Embed Size (px)
Citation preview

« Decentralization of HIV care in subsaharan Africa: lessons for resource
allocation»
Dr. Fred Eboko, IRD French Research Institute for the Development, Marseille.
France
Session : « The Impact of the Economic Crisis on HIV Programs: Is Integration to Health Systems the Solution? »
6th IAS Conference on HIV Pathogenis, Treatment and Prevention
Rome – 17-20 July 2011
Ministère de la Santé Publique du Cameroun
“Financing a sufficient and sustained response to the HIV epidemic in low-and middle-income countries has emerged as one of the world’s greatest health and development challenges, and one that will be with us for the foreseeable future. International assistance from donor governments, through bilateral aid and contributions to the Global Fund to Fight AIDS, Tuberculosis and Malaria (the Global Fund) and other financing channels such as UNITAID (the international drug purchase facility) is a critical part of this response”
(Kaiser Family & Unaids, 2010: 1)
A challenge
Background (1/2)A scientific answer to the challenges of Public Health
Context Continuous decrease in prices of ARV in Cameroon- 1999: 700 - 1000$ /patient/month.- 2001: 300-600 patients under ART- 2005: 2,5$/patient/ : 15 000 patients unnder ARV- May 1st 2007, ART Free Access - December 2009 : 76 228 patients treated 46.5% of eligible patients in Cameroon.
A new policy of decentralization A national and international issue
An objective Evaluate an ongoing process and propose objective insights
Background (2/2)
ANRS research program includes 4 projects :– Decentralization of ARV access in Africa: Evaluation of the
treatment of patients on ARV in district hospitals using a streamlined follow-up approach (Trial Esther/STRATALL)
– Impact of the Cameroonian access to an ARV program on the treatment and living conditions of the HIV infected population (EVAL)
– The problem of access to ART in Cameroon. Issues, Advances, Limits and Perspectives of health care decentralization (POLART)
– Scaling up and procurement of drugs and biological monitoring tools
ObjectivesEvaluation of the Impact of access to ARV on the living conditions of PLWHA– Adherence and medical effectiveness– Quality of Life– Risky sexual behaviors
Evaluation of the impact on the health system– Impact on medical knowledge and practice– Changes introduced in the organization of Health Care
MethodsQuantitative– Cross-sectional survey among 3151 HIV+ adults and 317 healthcare
personnel included in 27 treatment centers– Data capture of treatment centers characteristics
Qualitative : Semi-structured interviews of patients and healthcare staff
EVAL ANRS 12 116 Pr. Moatti (Inserm Marseille), Pr. Abega (UCAC Yaoundé)
A relatively high quality of healthcare in decentralized treatment centers– Average increase in CD4 count for patients treated for at
least 6 months not different from that found at a national level: 12.5 cells /µL/ month
– Significantly higher adherence for those patients treated at district treatment centers: 61.2% of patients have a high adherence score versus 44.5% in centralized treatment centers
– Physical Quality of Life comparable to that found at central service level and a better Mental Quality of Life
FEASABILITY DEMONSTRATED FOR DECENTRALISING ART TREATEMENT
EVAL ANRS 12 116 – Main results
Trial Esther/STRATALL ANRS 12 110Pr. Delaporte (IRD Montpellier), Dr Kouanfack (HCY Ydé)
Volet sciences sociales : Pr. Moatti (INSERM), Pr. Abega (†) /C. Abé (UCAC)
« Decentralization of ARV access in Africa: Evaluation of the treatment of patients on ARV in district hospitals using a
streamlined follow-up approach (STRATALL)”
Social Sciences Objectives Evaluation of the streamlined follow-up on 4 aspects:
- Quality of Life- Adherence - Socio-economic feasability - Behavioral Disinhibition
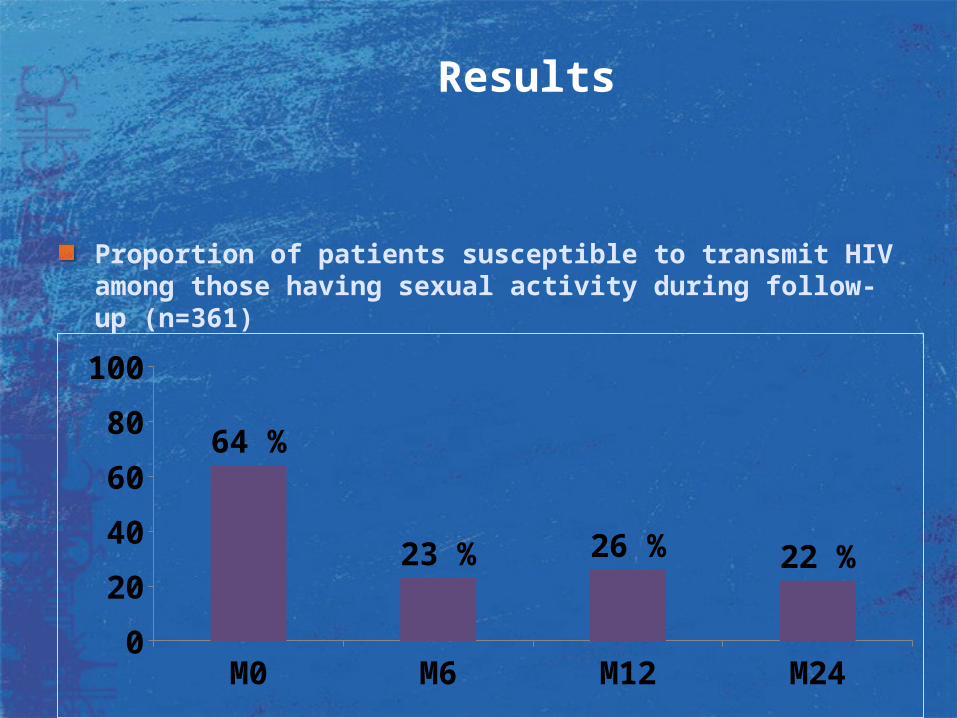
Results
Proportion of patients susceptible to transmit HIV among those having sexual activity during follow-up (n=361)
M0 M6 M12 M240
20
40
60
80
100
64 %
23 % 26 % 22 %
POLART ANRS 12 120Dr F. Eboko (IRD/FPAE), Pr. Sindjoun (GRAPS, Un. Ydé 2)
Objectives - Identify actors involved in the decentralization of ARV
treatment (institutions, local associations of PLWHA, international Cooperation)
- Analyze their roles and structures- Analyze the effect of external partners’ involvement in
the process of decentralization- Understand the qualitative factors which differentiate
health care quality from one site to another
Methods - Qualitative Study :
Interviews with patients: Therapeutic Itineraries and biographies Interviews with the different actors (institutions, local
associations of PLWHA, international Cooperation)
Elements of analysis
Decentralization can come in a variety of forms: deconcentration, devolution, privatization
Decentralization of access to ARV in Cameroon corresponds in a general way to a process of deconcentration
The involvement of external actors in certain provinces or health facilities leads to other types of decentralization which are not exclusive from each other: - Between devolution and privatization: the hospital “Fondation Suisse de
Petté”- Between decentralization and saturation: The intervention of the Swiss
MSF in Douala Reinforcement of the relative autonomy of UPEC at Nylon and of CMA at
Congo 2 but saturation of services due to the reputation and quality of health care/
The contribution of the Cameroonian program to international questions
Long term and financial sustainability of free access to medicines? Optimal degree of decentralization to enable scaling-up?
New distribution of tasks between healthcare providers (“task shifting”) to find solutions to the Human Resources crisis?
Impact of AIDS programs on the fight against other diseases (tuberculosis, malaria) and on the global reinforcement of the health care system?

