Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 9 , N O . 1 7 , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 2 . 0 4 5
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
Transcatheter Mitral Valve ReplacementInsights From Early Clinical Experience and Future Challenges
Ander Regueiro, MD,a Juan F. Granada, MD,b François Dagenais, MD,a Josep Rodés-Cabau, MDa
ABSTRACT
Fro
Fo
fro
Ne
fro
pa
Ma
Transcatheter mitral valve repair, particularly edge-to-edge leaflet repair, is a well-established alternative for patients
with severe primary mitral regurgitation (MR) considered at high or prohibitive surgical risk. More recently, transcatheter
mitral valve replacement (TMVR) has emerged as a potential therapeutic option for the treatment of severe MR. TMVR
may offer some advantages over transcatheter repair by providing a more complete and reproducible MR reduction.
Several devices are under preclinical and clinical evaluation, and the early experience with more than 100 patients has
demonstrated the feasibility of TMVR. In this review, we describe the TMVR systems currently in development and
the results obtained from early clinical experiences. We also discuss the main challenges in and future perspectives on
this emerging field. Future studies with a much larger number of patients are needed to provide consistent safety
and efficacy data on each of the TMVR systems. (J Am Coll Cardiol 2017;69:2175–92) © 2017 by the American College of
Cardiology Foundation.
M itral regurgitation (MR) is the most preva-lent form of valve disease in developedcountries, affecting w10% of people older
than 75 years of age (1,2). MR management is depen-dent on the cause, pathophysiology, natural history,and expected treatment efficacy. Mitral valve repairor replacement is the gold standard treatment forMR, but some studies have shown that up to one-half of the patients with severe symptomatic MR arenot referred for surgery (3,4). The mortality rate insuch patients reaches 50% at 5 years of follow-up,and up to 90% of surviving patients had at least 1 hos-pitalization for heart failure within the 5 years afterthe diagnosis of severe MR (3,4). Lack of surgicalreferral is related, in part, to the perceived risk ofthe procedure, and an alternative, less invasiveapproach in vulnerable patients would be desirable.It should be noted, however, that a significant pro-portion of patients with severe MR suffer from
m the aQuebec Heart and Lung Institute, Laval University, Quebec City,
undation, Skirball Center for Innovation, Orangeburg, New York. Drs. Rodé
m Edwards Lifesciences. The CRF Skirball Center for Innovation has rec
ovasc, Abbott Vascular, Sinomed, and Cephea. Dr. Granada is a cofounde
m the Fundacion Alfonso Martin Escudero (Madrid, Spain). Deepak L. Bha
per. Patrick O’Gara, MD, served as Guest Editor for this paper.
nuscript received November 15, 2016; revised manuscript received Febru
secondary MR, and no strong evidence exists yet forthe efficacy of any valve intervention in terms of sur-vival or improvement in quality of life in suchpatients (5).
Over the last decade, several transcatheter mitralvalve repair technologies adapted from differentsurgical techniques have emerged for treating MR inpatients at high or prohibitive surgical risk. Thetranscatheter mitral valve repair “tool box” is rapidlyexpanding, with up to 5 devices already approved inEurope, including the MitraClip (Abbott Vascular,Inc., Santa Clara, California), the DS1000 device(NeoChord, Inc., St. Luis Park, Minnesota), theCarillon (Cardiac Dimensions, Inc., Kirkland, Wash-ington), the CardioBand (Valtech Cardio, Or Yehuda,Israel), and the Mitralign device (Mitralign, Inc.,Tewksbury, Massachusetts). In current practice,transcatheter mitral valve repair is mainly limited tothe MitraClip device, which mimics the edge-to-edge
Quebec, Canada; and the bCardiovascular Research
s-Cabau and Dagenais have received research grants
eived research support from Edwards Lifesciences,
r of Cephea. Dr. Regueiro was supported by a grant
tt, MD, MPH, served as Guest Editor-in-Chief for this
ary 12, 2017, accepted February 12, 2017.

ABBR EV I A T I ON S
AND ACRONYMS
CT = computed tomography
LVEF = left ventricular ejection
fraction
LVOT = left ventricular outflow
tract
MR = mitral regurgitation
TAVR = transcatheter aortic
valve replacement
TMVR = transcatheter mitral
valve replacement
Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2176
leaflet repair described by Alfieri et al. (6).Since the introduction of MitraClip in 2003,more than 35,000 patients have been treated(7) with high success and safety rates, trans-lating into some degree of functionalimprovement in most patients (8–11).
Transcatheter mitral valve replacement(TMVR) may offer several theoretical advan-tages over transcatheter repair. Consideringthe complexity and heterogeneity of mitralvalve disease, the development of a trans-catheter mitral valve repair device to
target all anatomic variations and patient risk profileswill be difficult and presents several challenges.TMVR could offer a more universal concept fortreating mitral valve disease, with a more predictabledecrease in MR severity, in a procedure that couldpotentially be less invasive compared with currentsurgical techniques (12). Additionally, the utility ofTMVR will need to be further assessed due to thefact that surgical mitral valve repair has excellentresults in patients with severe primary MR (5), andit is unknown whether intervention will result inany changes in outcome in patients with severesecondary MR.
The objectives of this review were to provide anoverview of the main technical characteristics ofdifferent TMVR devices under preclinical and clinicalevaluation and to analyze the main clinical resultsand challenges experienced in the initial phases ofclinical validation. TMVR using transcatheter aorticvalve systems in patients with severely calcifiedmitral annuli (13) and valve-in-valve procedures forthe treatment of mitral surgical bioprostheticdysfunction (14) are beyond the focus of this review.
CHALLENGES FOR TMVR DEVELOPMENT
TARGET VALVE AND/OR DISEASE. One of the mainchallenges presented by TMVR relates to the positionand complex anatomy of the mitral valve. Transseptalaccess and a delivery catheter with high-flexure ca-pabilities are needed in order to reach the nativemitral valve with a fully percutaneous approach.Also, several aspects of the valve anatomy may in-crease the difficulty of TMVR: asymmetrical annulusand irregular geometry of valve leaflets; large di-mensions; no calcified structure in most cases; and acomplex subvalvular anatomy (which should bepreserved).
MR is a very heterogeneous disease resulting fromthe dysfunction of any of the components of themitral valve apparatus or surrounding structures. MRhas multiple causes with different stages of severity.
As MR evolves, there are changes to the ventricleassociated with geometrical distortion, which have awide range of variations as the disease progressesover time. Due to this extensive variability, it ischallenging to develop a “universal device concept”tailored to target all potential anatomic variationsseen in all MR types and patient risk profiles.
DEVICE DELIVERY. Similar to the transcatheter aorticvalve replacement (TAVR) experience, a fully percu-taneous transfemoral (venous) procedure would bethe less invasive and preferred approach for TMVR.However, that approach faces the challenges of ahigh-profile delivery system (to accommodate a largevalve prosthesis) that has to negotiate an extremeangle within a relatively small space (through thetransseptal approach) to reach the mitral valve. Thisis partially the reason why most TMVR systems todate have been developed to deliver the valve pros-thesis transapically, following a puncture of theventricular apex. The transapical approach has been acommon alternative in TAVR for patients withoutiliofemoral access and has the advantage of a veryshort distance between the access and the targetvalve, also allowing good alignment of the valveprosthesis with small movements of the deliverysystem. However, many studies have reportedpoorer outcomes associated with transapical TAVR(compared with transfemoral access), likely related toa higher degree of myocardial injury, along with thenegative effects of a thoracotomy in a high-risk andfrail population (15–17). The transition from trans-apical to transseptal delivery of clinically availableTMVR devices will require important engineeringmodifications in size and possible valve designs andanchoring mechanisms.
VALVE PROSTHESIS ANCHORING AND SEALING. Thepathophysiology and anatomic substrate of MR iscomplex and heterogeneous. One of the main chal-lenges in the development of TMVR is trying to obtainprosthesis stability similar to that of surgical mitralvalve replacement. In contrast to TAVR, where thelanding zone for the prosthesis is a tubular calcifiedstructure, the valve prostheses used to treat MR innative valves need to be anchored into a dynamic,D-shaped noncalcified structure. To tackle this issue,several mechanisms have been proposed (18,19),including: 1) application of counteracting axial forces,tensioning the device between a proximal and a distalconstraint (apical tether; Tendyne valve; AbbottVascular, Abbott Park, Illinois); 2) ventricular anchorsto grasp the free margins of the native leaflets (nativeleaflet engagement; Tiara valve; Neovasc, Richmond,British Columbia, Canada); 3) atrial and ventricular

