Embed Size (px)
Citation preview

© Change Management and Community Pharmacy Project i

Authors Chief Investigator Distinguished Professor Dexter Dunphy, University of Technology, Sydney Principal Investigators Professor Ian Palmer, Associate Dean (Research and Development), Faculty of Business, University of Technology, Sydney Professor SI (Charlie) Benrimoj, Dean, Faculty of Pharmacy, University of Sydney Ms Alison Roberts, PhD Candidate, Faculty of Pharmacy, University of Sydney Core Research Team Change Management and Community Pharmacy Project, Faculty of Business, University of Technology, Sydney: Ms Julie Allan, Project Director Ms Eleonora Feletto, Senior Research Assistant Ms Joanna Leonard, Research Assistant Sydney Health Projects Group, School of Public Health, University of Sydney1: Professor Michael Frommer, Adjunct Professor and DirectorDr Lucie Rychetnik, Senior Associate Ms Christine Madronio, Research Officer Dr Angela Todd, Senior Associate Medici Capital Pty Ltd: Mr Frank Sirianni, Principal Researcher for Project Mr Jock Rowland, Project Manager Mr Dominic Malvaso, Project Officer Other Research Team Members Ms Catherine Smithson, Consultant Ms Helen Stark, Consultant Ms Michelle Toms, Consultant Mr Bruce Annabel, Johnston Rorke2
1 Section 2 of the report was prepared by the Sydney Health Projects Group in conjunction with Professor Benrimoj and Ms Roberts from the University of Sydney. 2 Section 5: 4.6.5 was completed by Johnston Rorke in conjunction with Professor Benrimoj and Ms Roberts from the University of Sydney.
© Change Management and Community Pharmacy Project ii

Acknowledgements We are grateful for the financial support of this project provided by the Australian Government Department of Health and Ageing through the Third Community Pharmacy Agreement Research and Development Grants Program, administered by the Pharmacy Guild of Australia. We also gratefully acknowledge the hard work and contributions of the members of the EAG and Reference Group (see below) who contributed thoughtful advice throughout the project. EAG members:
John Bronger Barry Schultz Warwick Plunkett Allan Neate/John Primrose John Chapman
Reference Group:
Bill Scott John Daffey Shane Britnell
We also wish to thank the Research and Development Grants Division in the National Office of the Pharmacy Guild of Australia who were an unfailing source of information and useful advice throughout the project, in particular:
Lance Emerson Erica Vowles Simone Jones
Our thanks also go to The Pharmacy Guild of Australia’s Third Agreement Coordinators in the State branches for their help in many areas of the project. We are grateful to all those who helped us in data gathering, analysis and other areas, especially at UTS. A special thank you goes to:
Belinda Sant Daisy Bracken Geoff Breach Bernadette Yao.
Special thanks also to all the pharmacists and other participants in the study who took part in interviews, focus groups, case studies and the mail survey.
© Change Management and Community Pharmacy Project iii

Authors’ Disclaimer The authors do not accept any risk or responsibility for matters including byt not limited to losses, damages, costs and other consequences resulting directly or indirectly from using this report and any information or material available from it. To the maximum permitted by law, UTS excludes all liability to any person arising directly or indirectly from using this report and any information or material available from it.
© Change Management and Community Pharmacy Project iv

Executive Summary
SECTION 1: INTRODUCTION
Research ObjectivesActual vs Desired Outcomes
SECTION 2: FUTURE CERTAINTIES IN HEALTHExamination of social trends to identify future opportunities for the provision of cognitive services through community pharmaciesIntroduction of Characterising Opportunities Filter
SECTION 3: EXPLORING THE PHARMACISTS’ WORLDTargeted literature review of change management in community pharmacyResearch methodology: mail survey, focus groups, case studies, consumer forums, stakeholder interviews
SECTION 4: STRATEGIC OPTIONS FOR PHARMACY
Assessment of current cognitive services offeredIntroduction of Pharmacy Viability Matrix (PVM)Presentation of 24 pharmacy case studies, including 8 with additional innovative characteristicsFinancial and economic modeling analysis of the case studies andmail survey
SECTION 5: CLOSING THE GAPIntegrates research results from all sources to show how gap can be closed between current service delivery and desired future service deliveryIntroduction of Pharmind Wheel: implementing change in context of the health and pharmacy industryIntroduction of Pharmacy Change Readiness Wheel: a practical tool for pharmacists to use to check whether their pharmacy is ready to introduce a change in service provisionIntroduction of Pharmacy Implementation Wheel: a tool to help pharmacists design and implement change for their pharmacyPractical application of the five introduced tools
© Change Management and Community Pharmacy Project v

Executive Summary
EXECUTIVE SUMMARY
Objectives of the study The Final Report of the Change Management and Community Pharmacy Project (RFT 2003-06) is designed to fulfil the following overall objectives for the project:
Analyse the current and potential provision of services within community pharmacies
Assess product-service business mix and develop business models applicable to increasing cognitive service provision
Develop practical change strategies to support community pharmacies in the uptake of such services
Provide implementation programs for service uptake. An overall summary of how each of the tender objectives was addressed can be found in Section 1 “Introduction”.
Research methods used The overall development of the Project was undertaken by the four principal investigators subject to regular reporting and approval procedures by the External Advisory Group (EAG). A review of demographic, disease and health-service trends was undertaken to identify opportunities for community pharmacy to enhance existing professional services and introduce new professional services likely to be valued by the community and governments. An instrument was developed, the Characterising Opportunities Filter (COF), which presents seven dimensions the Guild can use to characterise the potential professional services community pharmacy can deliver. COF can also be used by owners of individual pharmacies to evaluate new options for service delivery. In addition, criteria are provided to assist in the selection and evaluation of services. In this section of the report we limited the discussion of these services to those that are health related only. The results are presented in Section 2 “Future Certainties in Health”. The exploration of current and potential services was also undertaken. A selective and targeted literature review examined local and overseas research studies relevant to pharmacy change, cognitive service provision and pharmacist related behavioural models for change. The results indicated areas where significant research had been undertaken and where further research is needed. In particular the review highlighted the fact that, while there is strong international evidence for many pharmacies moving to provide more services, nowhere in the world has a planned change management program been undertaken to enhance community pharmacy’s service offerings on a national basis. In the past the focus has been on changing the patient-pharmacist relationship but the emphasis is now moving to implementing change within the pharmacy itself. An ambitious field research program was designed and carried out covering pharmacists, internal and external stakeholders and consumers. The field research involving pharmacists used three major research approaches: focus groups, case studies of pharmacies, and a mail survey of a representative sample of Australian community pharmacies. The field research began with ten focus groups, made up of 102 pharmacists, drawn from locations around Australia. These focus groups were conducted jointly by experienced facilitators and members of the research team and alerted researchers to issues of concern to pharmacists in pharmacy change and service provision. The focus
© Change Management and Community Pharmacy Project vi

Executive Summary
groups provided important information for the subsequent development of research instruments used elsewhere in the study (e.g. in case studies and in the mail survey of pharmacies). Results of the focus group research are integrated in the report in section 5 and detailed in appendix 5. Twenty four case studies of pharmacies were then carried out and these are presented in section 4. The case studies are designed as practical examples of a range of product and service provision models in pharmacy which can be used in educational and training programs on pharmacy change. Finally a representative sample of Australian pharmacy owners/managers was carried out – surveys were mailed to 2,022 pharmacies and 403 responded. After resending the survey, the number of respondents increased to 575. General results of the survey relating to service provision and pharmacy change are presented in section 4 with the full results in appendix 3. A second research instrument was devised, the Pharmacy Viability Matrix, which allows systematic comparison of four basic pharmacy business strategies and their impact on service provision. The four strategies are defined by their range of products and services and their community scope and are labelled as Traditional Pharmacy, Expanded Pharmacy, Focused Specialty pharmacy and Multi Specialty pharmacy. Case study pharmacies and the pharmacies covered in the mail survey were classified into these four strategy types and compared on a number of dimensions. Financial analyses were also undertaken by Medici Capital to assess the relative financial viability of these four strategies. These analyses included: financial performance, risk score, cost index and indicative valuation. The main analysis of the four strategy types is presented in section 4 chapter 2. The study also explored the attitudes of health consumers and opinion leaders in the industry to current service provision by pharmacy and their attitudes to potentially increased service delivery in future. A total of 68 consumers and consumer representatives participated in the consumer forums. A systematic analysis was also made to identify the key stakeholders for pharmacy and 51 interviews conducted with representatives of these stakeholder groups. The large volume of focus group and interview data was analysed using a systematic social science content analysis method (with NVivo data management software) which facilitates the identification of major themes emerging in verbal data of this kind. This led to the development of three further instruments, the PharmInd Wheel, the Pharmacy Change Readiness Wheel and the Pharmacy Change Implementation Wheel. The qualitative data analysed using NVivo was incorporated into these three wheels. The PharmInd Wheel presents the data relevant to designing and implementing a change program for the industry as a whole. The argument presented is that enabling change to extended service provision, at the level of the individual pharmacy. will proceed more effectively when the Guild initiates and implements an industry wide national change program. This will provide a more supportive context within which pharmacy change is facilitated. The rationale for this change program and its key components is presented in the PharmInd Wheel. The basis for these arguments and suggested programs is drawn from two sources: (1) the interviews and forums with industry stakeholders and health consumers and (2) current literature on organisational change. The Pharmacy Change Readiness Wheel and the Pharmacy Change Implementation Wheel are designed as systematic tools for individual pharmacy owners or pharmacy network managers to design change programs for greater service provision at the pharmacy level. The basis for these arguments and suggested programs is drawn from two
© Change Management and Community Pharmacy Project vii

Executive Summary
sources: (1) field research including interviews and focus groups with pharmacists and case studies of pharmacies, and (2) current literature on organisational change. The Pharmacy Change Readiness Wheel assists pharmacy managers to assess whether their pharmacy is ready to undertake a significant change program or has more preparatory work to do before launching such a program. Once the pharmacy is ready for change, the Pharmacy Change Implementation Wheel then presents the pharmacist with a systematic approach to planning and implementing a change program to increase service provision at the pharmacy level. The use of all three Wheels is illustrated in a practical example – instituting a change program designed to deliver hypothetical disease state management services for asthma. A number of assumptions have been made as to what would constitute disease state management services, however, this example can readily be replicated for any similar cognitive service. Finally an additional study is provided to illustrate how a pharmacist (or the Guild) could go about costing service provision at the pharmacy level. In this case the hypothetical disease state management service example used is diabetes.
Results of the study: Future Certainties in Health (Section 2) first examines the prospective health profile of a growing and ageing Australian population and the role of pharmacy in providing for future health needs. It identifies some of the future demand characteristics in the health area, which include:
An increase in chronic and some communicable diseases Increased demand for inpatient and community-based health services A shift toward self-management by patients, supported by their carers A shift toward greater emphasis on health promotion and disease prevention
Pharmacies represent an existing community-based network with a powerful potential to contribute to many areas, including:
Healthy lifestyle and disease prevention The provision of community-based health services Advice to carers and patients in self-management of chronic illnesses Assisting in the quality use of medicines
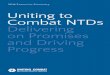
Specific services related to these generic areas of service provision are identified and it is argued that the Guild needs to develop a more comprehensive strategic view of service provision by the profession. In order to achieve this, the COF (figure i) was developed to assist the Guild to identify a wider range of opportunities, review these opportunities more systematically and identify in particular:
A core of essential services to be provided by all pharmacies An additional range of differentiated and specialised services to be offered
optionally by pharmacies in response to more localised consumer demand Use of a greater variety of delivery systems Ways of adequately funding all service offerings through government and other
sources
© Change Management and Community Pharmacy Project viii

