argued that if the glue is placed
‘‘intranidal,’’ then, by definition, no normal brain is threatened. There are two
major concerns for this approach. A considerable variation in the normal local-
ization of function exists, and cerebral pathology may cause neurologic function to
shift from its native location to another one. The other school, which we might call
the ‘‘physiologic’’ school, trades off the potential for patient movement for the
increased knowledge of the true functional anatomy of a given patient. Localization
of cerebral function may not always follow textbook descriptions, as described in
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359 353

the section on SAFE. Furthermore, the BAVMnidus or a previous hemorrhage may
result in a shift or relocalization of function. The ‘‘physiologic’’ approach demands,
at the present, careful titration of sedation to wake the patient for SAFE before
injection of embolic material.
The cyanoacrylate glues offer relatively ‘‘permanent’’ closure of abnormal
vessels. Although less durable, polyvinyl alcohol microsphere embolization is
also commonly used. If surgery is planned within days after PVA embolization, the
rate of recanalization is low and PVA is felt to be easier and safer to work with.
Advances in polymer development may obviate some of the risks of glue therapy.
Dural arterio-venous malformations
Dural AVM is currently considered an acquired lesion resulting from venous
dural sinus stenosis or occlusion, opening of potential arterio-venous shunts, and
subsequent recanalization. Symptoms are variable according to which sinus is
involved. Dural AVMs may be fed by multiple meningeal vessels, and therefore,
multistaged embolization is usually performed. SAFE is performed in certain
vessels such as the middle meningeal artery and the ascending pharyngeal artery
to evaluate the blood supply to peripheral cranial nerves and the possible
existence of dangerous extra- to intracranial anastomosis. Complete obliteration
is not always necessary considering the purpose of treatment, which is to reduce
risk of bleeding or to alleviate symptoms. Subsequent spontaneous thrombosis
can be expected in view of pathogenesis of this disease.
It is important to bear in mind that dural AV fistulas can induce increased venous
pressure. Venous hypertension of pial veins is a risk factor for intracranial
hemorrhage. Additionally, the venous hypertension should be factored into
estimating safe levels of reductions in systemic arterial, and therefore, cerebral
perfusion pressure.
Carotid cavernous and vertebral fistulae
Carotid cavernous fistulae (CCF) are direct fistulae usually caused by trauma
to the cavernous carotid artery leading to communication with the cavernous
sinus, usually associated with basal skull fracture. Treatment of CCF, a challeng-
ing surgical procedure, has become relatively easier with the development of
detachable balloons [12]. Vertebral artery fistulae are connections to surrounding
paravertebral veins, usually as a result of penetrating trauma, but may be
congenital, associated with neurofibromatosis, or result from blunt trauma. In
addition to cerebral involvement, spinal cord function may also be impaired.
Vein of Galen malformations
These are relatively uncommon but complicated lesions that present in infants
and require a multidisciplinary approach including an anesthesiologist skilled in
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359354

the care of critically ill neonates. The patients may have intractable congestive
heart failure, myocardial lesions, intractable seizures, hydrocephalus, and mental
retardation [13].
Spinal cord lesions
Embolization may be used for intramedullary spinal AVMs, dural fistulae, or
tumors invading the spinal canal. Often, general endotracheal anesthesia with
controlled ventilation is used to provide temporary apnea that may increase the
ability to see small spinal cord arteries at the limits of angiography imaging re-
solution and exquisitely sensitive to motion artifact. For selected lesions, intra-
operative somatosensory and motor-evoked potentials may be helpful in both
anesthetized and sedated patients. Intraoperative wake-up tests may be requested
to test neurologic function during embolization.
In cases where wake-up tests might be needed, preoperative discussion of the
logistics of the wake-up procedure and the testing process may facilitate the
intraoperative management of this part of the procedure.
Carotid test occlusion and therapeutic carotid occlusion
Carotid occlusion, both permanent and temporary, may be used in several
circumstances. Skull base tumors frequently involve the intracranial or petrous
portion of the carotid artery or its proximal Willisian branches. Large or other-
wise unclippable aneurysms may be partly or completely treated by proximal
vessel occlusion. To assess the consequences of carotid occlusion in anticipation
of surgery, the patient may be scheduled for a test occlusion in which ce-
rebrovascular reserve is evaluated in several ways. A multimodal combination of
angiographic, clinical, and physiologic tests can be used to arrive at the safest
course of action for a given patient’s clinical circumstances. The judicious use of
deliberate hypotension can increase the sensitivity of the test [14,15].
Intracranial aneurysm ablation
The two basic approaches for INR therapy of cerebral aneurysms are occlusion
of proximal parent arteries and obliteration of the aneurysmal sac. The aneu-
rysmal sac may be obliterated by use of coils and balloons. However, obliterating
the aneurysmal sac while sparing the parent vessel is still challenging [16].
Manipulation of the sac may cause distal thromboembolism and rupture. In-
complete obliteration may result in recurrence and hemorrhage. The anesthesi-
ologist should be prepared for aneurysmal rupture and acute SAH at all times,
either from spontaneous rupture of a leaky sac or direct injury of the aneurysm
wall by the vascular manipulation. It should be noted after coil ablation of
aneurysms, that at the present time, there is not the same degree of certainty that
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359 355

the lesion has been completely removed from the circulation as with application
of a surgical clip. There may be areas of the aneurysmal wall that are still in
contact with the arterial blood flow and pressure. Therefore, attention to post-
operative blood pressure control is warranted.
Balloon angioplasty of cerebral vasospasm from aneurysmal SAH
Angioplasty may be used to treat symptomatic vasospasm with correlating
angiographic stenosis refractory to maximal medical therapy [17]. Angioplasty is
usually reserved for patients that have already had the symptomatic lesion sur-
gically clipped (for fear of rerupture), or for patients in the early course of symp-
tomatic ischemia to prevent transformation of a bland infarct into a hemorrhagic
one. A balloon catheter is guided under fluoroscopy into the spastic segment and
inflated to mechanically distend the constricted area.
It is also possible to perform a ‘‘pharmacologic’’ angioplasty. There is the
greatest experience with papaverine, but there are potential CNS toxic effects (see
ref. [18] for a review), but other agents such as calcium channel blockers may
find a place for this purpose.
Sclerotherapy of venous angiomas
Craniofacial venous malformations are congenital disorders causing significant
cosmetic deformities, that may impinge on the upper airway and interfere with
swallowing. Absolute alcohol (95% ethanol) opacified with contrast is injected
percutaneously into the lesion, resulting in a chemical burn to the lesion and
eventually shrinking it. The procedures are short (30–60 minutes) but painful, and
general endotracheal anesthesia is used. Complex airway involvement may require
endotracheal intubation with fiberoptic techniques [19]. Because marked swelling
often occurs immediately after alcohol injection, the ability of the patient to
maintain a patent airway must be carefully assessed in discussion with the
radiologist before extubation. Alcohol has several noteworthy side effects. First,
upon injection it can cause changes in the pulmonary vasculature and create a short-
lived shunt or a ventilation-perfusion mismatch. Desaturation on the pulse
oximeter is frequently noted after injection. Absolute alcohol may also cause
hypoglycemia, especially in younger children. Finally, the predictable intoxication
and other side effects of ethanol may be evident after emergence from anesthesia.
Angioplasty and stenting for atherosclerotic lesion
Angioplasty with or without stenting for atherosclerosis has been tried in
cervical and intracranial arteries with favorable results [20,21]. Risk of distal
thromboembolism is the major issue to be resolved in this procedure and methods.
A catheter system that employs an occluding balloon distal to the angioplasty
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359356

balloon has been proposed [22]. Carotid angioplasty and stenting may provide a
therapeutic option for patients particularly at risk of surgery. However, efficacy and
indications in relation to carotid endarterectomy remain to be determined.
Preparation for anesthetic management include, in additional to the usual
monitors and considerations already discussed, placement of transcutaneous pac-
ing leads in case of severe bradycardia or asystole from carotid body stimulation
during angioplasty. Intravenous atropine or glycopyrrolate may be used in an
attempt to mitigate against bradycardia, which almost invariably occurs to some
degree with inflation of the balloon. This powerful chronotropic response may be
difficult or impossible to prevent or control by conventional means. If indicated by
hemodynamic instability, the anesthesiologist must have the ability to immediately
administer advanced cardiac life support, including catecholamine and temporary
cardiac pacing therapy.
Potential complications include vessel occlusion, perforation, dissection,
spasm, thromboemboli, occlusion of adjacent vessels, transient ischemic epi-
sodes, and stroke. Furthermore, compared to carotid endarterectomy, there ap-
pears to be an increased incidence of cerebral hemorrhage and/or brain swelling
after carotid angioplasty [23]. Although the etiology of this syndrome is
unknown, it has been associated with cerebral hyperperfusion, and it may be
related to poor postoperative blood pressure control.
Thrombolysis of acute thromboembolic stroke
In acute occlusive stroke, it is possible to recanalize the occluded vessel by
superselective intra-arterial thrombolytic therapy. Thrombolytic agents can be
delivered in high concentration by a microcatheter navigated close to the clot.
Neurologic deficits may be reversed without additional risk of secondary
hemorrhage if treatment is completed within 6 hours from the onset of carotid
territory ischemia and 24 hours in vertebrobasilar territory. One of the impedi-
ments in development in this area has been the fear of increasing the risk of
hemorrhagic transformation of the acute infarction patient. Despite an increased
frequency of early symptomatic hemorrhagic complications, treatment with intra-
arterial pro-urokinase within 6 hours of the onset of acute ischemic stroke with
middle cerebral artery (MCA) occlusion significantly improved clinical outcome
at 90 days [24].
Important points and objectives
There is a rapidly expanding list of application of INR procedures in the field
of the treatment of CNS disease. Anesthesiologists should be familiar with
specific procedures and their potential complications. Constant and effective
communication between the anesthesia and radiology teams is critical to safely
carry out INR procedures and to deal with intracranial catastrophe.
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359 357

Acknowledgments
The authors wish to thank Broderick Belenson, Mark Espinosa, Sabrina Larson,
and Gaurab Basu for assistance in preparation of the manuscript; Van V. Halbach,
MD, and Christopher F. Dowd, MD, John Pile-Spellman, MD, Lawrence Litt, MD,
PhD, and Nancy J. Quinnine, RN, for development of clinical protocols discussed
herein; members of the UCSF Center for Stroke and Cerebrovascular Disease,
UCSF Center for Cerebrovascular Research, and the Columbia University AVM
Study Group for continued support.
References
[1] Pile-Spellman J. Endovascular therapeutic neuroradiology. In: Taveras JM, editor. Neuroradiol-
ogy. 3rd edition. Baltimore: Williams & Wilkins; 1996. p. 1045–179.
[2] Strother CM. Interventional neuroradiology. AJNR Am J Neuroradiol 2000;21:19–24.
[3] YoungWL, Pile-Spellman J. Anesthetic considerations for interventional neuroradiology (review).
Anesthesiology 1994;80:427–56.
[4] Young WL, Pile-Spellman J, Hacein-Bey L, et al. Invasive neuroradiologic procedures for
cerebrovascular abnormalities: anesthetic considerations. Anesth Clinics North Am 1997;15
(3):631–53.
[5] Joint Writing Group of the Technology Assessment Committee American Society of Interven-
tional and Therapeutic Neuroradiology; Joint Section on Cerebrovascular Neurosurgery a
Section of the American Association of Neurological Surgeons and Congress of Neurological
Surgeons; Section of Stroke and the Section of Interventional Neurology of the American
Academy of Neurology. Reporting terminology for brain arteriovenous malformation clinical
and radiographic features for use in clinical trials. Stroke 2001;32:1430–42.
[6] Ravussin P, Tempelhoff R, Modica PA, et al. Propofol vs. thiopental-isoflurane for neurosurgical
anesthesia: comparison of hemodynamics, CSF pressure, and recovery. J Neurosurg Anesth
1991;3:85–95.
[7] Tcheng JE. Platelet integrin glycoprotein IIb/IIIa inhibitors: opportunities and challenges.
J Invasive Cardiol 1996;8:8B–14B.
[8] Rauch RA, Vinuela F, Dion J, et al. Preembolization functional evaluation in brain arteriovenous
malformations: the ability of superselective amytal test to predict neurologic dysfunction before
embolization. AJNR Am J Neuroradiol 1992;13:309–14.
[9] Hashimoto T, Young WL, Aagaard BD, et al. Adenosine-induced ventricular asystole to induce
transient profound systemic hypotension in patients undergoing endovascular therapy. Dose-
response characteristics. Anesthesiology 2000;93:998–1001.
[10] Pile-Spellman J, Young WL, Joshi S, et al. Adenosine-induced cardiac pause for endovascular
embolization of cerebral arteriovenous malformations: technical case report. Neurosurgery
1999;44:881–6; discussion 886–7.
[11] Vinuela F, Dion JE, Duckwiler G, et al. Combined endovascular embolization and surgery in the
management of cerebral arteriovenous malformations: experience with 101 cases. J Neurosurg
1991;75:856–64.
[12] Debrun GM, Vinuela F, Fox AJ, et al. Indications for treatment and classification of 132 carotid-
cavernous fistulas. Neurosurgery 1988;22:285–9.
[13] Setton A, Berenstein A. Interventional neuroradiology. Curr Opin Neurol Neurosurg 1992;
5:870–80.
[14] Marshall RS, Lazar RM, Mohr JP, et al. Higher cerebral function and hemispheral blood flow
during awake carotid artery balloon test occlusions. J Neurol Neurosurg Psychiatry 1999;66:
734–8.
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359358

[15] Marshall RS, Lazar RM, Pile-Spellman J, et al. Recovery of brain function during induced
cerebral hypoperfusion. Brain 2001;124:1208–17.
[16] Higashida RT, Halbach VV, Dowd CF, et al. Intracranial aneurysms: interventional neurovascular
treatment with detachable balloons—results in 215 cases. Radiology 1991;178:663–70.
[17] Newell DW, Eskridge JM, Mayberg MR, et al. Angioplasty for the treatment of symptomatic
vasospasm following subarachnoid hemorrhage. J Neurosurg 1989;71:654–60.
[18] Fogarty-Mack P, Pile-Spellman J, Hacein-Bey L, et al. Superselective intraarterial papaverine
administration: effect on regional cerebral blood flow in patients with arteriovenous malforma-
tions. J Neurosurg 1996;85:395–402.
[19] Roberts JT, Pile-Spellman J, Joseph M, et al. A patient with massive oral-facial venous malfor-
mation. J Clin Anesth 1991;3:76–9.
[20] Higashida RT, Tsai FY, Halbach VV, et al. Transluminal angioplasty for atherosclerotic disease of
the vertebral and basilar arteries. J Neurosurg 1993;78:192–8.
[21] Tsai FY, Matovich V, Hieshima G, et al. Percutaneous transluminal angioplasty of the carotid
artery. AJNR Am J Neuroradiol 1986;7:349–58.
[22] Theron J, Courtheoux P, Alachkar F, et al. New triple coaxial catheter system for carotid
angioplasty with cerebral protection [followed with Commentary by Ferguson R: Getting it right
the first time, p. 875–7]. AJNR Am J Neuroradiol 1990;11:869–74.
[23] Meyers PM, Higashida RT, Phatouros CC, et al. Cerebral hyperperfusion syndrome after percu-
taneous transluminal stenting of the craniocervical arteries [In Process Citation]. Neurosurgery
2000;47:335–43; discussion 343–5.
[24] Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke.
The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboem-
bolism. JAMA 1999;282:2003–11.
T. Hashimoto et al. / Anesthesiology Clin N Am 20 (2002) 347–359 359

Anesthesia for minimally
invasive neurosurgery
Joel O. Johnson, MD, PhDDepartment of Anesthesiology and Perioperative Medicine, University of Missouri–Columbia,
N314 UMHC, DC005.00, One Hospital Drive, Columbia, MO 65212, USA
There is ever-increasing literature on ‘‘minimally invasive’’ surgical tech-
niques. Changes in anesthetic practice must be made to accommodate surgical
requirements, which are dependent upon the specific procedure. Publications
outlining the surgical technique and outcomes of these procedures have included
the specialties of cardiothoracic surgery, otolaryngology, and general surgery, but
reports span the spectrum of other surgical specialties. Anesthesia for minimally
invasive procedures has been covered in some of these specialty areas [1–6].
Anesthesia for neuroendoscopy has recently been covered in an article by
Ambesh and Kumar [7].
Improvements in imaging, computing, and surgical instrumentation have
advanced the field of minimally invasive surgery. Direct imaging systems using
fiberoptic technology have allowed access to areas of the body formerly
accessible only through large openings in the skin. In addition, radiological
breakthroughs such as magnetic resonance imaging (MRI) and CT, combined
with the speed of modern computing, have resulted in the development of
three-dimensional assisted surgery. Brain tumor removal [8], functional endo-
scopic sinus surgery [9], and spinal instrumentation surgery [10] are now
improved by decreasing the amount of viable brain tissue removed, decreasing
surgical times, and better placement of pedicle screws resulting in improve-
ments in patient outcome. The development of open MRI systems has allowed
this imaging modality to move into the operating room, improving surgical
excision of intracranial tumors [11]. Finally, those same imaging systems can be
used to focus noninvasive gamma radiation on remote tumors, allow accurate
placement of biopsy needles or electrocoagulation probes, and possibly avoid
surgical trespass altogether (see boxed text). More recently, in utero fetal
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00006 -2
E-mail address: [email protected] (J.O. Johnson).
Anesthesiology Clin N Am
20 (2002) 361–375

surgery has progressed to the coverage of myelomeningocoele defects, possibly
leading to improved neurologic outcomes in patients with spinal dysraphism
[12]. The ability to repair cardiac congenital defects in utero and correction of
twin-to-twin transfusion syndrome is also making great strides [13,14].
These developments have impacted neurosurgery and anesthetic care of the
neurosurgical patient. Specific anesthetic considerations for neurosurgery remain
essentially unchanged; preservation of the integrity of brain tissue, intracranial
pressure control, modulation of the systemic hemodynamics to achieve optimal
surgical conditions, and a rapid return to the preanesthetic state, the details of
which are covered elsewhere in this text. However, numerous procedures once
done with an open technique or through a craniotomy are now accessible using a
minimally invasive approach with endoscopic or radiologic methods (Table 1).
Modification in anesthetic techniques must take place in some of these proce-
dures to account for special risks and considerations. This review will focus
Technological advances
CT, MRI guided stereotaxyOpen MRIInterventional radiology techniques [9]Frameless stereotaxyLaser surgery [40]Operating microscopicOptical fiberscopeRadio frequency ablationRobotics
Table 1
Minimally invasive neurosurgery
Endoscopic techniques Indications
Hydrocephalus, choroid plexus cauterization, third
ventriculostomy tumor biopsy myeloscopy,
fenestration of colloid, arachnoid cysts and the
septum pellucidum
Transphenoidal approach to supracellar masses
Acoustic neuroma
Thoracoscopic discectomy
Lumbar laminectomy [19]
Hematoma/abscess removal
Radiosurgery Arteriovenous malformation (AVM) ablation, Parkinson’s Disease
Stereotactic MRI and CT guidance
Frameless stereotaxy
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375362

specifically on anesthetic concerns for neuroendoscopy, stereotactic procedures,
synostosis repair, and radiosurgery.
Neuroendoscopy
The first endoscopic neurosurgical procedure was performed by Lespinasse, a
urologist, in 1910. He used a cystoscope to fulgurate the choroid plexus in two
children, one of whom died at the time of operation, and the other survived
5 years [15]. A rigid cystoscope (called by Walter Dandy a ‘‘ventriculoscope’’)
was used for treatment of hydrocephalus via choroid plexus fulguration or third
ventriculostomy [16], but fell out of favor with the development of cerebral spinal
fluid (CSF) diversion catheters. In the 1970s, advances in fiberoptics led to the
construction of steerable neuroendoscopes, allowing the neurosurgeon to perform
complex surgery within the confines of the ventricular space in adults, children,
infants, and neonates [17].
The neurosurgeon utilizes neuroendoscopy for treatment of hydrocephalus,
stereotactic biopsy, treatment of intracranial cysts, evacuation of hematomas or
abscesses, and treatment of syringomyelia. Endoscopy has been used for spine
surgery, and of course, for transphenoidal approaches to the pituitary [18,19]. An
innovative approach to craniosynostosis combines techniques used in plastic
surgery (endoscopic brow lift surgery) with neuroendoscopy to perform minimally
invasive strip craniectomies. Unique anesthetic considerations exist depending
upon positioning and surgical needs. Surgical complications have been reported,
but overall morbidity is less than 2% with a mortality of 0% to 1% [8,20–22].
Hydrocephalus
Neuroanesthesiologists caring for the pediatric neurosurgical population can
attest to the fact that shunts and shunt malfunctions constitute a large proportion
of pediatric cases. Those patients with hydrocephalus due to aqueductal stenosis
can have their CSF flow internally corrected through the creation of an opening in
the floor of the third ventricle. This procedure was first performed endoscopically
in 1923 by Jason Mixter with good results. The ensuing 70 years saw limited use
of stereotactic coordinates to percutaneously create a third ventriculostomy,
which was usually associated with a high complication rate [23]. Improvements
over those decades in the flow characteristics and valve designs of extracranial
peritoneal shunt systems led to their preferred use. However, the advent of
improved endoscopes has created a resurgence of interest in third ventriculos-
tomy for select patients [24].
Patients with acqueductal stenosis are the ideal candidates for endoscopic third
ventriculostomy, with late onset (older patients) obstruction having a more
successful long-term outcome. Other patient populations such as those with
neoplastic obstruction of the acqueduct of Sylvius, patients with meningomye-
locoele, and those with deep cisternal arachnoid cysts have undergone successful
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375 363

internal shunting. Relative contraindications include patients with abnormal
ventricular anatomy, those with an intraventricular hemorrhage or a history of
meningitis. Several authors use a cutoff of a minimum third ventricular size of
7 mm. Damage (hypothalamic) to the walls of the third ventricle may occur in
patients with a smaller ventricle. Preoperative surgical evaluation usually
includes imaging studies to define the anatomy and size of the ventricular
system. There are currently no reliable functional tests of the patency of the
acqueduct of Sylvius or the absorptive capability of the arachnoid villi that can be
performed intraoperatively.
Patient position for endoscopic entry into the third ventricle is routine supine.
The table is usually positioned at a 90-degree angle to the anesthesiologist, with
the operative side ‘‘out.’’ At our institution, cranial fixation is not utilized in most
cases. A coronal burr hole is placed that optimizes the angle of approach to the
floor of the third ventricle. The frontal horn is accessed and the endoscope is
advanced to the third ventricle, where the mamillary bodies can be visualized.
The tuber cinereum is located just beyond these structures. Beneath this mem-
brane is the basilar artery and cisterns. Fenestration of this membrane creates an
opening through which CSF is diverted, a bypass of the aqueduct of Sylvius.
Several methods have been described for creating this hole, including using a
rigid endoscope itself, a smaller blunt probe, or lasers. The opening is then dilated
with a Fogarty catheter to ensure patency and stop any venous bleeding that may
occur. The most important factor in maintaining patency is the continued CSF
flow through the newly created opening.
Surgical complications have been described, including acute increases in
intracranial pressure, injury to brain structures and bleeding complications, most
notably damage to the basilar artery [25]. Warmed (37�C) lactated Ringers
solution is the perfusate commonly used to clear the CSF and irrigate the
operating area. Normal saline irrigant has been reported to cause inflammatory
neurologic complications including high fever and headache [26]. Increases in
intracranial pressure will occur if egress of the irrigating fluid is not maintained.
In addition, rapid flow of the irrigation fluid has been reported to acutely distend
the third ventricle or activate specific hypothalmic nuclei resulting in acute
hemodynamic collapse [27].
Injury to brain structures may result in short-term memory loss (injury to
the fornix) [18], syndrome of inappropriate secretion of antidiuretic hormone
(SIADH)(hypothalamus) [28], and rare nerve palsies. A host of anecdotal compli-
cations without specific etiologies have particular interest to the anesthesiologist,
including transient confusion [18], headaches [24], and unresponsiveness. [29].
Hemorrhagic complications may have significance both intraoperatively and
in the postoperative period. Intraoperative hemorrhage is rare, and is usually
controlled with saline irrigation. Bleeding that obliterates the endoscopic image is
treated by aborting the procedure, external drainage, and angiography if neces-
sary. Case reports of bleeding or pseudoaneurysm formation after injury to the
basilar artery have been generated [25]. Intraventricular clots from any sources
may subsequently be removed endoscopically.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375364

Anesthetic considerations
Patients presenting for endoscopic treatment of hydrocephalus may range in
age from newborn to geriatric. Many of these cases are completed in an urgent
or semiurgent fashion, often with the pre-existing presence of a ventriculos-
tomy. A routine complete preoperative work-up addresses the patients systemic
illnesses and need for further preoperative consultation or treatment. Fasting
guidelines should be followed if possible. Patients with hydrocephalus may
have hypovolemia due to vomiting, fluid restriction, contrast agents, or os-
motic diuretics. Adequate volume replacement is a necessary consideration
prior to induction.
The newborn or infant less than 6 months of age represents a challenge in
several ways. Lack of suture fusion leads to increasing head circumference and
fewer classic clinical signs of intracranial hypertension. Although cerebral blood
flow (CBF) in the adult may is 50 mL/100 g/min, newborn flow is 23–40 mL/
100 g/min, and is even less in the premature infant [30]. The range of
autoregulation is shifted to the right in the infant; thus, normal CBF is maintained
at lower arterial pressures in the young. The metabolic rate of oxygen consump-
tion is 5.2 mL O2/100 g/min in 3–11-year-old children, indicating that although
there appears to be room to spare on the lower end of the arterial pressure scale
and CBF, the oxygenation requirements mandate careful attention to the avoid-
ance of hypoxia.
Preoperative medication is often not required in the adult patient, and is not
desirable in the newborn or infant less than 6 months of age. There is a risk of
hypoventilation leading to hypercarbia and arterial desaturation when premed-
ication with narcotics or barbiturates is instituted in infants or children [31,32].
However, the use of oral midazolam (0.5 mg/kg) does not caused changes in
oxygen saturation in preschool-aged children [33]. It is our practice to plan an
inhalation induction 10 to 15 minutes after oral midazolam premedication
(0.5 mg/kg) in children scheduled for neuroendoscopy. This approach avoids
excessive agitation during parental separation, preserves spontaneous breathing,
and facilitates inhalation induction without delaying awakening. Pediatric
patients with diminished consciousness or that have major medical problems
should undergo an intravenous (i.v.) induction. This category of patients often
have been admitted to the hospital and have indwelling intravenous access.
Monitoring for neuroendoscopy depends on the procedure, accompanying
medical problems, and the age of the patient. Routine American Society of
Anesthesiologists (ASA) monitors are placed upon arrival to the operating room.
Measurement of end-tidal carbon dioxide and end-tidal gas concentration is
necessary. An arterial catheter is inserted in the adult patient prior to induction.
Children, infants, and newborns benefit from direct arterial pressure measure-
ment, partially because of the opportunity to easily obtain blood samples. The
proportionate increase in dead space, high flow rates, and small tidal volumes
may underestimate PaCO2 and result in hypoventilation. Intermittent arterial
sampling allows for adjustment of the ventilation parameters, as well as
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375 365

measurement of the hematocrit, serum electrolytes, and osmolality. Arterial
access is usually obtained in this subgroup after induction of anesthesia and
securing of the airway.
Intraoperative complications during endoscopic treatment of third ventricu-
lostomy include cardiac arrest [27], hypertension [27], bradycardia [9,21,27,34],
and anecdotal reports of massive intraoperative hemorrhage [23]. In preparation
for these emergencies, resuscitation drugs including atropine and epinephrine
must be available, and used judiciously to avoid large increases in blood pressure,
which would accentuate hemorrhage. Immediate postoperative complications
such as SIADH [35], nerve palsies [34], and hemiparesis [34] may have to be
dealt with in the recovery room.
Neuroendoscopy has also been used in ascertaining the correct placement of
traditional ventricular shunt systems [36]. This technique offers visual confirma-
tion of the position of the tip of the implanted catheter.
Stereotactic-guided endoscopic biopsy
Image-guided biopsy within the ventricular system has been made possible
by combining improvements in three-dimensional graphics with endoscopy
[37]. Further improvements include the Toronto open MR unit that can be used
in the OR for real-time operative guidance [38]. Stereotactic-guided endoscopic
biopsy is useful for a less-invasive biopsy of intraventricular and subarachnoid
tumors, including pineal tumors [39]. When the surgeon biopsies a lesion in the
ventricular system, immediate hemostasis of the site is possible with visual
confirmation of the differences between normal and pathologic tissue [8]. This
offers improved reliability in obtaining an appropriate histologic specimen.
Advances in the field of pathology offer ‘‘smear’’ techniques that utilize smaller
biopsy specimens, which is especially important for tumors in or near func-
tionally important areas [40]. The risk profile is otherwise the same as that seen
with endoscopy.
Anesthetic considerations are similar to those described above, with a
special emphasis on the risk for intraventricular hemorrhage. The intraoperative
use of pressor agents and excessive coughing or bucking on emergence can
hypothetically cause a biopsy site to rebleed. In comparison to stereotactic
biopsy done with conventional head-frame devices (see below), patients are
under a general anesthetic.
Intracranial cysts, hematomas, and abscesses
This heterogeneous group of space-occupying lesions has been successfully
treated with neuroendoscopic techniques [8,20,27,28,41]. Although the operative
mortality is lower than with conventional therapy, there is distinct differences
depending on pathology. Fenestration of intracerebral cystic lesions appears to be
the most benign, with an operative morbidity of 1.4% [8]. Laser fenestration or
sectioning of the cyst wall is accomplished with a yttrium-aluminum-garnet
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375366

(YAG) or potassium-tytanil-phosphate (KTP) source [20,42]. Intracerebral and
intraventricular hematomas may be evacuated through the endoscope if the
operation is completed within 2 hours of the onset of bleeding and the volume
is less than 50 cc. The reported morbidity (10.4%) and mortality (10.7%) remain
lower than conventional surgical techniques, although the value of the surgery
compared to conservative (nonsurgical treatment) remains in doubt [8]. Finally,
although most brain abscesses are approached through stereotactic techniques,
endoscopic methods allow for microbiologic samples, visual confirmation of the
content, and visual evaluation of the success of draining the lesion.
Anesthetic considerations focus primarily on positioning concerns. Positioning
for this subgroup of patients depends on the location of the lesion. Entry to the
ventricular system [43] may be accomplished through frontal, lateral, and posterior
approaches. This necessitates careful planning and communication between the
surgeon and the anesthesia providers. The use of the laser for endoscopic sec-
tioning often reduces visibility in the operating room due to protective eyewear.
Syringomyelia
Spinal endoscopy was described as early as 1931, and has been explored as a
treatment for septated syringomelia [41]. Miniature endoscopes (1.2 mm)
with single irrigating channels are used to visualize the inside of the syringo-
melic cavity and bluntly fenestrate septations. Anesthetic concerns include
prone positioning, assurance of lack of movement, and rapid awakening to assess
neurologic function.
Endoscopic strip craniectomy
Strip craniectomy is the removal of a strip of bone containing a fused cranial
suture, for the treatment of cranial synostosis. This technique has a long history in
neurosurgery, beginning with the first reports in the late 1800s and progressing to
the present day. The extent of the procedure spans the range from a simple open-
strip craniectomy or wide-strip craniectomy [44] to total cranial vault remodeling
[45]. The combination of endoscopic techniques such as those used in plastic
surgical forehead lifts with strip craniectomy has led to an innovative approach to
these often bloody surgical procedures [46,47].
Positioning plays a major role in the surgical requirements for craniosynos-
tosis procedures [48,49]. A prone position with neck extension is used to
facilitate surgical exposure (sometimes referred to as a ‘‘sea lion’’ or ‘‘sphinx’’
position) [50]. An inflatable bean bag holds the patients head in a fixed position
(Fig. 1) [49].
Anesthetic concerns include airway control, patient positioning, and the
potential for intraoperative blood loss. The patient population specific for this
surgical procedure is limited to those under 6 months of age. Thus, an inhalation
induction, i.v. placement, and intubation after a dose of nondepolarizing neuro-
muscular blocking agent is accomplished while maintaining a warm environment.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375 367

Head position for intubation can be challenging in a patient with severe
scaphocephaly, necessitating a second pair of hands for stabilization.
Optimal placement and securing of the endotracheal (ET) tube is of the
utmost importance, as inadvertent extubation is a risk during prone positioning
and extension of the neck. Extension leads to an average 1.7-cm cephalad
movement of the tip of the ET tube [51], with a cords to carina distance of 4 to
6 cm. To ensure that the tip of the ET tube remains in the trachea, a maximum
depth without mainstem intubation or contact with the carina is achieved. With
the head in a neutral position, the ET tube is advanced until the right mainstem
bronchus is intubated, then withdrawn until bilateral breath sounds are
appreciated. After careful securing of the ET tube, the patient is positioned
prone with the arms at the side, and the head extended as described above. The
endotracheal tube is carefully positioned to ensure that ‘‘kinking’’ does not
occur with the beanbag assembly (Fig. 2). Breath sounds are checked and a
warming blanket applied.
The prone, head-extended position places the incision sites from 8 to 14 cm
above the level of the right heart, creating a gradient that allows for possible
venous air embolism (VAE). A precordial Doppler probe should be placed to
detect such an occurrence. Open craniectomy procedures for synostosis repair
have a reported incidence of VAE greater than 80%, with 30% of these
incidents being associated with hypotension [52]. Endoscopic techniques have
a decreased incidence of VAE (8%) as well as a lack of hemodynamic effect
(0%) (personal data).
Fig. 1. A child placed in the ‘‘sea-lion’’ or ‘‘sphinx’’ position prior to endoscopic strip craniectomy.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375368

Blood loss during craniosynostosis repair can be significant. One recent report
indicated that 96.3% of patients undergoing open calvarial surgery required
transfusion of packed red blood cells [53]. However, minimally invasive
techniques have been reported to cut the blood to an average of 35 mL in
patients undergoing endoscopic strip craniectomy for sagittal synostosis [54].
Involved craniofacial procedures are being done with minimally invasive
endoscopic techniques. Monoblock osteotomies using these procedures have
been reported to result in a decrease in surgical bleeding and surgical time [55].
Anesthetic considerations remain the same as discussed above.
Stereotactic procedures
Neurosurgeons began using stereotactic surgery for psychiatric and movement
disorders in the late 1940s. Published atlases of human stereotactic coordinates
allowed for the placement of specific brain lesions to treat psychosis, depression,
Parkinson’s disease, chorea, and a host of psychiatric disorders. The use of CT
combined with MRI led to the development of clinical tools that minimize the
error in accessing deep brain structures and also assist in the choice of an
approach path. Until recently, stereotactic devices were routinely used to hold the
surgical instrumentation, and as directional and depth gauges to arrive at the
appropriate site. These ‘‘head frames’’ represented an obstacle to the airway for
the anesthesiologist.
Fig. 2. The endotracheal tube is carefully secured to prevent kinking of the tube or displacement
during the surgical procedure.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375 369

