Embed Size (px)
Citation preview
Bi-Monthly Neunlefter for Professional Information Only June 2004
Ankle $prain
Auntie May Leen was taking her usual morning stroll in the park when suddenly while crossing over acurb she slipped and fell. Almost immediately, a sharp excruciating pain shot up from her right foot.She could see her right ankle ballooning before her eyes. With some help from a passer-by, AuntieMay Leen managed to limp back to her car and withstanding the horrible pain. She drove home andasked her husband to send her to the nearest clinic.
The above scenario is a classic example of an ankle sprain. Ankle sprain can occur even whilewalking on uneven grounds! Ankle sprain is one of the most common injury which is frequentlymisdiagnosed and receive the least proper treatment. lt is a condition whereby the ligaments of theankle joint is stretched or torn when there is a sudden inversion or eversion of the foot.
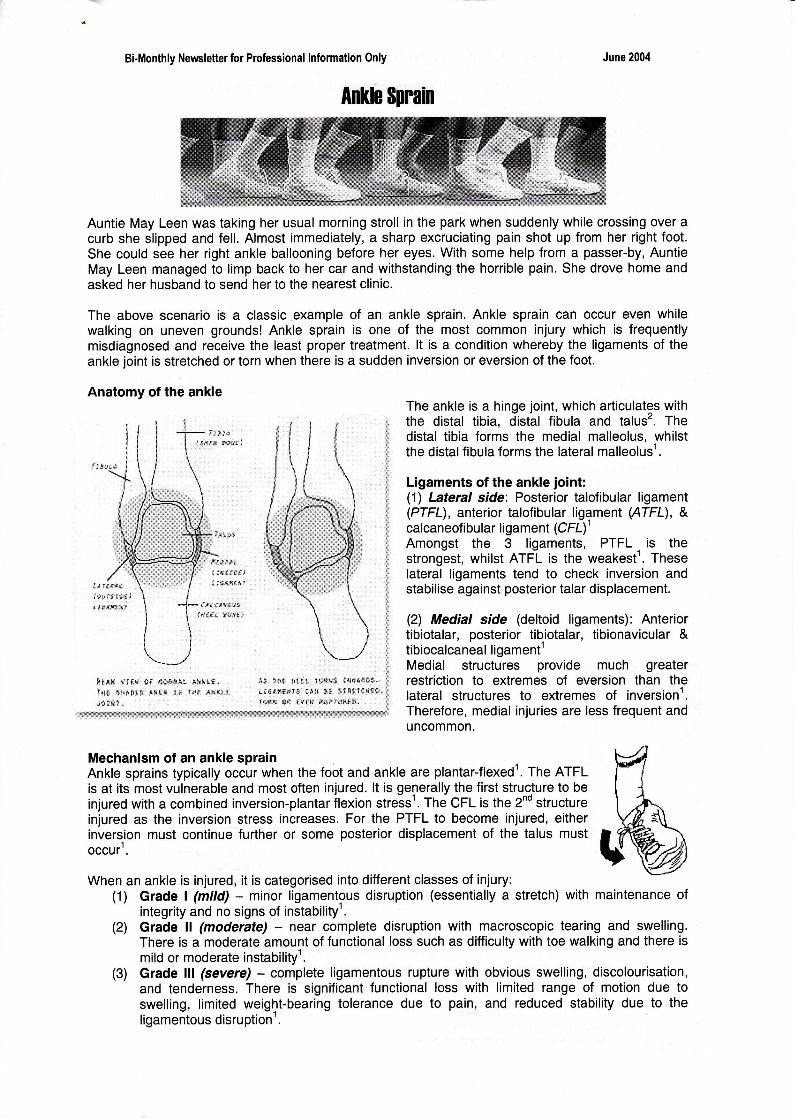
Anatomy of the ankle
n:[].* t't t!r {t ris[]tar'r. .4**.16.lr{ ttc*s{:tr rrt.r I t ls* .{?i?t.tid trti" -
*,I. grrll xllr. 1a:l*fts l{xt&tss,ti6.d!4Ht{rE {i,t *g !lsfY{.*a*,t$!is fr* .f v(sr ftrll'l{l{t:tl*,
The ankle is a hinge joint, which articulates withthe distal tibia, distal fibula and talus'. Thedistal tibia forms the medial malleolus, whilstthe distalfibula forms the lateral malleolus'.
Ligaments of the ankle joint:(1\ Lateral side: Posterior talofibular ligament(PTFL), anterior talofibular ligament (ATFL), &calcaneofibular ligament (C FL)'Amongst the 3 ligaments, PTFL. is thestrongest, whilst ATFL is the weakest'. Theselateral ligaments tend to check inversion andstabilise against posterior talar displacement.