Executive Summary
Figure i: Characterising Opportunities Filter
Payment by client
Other payers e.g. insurance
Payment by government
4By source of remuneration
7In relation to
resources required
6In relation to the business setting
5By community
pharmacy’s professional role
3In
spectrum of
pharmacy activity
2In spectrum of
client/ professional engagement
1In spectrum
of health care
Service-orientated
Professional care delivery
• Substitution by community pharmacy of service of service previously provided by others
• Used to be a pharmacy role and now trying to regain it again
• Loss of role
Combined
• Supplementation by community pharmacy of service provided by others
Skills:1. Basic
education2. Continuing
education3. Training
Incentives
Infrastructure
Options include:1. Shop2. Other
professional premises
3. Mixed (1) & (2) pharmacy only
4. With other professionals (1) – (3)
5. Patient’s home
6. Nursing home
7. Facilitators8. E-pharmacy9. Others
• Novel service being provided by community pharmacy
ProductSelf-management
Prevention
Early detection
Diagnosis and assessment
Treatment
Rehabilitation
Palliation
Section 2 concludes with an examination of the consequences for pharmacy and other community stakeholders if these decisions are adopted. Section 3 “Research Methodology” outlines the field research methodologies used in the study – the results of which are presented in section 4.
Section 4 “Strategic Options” focuses on assessing current and future service offerings by pharmacies. Section 4 addresses three questions:
What services are currently being offered by pharmacies and what is their perceived profitability and level of satisfaction?
What services are planned for the future? What factors influence the ability to deliver?
The analyses made to answer the first two questions come from Part 3 of the mail survey. In the survey, pharmacists were asked a series of questions about 33 enhanced services. Under the current Agreement the results show a high percentage of pharmacies offering these services. Pharmacists seemed consistently satisfied with these service offerings but perceive them as not particularly profitable. Services currently under consideration by the Guild for the 4th Community Pharmacy Agreement showed a range of over a third to a half of respondents already offering the services and many of those who are not yet offering them are planning to do so over the next year. Given the limitations of the survey we were not able to determine the depth of service offering; however, these results are
© Change Management and Community Pharmacy Project ix

Executive Summary
encouraging in that they indicate anticipatory readiness for change despite no current government funding for the services at this stage. The third question above deals with the ability of pharmacies to deliver. At present, it is the larger pharmacies, by size (square metres) and dispensing volume that appear to offer more services. Overall the majority of respondent pharmacists indicated that they were open to new ideas and potential changes in the workplace but other data from the survey indicate that over half of respondents will not change unless it is in reaction to some threat. Additionally, the Guild may need to recognise that some pharmacies, even if enthusiastic about change, may need to increase their capacity to change. The survey also examined factors that influence pharmacists to change – the most important factors were the relevance of the fit of the service with their business strategy, an understanding of the benefits of the new service, a financial analysis and costing of the new service, pharmacy layout and the availability of training. This built on work by Roberts et al (2003/4). The section concludes with recommendations to the Guild for the acceleration of change. Section 4 then presents the overall results for the four strategic options presented in the Pharmacy Viability Matrix (see figure ii). The Pharmacy Viability Matrix defines pharmacies by two variables: the community scope (vertical axis), that is, their market focus within their local community or extended beyond their local community; and the breadth of product/service choice (horizontal axis) they offer to their customers. For example, by definition, a Traditional Pharmacy only serves its local community and has a narrow range of products and/or services.
Figure ii: Pharmacy Viability Matrix
Focused Specialty Multi Specialty
Traditional Pharmacy Expanded Pharmacy
COMMUNITY
SCOPE
EXTENDED
LOCAL
NARROW BROAD
PRODUCT/SERVICE CHOICE
Core Pharmacy Product and Service Offering
All four strategic options were financially viable when subjected to the Medici Capital financial analysis which derives from a banking valuation perspective. However, there were
© Change Management and Community Pharmacy Project x

Executive Summary
systematic differences between the strategies on financial variables. On financial performance for example, Multi Specialty pharmacies performed best and Traditional Pharmacies worst. However Multi Specialty pharmacies have higher risk scores which may offset their financial performance. There are a variety of other characteristic differences between the pharmacies classified into the four business strategies – for example, Traditional pharmacies typically offered the lowest percentage of enhanced services compared to the other three categories and Multi Specialty pharmacies offer the most. The case studies give very specific and detailed examples of how these strategies work in practice. Section 5 presents the three Change Wheels introduced above. The results presented here are qualitative in character and the analyses are specifically directed to providing recommendations to the Guild for introducing a specific industry-wide change program to enhance the context within which change toward greater service provision can take place (PharmInd Wheel – figure iii).
Figure iii: PharmInd Wheel
Policies, Politics &
Perspectives
Administrative
Governance & Decision-Making
Processes
Resourcing &
Revenue Flows
Marketing & Selling
to Stakeholders & Consumers
Industry
Re-structuring
Non-pharmacy
Threats & Opportunities
Delivering &
Accelerating Industry Change
Health & Allied
Stakeholders
An important part of this chapter relates to the detailed data derived from key stakeholder representatives whose support can potentially accelerate the change or whose opposition can derail it. We provide a series of recommendations, based on these interviews, that amount to the Guild taking initiatives to develop an informal collaborative governance system for resolving differences in the industry and capitalising on common interests to consolidate pharmacy’s role as a vital part of a community-based primary health care service.
© Change Management and Community Pharmacy Project xi

Executive Summary
Figure iv: Pharmacy Change Readiness Wheel
Profitability
Perspective
Assessment of
Need for Change
Resource Availability
Measurements &
MetricsAssessing Risk
Change
Orientation
Information &
Knowledge Availability
Skills Audit
Time Availability &
Timing AnalysisHistory of Past
Changes
The remainder of section 5, as noted above, is addressed to pharmacists and uses the qualitative data derived from pharmacist interviews, focus groups and case studies. The Pharmacy Change Readiness Wheel (figure iv) and the Pharmacy Change Implementation Wheel (figure v) represent practical prescriptions for change implementation at the pharmacy level and are specifically designed for use by pharmacists. The first practical example at the end of the Report for the provision of asthma services shows how all three wheels can be applied to defining a comprehensive disease state management service. The second practical example, for diabetes management, creates a template for a financial analysis that can be applied to specific disease management services.
© Change Management and Community Pharmacy Project xii

Executive Summary
Figure v: Pharmacy Change Implementation Wheel
Allocating
Resources for the Change
Responding to &
Managing Resistanceto the Change
Aligning the
Change
Communicating
the Vision & theChange
Situating & Leading
the Change
Triggering the
Motivation to Change
Helping and
Assisting the Change
Marketing the
Change
Integrating &
Consolidating the Change
Planning the
Change
To conclude, we have made recommendations for Guild initiatives that may help move the industry context in a way that facilitates the introduction and expansion of change programs in pharmacies which will widen the scope of professional service offerings and promote health. These measures are designed to make multi level changes that can energise the potentially powerful health service delivery system comprising Australia’s 5,000 community pharmacies, making them an even more vital element in the creation of more integrated health service delivery in local communities. Detailed recommendations for Guild action are appended to this Executive Summary with references to the main text of the Report.
© Change Management and Community Pharmacy Project xiii

Recommendations
Recommendations
Macro Policy Issues
1. In order to effectively deliver and accelerate change, the Guild should ensure that it systematically addresses and considers adopting the recommendations in various sections of this report (Section 5: 1.9.1)
2. The Guild should utilise the PharmInd Wheel as a matter of priority noting that effective change management for industry consists of a structured approach to addressing stakeholder issues and delivery of a systematic change program for pharmacies. (Section 5: 1.9.1)
3. The Guild needs to move from a model of service delivery based primarily on ”all pharmacies offering all services” to a more flexible model where all pharmacies offer a core set of services but in addition specialised services are offered by a more limited number of pharmacies on the basis of their strategic choice and consumer need. (Section 2: 6)
4. The Guild should use systematic procedures and processes to assess new opportunities for service provision in pharmacy and use the structured framework for decision making outlined in the Characterising Opportunities Filter. (Section 2: 4.2)
5. Once services have been selected, the Guild needs to develop position papers on the role of community pharmacy in providing those services (e.g. the role of community pharmacy in specific disease states). (Section 2: 5.3)
6. Services that are selected for negotiation and implementation need to fit within the policy framework of and be matched with the needs of payers, i.e. governments, third party payers and consumers. (Section 2: 4.5)
7. To build industry-wide support for further service provision, the Guild should move to develop formal and informal collaborative governance structures with other health service providers. (Section 5: 1.4.3)
8. The Guild should pursue all possible means to integrate the policy positions and continuing collaboration between the Guild and PSA (Section 5: 1.2.8)
9. The Guild and the PSA should work with each other and with the Divisions of General Practice, to assist in supporting the further development of these structures at a local level (Section 5: 1.4.3)
10. As part of the process of negotiations relating to the 4th Community Pharmacy Agreement, the Guild should negotiate with the Australian Government to streamline the translation of negotiated new policy into implementation plans. (Section 5: 1.4.1)
11. The Guild should map the current structure of the industry using the Pharmacy Viability Matrix (PVM) and support further research into appropriate service groupings related to the PVM strategy types. This will facilitate the development of policies for increased service provision for pharmacy in the future. (Section 4: 2.3)
12. The Guild should work with leading pharmacies that are using these strategies to increase service provision related to the PVM strategic types; evaluate and document the success of these programs for increased service provision and then support the diffusion of this new knowledge through the industry. (Section 4: 2.3)
© Change Management and Community Pharmacy Project xiv

Recommendations
Systematic Methods of Identifying and Reviewing Opportunities
13. In its preparation for the 4th Agreement, the Guild needs to adopt the systematic approach to selecting and evaluating services proposed in this Report, using the Characterising Opportunities Filter, together with the recommended criteria. (Section 2: 5.3)
14. Using the seven dimensions in the Characterising Opportunities Filter, the Guild should undertake a mapping exercise for the introduction of future cognitive pharmaceutical services in community pharmacy. (Section 2: 4.2)
15. By making use of the Characterising Opportunities Filter, the Guild should determine the likely range of services to be provided by pharmacy and estimate the potential extent of their adoption in the next decade. (Section 5: 1.5.2)
16. Services identified in the mapping exercise should be prioritised according to the criteria for selecting and evaluating the opportunities. (Section 2: 5.2.5)
17. A greater focus needs to be given to the funding of cognitive pharmaceutical service opportunities from sources other than the Australian Government. (Section 2: 4.4)
18. The Guild should continue to conduct environmental scans and use appropriate channels to update pharmacists on emerging challenges and opportunities for the industry (Section 4: 1.4.2)
Macro Implementation Issues
19. Funding for research and development negotiated in the Fourth Agreement should be targeted towards opportunities identified as a result of previous recommendations in this Report. (Section 2: 7)
20. In addition to issues of policy, the Guild should give consideration to the implementation issues surrounding a particular service or set of services at the time of selecting the service, i.e. before negotiation. (Section 2: 4.5)
21. The Guild needs to plan to a. build up the industry’s capability to implement a service or group
of services prior to a program for new service provision being disseminated and
b. identify funding sources to assist in this. (Section 2: 4.2) 22. The Guild should place more emphasis on developing implementation plans and
financial reward structures when introducing new services. (Section 4: 1.5) 23. In making submissions for government funding, particularly for the 4th Agreement,
the Guild should ensure that policy proposals are accompanied by implementation plans with time horizons and resourcing estimates (for examples see Section 5 chapter 4). (Section 5: 1.2.9)
24. The Guild should address a number of factors needed to help increase service implementation, such as producing a clear benefits statement of the proposed services which addresses the business, professional and personal considerations involved. (Section 4: 1.6)
25. The Guild should make the Pharmacy Change Readiness and Pharmacy Change Implementation Wheels available to pharmacists (see later recommended communication strategy). (Section 4: 1.4.3)
26. The Guild should further investigate how network membership impacts on the rate of service adoption. (Section 4: 1.3.2)
© Change Management and Community Pharmacy Project xv