Such an obstacle is the Brown-Robert-Wells frame, a ring structure affixed to
the skull in the horizontal plane by four pins. The patient then is imaged with the
ring in place, to provide an external relationship to the internal structures of the
brain. An interlocking arc is placed on the ring, with the coordinates provided by
computer. An innovation to the ring structure involved a hinged portion, which
could be swung out of the way to provide for airway access. Occasionally,
however, the required position of the ring placed the hinged part at the back of the
head, making access to the airway difficult.
These devices have since given way to ‘‘frameless stereotaxy.’’ External
markers are placed on the patients head prior to imaging. These scalp markers are
left on and used as fiducial points to relate the surgical instrumentation (such as a
bipolar coagulation device) to the computer generated three-dimensional image
(Fig. 3). A pair of cameras mounted above the operating field supply a stereo-
scopic view of the surgical instrument to the computer, which then locates the tip
of the instrument within its three-dimensional image. In this way, the surgeon is
presented with a horizontal, sagittal, and coronal view of the position of the tip of
the instrument on the operating field. These innovations have eliminated the
problem of access to the airway encountered with many stereotactic head-frame
systems. In addition, these imaging techniques have been modified to provide for
stereotactic guidance during spine surgery [56].
Guidance devices continue to be used during stereotactic-guided endoscopy,
biopsy, and lesioning. These are generally attached to the cranial fixation devise
Fig. 3. Fiducial markers are placed prior to ‘‘frameless’’ stereotactic surgery.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375370

(pins), including ‘‘frame’’ devices similar to the aforementioned stereotactic
headframes. In particular, Parkinson’s disease in patients who have developed
resistance to levodopa treatment may present for stereotactic thalamotomy or
pallidotomy. Deep brain lesions are produced with a probe utilizing radio-
frequency current causing ionic oscillations and temperature increases to 80�Cfor 1 to 2 minutes in the target brain tissue.
Anesthetic considerations
Many stereotactic surgical procedures are done on an awake patient. Routine
ASA monitors are placed, and arterial pressure measurement is generally not
required. Because patients are commonly in a sitting or semirecumbent position,
the use of a precordial Doppler is prudent. Venous air embolism has been
reported associated with burr hole placement [57].
Placement of the burr hole can be accomplished with local anesthesia
infiltration by the surgeon. The use of sedatives or analgesics is highly depend-
ent upon the procedure being performed. The presence of a space-occupying
lesion and increased intracranial pressure precludes the use of medications,
which may increase pCO2. Sedatives such as midazolam are acceptable in many
situations, while narcotic medications are generally not required. Lesioning,
particularly for Parkinson’s disease, requires active participation by the patient to
assess the amount of rigidity and cogwheeling present on the contralateral side;
therefore, no medications are used. However, that does not negate the need for
an anesthesiologist.
Intraoperative complications include the possibility of venous air embolus,
seizure [58], bleeding [59], and failed biopsy [60]. The author’s experience has
included one patient who had an intraoperative seizure, requiring removal of the
stereotactic headframe, and a patient exhibiting severe bradycardia during pallid-
otomy. These examples underline the fact that although the anesthetic may be
minimal or nonexistent, the presence of an anesthesiologist for immediate
medical care of the surgically compromised patient is a necessity.
The pediatric patient having stereotactic procedures usually requires a light
general anesthetic. Although awake craniotomy has been reported in a 12 year
old [61], most children do not understand medical rationale. The use of
‘‘frameless stereotaxy’’ may decrease the number of pediatric patients that have
to be anesthetized for both their imaging and surgical portions of their stereo-
tactic surgery.
Thoracoscopic sympathectomy
Neurosurgeons are doing thoracic sympathectomies for hyperhidrosis and
pain syndromes [62,63]. A thoracoscopic approach offers good surgical results
while decreasing postoperative pain and complications. Neuroanesthesiologists
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375 371

experienced in the placement of double-lumen endotracheal tubes or bronchial
blockers and single-lung ventilation physiology will experience little problem
with this procedure. Postoperative pain control may be accomplished with local
anesthesia at the portal sites. This surgical procedure has moved into the same-
day surgery arena when the patient does not require chest tubes [64].
Keyhole foraminotomy
The use of small incisions and a posterior approach has led to good surgical
results in the treatment of radicular pain. Decompression of an involved nerve
using microsurgical approaches has been found to avoid the use of an anterior
approach to the cervical spine with or without fusion [65]. Anesthetic consid-
erations revolve around positioning the prone patient. Careful positioning and
padding are a priority. Respiratory function actually improves in the prone
position compared to the supine anesthetized position, which is associated with
a decrement in functional residual capacity. Care must be taken to avoid kinking
or compression of the endotracheal tube.
A more recently revealed consideration for neuroanesthesiologists is the rare
occurrence of blindness following surgery and anesthesia in the prone position
[66,67]. This complication may be due to anterior ischemic optic neuropathy, and
has been associated with prolonged prone positioning. Other possible factors
include hypotension, changes in central venous pressure [66] or orbital pressure,
anemia, or a combination of any of the above. There is at present no reliable
method for detecting persons at risk for this complication [68].
Radiosurgery
Since 1951, stereotactic radiosurgery has treated patients with particle radi-
ation, photon radiation, and multisource cobalt-60 gamma units [39]. The
‘‘gamma knife’’ has been used to treat acoustic neuromas [69], AVM [70],
trigeminal neuralgia [71], and pituitary tumors. The advantage of this type of
radiation surgery is that radiation is delivered via multiple narrow beams,
coalescing at the target site. Thus, a much larger amount of brain tissue is
exposed through multiple-beam pathways, limiting the damage to normal tissue.
Focusing the beams to a single small area where the cumulative energy is
destructive necessitates an anesthetic technique that prevents movement of the
patient. The pediatric population is benefited by airway control and at times a
light general anesthetic. However, the advantage of this noninvasive technique
lies in the avoidance of general anesthesia. Most adult patients require only mild
sedation, while heavy sedation may result in involuntary movement. General
anesthesia is indicated for adults who have movement disorders or who cannot
tolerate the long duration (4 hours) of these procedures.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375372

Summary
Neurosurgerical techniques utilizing minimally invasive approaches will
continue to emerge. For some of these future possibilities, anesthesia may not
be required. Other types of neurosurgery, whether performed by humans or a
machine, will require entry through the cranium and an absolute lack of move-
ment. Anesthesia will keep pace with these innovations by accurately controlling
the delivery of anesthetic to achieve optimal conditions. This control will allow
for a safer, more comfortable surgical procedure while decreasing blood loss and
morbidity associated with neurosurgery.
References
[1] Ahonen J, Olkkola KT, Verkkala K, et al. A comparison of remifentanil and alfentanil for use
with propofol in patients undergoing minimally invasive coronary artery bypass surgery. Anesth
Analg 2000;90:1269–74.
[2] Badner NH. Anesthesia for minimally invasive surgery. Can J Anaesth 1999;46:R101–10.
[3] Cunningham AJ. Anesthetic implications of laparoscopic surgery. Yale J Biol Med 1999;71:
551–78.
[4] Krucylak PE. Intraoperative considerations during minimal-access cardiac surgery. Semin Thor-
ac Cardiovasc Surg 1999;11:116–24.
[5] Petrat G, Weyandt D, Klein U. Anesthetic considerations in pediatric laparoscopic and thoraco-
scopic surgery. Eur J Pediatr Surg 1999;9:282–5.
[6] Wasnick JD, Acuff T. Anesthesia and minimally invasive thoracoscopically assisted coronary
artery bypass: a brief clinical report. J Cardiothorac Vasc Anesth 1997;11:552–5.
[7] Ambesh SP, Kumar R. Neuroendoscopic procedures: anesthetic considerations for a growing
trend: a review. J Neurosurg Anesthesiol 2000;12:262–70.
[8] Bauer BL, Hellwig D. Minimally invasive endoscopic neurosurgery—a survey. Acta Neurochir
Suppl (Wien) 1994;61:1–12.
[9] Slack R, Bates G. Functional endoscopic sinus surgery. Am Fam Physician 1998;58:707–18.
[10] Kamimura M, Ebara S, Itoh H, et al. Accurate pedicle screw insertion under the control of a
computer-assisted image guiding system: laboratory test and clinical study. J Orthop Sci
1999;4:197–206.
[11] Kettenbach J, Wong T, Kacher D, et al. Computer-based imaging and interventional MRI:
applications for neurosurgery. Comput Med Imaging Graph 1999;23:245–58.
[12] Bruner JP, Richards WO, Tulipan NB, et al. Endoscopic coverage of fetal myelomeningocele in
utero. Am J Obstet Gynecol 1999;180:153–8.
[13] Albanese CT, Harrison MR. Surgical treatment for fetal disease. The state of the art. Ann NY
Acad Sci 1998;847:74–85.
[14] Milner R, Crombleholme TM. Troubles with twins: fetoscopic therapy. Semin Perinatol
1999;23:474–83.
[15] Guazzo EP. Recent advances in paediatric neurosurgery. Arch Dis Child 1993;69:335–7.
[16] Harris LW. Endoscopic techniques in neurosurgery. Microsurgery 1994;15:541–6.
[17] Alvarez JA, Cohen AR. Neonatal applications of neuroendoscopy. Neurosurg Clin N Am
1998;9:405–13.
[18] Gaab MR, Schroeder HW. Neuroendoscopic approach to intraventricular lesions [see com-
ments]. J Neurosurg 1998;88:496–505.
[19] O’Dowd JK. Laparoscopic lumbar spine surgery. Eur Spine J 2000;9(Suppl 1):S3–7.
[20] Auer LM, Holzer P, Ascher PW, et al. Endoscopic neurosurgery. Acta Neurochir 1988;90:1–14.
[21] Jones RF, Kwok BC, Stening WA, et al. Neuroendoscopic third ventriculostomy. A practical
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375 373

alternative to extracranial shunts in non-communicating hydrocephalus. Acta Neurochir Suppl
(Wien) 1994;61:79–83.
[22] Rosenfeld JV. Minimally invasive neurosurgery. Aust N Z J Surg 1996;66:553–9.
[23] Jimenez DF. Third ventriculostomy. In: Jimenez DF, editor. Intracranial endoscopic neurosur-
gery. Park Ridge: American Association of Neurological Surgeons; 1998. p. 108.
[24] Schwartz TH, Yoon SS, Cutruzzola FW, et al. Third ventriculostomy: post-operative ventricular
size and outcome. Minim Invasive Neurosurg 1996;39:122–9.
[25] McLaughlin MR, Wahlig JB, Kaufmann AM, et al. Traumatic basilar aneurysm after endoscopic
third ventriculostomy: case report. Neurosurgery 1997;41:1400–3.
[26] Oka K, Yamamoto M, Nonaka T, et al. The significance of artificial cerebrospinal fluid as
perfusate and endoneurosurgery. Neurosurgery 1996;38:733–6.
[27] Handler MH, Abbott R, Lee M. A near-fatal complication of endoscopic third ventriculostomy:
case report. Neurosurgery 1994;35:525–7.
[28] Teo C, Rahman S, Boop FA, et al. Complications of endoscopic neurosurgery. Childs Nerv Syst
1996;12:248–53.
[29] Caemaert J, Abdullah J. Diagnostic and therapeutic stereotactic cerebral endoscopy. Acta Neuro-
chir. 1993;124:11–3.
[30] Newton RW. Intracranial pressure and its monitoring in childhood: a review. J R Soc Med
1987;80:566–70.
[31] Larsson LE, Nilsson K, Andreasson S, et al. Effects of rectal thiopentone and methohexitone on
carbon dioxide tension in infant anaesthesia with spontaneous ventilation. Acta Anaesthesiol
Scand 1987;31:227–30.
[32] Stanley TH, Leiman BC, Rawal N, et al. The effects of oral transmucosal fentanyl citrate
premedication on preoperative behavioral responses and gastric volume and acidity in children.
Anesth Analg 1989;69:328–35.
[33] Feld LH, Negus JB, White PF. Oral midazolam preanesthetic medication in pediatric outpatients.
Anesthesiology 1990;73:831–4.
[34] Jones RF, Stening WA, Brydon M. Endoscopic third ventriculostomy. Neurosurgery 1990;
26:86–91.
[35] Kunz U, Goldmann A, Bader C, et al. Endoscopic fenestration of the 3rd ventricular floor in
aqueductal stenosis. Minim Invasive Neurosurg 1994;37:42–7.
[36] Kellnar S, Boehm R, Ring E. Ventriculoscopy-aided implantation of ventricular shunts in pa-
tients with hydrocephalus. J Pediatr Surg 1995;30:1450–1.
[37] Seibel RM. Image-guided minimally invasive therapy. Surg Endosc 1997;11:154–62.
[38] Bernstein M, Al Anazi AR, Kucharczyk W, et al. Brain tumor surgery with the Toronto open
magnetic resonance imaging system: preliminary results for 36 patients and analysis of advan-
tages, disadvantages, and future prospects. Neurosurgery 2000;46:900–7.
[39] Camins MB. What’s new in neurological surgery. J Am Coll Surg 1996;182:115–21.
[40] Slowinski J, Harabin-Slowinska M, Mrowka R. Smear technique in the intra-operative brain
tumor diagnosis: its advantages and limitations. Neurol Res 1999;21:121–4.
[41] Hellwig D, Kuhn TJ, Bauer BL, et al. Endoscopic treatment of septated chronic subdural
hematoma. Surg Neurol 1996;45:272–7.
[42] Buki A, Doczi T, Veto F, et al. Initial clinical experience with a combined pulsed holmium-
neodymium-YAG laser in minimally invasive neurosurgery. Minim Invasive Neurosurg 1999;
42:35–40.
[43] Jimenez DF. Access to the ventricular system. In: Jimenez DF, editor. Intracranial endoscopic
neurosurgery. Park Ridge: The American Association of Neurological Surgeons; 1998. p. 29–37.
[44] Albright AL. Operative normalization of skull shape in sagittal synostosis. Neurosurgery 1985;
17:329–31.
[45] Olds MV, Storrs B, Walker ML. Surgical treatment of sagittal synostosis. Neurosurgery 1986;
18:345–7.
[46] Daniel RK, Tirkanits B. Endoscopic forehead lift. Aesthetics and analysis. Clin Plast Surg 1995;
22:605–18.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375374

[47] Jimenez DF, Barone CM. Endoscopic craniectomy for early surgical correction of sagittal cra-
niosynostosis. J Neurosurg 1998;88:77–81.
[48] Francel PC, Bell A, Jane JA. Operative positioning for patients undergoing repair of craniosyn-
ostosis. Neurosurgery 1994;35:304–6.
[49] Park TS, Broaddus WC, Harris M, et al. Vacuum-stiffened beanbag for cranial remodeling
procedures in modified prone position. Technical note. J Neurosurg 1989;71:623–5.
[50] Iwabuchi T, Ishii M, Julow J. Biparieto-occipital craniotomy with hyperextended neck—‘‘sea
lion’’ position. Acta Neurochir. 1979;51:113–7.
[51] Sugiyama K, Yokoyama K. Displacement of the endotracheal tube caused by change of head
position in pediatric anesthesia: evaluation by fiberoptic bronchoscopy. Anesth Analg 1996;
82:251–3.
[52] Faberowski LW, Black S, Mickle JP. Incidence of venous air embolism during craniectomy for
craniosynostosis repair. Anesthesiology 2000;92:20–3.
[53] Faberowski LW, Black S, Mickle JP. Blood loss and transfusion practice in the perioperative
management of craniosynostosis repair. J Neurosurg Anesthesiol 1999;11:167–72.
[54] Barone CM, Jimenez DF. Endoscopic craniectomy for early correction of craniosynostosis. Plast
Reconstr Surg 1999;104:1965–73.
[55] Tutino M, Chico F, Tutino M, et al. Endoscopic intracranial craniofacial and monobloc osteot-
omies with the aid of a malleable high-speed pneumatic drill: a cadaveric and clinical study. Ann
Plast Surg 2000;44:1–7.
[56] Welch WC, Subach BR, Pollack IF, et al. Frameless stereotactic guidance for surgery of the
upper cervical spine [see comments]. Neurosurgery 1997;40:958–63.
[57] Edelman JD, Wingard DW. Air embolism arising from burr holes. Anesthesiology 1980;
53:167–8.
[58] Merriam MA, Bronen RA, Spencer DD, et al. MR findings after depth electrode implantation for
medically refractory epilepsy. Am J Neuroradiol 1993;14:1343–6.
[59] Barnett GH, Miller DW, Weisenberger J. Frameless stereotaxy with scalp-applied fiducial
markers for brain biopsy procedures: experience in 218 cases. J Neurosurg 1999;91:569–76.
[60] Soo TM, Bernstein M, Provias J, et al. Failed stereotactic biopsy in a series of 518 cases.
Stereotact Funct Neurosurg 1995;64:183–96.
[61] Tobias JD, Jimenez DF. Anaesthetic management during awake craniotomy in a 12-year-old boy.
Paediatr Anaesth 1997;7:341–4.
[62] Johnson JP, Obasi C, Hahn MS, et al. Endoscopic thoracic sympathectomy. J Neurosurg
1999;91:90–7.
[63] Vanaclocha V, Saiz-Sapena N, Panta F. Uniportal endoscopic superior thoracic sympathectomy.
Neurosurgery 2000;46:924–8.
[64] Reardon PR, Preciado A, Scarborough T, et al. Outpatient endoscopic thoracic sympathectomy
using 2-mm instruments. Surg Endosc 1999;13:1139–42.
[65] Witzmann A, Hejazi N, Krasznai L. Posterior cervical foraminotomy. A follow-up study of 67
surgically treated patients with compressive radiculopathy. Neurosurg Rev 2000;23:213–7.
[66] Dilger JA, Tetzlaff JE, Bell GR, et al. Ischaemic optic neuropathy after spinal fusion. Can J
Anaesth 1998;45:63–6.
[67] Myers MA, Hamilton SR, Bogosian AJ, et al. Visual loss as a complication of spine surgery. A
review of 37 cases. Spine 1997;22:1325–9.
[68] Cheng MA, Sigurdson W, Tempelhoff R, et al. Visual loss after spine surgery: a survey. Neuro-
surgery 2000;46:625–30.
[69] Ogunrinde OK, Lunsford LD, Flickinger JC, et al. Cranial nerve preservation after stereotactic
radiosurgery for small acoustic tumors. Arch Neurol 1995;52:73–9.
[70] Lunsford LD. Stereotactic radiosurgical procedures for arteriovenous malformations of the brain.
Mayo Clin Proc 1995;70:305–7.
[71] Kondziolka D, Perez B, Flickinger JC, et al. Gamma knife radiosurgery for trigeminal neuralgia:
results and expectations. Arch Neurol 1998;55:1524–9.
J.O. Johnson / Anesthesiology Clin N Am 20 (2002) 361–375 375

Intracranial vascular surgery
Audree A. Bendo, MDDepartment of Anesthesiology, SUNY/Downstate Medical Center, 450 Clarkson Avenue,
Box 6, Brooklyn, NY 11203, USA
Intracranial aneurysms
Epidemiology
Subarachnoid hemorrhage (SAH) from rupture of an intracranial aneurysm is a
devastating disease, affecting an estimated 21,000 patients annually in North
America [1,2]. Despite considerable advances in the management of these pa-
tients, outcome remains poor, with overall mortality rates of 25% and significant
morbidity among approximately 50% of survivors [1,2].
In the most recent studies, the overall incidence of SAH is six to eight per
100,000 people [1,2]. The peak incidence for rupture is in the fifth and sixth
decades of life, and is greater for woman than men. Several potential risk factors
for aneurysm rupture have been identified (Table 1) [1,2].
The management of patients with unruptured intracranial aneurysms (UIAs)
remains controversial [2–4]. The International Study of Unruptured Intracranial
Aneurysms found the rupture rate of small aneurysms (< 10 mm diameter) was
0.05% per year in patients with no prior SAH, and 0.5% per year for large (>10 mm
diameter) aneurysms and for all aneurysms in patients with previous SAH [4]. This
study revealed that surgery did not reduce the rate of disability and death in patients
with unruptured aneurysms smaller than 10 mm in diameter and no history of
SAH [4]. Current recommendations for the treatment of UIAs have been published
by the Stroke Council of the American Heart Association [4].
A patient with aneurysmal SAH may be classified according to one of several
grading systems: Botterell’s original classification [5], the modification by Hunt
and Hess (Table 2) [6], or the more recent World Federation of Neurosurgeons
(WFNS) SAH scale (Table 3) [7]. These classifications are used by neuro-
surgeons to estimate surgical risk and outcome. Higher grades, or patients who
are clinically more impaired, are associated with the presence of cerebral
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00007 -4
E-mail address: [email protected] (A.A. Bendo).
Anesthesiology Clin N Am
20 (2002) 377–388

vasospasm, intracranial hypertension, and increased surgical mortality. In general,
the poorer the grade on hospital admission, the worse the prognosis.
The disease: clinical features and complications
The presence of blood in the subarachnoid space causes an abupt, marked rise
in intracranial pressure (ICP), which often results in systemic hypertension and
dysrhythmias. The abrupt increase in ICP accounts for the acute onset of a
sudden, severe headache. The classic presentation of aneurysmal SAH is that of
severe headache associated with stiff neck, photophobia, nausea, vomiting, and
often transient loss of consciousness. With this presentation, the diagnosis of
SAH is obvious. In about 50% of patients, a small bleed or ‘‘warning leak’’
precedes a major aneurysmal rupture [8]. Warning symptoms and signs tend to
be mild and nonspecific (headache, dizziness, orbital pain, slight motor or
sensory disturbance), and are generally ignored or misidagnosed by both patient
and physician.
The diagnosis of SAH is made by the combination of clinical findings and a
noncontrast CT scan of the head. When performed within a day of aneurysm
rupture, CT reveals a high-density (white) blood clot in basal subarachnoid
cisterns in about 95% of patients. This is followed by selected cerebral angiog-
raphy to document the presence and anatomic features of the aneurysm. Aneu-
rysms are classified according to location and size. They arise at a branch or
bifurcation, usually at a point where a major vessel makes a turn, changing the
axial flow of blood.
Table 1
Potential risk factors for aneurysm rupture
. Cigarette smoking
. Hypertension
. Alcohol consumption
. Cocaine and amphetamine abuse
. Oral contraceptive use
. Plasma cholesterol > 6.3 mmol/L
. Genetic conditions, e.g., ADPKD
. Familial (first-degree relatives)
Table 2
Hunt and Hess classification of patients with subarachnoid hemorrhage
Grade Criteria
0 Unruptured aneurysm.
I Asymptomatic, or minimal headache and slight nuchal rigidity.
II Moderate to severe headache, nuchal rigidity, no neurological deficit other than cranial nerve palsy.
III Drowsiness, confusion, or mild focal deficit.
IV Stupor, moderate to severe hemiparesis, early decerebration, vegetative disturbance.
V Deep coma, decerebrate rigidity, moribund.
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388378

Complications
There are several potential complications of SAH and surgical treatment of
aneurysms (Table 4). The most important of these are rebleeding, vasospasm,
intracranial hypertension, and hydrocephalus.
Rebleeding occurs most comonly during the first 24 hours following initial
SAH. The chance of rebleeding is abour 4% within the first day; after 48 hours, it
is 1.5% per day, with a cumulative rebleeding rate of 19% by the end of 2 weeks
[9]. Recurrent aneurysmal hemorrhage is a devastating complication associated
with increased morbidity and mortality.
Because of the incidence of rebleeding with conservative management of
SAH, early aneurysm clipping (days 0–3) is currently recommended for patients
who are alert on admission. The debate over ‘‘early versus late’’ surgery was
largely resolved following the report of The International Cooperative Study on
the Timing of Aneurysm Surgery [10,11]. In this trial, overall management results
demonstrated a similar mortality (20%) and good outcome (60%) for patients
with surgery planned for early (0–3 days) and late (11–14 days) intervals. The
least favorable outcome and highest mortality occurred in patients with planned
surgery for days 7 to 10 after SAH. Patients who were alert on admission did best
with early surgery. When only the North American patients were analyzed, early
surgery (days 0–3) provided the best results in lower grade patients [12]. There
was no difference in the incidence of intraoperative rupture between early and
late surgery, and although there was a relationship between ‘‘tightness’’ of the
brain during surgery and the interval from SAH to operation, aneurysm dissection
was no more difficult in early than in late surgery [11]. The timing of surgery
does not influence the risk for cerebral vasospasm [13].
Table 4
Potential complications of subarachnoid hemorrhage
. Rebleeding
. Vasospasm
. Intracranial hypertension
. Hydrocephalus
. Hyponatremia/volume contraction
. Seizures
Table 3
World Federation of Neurosurgeons (WFNS) SAH Scale [9]
WFNS grade GCS scale Motor deficit
I 15 Absent
II 13–14 Absent
III 13–14 Present
IV 7–12 Present or absent
V 3–6 Present or absent
Abbreviations: SAH, subarachnoid hemorrhage; GCS, Glasgow Coma Scale.
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388 379

Cerebral vasopasm is a major cause of morbidity and mortality in SAH
patients [10,14]. Angiographic evidence of vasospasm can be detected in up to
70% of patients. However, clinical vasospasm with ischemic deficits is observed
in approximately 30% of patients, most often between days 4–12, with a peak at
6–7 days following SAH [10]. The diagnosis of vasospasm is confirmed by
angiography. The transcranial Doppler (TCD) is a safe, repeatable, noninvasive
method to identify and quantify vasospasm, and can be used to evaluate the
effectiveness of various therapies [15].
The mechanism responsible for vasospasm is unknown; however, structural
and pathologic changes have been demonstrated in the vessel wall [16]. There is
also evidence that vasospasm after SAH correlates with the amount of blood in
the subarachnoid space, and removal of extravasated blood decreases the
occurrence and severity of ischemic deficits [14,16]. The component in blood
implicated in causing cerebral arterial vasospasm is oxyhemoglobin.
Many drugs have been investigated for prevention or treatment of vasospasm,
but most are ineffective. The calcium channel blocker, nimodipine, has become
standard prophylactic therapy. However, the efficacy of prophylactic nimodipine
after SAH has been seriously challenged [17]. A recent meta-analysis showed a
reduction in vasospasm in nimodipine groups, but a corresponding reduction in
mortality was slight and not statistically significant compared to control groups.
‘‘Triple H’’ therapy—hypervolemia, hypertension, and hemodilution—has
become the mainstay of treatment for ischemic neurologic deficits caused by
cerebral vasospasm [18–20]. To improve cerebral blood flow to areas of impaired
autoregulation, cerebral perfusion pressure is increased by intravascular volume
expansion and induced hypertension. Intravascular volume expansion is accom-
plished with infusion of crystalloid, colloid, or blood to a pulmonary capillary
wedge pressure of 12–18 mmHg or a central venous pressure of 10–12 mmHg. If
this regimen does not reverse the deficit, a vasopressor (eg, dopamine) is
introduced to raise systemic blood pressure until the neurologic deficits subside
or reverse. This therapy can worsen cerebral edema, increase ICP, and cause
hemorrhagic infarction. Systemic complications include pulmonary edema and
cardiac failure in patients at risk. Hemodilution, the last component of ‘‘triple H’’
therapy, decreases blood viscosity and improves cerebral blood flow. The optimal
hematocrit thought to maximize the oxygen delivery to tissues has been estimated
at 33%, but may be higher in the ischemic brain.
Another method for treating symptomatic vasospasm is cerebral angioplasty.
Transluminal angioplasty can be used to dilate constricted major cerebral vessels
in patients refractory to conventional treatment [21,22]. Superselective intra-
arterial infusion of papaverine dilates distal vessels not accessible to angioplasty
[23]. These procedures are usually performed under general anesthesia to
minimize movement and permit accurate placement of the intraarterial balloon
used to dilate the cerebral vessels. The risks of angioplasty include aneurysm
rupture, intimal dissection, vessel rupture, ischemia, and infarction.
Intacranial hypertension is present to some degree in most patients following
a SAH. In the uncomplicated case, intracranial hypertension does not require
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388380

specific treatment. Intracranial pressure gradually returns to normal by the end
of the first week. If an intracerebral hemorrhage, intraventricular hemorrhage,
vasospasm, or hydrocephalus develops, intracranial hypertension may be se-
vere and require treatment. Patients may require emergency ventriculostomy,
steroids, diuretics, or intubation and hyperventilation. ICP should be lowered
gradually, especially in patients with unclipped aneurysms. Abrupt lowering of
ICP by lumbar puncture, ventricular drainage, or rapid infusion of mannitol can
induce rebleeding.
Acute (obstructive) hydrocephalus after SAH complicates approximately
20% of the cases [24]. Although controversial, ventriculostomy has been re-
commended for treating acute hydrocephalus in patients with a diminished level
of consciousness after SAH [24]. Ventriculostomy has been associated with
increased rebleeding and infection.
Anesthetic management
Preoperative evaluation
When the neurologic examination is performed, the patient’s clinical grade is
noted. The patient’s CT scan or MR image is evaluated to assess the presence and
severity of intracranial hypertension. The severity, acuteness, and stage of the
SAH, the presence of intracranial hypertension, and the timing of surgery will
determine the anesthetic management.
Electrolyte abnormalities frequently occur secondary to the syndrome of
inappropriate antidiuretic hormone (SIADH) secretion or diabetes insipidus.
Hyponatremia is the most common electrolyte disturbance detected, and is often
associated with a high urinary sodium and osmolality, which is expected with
SIADH. Unlike a patient with SIADH, however, the patient with SAH usually
has a contracted intravascular volume despite hyponatremia. This cerebral salt-
wasting syndrome may be caused by release of an atrial natriuretic factor from the
damaged brain. The recommended therapy is to maintain normovolemia with
isotonic saline solutions. Other factors contributing to intravascular volume
contraction in these patients are supine diuresis secondary to increased thoracic
blood volume, negative nitrogen balance, decreased erythropoiesis, increased
catecholamine levels, and iatrogenic blood loss. Fluid balance and electrolyte
abnormalities should be corrected prior to surgery.
Electrocardiographic abnormalities are commonly associated with ruptured
cerebral aneurysms [25]. The ECG changes include ST-segment depression or
elevation, T-wave inversion or flattening, U-waves, prolonged Q-T intervals, and
dysrhythmia. The ECG changes are not necessarily associated with increased
operative morbidity and mortality or consistent increases in serum myoglobin or
creatine kinase. They usually resolve within 10 days following SAH, and require
no special treatment. When indicated, cardiac troponin-I levels should be drawn
to determine the clinical significance of these abnormalities [26]. When cardiac
dysrhythmia and occasional frank subendocardial ischemia result in cardiac
failure, appropriate treatment must be instituted.
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388 381