J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2177
flanges that engage the mitral annulus and mitralleaflets/chordae (mitral annulus clamping; CardiAQ-Edwards; Edwards Lifesciences, Irvine, California);4) a series of anchors around the edge of the valvethat either pierce the mitral valve tissue or providesfriction with radial interference (annular winglets;NaviGate valves; NaviGate Cardiac Structures, LakeForest, California); 5) a “champagne cork-like” effectproduced by a radial force along the valve stent(radial force; Intrepid valve; Medtronic, Minneapolis,Minnesota); and 6) simultaneous creation of a landingzone by implanting a ring or a docking system(external anchor; Caisson [anchor is fixed by mitralannulus clamping]; Maple Grove, Minnesota), MValve(subannular mitral ring; Herzliya, Tel Aviv, Israel),and HighLife valves (dock is anchored by mitralannulus clamping; HighLife Medical, Irvine, Califor-nia) (Central Illustration).
Valve sealing is also a major challenge in TMVR.The complex 3-dimensional (3D) anatomy with a dy-namic morphology of the mitral annulus, along withthe high-pressure gradient generated by the ventricleduring systole, may contribute to the occurrence ofsignificant paravalvular leakage following valveimplantation.
LEFT VENTRICULAR OUTFLOW TRACT OBSTRUCTION.
Left ventricular outflow tract (LVOT) area isdecreased following mitral surgery with annuloplastyrings and prostheses (20), and LVOT obstruction aftersurgical mitral valve procedures has also beendescribed (21). This phenomenon has not been limitedto the use of surgical prostheses, and it has also beendescribed following transcatheter mitral procedureswith nondedicated devices. The reported rate ofacute LVOT obstruction with transcatheter mitralvalve-in-ring procedures is 8.2% (14), and it increasesup to 9.3% following TMVR in the presence of severemitral annular calcification (13). Multiple factorsshould be evaluated when determining the risk ofLVOT obstruction after TMVR (22,23): the aortomitral-annular angle, which is the angle between theannular planes of these 2 valves (if the angle isobtuse, there may be a higher risk of obstruction, asthe struts of the prosthesis will encroach on theLVOT); degree of septal hypertrophy; left ventriclesize; and device protrusion and flaring into the LVOT.
PRE-PROCEDURAL PLANNING AND MULTIMODALITY
IMAGING. Pre-procedural multimodality imaging isessential for TMVR planning. Pre-procedural imagingis used to define the presence, type, and severity ofMR; to confirm patient eligibility according to theanatomic characteristics and the prosthetic valvedesigns; to identify patients at risk for possible
specific TMVR complications (e.g., LVOT obstruc-tion); and to determine pre-operative prediction offluoroscopic angulation and access location.
Echocardiography remains the gold standard fordiagnosing MR (5). A comprehensive echocardio-graphic examination helps to establish the cause,mechanism, and severity of MR and the impact of MRon myocardial function. Additionally, echocardiog-raphy with 3D segmentation of the mitral annulus canbe used as the initial screening imaging modality forTMVR in patients with impaired renal function whoare at risk for acute kidney injury with contrastcomputed tomography (CT).
Although echocardiography is the primary imagingmodality for the diagnosis and quantification of MR,CT is the preferred imaging modality for pre-procedural TMVR evaluation. However, withimproving 3D technology, transesophageal echocar-diography could assume a more important role overtime. Electrocardiogram (ECG)-gated cardiac CT of-fers 3D volumetric data sets with submillimeterspatial resolution, enabling a comprehensive assess-ment by providing an exact characterization of theanatomy of the subvalvular apparatus and the ge-ometry of the mitral valve (24). This process has alsobeen shown to be highly reproducible (25,26). Inaddition to ECG-gated cardiac CT, non–ECG-gated CTdata acquisition of the thorax may be performed toevaluate thoracic wall anatomy for device deploy-ment in transapical approaches and of the pelvis toevaluate the iliofemoral venous diameter in patientsundergoing transfemoral TMVR. Three-dimensionalCT reconstruction data are used during thescreening process to assess mitral valve anatomy anddetermine the appropriateness of different devicesfor each individual patient. Although it is currentlythe preferred modality for pre-procedural TMVRevaluation, there is still uncertainty about the mostimportant variables, as many of the measurementsare empirical, requiring validation (Figure 1). It isanticipated that the ideal means of measuring mitralvalve anatomy to guide device and patient selectionwill be refined with increasing clinical experience.The most important information that should beincluded in a pre-procedural TMVR comprehensivesystematic CT analysis is described in Table 1. Thedefinitions and methodology for each measurementare beyond the scope of this paper. More informationcan be found elsewhere (18,25–31).
PROSTHETIC VALVE STRUCTURAL DEGENERATION.
Although no long-term durability data exist forTMVR, there are some factors that should be consid-ered regarding the possibility of bioprosthesis

CENTRAL ILLUSTRATION Transcatheter Mitral Valve Replacement for Native Mitral Regurgitation
Regueiro, A. et al. J Am Coll Cardiol. 2017;69(17):2175–92.
(Top) Main challenges for transcatheter mitral valve replacement for treating native mitral regurgitation. (Bottom) Anchoring mechanisms of
transcatheter mitral valve prostheses. Ao ¼ aorta; LA ¼ left atrium; LV ¼ left ventricle; LVOT ¼ left ventricular outflow track.
Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2178

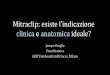
FIGURE 1 CT Pre-Procedural Data for TMVR
CT pre-procedural data showing several different measurements used to screen patients for TMVR on the basis of anatomic criteria. (A) Mitral
annulus measurements showing septal-to-lateral distance (dotted line) and intercommisural distance (solid line). (B) Distance between
papillary muscles heads. (C) Projected distance from papillary muscle head to the mitral annulus plane (solid line), projected distance between
papillary muscle head and the center of the mitral annulus (dashed line), and distance between papillary muscle head and ventricular wall
(dotted line). (D) Posterior leaflet length at the P2 level. (E) Aortomitral angulation. (F) Left atrium height (solid line) and short-axis
diameter (dotted line). CT ¼ multislice computed tomography; TMVR ¼ transcatheter mitral valve replacement.
J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2179
degeneration. First, surgical mitral bioprostheticvalves are more likely to suffer from early structuraldegeneration than surgical aortic bioprostheses. Also,surgical bioprostheses tend to degenerate morerapidly in younger patients (32). Although this may beof lesser concern in patients with a relatively shortlife expectancy, young patients with MR may have alonger life expectancy, which raises concerns aboutlong-term durability. A systematic clinical and echo-cardiographic follow-up of patients undergoingTMVR will be critical to provide consistent data for
valve durability and structural valve failure in thecoming years.
TMVR DEVICES UNDER
CLINICAL EVALUATION
CardiAQ-EDWARDS TRANSCATHETER MITRAL VALVE. TheCardiAQ-Edwards transcatheter mitral valve is aself-expanding trileaflet valve composed of bovinepericardial tissue (Table 2, Figure 2). The nitinol frameis composed of 2 sets of circumference-oriented,