Recommendations
Structuring and Guiding Future Service Provision
27. In relation to existing current service offerings, the Guild should work to ensure that the current level of adoption is extended and deepened. It is important to continue to consolidate the changes already introduced. (Section 4: 1.2.2.1)
28. The Guild needs to ensure it has widespread community support for the continuing provision of drug distribution through pharmacies as points of convenient access to the general community. (Section 5: 1.2.1)
29. The Guild needs to ensure that the high proportion of pharmacies now accredited for the Quality Care Pharmacy Program deliver a drug distribution system which underpins service provision to a high standard. (Section 5: 1.2.1)
30. The Guild needs to ensure that its competitive advantage of being sole provider of prescriptions funded by the Government is maintained on the basis that it provides sound advice to patients and other health professionals on the safe and effective use of medicines. (Section 5: 1.2.1)
31. The Guild should continue to encourage pharmacies to move their product/service mix in the direction of increasing the professional service component (Section 5: 1.2.2)
32. The Guild should advocate a two tier service delivery system consisting of core services and specialty health services. This must be done in such a way so as to ensure access for all Australians to the core service offering in community pharmacy, while allowing for differentiation in areas of specific need and/or demand. (Section 5: 1.2.7)
33. The Guild needs to define which health services and products make up the “core” offering in community pharmacy, and what can be considered “specialised”. (Section 2: 6)
34. The Guild should group services for more efficient implementation and maintenance. (Section 5: 1.2.3)
35. The Guild needs to provide a cost benefit analysis of the investment pharmacies need to make for implementing and delivering services. (Section 5: 1.5.3)
36. In the interests of equity, the Guild should propose continuing and extended special financial provision by governments for ‘essential’ services to disadvantaged groups (Section 5: 1.2.6)
37. The Guild should take steps to ”map” areas of disadvantage where special services are needed and advocate increased government funded service delivery in these areas. (Section 5: 1.2.6)
38. The Guild needs to examine the potential of IT infrastructure to overcome some of the deficits in service adoption and provision in pharmacies situated in rural and remote communities. (Section 5: 1.5.3)
39. The Guild needs to work closely with suppliers to develop a shared IT network with the capability of delivering more resources for service provision (product information and service support provision) to leverage pharmacy’s strengths. (Section 5: 1.5.3)
40. The Guild needs to expand the QCPP quality assurance process to cover the full range of services to be adopted by pharmacies, in line with the approach taken for HMR. (Section 5: 1.5.2)
© Change Management and Community Pharmacy Project xvi

Recommendations
Stakeholder Management
41. The Guild should conduct a stakeholder mapping exercise when proposing and implementing new services as a basis for increasing stakeholder involvement and support. (Section 5: 1.3.12)
42. The Guild should collaborate with other health service delivery providers to move toward more integrated service delivery as part of primary health care provision at the community level. (Section 5: 1.2.4)
43. For services that are considered “supplementary” or “substitution” services, there should be an evaluation of the consultation required with key stakeholders, before the opportunity is pursued. (Section 2: 4.2)
44. The Guild needs to emphasise to pharmacists and other stakeholders that products can be a nexus around which related services can be developed with mutual benefit in sales of both (where the services are charged for). (Section 4: 1.3.4)
45. The Guild needs to ensure that governments, the public and consumer organisations are aware of the quality standards achieved. (Section 5: 1.2.1)
Building Human Capability for Increased Service Provision
46. The Guild needs to collaborate with education and training providers such as PSA and universities, to construct professional service training packages that prepare pharmacists and pharmacy personnel to operate across groups of services. (Section 5: 1.2.3)
47. The Guild needs to negotiate with universities and other providers of professional training to include change management training in undergraduate and postgraduate pharmacy courses (Section 5: 1.5.5)
48. The Guild needs to encourage and incentivise these institutions to create the appropriate educational courses or training modules to develop the competencies in potential practitioners. (Section 5: 1.5.2)
49. The Guild should sponsor a Change Management Qualification tailored specifically to the needs of pharmacy. This qualification should be available in various modes of delivery including online. (Section 5: 1.5.5)
50. The Guild should work with the PSA to set standards of excellence for service delivery. (Section 4: 1.4.1)
51. The Guild should work with the PSA to develop professional qualifications for pharmacists or pharmacy staff offering services (Section 4: 1.4.1)
52. The Guild should ensure the provision of appropriate education and training to support service delivery and to maintain service quality (Section 5: 1.2.7)
53. The Guild should assist in setting national educational standards for management education, relating to service provision, as part of a pharmacist’s training. (Section 5: 1.9.1)
54. The Guild to work with PSA on specifying the competencies needed by practitioners in order to deliver related services to a defined standard of excellence. (Section 5: 1.5.2)
55. The Guild needs to select the institutions best fitted to develop these competencies. (Section 5: 1.5.2)
56. The Guild should work with educational providers to ensure that there are sufficient trained and/or accredited personnel to deliver new services. (Section 4: 1.4.1)
© Change Management and Community Pharmacy Project xvii

Recommendations
57. The Guild should ensure that any training or accreditation processes are endorsed and supported by the appropriate patient support organisation. (Section 5: 1.3.12)
58. The Guild should establish a Centre of Excellence in Community Pharmacy Change Management to assist in accelerating the implementation of services. (Section 5: 1.7.5)
Accelerating Implementation: A. Raising Awareness
59. It is important that the Guild addresses the issue that a significant number of its members believe that the Guild does not have a good understanding of the practical implementation of new services. (Section 5: 1.1.1)
60. The Guild should demonstrate to its members that it has a realistic understanding of the practical issues and financial implications of implementing new services at a pharmacy level.(Section 4: 1.5)
61. The Guild should mount a communication program to increase the awareness of its members of the need for change and the priorities and plans for industry change. This communication program should use the channels identified in this Report as those most influential for pharmacists. (Section 5: 1.9.1)
B. Funding
62. As the majority of pharmacists perceive that service provision has low profitability, the Guild should demonstrate how to enhance the potential profitability of existing and future services. (Section 4: 1.2.2.1).
63. The Guild needs to develop a strategy for assisting pharmacists to make a cultural change towards charging for specialised service provision. (Section 5: 1.2.5)
64. The Guild should encourage the introduction of fee-for-service for value-added professional services not subsidised by governments or third party payers. (Section 5: 1.2.5)
65. The Guild should fund further micro-cost analyses to test and refine the business case for an individual pharmacy providing services. (Section 5: 4.6.5)
66. As a matter of priority, cost analyses should be incorporated into the existing research into potential services for the 4th Agreement such as Diabetes and Asthma DSM, and Clinical Interventions, using the business case as a template. (Section 5: 4.6.5)
67. The Guild should fund further research, building on the financial analyses from this Report, to determine a reasonable rate of return for service provision which can be used to negotiate with government to extend support for funded services. (Section 4: 4.6.1)
© Change Management and Community Pharmacy Project xviii

Recommendations
C. Mobilising the change
68. The Guild should identify and work with pharmacy owners/managers who appear more open to change and more innovative to establish working prototypes of new initiatives. (Section 4: 1.4.3)
69. The Guild needs to encourage practitioners with expertise in these areas, who are members of the Guild and/or the PSA, to act as mentors to newly graduated practitioners to accelerate the further development of their professional competence. (Section 5: 1.5.2)
70. In actioning an overall change program for the industry, the Guild needs to: a. identify the most change oriented pharmacies b. work with these pharmacies to plan the introduction of selected
high priority services c. develop with these lead pharmacies the overall design of
appropriate educational programs d. select suppliers to complete program designs and deliver programs
on a trial basis to lead pharmacies e. offer programs on a broader basis through the industry,
incorporating volunteers from the lead pharmacies to present on these programs. (Section 5: 1.9.1)
f. evaluate the trials and revise educational programs g. document the benefits including profit and financial benefits (see
section 4 – current and future services in conjunction with Roberts et al 2004)
h. promulgate these through the channels identified in this study as those most used by pharmacists. (Section 5: 1.9.1)
© Change Management and Community Pharmacy Project xix

Table of Contents
TABLE OF CONTENTS AUTHORS ii ACKNOWLEDGEMENTS iii EXECUTIVE SUMMARY vi RECOMMENDATIONS xiv TABLE OF CONTENTS xx LIST OF FIGURES xxxi LIST OF TABLES xxxiii ABBREVIATIONS xxxv
SECTION 1: INTRODUCTION 1 INTRODUCTION: WHY IS CHANGE MANAGEMENT SO IMPORTANT
FOR THE IMPLEMENTATION OF SERVICES IN PHARMACY? 3 2 DESIRED AND ACTUAL PROJECT OUTCOMES 8
SECTION 2: FUTURE CERTAINTIES IN HEALTH 1 INTRODUCTION 15
1.1 PURPOSE OF THIS SECTION 15 1.1.1 OBJECTIVES 15 1.1.2 REPORT STRUCTURE 15 1.2 PRODUCT AND SERVICE ROLES OF COMMUNITY PHARMACY 16
2 PREDICTIONS FOR THE HEALTH SYSTEM 19
2.1 OVERVIEW 19 2.2 DEMOGRAPHIC PHENOMENA 20 2.2.1 THE SIZE OF THE POPULATION 20 2.2.2 AGE STRUCTURE OF THE POPULATION 20 2.2.3 GEOGRAPHICAL DISTRIBUTION OF THE POPULATION 21 2.3 DISEASE PATTERNS 22 2.3.1 BURDEN OF DISEASE AND INJURY 22 2.3.2 COMMUNICABLE DISEASES 24 2.3.3 CHRONIC DISEASES AND ASSOCIATED RISK FACTORS 25 2.4 SOME CONSEQUENCES OF DEMOGRAPHIC CHANGES AND DISEASE PATTERNS 30 2.5 SAFETY AND QUALITY OF HEALTH SYSTEMS 31 2.6 UNMANAGED LARGE SYSTEMS 34 2.7 INFORMATION AND COMMUNICATION TECHNOLOGY 35 2.8 COSTS 37 2.9 COMMUNITY EXPECTATIONS 39 2.10 WORKFORCE 41 2.11 DISCONTINUITIES 44
3 TRENDS IN THE UK, THE USA AND CANADA 45
3.1 UNITED KINGDOM 45 3.2 UNITED STATES OF AMERICA 46
© Change Management and Community Pharmacy Project xx

Table of Contents
3.3 CANADA 48 3.4 IMPLICATIONS 49
4 OPPORTUNITIES FOR COMMUNITY PHARMACY 50
4.1 OVERVIEW 50 4.2 CHARACTERISING OPPORTUNITIES FILTER 51 4.3 ASSUMPTIONS FOR IDENTIFYING OPPORTUNITIES 56 4.4 TYPES OF OPPORTUNITIES 56 4.5 TIMING OF OPPORTUNITIES 60 4.6 GROUPING OPPORTUNITIES 61
5 CRITERIA FOR SELECTING AND EVALUATING OPPORTUNITIES 63
5.1 OVERVIEW 63 5.2 CRITERIA FOR SELECTING OPPORTUNITIES 63 5.2.1 (A) CRITERIA AT THE CONSUMER LEVEL 63 5.2.2 (B) CRITERIA AT THE GOVERNMENT LEVEL 64 5.2.3 (C) CRITERIA AT THE LEVEL OF PROFESSIONAL ORGANISATIONS 64 5.2.4 (D) CRITERIA AT THE LEVEL OF PHARMACY BANNER GROUPS 65 5.2.5 (E) CRITERIA AT THE LEVEL OF THE INDIVIDUAL COMMUNITY PHARMACY 65 5.3 POTENTIAL EVALUATION CRITERIA 66 5.4 STAKEHOLDER RESPONSE TO THE ASSUMPTIONS, OPPORTUNITIES, AND CRITERIA 67
6 CORE VS. SPECIALTY HEALTH SERVICES 68 7 CONCLUSION 70
SECTION 3: EXPLORING THE PHARMACISTS’ WORLD 1 TARGETED PHARMACY LITERATURE REVIEW: COMMUNITY
PHARMACY, SERVICE PROVISION AND CHANGE 73 1.1 INTRODUCTION 73 1.2 METHODOLOGY 74 1.3 TYPES OF SERVICES IN COMMUNITY PHARMACY 74 1.3.1 PHARMACEUTICAL CARE 74 1.3.2 COGNITIVE SERVICES 75 1.4 PHARMACIST LEVEL 76 1.4.1 PHARMACISTS’ PERCEPTIONS OF CHANGE/NEW SERVICES 76 1.4.2 PHARMACISTS’ SKILLS 77 1.4.3 INTERPERSONAL COMMUNICATION AND CONFIDENTIALITY 77 1.4.4 INTER-PROFESSIONAL ISSUES 77 1.4.5 MENTORS 78 1.4.6 WORKFLOW 78 1.4.7 BEHAVIOUR 78 1.4.8 ATTITUDE 79 1.4.9 PERCEIVED ROLES 79 1.4.10 CORE ROLE - WHAT PHARMACISTS “SHOULD” BE DOING 79 1.4.11 STEPS FOR PROFESSIONAL CHANGE 80
© Change Management and Community Pharmacy Project xxi