Intraoperative management
The anesthetic goals for intracranial aneurysm surgery are to avoid aneurysm
rupture, maintain cerebral perfusion pressure and transmural aneurysm pressure,
and provide, a ‘‘slack’’ brain. Patients in WFNS scale I or II who appear anxious
should receive premedication. Cerebral perfusion pressure (CPP) is maintained by
using drugs in doses that avoid sudden or profound decreases in systemic blood
pressure or increases in ICP. Similarly, transmural pressure, which is defined as the
difference between mean arterial pressure and ICP, must be maintained. (The
pressure within an aneurysm is equal to the systemic blood pressure.) The
relationship between transmural pressure and wall stress or tension of the
aneurysm is linear. An increase in mean arterial pressure or fall in ICP will
increase transmural pressure, wall stress, and risk of aneurysm rupture. Methods to
control brain volume and ICP, such as hyperventilation, diuretics, spinal drainage,
and head position, facilitate surgical exposure and minimize the retraction pressure
that can cause tissue injury.
Standard monitoring plus an arterial pressure catheter are routinely used. A
central venous pressure (CVP) or pulmonary artery (PA) catheter is recommen-
ded in WFNS scale III or higher to provide a more accurate measure of the
patient’s volume status and cardiac function intraoperatively and postoperatively
in the prevention or management of cerebral vasospasm. Electrophysiologic
monitoring with the electroencephalogram (EEG) or somatosensory evoked
potentials (SSEPs) may be used to monitor the adequacy of cerebral perfusion
during induced hypotension or temporary/permanent aneurysm clip application.
When barbiturates are administered for brain protection, the EEG is used to guide
the dose required to achieve a burst suppression pattern.
To minimize the risk of hypertension and aneurysmal rupture during induction
of anesthesia, intravenous lidocaine and the beta-adrenergic antagonist (esmolol)
or labetalol are recommended. Following induction, ventilation is mechanically
controlled to maintain normocarbia, if ICP is normal. If intracranial hypertension
is present, the PaC02 is lowered to 30–35 mmHg. A deep plane of anesthesia
must be established prior to insertion of head pins, scalp incision, turning the
bone flap, and opening the dura to avoid a hypertensive response. When intra-
cranial hypertension is present, anesthesia should be deepened with additional
doses of thiopental and fentanyl until the skull is opened. Several techniques can
be instituted during aneurysm surgery to provide a ‘‘slack’’ brain and facilitate
dissection. These are hyperventilation of the lungs, osmotic diuresis, barbiturate
administration, and CSF drainage during the procedure.
The drugs most frequently used to maintain anesthesia during aneurysm
surgery are fentanyl and thiopental (bolus dosing or infusions) in conjunction
with isoflurane in oxygen. A propofol infusion instead of thiopental may also be
used for these procedures. In conditions of poor intracranial compliance, a
continuous infusion of thiopental (1–3 mg�kg�1�h�1) following a bolus dose
of 5 mg�kg�1 is recommended as the primary anesthetic for aneurysm surgery in
conjunction with a fentanyl infusion (1–4 mg�kg�1�h�1) and one-half MAC
concentration of isoflurane in oxygen. The total dose of fentanyl should not
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388382

exceed 10–12 mg�kg�1, unless postoperative ventilation is planned. Potential
disadvantages to using thiopental are blood pressure instability and prolonged
recovery from anesthesia. With this technique, a pulmonary artery catheter should
be inserted to monitor and optimize cardiovascular performance and intravascular
volume. Following an uneventful aneurysm clip application, the thiopental
infusion is discontinued to prevent a delay in recovery.
Prior to aneurysm clipping, isotonic crystalloid solutions without glucose are
administered to replace overnight fluid losses and provide hourly maintenance
fluid requirements. When the aneurysm is secured, intraoperative fluid deficits
are replaced and additional volume is administered. At the time of aneurysm
dissection, blood is available for transfusion in case the aneurysm ruptures. A
bolus of thiopental (3–5�mg�kg�1) may be given before temporary occlusion of a
major intracranial vessel and before aneurysm clipping. If temporary occlusion
lasts longer than 10 minutes, recirculation should be established, and additional
thiopental administered before reapplying the temporary clip. Following aneu-
rysm clipping, the central venous pressure and pulmonary capillary wedge
pressure are raised to 10–12 mmHg or 12–18 mmHg, respectively, with crys-
talloid, colloid, or blood. A postoperative hematocrit between 30–35% is
desirable. As discussed previously, intravascular volume expansion with hemo-
dilution is recommended to reduce the risk of postoperative cerebral vasospasm.
When considering the use of deliberate hypotension during aneurysm
dissection, the risk-benefit ratio must be assessed for each patient [27]. The
potential benefit of hypotension must be weighed against the risk of causing
cerebral ischemia or ischemia to other organs. Patients with a history of cardio-
vascular disease, occlusive cerebrovascular disease, intracerebral hematoma,
fever, anemia, and renal disease are not good candidates for induced hypotension.
Such patients should only be subjected to moderate reductions in systemic blood
pressure (20–30 mmHg), if at all. The most commonly used agents to induce
hypotension are sodium nitroprusside, isoflurane, and esmolol. Overall, induced
hypotension has declined in use and has been replaced by temporary clipping
[28,29]. The temporary occlusion of a feeding artery produces an acute reduction
in focal blood flow and a slack aneurysm, thus eliminating the need for induced
hypotension and its systemic effects. Depending on the location of the aneurysm,
either somatosensory evoked potentials or brain stem auditory evoked potentials
can be used to monitor the safety of temporary occlusion [28].
The major intraoperative complication of aneurysm surgery is hemorrhage.
When an aneurysm ruptures intraoperatively, there is potential for major ischemic
damage from hypotension and the surgical efforts to control bleeding. Hemor-
rhagic death is also possible. When the leak is small and the dissection is complete,
it may be possible for the surgeon to gain control with suction and then apply the
permanent clip to the neck of the aneurysm. Alternatively, temporary clips can be
applied proximal and distal to the aneurysm to gain control. Thiopental may be
given to provide some protection prior to the placement of the temporary clip.
During temporary occlusion, normotension should be maintained to maximize
collateral perfusion. If temporary occlusion is not planned or not possible and
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388 383

blood loss is not significant, the mean arterial pressure may be transiently
decreased to 50 mmHg or lower to facilitate surgical control. When bleeding is
excessive, aggressive fluid resuscitation and blood transfusion must commence
immediately. Administration of cerebroprotective agents may not be possible
because of associated hemodynamic effects. Under these conditions, induced
hypotension is not advised, as the intravascular volume must be restored first.
Intraoperative cerebral protection
Thiopental has been the drug of choice for intraoperative cerebral protection
during aneurysm surgery. In animal models, barbiturates have shown protection
during incomplete focal ischemia, but not during global ischemia [30]. Barbitu-
rates are the only agents shown to be useful in humans [30].
Many practitioners institute mild intraoperative hypothermia (32–34�C)during aneurysm surgery [31] to enhance the brain’s ability to tolerate ischemia
[32]. Its value is unproven, and its use may produce harmful side effects [33]. A
large multi-institutional study is underway to determine whether mild intraoper-
arive hypothermia will benefit this patient population [34].
The primary goals at the conclusion of surgery are to avoid coughing, strain-
ing, hypercarbia, and hypertension. For patients in WFNS grades I and II who
have no intraoperative complications, the endotracheal tube should be removed in
the operating room and a neurologic examination performed. Patients who have
intraoperative complications or have depressed consciousness preoperatively
(WFNS grades III–V) should remain intubated and receive mechanical ventila-
tion until their neurologic status improves.
Postoperative concerns
Variation in systemic blood pressure is common postoperatively, and contri-
butes significantly to morbidity and mortality in patients following aneurysm
repair. Causes of hypertension include preexisting hypertension, pain, and CO2
retention from residual anesthesia. The treatment of postoperative hypertension is
critical to prevent the formation of cerebral edema or hematoma. Antihypertensive
drugs should be administered after respiratory depression and pain are eliminated
as causes. The hypertensive response usually subsides within 12 hours. When
indicated, preoperative antihypertensive drugs are reinstituted and maintained.
After clipping of the aneurysm, cerebral vasospasm continues to pose a threat
to neurologic integrity. Postoperative hypotension must be avoided, and the
patient’s intravascular volume must be accurately assessed with either a central
venous pressure or pulmonary artery catheter. As previously discussed, a higher
than normal intravascular fluid volume should be maintained.
Arteriovenous malformations
An arteriovenous malformation (AVM) of the brain consists of a tangle of
congenitally malformed blood vessels that forms an abnormal communication
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388384

between the arterial and venous systems. The arterial afferents flow directly into
venous efferents without the usual resistance of an intervening capillary bed;
thus, oxygenated blood is shunted directly into the venous system, leaving
surrounding brain tissue transiently or permanently ischemic.
Neurological AVMs affect about 1% of the population in the United States, and
are about one tenth as common as aneurysms [35]. They occur at roughly equal
rates in males and females of all racial or ethnic backgrounds. Seizures (partial or
total) and headaches are the most frequent symptoms of AVMs. The onset of
complaints is usually between the ages of 20 and 40. Approximately 80% of
patients with AVMs develop symptoms by the time they are 40 years old. If the
patient does not develop symptoms by 40 or 50 years old, the lesions tend to remain
stable and asymptomatic (approximately 20%) [36]. The most common initial
presentation is spontaneous hemorrhage, followed by seizures, then less frequently
by progressive focal neurologic sensory/motor deficits occurring in a child or
young adult. Avein of Galen AVM in infants may present with hydrocephalus and/
or high-output cardiac failure. The natural history of AVMs is not completely
understood. The risk of hemorrhage is approximately 1–3% per year. The rate of
rebleeding is 6% in the first year after a hemorrhage and about 2% per year
thereafter [36]. Mortality from initial hemorrhage is high, with reports between
10–30%. Recurrence of hemorrhage with a fatal outcome is a constant danger.
There are several options for the management of AVMs, incuding surgical
excision, embolization, stereotactic radiosurgery (proton beams, gamma rays, or
linear accelerator), a combination of the above, and leaving AVMs alone. AVMs
of suitable size and location can be managed successsfully with surgical excision.
Surgical mortality ranges from 0.6% to 14%, and correlates with size, location,
and pattern of involvement of the AVM [36]. Early postoperative morbidity
ranges from 17% to 28%; however, outcome studies report improvement in
morbidity over time [37]. To avoid intraoperative or postoperative massive brain
swelling or hemorrhage of large AVMs, operations may be staged or follow
preoperative embolization.
Special anesthetic considerations
In addition to providing anesthesia for craniotomy and resection of the AVM,
anesthesia may be required for radiologic embolization of the AVM. Closed
embolization of cerebral AVMs is uncomfortable and invasive. This procedure
may be performed under local anesthesia with sedation or under general anes-
thesia. It has been performed successfully with various combinations of sedative
drugs (opioids, droperidol, midazolam, or propofol) that allow neurologic exami-
nations during the procedure and permit immediate diagnosis of complications
[21,36]. Children, uncoopeative patients, and those with intracranial hypertension
or airway problems usually require general anesthesia. General anesthesia does
not allow direct neurologic assessment. Potential complications of embolization
procedures are embolic or ischemic stroke and hemorrhage from the AVM, either
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388 385

acute or delayed. New onset or preexisting seizures may occur during the
embolization procedure requiring treatment with benzodiazepines or barbiturates.
The anesthetic management of patients with AVMs is similar to the management
of patients for aneurysm surgery. Depending on the presentation, the anesthetic
approach is modified. For example, a large bleed may present with symptoms
relating to mass effects and require maneuvers to reduce ICP. High flow through a
large intact AVMmay cause a ‘‘steal,’’ with resulting cerebral ischemia, and require
different techniques to improve CPP. With more extensive lesions, hypothermia
and high-dose barbiturates have been recommended for brain protection. Induced
hypotension may also be required to reduce lesion size and blood flow.
Hyperemic complications, defined as perioperative edema or hemorrhage,
may occur after removel of the AVM. Although the mechanism is unclear, one
theory proposes that breakthrough cerebral edema and hemorrhage result when
blood flow from the surgically obliterated AVM is diverted to the surrounding
brain. The smaller vessels in the brain surrounding the AVM are not accustomed
to the higher pressure-flow state, and autoregulation is exceeded, resulting in
severe brain swelling, edema, and hemorrhage. The clinical syndrome of cerebral
hyperperfusion with normal CPP has been called normal perfusion pressure
breakthrough [38]. Other studies report information that is not consistent with this
theory [39,40]. Immediate treatment should include the simultaneous application
of high-dose barbiturates, osmotic diuretics, hyperventilation, and maintenance of
a low normal mean arterial pressure (MAP). Hypothermia may also be instituted.
When marked brain swelling occurs intraoperatively, the patient should remain
intubated, hyperventilated, and sedated postoperatively. Hypertension during
emergence and postoperatively must be controlled, preferably with beta-blockers,
to prevent bleeding into the bed of the AVM.
Summary
The management of patients for intracranial vascular surgery is very challen-
ging, requiring an aggressive multidisciplinary approach to provide care and
improve outcome. This ensures early identification and treatment of the disease,
resuscitation when indicated, and continuous and intensive perioperative mon-
itoring to identify and treat potential complications. With advances in neuro-
imaging, interventional, and surgical techniques, we are increasingly involved in
providing neuroanesthetic skills and insightful care to facilitate the successful
management of these high-risk patients.
References
[1] King JT. Epidemiology of aneurysmal subarachnoid hemorrhage. Neuroimaging Clin N Am
1997;7(4):659–68.
[2] Wardlaw JM, White PM. The detection and management of unruptured intracranial aneurysms.
Brain 2000;123:205–21.
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388386

[3] Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients
with unruptured intracranial aneurysms, from the Stroke Council of the AHA. Circulation
2000;102:2300–8.
[4] The International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intra-
cranial aneurysms—risk of rupture and risks of surgical intervention. N Engl J Med 1998;339:
1725–33.
[5] Botterell EH, Longhead WM, Scott JW, et al. Hypothermia and interruption of the carotid or
carotid and vertebral circulation in the surgical management of intracranial aneurysms. J Neuro-
surg 1956;13:1–42.
[6] Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial
aneurysms. J Neurosurg 1968;28:14–20.
[7] Drake CG, Hunt WE, Sank K, et al. Report of World Federation of Neurological Surgeons
Committee on a universal subarachnoid hemorrhage grading scale. J Neurosurg 1988;68:985–6.
[8] Mayberg MR. Warning leaks and subarachnoid hemorrhage. West J Med 1990;153:549–50.
[9] Kassell NF, Torner JC. Aneurysmal rebleeding: a preliminary report from the Cooperative
Aneurysm Study. J Neurosurg 1983;13:479–81.
[10] Kassell NF, Torner JC, Haley EC, et al. The International Cooperative Study on the Timing of
Aneurysm Surgery. Part I: overall management results. J Neurosurg 1990;73:18–36.
[11] Kassell NF, Torner JC, Jane JA, et al. The International Cooperative Study on the Timing of
Aneurysm Surgery. Part II: surgical results. J Neurosurg 1990;73:37–47.
[12] Haley EC Jr, Kassell NF, Torner JC. The International Cooperative Study on the Timing of
Aneurysm Surgery. The North American Experience. Stroke 1992;23:205–14.
[13] MacDonald RL, Wallace MC, Coyne TJ. The effect of surgery on the severity of vasospasm.
J Neurusurg 1994;80:433–9.
[14] Kassell NF, Sasaki T, Colohan ART, et al. Cerebral vasospasm following aneurysmal subarach-
noid hemorrhage. Stroke 1985;16:562–72.
[15] Lindegaard KF. The role of transcranial doppler in the management of patients with subarach-
noid haemorrhage—a review. Acta Neurochir 1999;72:59–71.
[16] McGrath BJ, Guy J, Borel CO, et al. Perioperative management of aneurysmal subarachnoid
hemorrhage: part 2. Postoperative management. Anesth Analg 1995;81(6):1295–302.
[17] Barker FG II, Ogilvy CS. Efficacy of prophylactic nimodipine for delayed ischemic deficit after
subarachnoid hemorrhage: a metaanalysis. J Neurosurg 1996;84:405–14.
[18] Awad IA, Carter LP, Spetzler RF, et al. Clinical vasospasm after subarachnoid hemorrhage:
response to hypervolemia, hemodilution and arterial hypertension. Stroke 1987;18:365–72.
[19] Medlock MD, Dulebohn SC, Elwood PW. Prophylactic hypervolemia without calcium channel
blockers in early aneurysm surgery. Neurosurgery 1992;30:12–6.
[20] Origitano TC, Wascher TM, Reichman OH, et al. Sustained increased cerebral blood flow with
prophylactic hypertensive hypervolemic hemodilation (‘‘triple-H’’ therapy) after subarachnoid
hemorrhage. Neurosurgery 1990;27:729–39.
[21] Luginbuhl M, Remonda L. Interventional neuroradiology. Recent developments and anaesthe-
siologic aspects. Minerva Anestesiol 1999;65:445–54.
[22] Newell DW, Eskridge JM, Mayberg MR, et al. Angioplasty for the treatment of symptomatic
vasospasm following subarachnoid hemorrhage. J Neurosurg 1989;71:654–60.
[23] KakuY, YonekawaY, Tsukahara T, et al. Superselective intra-arterial infusion of papaverine for the
treatment of cerebral vasospasm after subarachnoid hemorrhage. J Neurosurg 1992;77:842–7.
[24] Rajshekhar V, Harbaugh RE. Results of routine ventriculostomy with external ventricular drain-
age for acute hydrocephalus following subarachnoid hemorrhage. Acta Neurochir (Wien) 1992;
115:8–14.
[25] Davis TP, Alexander J, Lesch M. Electrocardiographic changes associated with acute cerebro-
vascular disease: a clinical review. Prog Cardiovasc Dis 1993;36(3):245–60.
[26] Horowitz MB, Willet D, Keffer J. The use of cardiac troponin-I (c Tn I) to determine the
incidence of myocardial ischemia and injury in patients with aneurysmal and presumed aneur-
ysmal subarahnoid hemorrhage. Acta Neurochir (Wien) 1998;140:87–93.
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388 387

[27] Giannotta SL, Oppenheimer JH, Levy ML, et al. Management of intraoperative rupture of
aneurysm without hypotension. Neurosurgery 1991;28(4):531–5.
[28] Mizoi K, Yoshimoto T. Permissible temporary occlusion time in aneurysm surgery as evaluated
by evoked potential monitoring. Neurosurgery 1993;33:434–40.
[29] Oglivy CS, Carter BS, Kaplan S, et al. Temporary vessel occlusion for aneurysm surgery: risk
factors for stroke in patients protected by induced hypothermia and hypertension and intravenous
mannitol administration. J Neurosurg 1996;84:785–91.
[30] Bendo AA, Kass IS, Hartung J, et al. Anesthesia for neurosurgery. In: Barash PG, et al, editors.
Anesthesia. 4th edition. Philadelphia: JP Lippincott-Raven; 2001. p. 743–89.
[31] Craen RA, Gelb AW, Eliasziw M, et al. Current anesthetic practices and use of brain protective
therapies for cerebral aneurysm at 41 North American centers. J Neurosurgical Anesth 1994;
6:303.
[32] Karibe H, Sato K, Shimizu H, et al. Intraoperative mild hypothermia ameliorates postoperative
cerebral blood flow impairment in patients with aneurysmal subarachnoid hemorrhage. J Neuro-
surg 2000;47:594–601.
[33] Sessler DI. Mild perioperative hypothermia. N Eng J Med 1997;336:1730–7.
[34] Hindman BJ, Todd MM, Gelb AW, et al. Mild hypothermia as a protective therapy during
intracranial aneurysm surgery: a randomized prospective pilot trial. Neurosurgery 1999;44(1):
23–32.
[35] National Institute of Neurological Disorders and Stroke. Arteriovenous malformations and other
vascular lesions of the central nervous sytem fact sheet. NIH Publication No. 01-4854, October
2000. Available at: http://www.ninds.nih.gov/health_and_medical/pubs/arteriovenous.htm.
[36] Dodson BA. Interventional neuroradiology and the anesthetic management of patients with
arteriovenous malformations In: Cottrell JE, Smith DS, editors. Anesthesia and neurosurgery.
4th edition. St. Louis: Mosby; 2001. p. 399–423.
[37] Heros RC, Korosue K, Diebold PM. Surgical excision of cerebral arteriovenous malformations:
late results. Neurosurgery 1990;26:570–7.
[38] Batjer HH, Devous MD, Meyer YJ, et al. Cerebrovascular hemodynamics in arteriovenous mal-
formation complicated by normal perfusion pressure breakthrough. Neurosurgery 1988;22:
503–9.
[39] Young WL, Kader A, Ornstein E, et al. Cerebral hyperemia after arteriovenous malformation
resection is related to ‘‘breakthrough’’ complications but not to feeding artery pressure. Neuro-
surgery 1996;38:1085–93.
[40] Young WL, Prohovnik I, Ornstein E, et al. Pressure autoregulation is intact after arteriovenous
malformation resection. Neurosurgery 1993;32:491–6.
A.A. Bendo / Anesthesiology Clin N Am 20 (2002) 377–388388

Pediatric neuroanesthesia
Sulpicio G. Soriano, MD*, Elizabeth A. Eldredge, MD,Mark A. Rockoff, MD
Children’s Hospital and Harvard Medical School, 300 Longwood Avenue, Boston, MA 02115, USA
Recent advances in pediatric neurosurgery have dramatically improved the
outcome in infants and children afflicted with surgical lesions of the central
nervous system (CNS). Although most of these techniques were first applied to
adults, the physiologic and developmental differences that are inherent in
pediatric patients present challenges to neurosurgeons and anesthesiologists alike.
The aim of this paper is to highlight these age-dependent approaches to the
pediatric neurosurgical patient.
Developmental considerations
Age-dependent differences in cerebrovascular physiology and cranial bone
development influence the approach to the pediatric neurosurgical patient.
Cerebral blood flow is coupled tightly to metabolic demand, and both increase
proportionally immediately after birth. Estimates from animal studies place the
autoregulatory range of blood pressure in a normal newborn between 20 and
60 mmHg [1]. This range is consistent with relatively low cerebral metabolic
requirements and low blood pressure during the perinatal period. More impor-
tantly, the slope of the autoregulatory slope drops and rises significantly at the
lower and upper limits of the curve, respectively. This narrow range, with sudden
hypotension and hypertension at either end of the autoregulatory curve, places the
neonate at risk for cerebral ischemia and intraventricular hemorrhage, respec-
tively. Another developmental difference between adults and pediatric patients is
the larger percentage of cardiac output that is directed to the brain, because the
head of the infant and child accounts for a large percentage of the body surface
area and blood volume. These factors place the infant at risk for significant
hemodynamic instability during neurosurgical procedures.
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00008 -6
* Corresponding author.
E-mail address: [email protected] (S.G. Soriano).
Anesthesiology Clin N Am
20 (2002) 389–404

The infant cranial vault is also in a state of flux. Open fontanels and cranial
sutures lead to a compliant intracranial space. The mass effect of a tumor or
hemorrhage are often masked by a compensatory increase in the intracranial
volume through the fontanels and sutures. As a result, infants presenting with
signs and symptoms of intracranial hypertension have fairly advanced pathology.
Preoperative evaluation and preparation
Closed-claim studies have revealed that neonates and infants are at higher risk
for morbidity and mortality than any other age group [2,3]. Respiratory and
cardiac-related events account for a majority of these complications. However, a
major pitfall in the management of infants and children for neurosurgery is the
presence of coexisting diseases. Given the urgent nature of most pediatric
neurosurgical procedures, a thorough preoperative evaluation may be difficult.
However, a complete airway examination is essential, because some craniofacial
anomalies may require specialized techniques to secure the airway [4]. Most
cardiac morbidity due to congenital heart disease occurs during the first year of
life [5]. Congenital heart disease may not be apparent immediately after birth, and
the hemodynamic alterations caused by anesthetic agents, mechanical ventilation,
and blood loss during surgery can unmask these cardiac defects. Echocardiog-
raphy can be helpful in the assessment of the heart, and a pediatric cardiologist
should evaluate patients with suspected problems to help optimize cardiac
function prior to surgery. Other coexisting diseases that can alter the conduct
of anesthesia are list in Table 1.
Table 1
Perioperative concerns for infants and children with neurological disease
Condition Anesthetic implications
Congenital heart disease Hypoxia and cardiovascular collapse
Prematurity Postoperative apnea
Upper respiratory tract infection Laryngospasm and postoperative hypoxia/pneumonia
Craniofacial abnormality Difficulty with airway management
Denervation injuries Hyperkalemia after succinycholine
Resistance to nondepolarizing muscle relaxants
Chronic anticonvulsant therapy for epilepsy Hepatic and hematological abnormalities
Increased metabolism of anesthetic agents
Arteriovenous malformation Potential congestive heart failure
Neuromuscular disease Malignant hyperthermia
Respiratory failure
Sudden cardiac death
Chiari malformation Apnea
Aspiration pneumonitis
Hypothalamic/pituitary lesions Diabetes insipidus
Hypothyroidism
Adrenal insufficiency
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404390

Preoperative sedatives given prior to induction of anesthesia can ease the
transition from the preoperative holding area to the operating room [6]. Midazolam
given orally is particularly effective in relieving anxiety and producing amnesia. If
an indwelling intravenous (i.v.) catheter is in place, midazolam can be slowly
administered to achieve sedation. Alternatively, sedatives such as barbiturates can
be given rectally to induce sleep in preschool children who are uncooperative, and
this avoids the use of intramuscular injections. However, methohexital adminis-
tered rectally has been shown to induce seizures in patients with epilepsy [7].
Intraoperative management
Induction of anesthesia
The patient’s neurological status and coexisting abnormalities will dictate the
appropriate technique and drugs for induction of anesthesia. General anesthesia
can be established by inhalation of sevoflurane and nitrous oxide with oxygen. A
nondepolarizing muscle relaxant such as pancuronium is then administered to
facilitate intubation of the trachea. Alternatively, if the patient has i.v. access,
anesthesia can be rapidly induced with sedative/hypnotic drugs such thiopental
(5–8 mg/kg) or propofol (3–5 mg/kg). Patients at risk for aspiration pneumonitis
should have a rapid-sequence induction of anesthesia performed with thiopental
or propofol, immediately followed by a rapid-acting muscle relaxant such as
succinylcholine or rocuronium.
Airway management
Developmental differences in the cricoidthyroid and tracheobrochial tree have
a significant impact on management of the pediatric airway. The infant’s larynx is
funnel shaped, and narrowest at the level of the cricoid, making this the smallest
cross-sectional area in the infant airway. This feature places the infant at risk for
subglotic obstruction secondary to mucosal swelling after prolonged endotracheal
intubation with a tight-fitting endotracheal tube. Because the trachea is relatively
short, an endotracheal tube can migrate into a mainstem bronchus if the infant’s
head is flexed, as is the case for a suboccipital approach to the posterior fossa or
the cervical spine. Therefore, the anesthesiologist should auscultate both lung
fields to rule out inadvertent intubation of a mainstem bronchus after positioning
the patient. Nasotracheal tubes are best suited for situations when the patient will
be prone and when postoperative mechanical ventilation is anticipated. Further-
more, the endotracheal tube can kink at the base of the tongue when the head is a
flexed and also lead to pressure necrosis of the oral mucosa.
Maintenance of anesthesia
The choice of anesthetic agents for maintenance of anesthesia has been
shown not to affect the outcome of neurosurgical procedures [8]. The most
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404 391

frequently utilized technique for neurosurgery consists of the opioid fentanyl
administered at a rate of 2–5 mg/kg/h intravenously along with inhaled nitrous
oxide (70%) and low-dose isoflurane (0.2–0.5%). Deep neuromuscular block-
ade is maintained during most neurosurgical procedures to avoid patient
movement. Patients on chronic anticonvulsant therapy will require larger doses
of muscle relaxants and narcotics because of induced enzymatic metabolism of
these agents (Fig. 1) [9,10] .Muscle relaxation should be withheld, or should
not be maintained when assessment of motor function during seizure and spinal
cord surgery is planned.
Fluid restriction and diuretic therapy may lead to hemodynamic instability and
even cardiovascular collapse if sudden blood loss occurs during surgery.
Therefore, normovolemia should be maintained through the procedure. Normal
saline is commonly used as the maintenance fluid during neurosurgery because it
is mildly hyperosmolar (308 mOsm/kg), and it theoretically attenuates brain
edema. However, rapid infusion of normal saline (30 mL/kg/h) is associated with
hyperchloremic acidosis [11]. Hyperventilation and maximization of venous
Fig. 1. Patients on chronic anticonvulsant therapy have increased requirements for nondepolarizing
muscle relaxants. The recovery times for return of muscle function in the anticonvulsant was
significantly faster than the control group ( * p < 0.05, mean ± SD) [10].
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404392

drainage of the brain by elevating the head can minimize brain swelling. Should
these maneuvers fail, mannitol can be given at a dose of 0.25 to 1.0 g/kg
intravenously. This will transiently alter cerebral hemodynamics and raise serum
osmolality by 10–20 mOsm/kg [12]. However, repeated dosing can lead to
extreme hyperosmolality, renal failure, and further brain edema. Furosemide is a
useful adjunct to mannitol in decreasing acute cerebral edema, and has been
shown in vitro to prevent rebound swelling due to mannitol [13]. All diuretics
will interfere with the ability to utilize urine output as a guide to intravascular
volume status.
Vascular access
Due to limited access to the child during neurosurgical procedures, optimal
intravenous access is mandatory prior to the start of surgery. Typically, two large-
bore venous cannulae are sufficient for most craniotomies. Should initial attempts
fail, central vein cannulation may be necessary. Cannulation of femoral vein
avoids the risk of pneumothorax associated with subclavian catheters, and does
not interfere with cerebral venous return.
Monitoring
Given the potential for sudden hemodynamic instability due to venous air
emboli (VAE), hemorrhage, herniation syndromes, and manipulation of cranial
nerves, the placement of an intra-arterial cannula for continuous blood pressure
monitoring is mandatory for most neurosurgical procedures. An arterial catheter
will also provide access for sampling serial blood gases, electrolytes, and
hematocrit. The issue of central venous catheterization is controversial. Large-
bore catheters are too large for infants and most children, and central venous
pressures may not accurately reflect vascular volume, especially in a child in
the prone position. Therefore, the risks may outweigh the benefits of a central
venous catheter.
Standard neurosurgical technique may elevate the head of the table to improve
venous drainage, and is conducive to air entrainment into the venous system
through open venous channels in bone and sinuses (Fig. 2) [14]. Patients with
cardiac defects, such as patent foramen ovale or ductus arteriosus, are at risk for
arterial air emboli through these defects, and should be monitored carefully. A
precordial Doppler ultrasound can detect minute VAE, and should be routinely
used in conjunction with an end-tidal carbon dioxide analyzer and arterial
catheter in all craniotomies to detect VAE. Doppler probe is best positioned on
the anterior chest usually just to the right of the sternum at the fourth intercostal
space. An alternate site on the posterior thorax can be used in infants weighing
approximately 6 kg or less [15].
Recent advances in neurophysiologic monitoring have enhanced the ability to
safely perform more definitive neurosurgical resections in functional areas of the
brain and spinal cord. However, the CNS depressant effects of most anesthetic
agents limit the utility of these monitors. A major part of preoperative planning
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404 393

should include a thorough discussion of the modality and type of neurophysio-
logic monitoring to be used during any surgical procedure. In general, electro-
corticography (ECoG) and electroencephalography (EEG) require low levels of
volatile anesthetics and barbiturates. Somatosensory-evoked potentials used
during spinal and brainstem surgery can be depressed by volatile agents and to
a lesser extent, nitrous oxide. An opioid-based anesthetic is the most appropriate
agent for this type of monitoring. Spinal cord and peripheral nerve surgery may
require electromyography (EMG) and detection of muscle movement as an end
point. Therefore, muscle relaxation should be avoided or not maintained during
the monitoring period.
Positioning
Patient positioning for surgery requires careful preoperative planning to allow
adequate access to the patient for both the neurosurgeon and anesthesiologist.
Table 2 describes various surgical positions and their physiologic sequelae. The
prone position is commonly used for posterior fossa and spinal cord surgery,
although the sitting position may be more appropriate for obese patients who
may be difficult to ventilate in the prone position (Fig. 3). In addition to the
physiologic sequelae of this position, a whole spectrum of compression and
stretch injuries has been reported. Padding under the chest and pelvis can
support the torso. It is important to ensure free abdominal wall motion because
increased intra-abdominal pressure can impair ventilation, cause venocaval
Fig. 2. Supine infant. Note that the infant’s head lies at a higher plane than the rest of his body. This
increases the likelihood for venous air embolism during craniotomies.
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404394

compression, and increase epidural venous pressure and bleeding. Fig. 4
illustrates proper positioning for these patients. Soft rolls are used to elevate
and support the lateral chest wall and hips to minimize increase abdominal and
thoracic pressure. In addition, this should allow a Doppler probe to be on the
chest without pressure. Many neurosurgical procedures are performed with
the head slightly elevated to facilitate venous and cerebral spinal fluid (CSF)
drainage from the surgical site. However, superior sagittal pressures decreases
with increasing head elevation, and this increases the likelihood of VAE [14].
Fig. 3. Sitting position. The sitting position affords optimal chest wall compliance in children with
respiratory disease and obesity.
Table 2
Physiologic effects of patient positioning
Position Physiological effect
Head-elevated Enhanced cerebral venous drainage
Decreased cerebral blood flow
Increased venous pooling in lower extremities
Postural hypotension
Head-down Increased cerebral venous and intracranial pressure
Decreased functional residual capacity (lung function)
Decreased lung compliance
Prone Venous congestion of face, tongue, and neck
Decreased lung compliance
Increased abdominal pressure can lead to venocaval compression
Lateral decubitus Decreased compliance of down-side lung
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404 395

Extreme head flexion can cause brainstem compression in patients with posterior
fossa pathology, such as mass lesions or an Arnold-Chiari malformation.
Extreme rotation of the head can impede venous return through the jugular
veins and lead to impaired cerebral perfusion, increased intracranial pressure,
and cerebral venous bleeding.
Postoperative management
Close observation in an intensive care unit with serial neurologic examinations
and invasive hemodynamic monitoring is helpful for the prevention and early
detection of postoperative problems. Respiratory dysfunction is the leading
complication after posterior fossa craniotomies [16]. Airway edema is usually
self-limited, and may require endotracheal intubation as a stent. Occasionally,
ischemia or edema of the respiratory centers in the brainstem will interfere with
respiratory control and lead to postoperative apnea. Children with Chiari
malformations may be more prone to the respiratory depression [17]. Diabetes
insipidus can occur after surgery in the region of the hypothalamus and pituitary
gland, and can be managed acutely with an intravenous vasopressin infusion.
Postoperative nausea and vomiting can cause sudden rises in intracranial
pressure, and should be treated with a nonsedating antiemetic. However,
prophylactic administration of ondansteron during surgery is not effective in
decreasing the incidence of vomiting following craniotomies in children [18].
Fig. 4. Prone infant. Lateral rolls are used to elevate the infant and minimize thoracic and
abdominal pressure.
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404396