TABLE 1 CT Pre-Procedural Assessment for TMVR
Exam Anatomical structure Measurement
Cardiac CT scan Mitral annulus Intercommisural distance
(ECG-gated) Septal-to-lateral distance
Trigone-to-trigone distance
3D perimeter
Projected area
Projected perimeter
Mitral annular trajectory
Mitral annular calcification
En face view fluoroscopic angulation
Compromise-view angulation
Mitral leaflets Mitral leaflet length
Mitral leaflet calcification
Papillary muscles Distance between heads
Projected distance to the mitralannulus plane
Distance to the ventricular wall
Left atrium Long-axis diameter
Short-axis diameter
Left atrium height
LAA ostium to mitral annulus distance
Left ventricle Long-axis diameter
Width in long-axis view
Interventricular septum thickness
LVOT Aorto-mitral angle
Neo-LVOT cross-sectional area
Thorax CT scan Left ventricle apex Ideal intercostal space fortransapical approach
(Non-ECG-gated) Distance from sternal midline
Angulation for coaxial deployment
AbdominopelvicCT scan
Iliofemoral vein Iliofemoral venous diameter fortransfemoral approach
3D ¼ 3-dimensional; CT ¼ multislice computed tomography; ECG ¼ electrocardiogram; LAA ¼ left-atrial appendage; LVOT ¼ left ventricular outflow tract ejection fraction; TMVR ¼ transcathetermitral valve replacement.
Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2180
opposing anchors which secure the device to themitral annulus. The ventricular anchors rest behindthe mitral leaflets and subvalvular apparatus, pre-serving the chords and using native leaflets as sup-port. The symmetrical design requires no rotationalalignment. The frame is covered by a polyester fabricskirt designed to reduce the risk of paraprostheticleakage. The valve has a supra-annular positionintended to minimize the ventricular profile and,therefore, the risk of LVOT obstruction. The valve canbe implanted using a transapical or transfemoralapproach.
The procedure can be summarized in 5 steps: 1) thedelivery system is advanced across the interatrialseptum in the transseptal approach or using the apexin the transapical access approach; 2) after crossingthe mitral valve, a ventriculogram is obtained toreassess the mitral plane and correct the height of the
system (above the papillary muscles); 3) the leftventricular anchors are released by turning theretraction wheel to initiate leaflet capture; 4) thevalve is expanded to finalize leaflet capture; and5) after a correct position is confirmed, the valve isreleased (33).
The first-in-human implantation of the first-generation CardiAQ was done in 2012 (34). Sincethen, 13 cases have been reported, including 1additional patient treated through a transfemoralapproach with the second-generation valve (35,36).The main clinical results of this initial clinical expe-rience are summarized in Table 3. An early feasibilitystudy, which plans to enroll 28 patients, using thetransfemoral and transapical delivery systems iscurrently enrolling patients, and a larger prospectiveregistry including 200 patients started in 2016(Table 4).
NEOVASC TIARA MITRAL TRANSCATHETER HEART
VALVE. The Tiara valve is a self-expanding trileafletvalve made of bovine pericardium and a nitinolframe (Table 2, Figure 3). The valve is designed tofit the D-shaped mitral annulus. The atrial portionhelps to seat the prosthesis into the atrial portionof the mitral annulus and has a full atrial skirt.The ventricular anchors (2 anterior and 1 posterior)fix the valve onto the fibrous trigon and the posteriorpart of the annulus. There are 2 valve dimensions:the 35-mm valve has internal dimensions of 30 mmand 35 mm (area ranges: 6.3 cm2 to 9.0 cm2), andthe 40-mm valve has internal dimensions of 34.2 mmand 40 mm (area ranges: 9.0 cm2 to 12.0 cm2) (37).The valve is implanted using the transapicalapproach (38).
The procedure can be summarized in 4 steps: 1) theleft ventricular apex is exposed through a left mini-thoracotomy, a needle puncture is performed, anda J-tip wire is introduced across the mitral valve;2) the Tiara delivery system is introduced directlyand across the mitral valve, and the atrial portion ofthe prosthesis is unsheathed, oriented, and alignedwith the D-shaped mitral annulus to allow proper fit;3) the delivery system is then pulled back to seatthe atrial part of the valve; and 4) the ventricularanchors are released to secure and release theprosthetic valve (39).
The first cases using the Tiara mitral valve systemimplants were performed in January 2014 in Vancouver(38). Since then, 19 cases have been reported, 5 patientsin the TIARA-1 early feasibility study and 14 patientsunder a special access program (Table 3) (40). An earlyfeasibility trial is currently enrolling patients and plansto include a total of 30 patients (Table 4).

TABLE 2 TMVR Technologies Under Clinical Evaluation
CardiAQ-Edwards Neovasc Tiara Tendyne Intrepid TMVR
Valve shape Circular D-shaped D-shaped (outer stent)Circular (inner frame)
Circular
Frame Nitinol, self-expandable Nitinol, self-expandable Nitinol, double frame;Self-expandable
Nitinol, double stent;Self-expandable
Anchoring mechanism Mitral annulus capture with nativeleaflet engagement
Fibrous trigone capture withnative leaflet engagement
Apical tether Radial force and subannularcleats
Leaflets TrileafletBovine pericardium
TrileafletBovine pericardium
TrileafletPorcine pericardium
TrileafletBovine pericardium
Valve position Supra-annular Intra-annular Intra-annular Intra-annular
Access TransapicalTransseptal
Transapical Transapical Transapical
Delivery system size 33-F 32-F 36-F 35-F
Recapture No No Fully recapturable system aftercomplete deployment
No
Valve size(s) 30 mm 35 mm and 40 mm Outer frame ranges from30–43mmin the SL dimension and34–50 mm in the IC dimension
27 mm with 3 outer stent sizes(43, 46, and 50 mm)
Additional features Supra-annular positionIntra-annular sealing skirtTapered outflow
2 anterior and 1 posterioranchoring structures
Single inner valve size; Multipleouter frame sizes
Dual stent design; Outer frameprovides fixation and isolatesthe inner stent
TABLE 2 Continued
Caisson HighLife TMVR MValve system NCSI NaviGate Mitral
Valve shape D-shape Circular – Circular
Frame 2 components (anchor and valve);Nitinol, self-expandable.
2 components (ring and valve);Nitinol, self-expandable
Dock system to be used withcommercially available valves
Nitinol, self-expandable;Xenogeneic pericardium
Anchoring mechanism External anchor; Mitral annuluscapture with engagement atsubannular fibrous groove
External anchor; Valve insubannular mitral ring
External anchor; Mitral annuluscapture
Annular winglets
Leaflets TrileafletPorcine pericardium
TrileafletBovine pericardium
– Trileaflet
Valve position Supra-annular –
Access Transseptal Transapical (Transfemoral arteryfor loop placement)
Transapical Transapical, transatrial ortransfemoral
Delivery system size 31-F NA 32-F 30-F
Recapture Fully recapturable and retrievable No Fully retrievable NA
Valve size(s) 35–40 mm 31 mm NA Inflow/outflow: 30 mm/36 mm;30mm/40mm; 33mm/44mm
Additional features SAM Management feature1 delivery catheter for each system
(anchor and valve)
NA Universal dock system NA
IC ¼ intercommissural; NA ¼ not available; SAM ¼ systolic anterior motion of the mitral valve; SL ¼ septal-lateral; TMVR ¼ transcatheter mitral valve replacement.
J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2181
TENDYNE BIOPROSTHETIC MITRAL VALVE SYSTEM. TheTendynemitral valve system is composed of a trileafletporcine pericardial valve on a self-expanding nitinoldouble-frame stent, an adjustable tether, and an apicalfixation/sealing pad (Table 2, Figure 4). The valve isdesigned to fit the mitral annulus and can accommo-date a wide range of sizes. The inner stent is one sizeand circular to maintain an effective orifice area of>3.2 cm2. There is an atrial cuff designed to providesealing (prevention of diastolic paravalvular leak) andanchoring (preventing valve from pulling into theventricle when force is applied to the tether). A leftventricular apical tethering system with an apical padanchors the device and assists with apical closure. The
device is implanted using a transapical approach andcan be fully retrieved or repositioned even after fulldeployment (41).
The procedure can be summarized in 4 steps: 1)Standard transapical approach through a left mini-thoracotomy and left ventricle access. 2) A balloon-tipped catheter is advanced into the left atrium todeliver a standard 0.035-inch guidewire. The 36-Fdelivery system is advanced over the guidewire. Thevalve is brought into the left atrium and positionedabove the mitral annulus and allowed to partiallyexpand. 3) The valve’s rotational orientation is veri-fied and corrected if necessary to assure the D-shapedouter stent is oriented so that the straight side is