Table of Contents
1.5 PHARMACY LEVEL 80 1.5.1 RURAL VS URBAN 81 1.5.2 INTERNATIONAL MODELS 81 1.5.3 BARRIERS AND FACILITATORS TO CHANGE 81 1.5.4 STRATEGY 82 1.5.5 SERVICES 82 1.5.6 CHANGE 85 1.5.7 TOOLS 86 1.6 GOVERNMENT/INDUSTRY LEVEL 86 1.6.1 PUBLIC HEALTH 86 1.6.2 REMUNERATION 87 1.6.3 PROFESSIONAL STATUS 87 1.6.4 SERVICES 87 1.6.5 PHARMINTERCOM COUNTRY ANALYSIS 87 1.7 CONSUMER/STAKEHOLDER LEVEL 91 1.7.1 CONSUMERS 91 1.7.2 GP INTERACTIONS 92 1.8 CONCLUSION 93
2 RESEARCH METHODOLOGY 94 2.1 INTRODUCTION 94 2.2 NATIONAL MAIL SURVEY OF COMMUNITY PHARMACIES: THE SHAPE OF OUR FUTURE 94 2.2.1 INTRODUCTION AND OBJECTIVES 94 2.2.2 SAMPLE SELECTION 95 2.2.3 SURVEY DESIGN 96 2.2.4 SURVEY PRETESTING 97 2.2.5 PILOT SURVEY 97 2.2.6 MAIN SURVEY - DATA COLLECTION 97 2.2.7 MAIN SURVEY - DATA ANALYSIS 98 2.2.8 SURVEY LIMITATIONS 98 2.2.9 CONCLUSION 98 2.3 FOCUS GROUP METHODOLOGY 99 2.3.1 INTRODUCTION 99 2.3.2 FOCUS GROUP OBJECTIVES 99 2.3.3 METHODOLOGY 100 2.3.4 FORMAT OF THE SESSION 100 2.3.5 RECRUITMENT OF PARTICIPANTS 101 2.3.6 FOCUS GROUP LOCATIONS 101 2.3.7 FOCUS GROUP ANALYSIS PROCESS 102 2.3.8 LIMITATIONS OF THE FOCUS GROUPS RESEARCH 102 2.3.9 CONCLUSION 103 2.4 COMMUNITY PHARMACY CASE STUDIES 104 2.4.1 INTRODUCTION 104 2.4.2 METHODOLOGY 104 2.4.3 PROCESS 106 2.4.4 ANALYSIS 107 2.4.5 LIMITATIONS 108 2.4.6 CONCLUSION 108 2.5 STAKEHOLDER INTERVIEW METHODOLOGY 109 2.5.1 INTRODUCTION AND OBJECTIVES 109 2.5.2 METHODOLOGY 109
© Change Management and Community Pharmacy Project xxii

Table of Contents
2.5.3 PROCESS 109 2.5.4 LIMITATIONS 110 2.5.5 CONCLUSION 111 2.6 CONSUMER FORUM METHODOLOGY 112 2.6.1 RECRUITMENT OF PARTICIPANTS 112 2.6.2 FORMAT OF THE SESSION 113 2.6.3 CONSUMER FORUMS ANALYSIS PROCESS 114 2.6.4 LIMITATIONS OF THE CONSUMER FORUM RESEARCH 114 2.6.5 CONCLUSION 114 2.7 OVERALL METHODOLOGY CONCLUSION 115
SECTION 4: STRATEGIC OPTIONS FOR PHARMACY 1 ANALYSIS OF CURRENT AND FUTURE SERVICE OFFERINGS 119
1.1 INTRODUCTION 119 1.1.1 DEFINING “ABILITY TO DELIVER” 119 1.2 ASSESSMENT OF CURRENT SERVICE DELIVERY 120 1.2.1 ENHANCED SERVICES OFFERED BY COMMUNITY PHARMACIES 120 1.2.2 ASSESSMENT OF THIRD AGREEMENT SERVICE OFFERINGS 123 1.3 PHARMACY CHARACTERISTICS INFLUENCING THE ABILITY TO
DELIVER 130 1.3.1 COMPARISON OF SERVICES OFFERED BY PHARIA CATEGORISATION 130 1.3.2 COMPARISON OF PHARMACY NETWORKS 131 1.3.3 NUMBER OF SERVICES AND PHARMACY SIZE 133 1.3.4 NUMBER OF SERVICES AND DISPENSING VOLUME 134 1.4 PEOPLE RELATED FACTORS INFLUENCING THE ABILITY TO DELIVER 135 1.4.1 SPECIALLY TRAINED STAFF AVAILABLE TO DELIVER THE SERVICE 135 1.4.2 READINESS FOR CHANGE 136 1.4.3 MOBILISING THE CHANGE 137 1.5 SUPPORT AND ROLE OF GUILD 138 1.6 CONCLUSION 139
2 PHARMACY VIABILITY MATRIX 140
2.1 STRATEGY AND CHANGE FRAMEWORK 140 2.1.1 PPF PHARMACY MATRIX 141 2.2 PHARMACY VIABILITY MATRIX 142 2.2.1 COMMUNITY SCOPE CHARACTERISTICS 144 2.2.2 PRODUCT/SERVICE CHOICE CHARACTERISTICS 145 2.2.3 STRATEGIC FOCUS FOR EACH MODEL 145 2.3 APPLICATION OF THE PHARMACY VIABILITY MATRIX 149 2.3.1 APPLICATION OF THE PVM IN RELATION TO THE CHARACTERISING OPPORTUNITY FILTER (COF) 150 2.3.2 PVM IN THE REAL WORLD 151
3 ANALYSIS OF PHARMACY VIABILITY MATRIX (PVM) USING MAIL
SURVEY RESULTS 152 3.1 DEMOGRAPHICS BASIS OF PVM BUSINESS STRATEGIES 152 3.1.1 DEMOGRAPHIC DIFFERENCES BETWEEN PHARMACIES
© Change Management and Community Pharmacy Project xxiii

Table of Contents
USING THE PVM BUSINESS STRATEGIES 153 3.2 ATTITUDES TO CHANGE 156 3.3 PVM AND MILES AND SNOW BUSINESS STRATEGIES 158 3.4 SERVICE OFFERING 159 3.5 DIFFERENCES IN FINANCIAL PERFORMANCE BETWEEN THE STRATEGY TYPES (MEDICI CAPITAL) 162 3.5.1 OVERALL SUMMARY 164 3.6 CONCLUSION 165
4 CASE STUDY REPORTS 166
4.1 TRADITIONAL PHARMACY 166 4.2 EXPANDED PHARMACY 167 4.3 FOCUSED SPECIALTY 167 4.4 MULTI SPECIALTY 168 4.5 OTHER PHARMACY CHARACTERISTICS THAT CAN AFFECT THE
ADOPTION OF BUSINESS STRATEGIES 169 4.5.1 RURAL/REGIONAL VS. URBAN PHARMACIES 169 4.5.2 BANNER GROUP VS INDEPENDENT PHARMACIES 170 4.6 FINANCIAL ANALYSIS: CASE STUDY RESULTS FOR THE 4 BUSINESS STRATEGIES (PHARMACY VIABILITY MATRIX) 171 4.6.1 MEDICI CAPITAL CONCLUSIONS ON THE BIAS OF THE CASE STUDY SAMPLE RELATIVE TO THE MAIL SURVEY SAMPLE 173 4.7 TRANSITION WITHIN THE MATRIX 174 4.8 MEDICI CAPITAL CONCLUSIONS RELATING TO MULTI YEAR
LONGITUDINAL STUDY AND TRANSITIONAL COSTS 178 4.9 CASE STUDY NARRATIVES 179
5 INNOVATION IN PHARMACY 282
5.1 TYPES OF INNOVATION 283 5.2 CHARACTERISTICS OF INNOVATION 284 5.2.1 INCREMENTAL VS RADICAL 284 5.2.2 COMPATIBLE VS INCOMPATIBLE INNOVATION 284 5.3 STORIES OF INNOVATION 285 5.3.1 “TAILOR-MADE FOR YOU” 285 5.3.2 “THE INTEGRATED PHARMACY CLINIC” 286 5.3.3 “MULTI-SPECIALIST AGED CARE PROVIDER” 286 5.3.4 “90% LOYAL CUSTOMERS” 287 5.3.5 INNOVATIONS IN PHARMACY 288 5.3.6 OBSERVATION OF INNOVATIVE PHARMACIES 288 5.4 FINANCIAL ANALYSIS OF INNOVATION 289 5.4.1 RESULTS FOR CASE STUDIES OF INNOVATIVE PHARMACIES 289 5.5 CONCLUSION 290
SECTION 5: CLOSING THE GAP 1 PHARMIND WHEEL 293
1.1 INTRODUCTION 293 1.1.1 WHY CHANGE? 293 1.2 POLICIES, POLITICS AND PERSPECTIVES 295
© Change Management and Community Pharmacy Project xxiv

Table of Contents
1.2.1 CONSOLIDATING THE BASE: 295 1.2.2 EXPANDING FROM THE BASE 296 1.2.3 GROUPING SERVICES TO FACILITATE IMPLEMENTATION 296 1.2.4 SUPPORTING INTEGRATED HEALTH CARE DELIVERY 297 1.2.5 ENSURING ADEQUATE FUNDING FOR SERVICE PROVISION 297 1.2.6 SUPPORTING EQUITY IN ACCESS TO SERVICE PROVISION 298 1.2.7 REORGANISING FOR SERVICE PROVISION 298 1.2.8 INTEGRATING GUILD AND PSA ACTIVITIES 299 1.2.9 IDENTIFYING AND CLOSING THE CRITICAL IMPLEMENTATION GAP 299 1.2.10 DEFINING THE VALUE PROPOSITION 299 1.3 HEALTH AND ALLIED STAKEHOLDERS 300 1.3.1 THEORY – INTERORGANISATIONAL COLLABORATION 300 1.3.2 INTERVIEW ANALYSIS 301 1.3.3 PHARMACY ORGANISATIONS 303 1.3.4 PHARMACY SCHOOLS 305 1.3.5 WHOLESALERS 307 1.3.6 RETAIL COMPETITORS 309 1.3.7 CONSUMERS AND CONSUMER GROUPS 310 1.3.8 PATIENT SUPPORT ORGANISATIONS 311 1.3.9 OTHER HEALTH CARE PROFESSIONAL ORGANISATIONS 312 1.3.10 RURAL ASSOCIATIONS AND PHARMACISTS 314 1.3.11 REGULATORY AND OTHER INDUSTRY BODIES 315 1.3.12 CONCLUSION 316 1.4 ADMINISTRATIVE GOVERNANCE AND DECISION-MAKING PROCESSES 317 1.4.1 GOVERNMENTAL DELAYS AND COMPLEX PROCEDURES 318 1.4.2 THE IMPORTANCE OF PHARMACY NETWORKS 319 1.4.3 ENCOURAGE IMPROVED EFFICIENCIES IN SERVICE DELIVERY 320 1.5 RESOURCING AND REVENUE FLOW 321 1.5.1 CREATING AN ADEQUATE REVENUE FLOW TO FINANCE SERVICE
PROVISION 321 1.5.2 ENSURE THE SUPPLY OF QUALIFIED PERSONNEL TO SUPPORT
EXTENDED SERVICE PROVISION 322 1.5.3 WORK WITH SUPPLIERS TO DEVELOP THE INFRASTRUCTURE TO
FACILITATE SERVICE DELIVERY 324 1.5.4 COORDINATE WITH OTHER STAKEHOLDERS 325 1.5.5 BUILD CHANGE MANAGEMENT CAPABILITIES 326 1.6 MARKETING AND SELLING TO STAKEHOLDERS AND CONSUMERS 327 1.6.1 STRATEGIC MARKETING ARGUMENTS: 327 1.7 INDUSTRY RE-STRUCTURING 332 1.7.1 GREATER USE OF SUPPORT STAFF 332 1.7.2 NEW CONTRACTUAL ARRANGEMENTS 333 1.7.3 DEVELOPMENT OF FAMILY FRIENDLY WORKPLACES 333 1.7.4 GREATER LOCAL CO-ORDINATION IN SERVICE PROVISION 333 1.7.5 RESPONDING TO PRESSURE FOR EQUITY OF ACCESS TO SERVICES, PARTICULARLY IN RURAL AND REMOTE AREAS 334 1.7.6 CREATING OPERATING EFFICIENCIES BY DOING THINGS DIFFERENTLY 334 1.7.7 ADDRESSING PROBLEMS OF OWNERSHIP AND NUMBERS OF
PHARMACIES 335 1.7.8 RELATIONSHIP OF WHOLESALERS AND BANNER GROUPS TO PHARMACY 336
© Change Management and Community Pharmacy Project xxv