Clinical approaches
Neonatal emergencies
Most neonatal surgery is performed on an emergent basis [19], and there is more
than a 10-fold increase in perioperative morbidity and mortality in neonates when
compared with other pediatric age groups [2]. In addition to existing congenital
heart defects, congestive heart failure can occur in neonates with large cerebral
arteriovenous malformations, and this condition requires aggressive hemodynamic
support. Management of the neonatal respiratory system may be difficult because
of the diminutive size of the airway, craniofacial anomalies, laryngotracheal
lesions, and acute (hyaline membrane disease, retained amniotic fluid) or chronic
(bronchopulmonary dysplasia) disease. Because these conditions are in a state of
flux, they should be addressed preoperatively to minimize morbidity.
The neonatal central nervous system is capable of sensing pain and
mounting a stress response after a surgical stimulus [20]. However, neonatal
myocardial function is particularly sensitive to both inhaled and intravenous
anesthetics, and the use of these agents needs to be judicious to block surgical
stress without causing myocardial depression. An opioid-based anesthetic is
generally the most stable hemodynamic technique for neonates. The hepatic and
renal systems are also not fully developed, and neonates anesthetized with a
narcotic technique will often have delayed emergence and may require post-
operative mechanical ventilation.
Closure of a myelomeningocele or encephalocele presents special problems.
Positioning the patient for tracheal intubation may rupture the membranes
covering the spinal cord or brain. Therefore, careful padding of the lesion
(Fig. 5), and in some cases intubation of the neonate’s trachea in the left lateral
decubitus position, may be necessary. Most surgical closures of simple myelo-
meningoceles have relatively minimal blood loss. However, large lesions may
requirement significant undermining of cutaneous tissue to cover the defect and
pose larger risks for blood loss and hemodymanic instability. Recent advances in
the management of myelomeningoceles have lead to early intervention into the
intrauterine period [21]. The management of the fetus and mother during fetal
surgery has been reviewed extensively elsewhere [22,23].
Hydrocephalus
The most common neurosurgical procedure performed in major pediatric
centers is for the management of hydrocephalus. Regardless of the etiology,
whether it be overproduction of CSF due to choroid plexus papillomas or
obstruction of CSF flow secondary to a tumor or Chiari malformation, diagnosis
and alleviation of life-threatening intracranial hypertension should proceed
expeditiously. The mental status of the child should dictate the anesthetic
management as noted above, and intracranial hypertension can be managed
with hyperventilation and diuretics. Most neonates undergoing a closure of a
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404 397

myelomeningocele are potential candidates for a ventriculo-peritoneal shunt
(VPS), and may have both procedures performed in one sitting. The long-term
management of hydrocephalus with VPS invariably increases the incidence of
mechanical failure and shunt infections. Should the peritoneum be infected,
alternate sites for the drainage limb of these extracranial shunts include the right
atrium and pleural cavity.
Craniosynostosis
Repairs of craniosynostosis are likely to have the best result if done early in
life [24]. However, these procedures are associated with loss of a significant
percentage of an infant’s blood volume, with great losses occurring when more
Fig. 5. Positioning of a neonate with a myelomeningocele. (A) Prior to induction of general anesthesia,
the neonate is elevated on a soft padding with a center cutout to relieve pressure on the
myelomeningocele. (B) Positioning of the neonate for closure of the myelomeningocele.
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404398

sutures are involved [25]. Venous air embolism detected by echocardiography
and precordial Doppler occurred in 66% to 83% of craniectomies in infants
[25,26]. Fortunately, direct morbidity and mortality rarely occur. Venous air
emboli can be minimized by early detection with continuous precordial Doppler
ultrasound and maintaining euvolumia. When hemodynamic instability does
occur, the operating table can be placed in the Trendelenburg position, flooding
the surgical field with warm saline and sealing the sites of egress with bone wax
and direct pressure. These maneuvers will augment the patient’s blood pressure
and prevent further entrainment of intravascular air.
Tumors
Because the majority of intracranial tumors in children occurs in the posterior
fossa, CSF flow is often obstructed, and intracranial hypertension and hydro-
cephalus is often present. Most neurosurgeons approach this region with children
in the prone position. The patient’s head is often secured with a Mayfield head
frame. Pins used in small children can cause skull fractures, dural tears, and
intracranial hematomas. Elevation of the bone flap can tear the transverse and
straight sinuses, and massive blood loss and/or VAE can occur. Surgical resection
of tumors in the posterior fossa can also lead to brainstem and/or cranial nerve
damage. Sudden changes in blood pressure and heart rate may be sentinel signs
of encroachment on these structures. Damage to the respiratory centers and
cranial nerves can lead to apnea and airway obstruction after extubation of the
patient’s trachea. Children requiring stereotactic-guided radiosurgery or craniot-
omies need general anesthesia to tolerate the procedures. Special head frames
have been devised to allow airway manipulations, and should be used in these
patients [27].
Epilepsy
Surgical treatment has become a viable option for many patients with
medically intractable epilepsy. Two major considerations should be kept in mind.
Chronic administration of anticonvulsant drugs, phenytoin and carbamazepine,
induces rapid metabolism and clearance of several classes of anesthetic agents
including neuromuscular blockers and opioids [9,28]. Therefore, the anesthetic
requirements for these drugs are increased, and require close monitoring of their
effect and frequent redosing. Intraoperative neurophysiologic monitors can be
used to guide the actual resection of the epileptogenic focus, and general
anesthetics can compromise the sensitivity of these devices [29].
Because some epileptogenic foci are in close proximity to cortical areas
controlling speech, memory, and motor or sensory function, monitoring of patient
and electrophysiologic responses are frequently utilized to minimize iatrogenic
injury to these areas [30,31]. Cortical stimulation of the motor strip in a child
under general anesthesia will require either EMG or direct visualization of muscle
movement. Neuromuscular blockade should not be used in this situation. Neural
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404 399

function is best assessed in an awake and cooperative patient. Awake cranioto-
mies in children can be accomplished with local anesthesia and propofol and
fentanyl for sedation and analgesia, respectively [32]. Positioning of the patient is
critical for success of this technique. The patient should be in a semilateral
position to allow both patient comfort as well as surgical and airway access to the
patient. Propofol does not interfere with the ECoG if it is discontinued 20 minutes
before monitoring. Highly motivated children older that 10 years of age were able
to withstand the procedure without incident. However, it is imperative that
candidates for an awake craniotomy be mature and psychologically prepared to
participate in this procedure. Therefore, patients who are developmentally
delayed or have a history of severe anxiety or psychiatric disorders should not
be considered appropriate for an awake craniotomy. Very young patients cannot
be expected to cooperate for these procedures, and usually require general
anesthesia with extensive neurophysiologic monitoring to minimize inadvertent
resection of the motor strip and eloquent cortex. Repeat craniotomies for removal
of ECoG leads and depth electrodes used for chronic invasive EEG monitoring
and subsequent resection of the seizure focus are at risk for expansion of residual
pneumocephalus. It is important to avoid nitrous oxide until the dura is opened,
because intracranial air can persist up to 3 weeks following a craniotomy [33].
Vascular
Vascular anomalies are rare in infants and children. Most of these conditions
are congenital anomalies, and present early in life. Large arteriovenous malfor-
mations (AVM) in neonates may be associated with high output congestive heart
failure and require vasoactive support. Initial treatment of large AVMs often
consists of intravascular embolization in the radiologic suite [34]. Operative
management is commonly associated with massive blood loss, and these patients
require several i.v. access sites and invasive hemodynamic monitoring. Ligation
of an AVM can lead to sudden hypertension with hyperemic cerebral edema
[35]. Vasodilators such as labetalol or nitroprusside can be used to control a
hypertensive crisis.
Moyamoya syndrome is a rare chronic vaso-occlusive disorder of the internal
carotid arteries that presents as transient ischemic attacks and/or recurrent strokes
in childhood. The etiology is unknown, but the syndrome can be associated with
prior intracranial radiation, neurofibromatosis, Down’s syndrome, and a variety
of hematological disorders. The anesthetic management of these patients is
directed at optimizing cerebral perfusion by maintaining euvolumia and the
blood pressure within the patient’s preoperative levels [36]. Maintenance of
normocapnia is also essential in patients with Moyamoya syndrome because both
hyper- and hypocapnia can lead to stealing phenomenon from the ischemic region
and further aggravate cerebral ischemia [37]. A nitrous oxide and narcotic-based
anesthetic provides a stable level of anesthesia for these patients, and are
compatible with intraoperative EEG monitoring. Once the patient emerges from
anesthesia, the same maneuvers that optimize cerebral perfusion should be
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404400

extended into the postoperative period. These patients should receive i.v. fluids to
maintain adequate cerebral perfusion, and be given adequate narcotics to avoid
hyperventilation induced by pain and crying.
Trauma
Pediatric head trauma requires a multiorgan approach to minimizing mor-
bidity and mortality [38]. A small child’s head is often the point of impact in
injuries, but other organs can also be damaged. Basic life support algorithms
should be immediately applied to assure a patent airway, spontaneous respira-
tion, and adequate circulation. Immobilization of the cervical spine is essential
to avoid secondary injury with manipulation of the patient’s airway until
radiologic clearance is confirmed. Blunt abdominal trauma and long bone
fractures frequently occur with head injury, and can be major sources of blood
loss. To assure tissue perfusion during the operative period, the patient’s blood
volume should be restored with crystalloid solutions and/or blood products.
Ongoing blood loss can lead to coagulopathies, and should be treated with
specific blood components.
Infants with ‘‘Shaken Baby Syndrome’’ often present with a myriad of chronic
and acute subdural hematomas [39]. As with all traumatic events, the presence of
other coexisting injuries, fractures, and abdominal trauma should be identified.
Craniotomies for the evacuation of either epidural or subdural hematomas are at
high risk for massive blood loss and VAE. Postoperative management of these
victims is marked by the management of intracranial hypertension, and in the
most severe cases, determination of brain death.
Spine surgery
Spinal dysraphism is the primary indication for laminectomies in pediatric
patients. Many of these patients have a history of a meningomyelocele closure
followed by several corrective surgeries. These patients have been exposed to
latex products, and may develop hypersensitivity to latex. Latex allergy can
manifest itself by a severe anaphylactic reaction heralded by hypotension and
wheezing, and should be rapidly treated by removal of the source of latex, and
administration of fluid and vasopressors [40]. Patients at risk for latex allergy
should have a latex-free environment.
Tethered cord releases require EMG monitoring to help identify functional
nerve roots. EMG of the anal sphincter and muscles of the lower extremities is
performed intraoperatively to minimize inadvertent injury to nerves innervating
these muscle groups [41]. Muscle relaxation should be discontinued or antago-
nized to allow accurate EMG monitoring.
Neuroradiology
Recent advances in imaging technology have provided less invasive proce-
dures to diagnose and treat lesions in the CNS. Most neuroradiological studies
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404 401

such as CT scans and magnetic resonance imaging can be accomplished with
light sedation. Recommendations have been published by consensus groups of
anesthesiologists and pediatricians, and can serve as guidelines for managing
these patients [42,43]. General anesthesia is typically used for uncooperative
patients, patients with coexisting medical problems, and potentially painful
procedures such as intravascular embolization of vascular lesions [34].
Summary
The perioperative management of pediatric neurosurgical patients presents
many challenges to neurosurgeons and anesthesiologists. Many conditions are
unique to pediatrics. Thorough preoperative evaluation and open communication
between members of the health care team are important. A basic understanding of
age-dependent variables and the interaction of anesthetic and surgical procedures
are essential in minimizing perioperative morbidity and mortality.
References
[1] Pryds O. Control of cerebral circulation in the high-risk neonate. Ann Neurol 1991;30:321–9.
[2] Cohen MM, Cameron CB, Duncan PG. Pediatric anesthesia morbidity and mortality in the
perioperative period. Anesth Analg 1990;70:160–7.
[3] Morray JP, Geiduschek JM, Ramamoorthy C, et al. Anesthesia-related cardiac arrest in children:
initial findings of the Pediatric Perioperative Cardiac Arrest (POCA) Registry. Anesthesiology
2000;93:6–14.
[4] Nargozian CD. The difficult airway in the pediatric patient with craniofacial anomaly. Anes-
thesiol Clin North Am 1999;16:839–52.
[5] Boneva RS, Botto LD, Moore CA, Yang Q, Correa A, Erickson JD. Mortality associated with
congenital heart defects in the United States: trends and racial disparities, 1979–1997. Circu-
lation 2001;103:2376–81.
[6] McCann ME, Kain ZN. Management of perioperative anxiety in children. Anesth Analg 2001;
93;98–105.
[7] Rockoff MA, Goudsouzian NG. Seizures induced by methohexital. Anesthesiology 1981;54:
333–5.
[8] Todd MM, Warner DS, Sokoll MD, et al. A prospective, comparative trial of three anesthetics for
elective supratentorial craniotomy. Anesthesiology 1993;78:1005–20.
[9] Soriano SG, Kaus SJ, Sullivan LJ, et al. Onset and duration of action of rocuronium in children
receiving chronic anticonvulsant therapy. Paediatr Anaesth 2000;10:133–6.
[10] Soriano SG, Sullivan LJ, Venkatakrishnan K, et al. Pharmacokinetics and pharmacodynamics of
vecuronium in children receiving phenytoin or carbamazepine for chronic anticonvulsant ther-
apy. Br J Anaesth 2001;86:223–9.
[11] Scheingraber S, Rehm M, Sehmisch C, et al. Rapid saline infusion produces hyperchloremic
acidosis in patients undergoing gynecologic surgery. Anesthesiology 1999;90:1265–70.
[12] Soriano SG, McManus ML, Sullivan LJ, et al. Cerebral blood flow velocity after mannitol
infusion in children. Can J Anaesth 1996;43:461–6.
[13] McManus ML, Soriano SG. Rebound swelling of astroglial cells exposed to hypertonic man-
nitol. Anesthesiology 1998;88:1586–91.
[14] Grady MS, Bedford RF, Park TS. Changes in superior sagittal sinus pressure in children with
head elevation, jugular venous compression, and PEEP. J Neurosurg 1986;65:199–202.
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404402

[15] Soriano SG, McManus ML, Sullivan LJ, et al. Doppler sensor placement during neurosurgical
procedures for children in the prone position. J Neurosurg Anesthesiol 1994;6:153–5.
[16] Meridy HW, Creighton RE, Humphreys RB. Complications during neurosurgical procedures in
the prone position. Can J Anaesth 1974;21:445–52.
[17] Waters KA, Forbes P, Morielli A, et al. Sleep-disordered breathing in children with myelome-
ningocele. J Pediatr 1998;132:672–81.
[18] Furst SR, Sullivan LJ, Soriano SG, et al. Effects of ondansetron on emesis in the first 24 hours
after craniotomy in children. Anesth Analg 1996;83:325–8.
[19] Koka BV, Soriano SG. Anesthesia for neonatal surgical emergencies. Semin Anesthes 1992;9:
309–16.
[20] Anand KJ, Hickey PR. Pain and its effects in the human neonate and fetus. N Engl J Med 1987;
317:1321–9.
[21] Sutton LN, Sun P, Adzick NS. Fetal neurosurgery. Neurosurgery 2001;48:124–42.
[22] Gaiser RR, Kurth CD. Anesthetic considerations for fetal surgery. Semin Perinatol 1999;23:
507–14.
[23] O’Hara IB, Kurth CD. Anesthesia for fetal surgery. In: Greeley WJ, editor. Pediatric anesthesia.
Philadelphia: Churchill Livingstone; 1999. p. 15.1–15.11.
[24] Shillito J Jr. A plea for early operation for craniosynostosis. Surg Neurol 1992;37:182–8.
[25] Faberowski LW, Black S, Mickle JP. Incidence of venous air embolism during craniectomy for
craniosynostosis repair. Anesthesiology 2000;92:20–3.
[26] Harris MM, Yemen TA, Davidson A, et al. Venous embolism during craniectomy in supine
infants. Anesthesiology 1987;67:816–9.
[27] Stokes MA, Soriano SG, Tarbell NJ, et al. Anesthesia for stereotactic radiosurgery in children.
J Neurosurg Anesthesiol 1995;7:100–8.
[28] Tempelhoff R, Modica PA, Spitznagel EL. Anticonvulsants therapy increases fentanyl require-
ments during anaesthesia for craniotomy. Can J Anaesth 1990;37:327–32.
[29] Eldredge EA, Soriano SG, Rockoff MA. Neuroanesthesia. In: Adelson PD, Black PM, editors.
Surgical treatment of epilepsy in children. Philadelphia: W.B. Saunders; 1995. p. 505–20.
[30] Black PM, Ronner SF. Cortical mapping for defining the limits of tumor resection. Neurosurgery
1987;20:914–9.
[31] Penfield W. Combined regional and general anesthesia for craniotomy and cortical exploration.
Part I. Neurosurgical considerations. Anesth Analg 1954;33:145–55.
[32] Soriano SG, Eldredge EA, Wang FK, et al. The effect of propofol on intraoperative electro-
corticography and cortical stimulation during awake craniotomies in children. Paediatr Anaesth
2000;10:29–34.
[33] Reasoner DK, Todd MM, Scamman FL, et al. The incidence of pneumocephalus after supra-
tentorial craniotomy. Observations on the disappearance of intracranial air. Anesthesiology 1994;
80:1008–12.
[34] Burrows PE, Robertson RL. Neonatal central nervous system vascular disorders. Neurosurg Clin
North Am 1998;9:155–80.
[35] Morgan MK, Sekhon LH, Finfer S, et al. Delayed neurological deterioration following resection
of arteriovenous malformations of the brain. J Neurosurg 1999;90:695–701.
[36] Soriano SG, Sethna NF, Scott RM. Anesthetic management of children with moyamoya syn-
drome. Anesth Analg 1993;77:1066–70.
[37] Kuwabara Y, Ichiya Y, Sasaki M, et al. Response to hypercapnia in moyamoya disease. Cere-
brovascular response to hypercapnia in pediatric and adult patients with moyamoya disease.
Stroke 1997;28:701–7.
[38] Lam WH, MacKersie A. Paediatric head injury: incidence, aetiology and management. Paediatr
Anaesth 1999;9:377–85.
[39] Duhaime AC, Christian CW, Rorke LB, et al. Nonaccidental head injury in infants—the
‘‘shaken-baby syndrome.’’ N Engl J Med 1998;338:1822–9.
[40] Holzman RS. Clinical management of latex-allergic children. Anesth Analg 1997;85:529–33.
[41] Legatt AD, Schroeder CE, Gill B, et al. Electrical stimulation and multichannel EMG recording
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404 403

for identification of functional neural tissue during cauda equina surgery. Childs Nerv Syst 1992;
8:185–9.
[42] American Academy of Pediatrics Committee on Drugs. Guidelines for monitoring and manage-
ment of pediatric patients during and after sedation for diagnostic and therapeutic procedures.
Pediatrics 1992;89:1110–5.
[43] American Society of Anesthesiologists. Practice guidelines for sedation and analgesia by non-
anesthesiologists. A report by the American Society of Anesthesiologists Task Force on Sedation
and Analgesia by Non-Anesthesiologists. Anesthesiology 1996;84:459–71.
S.G. Soriano et al. / Anesthesiology Clin N Am 20 (2002) 389–404404

Major spine surgery
Patricia H. Petrozza, MDNeuroanesthesia Department of Anesthesiology (Section on Neuroanesthesia),
Wake Forest University School of Medicine, Medical Center Boulevard,
Winston-Salem, NC 27157-1009, USA
Rheumatoid arthritis
The cervical spine undergoes inflammatory and erosive changes in a sub-
stantial portion of patients with rheumatoid arthritis. It is estimated that as many
as 80% of patients with rheumatoid arthritis who manifest the condition for more
than 10 years time have cervical spine involvement [1]. Systemically, this disease
is characterized by inflammatory changes in the connective tissue of the patient’s
body. Chronic proliferative inflammation affects synovial membranes, producing
irreversible damage to joint capsules and articular cartilage. A rheumatoid
pannus refers to an inflammatory exudate overlying the lining layer of synovial
cells within a joint, but this term also may be used to demarcate an inflammatory
mass of fibrous tissue resulting from synovial joint degeneration. Erosion
occurring in cartilage and bone, together with infiltration and disruption of
supporting ligaments, leads to anatomic destruction of multiple joints with
subsequent malalignment.
More than 80% of all rheumatoid disease in the cervical spine is found at the
affected level of C1–C2 [2]. Most commonly, the body of C1 slips forward on
C2 as the vertebrae become malaligned. Destruction of the atlanto-occipital and
the atlanto-axial joints leads to loss of height of the lateral masses of C1 and
subsequent upward subluxation of the odontoid process through the foramen
magnum. This condition is termed vertical subluxation.
It is important to remember that normal vertebral alignment does not
necessarily correlate with the absence of spinal cord compression, especially at
C1–C2, where there may be a large mass of fibrous or inflammatory tissue (a
pannus) replacing or lying adjacent to the odontoid process. In a magnetic
resonance imaging (MRI) study, the posterior atlanto-dens interval (PADI) is an
important measurement. The PADI is the distance between the posterior cortex of
the odontoid and the nearest point on the posterior arch of the atlas. This distance
has been found to correlate with the presence and severity of myelopathy.
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00009 -8
E-mail address: [email protected] (P.H. Petrozza).
Anesthesiology Clin N Am
20 (2002) 405–415

Commonly, patients with spine involvement from rheumatoid arthritis com-
plain of midline cervical pain, occasionally referred to the trapezius or sub-
occipital areas. Sensory symptoms include paresthesias, numbness, and loss of
proprioception in various combinations usually involving the upper limbs.
Progressive myelopathy is the clearest indication for surgical intervention, and
evidence is accumulating that better surgical results are obtained in patients who
are less severely affected neurologically and systemically at the time of surgery
[3]. Surgical intervention may be inappropriate for some patients in whom
neurologic deficits are severe and movement is restricted. In one series, only
15% of such severely symptomatic patients regained independent ambulation
after surgery [4].
Preoperative evaluation1
The anesthesiologist must be cognizant of the systemic nature of rheumatoid
arthritis. Often, patients are prone to malnutrition, anemia, and poor wound
healing. Particular attention must be addressed to the cardiovascular system, as
cardiovascular disease is the leading cause of death in the rheumatoid patient.
Myocardial infarction secondary to coronary arteritis has been reported. A
common manifestation of rheumatoid-related cardiovascular disorders is pericar-
dial disease, and up to 45% of patients with pericardial involvement may exhibit
no symptoms [5]. Following a careful review of the cardiovascular system and
physical examination, an echocardiogram may add significant information if
clinically indicated.
The respiratory system is also likely to become compromised in the patient with
long-standing rheumatoid arthritis. The patient may be subject to pleural disease,
nodules within the lungs, interstitial pulmonary fibrosis, and obliterative bron-
chiolitis. Occasionally, pulmonary vasculitis leads to pulmonary hypertension.
Additional physiologic systems that must be evaluated include the renal
system, where amyloidosis or vasculitis may result in impaired renal function.
Similarly, if hepatic tissue has been destroyed by the systemic vasculitis, patients
may manifest hypoalbuminemia and elevated hepatic transaminases. Therapeutic
agents such as nonsteroidal anti-inflammatory agents may cause hepatotoxicity
and increased enzyme levels of alkaline phosphatase [6]. Patients on chronic
steroids will most likely require perioperative supplementation, while drugs such
as penicillamine, methotrexate, and azathioprine have immunosuppressant prop-
erties, and may retard wound healing.
Assessment of the airway is one of the critical tasks for the anesthesiologist,
and the patient with rheumatoid arthritis is likely to present several challenges.
More than 50% of rheumatoid patients will have jaw symptoms at some time
during the course of their illness [5]. Clinicians should palpate the temporoman-
dibular joint for tenderness and ascertain the extent of mouth opening.
1 The report by Matti and Sharrock [5] is the source for much of the discussion here on
preoperative evaluation in the rheumatoid patient.
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415406

Cricoarytenoid joint arthritis is a frequent finding in patients with rheumatoid
arthritis, and laryngeal involvement is common (59%) in patients with classic
symptoms [7]. Extrathoracic airway obstruction is also reported. Signs and
symptoms should be sought including hoarseness, shortness of breath or
wheezing, and dysphasia. Involvement of the cricoarytenoid joint with synovitis
maybe asymptomatic, allowing aspiration of pharyngeal contents, while severe
arthritis diminishes the mobility of the vocal cords and may result in narrowing of
the glottic opening so markedly that laryngeal obstruction and stridor result. If the
anesthesiologist’s suspicions are aroused by the preoperative assessment, evalu-
ation by an otolaryngologist is indicated.
Much of the previously mentioned pathologic lesions of the cervical spine are
of interest in a discussion of airway management. For instance, in patients with
atlanto-axial involvement, excessive flexion may cause cord compression. This
may be exaggerated if the odontoid process is unstable and migrates rostrally.
Patients with subaxial involvement (subluxation below C2) experience spinal
cord compromise with extension. Laryngeal deviation has also be noted in a
number of rheumatoid patients. The larynx may be angulated anteriorly, or
displaced caudally as well as rotated to the right or to the left. This angulation
may present difficulties with airway equipment like the laryngeal mask airway
[5]. Most often, for procedures involving the cervical spine, a carefully performed
fiberoptic intubation is preferred.
Intraoperative management
In many cases anterior subluxation of C1 on C2 can be corrected by extension
of the cervical spine, which results in better alignment. Posterior fixation and
fusion in this position are often sufficient. Careful perioperative imaging
examination [5] are necessary, however, to be certain that even with normal
vertebral realignment, soft tissue does not compress the spinal cord, necessitating
a direct decompression by an anterior approach.
Removal of the odontoid process leads to significant instability in most patients
with cervical rheumatoid disease and, consequently, a stabilization procedure fol-
lowing decompression is necessary. When vertical odontoid subluxation occurs,
access to this fragment can be obtained through a transoral-transpharyngeal route.
Often a tracheostomy may be necessary, although the highly motivated patient will
be able to tolerate endotracheal intubation for approximately 48 hours postoper-
atively to allow healing of the pharyngeal incision. If the surgeon suspects a breach
of the dura during odontoid resection, a lumbar cerebrospinal fluid (CSF) drain
may prevent formation of a significant CSF fistula.
Following anterior decompression of the upper cervical spine, often the patient
is placed prone for stabilization of the posterior spinal elements. Proper intra-
operative positioning is assured while the surgeon controls the head and neck.
Somatosensory evoked potential monitoring is often useful as instrumentation is
placed for fusion. Because the spinal cord is known to be compromised, direct
arterial pressure measurement through an arterial line is recommended, and the
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415 407

anesthesiologists should remain vigilant for blood loss, as occasionally the cervical
spine anatomy may be difficult and the vertebral arteries displaced [8].
As imaging of spinal column pathology in patients with rheumatoid arthritis
becomes more sophisticated, operations can be performed that are more likely
tailored to each patient’s specific pathology. Certainly, patients with fewer
systemic manifestations of the illness tend to have better outcomes, and many
patients who undergo posterior fusion procedures at C1–C2 exhibit good pain
relief despite the fact that often bone fusion at least by radiographic measures is
incomplete [1]. These patients will continue to present interesting challenges for
neurosurgeons and anesthesiologists in the decades to come.
Metastatic tumors of the spine
Metastatic tumors occur three to four times more frequently than primary
neoplasms within the vertebral column, and solitary vertebral lesions are often
metastatic. The four most common primary sites for the origin of tumors are the
breast, lung, prostate system, and hematopoietic system, and these sites account
for one half to two thirds of all causes of neoplastic cord compression [9].
Seventy percent of metastatic cord compression involves the thoracic segments of
the spine, while the lumbosacral segments and cervical segments are each
involved 15% of the time. Prognosis is affected by the tumor biology, pretreat-
ment neurologic status, and the choice of therapy.
Magnetic Resonance Imaging (MRI) scanning is extremely sensitive for
metastatic bone disease, and spinal CToften provides complimentary information.
In patients with hypervascular tumors, such as those related to metastatic kidney
and thyroid neoplasms, spinal angiography may be indicated to decrease tumor
vascularity and to locate critical spinal arterial supplies. Presurgical embolization
often reduces surgical morbidity [10].
A treatment plan must be individualized based on the patient’s general
condition, extent of cancer, type of tumor, and the degree and speed of onset
of neurologic deficit. Tokuhashi and associates have proposed a scoring system
using six parameters: general condition, number of vertebral metastases, addi-
tional spine lesions, metastases to internal organs, primary site, and severity of
spinal palsy. A maximum score of 12 can be obtained with each parameter given
a score of 0 to 2 points. Excisional surgery may be indicated for a total score of 9
or more, whereas palliative surgery may be used for a score of 5 or less [11].
Until recently, laminectomy through a posterior approach was considered to be
the surgical treatment of choice for epidural metastatic tumors. Unfortunately,
laminectomy offers inadequate access to the anterior aspect of the cord and
vertebral body, and may subject the patient to loss of spinal column stability. A
posterior lateral approach may be useful if the tumor is soft and can be removed
by suction or curettage. This method is often a useful method of palliation in a
severely debilitated patient.
An anterior approach has become the most widely favored for decompression
of the patient with spinal metastases, because most tumors involve the vertebral
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415408

body and secondarily involve the posterior vertebral elements. Anterior decom-
pression of the spinal cord by vertebral body resection (corpectomy) gives
superior results in terms of pain relief and recovery of neurologic function
compared with posterior laminectomy [12]. Following tumor resection, stabi-
lization requiring instrumentation is most frequently indicated to maintain spinal
alignment and prevent progressive deformity.
Although pain is the initial symptom of metastatic disease in the spine, it is
often difficult to make the exact diagnosis because the pain may be nonspecific or
referred to other sites. Often neurologic signs become common by the time of
diagnosis and these include various degrees of muscle weakness, bowel and
bladder dysfunction, and sensory symptoms. When patients begin to demonstrate
motor signs, 28% become paraplegic in less than 24 hours [13]. Early diagnosis is
crucial, as outcome depends on neurologic function before treatment.
Preoperative evaluation and assessment
Most operations for resection of tumors located anterior to the spinal cord are
performed in the thoracic spine. A thoracotomy is required, and preoperative
spirometry may be helpful. An arterial blood gas obtained prior to anesthesia will
likely aid postoperative pulmonary care, and a preoperative regimen of broncho-
dilators and nebulizing treatments often optimizes the patient’s condition for
surgery. An assessment of the patient’s coagulation status as well as platelet count
is important in planning intraoperative care, and at least 4 units of packed red
blood cells should be available at the start of surgery.
Intraoperative management
A double lumen endotracheal tube optimizes surgical exposure of the spine,
particularly in the thoracic region. A fiberoptic bronchoscope is required after the
patient is placed in the lateral position to verify endotracheal tube placement and
promote optimal lung isolation. If a patient’s cardiopulmonary status makes
single-lung ventilation inadequate, insufflation of oxygen or application of low
levels of continuous positive airway pressure to the deflated lung can often
maintain oxygenation.
Blood loss may be substantial, particularly during the tumor debulking, and
intra-arterial access for blood samples and a continuous monitor of mean arterial
blood pressure is necessary, while central venous pressure or pulmonary artery
pressure measurements may be advantageous for patients with cardiovascular
compromise. Optimally, the anesthetic technique should assure stable spinal cord
perfusion, appropriate monitoring, and assessment of the patient’s neurologic
status early in the recovery period.
A deflatable ‘‘bean bag’’ helps stabilize the torso as the patient is positioned
on his or her side. An axillary roll will be necessary to protect the brachial
nerve vascular bundle from compromise, and the arm on the side of the incision
must be carefully padded and positioned to allow access to the upper thoracic
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415 409

cage. Excessive lateral neck flexion should be avoided, as postoperative
congestion with significant neck pain may be a cause of patient morbidity.
Additionally, the common peroneal nerve of the dependent leg must be pro-
tected from pressure ischemia.
During decompressive surgery blood loss from epidural veins in the tumor bed
is often quite profuse. Frequent measurements of platelet count, coagulation
factors, and assessment of hemostasis by the surgical team will be necessary to
detect a dilutional coagulopathy and guide factor therapy. Transfusion-sparing
techniques such as the ‘‘cell saver’’ are not options when dealing with oncologic
surgery. As tumor resection often involves a vertebral body corpectomy, the patient
will require stabilization with spinal instrumentation to replace the vertebral body/
bodies and allow maximum rehabilitation in the postoperative period.
Postoperative care
Spinal decompressive surgery for metastatic tumors is often lengthy (in excess
of 8 hours). Common postoperative problems include hypothermia, coagulo-
pathy, residual pulmonary insult, and pain. Intravenous antibiotics are continued,
and perioperative dexamethasone is tapered. Drains are removed over time, and
most patients remain ventilated for 12 to 24 hours postoperatively. Sedation may
be obtained with mixtures of midazolam and fentanyl intravenously. Chest
physiotherapy (PT) is initiated, and careful postoperative fluid balance is
achieved. Pain is often managed with patient-controlled analgesia.
Surgical mortality rates after vertebral body resection range from 4% to 8%,
while the risk of neurologic deterioration as a result of a surgery occurs in 2% to
6% of patients [14]. Obviously, the use of modern and novel surgical techniques
for spinal decompression and stabilization must be balanced against the indi-
vidual patient’s overall prognosis for an improved quality of life.
Lumbar interbody fusion
Spondylolisthesis, trauma, and congenital abnormalities of the lumbar spine
predispose the spine to abnormal motion of the vertebral elements and supporting
structures resulting in neurologic deficits, deformity, and pain. Pain may continue
following one or more surgical procedures, and MRI demonstrates loss of disk
space, but no gross deformities of the motion segments such as the spinal facet
joints. Procedures that are designed to strengthen the unstable vertebral segments
with fusion are offered to limit motion within the spine and treat pain. Recent
studies have demonstrated improved functional outcomes in patients who
underwent posterior lateral lumbar fusion with or without instrumentation [15].
It appears that lumbar interbody fusion operations will continue to increase, while
instrumentation becomes more sophisticated.
Posterior lumbar interbody fusion techniques use corticocancellous bone strips
with or without pedicle screw instrumentation to achieve spine stability. The
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415410

posterior approach involves many challenges for the anesthesiologist and
surgeon. The patient must be positioned carefully in the prone position while
avoiding compression of the epidural veins. Bone dissection is quite lengthy, and
both arterial and venous bleeding may be problematic. Fluoroscopy is necessary
to facilitate placement of an interbody fixation or ‘‘pedicle’’ screw support.
Briefly, the approach to the lumbar spine involves extensive dissection so that
instrumentation can be placed through the interbody space with minimal
retraction of the spinal elements or nerve roots. Fusion is facilitated by multiple
types of fluoroscopically placed instrumentation including BAK and Ray cages,
or allograft bone dowels. Blood loss correlates with the number of vertebral
levels, which are instrumented as dissection is extensive.
Corticocancellous bone fusion was the initial method offered to achieve
stability in patients with ‘‘failed back syndrome,’’ but several new interbody
methods have been developed that show promise. These types of instruments are
simultaneously osteoconductive and stabilizing, and utilize approaches that are
often less invasive. For instance, using an anterior approach with BAK (Salzer-
SpineTech, Minneapolis, MN) fusion cages, neurologic complications occurred
in 2% of cases [16]. If the instrumentation is inserted through a direct anterior
approach, there is an approximately 2% incidence of permanent retrograde
ejaculation in men, which may lead to sterility [17]. This complication is thought
to be related to dissection of the sacral plexus near the disk space. Despite this
complication, implants and bone dowels combined with the anterior approach
have several advantages. Often patients achieve very good postoperative pain
relief because of the large amount of disk space distraction achieved with
instrumentation and implants. Also, an external rigid orthosis is not necessary,
and hospital costs are reportedly reduced compared with a 360� fusion [18].
Some central disk fragments may also be removed through an anterior approach
if necessary.
In general, the operative approach for an anterior lumbar interbody fusion
requires a second general or vascular surgeon to collaborate with the neuro-
surgeon. The patient undergoes a bowel preparation protocol the night before
surgery, and is placed supine upon an imaging compatible operating room table
such that both anterior-posterior (AP) and lateral images can be obtained through
the lumbar spine. Monitoring includes an arterial line, large bore venous access,
and Foley catheter. Occasionally, fusion bone may be obtained from the posterior
iliac crest with the patient lying in the lateral decubitus position prior to making
the abdominal incision. Infiltrating morphine locally may help with postoperative
pain from the bone donor site [19].
A left-sided paramedian incision is used to expose the spine. Peritoneum and
abdominal contents are retracted to the patient’s right, and the sigmoid colon is
retracted to the patient’s left. Dissection continues in the retroperitoneal plane.
Several structures are encountered, including the middle sacral vessels and
sympathetic nerves as well as left iliac vein and left gluteal vein on an approach
to the L4–L5 disk space. Anterior exposure is not recommended above the L3 to
L4 disk space due to the presence of large aortic branch vessels.
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415 411

