Embed Size (px)
Citation preview

BREECH DELIVERY
-Deepa Mishra M. Sc. Nursing (OBG)

INTRODUCTIONA breech birth is the birth of
a baby from a breech presentation, in which the baby exits the pelvis with the buttocks or feet first as opposed to the normal head-first presentation. In breech presentation, fetal heart sounds are heard just above the umbilicus. In a breech presentation, the lie is longitudinal and the podalic pole presents at the pelvic brim. It is the commonest malpresentation.

DEFINITIONIt is a longitudinal lie in which the
buttocks is the presenting part with or without the lower limbs.
According to Nima BhaskarA breech birth is the birth of a baby
from a breech presentation, in which the baby exits the pelvis with the buttocks or feet first as opposed to the normal head-first presentation.
According to Wikipedia

INCIDENCE3-4% of fetus present by breech
at term5% at 34 weeks20% at 28 weeks20% diagnosed initially in labour3.5% term singleton deliveries
and about 25% of cases before 30 weeks of gestation undergo spontaneous cephalic version up to term.

TYPES
Complete Breech (Flexed Breech)
Incomplete Breech(30-35%)

1. Complete Breech (Flexed Breech)
The normal attitude of full flexion is maintained.
The thighs are flexed at the hips and the
legs at knees.
The presenting part consists of two
buttocks, external genitalia and two feet.
It is commonly present in multiparae.

2. Incomplete Breech(30-35%)
Buttocks variety (70%)
Incomplete variety with procidentia: One or more little parts (footling, knees) precede the buttocks.
Sacro-anterior positions are more common than sacroposterior as in the first the concavity of the fetal front fits into the convexity of the maternal spines

Frank Breech• It is breech with extended legs where the
knees are extended while the hips are flexed.• More common in primigravida.
Footling Presentation• The hip and knee joints are extended on one
or both sides.• More common in preterm singleton breeches.
Knee Presentation• The hip is partially extended and the knee is
flexed on one or both sides
INCOMPLETE BREECH

TYPES OF INCOMPLETE BREECH

CLINICAL VARIETIES
Uncomplicated
It is defined as one where there
is no other associated obstetric
complications apart from the
breech, prematurity being
excluded.
Complicated
When the presentation is associated with conditions which
adversely influence the
prognosis such as prematurity,
twins, contracted pelvis, placenta
praevia etc.
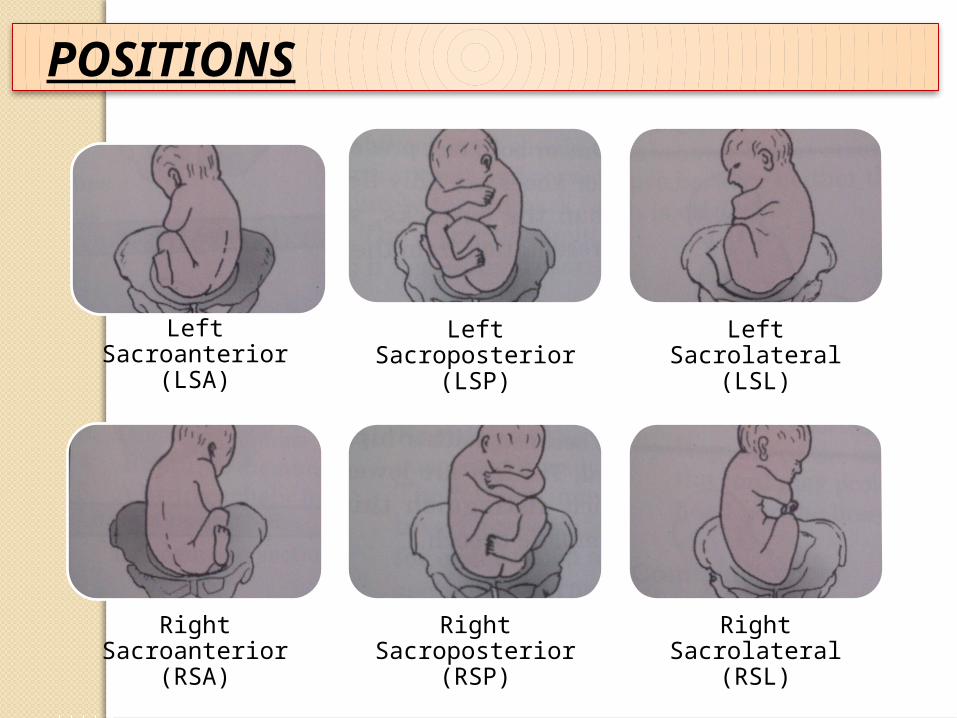
POSITIONS
Left Sacroanterior (LSA)
Left Sacroposterior (LSP)
Left Sacrolateral (LSL)
Right Sacroanterior
(RSA)
Right Sacroposterior
(RSP)
Right Sacrolateral (RSL)

