Embed Size (px)
Citation preview

���� ����������Vol. 37, pp. 385�392, 2009
���������� ������� 1�
���
���
��
���1 �
���
� ��
1 ���
��
���1
��
���
���
2 �
��
�
���
��3 �
��
���
���
��1
�� :�� 21� 9� 24��
� ���� 1� 1����� 38�C���� �!��"#$�%&�'()� �*+� ��
6��",�-./01�0��23456789:�;'(+� �� CT -�<=>? �!@AB+2CDEF� -!7%@B+� �� 7��"#� GHIJ1�0��2345�K�LGHIJ$%2MN5++!� �� MR OP%Q&'()*R%Q+�,()-S�T.@URV2�!W(+� XYZ[�+!\]Z^ O_� `abc"#Q/&"d0012 �!++!37847%@B+� 47L�`abc-d00122e�fg h5#_++!� �� 9��"ij`k&d053lmnop��q&rs�tcu!l OB+� l+>?AW$v0`&6w �infectious endocarditis, IE�"nxRyz"{Y|x&'()*R%&�5+� lL�}~�78%�q&r������ O_CD�9�-�B+� :O5#�����Z[ OB+2� `���; @<= �! IE �XY%@x������!W(@AB+� �C L��%5#G<.=$%2MN5+���./����>"��5��� 66��"�7%@B+�,UR �?5+`�� �+@_�� IE ���@���-�x� 'W" IE "nxRyz2�q&�'���()*R A�5+%�@��?3+W@_� �� IE ��2&'()*R �?5+�B@�� C�5+�-@�|x�
����$v0`&6w� ,UR� &'()*R
� �
��%C�5#���,UR��@��-�x1��3�� K�XY"�� � � 1 ,(¡)¢£@¤,¥¦�§¨ �� B|x� D�0��� ©*ª� $v�� `¥¦0��� «¬� ¥®¯<=�@¤2°±W(x2�� $v��+-�� `�
�"²¥�2³´µ¶·{¸'(x$v0`&6w�infectious endocarditis, IE� �²Ry"nµ�q&¥¦�*R A�|x2� K�*R�¹"º_#�� &'() E»,F()� _´¼x�q&�'���()�*R G5+@��@_� �� IE ��2&'()*R �?5+�B@�� C�5+�-@�|x�
� �
�: 1� 1������ �: ��� GHIJ$%�
1 ��������� ,�C«�2 ��������� ���3 ��������� «��`�¥¦«��
385
67

���: �� 39� 0�� �� 2,890 g� ���������: � ��������: �����������������: 38�C ���� !"##"$% &'�#� (�)'*+,� -./012345/067�8� &9#� �: 6��� ;<=>?@ABCA�DE�FGHIJK+,#� L� CTMN�OP !"�QR#DSTUV�WXG)�R#� �: 7��� � YZ[\BCA�DE�� ]�^YZ[\��D_`�##"� L�MR ab)cd�e��f)cghie��j=k��lfmD!"n,#� opqr�#"stqu aR#)vw� xyz{=>c�d=|�A�� !"##"� }GH~G)�R#��� ���: �� 9.5 kg, �� 37.5�C � ��96�22 mmHg, �� 124�min��� Children’s ComaScale E1V2M4� ����� 2 mm, ��������� i�S����� Y�?������ YZ\MMT 3��V� Y[\ MMT 3��V���������: WBC 1.11�104�ml, RBC 3.40�106�ml, Hb 9.0 g�dl, Plt 1.35�105 �ml, PT-INR 1.13,APTT 36.1, D-dimer FDP 35.8 mg�ml, CRP 7.22mg�dl���������: �FiO2 0.32 [�: pO2 211.9mmHg, pCO2 29.6 mmHg������ !�: CTR 59�� �������B�����N����M!"n,���"� MRI �#$�: cghie��jk�=��B������ T2B������j� T1B������j !"�� �� ¡� midline shift !"� chi ¢=�9�i£M]�¤)¥¦D!�"��� �Fig. 1-a�"� MRA �#$�: cd�e�� cghie�M!+,��D� c§hie�M!+,>���Fig. 1-b����% &' CT:cd�e�M� c¨�e�Qn�©C^M!+,�ª��],«¬M!+,�� �Fig. 1-c�� ]�¤Q�?@��=��>�fOPM!"n,�����()*+: c�d#$%$&='®A�C� 5 mmh�|�A�� !"� �Fig. 2-a���,-.: «Z�qu¯°��x±|(� �=x�d²�|D³´,� ]����µ¶A��·)¸
a
b
c
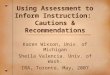
Fig. 1. a: Di#usion weighted MR image demonstrated a
wide and high intensity area in the territory of
left middle cerebral artery�MCA�.b: MR angiography showed occulusion of the
left internal carotid artery.
c: Enhanced CT revealed occluded left internal
carotid artery near the cervical bifurcation.
¹º»* +, ¼ n386
68