Once the proper spinal level has been identified byAP fluoroscopy, approximate
implant size and spacing are determined by a preoperative templating process.
Large-diameter implants are utilized to give maximal distraction and at least 3 mm
of penetration into both vertebral bodies. If it is necessary to remove fragments in
the spinal canal, an operating microscope may be used to perform a discectomy
through one of the access holes created by retractors while others are left in place to
maintain separation of the vertebral bodies. Patients are most likely extubated
immediately following surgery, mobilized the next day, and despite minor levels of
bowel dysfunction generally have a smooth postoperative course [16].
A laparoscopic method has been developed for an anterior lumbar interbody
fusion that has the advantage of reducing morbidity related to movement of the
abdominal contents and trauma to the abdominal wall. Due to the large amount of
vascular structures overlying the L4–S1 lumbar spine anteriorly, this approach
requires quite a bit of experience and tutelage under a laparoscopic surgeon, and
can only be offered to patients in whom a preoperative MRI does not show large
vessels overlying the disk space.
A common technique utilizes four portals for installation of carbon dioxide
and placement of the laparoscopic instrument and retractors. The patient is placed
in the Trendelenburg position, which often helps to mobilize the small intestines,
and sigmoid colon. Regan and colleagues recently reported on 240 consecutive
patients who underwent laparoscopic-instrumented interbody fusion and com-
pared these patients to a cohort of 591 consecutive patients who underwent open
anterior fusion with the same device [20]. In general, the laparoscopy group had
shorter hospital stays and reduced blood loss, but increased operative time.
Operative time decreased as the surgeon’s experience increased, but overall still
totalled approximately 1 hour longer for the laparoscopic anterior approach as
opposed to the open anterior approach. Blood loss was significantly less, totaling
approximately 207 cc for the anterior approach versus 41.7 cc for the laparo-
scopic approach. The operative complications were comparable in both groups,
and it was necessary to convert to an open procedure in the laparoscopy group
approximately 10% of the time.
Spinal instrumentation and techniques for fusion will no doubt continue to
evolve. In patient groups reported to the Food and Drug Administration under
prospective trials, titanium cages have shown high rates of apparent fusion.
Almost half of the eligible patients returned to work [21].
Visual loss after spine surgery
According to a report filed recently with the American Society of Anesthesi-
ologists Closed Claim Project, claims for postoperative blindness appear to be
rising [22]. Although the incidence of this concern has been reported to occur
with all types of surgery, a recent study on spine surgery patients gave the
incidence as 0.2%. This is approximately 10 times the risk of eye injury as after
other nonocular surgery [23].
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415412

The majority of lesions accounting for visual loss following surgery are
located within the optic nerve. Loss of central vision as well as loss of peripheral
visual fields can occur when this nerve sustains damage. Ischemic insult to the
optic nerve is separated into anterior ischemic optic neuropathy (AION) and
posterior ischemic optic neuropathy (PION). Each of these areas of the optic
nerve has a different blood supply and distinct predisposing factors that could
lead to infarction. Clinically, PION can be distinguished from AION by the
absence of acute disk swelling in PION.
The portion of the optic nerve, which involves the optic disk and the nerve
within the scleral canal, receives a blood supply from 8 to 10 small posterior ciliary
arteries that rise as branches from the ophthalmic artery. Posterior ciliary arteries
communicate with one another in the form of an incomplete anastomotic ring.
Often, the anastomotic ring is poorly developed so that downstream watershed
zones may form at the boundaries of areas supplied by specific posterior ciliary
artery branches. These zones may be vulnerable to ischemic nerve injury under
conditions of anemia, hypotension, and increases in venous pressure.
Postoperative AION often includes painless visual loss identified 1 or more
days following surgery [24]. Upon examination of the eye, disk edema will often
correlate with an area of field loss clinically. Ophthalmologic consultation should
be sought without delay, if the patient experiences new onset, postoperative
blindness, although vision loss may be permanent in this scenario.
PION presents with acute visual field loss similar to AION. This problem,
however, may develop more slowly than AION, and a symptom-free period may
precede the loss of vision [25]. Funduscopic examination will reveal no disk
swelling in PION. Blood supply to the posterior portion of the optic nerve arises
from branches of the ophthalmic artery, and the central retinal artery often sup-
plies branches to the central nerve fiber. At baseline, blood flow to the posterior
optic nerve is significantly less than that of the anterior portion. The segment of
the nerve most distal from the arterial supply is nourished primarily by readily
compressible centripetal pial vessels.
Ischemic optic neuropathy has been reported after spine procedures almost
exclusively in the prone position, and has most often been associated with lengthy
procedures involving multiple levels, long operative times, and significant blood
loss. Notable risk factors include pressure on the eye, hypotension, and anemia.
Meyer identified 37 patients who experienced visual loss after spine surgery
through a survey of members of the Scoliosis Research Society and a review of
the literature [26]. The patients had a mean age of 46.5 years. The average
operative time was 410 min, and blood loss was 3500 cc. Although most cases
had significant intraoperative hypotension (mean drop in systolic blood pressure
from 130 to 77 mmHg), comparison with a matched group of patients with no
visual symptoms showed no difference in the hematocrit or blood pressure
values. In his survey, Myers identified 37 patients, 8 or whom had AION, while
another 14 had PION.
Studies point to intraoperative hypotension and anemia as the most consistent
observations in patients developing postoperative ischemic optic neuropathy.
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415 413

Certain patient factors such as diabetes mellitus or hypertension may predispose
patients to inadequate delivery of blood to watershed perfusion zones. Addi-
tionally, the perfusion pressure of the anterior optic nerve is influenced by
arterial, venous, and intra-ocular pressures problems, each of which may be
exacerbated by the prone position. Concern over this very serious complication
has prompted the American Society of Anesthesiologists to develop a post-
operative visual loss registry, which will aid in establishing causes and circum-
stances of this particular problem.
It is not currently possible to specifically identify high-risk patients, and many
of the speculative factors that appear to be related to this complication are as yet
unproven in prospective trials. Certainly, efforts should be made to optimize
oxygen delivery and prevent tissue edema as well as increases in intraocular
pressure to assure adequate care of the visual system. Extremes of hemodilution
or hypotension should most likely be avoided, and consideration should be given
to staging very long planned operative procedures. An early postoperative check
for vision should be included in the routine examination.
References
[1] Santavirta S, Konttinen YT, Laasonen E, et al. Ten-year results of operations for rheumatoid
cervical spine disorders. J Bone Joint Surg Br 1991;73:116–20.
[2] Mathews JA. Atlanto-axial subluxation in rheumatoid arthritis. A 5-year follow-up study. Ann
Rheum Dis 1974;33:526–31.
[3] Peppelman WC, Kaus DR, Donaldson WF III, et al. Cervical spine surgery in rheumatoid
arthritis: improvement of neurologic deficit after cervical spine fusion. Spine 1993;18:2375–9.
[4] Casey ATH, Crockard HA, Bland JM, et al. Surgery on the rheumatoid cervical spine for the
non-ambulant myelopathic patient—too much, too late? Lancet 1996;347:1004–7.
[5] Matti MV, Sharrock NE. Anesthesia on the rheumatoid patient. Rheum Dis Clin North Am
1998;24(1):19–34.
[6] MacKenzie CR, Sharrock NE. Perioperative medical considerations in patients with rheumatoid
arthritis. Rheum Dis Clin North Am 1998;24(1):1–17.
[7] Geterud A, Bake B, Berthelsen B, et al. Laryngeal involvement in rheumatoid arthritis. Acta
Otolaryngol 1991;111:990–8.
[8] Johnston RA, Borthwick JM. Surgical management of the rheumatoid cervical spine. In: Schmi-
dek HH, editor. Schmidek & Sweet operative neurosurgical techniques: indications, methods,
and results. Philadelphia: W.B. Saunders, Co.; 2000. p. 1808–21.
[9] Byrne TN. Spinal cord compression from epidural metastases. N Engl J Med 1992;327:614–9.
[10] Sundaresan N, Choi IS, Hughes JEO, et al. Treatment of spinal metastases from kidney cancer by
presurgical embolization and resection. J Neurosurg 1990;73:548–54.
[11] Tokuhashi Y, Matsuzaki H, Toriyama H, et al. Scoring system for the preoperative evaluation of
metastatic spine tumor prognosis. Spine 1990;15:1110–3.
[12] Siegal T, Siegal T. Surgical decompression of anterior and posterior malignant epidural tumors
compressing the spinal cord: a prospective study. Neurosurgery 1985;17:424–32.
[13] Barcena A, Lobato RD, Rivas JJ, et al. Spinal metastatic disease: analysis of factors determining
functional prognosis and the choice of treatment. Neurosurgery 1984;15:820–7.
[14] Siegal T, Siegal T. Surgical management of malignant epidural tumors compressing the spinal
cord. In: Schmidek HH, editor. Schmidek & Sweet operative neurosurgical techniques: indica-
tions, methods, and results. Philadelphia: W.B. Saunders, Co.; 2000. p. 2171–97.
[15] Fischgrund JS, Mackay M, Herkowitz HN, et al. Degenerative lumbar spondylolisthesis with
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415414

spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and
arthrodesis with and without spinal instrumentation. Spine 1997;22:2807–12.
[16] Harrington JF Jr, Friehs G, Epstein MH. Surgical management of segmental spinal instability.
In: Schmidek HH, editor. Schmidek & Sweet operative meurosurgical techniques: indications,
methods, and results. Philadelphia: W.B. Saunders, Co.; 2000. p. 2280–302.
[17] Antonacci MD, Eismont FJ. Neurologic complications after lumbar spine surgery. J Am Acad
Orthop Surg 2001;9:137–45.
[18] Hacker RJ. Comparison of interbody fusion approaches for disabling low back pain. Spine
1997;22:660–6.
[19] Reuben SS, Vieira P, Faruqi S, et al. Local administration of morphine for analgesia after iliac
bone graft harvest. Anesthesiology 2001;95:390–4.
[20] Regan JJ, Yuan H, McAfee PC. Laparoscopic fusion of the lumbar spine: minimally invasive
spine surgery. A prospective multicenter study evaluating open and laparoscopic lumbar fusion.
Spine 1999;24:402–11.
[21] Ray CD. Threaded titanium cages for lumbar interbody fusions. Spine 1997;22:667–80.
[22] Cut postoperative blindness risks. Anesth Malpractice Prevent 1999;4(12):89–93.
[23] Roth S, Thisted RA, Erickson JP. Eye injuries after nonocular surgery: a study of 60,965
anesthetics from 1988 to 1992. Anesthesiology 1996;85:1020–7.
[24] Williams EL, Hart WM Jr, Tempelhoff R. Postoperative ischemic optic neuropathy. Anesth
Analg 1995;80:1018–29.
[25] Rizzo JF III, Lessell S. Posterior ischemic optic neuropathy during general surgery. Am J Oph-
thalmol 1987;103:808–11.
[26] Myers MA, Hamilton SR, Bogosian AJ, et al. Visual loss as a complication of spine surgery.
a review of 37 cases. Spine 1997;22:1325–9.
P.H. Petrozza / Anesthesiology Clin N Am 20 (2002) 405–415 415

Anesthetic management of traumatic
brain injury
Eric Bedell, MD*, Donald S. Prough, MDDepartment of Anesthesiology, University of Texas Medical Branch, 301 University Blvd.,
Galveston, TX 77555-0591, USA
Traumatic brain injury (TBI) represents a significant health issue in the United
States, with rates of 175–300 per 100,000 per year and a death rate of 15 to 30
per 100,000, accounting for up to 56,000 deaths [1,2]. Although brain injury,
secondary to vehicular injury, was historically the most common form of TBI, in
the latter part of the twentieth century, gunshot wounds became the most common
form of fatal brain injury, surpassing motor vehicle accidents [3]. Between 1979
and 1992 in the United States, brain injury secondary to vehicular trauma
decreased from 11.4/100,000 to 6.6/100,000 persons (43%), while injury from
firearms increased from 7.7/100,000 to 8.5/100,000 (10%) [3]. Even with modern
diagnosis and treatment, the prognosis for the patient with TBI remains poor. In a
recent study of hypothermia as a treatment for acute brain injury, a mortality of
27% occurred in the control group [4]. Because of the prevalence of TBI, an
understanding of the management of this group of patients is vital to the modern-
day health care provider in general, and the clinical anesthesiologist specifically.
In head-injured patients, the concepts of primary and secondary brain injury must
be considered to correctly prioritize interventions. Primary brain injury, which is
the damage caused directly by the traumatic insult, can result from contusion of
the brain (either at the site of impact or distant from the impact site), shock wave
disruption, depressed bone fragments, vascular occlusion, expanding intracranial
masses (eg, epidural, subdural, or intraparenchymal hematomas) and other
mechanisms. This form of damage may require rapid induction of anesthesia to
facilitate surgical intervention. Secondary brain injury occurs after the primary
injury, often as a result of correctable or preventable causes such as hypotension,
hypoxemia, or intracranial hypertension, and may markedly influence outcome.
Care begins with a structured care team following an orderly treatment plan. A
neurosurgeon or trauma surgeon is usually the leader of the neurotrauma care
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00010 -4
* Corresponding author.
E-mail address: [email protected] (E. Bedell).
Anesthesiology Clin N Am
20 (2002) 417–439

team, which also may include anesthesiologists, intensivists, radiologists, radio-
logic technicians, laboratory personnel, general surgeons, and nursing personnel.
The actual care then provided depends upon the individual patient’s needs and the
resources available.
This article reviews concepts of anesthetic management for the patient with
TBI. The recommended approaches to management are based upon physiologic
and pharmacologic data. Whenever possible, specific recommendations will
be made. At other times, conflicting information will be presented for readers
to consider.
Evaluation and stabilization
Upon initial presentation, a patient with TBI is usually considered to be at risk
for increased intracranial pressure (ICP), but this probability and its treatment
cannot become the only concern of the health care team. In any trauma patient,
priority must be first given to general evaluation and stabilization, with particu-
lar attention to the ‘‘ABC’s’’ of airway, breathing, and circulation. Although
these activities will be discussed sequentially, they proceed concurrently in
most situations.
Initial evaluation includes a rapid review of all injuries and determination of
baseline vital signs and level of consciousness. The head injury may not be the
only injury, and other injuries, such as chest or abdominal wounds, may be life-
threatening. A primary survey of the undressed patient, both front and back, with
a careful search for associated injuries should be performed. In moving the
patient, manual in-line axial stabilization of the cervical spine should be used
because of the risk that cervical spine injury could accompany head injury (see
below). A baseline level of consciousness should be ascertained. The Glasgow
Coma Scale (GCS) is a useful tool for such evaluation (Table 1). Studies
comparing the association between long-term outcome and GCS scores after
TBI have demonstrated that a lower initial GCS score is associated with higher
morbidity and mortality (Table 2). Changes from the initial GCS score are im-
portant in following clinical progress.
After rapid evaluation, the team directs attention to primary resuscitation,
particularly to the maintenance and protection of an adequate airway. In comatose
patients, an artificial airway usually must be established. The airway must be
reevaluated frequently, as a secure airway can rapidly be compromised. The
second priority is to provide adequate oxygenation and ventilation. The third
priority is to ensure the adequacy of circulation (including adequate peripheral
venous access and, if necessary, central venous or arterial access). Only after
addressing the ABCs should further care occur. The status of the ABC’s must be
reviewed frequently to recognize and reverse deterioration.
When a trauma patient first presents for care, an individual (or group) should
be assigned to assess the airway. The decision to provide an artificial airway (ie,
intubate or perform a tracheostomy) can be difficult and can have long-term
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439418

implications for management. It is important to appreciate the difference between
airway maintenance and airway protection. Airway maintenance means providing
an unobstructed pathway for gas flow between the atmosphere and the terminal
alveoli. Airway protection means either the ability to recognize and overcome
compromise within the airway (eg, tongue, vomitus, or pharyngeal secretions) or
the presence of a patent mechanical airway.
When evaluating the adequacy of the natural airway, quickly assess the level
of consciousness, examine the face and oropharynx for signs of injury or
obstruction, determine the presence or absence of bilateral breath sounds,
carefully examine for signs of airway obstruction (eg, stridor, retractions,
abdominal rocking), and establish the adequacy of arterial oxygenation using
pulse oximetry or arterial blood gas analysis. Also note vital signs (heart rate,
respiratory depth and frequency, blood pressure, temperature), review skin color,
and provide supplemental oxygen by means of a transparent, non-rebreathing
Table 2
Relationship of acute Glasgow Coma Scale (GCS) score to Glasgow Outcome Scale
Number (%) of cases
GCS score 3–4 GCS score 5–6 GCS score 7–9 Total cases
Dead/PVS 15 (78.9%) 19 (45.2%) 9 (25.7%) 43
SD/MD/GR 4 (21.2%) 23 (54.8%) 26 (74.3%) 53
Total cases 19 42 35 96
Abbreviations: The Glasgow Outcome Scale consists of five categories: death; PVS, persistent
vegetative state; SD, severe disability; MD, moderate disability; GR, good recovery.
From Jaggi JL, Obrist WD, Gennarelli TA, Langfitt TW. Relationship of early cerebral blood flow and
metabolism to outcome in acute head injury. J Neurosurg 1990;72:176–182 [113]; with permission.
Table 1
Glasgow coma scale (GCS)
Component Response Score
Eye opening Spontaneously 4
To verbal command 3
To pain 2
None 1
Motor response (best limb) Obeys verbal command 6
Localizes pain 5
Flexion withdrawal 4
Flexion (decortication) 3
Extension (decerebration) 2
No response (flaccid) 1
Best verbal response Oriented and converses 5
Disoriented and converses 4
Inappropriate words 3
Incomprehensible sounds 2
No verbal response 1
Total score eye opening + motor response + verbal response 3B15
Reprinted from Teasdale G, Jennett B. Assessment of coma and impaired consciousness: a practical
scale. Lancet 1974;2:81–84 [112]; with permission from Elsevier Science.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 419

mask with high-flow 100% oxygen. The decision to provide an artificial airway
should be made by the team leader, and those managing the airway and should be
based upon specific indications. Table 3 lists some of the indications for tracheal
intubation. Individualization of care is important in managing the patient with
TBI, and as such, established protocols may require modification.
It is important to note that concern about increased ICP influences the
approach to the airway but does not contraindicate endotracheal intubation.
Endotracheal intubation in an unanesthetized patient will increase blood pressure,
heart rate, and ICP [5,6]. However, of greater clinical importance is the fact that
cerebral blood volume (CBV) is increased by hypoxia and hypercarbia [7], that
ICP is increased by untreated hypoxia [8], or hypercarbia [9], and that aspiration
of oral or gastric contents not only interferes with gas exchange but also increases
long-term morbidity and mortality [10,11]. The increase in ICP with airway
manipulation can be reduced by appropriate use of medications [12–14].
Having made the decision to provide an artificial airway, many techniques of
intubation and choices of drugs are possible. In general, the best technique is the
one with which the team members are most proficient. Head-trauma patients are
high-risk individuals in whom experimentation with new techniques or training
of inexperienced personnel may be imprudent. In general, there are two
approaches to the tracheal intubation of head-trauma patients: oral intubation
using direct laryngoscopy and nasal intubation (either blind or fiberoptically
guided). Each approach has advantages and disadvantages.
Associated cervical spine injury is present in approximately 2% [15] to 21%
[16] of trauma patients. Uncontrolled movement of the neck in patients with
cervical spine injury can precipitate neurologic injury, and is therefore to be
Table 3
Indications for endotracheal intubation
Absolute
Apnea, bradypnea (respiratory frequency < 6/min)
Hypoxia on 100% O2 (PaO2 < 70 mmHg, SpO2 < 90%)
Hypercarbia (PaCO2 > 65 mmHg)
Absence of airway protective reflexes (cough, gag, swallow)
Mechanical airway obstruction
Expanding oral or neck mass
Need for the administration of barbiturates, sedatives, or muscle relaxants
Hemodynamic instability/severe hypotension
Glasgow Coma Scale score < 8 (see Table 1)
Relative
Progressive tachypnea (respiratory frequency >35/min)
Flail chest
Pulmonary aspiration
Combative behavior
Hypothermia (core temperature < 34.5�C)Seizures
Increased intracranial pressure
Mild hypoxia or hypercarbia
Metabolic acidosis (pH < 7.25)
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439420

avoided. Because of this possibility, the use of awake/sedated nasal intubation,
which does not require head movement, has been advocated [17]. Contra-
indications to awake nasal intubation include fractures of the skull base, La
Forte fractures, bleeding diatheses, and midface disruption [18,19]. The technique
is much more difficult in patients with slow or absent respirations, and is
relatively contraindicated [20,21]. Fiberoptic visualization is often utilized but
has a number of limitations, including the requirement of a cooperative patient,
need for specialized equipment and training, and vastly increased difficulty when
the airway is contaminated with blood, vomitus, or excessive secretions [20–22].
Direct laryngoscopy of patients with cervical injury can be used if accompanied
by manual in-line axial stabilization of the head and neck by an assistant [23]. In
the absence of in-line stabilization, neck movement, especially in the upper
cervical spine, has been demonstrated in patients without neck injury [24].
Manual in-line stabilization (previously termed in-line axial traction) decreases
movement of the neck in cadaveric models of cervical spine injury [25], which
theoretically reduces the risk of aggravating cervical spine injury, but also
increases difficulty with visualization and tracheal intubation [26]. Regardless
of the intubation technique chosen, adequate planning and preparation should
precede intubation. The patient should be preoxygenated with 100% oxygen (O2)
by mask; intubating equipment and suction should be present and functioning; all
desired and emergency drugs should be present; and a means of establishing a
surgical airway should be available if endotracheal intubation fails.
Intravenous drugs can be used as adjuvants during intubation to create more
controlled and stable intubating conditions and to blunt the systemic effects of
intubation (increased blood pressure and ICP) [12–14]. Drugs also can precip-
itate hypotension, result in total airway loss if intubation is unsuccessful, generate
life-threatening electrolyte imbalances (eg, hyperkalemia after succinylcholine in
chronically paraplegic or quadriplegic patients), trigger an anaphylactic or
anaphylactoid reaction, or interact in unexpected ways with the patient’s other
medications or other medical conditions. Only trained, experienced individuals
who are prepared to recognize and manage drug-induced complications should
administer drugs.
Induction agents such as sodium thiopental, etomidate hydrochloride, and
propofol have been used to induce anesthesia before intubation. Each decreases
the systemic response to intubation, blunts ICP changes, and decreases the
cerebral metabolic rate for oxygen (CMRO2). Induction agents also cause apnea
and loss of protective airway reflexes; thus, an artificial airway must be secured,
and controlled ventilation must be initiated after their administration. Another
concern includes cardiovascular depression with propofol and thiopental, which
can lead to hypotension, especially in the presence of uncorrected hypovolemia.
Hypotension is a primary risk factor for poor outcome after head trauma [27–31].
Etomidate is unique in that induction doses usually cause little change in blood
pressure, although it reduces CMRO2 [32]. Etomidate administration, however,
can result in an exaggerated response to intubation, such as tachycardia, and has
been associated with myocardial ischemia in patients with high cardiac risk [33].
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 421

Finally, ketamine, a dissociative anesthetic that preserves spontaneous ventilation
with limited cardiovascular compromise, would seem to be an appropriate agent
for use in establishing an airway in patients with TBI. This agent though, has
been associated with increased cerebral blood flow and increased ICP, and as
such, is relatively contraindicated as a single agent for patients with risk for or
preexisting increased ICP [34–36]. Whatever agent is chosen to blunt the
response to intubation, the individual providing the medication must be imme-
diately prepared to assume control of the airway, protect the patient from
pulmonary aspiration, assure adequate oxygenation and ventilation, and treat
systemic hemodynamic responses such as hypotension and tachycardia.
Muscle relaxants are often combined with induction drugs to secure the
airway. Succinylcholine hydrochloride, which is the only ultrashort-acting,
depolarizing muscle relaxant presently approved by the Federal Drug Adminis-
tration, produces complete muscle relaxation within 60 to 120 seconds of
administration, with return of muscle strength in a matter of minutes. However,
it can lead to life-threatening hyperkalemia, trigger malignant hyperthermia, and
increase ICP [37,38]. The increase in ICP can be blunted by administration of an
adequate dose of an induction agent such as thiopental [39]. However, even
without treatment, the increase in ICP is transient and of questionable clinical
significance [39]. Increases in ICP secondary to hypoxia and hypercarbia are well
documented and much more likely to be clinically important.
Nondepolarizing neuromuscular blocking agents, such as vecuronium bro-
mide, cis-atracurium bresylate, and rocuronium bromide, do not carry the risks of
hyperkalemia, malignant hyperthermia, and increased ICP. Given in large doses,
these drugs produce good-to-excellent intubating conditions within 120 to 180
seconds. However, profound relaxation will persist for 30 to 120 minutes,
mandating expeditious placement of an artificial airway.
All sedative/hypnotics and muscle relaxants used to facilitate endotracheal
intubation compromise protective airway reflexes. In trauma patients, it is
impossible to know when food was last ingested. There may be food, gastric
secretions, or blood within the stomach that may be aspirated into the lungs if
passive or active regurgitation occurs. Because of the risk of ‘‘a full stomach,’’ a
rapid sequence induction technique should be used when drugs are given that
remove protective reflexes. The rapid sequence induction consists of preoxygen-
ation and denitrogenation with 100% oxygen, application of cricoid pressure
[40], administration of induction agents and muscle relaxants, and immediate
direct laryngoscopy with intubation of the trachea. Positive-pressure ventilation is
avoided between the time of drug administration and intubation. Correctly
applied cricoid pressure is believed to decrease the risk of passive regurgitation
and aspiration of gastric contents by mechanically occluding the esophagus at the
level of the cricoid ring. However, application of cricoid pressure in cadavers
caused cervical spine displacement in cases of ligamentous or bony disruption
[41], raising concerns about the safety of cricoid pressure in situations in which
cervical spine injury is present or likely. Even in healthy patients with no
identified risks for cervical spine instability, single-handed cricoid pressure
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439422

(applied to only the anterior neck without posterior support) was associated with
a mean neck displacement of 4.6 mm (range of 0–8 mm) [42]. Therefore, the risk
of iatrogenic cervical cord injury in such patients must be weighed against the
risk of gastric aspiration. Even with the risks of direct laryngoscopy, several
retrospective studies have suggested that direct laryngoscopy, even in the
presence of known cervical spine injuries, is as safe as alternate techniques
[43]. If endotracheal intubation is needed in a patient with known cervical spine
injury, other options such as blind nasal or fiberoptic intubation should be
considered if time and clinical circumstances permit. If direct laryngoscopy with
the application of cricoid pressure is to be used, the use of bi-manual cricoid
pressure (anterior compression of the cricoid cartilage with simultaneous support
of the posterior neck) has also been proposed [44]. Effective evaluation and acute
stabilization of the head-trauma patient must precede all other interventions.
Necessary airway management should not be delayed or withheld because of fear
of increased ICP or the need for other diagnostic studies such as computed
tomographic (CT) scans, angiography, or cervical radiographs.
Having evaluated and dealt with airway, ventilation, and oxygenation issues,
the trauma team can proceed to hemodynamic evaluation. This evaluation
includes an estimation of intravascular volume, establishment of adequate
vascular access (peripheral venous, central venous, and arterial catheterization),
review of estimated blood loss, acquisition of baseline laboratory studies, and
resuscitation. Because of the potential for unrecognized blood and fluid loss,
hypovolemia is always a possibility. Heart rate and blood pressure are insensitive
indicators of volume status. Young, previously healthy patients can lose nearly
30% of their blood volume yet not manifest overt hypotension in the supine
position. Reflex systemic hypertension is commonly observed with head trauma,
further confounding clinical assessment of intravascular volume.
The importance of avoiding hypotension cannot be overemphasized. Tables 4
and 5 illustrate the effects of hypotension on outcome after head injury. Fig. 1
graphically represents the influence of in-hospital hypotension on the long-term
Table 4
Outcome by secondary insult occurring from time of injury through resuscitation at Traumatic Coma
Data Bank Hospital Emergency Department for mutually exclusive insults
Number % of totalOutcome (%)
Secondary insults of patients patients GR or MD SD or PVS Dead
Total cases 717 100 43.0 20.2 36.8
Neither 308 43.0 53.9 19.2 26.9
Hypoxia 161 22.4 50.3 21.7 28.0
Hypotension 82 11.4 32.9 17.1 50.0
Both 166 23.2 20.5 22.3 57.2
Hypoxia, PaO2 < 60 mmHg; hypotension, systolic blood pressure < 90 mmHg.
Abbreviations: GR, good recovery; MD, moderate disability; SD, severe disability; PVS, persistent
vegetative state.
From Chesnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining
outcome from severe head injury. J Trauma 1993;34:216–222 [29]; with permission.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 423

outcomes of patients with head injury. Failure to recognize, intervene, and correct
hypotension, even at the earliest stages of management, is associated with poorer
outcome, and blood pressure should be the primary focus of initial evaluation and
resuscitation of the head-injured patient after airway management. Although
hypoxemia should be avoided, head injury appears to be much more adversely
influenced by hypotension.
The choice of resuscitation fluid after head trauma is a matter of ongoing debate.
Relatively isotonic crystalloid solutions (lactated Ringer’s solution and 0.9%
saline) have been used extensively for years. It is important to remember that the
osmolarity of lactated Ringer’s solution is only 273 mOsm/L, while that of 0.9%
saline is 308 mOsm/L. Large volumes of lactated Ringer’s solution will decrease
serum osmolarity and thus increase total brain water [45,46]. Some institutions
limit the volume of lactated Ringer’s solution to 2000 mL, while others use 0.9%
saline as the crystalloid of choice. Because of crystalloid distribution throughout all
extracellular spaces, a ratio of 5:1 is required to replace blood loss (ratio of
interstitial fluid volume to plasma volume). In major blood loss, this may represent
a considerable volume, especially because the ratio of crystalloid to blood loss
increases as protein dilution occurs [47]. Also, rapid infusion of unwarmed fluid
can lead to hypothermia. Despite years of treatment with fluid restriction of head-
injured patients, experimental and clinical data strongly suggest that there is little
correlation between total fluid administration and clinical outcome [48]; moreover,
if inadequate resuscitation results in hypotension, ICP may increase [49].
Hypertonic crystalloid solutions such as 3% and 7.5% saline have been used to
avoid the large volumes of isotonic crystalloids necessary for resuscitation.
Hypertonic solutions increase intravascular volume by shifting water from the
intracellular to the extracellular space [50]. These agents increase intravascular
volume and improved hemodynamic stability in hypovolemic shock [51] and
reduce ICP but do not reliably restore cerebral oxygen delivery after experimental
head trauma [52]. The total volume of hypertonic saline should be limited to
minimize electrolyte imbalance and hyperosmolality.
Table 5
Outcome by secondary insult present at time of arrival at Traumatic Coma Data Bank Hospital
Emergency Department for mutually exclusive insults
Number % of totalOutcome (%)
Secondary insults of patients patients GR or MD SD or PVS Dead
Total cases 699 100.0 42.9 20.5 36.6
Neither 456 65.2 51.1 21.9 27.0
Hypoxia 78 11.2 44.9 21.8 33.3
Hypotension 113 16.2 25.7 14.1 60.2
Both 52 7.4 5.8 19.2 75.0
Hypoxia, PaO2 < 60 mmHg; hypotension, systolic blood pressure < 90 mmHg.
Abbreviations: GR, good recovery; MD, moderate disability; SD, severe disability; PVS, persistent
vegetative state.
From Chesnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining
outcome from severe head injury. J Trauma 1993;34:216–222 [29]; with permission.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439424

Fig. 1. Outcome (Glasgow Outcome Scale at 12 months after injury) as influenced by in-hospital hypotension (one or more episodes of systolic blood pressure #90 mmHg)
for 493 patients in the Traumatic Coma Data Bank (TCDB). Early hypotension is that present on arrival at the TCDB hospital. Late hypotension occurred any time during
the patient’s stay in the intensive care unit beginning after the first shift. From Chesnut RM. Secondary brain insults after head injury: clinical perspectives. New Horiz
1995;3:366–375 [114]; with permission.
E.Bedell,
D.S.Prough/Anesth
esiologyClin
NAm
20(2002)417–439
425

Isotonic colloidal solutions (hetastarch, pentastarch, albumin, and blood) are
useful for acute volume expansion, and are given in a ratio of 1:1 to replace blood
loss. Because of concerns about compatibility, infection, and availability, the use
of blood products for initial resuscitation should be restricted to severe ongoing
hemorrhage, severely compromised oxygen delivery, and bleeding diatheses
[53,54]. Six percent hetastarch and 5% albumin are frequently given instead of
packed red cells or crystalloid. Hetastarch, in volumes greater than 20 mL/kg, has
been associated with abnormal clotting profiles and a risk of increased bleeding
[55,56], while 5% albumin, as a human product, is expensive, limited in
availability, and has been associated in rare instances with anaphylactic reactions.
Meta-analyses suggest that overall survival is not increased by the use of albumin
or colloid [57] and perhaps is even worsened [58]. In the future, synthetic blood
products, such as recombinant hemoglobin, may become available for use in
resuscitation. These agents would allow rapid volume expansion without the risks
of incompatibility, infection, or scarcity while improving oxygen delivery [59].
To date though, these agents have not been efficacious, and the only agent studied
in a clinical setting was withdrawn because of increased patient mortality [60].
Hypotonic solutions and glucose-containing solutions deserve special men-
tion. Because of redistribution of hypotonic solutions throughout total body
water, 5% dextrose in water (D5W) is ineffective as a resuscitation fluid. Only
7% of intravenously administered D5W remains intravascularly after equili-
bration; therefore, the volumes required to resuscitate even limited blood loss
may cause severe hyponatremia and may aggravate cerebral edema. Hyper-
glycemia in conjunction with TBI has been associated with worsened outcome
both in animal and human studies [61–63]. Consequently, glucose-containing
solutions, unless required to correct hypoglycemia, should be avoided in head
trauma. Because hypovolemia, hypotension, and shock are so important, and
because it is not clear which fluid is best (given the above caveats), the choice of
resuscitation fluid is more a matter of personal preference than a choice based
upon clear scientific outcome studies.
With the ABC’s addressed, attention can shift to the management of specific
injuries. For the purposes of this article, we will assume an isolated TBI. (In
clinical practice, other injuries could be of higher priority and require more
prompt attention. The early goals of management are to diagnose the extent of all
injuries, to resuscitate and stabilize the head-injured patient, and to expedite
needed surgical intervention.)
Management
After the initial evaluation and resuscitation are completed, the management of
blood pressure and ICP becomes paramount and is based on the interrelationships
between brain trauma, intracranial pressure, and hemodynamic manipulations.
Conventionally, invasive ICP monitoring is used if GCS is � 8. This is usually
deferred for patients scheduled for immediate craniotomy. In those patients
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439426

scheduled for non-neurosurgical procedures under general anesthesia (eg, extrem-
ity surgery), one should consider placement of ICP monitoring devices for those
with GCS � 12 as they are at risk for intraoperative deterioration, and strongly
consider placement for those with an initial GCS � 8.
Irreversible ischemic cell damage occurs rapidly when there is inadequate
cerebral blood flow (CBF) that contributes to brain injury [27] on a global,
regional, or focal level. The actual determinants of CBF are complex, and
there are no tests or studies to monitor CBF real-time in an emergency setting.
The supervisory physician must thus make empirical management decisions
about the adequacy of CBF, based on the clinical situation and on an estimation
of cerebral perfusion pressure (CPP), which is defined as mean arterial blood
pressure (MAP) minus ICP or central venous pressure (CVP), whichever is
higher. In clinical practice, a CPP of 60–80 mmHg generally is considered
adequate [64].
CPP represents the blood pressure gradient across the brain’s vascular bed, and
thus determines blood flow through the brain. This relationship can be modeled
through a modification of Ohm’s Law, which states that the pressure gradient
(arterial pressure minus venous pressure) equals the flow times the resistance:
Pressure ¼ Flow� Resistance
This model must be used with care. It would be easy to mistakenly assume that
the resistive element in the equation is fixed. In reality, there is great variability in
cerebral vascular resistance due to local and systemic factors. Both experimental
and clinical brain trauma are associated with acutely increased cerebrovascu-
lar resistance.
In healthy, nontraumatized patients, cerebral vascular resistance is regulated
predominantly at the precapillary arterioles to maintain a constant blood flow
adequate to supply the needs of the brain tissue. Classic examples of these
changes are listed in Table 6. These changes in resistance are the foundation for
the concept of cerebral autoregulation, which holds that CBF is regulated through
alterations in arteriolar muscular tone under a wide variety of situations to
maintain a balance between CBF and CMRO2. Normal autoregulatory profiles
for humans are well described, and are shown in Fig. 2, although these responses
are altered in disease states and after TBI. In normal individuals, there is a direct
relationship between blood pressure and cerebral vascular resistance, allowing for
a constant blood flow over a wide range of MAPs.
Table 6
Effect of systemic and local factors on cerebrovascular resistance
Causes of cerebral vasoconstriction Causes of cerebral vasodilation
Increased blood pressure Decreased blood pressure
Decreased PaCO2 Increased PaCO2
Decreased blood viscosity Increased blood viscosity
Barbiturates Hypoxia (SaO2 < 60 mmHg)
Decreased cerebral metabolic demands Increased cerebral metabolic demands
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 427

