Embed Size (px)
Citation preview
Classification of gestational trophoplastic
diseases (GTD)Incidence of malignant GTDPathophysiologyClinical presentationHow to diagnose malignant GTDPrognoses of malignant GTDTreatment of malignant GTD
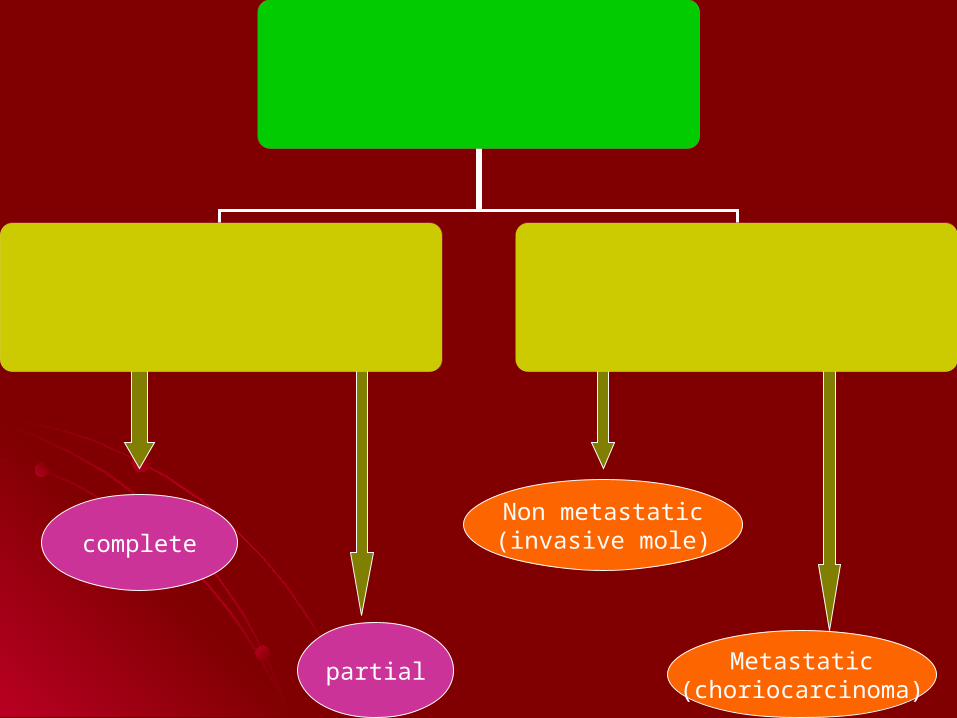
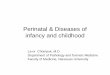
complete
partial
Non metastatic)invasive mole(
Metastatic)choriocarcinoma(
1.Chorio carcinoma will follow complete H.mole in
50%
2 .Chorio carcinoma will follow partial H.mole in
0.5%
3. Whole HCG assay is used for follow up after
H.mole evacuation.
4. Serum progesteron is not used as tumor marker for malignant GTD.
5. Surgery is superior to chemotherapy in the treatment of malignant GTD
MALEGNANT GESTATIONAL TROPHOPLASTIC DISEASES
Incidence west: 1 in 30000