Table of Contents
1.8 NON-PHARMACY THREATS AND OPPORTUNITIES 337 1.8.1 GROUPING OF PHARMACY SERVICES AND THEIR COORDINATION IN GEOGRAPHIC AREAS – A NEW
OPPORTUNITY, AND A POTENTIAL ACCC THREAT 338 1.8.2 THE RELATIONSHIP WITH GPS 338 1.9 DELIVERING AND ACCELERATING CHANGE 339 1.9.1 DEVELOPING A VISION FOR THE INDUSTRY 340
2 PHARMACY CHANGE READINESS WHEEL 343
2.1 INTRODUCTION 343 2.2 PROFITABILITY PERSPECTIVE 344 2.2.1 PROFITABILITY PERSPECTIVE 1: PROFITABILITY NEEDS TO BE THERE AT THE START – OR SHORTLY THEREAFTER 345 2.2.2 PROFITABILITY PERSPECTIVE 2: PROFITABILITY WILL COME LATER – FOR A VARIETY OF REASONS. 347 2.2.3 PROFITABILITY PERSPECTIVE 3: PROFITABILITY WILL NOT COME LATER – WE SUBSIDISE 349 2.2.4 BRINGING THE “PROFITABILITY PERSPECTIVES” TOGETHER 349 2.3 HISTORY OF PAST CHANGES 350 2.3.1 POSITIVE EXPERIENCES OF PAST CHANGES 350 2.3.2 NEGATIVE EXPERIENCES OF PAST CHANGES 351 2.3.3 EFFECT OF PAST CHANGES 352 2.4 ASSESSMENT OF THE NEED FOR CHANGE 354 2.4.1 PRESSURE TO INTRODUCE THE CHANGE (REACTIVE) 354 2.4.2 ASSESSMENT OF NEW MARKET OPPORTUNITIES (PROACTIVE). “PUSHING THE ENVELOPE” 357 2.4.3 FIT WITH BUSINESS MODEL 357 2.4.4 PERSONAL REWARDS 358 2.5 RESOURCE AVAILABILITY 360 2.5.1 SPACE 360 2.5.2 STAFF 361 2.5.3 “REPUTATIONAL CAPITAL” - EXTERNAL ALLIANCES AND RELATIONSHIPS 362 2.5.4 “WORKING CAPITAL” 363 2.6 MEASUREMENTS AND METRICS 364 2.6.1 CHOOSING MEASURES 364 2.6.2 USING THE MEASURES TO EVALUATE CHANGE SUCCESS 365 2.7 ASSESSING RISK 366 2.7.1 REPUTATION 367 2.7.2 COORDINATION 367 2.7.3 NEW LIABILITIES 368 2.7.4 INADEQUATE RETURNS 368 2.8 CHANGE ORIENTATION 369 2.8.1 YOUR GENERATION 370 2.8.2 YOUR PROFESSIONAL IDENTITY: HEALTH CARE PROVIDER VS RETAILER AND BUSINESS MANAGER 372 2.9 INFORMATION AND KNOWLEDGE AVAILABILITY 374 2.9.1 WORKABLE KNOWLEDGE 375 2.9.2 STRATEGIES FOR OBTAINING WORKABLE KNOWLEDGE 377 2.10 SKILLS AUDIT 379 2.10.1 SKILL AREAS 380 2.11 TIME AVAILABILITY AND TIMING ANALYSIS 383 2.11.1 TIME TO EVALUATE THE NEED FOR THE CHANGE 383
© Change Management and Community Pharmacy Project xxvi

Table of Contents
2.11.2 TIME TO PREPARE FOR IT 383 2.11.3 TIME TO IMPLEMENT IT 384 2.11.4 TIME VERSUS QUALITY OF LIFE 385 2.11.5 TIMING OF THE PROPOSED CHANGE 385 2.11.6 PLATE TOO FULL 385 2.11.7 CHANGE WEARY 386 2.11.8 STRATEGIES FOR FREEING UP TIME 386 2.12 PHARMACY CHANGE READINESS ASSESSMENT 388 2.12.1 QUESTIONS 388 2.13 CONCLUSION 390
3 PHARMACY CHANGE IMPLEMENTATION WHEEL 391
3.1 INTRODUCTION 391 3.2 PLANNING THE CHANGE 392 3.2.1 THE IMPORTANCE OF PLANNING 392 3.2.2 WHAT DOES CHANGE PLANNING CONSIST OF? 394 3.2.3 WHAT CHANGE PLANNING DOES NOT CONSIST OF 394 3.2.4 RELATE THE PLAN TO THE BUSINESS STRATEGY 394 3.2.5 CHOOSE THE PLANNING HORIZON 395 3.2.6 DEFINE THE SCOPE OF THE CHANGE 396 3.2.7 CREATE PLANS FOR THE OTHER ELEMENTS OF THE WHEEL 396 3.2.8 PROGRESSIVELY MONITOR OUTCOMES 396 3.2.9 DO THE FINANCIALS 397 3.3 HELPING AND ASSISTING THE CHANGE 398 3.3.1 START WHERE THERE ARE EXISTING RESOURCES 398 3.3.2 CONSIDER YOUR LEVEL OF EXPERIENCE IN IMPLEMENTING CHANGE 399 3.3.3 USE THE RESOURCES OF YOUR BANNER GROUP OR NETWORK 399 3.3.4 ENSURE YOU HAVE QUALITY STAFF 400 3.3.5 CREATE A LEARNING ORGANISATION AND REWARD INNOVATION 401 3.3.6 CARE FOR YOURSELF 401 3.4 ALLOCATING THE RESOURCES FOR CHANGE 402 3.4.1 CAPITAL/FINANCE 402 3.4.2 ORGANISATIONAL DESIGN 403 3.4.3 TECHNOLOGY, EQUIPMENT AND SYSTEMS 404 3.4.4 EQUIPMENT 405 3.4.5 SYSTEMS 405 3.4.6 WORKFORCE 406 3.5 RESPONDING TO AND MANAGING RESISTANCE TO CHANGE 408 3.5.1 RESISTANCE FROM EXTERNAL STAKEHOLDERS 408 3.5.2 RESISTANCE FROM INTERNAL STAKEHOLDERS 412 3.6 MARKETING THE CHANGE 414 3.6.1 WHY IS MARKETING IMPORTANT? 414 3.6.2 IDENTIFY AND STUDY YOUR MARKET SEGMENT FOR THE NEW SERVICE 414 3.6.3 IF NECESSARY, GET SPECIALIST ADVICE AND BACK UP 416 3.6.4 CLARIFY YOUR MESSAGE 416 3.6.5 SELECT MARKETING CHANNELS YOUR TARGET MARKET PAY ATTENTION TO 416 3.6.6 USE MULTIPLE MUTUALLY REINFORCING RELEVANT CHANNELS WHERE APPROPRIATE 418 3.6.7 DEVELOP YOUR CAMPAIGN AND PLAN FOR ONGOING
© Change Management and Community Pharmacy Project xxvii

Table of Contents
REINFORCEMENT 418 3.6.8 MAKE SURE THAT YOU CAN DELIVER ON YOUR VALUE PROPOSITION 419 3.7 ALIGNING THE CHANGE 420 3.7.1 WHAT IS ALIGNMENT? 420 3.7.2 IDENTIFY AND ELIMINATE ORGANISATIONAL DISJUNCTIONS 420 3.7.3 WORK TOWARD INCREASING CONSISTENCY IN ALL ASPECTS OF THE
LIFE OF THE PHARMACY 421 3.7.4 ENSURE YOU HAVE CREATED CULTURAL ALIGNMENT 422 3.8 COMMUNICATING THE VISION AND THE CHANGE 423 3.8.1 WHAT IS A VISION? 423 3.8.2 DEVELOP A VISION FOR YOUR PHARMACY 424 3.8.3 COMMUNICATE THE VISION TO YOUR STAFF 425 3.8.4 COMMUNICATE THE VISION TO YOUR CUSTOMERS 426 3.8.5 COMMUNICATE THE VISION TO OTHER STAKEHOLDERS 426 3.8.6 SHARE IN THE WIDER VISION OF AN INTEGRATED PRIMARY HEALTH CARE SYSTEM 427 3.9 INTEGRATING AND CONSOLIDATING THE CHANGE 429 3.9.1 INTEGRATE YOUR CHANGE PROGRAM EXTERNALLY 429 3.9.2 INTEGRATE AND COORDINATE WITHIN THE NETWORK AND PHARMACY 430 3.9.3 DEVELOP A “CLEAR LINE OF SIGHT” 431 3.9.4 BUILD A SERVICE CULTURE 431 3.10 SITUATING AND LEADING THE CHANGE 432 3.10.1 SITUATE AND LEAD THE CHANGE INTERNALLY 433 3.10.2 TEAMWORK BEGINS AT THE TOP 434 3.10.3 SITUATE AND LEAD THE CHANGE EXTERNALLY 435 3.11 TRIGGERING THE MOTIVATION TO CHANGE 437 3.11.1 WHY CHANGE? 437 3.11.2 PROFESSIONAL DEVELOPMENT OPPORTUNITIES 438 3.11.3 KEEPING UP AND GAINING COMPETITIVE ADVANTAGE 439 3.11.4 DEMOTIVATORS 440 3.11.5 SUMMARY 440 3.12 FURTHER READING 441
4 PRACTICAL APPLICATIONS 442
4.1 A PHARMACY CHANGE MANAGEMENT PROGRAM — DELIVERING
ASTHMA MANAGEMENT SERVICES 442 4.1.1 PHASE 1: IDENTIFYING PHARMACY-LEVEL, FUTURE OPPORTUNITIES FOR
THE DELIVERY OF ASTHMA SERVICES 443 4.2 PHASE 2: PREPARING FOR INDUSTRY LEVEL CHANGE: PHARMIND CHANGE WHEEL 446 4.2.1 PHARMIND WHEEL: POLICIES, POLICIES AND PERSPECTIVES 446 4.2.2 PHARMIND WHEEL: HEALTH AND ALLIED STAKEHOLDERS 447 4.2.3 ADMINISTRATIVE GOVERNANCE AND DECISION-MAKING PROCESSES 448 4.2.4 PHARMIND WHEEL: RESOURCING AND REVENUE FLOWS 448 4.2.5 PHARMIND WHEEL: MARKETING AND SELLING TO STAKEHOLDERS AND
CONSUMERS 449 4.2.6 PHARMIND WHEEL: INDUSTRY RE-STRUCTURING 449 4.2.7 PHARMIND WHEEL: NON-PHARMACY THREATS AND OPPORTUNITIES 450
© Change Management and Community Pharmacy Project xxviii