���������� �������������� ������������ �!"#$%&'()*+,-#./0 D-123456789: ;<=�>?@���ABCD6EF56G4HIJK07LM�NO��� 10 PQR�STU5��VW�XY���Z[ 10 mm\]*^\��_�`��abc�� �Fig. 2-b�� defg\*h��iX�������jkl�mnc��`�o�� �> 9p(�NqSr�stuv: ;
w!!"#x2y5z{v�|}��������: S~�������7Z[ 10mm\7���bi �Fig. 3-a, b�� S~7����������� ���V���Y��Y�����u��� ��>������ �7�7��l�� ¡�¢£¤¥�bi��fo}��������: S~����uc��Y�*�� S��7¦§f¨>©ª,« �Fig. 4�� Sr7¬®¯�°£S��S±7²³®¯� ´µf
a
b
Fig. 2. a: Transthoracic echocardiography on admission
performed a tumor-like lesion�arrow� in theleft atrium.
LA: left atrium, LV: left ventricle, RA: right
atrium, Ao: aorta
b: Transthoracic echocardiography following
after ten hours showed the growth of the
tumor like lesion�arrow��
a
b
Fig. 3. a: The tumor like lesion �arrow� in the leftatrium.
b: A vegitation �arrow� appeared in the leftatrium after myocardial incision on the left
auricular appendage.
�� ���¶��·¸lS�¨7 1¹ 387
69

�������� ������������� �� �������������� ������������ !"#�$�%�& ��'�����(�)*����+$�� �,-./�01���� )2$������: 3��������4�01�'5�������6������ �78#9$�!,���:�';<=���� �">��& ���?@;AB�=CDEF�GH�IB 80 mg�kg�day J 4KL� gMN��� 260 mg�kg�dayJ 5!LO"#$��� P�Q� R%#S&�!,T'�:(UV)J��� !,���:WXUY�Z��� *[�\� D-]�<H^_ 1 g�kg�4 �#$� 10 mmHg `a#b�Z�� cd�#+c�e�,/�f� g� 3Q 7!-#*[�\h�i^J.j��� ��� &�)k/lmno0:���!,� 1p� 2qrs#3tk!,�:J9$�4�2)5�01���� )2$�� Qu����v6789:�wx MMT 3�V� ax MMT 4�V��y;��7<e=�>z�+'� ?@;AB�=CDEF�GH�IB#${?Q� @� 66!-#A7�)$�� )�� �7����A7QU IE #"@tk|>�/BCD0:���*E MR J9$�6�& )2$��
� �
F�G#�*�HIt}~�� �� IE �G#�
J��/lm#��kKm!��LBC�+$�M�+k� �N���'��� ����)*[��LE��BCJKm���*�O��1P��)*�� ���O���� ��#��k/!����@QRS�T� 10UT#3�VL 2.1�2.5T4�5���T�P �W}�X#�)�� P����!�rs��!�rs���� 3 : 1�& 4�� �T�P ��Y3�+k� �!�rst)��/lm���� 10 UT#3� 0.2�0.86 T�+k4��6�� no��U.U.����+'� Za�� 32�35.4� �O���*k1�� �[�#� �� U.U.�#�otkU�J�*�/lm��no64�U�36�� w�\5��2�LE�LBC�����!��KmJ�~����U� 32�� �!�rsJno�tkU� 16�� �� 12��O�& �*k2�� P�]#U Powel ����#no64�U�� 30�50��O���*kU�U+k7�
� *g Uno64�U����+$�� P �`����)no����� fibromusculardysplasia8�. neurofibromatosis9� ��2^n�#�Jtk!��._`�1p� �� !,¡¢� �)£10�O�& �*k� /!�¤¥#�kKmE¦��a��� P�no#§��g�LBC#�*�tk�[�2��O��� �b/BC#�*�tk¨c�3�.b©�11��O�+'Td��1S�e� �*)*�IE �������Uf�.b!���#|>g�ªhJ«¬�Ji�� >!�� �j��� �k®#��kml�)£�¯)m°�eJntko!��rs�+k12�� �#� ±prs���_`����Q`��rs� �k²3�³´+'� � �#>!�µ�k��� IE @�tk�¶·� �*k� Niwa ��_`��rs� IE #qs�� 239 T��� 170 T� �T 69 T���� 116 T�48.5��#¸�2��J���� � P���10.5�# IE #�k/lm��� ��JO���*k13�� P�Tr�� �rsJ¹�)* IE @�G�O�14��16�Uº1& � Nakatani �� IE #qs�� 848T��� 149T�17.2��#�rsJ��)2$��O���*k17�� ��#��tk�� Giv-ner ��O�#� ��rsJ¹�)* IE @�RS� 9 ��+$�14�� &�#��� �">� IE#���� Choi ��O���� �rsJ¹�)*
Fig. 4. Pathological findings showed infiltration of
neutrophils in the endocardium. Hematoxylinand eosin staining: �40�
st»u vF ¼ �388
70