oriental: 1 in 11000 Geographical area Preceding pregnancy H.mole :50% normal pregnancy: 40% abortion or ectopic:5% non gestational:5% Maternal B.group
more with group A , less with group O
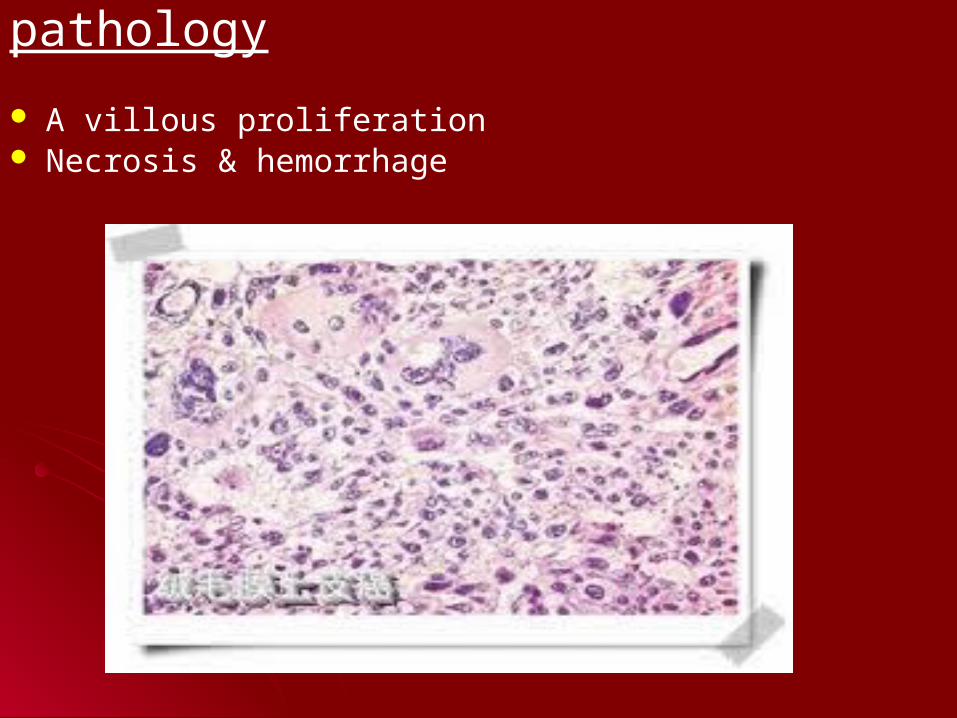
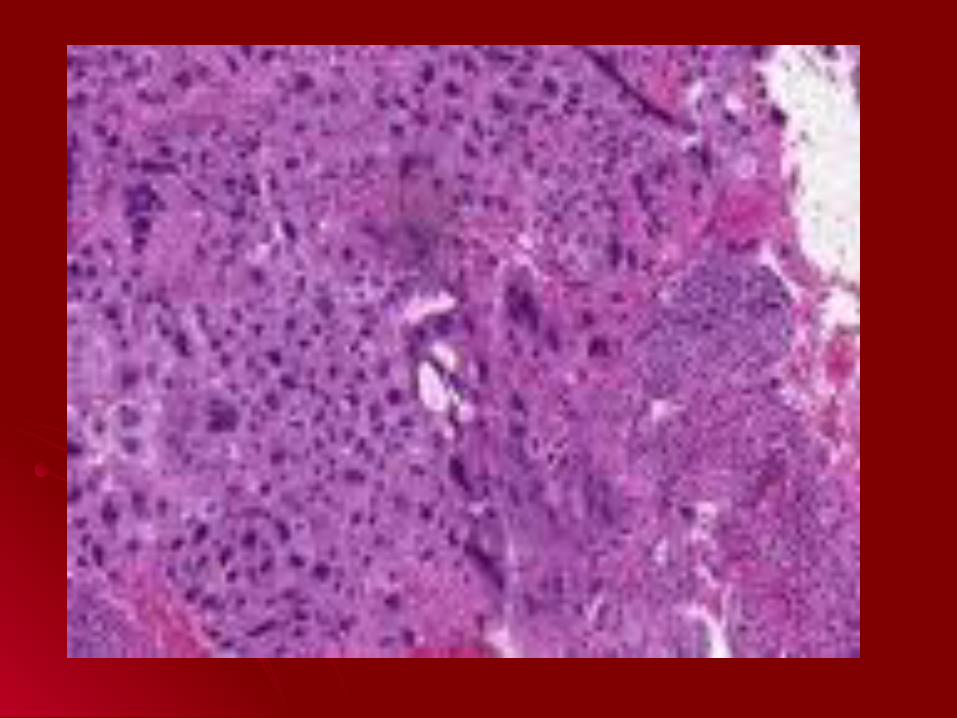
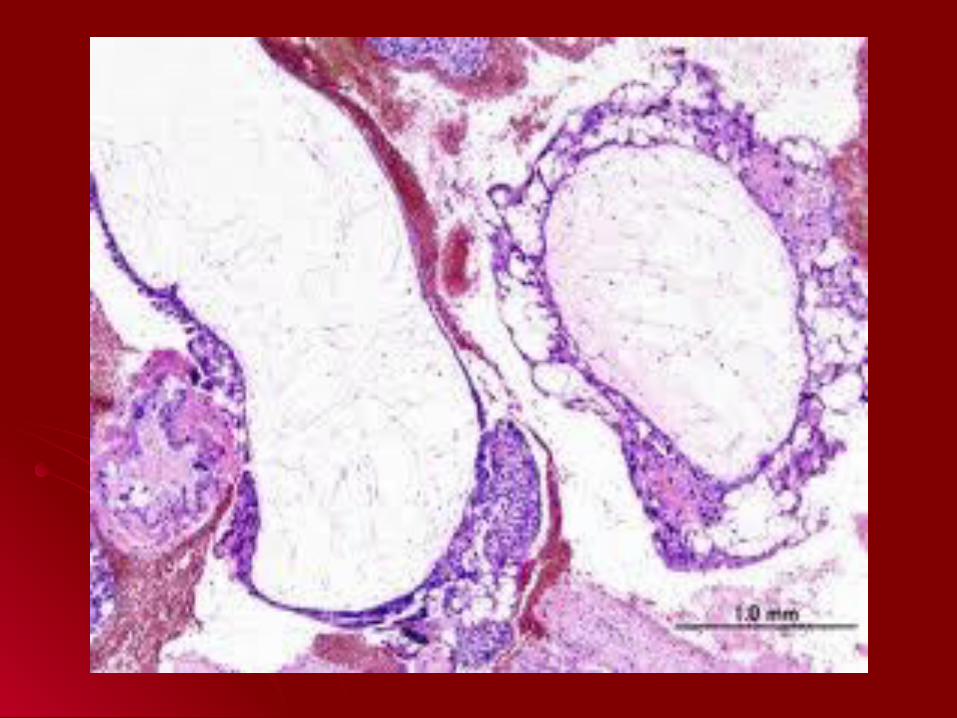
pathology
A villous proliferation Necrosis & hemorrhage
Clinical presentationVaginal bleedingAmenorrheaAbdominal massSymptoms of distant metastasis
(pulmonary, GIT , brain)
Diagnosis1. B hCG follow up after H. mole evacuation A. urinary hCG >30000 iu/24hr or serum hCG >20000 iu/L B. progressive increase of hCG at any time after evacuation of H.mole C. detected hCG 5-6 months after evacuation or
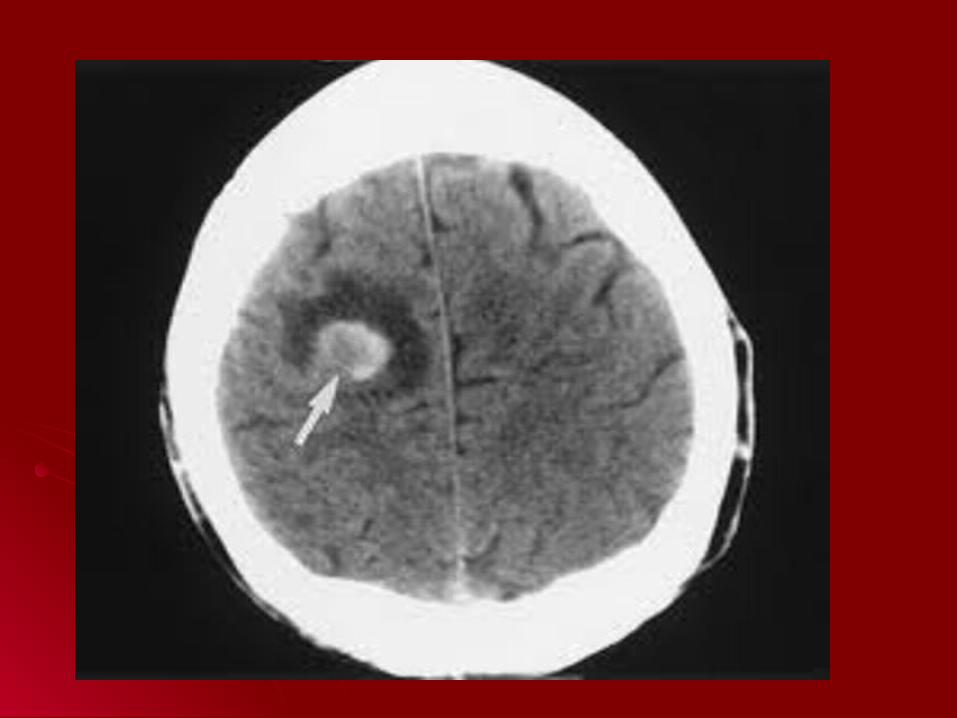
platue level for 3 months D. evidence of intracranial , hepatic or GIT
metastasis E. persistent vaginal bleeding with raised hCG F. pulmonary metastasis with raised hCG
2. Histopathology
3. U/S ,CXR & CT scan

Prognosis hCG level: 100000 iu/24 hr in urine 40000 iu/L in blood
Interval between preceding pregnancy & diagnosis
4 months
Intracranial or hepatic metastasis
Size of the tumor : 8 cm
Previous chemotherapy
Preceding gestation is term pregnancy
Treatment 1.Chemotherapy : very sensitive tumor
2.surgery: Sever bleeding Complete family Resistant to chemotherapy Persistent uterine mass or solitary nodule To decrease the duration of chemotherapy
3. radiotherapy: very poor results






Low risk group Methotrxate 1mg/kg & folinic acid 6mg im or 15 mg
orally after 30 hrs for 8 days & rest for 6 days before starting
further course 80% of cases respond to this treatment if resistant to this drug develops then actinomycin D in
dose of 10- 13 µgm/kg/day iv for 5 days
High risk groupComplicated multiple drugs