(2) Medial side (deltoid ligaments): Anteriortibiotalar, posterior tibiotalar, tibionavicular &tibiocalcaneal li gament'Medial structures provide much greaterrestriction to eltremes of eversion than thelateral structures to extremes of inversionl,Therefore, medial injuries are less frequent anduncommon.
Mechanism of an ankle sprainAnkle sprains typically occur when the foot and ankle are plantar-flexed'. The ATFLis at its most vulnerable and most often injured. lt is generally the first structure to beinjured with a combined inversion-plantar ilexion stresst. The CFL is the 2nd structureinjured as the inversion stress increases. For the PTFL to become injured, eitherinversion must continue further or some posterior displacement of the talus mustoccur .
When an ankle is injured, it is categorised into different classes of injury:(1) Grade | (mild) - minor ligamentous disruption (essentially a stretch) with maintenance of
integrity and no signs of instability'.(2) Grade ll (moderate) - near complete disruption with macroscopic tearing and swelling.
There is a moderate amount of functional loss such as difficulty with toe walking and there ismild or moderate instabilityl.
(3) Grade lll (severe) - complete ligamentous rupture with obvious swelling, discolourisation,and tenderness. There is significant functional loss with limited range of motion due toswelling, limited weight-bearing tolerance due to pain, and reduced stability due to theligamentous disruption'.

Ankle sprain can also be categorised as being acute or chronic injury. Symptoms include :(1) sensation of a tear or pop with a "rolling over" of the ankle (suggesting ATFL or CFL tear)l(2) anteriorly based pain with inability to bear weight following the foot's "getting stuck", whilst
the leg continues to rotate (suggest syndesmosis injury)'(3) swelling"(4) discolourisation'(5) inability to move the ankle properly(6) pain in the ankle even when non-weight-bearing"
An acute ankle injury can be obtained from the history and physical examinationt. An assessment ofankle sprain injuries should also include sensory examination to identify whether the nerves werestretched during the period of injury1. The initial aims of treating an ankle sprain involve minimisingswelling and inflammation. lmportant factors contributing to early recovery include protection, earlymotion, weight bearing and rehabilitation'.
Rest
It is recommended not toweight-bear too much onthe affected foot. as thiswill cause further injury.
lmmobilisation
Having proper support andimmobilisation, aids therecovery of the injuredligament and surrounding softtissue. An ankle brace will helpto immobilise the ankle joint,preventing inversion andeversion movements.
Reference:1.
Ankle Sprain Management
Cold Compression
Apply cold pack ai the site ofinjury as often as possible. Thecold will provide_local contractionof blood vessels'.This will reduceswelling & pain .
flrr'i" *iir n"rp to reduce\*1d fluid pooling at the feet.
Ankle Exercises
Can aid in strengthening theankle and maintaining jointrange of motion of the ankle,thus reducing stiffness.
Medication,
Anti-inflammatorymedication can help toreduce inflammation.
Tip: Try using a pillowundemeath the ankle
lf the pain if unbearable during weight bearing, it is advisable to use a walkingaid (e.9. crutches, quadripod) to aid walking'. The period for recovery fromankle sprain varies, depending on factors such as age, severity of injury'.
Ankle sprain must not be looked upon lightly. Proper care and managementmust be taken seriously to prevent the ankle from re-injuring, causing repeatedtrauma to the joint, ligaments and soft tissue. There is a higher probability ofsustaining another ankle, especially if it is mismanaged. As a result, theindividual may suffer from chronic pain of the ankle joint and may lead to otherassociated problems.
How to prevent further ankle iniury?-Avoid sharp turns & quick changes in direction & movemenf
Pertorm gentle stretches prior to any sporting activitiessIt is advisable to wear the ankle brace for at least 3 monthseven if there is no pains
Braddom, R.L., Bushchbacher, R.M., Dumitru, D., Johnson, E.W., Matthews, D. & Sinaki, M.(2000). Physical Medicine and Rehabilitation (2no Edition). Saunders. pp.843-847.Brotzman, S.B. (1996). Clinical Orthopaedic Rehabilitation. Mosby. pp.246-257.Rouzier, P. (1999) The Sports Medicine Patient Advisor. Sports Medicine Press.
A Newsletter of DORSET REHABEmail : [email protected] : www. geocities.com/dorset_rehab
2.3.
Ankle Brace





