FIGURE 2 CardiAQ-Edwards Valve
(A) Valve prosthesis (provided by Edwards Lifesciences). (B) Fluoroscopy. (C) Three-dimensional transesophageal echocardiography from the
surgeon’s point of view.
TABLE 3 TMVR Syst
Baseline characteristics
Age, yrs
Female
STS PROM score
NYHA functional clas
LVEF, %
<30%
30%–49%
$50%
Ischemic/functional M
Procedural and 30-day
Technical success
Valve dislocation/em
Conversion to open-
Post-procedural $ m
LVOT obstruction
Procedural mortality
30-day moderate or
All-cause 30-day mo
Follow-up
Follow-up, months
MR $ moderate
NYHA functional clas
Mortality
Values are mean (range), mstudy implants, 5 compassechocardiography was perffollow-up for up to 18 mo
LVEF ¼ left ventricular eTables 1 and 2.
Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2182
aligned with the anterior aspect of the mitral orifice.The valve is deployed into the mitral orifice. 4) Theapical pad is threaded over the tether and positionedon the epicardium at the left ventricular access; a
em Preliminary Clinical, Procedural, and Follow-Up Features
CardiAQ-Edwards(N ¼ 13)
Intrepid TMVR(N ¼ 27)
Fortis*(N ¼ 13)
NA 74 (58–90) 71 � 8
2/13 (15.4) 9/27 (33.3) 3/13 (23.1)
NA 6.2 (1.0–23.3) 7.2 � 3.6
s $III NA 23/27 (85.3) 13/13 (100)
40 (20–72) NA 34
NA 5/27 (18.5) NA
NA 14/27 (51.8) NA
NA 8/27 (29.6) NA
R 9/13 (69.2) 21/27 (77.8) 12/13 (92.3)
data
12/13 (92.3) 24/26 (92.3)‡ 10/13 (76.9)
bolization NA NA 2/15 (15.4)
heart surgery NA NA 2/15 (15.4)
oderate MR NA 0/26 (0.0) 0/9 (0.0)
NA 0/26 (0.0) 0/9 (0.0)
2/13 (15.4) 4/27 (14.8) 4/13 (30.8)§
severe MR NA NA NA
rtality 7/13 (53.8) 6/25 (24.0) 5/13 (38.5)
NA 8.1 (0–20.7) 6 (1–15)
NA 0/24 (0.0) 0/8 (0.0)
s $III NA 2/18 (11.1) 2/8 (25.0)
7/13 (53.8) 7/27 (25.9) 6/13 (46.2)
ean � SD, or n/N (%). *In late 2015, Edwards Lifesciences stopped the FORTIS program. Thionate use implants. Results of the first 30 early feasibility study cases are available (43ormed in 26 of the 27 patients with a prosthesis in situ. ¶Follow-up data for longer than 30 dnths.
jection fraction; MR ¼ mitral regurgitation; NYHA ¼ New York Heart Association; STS PROM
tension tool is used to adjust the tether length fromthe valve to the ventricular apex to provide valvestability. The apical pad is secured and assists withclosure of the apex (42).
Neovasc Tiara(N ¼ 19)
Tendyne†(N ¼ 30)
Caisson(N ¼ 5)
HighLife(N ¼ 6)
73 (39–89) 75.9 (55–91) 77.4 (70–91) 69 (57–79)
6/19 (31.6) 5/30 (16.7) 3/5 (60.0) 2/6 (33.3)
10.7 (2.09–47.7) 7.3 (2.0–16.0) 8.8 (5–10) 3.3 (2.5–4.9)
19/19 (100) 16/30 (53) 5/5 (100) 6/6 (100)
34 (15–65) 47.1 � 9.2 42.6 (28–58) 33.7 (20–50)
5/19 (26) 3/29 (10.3) 1/5 (20.0) 1/6 (16.7)
13/19 (68) 14/29 (48.3) 2/5 (40.0) 4/6 (66.7)
1/19 (5) 12/29 (41.4) 2/5 (40.0) 1/6 (16.7)
12/19 (63.2) 23/30 (76.7) 3/5 (60.0) 3/6 (50.0)
16/19 (84.2) 28/30 (93.3) 4/5 (80.0) 5/6 (83.3)
3/19 (15.8) 0/30 (0.0) 0/5 (0.0) 0/5 (0.0)
3/19 (15.8) 0/30 (0.0) 0/5 (0.0) 1/6 (16.7)
NA 1/30 (3.3) 0/4 (0.0) 0/6 (0.0)
0/19 (0.0) 1/30 (3.3) 0/4 (0.0) 0/6 (0.0)
0/19 (0.0) 0/30 (0.0) 0/5 (0.0) 1/6 (16.7)
NA 0/26 (0.0)k 0/3 (0.0) 0/4 (0.0)
3/19 (15.8) 1/30 (3.3) 1/4 (25.0) 2/6 (33.3)
NA NA¶ 3.4 (3–4) 4.1 (3–6)
0/14 (0.0) 0/5 (0.0) 0/4 (0.0) 0/4 (0.0)
NA NA 0/3 (0.0) 0/4 (0.0)
3/19 (15.8) 0/5 (0.0) 1/4 (25.0) 2/6 (33.3)
e valve is not currently available. †>50 implants up to June 2016; 32 early feasibility). ‡In 1 patient, deployment was not attempted. §In-hospital mortality. kRepeatedays from 5 patients, 2 patients with follow-up for up to 6 months, and 3 patients with
¼ Society of Thoracic Surgeons’ perioperative mortality risk; other abbreviations as in

TABLE 4 Ongoing and Future Studies on TMVR Therapies for Treating MR
Device Manufacturer Study Study DesignEstimatedEnrollment Primary Outcome Measures
CardiAQ-Edwards Early feasibility study(NCT02718001)
Prospective registry 28 patients Safety assessed by freedom from device or procedure-relatedadverse events at 30 days
CardiAQ-Edwards RELIEF trial (NCT02722551) Prospective registry 200 patients Freedom from major adverse cardiac and cerebrovascularevents at 30 days per MVARC definition.
Freedom from individual adverse events at 30 days
Neovasc Tiara TIARA-I (NCT02276547) Prospective registryEFS trial
30 patients Freedom from all-cause mortality and major adverse events,defined as disabling stroke, myocardial infarction, renalfailure requiring dialysis, life-threatening bleeding, andcardiac surgical or transcatheter reintervention at 30 days
Tendyne Early feasibility study of theTendyne Mitral valve system(NCT02321514)
Prospective registryEFS trial
110 patients Safety assessed by freedom from device or procedure relatedadverse events at 30 days
Performance assessed by freedom from device malfunction at30 days
Intrepid Twelve Transcatheter Mitral ValveReplacement Pilot Study*(NCT02428010)
Prospective registryEFS trial
10 patients Adverse events associated with the delivery and/orimplantation of the device at 30 days
Caisson PRELUDE (NCT02768402) Prospective registryEFS trial
20 patients Freedom from major adverse events including death, stroke,myocardial infarction, and surgical reintervention through30 days
MValve DOCK 1 (NCT02719912) Prospective registryEFS trial
30 patients Composite serious adverse cardiac events and stroke at30 days
*Information submitted to ClinicalTrials.gov in April 23, 2015, before Medtronic acquisition of Twelve, Inc.
DOCK I ¼ Mitral Valve Replacement With MValve Dock and Lotus; EFS ¼ early feasibility study; Mfr ¼ manufacturer; MVARC ¼ Mitral Valve Academic Research Consortium; PRELUDE ¼ CaissonTranscatheter Mitral Valve Replacement (TMVR) System Early Feasibility Study; RELIEF ¼ CardiAQ-Edwards Transcatheter Mitral Valve Replacement (TMVR) Study; TIARA ¼ Early Feasibility Study of theNeovasc Tiara� Mitral Valve System; other abbreviations as in Tables 1 and 3.
J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2183
The first-in-human implantation of the Tendynevalve was performed in October 2014 (41). The resultsof the first 30 patients treated with this valve havebeen reported and are summarized in Table 3 (43). Anearly feasibility study of the Tendyne mitral valvesystem is currently recruiting patients (Table 4).
MEDTRONIC INTREPID TMVR. The Intrepid TMVR isa tri-leaflet bovine pericardial valve contained in a
FIGURE 3 Tiara Valve
(A) Valve prosthesis. (B) Fluoroscopy. (C) Three-dimensional transesoph
Cheung et al. (38).
self-expanding nitinol frame, which has dual structuredesign consisting of a circular inner stent to house thevalve and a conformable outer fixation ring to engagethe mitral anatomy. The outer fixation ring is designedto accommodate the variability of the native mitralannulus while isolating the inner valve assemblythroughout the cardiac cycle. A flexible brim isattached to the atrial end of the fixation ring, whichfacilitates imaging during the procedure (44). The
ageal echocardiography from the surgeon’s point of view. Reprinted with permission from