After TBI, vascular reactivity is acutely altered [65]. Pressure autoregulation
is lost at lower levels of CPP [66]. In experimental animals, loss of autoregu-
lation has led to increased neurologic injury with even mild hemorrhagic hypo-
tension [67]. Moreover, in the acute interval after both experimental [67]
and clinical [27] traumatic brain injury, CBF is substantially reduced; one third
of patients have decreased regional or global CBF to a level that can cause
cerebral ischemia within 8 hours of injury [68]. Posttraumatic impairment of
pressure autoregulation may further reduce CBF at blood pressures that might
otherwise be considered safe, which may explain the worsened outcome
associated with hypotension.
In contrast, hypertension after TBI could increase intracranial hemorrhage or
disrupt the upper limits of pressure autoregulation leading to excessive CBV
[69,70]. Initially, a patient with TBI may manifest systemic hypertension. In
some patients, an increase in MAP may be necessary to overcome increased ICP
(and thus maintain CPP). Treating systemic hypertension before ruling out
increased ICP may lead to inadequate CPP [71], while failure to treat systemic
hypertension in the presence of an intracranial bleed may lead to hematoma
expansion and higher ICP. Evidence of increased ICP and the presence of
systemic hypertension should be an indication for early diagnostic procedures.
A judgment should be made about the presence of increased ICP or about
Fig. 2. The relationship of cerebral blood flow (CBF) to cerebral perfusion pressure (CPP), PaCO2,
and PaO2. Units on the abscissa are in mmHg. From Michenfelder JD. The awake brain. In:
Michenfelder, JD, editor. Anthesthesia and the brain: clinical, functional, metabolic, and vascular
correlates. New York: Churchill Livingstone; 1998. p. 3–21 [115]; with permission.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439428

whether the hypertension is leading to further patient compromise before treating
systemic hypertension aggressively. With the availability of CT scanners in most
medical centers, the rapid diagnosis of intracranial mass lesions should be
possible without significant delay. In summary, it is prudent to keep in mind
the possible alterations in cerebral vascular reactivity and avoid even mild
hypotension, while at the same time guarding against uncontrolled or sustained
hypertension. A reasonable guideline for blood pressure management is a CPP of
60 to 100 mmHg.
Changes in arterial carbon dioxide tension (PaCO2) also influence CBF.
Cerebral vascular reactivity to PaCO2 was noted in the early 1950s in association
with high-altitude military aircraft [72]. It was hypothesized that severe hypo-
capnia had deleterious effects [73], reflecting the basic question, ‘‘Can hypocarbia
produce cerebral vasoconstriction sufficient to precipitate cerebral ischemia?’’
Animal studies and clinical electrophysiologic data have not supported the concept
that hypocarbia induces cerebral ischemia in normal brain [74,75]. The study of the
effects of hypocarbia on abnormal brains (eg, TBI) has yielded different results.
Animal studies have demonstrated that hypocarbia, in association with anemia,
hypotension, or brain retraction, can lead to ischemia injury, and there is growing
evidence that hypocarbia may be associated with worsened long-term outcome in
head-trauma patients [76–78]. The routine use of hyperventilation in head-trauma
patients is, therefore, no longer recommended. Two relative indications for the use
of hyperventilation include acute increases in ICP and the need to improve surgical
exposure. Use of prolonged hyperventilation may require the insertion of a
regional or focal measure of the adequacy of cerebral oxygenation, such as jugular
venous oximetry or brain tissue oxygen sensors (see below).
Management of ICP also contributes to maintaining an adequate CPP.
Intracranial pressure is the relationship between the volume of the skull and its
contents. This relationship is described by the elastance curve, which relates ICP
and intracranial volume (Fig. 3). As the volume of the intracranial contents ap-
proaches the available space (the knee of the curve), the pressure increases
rapidly. Beyond this point, even small additional volume increases can dramat-
ically increase ICP.
The intracranial contents can be arbitrarily divided into four groups: solid
mass, water, cerebrospinal fluid (CSF), and intravascular blood. Management
techniques can be aimed at all four areas with varying degrees of success. Solid
intracranial contents include nonwater brain parenchyma plus missile compo-
nents, bone fragments, and hematomas. These elements cannot be pharmacolog-
ically or physiologically manipulated. Surgical decompression or decreasing the
relative volume of the other intracranial contents remain the only practical
options. Therefore, it is vital to understand the techniques, risks, and potential
benefits of altering the volume of the other intracranial components in the
management of ICP.
CSF drainage can be used to decrease ICP as well as to control hydrocephalus
and improve surgical exposure. Pharmacologic manipulation of CSF production
and elimination using acetazolamide is slow in onset and difficult to titrate. The
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 429

intraoperative adjustment of CSF volume is not a primary technique for the
management of ICP during anesthesia unless a ventriculostomy is in place.
However, graded CSF drainage is used to control ICP in some centers.
Reducing intracranial water content is important in the management of
intracranial hypertension associated with TBI. Brain water content depends upon
the cellular integrity and function of the blood–brain barrier, the osmolality of
blood, and the osmolality of the fluid administered. Brain water is minimally
influenced by changes in colloid osmotic pressure, but is highly influenced by
acute changes in osmolality [79]. Hypotonic fluids increased brain water [46],
and hypertonic fluids decreased brain water in animals [50]. Overall brain water
can also be reduced through administration of osmotic agents such as mannitol
(in doses of 0.5–1 g/kg). Although countless clinicians have observed decreased
ICP after administration of these agents, the precise mechanism of action of
mannitol has been questioned [80]. In contrast, glucocorticoids do not decrease
traumatic brain edema [81], despite their established efficacy in reducing vaso-
genic edema associated with brain tumors. Glucocorticoids are indicated for the
acute treatment of spinal cord injury, and should be initiated as soon as
reasonable following injury [82].
Adjustment of intracranial blood volume remains the mainstay of acute ICP
management. CBV is approximately 3.5 mL/100 g brain tissue in healthy
individuals [83], or about 50 mL, approximately one-fourth of which is arterial
and three-fourths venous. It is important to appreciate the difference between CBV
and CBF, and the difference between arterial and venous blood volume. CBF is the
Fig. 3. Elastance curve for the cranial vault. Additional volume is well tolerated if reserves are good;
however, as intracranial volume increases to a critical point, intracranial pressure (ICP) increases
rapidly with further small increments in intracranial volume.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439430

rate at which blood traverses the cerebral vascular bed (generally 55 mL/min-
100 g), while CBV is the actual volume of blood contained within the vascular bed.
CBF and CBV are not directly coupled; an increase in CBF does not necessarily
lead to an increase in CBV. An acute increase in CBF may lead to reflex arteriolar
vasoconstriction and an overall decrease in CBV (and thus a decrease in ICP)
[64,84]. Similarly, the management of arterial and venous blood volumes must be
considered separately. The arterial vascular system will autoregulate based upon
local and systemic factors, while the volume in the venous circuit usually responds
passively to external factors such as venous distending pressure.
Alteration of arterial CBV remains a principal tool in management of ICP after
head trauma. By manipulating the reactive arterial vascular system, it is possible
to induce arterial vasoconstriction and to decrease arterial CBV. Table 6 lists
some of the arterial responses to various local and systemic challenges. Peri-
arteriolar hydrogen ion concentration ([H+]) powerfully influences cerebral
arteriolar tone. Clinical management usually emphasizes PaCO2. As the PaCO2
increases, [H+] increases. Arteriolar diameter increases, leading to a concomitant
decrease in cerebral vascular resistance, an increase in CBF, and an increase in
CBV. The opposite occurs with decreased [H+] (decreased PaCO2). The effects of
lowering PaCO2 are rapid in onset (2–3 minutes) and remain for a number of
hours. This acute effect is lost, however, as buffering of periarteriolar [H+]
diminishes the effect of hyperventilation on arteriolar vascular tone. By 24 hours,
the initial vasoconstriction is gone, and an abrupt return to normal PaCO2 may
lead to cerebral vasodilation and increased ICP [85]. In normal brain, increases in
CO2 to greater than 80 mmHg do not lead to greater cerebral vasodilation, as
relaxation is maximal. Similarly, in normal brain, hyperventilation to PaCO2
below 20 mmHg does not lead to further vasoconstriction, as either local factors
or mechanical factors inhibit further vasoconstriction.
After cerebral ischemia or TBI, the role of PaCO2 is less clear. Excessively
low PaCO2 may contribute to or cause ischemia [78] and worsen long-term
cellular survival. The measurement of cerebral oxygenation using cerebral
venous oxygen saturation has shown that hyperventilation can lead to significant
decreases in saturation [86]. Although low PaCO2 may constrict normal arterio-
les, thereby shunting blood to ischemic areas [87], this ‘‘Robin Hood’’ process of
stealing blood from ‘‘rich’’ tissue beds to give to ‘‘poor’’ regions has been
difficult to prove. Redistribution of blood flow from normal areas to ischemic
areas has been unpredictable [88] and ideally requires continuous real-time
monitoring for proof of efficacy. Hyperventilation should thus be restricted to
short intervals with specific goals such as acutely decreasing ICP or improving
surgical exposure, and consideration for the use of jugular venous saturation
monitoring should be made [89]. PaCO2 should be allowed to return toward
normal as soon as the acute indications pass. It is intriguing to note that the
effects of hyperventilation can be modified in patients with TBI. Use of
supplemental inspired oxygen to develop hyperoxia (arterial oxygen tension
[PaO2] > 200 mmHg) has been shown to ameliorate the effects of hyperventila-
tion and improve jugular saturation in patients with TBI [90,91]. The utility of
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 431

hyperoxia as a clinical tool is as yet unproven, but represents an ongoing area of
provocative research.
Hypoxia remains one of the most potent arteriolar cerebrovascular dilators.
Hypoxia or ischemia leads to marked vasodilation, increased arterial vascular
volume, and increased ICP. Normal systemic oxygenation does not necessarily
imply adequate cerebral oxygenation; CBF and oxygen-carrying capacity must
also be adequate. Techniques for monitoring transcranial cerebral oxygen
saturation [92,93], jugular venous oxygen saturation [94], and brain tissue partial
pressure of oxygen (PO2) are being developed or are available to provide real-
time information about the adequacy of cerebral oxygenation. In the future, these
techniques may become available for routine evaluation of head-injured patients.
At present, maintenance of adequate CPP and oxygen-carrying capacity remain
the primary tools for preserving cerebral oxygenation.
The phenomenon of pressure autoregulation is also critical in regulating CBV.
Cerebral arteriolar smooth muscle responds to increased intravascular pressure
with increased vascular tone within the range of pressure autoregulation. As
blood pressure increases, arteriolar vasoconstriction maintains constant flow and
decreases arterial blood volume. By the same mechanism, decreased blood
pressure (or hypotension) produces arteriolar dilation and increases arterial blood
volume. Because hypotension-induced reflex vasodilation may increase CBVand
ICP in head-injured patients [49], protection against hypotension remains a key
component in the management of arterial blood volume and ICP.
Red cell rheology and blood viscosity play a role in arterial vasoconstriction.
Decreasing hematocrit decreases blood viscosity, which leads to vasoconstriction
of normal brain arterioles [95]. Thus, hemodilution increases CBF and results in
reflex vasoconstriction, which has been termed ‘‘blood viscosity autoregulation’’
[96]. The clinical importance of this phenomenon is controversial [97]. Admin-
istration of mannitol alters red cell deformability and decreases viscosity
unrelated to changes in hematocrit [98]. This observation may explain mannitol-
induced decreases in ICP that are not related to total brain water or hemodilu-
tion [99–101].
Vascular autoregulation is determined by many factors, including viscosity and
CBF. In addition, if oxygen-carrying capacity is decreased below the metabolic
requirements of the brain, cerebral vasodilation will occur. The difference of the
impact of hemodilution-induced vasoconstriction and vasodilation secondary to
inadequate oxygen delivery is difficult to determine clinically. In practice, the
optimal hematocrit for head-injured patients remains undefined.
Pharmacologic interventions are another important means of altering arteriolar
resistance and arterial blood volume. Table 7 lists some commonly administered
drugs and their effects on cerebral arterial tone. Volatile inhalational agents and
nitrous oxide cause arterial vasodilation; although hyperventilation modifies
drug-induced cerebral vasodilation, it does not reliably prevent increases in
ICP. Therefore, intravenous agents such as narcotics, benzodiazepines, and short-
acting hypnotics have been used for anesthesia in cases of head trauma. With
either inhalational or intravenous techniques, hypotension must be avoided. Some
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439432

intravenous agents, including propofol and thiopental [102], cause systemic
vasodilation or myocardial depression, which may lead to hypotension, especially
in conjunction with uncorrected hypovolemia. Therefore, blood pressure must be
monitored and hypotension treated promptly and aggressively. Because of the
risks and benefits of different anesthetic approaches, the clinician should be
careful about the choice of drugs for individual patients.
Cerebral venous blood volume depends upon CBF, gravity, and restriction to
outflow. Increased blood viscosity decreases flow (by increasing resistance),
leading to increased blood volume. Decreasing the venous pressure differential
(by increasing CVP [103], lowering the head [104], or inducing cerebral
venodilation) will increase venous CBV. Increasing the resistance to venous
outflow by bandaging the neck or extreme lateral rotation of the head can
increase venous CBV [83,105]. Maneuvers that facilitate cerebral venous
drainage and therefore potentially decrease venous CBV, are listed in Table 8.
However, if such maneuvers decrease CPP (eg, head elevation leading to
hypotension), the benefits of improved venous return may be negated [106].
Attempts to limit secondary brain injury should ideally include the initiation of
protective measures that would improve the outcome of damaged cells and protect
normal tissue from harm. The concept of brain protection is used extensively in
Table 7
Effects of selected drugs on cerebral vascular resistance, systemic vascular resistance, and myocar-
dial contractility
Drug CVR SVR Myocardial
Ketamine Decreased Increased Increased
Halothane Decreased Unchanged Decreased
Isoflurane Decreased Decreased Unchangeda
Sevoflurane Decreased Decreased Unchangeda
Nitrous oxide Decreased Unchanged Decreased
Barbiturates Increased Decreased Decreased
Benzodiazepines Increased Decreased Unchanged
Narcotics Variable Decreased Unchanged
Etomidate Increased Unchanged Unchanged
Propofol Increased Decreased Decreased
Abbreviations: CVR, cerebral vascular resistance; SVR, systemic vascular resistance.a Note that systemic arterial dilation may preserve cardiac output, thus masking myocar-
dial depression.
Table 8
Techniques to decrease cerebral venous blood volume
Avoid extremes of neck rotation
Avoid direct jugular compression
Elevate head (caution: hypotension negates effect on CPP)
Decrease blood viscosity (mannitol)
Avoid sustained increases in intrathoracic pressure
Avoid cerebral venodilators (e.g., nitroglycerine, etc.)
Abbreviations: CPP, cerebral perfusion pressure; ICP, intracranial pressure.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 433

cardiac surgery and neurosurgery. Techniques to decrease the likelihood of
permanent ischemic injury to brain, such as active hypothermia preceding
complete circulatory arrest, are now accepted practices [107]. The efficacy of
these techniques after ischemic or traumatic insults is less established. Preliminary,
single-institution studies evaluating hypothermia and long-term outcome after
head trauma suggested that decreasing the temperature of the brain shortly after
injury improved morbidity and mortality [108–110]; however, a recent multicenter
trial did not reproduce these earlier findings [4]. An interesting finding in that trial
was the fact that the worst outcome occurred in patients who arrived at the hospital
and were rapidly rewarmed. A variety of drugs that influenced outcome after
ischemic and traumatic brain injury in experimental animals have also been studied
in clinical trials but to date have not been shown to improve outcome. At present,
the most important goal is the reestablishment of adequate brain tissue oxygenation
to limit further cellular compromise. Based upon the clinical presentation, a
specific care plan should encompass patient needs, and allow for rapid evaluation
and treatment and flexibility based upon new research.
Summary
The management of TBI remains an important and frustrating component of the
practice of anesthesiology and critical care medicine. The difficulties in manage-
ment of TBI as well as the poor response rates to medical therapy after TBI are not
new. The following passage appeared in the introductory chapter of a text on TBI
from 1897: ‘‘The manner of treatment is of importance in only a minority of cases,
since many subjects of intracranial injury are fated to die whatever measures may
be adopted for their relief, and a still greater number are destined to recover though
left entirely to the resources of nature. It is probable that in by far the larger
proportion of cases in which the issue is determined by treatment it is met in the
initial stage, and by insuring restoration from primary shock’’ [111].
Although secondary insults from factors such as hypotension, hypoxemia, and
hyperventilation increase morbidity and mortality, data are not yet available to
indicate whether scrupulous prevention and prompt treatment of secondary
injuries will reduce morbidity and mortality. In addition, no specific intervention
to date has improved overall long-term outcome. With ongoing research, perhaps
active interventions will become available. Until that time, thoughtful and care-
ful attention to physiologic management provides the greatest opportunity for a
good outcome.
References
[1] Jennett B. Epidemiology of head injury. J Neurol Neurosurg Psychiatry 1996;60:362–9.
[2] Kraus JF, McArthur DL. Epidemiologic aspects of brain injury. Neurol Clin 1996;14:435–50.
[3] Sosin DM, Sniezek JE, Waxweiler RJ. Trends in death associated with traumatic brain injury,
1979 through 1992. JAMA 1995;273:1778–80.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439434

[4] Clifton GL, Miller ER, Choi SC, Levin HS, McCauley S, Smith KR Jr, et al. Lack of effect of
induction of hypothermia after acute brain injury. N Engl J Med 2001;344:556–63.
[5] Burney RG, Winn R. Increased cerebrospinal fluid pressure during laryngoscopy and intubation
for induction of anesthesia. Anesth Analg 1975;54:687–90.
[6] Shapiro HM, Wyte SR, Harris AB, Galindo A. Acute intraoperative intracranial hypertension
in neurosurgical patients: mechanical and pharmacologic factors. Anesthesiology 1972;4:
399–405.
[7] Fortune JB, Feustel PJ, deLuna C, Graca L, Hasselbarth J, Kupinski AM. Cerebral blood flow
and blood volume in response to O2 and CO2 changes in normal humans. J Trauma 1995;39:
463–72.
[8] Brown MM, Wade JPH, Marshall J. Fundamental importance of arterial oxygen content in the
regulation of cerebral blood flow in man. Brain 1985;108:81–93.
[9] Kety SS, Schmidt CF. The effects of active and passive hyperventilation on cerebral blood flow,
cerebral oxygen consumption, cardiac output and blood pressure of normal young men. J Clin
Invest 1946;25:107–19.
[10] LeFrock JL, Clark TS, Davies B, Klainer AS. Aspiration pneumonia: a ten-year review. Am
Surg 1979;45:305–15.
[11] Olsson GL, Hallen B, Hambraeus-Jonzon K. Aspiration during anaesthesia: a computer-aided
study of 185 358 anaesthetics. Acta Anaesthesiol Scand 1986;30:84–92.
[12] Moss E, Powell D, Gibson RM, McDowall DG. Effect of etomidate on intracranial pressure and
cerebral perfusion pressure. Br J Anaesth 1979;51:347–51.
[13] Unni VKN, Johnston RA, Young HSA, McBride RJ. Prevention of intracranial hypertension
during laryngoscopy and endotracheal intubation. Br J Anaesth 1984;56:1219–23.
[14] White PF, Schlobohm RM, Pitts LH, Lindauer JM. A randomized study of drugs for preventing
increases in intracranial pressure during endotracheal suctioning. Anesthesiology 1982;
57:242–4.
[15] O’Malley KF, Ross SE. The incidence of injury to the cervical spine in patients with cranio-
cerebral injury. J Trauma 1988;28:1476–8.
[16] Alker GJ, Oh YS, Leslie EV, Lehotay J, Panaro VA, Eschner EG. Postmortem radiology of head
and neck injuries in fatal traffic accidents. Radiology 1975;114:611–7.
[17] Kapp JP. Endotracheal intubation in patients with fractures of the cervical spine. J Neurosurg
1975;42:731–2.
[18] Muzzi DA, Losasso TJ, Cucchiara RF. Complication from a nasopharyngeal airway in a patient
with a basilar skull fracture. Anesthesiology 1991;74:366–8.
[19] Seebacher J, Nozik D, Mathieu A. Inadvertent intracranial introduction of a nasogastric tube, a
complication of severe maxillofacial trauma. Anesthesiology 1975;42:100–2.
[20] Hastings RH, Marks JD. Airway management for trauma patients with potential cervical spine
injuries. Anesth Analg 1991;73:471–82.
[21] Wood PR, Lawler PG. Managing the airway in cervical spine injury. A review of the Advanced
Trauma Life Support protocol. Anaesthesia 1992;47:792–7.
[22] Ovassapian A, Yelich SJ, Dykes MH, Brunner EE. Fiberoptic nasotracheal intubation—inci-
dence and causes of failure. Anesth Analg 1983;62:692–5.
[23] Criswell JC, Parr MJA. Emergency airway management in patients with cervical spine injuries.
Anaesthesia 1994;49:900–3.
[24] Sawin PD, Todd MM, Traynelis VC, Farrell SB, Nader A, Sato Y, et al. Cervical spine motion
with direct laryngoscopy and orotracheal intubation. An in vivo cinefluoroscopic study of
subjects without cervical abnormality. Anesthesiology 1996;85:26–36.
[25] Gerling MC, Davis DP, Hamilton RS, Morris GF, Vilke GM, Garfin SR, et al. Effects of
cervical spine immobilization technique and laryngoscope blade selection on an unstable cer-
vical spine in a cadaver model of intubation. Ann Emerg Med 2000;36:293–300.
[26] Hastings RH, Wood PR. Head extension and laryngeal view during laryngoscopy with cervical
spine stabilization maneuvers. Anesthesiology 1994;80:825–31.
[27] Bouma GJ, Muizelaar JP, Choi SC, Newlon PG, Young HF. Cerebral circulation and metab-
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 435

olism after severe traumatic brain injury: the elusive role of ischemia. J Neurosurg 1991;
75:685–93.
[28] Changaris DG,McGraw CP, Richardson JD, Garretson HD, Arpin EJ, Shields CB. Correlation of
cerebral perfusion pressure and Glasgow Coma Scale to outcome. J Trauma 1987;27:1007–13.
[29] Chesnut RM, Marshall LF, Klauber MR. The role of secondary brain injury in determining
outcome from severe head injury. J Trauma 1993;34:216–22.
[30] Marmarou A, Anderson RL, Ward JD, Choi SC, Young HF, Eisenberg HM, et al. Impact of ICP
instability and hypotension on outcome in patients with severe head trauma. J Neurosurg
1991;75:S59–66.
[31] Pietropaoli JA, Rogers FB, Shackford SR, Wald SL, Schmoker JD, Zhuang J. The deleterious
effects of intraoperative hypotension on outcome in patients with severe head injuries. J Trauma
1992;33:403–7.
[32] Dearden NM, McDowall DG. Comparison of etomidate and althesin in the reduction of in-
creased intracranial pressure after head injury. Br J Anaesth 1985;57:361–8.
[33] Butterworth JF, Bean VE, Royster RL. Sufentanil is preferable to etomidate during rapid-
sequence anesthesia induction for aortocoronary bypass surgery. J Cardiothorac Anesth
1989;3:396–400.
[34] Albanese J, Arnaud S, Rey M, Thomachot L, Alliez B, Martin C. Ketamine decreases intra-
cranial pressure and electroencephalographic activity in traumatic brain injury patients during
propofol sedation. Anesthesiology 1997;87:1328–34.
[35] Gardner AE, Dannemiller FJ, Dean D. Intracranial cerebrospinal fluid pressure in man during
ketamine anesthesia. Anesth Analg 1972;51:741–5.
[36] Takeshita H, Okuda Y, Sari A. The effects of ketamine on cerebral circulation and metabolism
in man. Anesthesiology 1972;36:69–75.
[37] Lanier WL, Milde JH, Michenfelder JD. Cerebral stimulation following succinylcholine in
dogs. Anesthesiology 1986;64:551–9.
[38] Marsh ML, Dunlop BJ, Shapiro HM, Gagnon RL, Rockoff MA. Succinylcholine-intracranial
pressure effects in neurosurgical patients. Anesth Analg 1980;59:550–1.
[39] Kovarik WD, Mayberg TS, Lam AM, Mathisen TL, Winn HR. Succinylcholine does not
change intracranial pressure, cerebral blood flow velocity, or the electroencephalogram in
patients with neurologic injury. Anesth Analg 1994;78:469–73.
[40] Sellick BA. Cricoid pressure to control regurgitation of stomach contents during induction of
anaesthesia [letter]. Lancet 1961;2:404–6.
[41] Donaldson WF III, Towers JD, Doctor A, Brand A, Donaldson VP. A methodology to evaluate
motion of the unstable spine during intubation techniques. Spine 1993;18:2020–3.
[42] Gabbott DA. The effect of single-handed cricoid pressure on neck movement after applying
manual in-line stabilisation. Anaesthesia 1997;52:586–8.
[43] Grande CM, Barton CR, Stene JK. Appropriate techniques for airway management of emer-
gency patients with suspected spinal cord injury. Anesth Analg 1988;67:714–5.
[44] Yentis SM. The effects of single-handed and bimanual cricoid pressure on the view at laryngo-
scopy. Anaesthesia 1997;52:332–5.
[45] Tommasino C, Moore S, Todd MM. Cerebral effects of isovolemic hemodilution with crystal-
loid or colloid solutions. Crit Care Med 1988;16:862–8.
[46] Zornow MH, Todd MM, Moore SS. The acute cerebral effects of changes in plasma osmolality
and oncotic pressure. Anesthesiology 1987;67:936–41.
[47] Bock JC, Barker BC, Clinton AG, Wilson MB, Lewis FR. Post-traumatic changes in, and effect
of colloid osmotic pressure on the distribution of body water. Ann Surg 1989;210:395–405.
[48] Schmoker JD, Shackford SR, Wald SL, Pietropacli JA. An analysis of the relationship between
fluid and sodium administration and intracranial pressure after head injury. J Trauma 1992;33:
476–81.
[49] Rosner MJ, Rosner SD, Johnson AH. Cerebral perfusion pressure: management protocol and
clinical results. J Neurosurg 1995;83:949–62.
[50] Gunnar W, Jonasson O, Merlotti G, Stone J, Barrett J. Head injury and hemorrhagic shock:
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439436

studies of the blood brain barrier and intracranial pressure after resuscitation with normal saline
solution, 3% saline solution, and dextran-40. Surgery 1988;103:398–407.
[51] Nguyen TT, Zwischenberger JB, Watson WC, Traber DL, Prough DS, Herndon DN, et al.
Hypertonic acetate dextran achieves high-flow-low-flow pressure resuscitation of hemorrhagic
shock. J Trauma 1995;38:602–8.
[52] DeWitt DS, Prough DS, Deal DD, Vines SM, Hoen H. Hypertonic saline does not improve
cerebral oxygen delivery after head injury and mild hemorrhage in cats. Crit Care Med
1996;24:109–17.
[53] Fresh Frozen Plasma, Cryoprecipitate, and Platelets Administration Guidelines Development
Task Force of the College of American Pathologists. Practice parameter for the use of fresh-
frozen plasma, cryoprecipitate, and platelets. JAMA 1994;271:777–81.
[54] Stehling L, Luban NLC, Anderson KC, Sayers MH, Long A, Attar S. Guidelines for blood
utilization review. Transfusion 1994;34:438–48.
[55] Cully MD, Larson CP, Silverberg GD. Hetastarch coagulopathy in a neurosurgical patient.
Anesthesiology 1987;66:706–7.
[56] Strauss RG, Stump DC, Henriksen RA, Saunders R. Effects of hydroxyethyl starch on fibri-
nogen, fibrin clot formation, and fibrinolysis. Transfusion 1985;25:230–4.
[57] Velanovich V. Crystalloid versus colloid fluid resuscitation: a meta-analysis of mortality. Sur-
gery 1989;105:65–71.
[58] Schierhout G, Roberts I. Fluid resuscitation with colloid or crystalloid solutions in critically ill
patients: a systematic review of randomised trials. BMJ 1998;316:961–4.
[59] Cole DJ, Drummond JC, Patel PM, Nary JC, Applegate RL II. Effect of oncotic pressure of
diaspirin cross-linked hemoglobin (DCLHbTM) on brain injury after temporary focal cerebral
ischemia in rats. Anesth Analg 1996;83:342–7.
[60] Sloan EP, Koenigsberg M, Gens D, Cipolle M, Runge J, Mallory MN, et al. Diaspirin cross-
linked hemoglobin (DCLHb) in the treatment of severe traumatic hemorrhagic shock: a
randomized controlled efficacy trial. JAMA 1999;282:1857–64.
[61] Lam AM, Winn HR, Cullen BF, Sundling N. Hyperglycemia and neurological outcome in
patients with head injury. J Neurosurg 1991;75:545–51.
[62] Pulsinelli WA, Levy DE, Sigsbee B, Scherer P, Plum F. Increased damage after ischemic stroke
in patients with hyperglycemia with or without established diabetes mellitus. Am J Med
1983;74: 540–4.
[63] Pulsinelli WA, Waldman S, Rawlinson D, Plum F. Moderate hyperglycemia augments ischemia
brain damage: a neuropathologic study in the rat. Neurology 1982;32:1239–46.
[64] Rosner MJ. Introduction to cerebral perfusion pressure management. Neurosurg Clin N Am
1995;6:761–73.
[65] Overgaard J, TweedWA.Cerebral circulation after head injury. Part 1: CBF and its regulation after
closed head injury with emphasis on clinical correlations. J Neurosurg 1974;41:531–41.
[66] Lewelt W, Jenkins LW, Miller JD. Autoregulation of cerebral blood flow after experimental
fluid percussion injury of the brain. J Neurosurg 1980;53:500–11.
[67] DeWitt DS, Prough DS, Taylor CL, Whitley JM. Reduced cerebral blood flow, oxygen delivery,
and electroencephalographic activity after traumatic brain injury and mild hemorrhage in cats.
J Neurosurg 1992;76:812–21.
[68] Bouma GJ, Muizelaar JP, Stringer WA, Choi SC, Fatouros P, Young HF. Ultra-early evaluation
of regional cerebral blood flow in severely head-injured patients using xenon-enhanced com-
puterized tomography. J Neurosurg 1992;77:360–8.
[69] Bouma GJ, Muizelaar JP. Cerebral blood flow, cerebral blood volume, and cerebrovascular
reactivity after severe head injury. J Neurotrauma 1992;9:S333–48.
[70] Kontos HA, Wei EP, Dietrich WD, Navari RM, Povlishock JT, Ghatak NR. Mechanism of
cerebral arteriolar abnormalities after acute hypertension. Am J Physiol 1981;240:H511–27.
[71] Bouma GJ, Muizelaar JP, Bandoh K, Marmarou A. Blood pressure and intracranial pressure-
volume dynamics in severe head injury: relationship with cerebral blood flow. J Neurosurg
1992;77:15–9.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 437