Table of Contents
4.2.8 PHARMIND WHEEL: DELIVERING AND ACCELERATING INDUSTRY CHANGE 450
4.3 PHASE 3: IDENTIFYING THE FIT BETWEEN OPPORTUNITIES AND INDIVIDUAL PHARMACY BUSINESS STRATEGIES: THE PHARMACY VIABILITY MATRIX 452
4.4 PHASE 4: IDENTIFYING INDIVIDUAL PHARMACY READINESS FOR THE CHANGE: CHANGE READINESS WHEEL 453 4.4.1 CHANGE READINESS WHEEL: PROFITABILITY PERSPECTIVE 453 4.4.2 CHANGE READINESS WHEEL: HISTORY OF PAST CHANGES 453 4.4.3 CHANGE READINESS WHEEL: ASSESSMENT OF NEED FOR CHANGE 454 4.4.4 CHANGE READINESS WHEEL: RESOURCE AVAILABILITY 455 4.4.5 CHANGE READINESS WHEEL: MEASUREMENTS AND METRICS 455 4.4.6 CHANGE READINESS WHEEL: ASSESSING RISK 456 4.4.7 CHANGE READINESS WHEEL: CHANGE ORIENTATION 456 4.4.8 CHANGE READINESS WHEEL: INFORMATION AND KNOWLEDGE
AVAILABILITY 457 4.4.9 CHANGE READINESS WHEEL: SKILLS AUDIT 457 4.4.10 CHANGE READINESS WHEEL: TIME AVAILABILITY AND TIMING ANALYSIS 458 4.4.11 CHANGE READINESS WHEEL: OVERALL EVALUATION OF YOUR
PHARMACY’S READINESS FOR CHANGE 458 4.5 PHASE 5: IMPLEMENTING THE CHANGE WITHIN THE PHARMACY: CHANGE IMPLEMENTATION WHEEL 459 4.5.1 CHANGE IMPLEMENTATION WHEEL: PLANNING THE CHANGE 459 4.5.2 CHANGE IMPLEMENTATION WHEEL: HELPING AND ASSISTING THE CHANGE 460 4.5.3 CHANGE IMPLEMENTATION WHEEL: ALLOCATING RESOURCES FOR THE CHANGE 461 4.5.4 CHANGE IMPLEMENTATION WHEEL: RESPONDING TO AND MANAGING RESISTANCE TO THE CHANGE 461 4.5.5 CHANGE IMPLEMENTATION WHEEL: MARKETING THE CHANGE 462 4.5.6 CHANGE IMPLEMENTATION WHEEL: ALIGNING THE CHANGE 462 4.5.7 CHANGE IMPLEMENTATION WHEEL: COMMUNICATING THE VISION AND THE CHANGE 463 4.5.8 CHANGE IMPLEMENTATION WHEEL: INTEGRATING AND
CONSOLIDATING THE CHANGE 463 4.5.9 CHANGE IMPLEMENTATION WHEEL: SITUATING AND LEADING THE CHANGE 464 4.5.10 CHANGE IMPLEMENTATION WHEEL: TRIGGERING THE MOTIVATION TO CHANGE 464 4.6 PHASE 6: BUSINESS CASE FOR A DIABETES DSM SERVICE 466 4.6.1 INTRODUCTION 466 4.6.2 OBJECTIVE 466 4.6.3 DEFINITION OF COST 466 4.6.4 COST ANALYSIS 467 4.6.5 THE DIABETES DSM BUSINESS CASE 470
5 CLOSING THE GAP: CONCLUSION 473
© Change Management and Community Pharmacy Project xxix

Table of Contents
SECTION 6: CONCLUSION 1 CONCLUSION 475
REFERENCE LIST 1 REFERENCE LIST 479
APPENDICES 1 FUTURE CERTAINTIES IN HEALTH: LITERATURE SUMMARIES 495 2 SURVEY MATERIAL 530 3 DETAILED MAIL SURVEY RESULTS 531 4 FOCUS GROUP MATERIAL 605 5 FOCUS GROUP REPORT 611 6 CASE STUDY MATERIAL 621 7 STAKEHOLDER INTERVIEW MATERIAL 632 8 CONSUMER FORUM MATERIAL 635 9 CONSUMER FORUM RESULTS 643 10 DIABETES BUSINESS CASE 648 11 UTS ETHICS APPROVAL 663
© Change Management and Community Pharmacy Project xxx

Table of Contents
LIST OF FIGURES
SECTION 2: FUTURE CERTAINTIES IN HEALTH FIGURE 2.1 AGE DISTRIBUTION OF EMPLOYED PHARMACISTS IN SAMPLE
POPULATION, 2001 43 FIGURE 2.2: TYPES OF COMMUNITY PHARMACIES IN CANADA, 1994 AND 2002 48 FIGURE 2.3: OPPORTUNITIES FOR COMMUNITY PHARMACY 50 FIGURE 2.4: DELIVERY OPTIONS FOR NEW SERVICES 53
SECTION 3: EXPLORING THE PHARMACISTS’ WORLD FIGURE 3.1: FOCUS GROUP LOCATION MAP 102
SECTION 4: STRATEGIC OPTIONS FOR PHARMACY FIGURE 4.1: SERVICES OFFERED BY PHARMACIES 122 FIGURE 4.2: NUMBER OF HMRS CONDUCTED PER REGISTERED PHARMACY PER
MONTH 124 FIGURE 4.3: NUMBER OF PHARMACIES CURRENTLY OFFERING AND THOSE
PLANNING TO ADOPT THIRD AGREEMENT SERVICES 125 FIGURE 4.4: SATISFACTION WITH SERVICE, PROFITABILITY AND TAKE-UP BY
CUSTOMERS FOR THIRD AGREEMENT SERVICES 126 FIGURE 4.5: RESPONSE RATES FOR THOSE CURRENTLY OFFERING AND THOSE
PLANNING TO ADOPT SELECTED SERVICES 127 FIGURE 4.6: RESPONSES TO SERVICE, PROFITABILITY AND CUSTOMER TAKE-UP OF POSSIBLE FUTURE AGREEMENT SERVICES 129 FIGURE 4.7: SERVICE OFFERING AS CATEGORISED BY PHARIA 131 FIGURE 4.8: RESPONSES FOR NETWORK INFLUENCE (N=222) 132 FIGURE 4.9: SERVICE OFFERING COMPARED AGAINST NETWORK OR NON-NETWORK PHARMACIES 132 FIGURE 4.10: SERVICE OFFERING BY PHARMACY SIZE 133 FIGURE 4.11: SERVICE OFFERING COMPARED AGAINST DISPENSING VOLUME 134 FIGURE 4.12: SUMMARY OF SURVEY RESPONSES REGARDING IMPORTANCE OF
FACTORS INFLUENCING DECISION TO IMPLEMENT A NEW SERVICE 138 FIGURE 4.13: PPF PHARMACY MATRIX 141 FIGURE 4.14: PHARMACY VIABILITY MATRIX 143 FIGURE 4.15: TRADITIONAL PHARMACY 145 FIGURE 4.16: EXPANDED PHARMACY 146 FIGURE 4.17: FOCUSED SPECIALTY 147 FIGURE 4.18: MULTI SPECIALTY 148 FIGURE 4.19: PVM DISTRIBUTION BY LOCATION 153 FIGURE 4.20: PVM DISTRIBUTION BY ANNUAL DISPENSING VOLUME 154 FIGURE 4.21: PVM DISTRIBUTION BY NETWORK 154 FIGURE 4.22: PVM DISTRIBUTION BY SIZE OF PHARMACY 155 FIGURE 4.23: PVM DISTRIBUTION BY TRADING HOURS 155 FIGURE 4.24: PVM DISTRIBUTION BY MILES AND SNOW BUSINESS STRATEGY 158 FIGURE 4.25: SERVICES OFFERED BY PVM CATEGORY 161 FIGURE 4.26: ANALYSIS OF VARIABLES FOR THE PVM MODELS 173
© Change Management and Community Pharmacy Project xxxi

Table of Contents
FIGURE 4.27: EQUAL PRODUCT/SERVICE MIX 174 FIGURE 4.28: TRADITIONAL PHARMACY INCREASING SERVICE PROVISION 174 FIGURE 4.29: TRADITIONAL PHARMACY INCREASING SERVICE PROVISION AND
MOVING TO FOCUSED SPECIALTY 175 FIGURE 4.30: TRADITIONAL PHARMACY INCREASING SERVICE PROVISION AND
MOVING TO MULTI SPECIALTY 175 FIGURE 4.31: TRADITIONAL PHARMACY INCREASING SERVICE PROVISION AND
MOVING TO EXPANDED PHARMACY 176 FIGURE 4.32: TRADITIONAL PHARMACY INCREASING PRODUCT PROVISION 176 FIGURE 4.33: TRADITIONAL PHARMACY INCREASING PRODUCT PROVISION AND
MOVING TO FOCUSED SPECIALTY 177 FIGURE 4.34: TRADITIONAL PHARMACY INCREASING PRODUCT PROVISION AND
MOVING TO MULTI SPECIALTY 177 FIGURE 4.35: TRADITIONAL PHARMACY INCREASING PRODUCT PROVISION AND
MOVING TO EXPANDED PHARMACY 178 FIGURE 4.36: PRODUCT VS BUSINESS MODEL INNOVATION CHART 283 FIGURE 4.37: TYPOLOGY OF INNOVATION 285
SECTION 5: CLOSING THE GAP FIGURE 5.1: PHARMIND WHEEL 294 FIGURE 5.2: PHARMACY CHANGE READINESS WHEEL 344 FIGURE 5.3: TOP 10 SERVICES RANKED BY PHARMACIST SATISFACTION IN TERMS OF THE SERVICE THEY OFFER 351 FIGURE 5.4: USEFULNESS OF VARIOUS SOURCES OF INFORMATION AS RANKED BY THE SURVEY 376 FIGURE 5.5: CHANGE IMPLEMENTATION WHEEL 391 FIGURE 5.6: FACILITATORS OF CHANGE 407 FIGURE 5.7: CHARACTERISING OPPORTUNITIES FILTER 443 FIGURE 5.8: PHARMACY VIABILITY MATRIX 452
© Change Management and Community Pharmacy Project xxxii

Table of Contents
LIST OF TABLES
SECTION 1: INTRODUCTION TABLE 1.1: DESIRED VS. ACTUAL PROJECT OUTCOMES 8
SECTION 2: FUTURE CERTAINTIES IN HEALTH TABLE 2.1 ESTIMATED CURRENT AND PROJECTED * MEDIAN AGE (YEARS) FOR
AUSTRALIA 20 TABLE 2.2 PROPORTION OF THE POPULATION IN EACH AGE GROUP 20 TABLE 2.3 POPULATION PROJECTIONS FOR CAPITAL CITIES AND THE ACT, SERIES B 21 TABLE 2.4 STATISTICAL LOCAL AREAS (NSW) WITH THE HIGHEST PROJECTED
GROWTH RATES FOR PEOPLE AGED 65 PLUS (1999-2019) 21 TABLE 2.5 LEADING CAUSES OF BURDEN OF DISEASE AND INJURY, AUSTRALIA,
1996 22 TABLE 2.6 LEADING CAUSES OF DISEASE AND INJURY IN AUSTRALIA, BY GENDER, 1996 23 TABLE 2.7 TOTAL HEALTH AND WELFARE SERVICES EXPENDITURE AS A
PROPORTION OF GDP, 1996-97 TO 2000-01 38 TABLE 2.8 CHARACTERISING OPPORTUNITIES FILTER: SEVEN DIMENSIONS 51 TABLE 2.9: POSITION OF PERSON CONDUCTING HMRS 54
SECTION 3: EXPLORING THE PHARMACISTS’ WORLD TABLE 3.1: RESEARCH METHODOLOGY OUTLINE 94 TABLE 3.2: RANDOMISED SPLIT OF DATABASE 95 TABLE 3.3: CONSUMER FORUM SUMMARY 114 TABLE 3.4: SUMMARY OF EMPIRICAL RESEARCH METHODOLOGIES 115
SECTION 4: STRATEGIC OPTIONS FOR PHARMACY TABLE 4.1: ENHANCED SERVICES OFFERED BY PHARMACIES 121 TABLE 4.2: NUMBER OF PHARMACIES OFFERING/PLANNING TO OFFER THIRD
AGREEMENT SERVICES 123 TABLE 4.3: FACTORS INFLUENCING DELIVERY OF CURRENT THIRD AGREEMENT
SERVICES OFFERED 125 TABLE 4.4: RESPONSE RATES FOR POSSIBLE FOURTH AGREEMENT SERVICES 127 TABLE 4.5: FACTORS INFLUENCING DELIVERY OF POSSIBLE CANDIDATES FOR
FOURTH AGREEMENT SERVICES 128 TABLE 4.6: RESPONSES BY PHARIA 130 TABLE 4.7: NUMBER OF RESPONDENTS OFFERING SERVICES AS GROUPED BY
PHARIA 131 TABLE 4.8: SURVEY RESPONSES BY NON-NETWORK AND NETWORK 133 TABLE 4.9: RESPONSES BY PHARMACY SIZE 134 TABLE 4.10: SURVEY RESPONSES BY DISPENSING VOLUME 134 TABLE 4.11: RELATIONSHIP BETWEEN SERVICE TAKE-UP BY CONSUMERS AND
HAVING A SPECIALLY TRAINED PERSON FOR THIRD AGREEMENT PROGRAMS AND POTENTIAL CANDIDATES FOR FOURTH AGREEMENT. 135
© Change Management and Community Pharmacy Project xxxiii