�� 54�����18�� ����� ��� ����������� IE ���� �����������15�� IE���������� !"�#$%����&'� �#(� �)� * )�����+����,��-�� 20�40���./���19��21�� Eishi ���022���/1� .�2�34� IE ����������&'����64.6� ���� 5�6��&'�78���010�16�23��33������ �'�9�:������;����� ��<=�� M1 segment ��;�34�� >�<=���?������'�����0��@�/A� �,/�(BC�!D��"E(B���'��;�� �&'��-FG�� IE �#�%�HIJ���$��-FG���%�/��� 2K� theory �LM�/���� N&JOP� vasavasorum Q��� R � � � '(J)Q�S�J�)��T���%� vasa vasorum theory27���N&JOP�(B'U��'�� V�J�)��T���%� embolic theory35�36� ���� *(B���W+�X��@�/� "EQYZW+>X��@�/�37�� �['�+�\]���'+��� �?������3���A/� theory �,^��C�-.����� �C�/�0��� �C�_`����12�a*��5�C�� >X����b,^�c./��de��&'�0�3���� (fgh� 3i"�j4�kl����� m5J��6n� ��� IE o�7p������qrs�+���tuvswxy�89�LM�/�� z�� /�0��{ :_`�12�|;�<*��@�/�5�C�� }��tuvswxy���C�=>��@� ��~��?��������b@��l���5���9�c./��
����
1� A�]B� �C�D� �E�}� �F��� ���� GHD� ��I�� ���J� �K�L� de�'J�(B����M� de�� ! 1995; 20: 11�15�
2� ��NO� ����� de��'J�(B��� de�� ! 1986; 11: 165�172�
3� ��P�� �~�� ���J� �QR�}� de�'J�(B���=S��T� � !R 1981; 9: 707�714�
4� Schoenberg S, Mellinger F, and Schoenberg G.Cereberovascular disease in infants and chil-
dren: a study of incidence, clinical features, and
survival. Neurology 1978; 28: 763�768.5� Eeg-Olofsson O, and Ringheim Y. Stroke inchildren clinical characteristics and prognosis.
Acta Pediatr Scand 1983; 72: 391�395.6� Satoh S, Shirane R, and Yoshimoto T. Clinicalsurvey of ischemic cereberovascular disease in
children in a district of Japan. Stroke 1991; 22:
586�589.7� Powel FC, Hanigan WC, and McCluney KW.Subcortical infarction in children. Stroke 1994;
25: 117�121.8� Lemahieu SF, and Marchau MMB. Intracra-nial fibromuscular dysplasia and stroke in chil-
dren. Neuroradiology 1979; 18: 99�102.9� Pellok JM, Kleinman PK, McDonald BM, andWixson D. Childhood hypertensive stroke with
neurofibromatosis. Neurology 1980; 30: 656�659.
10� UV¡P� �¢���� �£WXP� �Y¤¥� Z/¦§� �[¨� ©ªJ�'O��~��c./��&'� 1 de0� de \«2006; 59: 1955�1960�
11� *�¬]� �F^� ®_¯P� FRX°� `FP�� ±��²� ³`a´� µbc�¶� ·R¸}� �/¹� de��&'�,�d> �º» 240�\«!¼� ���� 1985; 17: 307�313.
12� Chu VH, Cabell CH, Benjamin DK Jr, Kuni-holm EF, Fowler VG Jr, Engemann J, Sexton
DJ, Corey GR, and Wang A. Early predictors
of in-hospital death in infective endocarditis.
Circulation 2004; 109: 1745�1749.13� Niwa K, Nakazawa M, Tateno S, YoshinagaM, and Terai M. Infective endocarditis in con-
genital heart disease: Japanese national col-
laboration study. Heart 2005; 91: 795�800.14� Givner LB, Mason EO Jr, Tan TQ, Barson
WJ, Schutze GE, Wald ER, Bradley JS,
Ho#man J, Yogev R, and Kaplan SL. Pneu-
mococcal endocarditis in children. Clinical In-
fectious Diseases 2004; 38: 1273�1278.
'+���'�e��N&J�' )� 10 389
71