[72] Lundberg N, Kjallquist A, Bien C. Reduction of increased intracranial pressure by hyperventi-
lation. Acta Psychiatr Neurol Scand 1959;34(Suppl):5–57.
[73] Michenfelder JD, Theye RA. The effects of profound hypocapnia and dilutional anemia on
canine cerebral metabolism and blood flow. Anesthesiology 1969;31:449–57.
[74] Harp JR, Wollman H. Cerebral metabolic effects of hyperventilation and deliberate hypoten-
sion. Br J Anaesth 1973;45:256–62.
[75] Patel VM, Maulsby RL. How hyperventilation alters the electroencephalogram: a review of
controversial viewpoints emphasizing neurophysiological mechanisms. J Clin Neurophysiol
1987;4:101–20.
[76] Cold GE. Does acute hyperventilation provoke cerebral oligaemia in comatose patients after
acute head injury? Acta Neurochir 1989;96:100–6.
[77] Enevoldsen EM, Jensen FT. Autoregulation and CO2 responses of cerebral blood flow in
patients with acute severe head injury. J Neurosurg 1978;48:689–703.
[78] Muizelaar JP, Marmarou A, Ward JD, Kontos HA, Choi SC, Becker DP. Adverse effects of
prolonged hyperventilation in patients with severe head injury: a randomized clinical trial. J
Neurosurg 1991;75:731–9.
[79] Zornow MH, Prough DS. Fluid management in patients with traumatic brain injury. New Horiz
1995;3:488–97.
[80] Hartwell RC, Sutton LN. Mannitol, intracranial pressure, and vasogenic edema. Neurosurgery
1993;32:444–50.
[81] Cooper PR, Moody S, Clark WK, Kirkpatrick J, Maravilla K, Gould AL, et al. Dexamethasone
and severe head injury. A prospective double-blind study. J Neurosurg 1979;51:307–16.
[82] Bracken MB, Shepard MJ, Holford TR, Leo-Summers L, Aldrich EF, Fazl M, et al. Admin-
istration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the
treatment of acute spinal cord injury. Results of the Third National Acute Spinal Cord Injury
Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:
1597–604.
[83] Penn RD, Walser R, Ackerman L. Cerebral blood volume in man: computer analysis of a
computerized brain scan. JAMA 1975;234:1154–5.
[84] Kontos HA, Wei EP, Navari RM. Responses of cerebral arteries and arterioles to acute hypo-
tension and hypertension. Am J Physiol 1978;234:H371–83.
[85] Grubb RL Jr., Raichle ME, Eichling JO, Ter-Pogossian MM. The effects of changes in PaCO2
on cerebral blood volume, blood flow, and vascular mean transit time. Stroke 1974;5:630–9.
[86] Cruz J, Miner ME, Allen SJ, Alves WM, Gennarelli TA. Continuous monitoring of cerebral
oxygenation in acute brain injury: assessment of cerebral hemodynamic reserve. Neurosurgery
1991;29:743–9.
[87] Artru AA, Merriman HG. Hypocapnia added to hypertension to reverse EEG changes during
carotid endarterectomy. Anesthesiology 1989;70:1016–8.
[88] Waltz AG, Sundt TM Jr, Michenfelder JD. Cerebral blood flow during carotid endarterectomy.
Circulation 1997;45:1091–6.
[89] De Deyne C, Van Aken J, Decruyenaere J, Struys M, Colardyn F. Jugular bulb oximetry: review
on a cerebral monitoring technique. Acta Anaesthesiol Belg 1998;49:21–31.
[90] Matta BF, Lam AM, Mayberg TS. The influence of arterial oxygenation on cerebral venous
oxygen saturation during hyperventilation. Can J Anaesth 1994;41:1041–6.
[91] Thiagarajan A, Goverdhan PD, Chari P, Somasunderam K. The effect of hyperventilation and
hyperoxia on cerebral venous oxygen saturation in patients with traumatic brain injury. Anesth
Analg 1998;87:850–3.
[92] Pollard V, Prough DS, DeMelo AE, Devo DJ, Uchida T, Stoddart HF. Validation in volunteers
of a near-infrared spectroscope for monitoring brain oxygenation in vivo. Anesth Analg 1996;
82:269–77.
[93] Pollard V, Prough DS, DeMelo AE, Devo DJ, Uchida T, Widman R. The influence of carbon
dioxide and body position on near-infrared spectroscopic assessment of cerebral hemoglobin
oxygen saturation. Anesth Analg 1996;82:278–87.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439438

[94] Gopinath SP, Robertson CS, Contant CF, Hayes C, Feldman Z, Narayan RK, et al. Jugular
venous desaturation and outcome after head injury. J Neurol Neurosurg Psychiatry 1994;
57:717–23.
[95] Muizelaar JP, Bouma GJ, Levasseur JE, Kontos HA. Effect of hematocrit variations on cerebral
blood flow and basilar artery diameter in vivo. Am J Physiol 1992;262:H949–54.
[96] Muizelaar JP, Wei EP, Kontos HA, Becker DP. Cerebral blood flow is regulated by changes in
blood pressure and in blood viscosity alike. Stroke 1986;17:44–8.
[97] Brown MM, Marshall J. Regulation of cerebral blood flow in response to changes in blood
viscosity. Lancet 1985;1:604–9.
[98] Burke AM, Quest DO, Chien S, Cerri C. The effects of mannitol on blood viscosity. J Neuro-
surg 1981;55:550–3.
[99] Johnston IH, Harper AM. The effect of mannitol on cerebral blood flow. J Neurosurg 1973;38:
461–71.
[100] Muizelaar JP, Lutz HA III, Becker DP. Effect of mannitol on ICP and CBF and correlation with
pressure autoregulation in severely head-injured patients. J Neurosurg 1984;61:700–6.
[101] Muizelaar JP, Wei EP, Kontos HA, Becker DP. Mannitol causes compensatory cerebral vaso-
constriction and vasodilation in response to blood viscosity changes. J Neurosurg 1983;59:
822–8.
[102] Illievich UM, Petricek W, Schramm W, Weindlmaur-Goettel M, Czech T, Spiss CK. Electro-
encephalographic burst suppression by propofol infusion in humans: hemodynamic consequen-
ces. Anesth Analg 1993;77:155–60.
[103] Todd MM, Weeks JB, Warner DS. The influence of intravascular volume expansion on cerebral
blood flow and blood volume in normal rats. Anesthesiology 1993;78:945–53.
[104] Feldman Z, Kanter MJ, Robertson CS, Contant CF, Hayes C, Sheinberg MA, et al. Effect of
head elevation on intracranial pressure, cerebral perfusion pressure, and cerebral blood flow in
head-injured patients. J Neurosurg 1992;76:207–11.
[105] Mavrocordatos P, Bissonnette B, Ravussin P. Effects of neck position and head elevation on
intracranial pressure in anaesthetized neurosurgical patients: preliminary results. J Neurosurg
Anesthesiol 2000;12:10–4.
[106] Rosner MJ, Coley IB. Cerebral perfusion pressure, intracranial pressure, and head elevation.
J Neurosurg 1986;65:636–41.
[107] Williams MD, Rainer WG, Fieger HG Jr, Murray IP, Sanchez ML. Cardiopulmonary bypass,
profound hypothermia, and circulatory arrest for neurosurgery. Ann Thorac Surg 1991;52:
1069–75.
[108] Clifton GL, Allen S, Barrodale P, Plenger P, Berry J, Koch S. A phase II study of moderate
hypothermia in severe brain injury. J Neurotrauma 1993;10:263–71.
[109] Clifton GL, Jiang JY, Lyeth BG, Jenkis LW, Hamm RJ, Hayes RL. Marked protection by
moderate hypothermia after experimental traumatic brain injury. J Cereb Blood Flow Metab
1991;11:114–21.
[110] Marion DW, Penrod LE, Kelsey SF, Obrist WD , Kochanek PM, Palmer AM, et al. Treatment
of traumatic brain injury with moderate hypothermia. N Engl J Med 1997;336:540–6.
[111] Phelps C. Principles of treatment. In: Traumatic Injuries of the Brain and its Membranes: with a
special study of Pistol-shot wounds of the head in their medico-legal and surgical relations.
New York: D. Appleton & Co. 1897. p. 206–32.
[112] Teasdale G, Jennett B. Assessment of coma and impaired consciousness: a practical scale.
Lancet 1974;2:81–4.
[113] Jaggi JL, Obrist WD, Gennarelli TA, Langfitt TW. Relationship of early cerebral blood flow
and metabolism to outcome in acute head injury. J Neurosurg 1990;72:176–82.
[114] Chesnut RM. Secondary brain insults after head injury: clinical perspectives. New Horiz
1995;3:366–75.
[115] Michenfelder JD. The awake brain. In: Michenfelder JD, editor. Anesthesia and the Brain:
Clinical, Functional, Metabolic, and Vascular Correlates. New York: Churchill Livingstone;
1988. p. 3–21.
E. Bedell, D.S. Prough / Anesthesiology Clin N Am 20 (2002) 417–439 439

Current concepts in neurocritical care
Brenda G. Fahy, MD*, Vadivelu Sivaraman, MDDepartment of Anesthesiology, University of Maryland Medical System, 22 S. Greene Street,
Suite S11C00, Baltimore, MD 21201, USA
Stroke
Stroke is the third leading cause of death and the leading cause of adult
disability in the United States. The National Institute of Neurological Disorders
and Stroke defines stroke as sudden loss of brain function resulting from an
interference with brain blood supply. This includes both ischemic and hemor-
rhagic insults with ischemic stroke predominant (85%). Subarachnoid hemorrhage
(SAH), with its specialized management, will be covered in the next section. Once
only supportive, therapy for acute ischemic stroke now includes therapeutic
options with tissue plasminogen activator (tPA).
Acute vascular occlusion, although rarely complete, limits oxygen and glucose
delivery to that respective region of the brain. This results in a core area of tissue
that infarcts almost immediately due to lack of blood and nutrient supply with a
surrounding area of ischemic penumbra. The penumbra may not result in tissue
infarction if ischemia can be reversed. Medical interventions target the potentially
salvageable brain tissue.
Intracranial hemorrhage (ICH), although less frequent than ischemic stroke, has
a high mortality rate due to the extent of cerebral damage. Thrombolytics and
anticoagulation are contraindicated with recent ICH. The mainstays of therapy
include blood pressure management (as hypertensive disease is common), in-
tracranial pressure (ICP) control, and optimization of cerebral perfusion. A de-
cision for emergent surgical evacuation should be made in consultation with
neurosurgery. These patients may require intraventricular catheter (IVC) place-
ment for ICP monitoring and cerebrospinal fluid (CSF) drainage.
Because time is crucial to minimize tissue death, there must be rapid as-
sessment of the stroke patient including neurologic and physical examination and
general medical assessment. It is crucial to establish the timing of the onset of
stroke symptoms for possible administration of tPA. A head CT should be per-
formed to rule out ICH, but this stage rarely shows ischemic changes. Although
0889-8537/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0889 -8537 (01 )00011 -6
* Corresponding author.
E-mail address: [email protected] (B.G. Fahy).
Anesthesiology Clin N Am
20 (2002) 441–462

not a complete neurologic examination, the National Institute of Health Stroke
Scale Score (NIH-SSS) [1] (Table 1) utilizes a standardized scale to indicate the
severity of neurological dysfunction.
Table 1
NIH-SSS [1]
Level of consciousness (LOC) Alert 0
Drowsy 1
Stuporous 2
Coma 3
LOC questions (month and age) Answers both correctly 0
Answers one correctly 1
Incorrect 2
LOC commands (close eyes, make fist) Obeys both correctly 0
Obeys one correctly 1
Incorrect 2
Best gaze Normal 0
Partial gaze palsy 1
Forced deviation 2
Visual No visual loss 0
Partial hemianopia 1
Complete hemianopia 2
Bilateral hemianopia 3
Facial palsy Normal 0
Minor paresis 1
Partial paresis 2
Complete palsy 3
Best motor (repeat for each arm and leg) No drift 0
Drift 1
Can’t resist gravity 2
No effort against gravity 3
Limb ataxia Absent 0
Present in upper or lower 1
Present in both 2
Sensory Normal 0
Partial loss 1
Dense loss 2
Dysarthria Normal articulation 0
Mild to moderate dysarthria 1
Near unintelligible or worse 2
Mute 3
Best language No aphasia 0
Mild to moderate aphasia 1
Severe aphasia 2
Mute 3
Change from previous exam Same 0
Better 1
Worse 2
Change from baseline Same 0
Better 1
Worse 2
Abbreviation: NIH-SSS, National Institute of Health Stroke Severity Score.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462442

During patient evaluation measures should be instituted to optimize blood
flow. Hypertension is common in acute stroke, and should be treated cautiously
to prevent cerebral ischemia. Treatment exceptions include hypertension asso-
ciated with ICH and during the period surrounding tPA administration in
ischemic strokes. The American Heart Association has established blood pressure
guidelines (Table 2). Blood pressure should not exceed 185/110 at the time of tPA
Table 2
Therapy guidelines for thrombolytic candidates
Blood pressure (mmHg) Treatment
Pretreatment SBP > 185
or DBP >110
Nitroglycerin paste or 1 to 2 doses of intravenous labetalol,
10 to 20 mg each. If these do not reduce blood pressure to
< 185/110 mm Hg over 1 h, the patient should not be treated
with rtPA.
During and after Thrombolytics
Monitor BP Every 15 minutes x 2 hours, then 30 minutes for 6 hours,
then hourly x 16 hours
SBP: 180–230 or
DBP: 105–130
Labetalol, 10 mg IV over 1–2 min, repeat or double every
10–20 min; total maximum dose 150 mg
SBP >230 or
DBP: 121–140
Use labetalol, 10 mg IV over 1–2 min, repeat or double every
10 min, to a maximum of 150 mg
DBP >140 Sodium nitroprusside with continuous blood pressure monitoring
Abbreviations: BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Table 3
Inclusion and exclusion criteria for use of thrombolysis in acute ischemic stroke
Inclusion criteria
Ischemic stroke with a measurable defect on NIHSSS
Clearly defined time of onset within 3 h of the start of treatment
Age >18 y
Exclusion criteria
Contraindications include:
Evidence of intracranial hemorrhage on pretreatment CT scan
Suspicion of SAH, even if CT scan normal
Known arteriovenous malformation, aneurysm, or intracranial neoplasm
Prior intracranial hemorrhage
Intracranial or spinal surgery, serious head injury, or prior stroke in previous 3 mos
Active internal bleeding
Known bleeding diathesis including but not limited to: a) platelet count <100,000/mm3, (b)
prothrombin time >15 seconds, (c) international normalized ratio >1.7, (d) current use of oral
anticoagulants; (e) use of heparin within 48 h and prolonged partial thromboplastin time
Uncontrolled blood pressure at time of treatment (refer to Table 2)
Recent (in previous 3 months): intracranial surgery, serious head trauma, or previous stroke
Major surgery (in past 14 days)
Pregnancy
Seizure at stroke onset
Abbreviations: NIHSSS, National Institute of Health Stroke Severity Score; SAH, subarachnoid
hemorrhage.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 443

treatment [2]. Hypotension, or relative hypotension in a hypertensive patient,
should be treated aggressively and an etiology sought. Cerebral blood flow
during stroke is blood pressure dependent. Hypotension must be reversed to
prevent further ischemia with subsequent infarction.
Intravenous tPA is the only Federal Drug Administration approved primary
treatment for acute ischemic stroke, and must be started within 3 hours of stroke
onset. Appropriate indications and contraindications are detailed in Table 3. The
most serious tPA complication is ICH. The risk of ICH after tPA increases with
higher NIH-SSS scores [1]. Chronic anticoagulation in patients with atrial
fibrillation is clearly warranted [3]. A comprehensive review of all therapies
following acute stroke management is beyond the scope of this paper, and has
been reviewed elsewhere [4].
Other neurologic complications following stroke include seizure and uncon-
trolled ICP. Seizures occur in 5% of strokes, usually with large strokes or cortical
involvement. No evidence exists for prophylactic anticonvulsants; however, sei-
zures can be treated acutely with benzodiazepines followed by phenytoin. Uncon-
trolled ICP is the leading cause of death in the first week following stroke. ICP
measurements may be helpful with acutely deteriorating patients and help guide
therapy. If an IVC is placed for ICP monitoring, it can permit therapeutic CSF
drainage. Other therapeutic measures include elevating the head of the bed and
hyperosmolar therapy with mannitol. Hyperventilation should be instituted cau-
tiously due to concerns of worsening cerebral ischemia by hypocapnia-induced ce-
rebral vasoconstriction decreasing cerebral blood flow. High-dose barbiturates may
be used with uncontrolled ICP refractory to other therapies. Appropriate intensive
supportive care must assure maintenance of hemodynamic stability during high-
dose barbiturates. Decompressive craniectomy has been used with intracranial hy-
pertension in hemispheric infarctions [5], but its value requires further clarification.
Medical complications are common following stroke. Coronary artery disease
is present in a majority of stroke patients. Monitoring for detection and treatment
of myocardial ischemia and infarction, arrhythmias, and congestive heart failure
is warranted. Pulmonary complications include pneumonia, which can occur with
dysphagia when oropharyngeal contents are aspirated. Stroke patients have a high
risk of deep venous thrombosis (DVT), and may develop a pulmonary embolism
(PE). Current prophylaxis recommendations in ischemic stroke for DVT and PE
include low-dose unfractionated heparin, low molecular weight heparin, or
danaparoid [6]. If anticoagulation is contraindicated, elastic stockings (ES) and
intermittent pneumatic calf compression (IPC) can be used. Hyperthermia in the
poststroke period increases morbidity and mortality [7]. Fever increases brain
metabolic demand, and should be avoided following stroke.
Subarachnoid hemorrhage
Nontraumatic subarachnoid hemorrhage (SAH) occurs in an estimated 30,000
Americans each year. Despite recent diagnostic and treatment advances, 25% of
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462444

SAH patients will die, and 50% of survivors will suffer significant morbidity [8].
These patients require intensive care unit admission for neurologic observation
and cardiopulmonary monitoring. The majority of SAH patients will have a
cerebral aneurysm. [9]. SAH therapy is aimed at prevention and early detection of
neurologic complications, and treatment of medical complications.
Neurologic complications include rebleeding, hydrocephalus, seizure, and cere-
bral vasospasm. The most immediate concern is the risk of rebleeding with a mor-
tality rate of 70%. The risk of rebleeding is 4% during the first 24 hours and 1–2%
per day during the following 4 weeks [ 10]. Because rebleeding rates are increased
with high systolic blood pressure, simple treatment measures include blood
pressure management, adequate pain control, and stool softeners until the aneu-
rysm is secured. Early securing of the aneurysm is important not only to prevent
rebleeding but also to allow more therapeutic options for subsequent cerebral
vasospasm [11]. Antifibrinolytic therapy is no longer recommended because it
increased secondary ischemia risk [12] and failed to improve outcome [13].
Acute hydrocephalus occurs in approximately 25% of patients after initial SAH,
and can impair consciousness. Treatment is CSF drainage via an IVC. Over-
drainage of CSF should be avoided, as it increases the risk of rebleed and cerebral
vasospasm [14]. Blood in the ventricular system can obstruct the CSF drainage and
absorption. Some SAH patients will require permanent shunt procedures following
IVC drainage.
Seizures occur in approximately 10% to 20% of patients with SAH, typically in
the first 24 hours. Seizures may increase cerebral blood flow, potentially causing a
rebleed. Respiratory compromise may occur with resultant hypoxemia. To prevent
these complications, prophylactic intravenous phenytoin therapy is administered.
Cerebral vasospasm following SAH is the most significant cause of mortality
and morbidity in survivors of the initial SAH [9]. Cerebral vasospasm is an is-
chemic neurologic deficit associated with focal narrowing of intracranial arteries.
Although the amount of SAH initially visualized on the CT scan is related to
vasospasm [15], the pathogenic mechanisms of cerebral vasospasm need to be
better defined. This is due to the complex nature of the pathophysiology of
vasospasm and difficulty with its reproduction in animal models [16]. Blood
products, especially oxyhemoglobin, have long been accepted as contributors to
cerebral vasospasm [17]. More recent studies have examined oxyhemoglobin as an
initiator of arterial wall contraction during cerebral vasospasm [18]. Although not
completely elucidated, it has been postulated that cerebral vasospasm may result
from oxyhemoglobin through a variety of pathways including arterial muscle
fibers effects, local release of vasoactive compounds from the arterial wall,
superoxide free radical production, and increased activity of lipid peroxidases.
Cerebral vasospasm usually begins 4 days following SAH, peaks at 7–10 days,
and may continue for several weeks [19]. Transcranial doppler studies with ele-
vated velocities can identify potential vasospasm. Angiography, however, is the
gold standard for confirming the diagnosis of cerebral vasospasm. Clinical signs
of vasospasm may manifest as altered level of consciousness or focal neurologic
deficits over the course of minutes to hours. Because the neurologic signs can be
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 445

subtle (pronator drift or slight change in consciousness level), serial neurologic
examinations are crucial. The specific neurologic signs manifested will depend
on the location of vasospasm and whether collateral circulation exists. Any acute
neurologic deterioration needs to be investigated to rule out other etiologies in-
cluding ICH and hydrocephalus.
Early recognition and treatment of the potentially reversible ischemic deficit of
vasospasm is the key. Delaying therapy until the appearance of a significant
neurologic deficit may result in cerebral infarction. Clinical signs of vasospasm
occur in approximately 30% of SAH, while angiographic evidence may occur in
up to 70% [20].
Currently, hypervolemia, hemodilution, and hypertension therapy (HHH) are
the main therapies for cerebral ischemia secondary to cerebral vasospasm. During
cerebral vasospasm, cerebral blood flow regulation is assumed to become
pressure dependent [21]. Hypovolemia occurs after SAH [22], correlating with
symptomatic vasospasm [23]. Hypervolemic therapy with volume expansion has
reversed neurologic deficits and increased cerebral blood flow. The resultant
hemodilution as a result of hypervolemia therapy theoretically decreases blood
viscosity, improving circulation to the ischemic area. After securing of the
aneurysm to prevent the risk of a rebleed, hypertensive therapy becomes an
additional option to improve pressure-dependent cerebral blood flow. Despite its
widespread use, there is only one prospective randomized study of hypervolemic
therapy involving 30 hypertensive patients with SAH [24]. They were random-
ized to begin volume expansion and antihypertensive therapy with vasodilators
and centrally acting drugs compared to controls that received diuretics. The
incidence of vasospasm and mortality was significantly higher in the group
treated with diuretics without volume expansion.
Several reports from studies describe improvement in neurologic deficits with
elevating blood pressure, augmenting cardiac output, volume replacement, and/or
hemodilution [25–27] when compared with historic controls. There were no
control groups for these studies. However, studies have yet to determine which
component(s) of HHH are most critical. Potential complications include pulmo-
nary edema, myocardial ischemia, hemorrhagic infarction, and worsening cereb-
ral edema [28].
Calcium antagonists usage to prevent or treat cerebral ischemia was based on
the assumption that these drugs counteracted calcium influx in the vascular
smooth. A meta-analysis of all published randomized nimodipine confirmed the
benefit of prophylactic nimodipine in reducing neurologic deficits, cerebral
infarction, and mortality, and improving outcome secondary to vasospasm [29].
Nimodipine, 60 mg orally every 4 hours for 21 days, usually is well tolerated, and
may cause a mild degree of hypotension. It is one of the corner stones of therapy
for prophylaxis against vasospasm. Another calcium antagonist, nicardipine,
failed to show prophylactic benefit, and had side effects including hypotension,
pulmonary edema, and renal failure [30]. The calcium antagonist, fausidil
hydrochloride, in a prospective randomized trial reduced angiographic and
symptomatic vasospasm with improved outcomes [31].
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462446

Endovascular treatment for vasospasm with balloon angioplasty or selective
arterial injection of vasodilators such as papaverine may improve neurologic
symptoms when other medical therapies have failed.
Lysis of the intracisternal blood clot by injection of intracisternal recombinant
tPA has been shown to decrease angiographic and symptomatic vasospasm but not
outcome [32]. One study suggested a nonstatistical trend toward decreased
occurrence of severe vasospasm with intracisternal recombinant tPA [33].
Tirilizad, a 21-aminosteroid, inhibits lipid peroxidation and prevented cerebral
vasospasm in an SAH animal model [34]. A European-Australian multicenter
study showed tirilizad mesylate at 6 mg/kg was associated with better neurologic
outcomes and reduced mortality versus controls [35]. However, it was felt that
anticonvulsant therapy may increase drug clearance, and women received less
benefit due to increased metabolism. However, the beneficial effects could not be
reproduced in the North American Study [36] or in two additional trials with a
higher dose (15 mg/kg) [37,38].
Other drugs tested clinically include the hydroxyl radical scavenger, nicara-
ven. It decreased symptomatic vasospasm; but did not alter outcome at 3 months
[39]. Ebselen, a seleno-organic compound that inhibits lipid peroxidation,
improved 3-month outcome without effecting symptomatic vasospasm [40].
Decreased nitric oxide (NO) activity may play a role in the pathogenesis of
vasospasm. Preliminary data with intrathecal administration of NO donors such
as sodium nitroprusside to a small group of patients with clinical or radiographic
evidence of Grade III SAH (Table 4) resulted in 12 of 15 having at least a good or
better outcome. Intrathecal sodium nitroprusside was also prophylactically
administered to 10 patients with Grade III SAH; none developed vasospasm
[41]. Side effects included three hypotensive episodes and frequent nausea.
Medical complications following SAH are common, and are responsible for
23% of deaths [42]. Sepsis and pneumonia occur in 14.8% of patients [43]. Due
to an inability to protect the airway, this patient population is prone to aspiration
and subsequent pneumonia. Aggressive pulmonary hygiene to prevent atelec-
tasis and antibiotics for bacterial pneumonia may be necessary. Neurogenic
pulmonary edema [44] and non-neurogenic pulmonary edema may occur
following SAH. Therapy includes inotropic support, if indicated, and gentle
diuresis due to concerns over maintaining adequate volume status with the risk
of cerebral vasospasm.
Table 4
Hunt and Hess Scale for Subarachnoid Hemorrhage
Grade Neurological status
I Asymptomatic
II Severe headache or nuchal rigidity; no neurological deficit
III Drowsy; minimal neurological deficit
IV Stuporous; moderate to severe hemiparesis
V Deep coma; decerebrate posturing
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 447

Cardiac arrhythmias are frequent following SAH including sinus tachycardia or
bradycardia, ventricular or atrial extrasystole, and atrial fibrillation. Life threat-
ening arrhythmias (asystole, AV block) occur 5% of the time. EKG abnormalities
and cardiac enzyme elevations [creatine kinase (CPK) or troponin] are frequent
following SAH. In a small retrospective series of 72 patients, nine patients had
echocardiographic wall motion abnormalities. All were Grade III–IV (Table 4); all
had CPK mb >2% [45]. There is currently no large prospective study examining
cardiac enzyme elevation and echocardiographic changes.
Hyponatremia is common after SAH, typically developing several days after
hemorrhage. In the general medical population the etiology is often the syndrome
of inappropriate antidiuretic hormone secretion (SIADH), necessitating fluid
restriction. However, in the SAH population, there is evidence that cerebral salt
wasting causing hypovolemia, and sodium depletion can occur following SAH
[22]. Due to concerns over hypovolemia aggravating cerebral vasospasm, appro-
priate therapy for cerebral salt wasting includes sodium and fluid replacement.
DVT (incidence 1% to 5%) and PE (incidence 0.8%) can occur following
SAH. During the acute phase these patients are not candidates for anticoagulation
due to recent SAH and often recent cranial surgery. ES or IPC can be used. If
diagnosed with DVT or PE, an inferior vena caval filter can be placed.
New potential monitoring modalities for SAH patients may include intra-
cerebral microdialysis. These microdialysis catheters inserted in the cortex at the
end of aneurysm surgery can measure markers of cellular injury and ischemia as
well as neurotransmitters. During bedside microdialysis monitoring in a small
series of SAH patients, impending ischemia was signaled by changes in lactate
and glutamate, while increases in glycerol were associated with ischemic deficits
[46]. This early detection of impending ischemia may lead to earlier intervention
and prevention of cerebral infarction.
Traumatic brain injury
Each year in theUnited States, traumatic brain injury (TBI) causes 52,000 deaths
and 80,000 permanent severe disability, and is themost common cause of death and
disability in young people. If TBI causes coma, there is a significant risk of
hypotension, hypoxia, and intracranial hypertension. Any of these sequelae can
exacerbate the degree of neurologic injury or cause death.
Although primary injury occurs at the moment of impact, secondary injury
due to the physiologic and metabolic processes caused by the primary injury
occurs later. Secondary injury processes at the cell level may include calcium
toxicity, lipid peroxidation, free radical generation, and excitatory neurotrans-
mitter release [47].
Secondary brain injury is the primary cause of hospital deaths after TBI.
Within hours of injury, vasogenic fluid accumulates in the brain, causing cerebral
edema. This causes an increase in ICP, allowing cerebral ischemia to occur at a
lower blood pressure threshold. Numerous pharmacologic agents including free
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462448

radical scavengers, antagonists of excitatory neurotransmitters, and calcium
channel antagonists have been investigated to attempt to block the secondary
injury resulting from TBI. Efficacy remains to be proven [47].
Secondary insults to the brain caused by hypoxemia and hypotension can
worsen outcome [48]. To decrease theses risks, attention must be given to airway,
breathing, and circulation. TBI patients may present with other traumatic injuries
such as a pneumothorax, hemothorax, or flail chest that require treatment to
prevent hypoxemia. Airway protective reflexes may be absent with impaired
consciousness. Appropriate establishment of an airway if needed is of paramount
importance. Patients with a Glasgow Coma scale (see Table 5) of 8 or less are
unable to protect their airway, and should be endotracheally intubated to prevent
hypoxemia. Endotracheal intubation of these patients decreases the mortality
significantly [49]. An orotracheal tube placement is usually preferred until a
basilar skull fracture can be excluded due to possible brain entry via the cribiform
plate with nasal placement. TBI patients are prone to aspiration pneumonia, and
should receive aggressive pulmonary toilet and appropriate antibiotics if bacterial
pneumonia ensues.
Hypotension needs to be prevented to decrease the risk of secondary brain
insult. A single episode of 90 mmHg or less systolic blood pressure with TBI
worsens outcome [48]. If hypotension cannot be prevented, diagnosis and
treatment should be rapid.
Table 5
Glasgow Coma Scale (GCS)
Criteria points awarded best eye opening
Spontaneously 4
To speech 3
To pain 2
None 1
Best verbal response
Oriented 5
Confused 4
Inappropriate 3
Incomprehensible 2
None 1
Best motor response
Obeys commands 6
Localized pain 5
Withdraws 4
Flexion to pain 3
Extension to pain 2
None 1
The highest level of response in each command is recorded and the sum of the three categories
provides the GCS.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 449

The most significant cause of morbidity and mortality in TBI who survive to
hospitalization is uncontrolled intracranial hypertension [50]. As already ad-
dressed above, initial management should be directed to opening, protecting,
and maintaining the airway to prevent hypoxia and the deleterious effects of hy-
percarbia. If the patient has a clear cervical spine, the head of the bed may be
elevated to improve cerebral venous drainage. Although static, CT scanning
rapidly shows pathology and allows immediate intervention. CT scan signs of
elevated ICP include midline shift, compression or obliteration of mesencephalic
cisterns and the presence of subarachnoid blood (Fig. 1) [51]. ICP monitoring to
allow appropriate interventions is vital. Indications for ICP monitoring include
Fig. 1. CT scan illustrating hemorrhage with obliteration of mesencephalic cisterns and right to left
midline shift. (From Prys-Roberts C, Brown Burnell R Jr. International Practice of Anesthesia; 2(4),
2/125/2 and 2/125/3; reprinted by permission of ButterworthHeinemann, a division of Reed Educational
& Professional Publishing Ltd.)
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462450

Glasgow Coma Score of 8 or less and lesions prone to cerebral edema. Several
continuous ICP monitoring devices are illustrated in the following diagram
(Fig. 2), with advantages and disadvantages listed in Table 6. The most reliable
for CSF drainage and ICP measurement is the IVC. The intraparenchymal
Fig. 2. Intracranial pressure monitoring sites. (From Prys-Roberts C, Brown Burnell R Jr. International
Practice of Anesthesia; 2(4), 2/125/2 and 2/125/3; reprinted by permission of Butterworth Heinemann,
a division of Reed Educational & Professional Publishing Ltd.)
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 451

fiberoptic ICP monitoring system (Fig. 3) measures brain tissue pressure that has
been shown to correlate well with ventricular pressure [52].
After correction of hypoxia and hypercarbia and proper positioning, if possible,
to improve central venous drainage, ICP therapy involves elevation of serum
osmolality (300 mosmol/kg approximately) by the use of osmotic diuretics or loop
diuretics. The administration of mannitol should ideally occur with consultation of
the neurosurgical team in TBI. If intracranial bleeding is present, mannitol may
allow an intracerebral hematoma to expand by shrinking healthy brain tissue. In
the pediatric population, hyperemia often causes diffuse swelling, and mannitol
may further elevate ICP by increasing cerebral blood volume.
Because of concerns that large doses of mannitol may cause a reverse
osmotic gradient by removing so much tissue water that water and mannitol are
Table 6
Intracranial pressure monitor comparison
IVC SAB Fibreoptic
Accuracy ± ± ± ± ± ± ± ±
CSF drainage ± ± ± ± ± ± �Infection potential ± ± ± ± ± ± ± ± ±
Recalibration possible ± ± ± ± ± ± ± �Brain tissue disruption ± ± ± ± � ± ± ±
Abbreviations: CSF, cerebrospinal fluid; IVC, Intraventricular catheter; SAB, subarachnoid bolt,
Fig. 3. Fiberoptic Camino Intracranial Pressure Monitoring System. (From Prys-Roberts C, Brown
Burnell R Jr. International Practice of Anesthesia; 2(4), 2/125/2 and 2/125/3; reprinted by permission
of Butterworth Heinemann, a division of Reed Educational & Professional Publishing Ltd.)
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462452

drawn in to the cell [53], smaller doses (0.25 mg/kg) have been effective
especially when repetitive dosing is required in the intensive care unit [54]. The
osmotic diuretics have a faster onset of action (15 minutes) than the loop
diuretics (30 minutes). Loop diuretics such as furosemide can lower ICP and
potentiate the ICP-lowering effects of mannitol. Hypertonic saline in an animal
hemorrhagic shock model [55] and a small human TBI series showed improved
ICP [56]. More controlled studies are required assessing other variables to fully
assess this therapy. Diuretic therapy may produce dehydration, hypotension,
and electrolyte disturbances including hypernatremia, hypokalemia, hypophos-
phatemia, and hypomagnesemia. These electrolyte disturbances can precipitate
cardiac arrhythmias.
Hyperventilation due to hypocapnia causes cerebral vasoconstriction, which
decreases cerebral blood flow and thus decreases ICP. Due to concern that
hyperventilation can decrease cerebral blood flow in areas after TBI to the point
of ischemia hyperventilation, it is used cautiously [57]. Prophylactic hyper-
ventilation has been shown to worsen outcome following TBI.
With acute ICP elevations, seizure must be considered, particularly if the
patient recently received paralytic drugs, preventing observation of tonic–clonic
seizure activity. Seizures can rapidly increase cerebral blood flow, and thus ICP.
The first priority in a nonventilated seizing patient is to establish a patent airway
and ensure adequate oxygenation. Arresting the seizure is paramount, and an
intravenous barbiturate may be required. Diazepam decreases cerebral blood
flow, cerebral metabolic rate, and ICP while raising the seizure threshold. When
treatment fails to reduce ICP, other etiologies must be sought such as intracranial
bleeding, status epilepticus, or worsening cerebral edema. Due to the high
incidence of posttraumatic seizures, anticonvulsant drugs are routinely admini-
stered prophylactically. Prophylactic phenytoin is indicated in the first week
following TBI [58]. If a seizure occurs beyond the initial injury phase, longer
administration of anticonvulsant therapy is indicated.
Although some centers have advocated the use of paralysis for ICP control, the
trend is to avoid paralytics due to adverse effects including the inability to monitor
neurologic changes, higher incidence of pneumonia, and prolonged weakness
[59]. Adequate pain control and sedation are important to prevent ICP elevations;
however, serial neurologic examinations are important for frequent assessment,
and should be obtained if possible. Shorter acting sedatives, which can be stopped
intermittently to allow serial neurologic examinations, are often being utilized.
Propofol has resulted in better control of ICP with improved outcome in TBI
patients but required more vasopressors [60].
With refractory ICP elevations (>25 mmHg), high-dose barbiturates can be
used if the patient is hemodynamically stable. Satisfactory ICP control may occur
in approximately one-quarter of patients with barbiturate infusion [61]. Due to the
potential complications associated with high-dose barbiturate infusion, its use is
limited to critical care settings that can provide appropriate monitoring and
support. Consideration should be given to monitoring for oligemic cerebral
hypoxia during high-dose barbiturate therapy [62].
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 453