FIGURE 4 Tendyne Valve
(A) Valve prosthesis. (B) Fluoroscopy. (C) Three-dimensional transesophageal echocardiography from the surgeon’s point of view. Reprinted
with permission from Muller et al. (43).
Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2184
outer stent is being investigated in 3 sizes of 43, 46,and 50 mm. The circular inner stent houses a 27-mmvalve across the 3 outer stent sizes (Table 2, Figure 5).There is no need for rotational alignment or to searchfor leaflets. Fixation and sealing are achieved througha combination of design features: 1) the outer fixationring is larger in circumference than the native mitralvalve annulus with varying degrees of radial stiffnessalong its axial length; 2) the flexible atrial portion de-flects inward while the stiff ventricular mid-sectionresists compression and maintains its shape, produc-ing a final ‘champagne cork-like’ conformation (nar-row neck and wider body) to resist migration undersystolic pressures and; 3) 3 circumferential rings of
FIGURE 5 Intrepid TMVR
(A) Valve prosthesis. (B) Fluoroscopy. (C) Three-dimensional transesoph
TMVR ¼ transcatheter mitral valve replacement. A was reprinted from M
Publishing. B and C are courtesy of Dr. Vinayak Bapat, Guy’s and St. Tho
frictional elements on the outer stent further helpfixation. The prosthesis is designed to preserve thenative leaflets and chordae and leverage them to sealaround the device (44).
The Intrepid TMVR delivery system is currentlydesigned for transapical access only and consists ofan apical introducer sheath (with dilator) and a hy-draulically actuated delivery catheter. The procedurecan be summarized in 5 steps: 1) after standardtransapical access, the system is advanced across themitral valve; 2) the valve is expanded until the brim iscompletely deployed; 3) the system is retracted intothe desired position on the annulus; 4) the fixationring is expanded; and 5) the valve is released, the
ageal echocardiography from the surgeon’s point of view.
eredith et al. (44), printed with permission from Europa Digital &
mas’ NHS Foundation Trust, London, United Kingdom.

FIGURE 6 Caisson Valve
(A) Valve prosthesis. (B) Fluoroscopy. (C) Two-dimensional transesophageal echocardiography. A was provided by Caisson Interventional.
B and C are courtesy of Dr. Mathew Williams, NYU Langone Medical Center, New York, New York.
J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2185
sheath is removed, and the incision is closed. Steps 3through 5 are performed under rapid ventricularpacing. Duration of rapid pacing has averaged at 30 sduring deployment (45).
The first case to use an Intrepid TMVR in a humanwas performed in September 2014. Since then, 27patients have been treated, and the main clinical re-sults are summarized in Table 3 (44,46,47). A pro-spective registry is ongoing (Table 4).CAISSON TMVR SYSTEM. The Caisson TMVR systemconsists of 2 main components, an anchor and avalve (Table 2, Figure 6). The anchor is a D-shaped,self-expanding nitinol structure. It serves as a foun-dation that grips the native valve annulus. The
FIGURE 7 HighLife Valve
(A) Valve prosthesis. (B) Fluoroscopy. (C) Transesophageal echocardiogra
German Heart Center Munich, Munich, Germany.
anchor is implanted onto the mitral valve such thatthe tips of the ventricular feet engage under themitral valve annulus, and the atrial holding featuresengage with the atrial surface of the mitral valveannulus. The valve is composed of a self-expandingnitinol frame with a trileaflet porcine pericardialvalve and is designed to nest in the anchor. Both thevalve and the anchoring system are retrievable (48).The valve is delivered completely percutaneously,using the transfemoral approach with a 31-F deliverysystem (49).
Five patients were treated through October 2016,4 in a U.S. early feasibility study and 1 patient underthe Canadian special access program (49). The main
phy from the surgeon’s point of view. Courtesy of Dr. Rüdiger Lange,

FIGURE 8 MValve
(A) Valve prosthesis. (B) Fluoroscopy. (C) Transesophageal echocardiography from the surgeon’s point of view. Courtesy of Dr. Maurice
Buchbinder, Stanford University/VA Palo Alto Healthcare System, Palo Alto, California.
Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2186
clinical results of this initial experience are summa-rized in Table 3. The first-in-human early feasibilitystudy is ongoing and plans to include 20 patients in5 centers (Table 4).
HighLife TMVR DEVICE. The HighLife device iscomposed of 2 components: a ring that is placedaround the native leaflets (subannular implant) and aprosthetic valve that is placed inside the ring (Table 2,Figure 7). The valve prosthesis is composed of a31-mm nitinol frame and a trileaflet bovine pericardialvalve that has a pre-formed groove in the annularregion. The subannular implant consists of a polymertube with nitinol hooks for ring closure that is placedaround the prosthesis to avoid displacement of thevalve into the left ventricle. In its final position, thenative leaflets are trapped between the subannularimplant and the prosthetic valve (50).
The procedure can be summarized in 3 steps: 1) aguidewire is introduced through the femoral arteryand is looped around the native mitral valve leaflets;2) the subannular implant ring is placed over theguidewire loop; and 3) the prosthetic valve isimplanted through a transapical approach similar to avalve-in-ring implant. A single-center early feasibilityand safety study is ongoing. Results from the first6 patients treated with this device have been reportedand are summarized in Table 3 (51).
MValve SYSTEM. The MValve system is not a valvebut a docking device designed to fit other trans-catheter prostheses that are anchored within thedocking system (Table 2, Figure 8). The MValve sys-tem can be implanted using a transapical approachand is designed to be compatible with a variety of
commercially available transcatheter valves. Theanchoring of the docking system is designed to allowpreservation of the native leaflet function, offering atrue chord-sparing approach. The MValve systemenables positioning due to its fluoroscopic visibility,atrioventricular positioning, and a sealing elementthat is intended to minimize the risk of paravalvularleak. The docking system can be recaptured andretrieved after full deployment (52).
The first-in-human implantation was performed inSeptember 2015. There were no major periproceduralcomplications, and immediate post-operative echo-cardiography revealed no residual MR and good valveposition. The patient died 20 days after the proceduredue to pneumonia. The early feasibility and safetystudy of the MValve in conjunction with the Lotustranscatheter heart valve (Boston Scientific, Marl-borough, Massachusetts) is planned to start by thesecond quarter of 2017 (Table 4). The company iscurrently also working on the design of the next-generation MValve device. The goal for this new-generation device is implantation in a single-stepprocedure, and it will have a proprietary valve builtand secured within the MValve dock. It will beadaptable for transseptal implantation with a profileof 24-F (53).
NCSI NaviGate MITRAL VALVE. The NaviGate valveis a self-expandable TMVR system composed of anitinol stent-frame with a truncated cone 21 mm inheight (Table 2, Figure 9). Several annular wingletsanchor the valve within the mitral annulus. The valvecan be delivered using transatrial, transapical, ortransseptal access. The delivery system has a

FIGURE 9 NaviGate Valve
(A) Valve prosthesis. (B) Valve prosthesis after explantation in an animal model. (C) The 2-dimensional transesophageal echocardiography
short-axis view during preclinical evaluation. Images provided by NaviGate Cardiac Structures.
J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2187
diameter of 30-F at the distal part and 18-F at thelevel of the catheter shaft (54). The first-in-humanimplantation of the NaviGate valve was performedin October 2015. According to the manufacturer’s in-formation, the early feasibility and safety study witha transatrial approach is planned to start during 2017and will include 30 patients in 2 centers (55). Furtherinformation regarding this trial has is not yetavailable.
TECHNOLOGIES UNDER
PRECLINICAL EVALUATION
AccuFit TMVR SYSTEM. The AccuFit TMVR system(Sino Medical Science Technology, Inc., Tianjin,China) is composed of a circular, self-expanding, self-centering frame device that has an atrial flange, aventricular flange, and an annulus support(Figure 10). It has a supra-annular design and is self-centering. The valve is made of 3 bovine pericardialleaflets. The valve is anchored mainly through sand-wiching the annulus and native valve leaflets be-tween the atrial and ventricular flanges. Theprosthetic valve is implanted using a transapicalapproach with a 38-F caliber system (56). The first-in-human study will be initiated in the first quarter of2017 (57).
CARDIOVALVE TMVR SYSTEM. The CardiovalveTMVR is a self-expandable trileafleat valve(Figure 10). The system is advanced using the trans-femoral approach with a 28-F introducer. The heightof the crimped valve is 32 mm. Once the valve isdeployed, the protrusion into the left ventricle is
approximately 12 mm. The valve is anchored into themitral annulus over 24 focal “sandwiching” points,with a symmetrical design that does not requirerotational positioning. There are 3 differently sizedvalves with diameters that range from 40 to 50 mm.The system is under preclinical evaluation, andthe first-in-human implantations are planned for2017 (58).
CEPHEA TMVR SYSTEM. The Cephea TMVR system(Cephea Valve Technologies, San Jose, California)consists of a self-expanding double-disk structureand a bovine trileaflet valve (Figure 10). The pros-thesis has a multilevel conformability design, makingthe valve capable of adapting to various anatomies.The atrial disc rests on the floor of the left atrium, thecenter column provides a stable platform for leafletsupport, and the ventricular disc anchors to the sub-annular region. This modular architecture isolates theprosthesis from external annular and myocardialdeformation. The prosthesis can be deployed using anantegrade approach (transatrial or transseptal) andcan be fully recaptured. There is a 2-step deploymentthat uses multiple redundant mechanism to anchorthe valve. During the first step, the frame aligns andself-orients to the subannular plane, and anchorsusing the native annulus as a support, and during thesecond step, the frame self-centers and seals bysupra-annular fixation (59,60). The first-in-humanimplantations are planned for 2017.
SATURN TMVR TECHNOLOGY. The Saturn technol-ogy (InnovHeart Srl, Milan, Italy) is composed of anannular structure that encircles the mitral valve andprovides support for the valve prosthesis (Figure 10).