Table of Contents
TABLE 4.12: RESPONSES TO MILES AND SNOW STRATEGY QUESTIONS 137 TABLE 4.13: BREAKDOWN OF PHARMACIES RESPONDING FOR PVM 152 TABLE 4.14: ANALYSIS OF CHANGE QUESTIONS 157 TABLE 4.15: SERVICE OFFERING BY PVM CATEGORY 160 TABLE 4.16: PHARMACY VIABILITY MATRIX CATEGORISED RESULTS 162 TABLE 4.17: FINANCIAL RESULTS AND BUSINESS MEASURES BY CATEGORY 163 TABLE 4.18: CASE STUDY CLASSIFICATIONS 166 TABLE 4.19: RURAL/REGIONAL VS. URBAN PHARMACIES FROM CASE STUDIES 169 TABLE 4.20: BANNER GROUP VS. INDEPENDENT PHARMACIES FROM CASE STUDIES 170 TABLE 4.21: PHARMACY VIABILITY MATRIX CATEGORISED RESULTS 171 TABLE 4.22: FINANCIAL RESULTS AND BUSINESS MEASURES BY CATEGORY 172 TABLE 4.23: INNOVATIVE PHARMACIES 289
SECTION 5: CLOSING THE GAP TABLE 5.1: STAKEHOLDER INTERVIEW SUMMARY 302 TABLE 5.2: SERVICE ADOPTION ANALYSIS 345 TABLE 5.3: SERVICES DISCONTINUED BY FOCUS GROUP PHARMACISTS 352 TABLE 5.4: SERVICES PHARMACISTS ARE PLANNING TO ADOPT – FROM MAIL
SURVEY 353 TABLE 5.5: SERVICES RATED BY DIFFICULTY TO IMPLEMENT AND IMPACT ON
PROFITABILITY FROM FOCUS GROUPS 399 TABLE 5.6: DIABETES DSM BUSINESS CASE 472
© Change Management and Community Pharmacy Project xxxiv

Abbreviations
Abbreviations AACP Australian Association of Consultant Pharmacy ACT Australia Capital Territory ADR Adverse Drug Reaction AHS Aboriginal Health Services ANOVA Analysis of Variance APAC Australian Pharmaceutical Advisory Council BGL Blood Glucose Level BP Blood Pressure CEO Chief Executive Officer CI Confidence Interval CMI Consumer Medical Information COPD Chronic Obstructive Pulmonary Disease COPRA Council of Pharmacy Registering Authorities (replaces
APRA) CPE Continuing Professional Education CPS Cognitive Pharmaceutical Services CQI Continuous Quality Improvement DAA Dose Administration Aids DMMR Domiciliary Medication Management Review FTE Full-time Equivalent GP General Practitioner GP Gross Profit HMR Home Medicine Review HIC Health Insurance Commission KPI Key Performance Indicator MBF Medical Benefits Fund MIC Medicines Information to Consumers NSW New South Wales NT Northern Territory PhARIA Pharmacy Access Remoteness Index of Australia PBS Pharmaceutical Benefits Scheme PGA Pharmaceutical Guild of Australia PSA Pharmaceutical Society of Australia QCPP Quality Care Pharmacy Program Qld Queensland QUM Quality Use of Medicines RMMR Residential Medication Management Review SA South Australia
© Change Management and Community Pharmacy Project xxxv

Abbreviations
Tas Tasmania Vic Victoria WA Western Australia “The Third Agreement” Community Pharmacy Agreement (between the Pharmacy
Guild of Australia and the Australian Government) “The Guild” Pharmacy Guild of Australia “The Society” Pharmaceutical Society of Australia Operational definition: Cognitive Pharmacy Services (CPS): “the use of specialized knowledge by the pharmacist for the patient or health care professionals for the purpose of promoting effective and safe drug therapy” (Cipolle et al. 1998, p.269)
© Change Management and Community Pharmacy Project xxxvi

SECTION 2: FUTURE CERTAINTIES IN HEALTHExamination of social trends to identify future opportunities for the provision of cognitive services through community pharmaciesIntroduction of Characterising Opportunities Filter
SECTION 3: EXPLORING THE PHARMACISTS’ WORLDTargeted literature review of change management in community pharmacyResearch methodology: mail survey, focus groups, case studies, consumer forums, stakeholder interviews
SECTION 5: CLOSING THE GAPIntegrates research results from all sources to show how gap can be closed between current service delivery and desired future service deliveryIntroduction of Pharmind Wheel: implementing change in context of the health and pharmacy industryIntroduction of Pharmacy Change Readiness Wheel: a practical tool for pharmacists to use to check whether their pharmacy is ready to introduce a change in service provisionIntroduction of Pharmacy Implementation Wheel: a tool to help pharmacists design and implement change for their pharmacyPractical application of the five introduced tools
SECTION 1: INTRODUCTIONResearch ObjectivesActual vs Desired Outcomes
SECTION 4: STRATEGIC OPTIONS FOR PHARMACY
Assessment of current cognitive services offeredIntroduction of Pharmacy Viability Matrix (PVM)Analysis of PVM from mail survey resultsPresentation of 24 pharmacy case studiesInnovation in Community Pharmacy

Section 1 – Introduction 1. Introduction
Introduction to the study: why is change management so important for the implementation of services in pharmacy?
Desired and actual project outcomes

Section 1: Introduction
Section 1: Chapter 1
1 Introduction: Why is Change Management so Important for the Implementation of Services in Pharmacy?
The pace of change in modern societies can be overwhelming for many organisations and poses massive problems of adjustment at the industry level. One of the main drivers is technological change – technological innovations like keyhole surgery can transform a profession by, for example, changing the specialist skills surgeons need to operate; changes in information technology such as the Internet can transform delivery systems, making it possible, for example, for consumers to bypass national boundaries and buy their pharmaceutical supplies in a global market. In the economic sphere too deregulation of markets can quickly revolutionise an industry, creating very different requirements for business success. Political developments such as the current US/Australia Free Trade Agreement can also impact on industries and on individual businesses. In a global world, change is accelerated and often takes the form of radical discontinuities rather than slow evolutionary growth or decline (Drucker 1980; Strebel 1992; Stace and Dunphy 2001; Palmer, Dunford and Akin 2005). In such volatile conditions there is often no time for slow adaptation at the organisational level – the price of survival is proactivity – the active pursuit of change based on anticipation of future trends – and agility – the ability to move an organisation quickly and flexibly to reposition it in emerging markets. The major buffer that can provide some guarantee of sustainability in a world of declining certainties and emerging opportunities is to build a capability for managing change. Governments can change policies, for example in health care, but the policies are simply pieces of paper unless there is a plan and program for their implementation and the will and skill to turn the policies into changed behaviour. Similarly at the organisational level, boards of management and executive teams can develop business strategies for survival and growth but these are simply files in the CEO’s computer unless there are change programs that translate the strategies into action on a day to day basis. There is an enormous gap between the development of policies or strategies and their embodiment in the minds and hearts of the people who must put them into effect. This report deals with filling that gap. The report is specifically addressed to the issue of assisting pharmacies move from being primarily product-focused to providing a product /service mix where ‘cognitive’ services are a larger element of the offering and where retail products are more closely related to the pharmacy’s service offerings. This represents a shift in the mindset of many pharmacists. Fortunately, as we shall document from our own and others’ research, this attitudinal shift is well underway. The majority of pharmacists surveyed (87.4%) report that they want to move their operations in this direction and the Guild has led the way in this. However wanting to move in this direction is a world away from actually doing it. There is also opposition from within the ranks of pharmacists – 40% reported that there is currently too much change imposed on community pharmacy. Again, fortunately, there are pharmacists who are actively innovating in introducing the change to greater cognitive or professional service offerings. We document innovative change in a number of case studies of
© Change Management and Community Pharmacy Project 3

Section 1: Introduction
innovative pharmacies. We also provide evidence of the rise of a number of different strategic approaches to developing more service offerings. These newer strategic approaches represent pathways to a different and more viable future for pharmacy. Section 1 of the report ‘Introduction’ presents the objectives of the research project and outlines the actual versus desired outcomes – a Tender requirement. Section 2 ‘Future Certainties in Health’ presents the results of a future search undertaken to examine societal trends and to identify future opportunities for the provision of cognitive services through community pharmacies. The report then goes on to examine these opportunities and to discuss how those that are more promising can be selected for further development. In section 2, we introduce the first of five intellectual tools, each of which represents a systematic approach to helping the profession and pharmacists in particular make viable strategic choices about the introduction of future service offerings. This is the ‘Characterising Opportunities Filter’ (COF). This first tool enables a systematic analysis to be made of specific service offerings across seven dimensions. The Characterising Opportunities Filter is designed to map different potential approaches to offering a service. Using a systematic approach such as this means that a pharmacist interested in offering a new service does not have to offer it in a standard way or simply copy what other pharmacists have done. There are more available choices about service delivery than many pharmacists would otherwise realise and this provides for the possibility of differentiation in service offerings – for example, in specialising in prevention rather than palliation (place in the spectrum of health care) or delivery to the patient rather than delivery through the pharmacy (service setting). The Characterising Opportunities Filter can also be used by the Guild in selecting high priority services to be incorporated into negotiations for support with the government or with other potential providers such as health funds. Similarly it can be used to develop non-subsidised service offerings in collaboration with pharmacies and pharmacy networks. In this latter case, we suggest that these services will need to be consumer funded. Section 3 ‘Exploring the Pharmacists’ World’ outlines the research methodologies used throughout this research study to understand how pharmacists view cognitive service provision and change management issues now and what they see as important issues to deal with in the future. Our methodologies include: literature reviews in a number of areas, focus groups with pharmacists, a survey of over 2,000 pharmacies with 575 responses, 24 case studies of individual pharmacies, interviews with representatives of 51 stakeholders and seven consumer forums. This section does not present the results of these methodologies as the results are incorporated into later sections of the report. We then move on in Section 4 ‘Strategic Options for Pharmacy’ to review our results, placing them in the context of strategic options or choices for pharmacists and for the industry as a whole. We use our data sources, particularly the mail survey, to examine which services have been taken up by pharmacists and their future intentions for further service adoption. It is in this section that we introduce our second tool – the Pharmacy Viability Matrix (PVM). This matrix outlines four fundamental strategic choices for pharmacy and also produces empirical evidence to show that these approaches are distinctively different. One of these choices is the Traditional Pharmacy. We think that there will be an important place for the Traditional Pharmacy for years to come, particularly in rural areas. However
© Change Management and Community Pharmacy Project 4