Although effective in reducing cerebral edema with brain tumors, the routine
use of steroids in TBI is not recommended [63]. A review of 13 steroid trials
revealed no reduction in mortality [64]. The administration of steroids can result
in hyperglycemia, which may worsen outcome with head injury.
The generation of free radicals may worsen secondary injury. However,
clinical trials involving two free radical scavengers, polyethylene glycol-super-
oxidedismutase and tirilizad, did not effect outcome [65]. Other potential
therapies to decrease secondary injury include blockade with glutamate antago-
nists to prevent excitatory neurotransmission. Although still under investigation,
glutamate antagonists have not shown significant improved [65] outcome, and
may have behavioral side effects, limiting its use [66].
Hypothermia has been explored as a possible therapy to provide protection
from cerebral ischemia following TBI. A multicenter US trial in TBI did not show
improvement with hypothermia [67]. However, hyperthermia has been shown to
worsen brain infarct during cerebral ischemia [68], and thus should be avoided.
In controlling ICP, maintaining adequate cerebral perfusion pressure is
important. Unless there is brainstem failure, hypotension with an isolated head
injury should force one to search for other causes including hemorrhage or spinal
cord injury. With traumatic brain injuries, a minimum CPP of 70 mmHg has been
shown to result in improved morbidity, mortality, and outcome [69]. The absolute
level of CPP required is still under investigation [70], and whether higher CPP
levels will improve outcome have yet to be proven.
Other bedside monitoring methods to detect cerebral ischemia and intervene to
prevent secondary injury following TBI are being investigated. Jugular bulb
hemoglobin saturation (SjvO2) measures the saturation of the brain effluent blood
providing an estimating global cerebral oxygenation. It can provide information on
effectiveness of therapeutic interventions [71]. Desaturations are strongly associ-
ated with poor outcome [72]. Limitations of SjvO2 include the inability to detect
small ischemia regions. Still experimental, direct brain tissue partial pressure of
oxygen (PO2) can be measured by probes placed in brain parenchyma that detect
tissue oxygenation changes in small focal areas of the brain. Changes in brain tissue
PO2 correlate with outcome [73] and elevations in lactate and glutamate [74].
Intracerebral microdialysis can also detect cerebral ischemia during TBI. Cerebral
ischemia increased lactate, and was associated with a poor outcome [75].
Other imaging modalities are being developed that may permit monitoring of
the metabolic state of the brain following TBI. Although static, the CT scan has
the ability to identify pathology and allow immediate intervention. Portable CT
scanners are currently under development and may avoid transportation for CT
scans of the intensive care unit patients. Xenon CT may provide cerebral blood
flow information following TBI [76]. Magnetic resonance imaging (MRI) use
early after TBI is limited due to the lengthy scan time for images compared to
CT. MRI compatibility limits monitoring, and may hamper supportive and
resuscitative abilities while in the MRI scanner. However, newer MRI tech-
nologies under development may reveal early cerebral edema and allow func-
tional imaging.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462454

Medical complications can further complicate the course during head injury.
Abnormal coagulation tests are common after head injury, and the severity of
coagulopathy worsens outcome [77]. Because of the high risk of hemorrhage in
this patient population, correction of clotting abnormalities should be attempted.
Pulmonary complications are frequent with head injury. Neurogenic pulmo-
nary edema is more common with severe isolated TBI. The chest radiograph
typically shows fluffy infiltrates, and requires positive pressure ventilation and
supportive care to prevent hypoxemia. Pulmonary infections are the most
common infection and a major source of morbidity. Aggressive pulmonary
hygiene is the key, including postural drainage. However, Trendelenburg posi-
tioning to accomplish optimal postural drainage may be poorly tolerated due to
ICP elevations. These patients often lose airway protective reflexes and aspirate.
Those who require long-term ventilation or require suctioning for pulmonary
hygiene will require tracheostomies. Due to the prolonged bed rest and additional
injuries, the TBI patient is at risk for DVT and PE. With recent trauma and
potential for ICH, TBI patients are often not candidates for anticoagulation.
Devices such as IPC or ES are usually employed. If a patient with an ICH is
diagnosed with a DVT or PE, an inferior vena caval filter can be placed.
Blood pressure and heart rate elevation occurs following TBI probably due to
a sympathetic response. This can result in hypertension, which may raise ICP and
cause ICH. It may also precipitate myocardial ischemia.
With TBI, diabetes insipidus and SIADH can occur. Diabetes insipidus is
common following severe head injury, and can be permanent or transient with
eventual resolution. Serum hyperosmolality, urine hyposmolality, and ultimately
the response to exogenous antidiuretic hormone (ADH) administration (intra-
venous pitressin in the acute setting), confirm diagnosis. The diagnosis of
SIADH is confirmed with serum hyposmolality, urinary hyperosmolality, and
adequate blood volume. The mainstay of treatment is fluid restriction. Active
correction of hyponatremia with hypertonic saline should be reserved for those
patients with extreme hyponatremia (serum sodium < 120 mmol/L) or life-
threatening side effects. Serum sodium correction should be done judiciously due
to the concern of central pontine myelinolysis from a rapid increase in the serum
sodium concentration.
TBI is a risk factor for stress-induced gastritis and erosions. Prophylactic
therapy requires more solid data. Potential complications include gastrointestinal
hemorrhage. Due to the hypermetabolic state during TBI, early enteral feeding is
advocated. These patients often require placement of a chronic feeding tube
because of swallowing difficulties.
Spinal cord injury
There are approximately 10,000 new cases of spinal cord injury in the United
States yearly, with the average age at time of injury in the early thirties. The
most common cause of spinal cord injuries is motor vehicle accidents. Spinal
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 455

cord injuries occur in 2.6% of major trauma victims. Cervical spine injuries are
most common followed by thoracic and lumbar spine injuries. Of these spine
injuries, a little less that half will suffer complete loss of sensory and motor func-
tions [78].
All trauma victims with a suspicion of spinal trauma as well as those patients
with a high index for a spinal cord injury (head injury, altered mental status, neck
or back pain, drug or alcohol intoxication) should have spinal immobilization.
The primary injury to the spinal cord happens at the time of impact, and is
irreversible. The forces may cause spinal cord contusion, hemorrhage, or shear
injury. Maximizing the medical management of the patient can minimize
secondary injury. Prehospital spinal immobilization has become a standard of
care in the United States. These measures include placement of a rigid cervical
collar, log rolling only of the patient, and transportation on a rigid spine board.
During the initial hospital assessment of the spinal cord-injured patient, evalu-
ation of airway, breathing, and circulation are critical. One most ensure and
maintain a patent airway, maintain adequate oxygenation, and restore and
maintain an adequate blood pressure. Patients with high cervical lesions often
present with apnea, requiring mechanical ventilation. If apnea or respiratory
failure ensues, options for intubation include orotracheal intubation with in-line
traction, fiberoptic intubation, or if these fail, cricothyroidotomy or tracheostomy.
Failed intubation is more common with spinal cord because in-line immobiliza-
tion prevents optimal positioning for intubation. Cervical injuries at the level of
the phrenic nerve (C3 through C5) risk acute respiratory failure due to loss of
diaphragmatic muscles of breathing. With spinal cord injuries above T6 sym-
pathetic denervation leads to unopposed parasympathetic activity. Patients often
experience bradycardia, caused by loss of vascular tone and hypotension.
Aggressive intravenous fluid replacement should occur. Adequate blood pressure
should be maintained to decrease the risk of spinal cord ischemia. Aggressive
blood pressure maintenance with a mean arterial blood pressure of above
85 mmHg has improved neurologic outcome [79].
Complete neurologic examination should be performed on admission. This
includes evaluation of motor strength, sensory assessment, deep tendon reflexes,
and Babinski’s responses. Anal sphincter tone must also be examined. Further
evaluation to assess for spinal trauma is directed by patient’s clinical condition.
Spinal evaluation to clear the spine is controversial [80,81]. Trauma victims with
suspected spinal cord injury should undergo radiographic examination of the
cervical, thoracic, and lumbar spines. Any patient with persistent neck pain needs
further studies to rule out a ligamentous injury with normal plain cervical
radiographs. A patient with a fixed neurologic deficit presumed secondary to
spinal cord with normal plain spine radiographs warrants further imaging to rule
out soft tissue spinal cord compression. Initial assessment of the trauma patient
with a spinal cord injury can be complicated by the lack of sensation. These
patients are often multitrauma victims, and being insensate may lack physical
signs of intra-abdominal or thoracic trauma. A high index of suspicion must be
maintained, and the diagnosis must often be made radiographically.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462456

Primary injury occurs at the time of impact followed by secondary injury
processes. These may include autoregulatory loss, edema, and ischemia. Postu-
lated cellular mechanisms following secondary injury include calcium toxicity,
lipid peroxidation, free radical generation, and excitatory neurotransmitter release
[82–84]. Several clinical trials have attempted to limit these secondary injury
processes. A multicenter trial conducted by the National Acute Spinal Cord
Injury Study revealed a methylprednisolone bolus (30 mg/kg) followed by
continuous infusion (5.4 mg/kg) for 24 hours improved neurologic outcome
after spinal cord injury if administered within 8 hours of injury [85]. Postulated
mechanisms included decreased edema, inflammation, and lipid peroxidation. A
follow-up study revealed spinal cord injury patients treated with the above
methylprednisolone regime 3 to 8 hours after injury had better neurologic
outcome [85] but a higher infection rate if the methylprednisolone infusion
continued for 48 compared to 24 hours [86]. An additional study group compared
tirilazad administration (2.5 mg/kg) every 6 hours for 48 hours with the previous
methylprednisolone regime. All patients received 30 mg/kg bolus of methyl-
prednisolone due to ethical concerns [87]. At 24 hours tirilazad and methyl-
prednisolone were equally effective; however, 48-hour outcomes were better for
the methylprednisolone group. Infection rates were higher in the methylpredni-
solone group.
Gangliosides are glycolipids located in cell membranes and enhanced neurite
outgrowth and neuronal regeneration in animals [88]. In a prospective clinical
trial comparing GM-1 ganglioside to placebo, the treated spinal cord patients had
significant improvement in motor function [89], even allowing enrollment up to
72 hours after injury.
Spinal cord injury patients are at risk for a multitude of medical problems. An
upper or midcervical injury involving the phrenic nerve (C3–C5) will often cause
acute respiratory failure. More cephalad injuries will require tracheostomy for
permanent mechanical ventilation to prevent apnea. Intercostal nerve transfer
with phrenic nerve pacemaker implant has shown promising results in six patients
after high cervical spine injury [90]. Any patient who has a spinal cord injury C6
or higher must be closely monitored for respiratory insufficiency over the first
several days of admission postinjury. Those who have initially have an adequate
airway status may deteriorate due to spinal cord edema raising the cervical injury
level. These patients require aggressive pulmonary hygiene, and frequently
develop pneumonia, which may require antibiotic therapy. Due to prolonged
immobilization, spinal cord-injured patients are at risk for pressure necrosis and
decubitus ulcers. Frequent turning may not prevent long-term skin breakdown,
and these patients may require specialty beds to minimize further skin breakdown
and prevent decubiti ulcers.
Acute spinal cord injury patients have the highest risk of DVT among hospital
admission [91], with PE being the third most common cause of death [92]. The
highest risk period for venous thromboembolism occurs in the acute injury phase.
Although several small randomized trails of prophylaxis have been performed in
the spinal cord patient [93–95] large well-controlled studies of prophylaxis for
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 457

DVT have yet to be done. Low-dose fractionated heparin, IPC, or ES probably do
not provide adequate protection alone [96,97]. Duplex surveillance scanning for
spinal cord injury patients may be beneficial. If a DVT or PE develop, these
patients may not be candidates for systemic anticoagulation due to concomitant
trauma injuries or spinal cord hematoma. An inferior vena caval filter may be
placed. Prophylaxis recommendations include low molecular weight heparin in
the absence of contraindications [6].
Conclusion
The management of the neurologic critical care patient (stroke, SAH, TBI,
spinal cord injury) requires rapid recognition and treatment to limit or ideally
prevent further neurologic sequelae. Medical complications further increase the
morbidity and mortality in this patient population. New therapies and interven-
tions are currently under investigation. These may lead to further advances in the
management of this specialized patient population.
References
[1] The NINDS t-PA Study Group. Intracerebral hemorrhage after intravenous t-PA therapy for
ischemic stroke. Stroke 1997;28:2109–18.
[2] Adams HP, Brott TG, Furlan AJ, Gomez CR, Grotta J, Helagson J, et al. Guidelines for throm-
bolytic therapy for acute stroke: a supplement to the guidelines for the management of patients
with acute ischemic stroke. Circulation 1996;94:1167–74.
[3] Miller VT, Pearce LA, Feinberg WM, Rothrock JF, Andeson DC, Hart RG. Differential effect of
aspirin versus warfarin on clinical stroke types in patients with atrial fibrillation. Stroke Pre-
vention in Atrial Fibrillation Investigators. Neurology 1996;46(1):238–40.
[4] Guyatt G, Schunemann H, Cook D, Jaeschke R, Pauker S, Bucher H. Grades of recommendation
for antithrombotic agents. Chest 2001;119(Suppl 1):3S–7S.
[5] Gerriets T, Stolz E, Modrau B, Fiss I, Seidel G, Kaps M. Sonographic monitoring of midline shift
in hemispheric infarctions. Neurology 1999;52(1):45–9.
[6] Geerts WH, Heit JA, Clagett GP, Pineo GF, Colwell CW, Anderson FA Jr, et al. Prevention of
venous thromboembolism. Chest 2001;119:132S–75S.
[7] Castillo J, Davalos A, Marrugat J, Noya M. Timing for fever-related brain damage in acute
ischemic stroke. Stroke 1998;29:2455–60.
[8] Mayberg MR, Batjer HH, Dacey R, Diringer M, Haley EC, Heros RC, et al. Guidelines for the
management of aneurysmal subarachnoid hemorrhage. A statement for healthcare professionals
from a special writing group of the Stroke Council. American Heart Association. Circulation
1994;90(5):2592–605.
[9] Kassell NF, Torner JC, Haley EC Jr, Jane JA, Adams HP, Kongable GL. The International
Cooperative Study on the timing of aneurysm surgery. Part 1: overall management results.
J Neurosurg 1990;73:18–36.
[10] Kassell NF, Torner JC. Aneurysmal rebleeding: a preliminary report from the Cooperative
Aneurysm Study. Neurosurgery 1983;13(5):479–81.
[11] Ljunggren B, Saveland H, Brandt L, Zygmunt S. Early operation and overall outcome in
aneurysmal subarachnoid hemorrhage. J Neurosurg 1985;62:547–51.
[12] Roos YB, Rinkel GJ, Vermeulen M, Algra A, van Gijn L. Antifibrinolytic therapy for aneur-
ysmal subarachnoid haemorrhage. Cochrane Database Syst Rev 2000;2:CD001245.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462458

[13] Roos Y. Antifibrinolytic treatment in subarachnoid hemorrhage: a randomized placebo-controlled
trial. STAR Study Group. Neurology 2000;54(1):77–82.
[14] Kasuya H, Shimizu T, Kagawa M. The effect of continuous drainage of cerebrospinal fluid in
patients with subbarachnoid hemorrhage: a retrospective analysis of 108 patients. Neurosurgery
1991;28:56–9.
[15] Fisher CM, Kistler JP, Davis JM. Relation of cerebral vasospasm to subarachnoid hemorrhage
visualized by computed tomographic scanning. Neurosurgery 1980;6:1–9.
[16] Megyesi JF, Vollrath B, Cook DA, Findlay JM. In vivo animal models of cerebral vasospasm:
a review. Neurosurgery 2000;46:448–61.
[17] Sonobe M, Suzuki J. Vasospasmogenic substance produced following subarachnoid haemor-
rhage, and its fate. Acta Neurochir (Wien) 1978;44:97–106.
[18] Macdonald RL, Weir BK. A review of hemoglobin and the pathogenesis of cerebral vasospasm.
Stroke 1991;22:971–82.
[19] Weir B, Grace M, Hansen J, Rothberg C. Time course of vasospasm in man. J Neurosurg 1978;
48:173–8.
[20] Whiting DM, Barnett GH, Little JR. Management of subarachnoid hemorrhage in the critical
care unit. Cleve Clin J Med 1989;56:775–85.
[21] Takeuchi H, Handa Y, Kobayashi H, Kawaro H, Hayashi M. Impairment of cerebral autoregu-
lation during the development of chronic cerebral vasospasm after subarachnoid hemorrhage in
primates. Neurosurgery 1991;28:41–8.
[22] Maroon JC, Nelson PB. Hypovolemia in patients with subarachnoid hemorrhage: therapeutic
implications. Neurosurgery 1979;4:223–6.
[23] Solomon RA, Post KD, McMurtry JG III. Depression of circulating blood volume in patients
after subarachnoid hemorrhage: implications for the management of symptomatic vasospasm.
Neurosurgery 1984;15:354–61.
[24] Rosenwasser RH, Delgado TE, BuchheitWA, FreedMH. Control of hypertension and prophylaxis
against vasospasm in cases of subarachnoid hemorrhage: a preliminary report. Neurosurgery 1983;
12:658–61.
[25] Awad IA, Carter LP, Spetzler RF, Medina M, Williams FC Jr. Clinical vasospasm after subar-
achnoid hemorrhage: response to hypervolemic hemodilution and arterial hypertension. Stroke
1987;18:365–72.
[26] Kassell NF, Peerless SJ, Durward QJ, Beck DW, Drake CG, Adams HP. Treatment of ischemic
deficits from vasospasm with intravascular volume expansion and induced arterial hyperten-
sion. Neurosurgery 1982;11:337–43.
[27] Levy ML, Giannotta SL. Cardiac performance indices during hypervolemia therapy for cerebral
vasospasm. J Neurosurg 1991;75:27–31.
[28] Rosenwasser RH, Jallo JI, Getch CC, Liebman KE. Complications of Swan-Ganz catheterization
for hemodynamic monitoring in patients with subarachnoid hemorrhage. Neurosurgery 1995;
37(5):872–5.
[29] Barker FG II, Ogilvy CS. Efficacy of prophylactic nimodipine for delayed ischemic deficit after
subarachnoid hemorrhage: a metaanalysis. J Neurosurg 1996;84(3):405–14.
[30] Haley EC Jr, Kassell NF, Torner JC, Truskowski LL, Germanson TP. A randomized trial of two
doses of nicardipine in aneurysmal subarachnoid hemorrhage: a report of the Cooperative
Aneurysm Study. J Neurosurg 1994;80:788–96.
[31] Shibuya M, Suzuki Y, Sugita K, Saito I, Sasaki T, Takakura K, et al. Effect of AT877 on
cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Results of a prospective place-
bo-controlled double-blind trial. J Neurosurg 1992;76:571–7.
[32] Sasaki T, Ohta T, Kikuchi H, Takakura K, Osui M, Ohnishi H, et al. A phase II clinical trial of
recombinant human tissue-type plasminogen activator against cerebral vasospasm after aneur-
ysmal subarachnoid hemorrhage. Neurosurgery 1994;35:597–605.
[33] Findlay JM, Kassell NF, Weir BK, Haley EC Jr, Kongable G, Germanson T, et al. A randomized
trial of intraoperative, intracisternal tissue plasminogen activator for the prevention of vaso-
spasm. Neurosurgery 1995;37(1):168–76.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 459

[34] Zuccarello M, Marsch JT, Schmitt G, Woodward J, Anderson DC. Effect of the 21-aminosteroid
U-74006F on cerebral vasospasm following subarachnoid hemorrhage. J Neurosurg 1989;71:
98–104.
[35] Kassell NF, Haley EC Jr, Apperson-Hansen C, Alves WM. Randomized, double-blind, vehicle-
controlled trial of tirilazad mesylate in patients with aneurysmal subarachnoid hemorrhage:
a cooperative study in Europe, Australia, and New Zealand. J Neurosurg 1996;84:221–8.
[36] Haley EC Jr, Kassell NF, Apperson-Hansen C, Malle MH, Anes WM. A randomized, double-
blind, vehicle-controlled trial of tirilazad mesylate in patients with aneurysmal subarachnoid
hemorrhage: a cooperative study in North America. J Neurosurg 1997;86:467–74.
[37] Lanzino G, Kassell NF, Dorsch NW, Pasqualin A, Brandt L, Schmiedek P, et al. Double-blind,
randomized, vehicle-controlled study of high-dose tirilazad mesylate in women with aneurysmal
subarachnoid hemorrhage. Part I. A cooperative study in Europe, Australia, New Zealand, and
South Africa. J Neurosurg 1999;90:1011–7.
[38] Lanzino G, Kassell NF. Double-blind, randomized, vehicle-controlled study of high-dose tirila-
zad mesylate in women with aneurysmal subarachnoid hemorrhage. Part II. A cooperative study
in North America. J Neurosurg 1999;90:1018–24.
[39] Asano T, Takakura K, Sano K, Kikuchi H, Nagai H, Saito I, et al. Effects of a hydroxyl radical
scavenger on delayed ischemic neurological deficits following aneurysmal subarachnoid hem-
orrhage: results of a multicenter, placebo-controlled double-blind trial. J Neurosurg 1996;84:
792–803.
[40] Saito I, Asano T, Sano K, Takakura K, Abe H, Yoshimoto T, et al. Neuroprotective effect of an
antioxidant, ebselen, in patients with delayed neurological deficits after aneurysmal subarachnoid
hemorrhage. Neurosurgery 1998;42:269–77.
[41] Thomas JE, Rosenwasser RH. Reversal of severe cerebral vasospasm in three patients after
aneurysmal subarachnoid hemorrhage: initial observations regarding the use of intraventricular
sodium nitroprusside in humans. Neurosurgery 1999;44(1):48–57.
[42] Solenski NJ, Haley EC Jr, Kassell NF, Kongable G, Germanson T, Truskowski L, et al. Medical
complications of aneurysmal subarachnoid hemorrhage: a report of the multicenter, cooperative
aneurysm study. Participants of the Multicenter Cooperative Aneurysm Study. Crit Care Med
1995;23:1007–17.
[43] Hernesniemi J, Vapalathi M, Niskanen M, Tapaninaho A, Kari A, Luukkonen M, et al. One-year
outcome in early aneurysm surgery: a 14 year experience. Acta Neurochir (Wien) 1993;122:1–10.
[44] Di Pasquale G, Andreoli A, Lusa AM, Ormbinati S, Biancoli S, Cere E, et al. Cardiologic
complications of subarachnoid hemorrhage. J Neurosurg Sci 1998;42(Suppl 1):33–6.
[45] Mayer SA, Lin J, Homma S, Solomon RA, Lennihan L, Sheiman D, et al. Myocardial injury and
left ventricular performance after subarachnoid hemorrhage. Stroke 1999;30(4):780–6.
[46] Nilsson OG, Brandt L, Ungerstedt U, Saveland H. Bedside detection of brain ischemia using
intracerebral microdialysis: subarachnoid hemorrhage and delayed ischemic deterioration. Neu-
rosurgery 1999;45:1176–854.
[47] Bullock MR, Lyeth BG, Muizelaar JP. Current status of neuroprotection trials for traumatic brain
injury: lessons from animal models and clinical studies. Neurosurgery 1999;45:207–17.
[48] Chestnut RM, Marshall LF, Klauber MR, Blunt BA, Baldwin N, Eisenberg HM, et al. The role
of secondary brain injury in determining outcome from severe head injury. J Trauma 1993;34:
216–22 [abstract].
[49] Winchell RJ, Hoyt DB. Endotracheal intubation in the field improves survival in patients with
severe head injury. Arch Surg 1997;132:592–97.
[50] Miller JD, Becker DP, Ward JD, Sullivan HG, Adams WE, Resner MJ. Significance of intra-
cranial hypertension in severe head injury. J Neurosurg 1977;47:503–16.
[51] Eisenberg HM, Gary HE Jr, Aldrich EF, Saydjari C, Turner B, Foulkes MA. Initial CT findings
in 753 patients with severe head injury. A report from the NIH Traumatic Coma Data Bank.
J Neurosurg 1990;73:688–98.
[52] Chambers IR, Mendelow AD, Sinar EJ, Modha P. A clinical evaluation of the Camino subdural
screw and ventricular monitoring kits. Neurosurgery 1990;26:421–3.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462460

[53] Cottrell JE, Robustelli A, Post K, Tundorf H. Furosemide- and mannitol-induced changes in
intracranial pressure and serum osmolality and electrolytes. Anesthesiology 1977;47:28–30.
[54] McGraw CP, Howard G. Effect of mannitol on increased intracranial pressure. Neurosurgery
1983;13:269–71.
[55] Prough DS, Whitley JM, Taylor CL, Deal DD, Dew HDS. Regional cerebral blood flow following
resuscitation from hemorrhagic shock with hypertonic saline. Anesthesiology 1991;75:319–27.
[56] Munar F, Ferrer AM, de Nadal M, Poca MA, Pedroza S, Saguqui H, et al. Cerebral hemody-
namic effects of 7.2% hypertonic saline in patients with head injury and raised intracranial
pressure. J Neurotrauma 2000;17(1):41–51.
[57] The Brain Trauma Foundation. The American Association of Neurological Surgeons. The joint
section on neurotrauma and critical care: hyperventilation. J Neurotrauma 2000;17(6–7):513–20.
[58] Temkin NR, Dikmen SS, Wilensky AJ, Keihm J, Chabal S, Winn HR. A radnomized, double-
blind study of phenytoin for the prevention of post-traumatic seizures. N Engl J Med 1990;323:
497–502.
[59] Fahy BG, Matjasko MJ. Disadvantages of prolonged neuromuscular blockade in patients with
head injury. J Neurosurg Anesthiol 1994;6(2):136–8.
[60] Kelly DF, Goodale DB, Williams J, Herr DL, Chappell ET, Rosner MJ, et al. Propofol in the
treatment of moderate and severe head injury: a randomized, prospective double-blinded pilot
trial. J Neurosurg 1999;90:1042–52.
[61] Marshall LF, Shapiro MR. Barbiturate control of intracranial hypertension in head injury and
other conditions: iatrogenic coma. In: Ingvar DH, Lassen NA, editors. Cerebral function, metab-
olism and circulation. Copenhagen: Munksgaard. 1977. p. 156–7.
[62] The Brain Trauma Foundation. The American Association of Neurological Surgeons. The joint
section on neurotrauma and critical care: use of barbiturates in the control of intracranial hyper-
tension. J Neurotrauma 2000;17(6–7):527–30.
[63] The Brain Trauma Foundation. The American Association of Neurological Surgeons. The joint
section on neurotrauma and critical care: role of steroids. J Neurotrauma 2000;17(6–7):531–5.
[64] Alderson P, Roberts I. Corticosteroids for acute traumatic brain injury. Cochrane Database Syst
Rev 2000;CD000196.
[65] Doppenberg EM, Choi SC, Bullock R. Clinical trials in traumatic brain injury: what can we learn
from previous studies? Ann NY Acad Sci 1997;825:305–22.
[66] Teasdale GM, Graham DI. Craniocerebral trauma: protection and retrieval of the neuronal
population after injury. Neurosurgery 1998;43:723–38.
[67] Clifton GL, Miller ER, Choi SC, et al. Lack of effect of induction of hypothermia after acute
brain injury. N Engl J Med 2001;344(8):556–63.
[68] Dietrich WD. The importance of brain temperature in cerebral injury. J Neurotrauma 1992;
9(suppl):475–85.
[69] Rosner MJ, Rosner SD, Johnson AH. Cerebral perfusion pressure: management protocol and
clinical results. J Neurosurg 1995;83:949–62.
[70] Eker C, Asgeirsson B, Grande PO, Schalen W, Nordstrom CH. Improved outcome after severe
head injury with a new therapy based on principles for brain volume regulation and preserved
microcirculation. Crit Care Med 1998;26:1881–6.
[71] Cruz J, Miner ME, Allen SJ, Alves WM, Gennarelli TA. Continuous monitoring of cerebral
oxygenation in acute brain injury: assessment of cerebral hemodynamic reserve. Neurosurgery
1991;29:743–9.
[72] Gopinath SP, Robertson CS, Contant CF, Hayes C, Feldman Z, Narayan CK, et al. Jugular venous
desaturation and outcome after head injury. J Neurol Neurosurg Psychiatry 1994;57:717–23.
[73] Valadka AB, Gopinath SP, Contant CF, Uzura M, Robertson CS. Relationship of brain tissue PO2
to outcome after severe head injury. Crit Care Med 1998;26:1576–81.
[74] Valadka AB, Goodman JC, Gopinath SP, Uzura M, Robertson CS. Comparison of brain tissue
oxygen tension to microdialysis-based measures of cerebral ischemia in fatally head-injured
humans. J Neurotrauma 1998;15:509–19.
[75] Goodman JC, Valadka AB, Gopinath SP, Veura M, Robertson CS. Extracellular lactate and
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462 461

glucose alterations in the brain after head injury measured by microdialysis. Crit Care Med
1999;27(9):1–15.
[76] Marion DW, Darby J, Yonas H. Acute regional cerebral blood flow changes caused by severe
head injuries. J Neurosurg 1991;74:407–14.
[77] Olson JD, Kaufman HH, Moake J, O’Gorman TW, Hoots K, Wagner K, et al. The incidence and
significance of hemostatic abnormalities in patients with head injuries. Neurosurgery 1989;24:
825–32.
[78] DeVivo MJ, Rutt RD, Black KJ, Go BK, Srover SL. Trends in spinal cord injury demographics
and treatment outcomes between 1973 and 1986. Arch Phys Med Rehabil 1992;73:424–30.
[79] Vale FL, Burns J, Jackson AB, Hadley MN. Combined medical and surgical treatment after acute
spinal cord injury: results of a prospective pilot study to assess the merits of aggressive medical
resuscitation and blood pressure management. J Neurosurg 1997;87:239–46.
[80] MacDonald RL, Schwartz ML, Mirich D, Sharkey PW, Nelson WR. Diagnosis of cervical spine
injury in motor vehicle crash victims: how many x-rays are enough? J Trauma 1990;30:392–7.
[81] Nunez DB, Zuluaga A, Fuentes-Bernardo DA, Rivas LA, Becerra JL. Cervical spine trauma:
how much more do we learn by routinely using helical CT? Radiographics 1996;16:1307–18.
[82] Hsu CY, Halushka PV, Hogan EL, Banik NL, Lee WA, Perot PL Jr. Alteration of thromboxane
and prostacyclin levels in experimental spinal cord injury. Neurology 1985;35:1003–9.
[83] Panter SS, Yum SW, Faden AI. Alteration in extracellular amino acids after traumatic spinal cord
injury. Ann Neurol 1990;27:96–9.
[84] Young W, Koreh I. Potassium and calcium changes in injured spinal cords. Brain Res 1986;
365:42–53.
[85] Bracken MB, Shepard MJ, Collins WF, Holford TR, Young W, Baskin DS, et al. A randomized,
controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury.
Results of the SecondNational Acute Spinal Cord Injury Study. N Engl JMed 1990;322:1405–11.
[86] Bracken MB, Holford TR. Effects of timing of methyl-prednisolone or naloxone administration
on recovery of segmental and long-tract neurological function in NASCIS 2. J Neurosurg 1993;
79:500–7.
[87] Bracken MB, Shepard MJ, Holford TR, Leo-Summer SL, Aldrich EF, Fazl M, et al. Admin-
istration of Methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the
treatment of acute spinal cord injury. Results of the third national acute spinal cord injury
randomized controlled trial. JAMA 1997;277(20):1597–604.
[88] Geisler FH, Dorsey FC, Coleman WP. Past and current clinical studies with GM-1 ganglioside in
acute spinal cord injury. Ann Emerg Med 1993;22:1041–7.
[89] Geisler FH, Dorsey FC, Coleman WP. Recovery of motor function after spinal cord injury—a
randomized, placebo-controlled trial with GM-1 ganglioside. N Engl J Med 1991;324:1829–38.
[90] Krieger LM, Krieger AJ. The intercostal to phrenic nerve transfer: an effective means of rean-
imating the diaphragm in patients with high cervical spine injury. Plast Reconstr Surg 2000;
105(4):1255–61.
[91] Consortium for Spinal Cord Medicine. Prevention of thromboembolism in spinal cord injury.
J Spinal Cord Med 1997;20:259–83.
[92] DeVivo MJ, Krause JS, Lammertse DP. Recent trends in mortality and causes of death among
persons with spinal cord injury. Arch Phys Med Rehabil 1999;80:1411–9.
[93] Green D, Lee MY, Ito VY, Cohn T, Press J, Filbrandt PR, et al. Fixed vs adjusted-dose heparin in
the prophylaxis of thromboembolism in spinal cord injury. JAMA 1988;260:1255–8.
[94] Green D, Lee MY, Lim AC, Chmiel JS, Velter M, Pang T, et al. Prevention of thromboembolism
after spinal cord injury using low-molecular-weight heparin. Ann Intern Med 1990;113:571–4.
[95] Green D, Rossi EC, Yao JS, FlinnWE, SpiessM. Deep vein thrombosis in spinal cord injury: effect
of prophylaxis with calf compression, aspirin, and dipyridamole. Paraplegia 1982;20:227–34.
[96] Merli GJ, Crabbe S, Doyle L, Ditonno JF, Herbision GJ. Mechanical plus pharmacological
prophylaxis for deep vein thrombosis in acute spinal cord injury. Paraplegia 1992;30:558–62.
[97] Watson N. Venous thrombosis and pulmonary embolism in spinal cord injury. Paraplegia
1968;6:113–21.
B.G. Fahy, V. Sivaraman / Anesthesiology Clin N Am 20 (2002) 441–462462