From economics to politicis? Multidisciplinary proposals. Work in
progress
« Cameroun, Burkina Faso, BotswanaAIDS Policy in Africa. A Comparative Approach ». (2007-2011)(Eboko, Owona N., Enguéguélé, 2009)
Governance and AIDS in Africa. Barriers, limits and perspectives (Senegal, Burkina Faso, Cameroon, Cote d’Ivoire) ».
Learning from defeat and success in Funding and Governance …
Thanks
Patients
AIDS NGOs in Cameroon
Healthcare professionals and personnel of Healthcare facilities
Ministry for Public Health in Cameroon
National AIDS Committee
Regional Delegation of Public Health
National Agency for research on AIDS and Hepatitis B & C (ANRS, France)
French Cooperation (SCAC, Yaounde)
AIDES

THE ITALIAN GOVERNMENT STILL OWES 260 MILLION EUROS TO THE GLOBAL FUND AND
NEVER PLEDGED FOR 2011 - 2013
ITALY:KEEP THE PROMISE, NOW!
FUND THE FUND, NOW! AIDS, TUBERCOLOSIS AND MALARIA WILL NOT WAIT!
The teamsCameroonL’UCAC : – Institut de Recherche Socio-anthropologique
(IRSA) Dir. : Pr. S.C. Abega/ Pr C. Abé
– Groupe d’Études, de Recherche et de Conseil sur l’Insertion Sociale (GERCIS)Dir. : Pr. R. Nantchouang
L’Université de Yaoundé 2 – Groupe de Recherches Administratives, Politiques
et Sociales (GRAPS) Dir. : Pr. L. Sindjoun
L’Université de Yaoundé 1 :– Center for Applied Social Sciences – Research
and Training (CASS-RT)Dir. : Pr. P. Nkwi
Fondation Paul Ango Ela pour la géopolitique en Afrique Centrale (FPAE) Yaoundé)Dir. : Mme K. Ango Ela
FranceL’UMR 912 INSERM-IRD-U2 – (www.ur002.ird.fr)
Dir. : Pr. J.-P. Moatti