Conclusions
• There were no deleterious neurologic findings with brief,
closely monitored treatment interruption in participants who
previously started ART during acute HIV infection
• Some participants did experience increased depression,
anxiety, or distress after viral rebound, although there were no
group differences pre- and post-ATI
• Global NPZ scores improved slightly post-ATI, which may be due
to practice effect over a short testing interval.
• Two ATI participants had detectable CSF HIV RNA with plasma
viral rebound, one during fairly low cps/mL of plasma HIV RNA. Both
were in the VHM intervention study and received active drug.
Neither had any neurologic exam findings.
• Sensitive DTI measures could not detect neuroimaging changes
with brief ATI
• While we found ATI to be safe in this context, the neurologic
impact is not known for ATI participants with chronic HIV, or for
longer ATI periods with higher thresholds for restarting ART (e.g.
plasma viral load >2,000 cps/mL for 4 weeks). Close neurologic
monitoring is needed for further ATI studies pursuing HIV remission
or cure.
AcknowledgementsWe are grateful for the RV254/SEARCH 010
participants and support through the International NeuroHIV Cure
Consortium (INHCC.net) This work was supported by K23MH114724,
R01MH095613, R01MH095613, and NIMH support of cooperative agreement
W81XWH-07-2-0067, as well as the US Military HIV Research Program.
The views expressed are those of the authors and should not be
construed to represent the positions of the U.S. Army or the
Department of Defense.
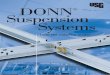
Undetected CSF HIV RNA
Quantified CSF HIV RNA
**p=0.004
plasmane
opterin
Cerebrospinal fluid resultsDetectable CSF HIV RNA in 2 of 39 CSF
samples (two separate participants) discussed below
• Pre-ATI LPs: n=18 (median 36 days prior, IQR: 7, 69)
• During ATI LPs: n=16 (median 19 days into ATI, IQR: 10,26)
• Last day of ATI LPs (pre-ART): n=5 (median = 28 days into ATI,
IQR: 23, 37)
• Two participants in VHM study receiving active drugs had
detectable CSF HIV RNA with viral rebound• #1: 29 days into
ATI:
• plasma HIV RNA = 329 cps/mL • CSF HIV RNA = 25 cps/mL
• #2: 32 days into ATI, on last day of ATI before ART: • plasma
HIV RNA = 35,796 cps/mL• CSF HIV RNA = 42 cps/mL
* Neither participant had neurologic abnormalities
Diffusion tensor imaging results
Figure 5. Comparing pre-ATI with during ATI DTI findings (n=12;
median 27 days into ATI [IQR: 17, 35] and 5 days before restarting
ART [IQR: 1, 9])
Background• The central nervous system (CNS) is a likely
reservoir of
HIV and is vulnerable to viral rebound and increased
inflammation upon cessation of ART.
• Careful evaluations of CNS outcomes are critical for HIV
remission studies employing analytic treatment interruption
(ATI).
Methods• This study investigated changes in neurologic
measures
in 24 participants across three small, closely monitored HIV
remission trials involving ATI in participants who previously
initiated ART during acute HIV infection (AHI).
o n=6 participants initially started ART in Fiebig I AHI and
later underwent ATI with no added intervention
o n=7 participants received a combination of vorinostat,
hydroxychloroquine, maraviroc (VHM) pre-ATI (plus n=1 who received
VHM placebo)
o n=8 participants received the broadly neutralizing VRC01
antibody at and during ATI (plus n=2 who received VRC01
placebo)
• Criteria for restarting ART included confirmed plasma HIV RNA
>1,000 cps/mL.
• Pre-ATI and post-ATI (on the day of, or after ART resumption)
assessments included standard measures of mood and anxiety;
ACTG-derived macroneurological exam; Color Trails 1 and 2; Grooved
Pegboard; Trail-making A; and the computerized Flanker Task.
• Elective tests included cerebrospinal fluid (CSF) sampling
(pre-ATI, during ATI at first plasma HIV RNA > 20 cps/mL, and
post-ATI) and brain diffusion tensor imaging (DTI; pre-ATI and
during ATI).
• Analyses employed paired t-test and ANOVA.
Participant demographics
Depression, anxiety and distress results
Figure 1(A).PHQ-9 depression and (B) HADS-D depression scores
pre- and post-ATI (n=14). Median of 17 days post-ATI
Figure 2. (A)HADS-A anxiety and (B) Distress thermometer scores
pre- and post-ATI(n=14). Median of 17 days post-ATI.
Macroneurological exam findings
Figure 3. Number of neurologic findings by participant pre- and
post-ATI (n=23). Post-ATI = median of 11 days. Additionally, the
proportion of participants with any neurologic findings was
unchanged pre- and post-ATI at 26%.
Neuropsychological testing results
Figure 4. (A) Global z-score for four neuropsychological tests
pre-and post-ATI (n=12) and (B) Flanker computed score pre, during,
and post-ATI (n=16) . Median post-ATI = 18 days.
A B
CROI 2018 March 4-7Boston, MA
Poster # 445 Joanna Hellmuth1, Donn Colby2, Eugene Kroon2, Carlo
Sacdalan2, Phillip Chan2,Jintana Intasan2, Victor Valcour1, Trevor
Crowell3,4, Linda Jagodzinski3, Khunthalee Benjapornpong2, Nelson
L. Michael3,4, Jintanat Ananworanich3,4, Robert Paul5, Serena
Spudich6, on behalf of the SEARCH
010/RV254 Study
Group1.MemoryandAgingCenter,DepartmentofNeurology,UniversityofCalifornia,SanFrancisco,California,USA;2.SEARCH,ThaiRedCrossAIDSResearchCenter,Bangkok,Thailand;3.U.S.MilitaryHIVResearchProgram,WalterReedArmyInstituteofResearch,SilverSpring,Maryland,USA;4.HenryM.JacksonFoundationfortheAdvancementofMilitaryMedicine,Bethesda,
Maryland,USA;5.MissouriInstituteofMentalHealth,UniversityofMissouri-St.Louis,MO,USA;6.YaleUniversity,NewHaven,Connecticut,USA
0
5
10
15
PH
Q9
depr
essi
on s
core
pre-ATI post-ATI
p=0.510
0
2
4
6
pre-ATI post-ATI
n=23
p=0.516
# of
neu
rolo
gic
findi
ngs
0
5
10
pre-ATI post-ATI
p=0.677
HA
DS
-A a
nxie
ty s
core
0
2
4
6
8 p=0.252
pre-ATI post-ATID
istr
ess
ther
mom
eter
0
5
10
HA
DS
-D
depr
essi
on s
core
p>0.999
pre-ATI post-ATI
ATIparticipantdemographicsAge, years (IQR) 32 (26.4, 34.9)Sex,
(M:F) 23:1Fiebig I/II (%) 54HIV subtype
CRF01_AE (%) 75
CRF01_AE/B (%) 12.5B (%) 12.5
Years on ART, (IQR) 3.8 (2.6, 4.8)CD4, cells/mm3 (IQR) 746 (564,
870)Plasma HIV RNA at ATI