FIGURE 10 TMVR Technologies Under Preclinical Evaluation
(A) AccuFit TMVR. (B) Cardiovalve. (C) Cephea. (D) Saturn TMVR. (E) Abbott TMVR. TMVR ¼ transcatheter mitral valve replacement. A was reprinted from Abdelaghani
et al. (56), with permission from Europa Digital & Publishing. B is reprinted with permission from De Backer et al. (69). D was provided by InnovHeart. E was provided
by Abbott Vascular.
Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2188
Both parts are designed to be connected by means ofguidewires. The transapical procedure has alreadybeen preclinically validated. The procedure using atransseptal approach is under development. The firstpart of the procedure consists of positioning a pair ofguidewires to embrace the mitral leaflets at a levelimmediately below the mitral annulus. The annularstructure is then introduced over-the-wire in the leftventricle. The second part consists of introducingonto the left ventricle the collapsed central stentengaged over the connecting guidewires to reconnectthe component to the annular structure, followedby the final positioning and release of the centralstent (61).
ABBOTT TMVR. The Abbott TMVR system (AbbottVascular, Abbott Park, Illinois) is a self-expandingbovine trileaflet valve with 2 components: a nitinolannular portion and a braided nitinol atrial section(Figure 10). The atrial section is intended to avoidparavalvular leakage. Fixation of the valve is accom-plished by leaflet capture and atrial sealing. The
procedure is done using the transapical approach(62). A transfemoral delivery system is indevelopment.
There are several other devices under preclinicalevaluation. However, design features of and preclin-ical results using these devices are very limited at thepresent time.
INSIGHTS FROM TMVR EARLY
CLINICAL EXPERIENCE
PATIENT CLINICAL CHARACTERISTICS AND SELECTION.
According to early observations reported withvarious systems, patients currently selected forTMVR are those considered at high or prohibitivesurgical risk, as determined by surgical risk scoresand evaluation by the heart team. To date, mostpatients have been treated on the basis of compas-sionate clinical use programs. There are, however,scarce data for the reasons for selecting TMVRover other approved transcatheter therapies, such as

TABLE 5 Early Clinical Experience With TMVR in Native
Severe MR (N ¼ 115)*
Patient characteristics
Age, yrs 73.8 (39–91)
Female 30/115 (26.1)
STS score 7.5 (1.0–47.7)
NYHA functional class $III 83/101 (82.2)
Ischemic/functional MR 85/114 (74.6)
LVEF <50% 65/86 (75.6)
Valve type and approach
Devices
Tendyne 30/115 (26.1)
Intrepid 27/115 (23.5)
Neovasc Tiara 19/115 (16.2)
CardiAQ-Edwards 13/115 (11.3)
FORTIS† 13/115 (11.3)
HighLife 6/115 (5.2)
Caisson 5/115 (4.3)
MValve 1/115 (1.0)
NCS NaviGate 1/115 (1.0)
Transfemoral approach 7/115 (6.1)
Procedural and 30-day outcomes
Technical success 100/113 (88.4)
Procedural mortality 10/114 (8.8)
LVOT obstruction 1/96 (1.0)
Post-procedural $ moderate MR 1/77 (1.3)
30-day mortality 26/112 (23.2)
Values are weighted mean (range) or n/N (%). *Patient baseline and proceduralcharacteristics are derived from previously presented data. Patients who weretreated but not reported are not included in the analysis. †In late 2015, EdwardsLifesciences stopped the FORTIS program because of valve thrombosis. The valveis not currently available.
Abbreviations as in Tables 1 and 3.
J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2189
the MitraClip device. In fact, no data exist as towhether or not the patients selected for TMVR wereconsidered suboptimal candidates for MitraCliptherapy.
The main clinical characteristics of the patientsundergoing TMVR are summarized in Table 5. Pa-tients who have undergone TVMR were in their mid-70s, and most of them (74%) were male. Most pa-tients (76%) had low left ventricular ejection frac-tions (LVEF), and MR was of ischemic origin in themajority. Comorbidities such as chronic kidney dis-ease and chronic pulmonary obstructive diseasewere among the most frequently reported. Of note,secondary MR was diagnosed in most patients whounderwent TMVR, despite the lack of definite evi-dence supporting a clinical benefit with this clinicalapproach.
Unfortunately, scarce data exist for patient inclu-sion and/or exclusion criteria and patient screening.Although there are no definite data on the number ofpatients screened versus those finally undergoing the
procedure for the different transcatheter valve plat-forms, the screening failure rate at this stage seems tobe high. It will be very important to collect this in-formation in future studies in order to better deter-mine the subset of patients who may potentiallybenefit from this technology.
PROCEDURAL ASPECTS. A total of 115 cases with9 different dedicated transcatheter mitral valveprosthetic devices have been reported to date. Themajority of procedures (94%) were performed using atransapical approach under general anesthesia andfluoroscopic and transesophageal echocardiographicguidance. One device in particular was used exclu-sively in the transfemoral approach (Caisson pros-thesis), whereas another could be implanted usingtransapical or transfemoral approach (CardiAQdevice).
Although these were the very early and/or first-in-human phase experiences with different TMVRdevices, the average technical success (valve suc-cessfully implanted with a normally functioningvalve post-procedure) was high (88%; ranging from75% to 100%). The main technical issues were relatedto: 1) transcatheter valve instability or inappropriatevalve fixation due to incomplete capture of the pos-terior mitral leaflet; 2) issues with the subvalvularmitral apparatus; 3) problems with the hemostasis ofthe transapical access (usually due to myocardialtears); 4) leaflet malfunction following valve im-plantation; and 5) interaction with a previouslyimplanted aortic valve. Of note, the fact that mostcurrent TMVR systems are not fully retrievable led toconversion to open heart surgery and valve explan-tation in most patients experiencing technical issuesduring the TMVR procedure.
LVOT obstruct ion . This life-threatening complica-tion occurred in a single case (<1%) in these initialseries of TMVR. This probably reflects appropriatepatient selection criteria using 3D CT, excluding thosepatients with very small LVOTs that would predictexcessive risk. Also, the fact that several TMVR plat-forms involve capturing the anterior leaflet amongthe mechanisms for valve anchoring might havedecreased the risk of this complication.
Valve per formance : hemodynamic resul ts .Results of valve performance associated with thedifferent transcatheter valve platforms have beenvery good, with mean transvalvular gradientsof #3 mm Hg in all cases and a very low rate (<2%) ofsignificant paravalvular leakage. These resultscompare favorably with those obtained with trans-catheter mitral valve repair systems and are close tothose reported following surgical mitral valve repair

Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2190
and/or replacement. However, the presence of mitralannular calcification has been an exclusion criterionfor all TMVR systems, and there are no data on howthese devices would perform in the setting of severeannular calcification, where paravalvular leakage andanchoring could be issues.
30-day morta l i ty . To date, the average 30-daymortality rate following TMVR has been 23%,ranging from 0% to 53%. Approximately one-half ofthe deaths occurred periprocedurally and weremainly related to unsuccessful TMVR, frequentlyleading to conversion to open-heart surgery. Also,access site management issues were responsible forsome episodes of death in this initial experience,mainly secondary to myocardial tears. The other halfof in-hospital and/or 30-day deaths occurred later on,following the initial periprocedural period. In thesecases, multiorgan failure was the most commonlyreported cause of death. Although procedural com-plications and failure to achieve technical successcontributed to these deaths in many cases, other pa-tients died within the weeks following a successful,uncomplicated TMVR procedure. In these cases,the reasons explaining post-TMVR mortality areprobably multifactorial. First, patients’ comorbid-ities, including noncardiac diseases and frailty issues,might have played a role. Second, the transapicalapproach has been associated with a higher rate ofperiprocedural complications (particularly majorand/or life-threatening bleeding) and mortality in theTAVR field (63). In addition to the negative effects ofthoracotomy in an elderly and frail population, thehigher degree of myocardial injury associated withthe transapical approach may be particularly delete-rious in patients with reduced LVEF pre-procedurally,such as those harboring severe functional MR.Finally, acute abolishment of the volume overloadassociated with severe MR in patients with severelydepressed (<30%) LVEF may have temporary nega-tive effects, including a further reduction in LVEFthat may complicate the post-operative period. This iswell known in the surgical field (64) and should beconsidered when evaluating these patients for TMVR.
LATE OUTCOMES. Intermediate term data for out-comes after TMVR are limited to only 2 platforms(Intrepid and Fortis [Edward Lifescience). There havebeen no reports of structural valve degeneration,valve dislocation requiring reintervention, or new orworsening paravalvular leakage over 6 to 12 monthsof follow-up.
Concerns have arisen regarding the risk of valvethrombosis after TAVR (65). There is, however,
scarce information about the risk of valve throm-bosis after TMVR. The TMVR program with theFortis valve was temporarily halted due to issues ofvalve thrombosis (66). No details about thiscomplication were provided, but 1 of the patients inthe current series had a clinically relevant episodeof valve thrombosis a few weeks after TMVR withthe Fortis valve. One episode of valve thrombosiswas reported following implantation of the Ten-dyne valve. The patient, whose anticoagulationtherapy was subtherapeutic (INR ¼ 1.5), had anincreased mitral gradient at the 30-day follow-upand evidence of leaflet thrombosis on CT imaging.Complete resolution of the thrombus with normal-ization of the prosthetic valve function was docu-mented by echography and CT followingintensification of oral anticoagulation therapy (43).Anticoagulation is recommended for at least thefirst 3 months after surgical mitral valve replace-ment (67,68). While waiting for more data onantithrombotic therapy post-TMVR, anticoagulationtherapy for the first months following the proced-ure should probably be used. Future studies shouldalso determine the risk and efficacy of adding an-tiplatelet therapy in addition to anticoagulation insuch patients.
CONCLUSIONS
TMVR is evolving to become a potentially newalternative for treating patients with severe MR whoare at very high or prohibitive surgical risk. Thecomplexity of the mitral valve apparatus and theheterogeneity of the disease have limited theimplementation of this therapy to date. Several de-vices are under clinical evaluation, and the earlyexperience with more than 100 patients hasdemonstrated the feasibility of TMVR. Presently,multiple TMVR systems are being evaluated inseveral centers in an overall small number of highlyselected patients. Future studies with a much largernumber of patients are needed to provide consistentsafety and efficacy data for each of the TMVR sys-tems. This will determine whether or not TMVRcould become a real alternative for the increasingnumber of patients with severe MR for whom moreaggressive approaches are not suitable.
ADDRESS FOR CORRESPONDENCE: Dr. JosepRodés-Cabau, Quebec Heart and Lung Institute, LavalUniversity, 2725 Chemin Ste-Foy, G1V 4GS QuebecCity, Quebec, Canada. E-mail: [email protected].

J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7 Regueiro et al.M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2 Transcatheter Mitral Valve Replacement
2191
RE F E RENCE S
1. Coffey S, Cairns BJ, Iung B. The modern epide-miology of heart valve disease. Heart 2016;102:75–85.
2. Nkomo VT, Gardin JM, Skelton TN,Gottdiener JS, Scott CG, Enriquez-Sarano M.Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–11.
3. Mirabel M, Iung B, Baron G, et al. What are thecharacteristics of patients with severe, symptom-atic, mitral regurgitation who are denied surgery?Eur Heart J 2007;28:1358–65.
4. Goel SS, Bajaj N, Aggarwal B, et al. Prevalenceand outcomes of unoperated patients with severesymptomatic mitral regurgitation and heart fail-ure: comprehensive analysis to determine thepotential role of MitraClip for this unmet need.J Am Coll Cardiol 2014;63:185–6.
5. Nishimura RA, Vahanian A, Eleid MF, Mack MJ.Mitral valve disease—current management andfuture challenges. Lancet 2016;387:1324–34.
6. Alfieri O, Maisano F, De Bonis M, et al. Thedouble-orifice technique in mitral valve repair: asimple solution for complex problems. J ThoracCardiovasc Surg 2001;122:674–81.
7. Maisano F. Transcatheter mitral valve repairoutcomes after 30,000 treated patients. Paperpresented at: Transcatheter valve therapies (TVT):a multidisciplinary heart team approach; June 18,2016; Chicago, IL.
8. Feldman T, Kar S, Rinaldi M, et al., for theEVEREST investigators. Percutaneous mitral repairwith the MitraClip system: safety and midtermdurability in the initial EVEREST (EndovascularValve Edge-to-Edge REpair Study) cohort. J AmColl Cardiol 2009;54:686–94.
9. Feldman T, Foster E, Glower DD, et al., for theEVEREST II investigators. Percutaneous repair orsurgery for mitral regurgitation. N Engl J Med2011;364:1395–406; erratum N Engl J Med 2011;365:189.
10. Feldman T, Kar S, Elmariah S, et al., for theEVEREST II investigators. Randomized comparisonof percutaneous repair and surgery for mitralregurgitation: 5-year results of EVEREST II. J AmColl Cardiol 2015;66:2844–54.
11. Maisano F, Franzen O, Baldus S, et al. Percu-taneous mitral valve interventions in the realworld: early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomizedpost-approval study of the MitraClip therapy inEurope. J Am Coll Cardiol 2013;62:1052–61.
12. Maisano F, Alfieri O, Banai S, et al. The futureof transcatheter mitral valve interventions:competitive or complementary role of repair vs.replacement? Eur Heart J 2015;36:1651–9.
13. Guerrero M, Dvir D, Himbert D, et al. Trans-catheter mitral valve replacement in native mitralvalve disease with severe mitral annular calcifica-tion: results from the first multicenter globalregistry. J Am Coll Cardiol Intv 2016;9:1361–71.
14. Paradis JM, Del Trigo M, Puri R, Rodés-Cabau J. Transcatheter valve-in-valve and valve-in-ring for treating aortic and mitral surgical
prosthetic dysfunction. J Am Coll Cardiol 2015;66:2019–37.
15. Ribeiro HB, Nombela-Franco L, Muñoz-García AJ, et al. Predictors and impact ofmyocardial injury after transcatheter aortic valvereplacement: a multicenter registry. J Am CollCardiol 2015;66:2075–88.
16. Urena M, Webb JG, Eltchaninoff H, et al. Latecardiac death in patients undergoing transcatheteraortic valve replacement: incidence and predictorsof advanced heart failure and sudden cardiacdeath. J Am Coll Cardiol 2015;65:437–48.
17. Fröhlich GM, Baxter PD, Malkin CJ, et al., forthe National Institute for Cardiovascular OutcomesResearch. Comparative survival after transapical,direct aortic, and subclavian transcatheter aorticvalve implantation (data from the UK TAVI regis-try). Am J Cardiol 2015;116:1555–9.
18. Blanke P, Naoum C, Webb J, et al. Multi-modality imaging in the context of transcathetermitral valve replacement: establishing consensusamong modalities and disciplines. J Am Coll Car-diol Img 2015;8:1191–208.
19. Preston-Maher GL, Torii R, Burriesci G.A technical review of minimally invasive mitralvalve replacements. Cardiovasc Eng Technol 2015;6:174–84.
20. Rosendal C, Hien MD, Bruckner T, Martin EO,Szabo G, Rauch H. Left ventricular outflow tract:intraoperative measurement and changes causedby mitral valve surgery. J Am Soc Echocardiogr2012;25:166–72.
21. Wu Q, Zhang L, Zhu R. Obstruction of leftventricular outflow tract after mechanical mitralvalve replacement. Ann Thorac Surg 2008:1789–91.
22. Blanke P, Naoum C, Dvir D, et al. PredictingLVOT obstruction in transcatheter mitral valveimplantation: concept of the Neo-LVOT. J Am CollCardiol Img 2016 Mar 9 [E-pub ahead of print],http://dx.doi.org/10.1016/j.jcmg.2016.01.005.
23. Bapat V, Pirone F, Kapetanakis S, Rajani R,Niederer S. Factors influencing left ventricularoutflow tract obstruction following a mitral valve-in-valve or valve-in-ring procedure, part 1. Cath-eter Cardiovasc Interv 2015;86:747–60.
24. Delgado V, Tops LF, Schuijf JD, et al. Assess-ment of mitral valve anatomy and geometry withmultislice computed tomography. J Am Coll Car-diol Img 2009;2:556–65.
25. Abdelghani M, Spitzer E, Soliman OI, et al.A simplified and reproducible method to size themitral annulus: implications for transcathetermitral valve replacement. Eur Heart J CardiovascImaging 2016 Jun 2 [E-pub ahead of print], http://dx.doi.org/10.1093/ehjci/jew132.
26. Thériault-Lauzier P, Mylotte D, Dorfmeister M,et al. Quantitative multi-slice computed tomog-raphy assessment of the mitral valvular complexfor transcatheter mitral valve interventions part 1:systematic measurement methodology and inter-observer variability. EuroIntervention 2016;12:1011–20.
27. Blanke P, Dvir D, Cheung A, et al. Mitralannular evaluation with CT in the context oftranscatheter mitral valve replacement. J Am CollCardiol Img 2015;8:612–5.
28. Blanke P, Dvir D, Cheung A, et al. A simplifiedD-shaped model of the mitral annulus to facilitateCT-based sizing before transcatheter mitral valveimplantation. J Cardiovasc Comput Tomogr 2014;8:459–67.
29. Blanke P, Dvir D, Naoum C, et al. Prediction offluoroscopic angulation and coronary sinus loca-tion by CT in the context of transcatheter mitralvalve implantation. J Cardiovasc Comput Tomogr2015;9:183–92.
30. Thériault-Lauzier P, Dorfmeister M, Mylotte D,et al. Quantitative multi-slice computed tomog-raphy assessment of the mitral valvular complexfor transcatheter mitral valve interventions part 2:geometrical measurements in patients with func-tional mitral regurgitation. EuroIntervention 2016;12:e1021–30.
31. Natarajan N, Patel P, Bartel T, et al. Peri-procedural imaging for transcatheter mitral valvereplacement. Cardiovasc Diagn Ther 2016;6:144–59.
32. Pibarot P, Dumesnil JG. Prosthetic heartvalves: selection of the optimal prosthesis andlong-term management. Circulation 2009;119:1034–48.
33. Sondergaard L, Ussia GP, Dumonteil N,Quadri A. The CardiAQ transcatheter mitral valveimplantation system. EuroIntervention 2015;11Suppl W:W76–7.
34. Søndergaard L, De Backer O, Franzen OW,et al. First-in-human case of transfemoral CardiAQmitral valve implantation. Circ Cardiovasc Interv2015;8:e002135.
35. Ussia GP, Quadri A, Cammalleri V, et al.Percutaneous transfemoral-transseptal implanta-tion of a second-generation CardiAQ mitral valvebioprosthesis: first procedure description and 30-day follow-up. EuroIntervention 2016;11:1126–51.
36. Sondergaard L. CardiAQ-Edwards TMVR. Pa-per presented at: PCR London Valves; September19, 2016; London, United Kingdom.
37. Cheung A. Transcatheter mitral valvereplacement Neovasc Tiara: design and clinicaltrial updates. Paper presented at: Transcathetercardiovascular therapeutics (TCT); October 31,2016; Washington, DC.
38. Cheung A, Webb J, Verheye S, et al. Short-term results of transapical transcatheter mitralvalve implantation for mitral regurgitation. J AmColl Cardiol 2014;64:1814–9.
39. Verheye S, Cheung A, Leon M, Banai S. TheTiara transcatheter mitral valve implantation sys-tem. EuroIntervention 2015;11 Suppl W:W71–2.
40. Cheung A. Neovasc TIARA. Paper presentedat: PCR London Valves; September 19, 2016;London, UK.
41. Quarto C, Davies S, Duncan A, et al. Trans-catheter mitral valve implantation: 30-dayoutcome of first-in-man experience with an