15� ������ ����� ����� �������� �� � �� ����� �� � ���� ��� ���� ������������� �� �!"�#�$��� ��%&' 1�(�� )(*�+ 2006;59: 2153�2157�
16� ,-� � �./�� 0�1� �2 3� #�%�45�!"#%6�$&'%789 1&(�� )(*�+ 2007; 60: 267�271�
17� Nakatani S, Matsutake K, Hozumi T, Yoshi-kawa J, Akiyama M, Yoshida K, Ishizuka N,
Nakamura k, Taniguchi Y, Yoshioka K, Ka-
wazoe K, Akaishi M, Niwa K, Nakazawa M,
Kitamura S, and Miyatake K. Current charac-
teristics of infective endocarditis in Japan �ananalysis of 848 cases in 2000 and 2001�. Circ J2003; 67: 901�905.
18� Choi M, and Mailman TL. Pneumococcal en-docarditis in infants and children. Pediatr In-
fect Dis J 2004; 23: 166�171.19� Heiro M, Nikoskelainen J, and Engblom E.
Neurologic manifestations of infective endo-
carditis: a 17-year experience in a teaching hos-
pital in Finland. Arch Intern Med 2000; 160:
2781�2187.20� Gillinov AM, Shah RV, Curtis WE, Stuart RS,Cameron DE, Baumgartner WA and Greene
PS. Valve replacement in patients with endo-
carditis and acute neurologic deficit. Ann Tho-
rac Surg 1996; 61: 1125�1129.21� Kanter MC, and Hart RG. Neurologic compli-cation of infective endocarditis. Neurology
1991; 41: 1015�1020.22� Eishi K, Kawazoe K, Kuriyama Y, Kitoh Y,
Kawshima Y, and Omae T. Surgical manage-
ment of infective endocarditis associated with
cerebral complications. Multi-center retospec-
tive study in Japan. 1995; 110: 1745�1755.23� ��:'(� ;)<=� ��>(� ?@A��
�)*+� B �,� CD-� �.%/01E238�4�&'56FG$%/079 1HI�� %JKL* 2004; 32: 493�499�
24� ��"*� 8MN� 9OPQ� �)R �S T� :�;<� Osler UV �=WXYZ
[$FG$��� \]>^_� K`���a78� %78�?�&' 1 ��� =@�+2004; 46: 1681�1685�
25� bAcd� !e3B� fC1� DEFG� )%9gh$78�i?&'#�$��� 9 1� �jklmnmH�opqklrm�stIuvwm�xJ&'KLyz9K{�� L�L|} 1999; 60: 950�953�
26� �CM~� �NB�� ���O� �PT�� BA��� ���Q� R��S� ����� �)��� �2L* 1997; 50: 304�307�
27� TAU� V�~B� WX�Y� �Z�[� \�A� �J%6��%&'#�$��� 9 1�� �] 2006; 38: 640�644�
28� �^�� AC�d� ��_`� �X_R�a)b�� cFG$hd$��� ���%�78�i?&'e pseudomesotheliomatous.L��|} 2003; 41: 728�732�
29� <�f� �C��� �g�� �P, � [$�%78�h�'�i�$9�/�#�$��� �j&���&'klm cI9�� ¡n¢Mo£¤¥^i¦} 2008; 15: 48�51�
30� , §� ¨©<Q� A�ª� p¦�« I¬#�$��� ��.%/08d�i?&'q(9®¯�e°rs±²I9"³K{� "³ 2007; 56: 1186�1189�
31� �´b<� �µ�t� �¶·�� %78�%¬� R��¸¹�°gh�$&'�.%/01E2FG$56%/079 1 HI�� NoShinkei Geka 2006; 34: 1051�1055�
32� �)�º� %78�i?&'#�$��� �Infectiveendocarditis, IE� 9 1�� u¢�*¤||} 1999; 14: 210�218�
33� Li WK, Chen YS, Wann SR, Liu YC and TsaiHC. Lactococcus garvieae endocarditis with
initial presentation of acute cerebral infarction
in a healthy immunocompetent man. Inter
Med 2008; 47: 1143�1146.34� Molinari GF, Smith L, and Goldstein NM.
Pathogenesis of cerebral mycotic aneurysm.
Neurology 1973; 23: 325�332.35� Frazee JG, Cahan LD, and Winter J. Bacterialintracranial aneurysm. J Neurosurg 1980; 53:
633�641.
�v»w xX ¼ Y390
72