Prematurity
Factors preventing spontaneous version
Favorable adaptation
Undue mobility of the fetus
Fetal abnormality
Etiology Of Breech Presentation
CLINICAL
SONOGRAPHY
RADIOLOGY
DIAGNOSIS

CLINICAL Complete Breech Frank Breech
Per Abdomen Fundal Grip Head-
suggested by hard and globular mass
Head is ballottable
Head Irregular small
parts of the feet may be felt by the side of the head.
Head is non-ballottable due to splinting action of the legs on the trunk.
Lateral Grip Fetal back is to one side and the irregular limbs to the other
Irregular parts are less felt on the side

CLINICAL Complete
BreechFrank Breech
Pelvic Grip
F.H.S.
Breech- suggested by soft, broad and irregular mass.
Breech is usually not engaged during pregnancy
Usually located at a higher level round about the umbilicus
Small, hard and a conical mass is felt
The breech is usually engaged
• Located at a lower level in the midline due to early engagement of the breech
Per Vaginum During Pregnancy
During labour
Soft and irregular parts are felt through the fornix
Palpation of ischial
tuberosities, sacrum and the feet by the sides of the buttocks
The foot felt is identified by the prominence of the heel and lesser mobility of the great toe.
Hard feel of the sacrum is felt, often mistaken for the head
• Palpation of ischial
tuberosities, anal opening and sacrum only

Ultrasonography
1. It confirms the clinical diagnosis- specially in primigravidae with engaged frank breech or with tense abdominal wall and irritable uterus.2. It can detect fetal congenital abnormality and also congenital anomalies of the uterus.3. Type of breech (complete or incomplete).4. It measures biparietal diameter, gestational age and approximate weight of the fetus.5. It also localizes the placenta.6. Assessment of liquor volume (important for ECV).7. Attitude of the head- flexion or hyperextension (Important for decision making at the time of delivery).8. CT and MRI can be used to assess the pelvic capacity in addition to all the above mentioned information.

DURING PREGNANCY
• A transverse groove may be seen above the umbilicus in sacro-anterior corresponds to the neck.
• If the patient is thin, the head may be seen as a localized bulge in one hypochondrium
Inspection
• Fundal Grip: The head is felt as a smooth, hard, round ballottable mass which is often tender.
• Umbilical Grip: The back is identified and a depression
• First pelvic Grip: The breech is felt as a smooth, soft mass continues with the back. Trial to do ballottement to the breech shows that the movement is transmitted to the whole trunk.
Palpation
FHS is heard above the level
of the umbilicus. However in
frank breech it may be heard at
or below the level of the umbilicus.
Auscultation
• To confirm the diagnosis.
• To detect the type of breech.
• To detect gestational age and foetal weight: Different measures can be taken to determine the foetal weight as the biparietal diameter with chest or abdominal circumference using a special equation.
• To exclude hyperextension of the head.
• To exclude congenital anomalies.
• Diagnosis of unsuspected twins.
Ultrasonography

DURING LABOUR
The 3 bony landmarks of breech namely 2 ischial tuberosities and tip of the scarum.
The feet are felt beside the buttocks in complete breech.
Fresh meconium may be found on the examining fingers.
Male genitalia may be felt.

Delivery of the buttocks
Shoulders
Head
MECHANISM OF LABOUR
• The engagement diameter is the bitrochantric diameter 10 cm which enters the pelvis in one of the oblique diameters.
• Descent of the buttocks occurs until the anterior buttock touches the pelvic floor.
• Internal rotation of the anterior buttock occurs through 1/8th of a circle placing it behind the symphysis pubis.
• Further descent with lateral flexion of the trunk occurs until the anterior hip hinges under the symphysis pubis which is released first followed by the posterior hip.
• Delivery of the trunk and the lower limbs follow.
• Restitution occurs so that the buttocks occupy the original position as during engagement in oblique diameter.
Delivery of Buttocks
• Bisacromial diameter (12 cm or 4 ¾”) engages in the same oblique diameter as that occupied by the buttocks at the brim soon after the delivery of breech.
• Descent occurs with internal rotation of the shoulders bringing the shoulders to lie in the antero-posterior diameter of the pelvic outlet. The trunk simultaneously rotates externally through 1/8th of a circle.
• Delivery of the posterior shoulder followed by the anterior one is completed by anterior flexion of the delivered trunk.
• Restitution and external rotation :
Delivery of Shoulders