Section 1: Introduction
this strategic choice is already under increasing threat for reasons we outline later in the report. We produce empirical evidence to show that there are three emerging new strategic options for pharmacies in the areas of both health related and non-health related product and services:
The Expanded Pharmacy which operates locally, as does a Traditional Pharmacy, but broadens the range of product and service offerings
The Focused Specialty pharmacy which concentrates on adding a single specialised service offering, such as diabetes management, to a niche market located in an extended community or catchment area.
The Multi Specialty pharmacy which operates across an extended community base or catchment area and expands its product and service offerings.
These are all departures from the Traditional Pharmacy which provide new opportunities for increased service delivery while continuing to retail health related products. However pharmacies in all strategic business models still maintain as part of their strategy a common base core product and service offering which is currently largely defined by the current agreements between the Guild and the Australian Government. We found no examples of pharmacies which were “service only”, i.e. selling no products and we see no evidence in the Australian study of pharmacies moving in this direction. All pharmacies in the study offered products and services but the product to service mix varied substantially across pharmacies. This study therefore is examining strategies for increasing the service component of the product to service mix and the potential impact of such an increase on the viability of the industry and of individual pharmacies or pharmacy networks. We present evidence for the existence of substantial numbers of pharmacies moving in each of these new strategic directions, describe how these strategic choices differ and the differing change management issues involved. We also examine the financial implications of all four approaches (Traditional Pharmacy, Expanded Pharmacy, Focused Specialty and Multi Specialty), examining how strategic choice affects a variety of financial indicators. Case studies are used to provide illustrative examples of each strategy. These case studies are designed to be used as training tools in courses covering cognitive service delivery and as models for consideration by other pharmacy owners. The case studies also include analyses indicating how the strategic choices made affect the financial results of each pharmacy. Out of the 24 case studies eight pharmacies were selected to illustrate innovation in pharmacy. We discover a number of different approaches to innovation in these cases and show how it is possible to innovate with positive financial outcomes. Section 5 ‘Closing the Gap’ brings together our research results from all sources to show how the gap can be closed between developing policies for service delivery and implementing them so that they are sustainable in the longer term. It is here that we introduce the last three intellectual tools designed to assist in the effective implementation of change. The first tool is the PharmInd Wheel which concentrates on the implementation of change in the context of the health industry and in particular the pharmacy industry. PharmInd is an acronym for Pharmaceutical Industry and we use the initial letters to define eight areas where change will be needed to redefine the industry context to facilitate change at the pharmacy level. If changes are not introduced in the way the industry is structured and operates, the industry characteristics will act as a brake on attempts by pharmacists to make changes to service delivery in their pharmacies. For example, if powerful stakeholders such as the
© Change Management and Community Pharmacy Project 5

Section 1: Introduction
AMA or Nurses Association oppose pharmacists offering more health-related services then this may create resistance to change amongst their members at the local level and frustrate individual pharmacists efforts to change. Similarly, if non-government subsidised services are to be introduced at the local community level but there is widespread resistance on the part of pharmacists themselves to charging for services and on the part of their customers to pay for such services and the Guild opposes fee-for-service, then once again this will make it difficult for most pharmacists to offer such services on a substantial scale. Services are by definition labour and knowledge intensive and therefore unlikely to be introduced on a substantial scale unless paid for. Our discussion of the PharmInd Wheel draws on a variety of our data sources but arose particularly from the analysis of interviews with pharmacists and key stakeholders. To arrive at the points we present here, we used a computer based form of content analysis, NVivo, to identify themes that emerged in these interviews. We relate these themes to the areas of strategic change for the industry context represented in the PharmInd Wheel. So the issues we raise are a synthesis of the ideas expressed by those who are directly involved in the industry. Our discussion of these issues leads us to make recommendations, particularly for the Guild, for action to be taken at the industry level which will facilitate the extension of service delivery by pharmacies. We particularly emphasise the important role of key stakeholders in supporting service delivery. Ultimately service delivery takes place through pharmacies at the local community level. It is here that we introduce our last two intellectual tools – the Pharmacy Change Readiness Wheel and the Pharmacy Change Implementation Wheel. The Pharmacy Change Readiness Wheel is designed as a tool for pharmacists to use to check whether their pharmacy is ready to introduce a change in service provision. Too often managers commence a change without having adequately assessed their own readiness for change and that of the organisation they are managing. The ten segments of the wheel represent ten key issues that pharmacists need to address before they decide to proceed with a new change program. Once again, we arrived at the definition of these areas through the use of NVivo to code issues of change readiness raised by pharmacists in interviews, focus groups and case studies. The Change Readiness Wheel allows the pharmacy owner to assess the level of readiness for change in the pharmacy and to decide whether to go ahead with the change now or to put further resources into overcoming existing deficits that may render the change program ineffective if not dealt with first. For example, current pharmacy employees may not have the knowledge, skills and resources to deliver the service to an acceptable standard. For the pharmacy owner who has decided to proceed with a change in service provision, we provide our fifth and final tool the Pharmacy Implementation Wheel. Similarly to the previous wheel, there are ten issues to be addressed and these issues also arose out of an NVivo analysis of interviews, focus groups and case studies. Each segment of this wheel is summarised by questions for the pharmacist to answer in designing and delivering an effective change program that will increase effective service delivery, contributing both to improved customer health care and business viability. For example, some questions direct attention to the need to anticipate possible resistance from external stakeholders who may be affected by the change so that plans can be formulated to include these stakeholders in the service provision and to share in the potential rewards (for example, in the case of GPs, screening may result in more patient referrals). The last part of section 5 is headed: ‘Practical Applications: A Pharmacy Change Management Service Program – Delivering Asthma & Diabetes Management Services’. We use Asthma Services as a concrete example and show how to apply the five intellectual
© Change Management and Community Pharmacy Project 6

Section 1: Introduction
© Change Management and Community Pharmacy Project 7
tools introduced earlier to create a change program, at the industry and pharmacy levels, to introduce asthma services. We also examine a financial model for the implementation at the pharmacy level for a Diabetes Service; this analysis can be used as a prototype for estimating the financial costs and benefits of introducing any new service. The effective implementation of change is a vital but neglected part of industry change. The construction of policies, however appropriate they are, does not ensure that the change will occur or that the change envisaged in the policies will actually take place. We conclude that the industry as a whole and individual pharmacies in particular need to systematically build the capabilities for change management so that there can be an effective and efficient expansion of service provision through the Australia-wide network of pharmacies. A significant feature of this report is that we argue, on the basis of our research, that this will not take place through the provision of a uniform set of cognitive services offered by all pharmacies. New strategic options for pharmacy are emerging which represent differentiated business models of product/service delivery and which will adopt different services and at different rates. These emerging strategic models are viable under the current structure of industry conditions, that is under a government regulated system. However the current system also puts constraints on the ability of pharmacies to offer new professional services which are not subsidised through the government. Current government subsidies are heavily weighted toward rewarding pharmacists for dispensing medications rather than providing services and toward dealing with crises of ill health rather than providing services that promote positive health. Change at the industry level and change at the pharmacy level are intimately interconnected. Industry change and pharmacy change need to proceed in parallel. We have made recommendations for Guild initiatives that may help move the industry context in a way that facilitates the introduction and expansion of change programs in pharmacies to widen the professional service offerings and to promote health. These measures are designed to make multi level changes that can energise the potentially powerful health service delivery system comprising Australia’s 5,000 community pharmacies, making them an even more vital element in the creation of a more integrated health service delivery in local communities.

Section 1: Introduction
Section 1: Chapter 2
2 Desired and Actual Project Outcomes The following table outlines the desired outcomes from the project, as stated in the Tender, against the actual outcomes for the study. Table 1.1: Desired vs. Actual Project Outcomes Desired Outcome Summary of outcome achievement process from
tender document Actual Outcome
1. Meet the needs and expectations of consumers (Tender Page 24)
Consumer focus groups and local Consumer Representative Forums will identify needs and expectations of consumers.
Consultations with other stakeholders who
are users of community pharmacy, such as general practitioners and allied health professionals, will ensure that broader needs and expectations are considered.
The research will also facilitate individual
pharmacist’s ability to seek and effectively use consumer feedback – this is one of the skills pharmacists would acquire through learning strategies
The needs of consumers are outlined in the consumer forum analysis (see appendix 9) and summarised in the PharmInd wheel (section 5 chapter 1)
Stakeholder interviews have been analysed
in the PharmInd wheel (section 5: 1.3.1) and the expectations and views of various stakeholder groups have been outlined
This is addressed in Marketing Change and Communicating the Vision and the Change (Pharmacy Change Implementation Wheel)
© Change Management and Community Pharmacy Project 8

Section 1: Introduction
Desired Outcome Summary of outcome achievement process from
tender document Actual Outcome
2. Identify and target different pharmacy segments with appropriate change strategies (Tender Page 24)
Work with the Guild to identify groups of pharmacies on the basis of the following categories: successful adopters versus unsuccessful adopters and non adopters, banner groups versus individual operators, urban verus rural/remote locations, etc;
Run focus groups with representatives of each type;
Identify the different restraining factors (barriers) and supporting factors (facilitators) for each category of pharmacy that affect the decision to adopt, implement and maintain service delivery;
The case studies were classified and analysed according to these categories. The examination of successful vs non-successful adopters of change was found impractical and was to be substituted for categorisation in the Pharmacy Viability Matrix. All case study pharmacies were considered to be successful adopters of change as they had all managed change in some way. They are used as profiles of typologies of pharmacies in the Australian context.
The focus groups covered these issues and the discussion (as per the Interim Report) is seen in appendix 5. The facilitators are also addressed in the following sections: Helping and assisting change, allocating resources for change, integrating and consolidating change, situating and leading change, and triggering the motivation to change (Pharmacy Change Implementation Wheel). Barriers are assessed in responding to and managing
© Change Management and Community Pharmacy Project 9

Section 1: Introduction
Desired Outcome Summary of outcome achievement process from tender document
Actual Outcome
Develop models for the optimum path to adoption, implementation and maintenance for those in each segment, with specific change strategies and financial modelling that will assist owners to move to a service delivery model where appropriate;
Differentiate these change strategies on the
basis of choosing the optimum path from a pharmacy’s current business positioning to its future choice of positioning, based on some variation of one of the four core future service delivery strategies of cost leadership, multi-segment appeal, cost niche, or focused niche; and
Examine the implications for investment in
networking, staffing and physical layout of the pharmacy, and for factors that define the environment of change such as government policy.
the resistance to change (Pharmacy Change Implementation Wheel) and non-pharmacy threats and opportunities (PharmInd Wheel)
This is addressed in the Pharmacy Viability Matrix, the financial analysis of the case studies and mail survey, the Change Readiness Wheel and the delivery options for service delivery
The Pharmacy Viability Matrix was developed and applied to indicate the future positioning for pharmacy. The Transitional and Longitudinal study looks at movement between these business models (see section 4 chapter 4).
These are outlined in the following sections: Resourcing and Revenue Flow (PharmInd Wheel), Resource availability (Pharmacy Change Readiness Wheel) and Allocating resources for change (Pharmacy Change Implementation Wheel)
© Change Management and Community Pharmacy Project 10

Section 1: Introduction
Change Management and Community Pharmacy Project 11
red Outcome Summary of outcome achievement process from tender document
Actual Outcome
©
Desi
3. Consider the different stages of the process of adoption of change (Tender Page 25)
The process of adoption is divided into the following stages:
awareness of the issue and motivation to change;
decision to adopt or not adopt; planning for implementation; initial implementation and evaluation of
early implementation; and Consolidation and extension of
implementation.
The Pharmacy Change Readiness and Change Implementation Wheels address these stages in the adoption of change for community pharmacies.
The PharmInd Wheel considers industry level change for the Guild.
4. Address ways to quickly and effectively gain the commitment of different stakeholder groups to aid the reaching and implementation of agreements to different roles for pharmacy (Tender Page 25)
This will happen primarily through the involvement of stakeholders in Diagnosis Action [II], and Change Implementation Actions [III], [V] and [VI]
The stakeholder interviews highlighted prominent issues for the various stakeholder groups. The PharmInd Wheel outlines actions that can be pursued with respect to these issues.
5. Provide an implementation program including priorities (Tender Page 25)
The implementation program is set out in Change Implementation Actions [I – VI].
For pharmacies: the Pharmacy Change Implementation Wheel addresses the program that can be followed.
For the Guild: the PharmInd Wheel 6. Provide well-argued, well-grounded and tested change management strategies (Tender Page 25)
We emphasise here the extensive experience in change management of consortium members in a variety of industries.
The report draws on extensive knowledge of the change management literature and the experience of change management experts in the project team.
7. Provide guidance to key stakeholders about the roles, actions and resources required to optimise the capacity of community pharmacy to change and deliver high value services in health care (Tender Page 26)
This will be a major outcome of Diagnosis Actions [I – II] and Change Implementation Actions [I – VI].
This is outlined in the PharmInd Wheel

© Change Management and Community Pharmacy Project 12