36� Katz RI, Goldberg HI, and Selzer ME. My-cotic aneurysm: Case report with novel sequen-
tial angiographic findings. Arch Intern Med
1974; 134: 939�974.
37� ���� ����� ��� �� �� ����� ����� ����� ������ !"#$%&"'(�)*+,- 1.� )/012 2002; 30: 73�78�
34*+5678$%9:�;3�<- 1. 391
73

Abstract
Internal Carotid Artery Occlusion Caused by
Infantile Infectious Endocarditis
Yoshitaka Mizuniwa1, Jun Hiramoto1, Yu Furuya1, Shinji Muto2,
Masahide Chikada3, and Takuo Hashimoto1
We present a case of occlusion of the internal carotid artery in an infant with infectious endocarditis. A
one-year-old boy su#ered a generalized tonic seizure during treatment for fever of 38�39�C.. Cranial MRIand MR angiography revealed cerebral infarction in the left middle cerebral artery territory and occlusion of
the left internal carotid artery. A tumor-like lesion in the left atrium was suspected as the source of the
embolosm. He underwent a cardiotomy to prevent a recurrence of cerebral embolism with resection of the
tumor-like lesion in the left atrium. The operative diagnosis was a vegetation caused by infectious
endocarditis in the left atrium. After e#ective treatment with antibiotics, he was discharged with moderate
right hemiparesis.
This rare case serves as a reminder and warning that screening examinations of the heart are essential,
especially in cases of pediatric cerebral infarction with occlusion of a main branch artery.
1 Department of Neurosurgery, St. Marianna University School of Medicine2 Department of Pediatrics, St. Marianna University Schol of Medicine3 Department of Cardiovascular surgery, St. Marianna University School of Medicine
���� �� � �392
74






![3406[21] - Marianna Uigakukai.marianna-u.ac.jp/idaishi/www/346/01-34-06Sayuri Shirai.pdf · Abstract A Case of Rapidly Progressive Glomerulonephritic Syndrome Carried by Anti-glomerular](https://img.pdfslide.us/doc/110x75/5e4b5fbd1c6106693c54dcc9/340621-marianna-shiraipdf-abstract-a-case-of-rapidly-progressive-glomerulonephritic.jpg)













![Trends in the incidence of primary malignant brain tumors ... · PDF fileradiation and rare hereditary syndromes such as neurofibromatosis [4]. The relation between primary malignant](https://img.pdfslide.us/doc/110x75/5ab80d297f8b9ad3038c5f97/trends-in-the-incidence-of-primary-malignant-brain-tumors-and-rare-hereditary.jpg)