• Engagement occurs either through the opposite oblique diameter as that occupied by the buttocks or through the transverse diameter. The engaging diameter of the head is suboccipito-frontal (10 cm).
• Descent with increasing flexion occurs.
• Internal rotation of the occiput occurs anteriorly, through 1/8th or 2/8th of a circle placing the occiput behind the symphysis pubis.
• Further descent occurs until the sub-occiput hinges under the symphysis pubis.
• The head is born by flexion- The chain, mouth, nose, forehead, vertex and occiput appearing successively. The expulsion of the head from the pelvic cavity depends entirely upon the bearing efforts and not at all on uterine contractions.
• Sacro-posterior position: The mechanism is not substantially modified. The head has to rotate through 3/8th of a circle to bring the occiput behind the symphysis pubis.
Delivery of Head
MATERNAL
FETAL
PROGNOSIS

The Fetal Dangers• Intracranial Haemorrhage• Asphyxia• Injuries
Prevention of the Fetal Hazards• The incidence of breech can be minimized by
external cephalic version where possible.• If the version fails or is contraindicated, delivery is
done by elective caesarean section.• A skilled obstetrician along with an organized team
consisting of a skilled anesthetist and an assistant should conduct vaginal breech delivery.
• Vaginal manipulative delivery should be done by a skilled person with utmost gentleness, specially during delivery of the head.
ANTENATAL MANAGEME
NT
Identification of the
complicating factors
External cephalic version
Formulation of the
line of managem
ent

Indications:
Procedure
Preliminaries
Benefits of External Cephalic Version
Causes of failure of version
Dangers of Version
Management, if version fails or is contraindicated
External Cephalic Version

Indications for caesarian
Big Baby (estimated fetal weight>3.5 kg)
Hyperextension of the head
Footling presentation (risk of cord prolapse)
Suspected pelvic contraction
Any obstetrical or medical complications
During First Stage
Cases seen first time in labour with presence of complications
Arrest in the progress of labour
Non-reassuring FHR pattern
Cord presentation or prolapse
ELECTIVE CAESARIAN SECTION

Indications for vaginal breech delivery
Adequate pelvis
Average fetal weight (1.5-3.5 kg)
Flexed head and without any other complications
Management of Vaginal Breech Delivery
First Stage
Second Stage
VAGINAL BREECH DELIVERY

Preliminaries for conduction of normal labour
Anaesthetist to administer anaesthesia as and when requiredAn assistant to push down the fundus during contractions.
Instruments and suture materials for episiotomy
A pair of obstetric forceps for the after coming head, if required.
Appliances for revival of the baby, if asphyxiated
Principles in conduction
Never to rush
Never pull from below but push from above
Always keep the fetus with the back anteriorly.
ASSISTED BREECH DELIVERY
Steps
Patient is to be placed in lithotomy position when the posterior buttock distends the perineum.To avoid aortocaval compression
Antiseptic cleaning
Pudendal block
Episiotomy
Patient is encouraged to bear down
Soon after the trunk upto the umbilicus is born
Delivery of the arms
Delivery of the after coming head
Burn-Marshall method
Forceps deliveryMalar Flexion and Shoulder traction (modified Mauriceau-Smellie- Veit technique)Resuscitation of the baby
Third Stage
ASSISTED BREECH DELIVERY

MANAGEMENT OF COMPLICATED
BREECH DELIVERY
Delayed in Descent of the Breech
Extended Arms
Arrest of the After-coming
Head

Arrested at the Outlet
In the absence of outlet contraction and feto-pelvic disproportion
Arrest of the breech at or above the level of ischial
spines
Frank Breech Extraction (Pinard’s Maneuver)
Delayed in Descent of the Breech

Extended arms is due to faulty technique in delivery using unnecessary traction, forgetting the principle of
‘never pull but push from above’
Diagnosis is made by noting the winging of the scapula and absence of the flexed limbs in front of the chest.
Management :
The management calls for the urgent delivery of the arms, first the posterior and then the anterior one.
The delivery of the arm may be accomplished by adopting any one of the following methods:
Classical
Lovset
Extended Arms

At the Brim
In the Cavity
At the Outlet
Delivery of the head through an incompletely dilated cervix
Occipito- posterior position of the head through an incompletely dilated cervix
Arrest of After Coming Head

CONCLUSION:
The incidence of Breech presentation expected to be low in hospitals where high parity births are minimal and routine external cephalic version done in antenatal period. Breech presentation can be managed by early diagnosis and effective management strategies. By using different maneuvers and skillful observation of the obstetrician.