Regueiro et al. J A C C V O L . 6 9 , N O . 1 7 , 2 0 1 7
Transcatheter Mitral Valve Replacement M A Y 2 , 2 0 1 7 : 2 1 7 5 – 9 2
2192
apically tethered device. Innovations (Phila) 2016;11:174–8.
42. Perpetua EM, Reisman M. The Tendynetranscatheter mitral valve implantation system.EuroIntervention 2015;11 Suppl W:W78–9.
43. Muller D, Farivar RS, Jansz P, et al., for theTendyne Global Feasibility Trial investigators.Transcathetermitral valve replacement for patientswith symptomatic mitral regurgitation: a globalfeasibility trial. J Am Coll Cardiol 2017;69:381–91.
44. Meredith I, Bapat V, Morriss J, McLean M,Prendergast B. Intrepid transcatheter mitral valvereplacement system: technical and productdescription. EuroIntervention 2016;12 Suppl Y:Y78–80.
45. Bapat V. Intrepid Taped Case. Paper presentedat: Transcatheter Valve Therapies (TVT): a multi-disciplinary heart team approach; June 16, 2016;Chicago, IL.
46. Meredith IT. Medtronic Intrepid TMVR. Paperpresented at: PCR London Valves. September 19,2016; London, UK.
47. Bapat V. Intrepid design and clinical trial up-date. Paper presented at: Transcatheter Cardio-vascular Therapeutics (TCT); October 29, 2016;Washington, DC.
48. Williams M. The Caisson transcatheter mitralvalve replacement system. Paper presented at: PCRLondon Valves; September 18, 2016; London, UK.
49. Williams M. Caisson: design and clinical trialupdates. Paper presented at: Transcatheter Car-diovascular Therapeutics (TCT); October 31, 2016;Washington, DC.
50. Lange R, Piazza N. The HighLife transcathetermitral valve implantation system. Euro-Intervention 2015;11 Suppl W:W82–3.
51. Lange R. A two-component, self-centeringTMV system. Paper presented at: TranscatheterCardiovascular Therapeutics (TCT); October 31,2016; Washington, DC. Available at: https://www.tctmd.com/slide/highlife-design-and-clinical-trial-updates. Accessed March 6, 2017.
52. Buchbinder M. MValve: design highlightsand clinical update. Paper presented at:Transcatheter Valve Therapies (TVT): a
multidisciplinary heart team approach; June 16,2016; Chicago, IL.
53. Buchbinder M. M-Dock: design and clinical trialupdate. Paper presented at: TranscatheterCardiovascular Therapeutics (TCT); October 31,2016; Washington, DC. Available at: https://www.tctmd.com/slide/m-dock-design-and-clinical-trial-updates. Accessed March 6, 2017.
54. Navia JL. My choice for percutaneous mitralvalve replacement. Paper presented at: AmericanAssociation for Thoracic Surgery Annual Meeting;April 25, 2015; Baltimore, MD. Available at: http://webcast.aats.org/2015/Detail.php?d¼Saturday&s¼1.Accessed March 6, 2017.
55. NaviGate Cardiac Structures, Inc. First Navigatepatient at 8 months shows excellent mitral valvefunction and has returned to work. Navigate CardiacStructures, Inc. June 23, 2016. Available at: http://www.navigatecsi.com/announcement/first-navi-patient-at-8-months-shows-excellent-mitral-valve-function-and-has-returned-to-work/. AccessedMarch 1, 2017.
56. Abdelghani M, Onuma Y, Zeng Y, et al. TheSino Medical AccuFit transcatheter mitral valveimplantation system. EuroIntervention 2015;11Suppl W:W84–5.
57. Serruys PW. AccuFit transapical mitral valvereplacement system: a technical update. Paperpresented at: EuroPCR; May 19, 2016; Paris,France.
58. Maisano F. Valtech TMVR: design highlightsand clinical update. Presented at: TranscatheterValve Therapies (TVT): a multidisciplinary heartteam approach; June 16, 2016; Chicago, IL.
59. Granada JF. Transcatheter mitral valve thera-pies: new rings, anchors and techniques. Cephea.Paper presented at: EuroPCR; May 21, 2015; Paris,France.
60. Leon MB. The Cephea transcatheter mitralvalve replacement system. Paper presented at:PCR London; September 18, 2016; London, UK.
61. Denti P. Saturn Project: a novel approach totranscatheter replacement. Paper presented at:Mitral Valve Meeting (MVM); February 7, 2017;Zurich, Switzerland.
62. Cheung A. St. Jude TMVR: design develop-ment update. Paper presented at: TranscatheterCardiovascular Therapeutics (TCT); October 31,2016; Washington, DC.
63. Biancari F, Rosato S, D’Errigo P, et al., for theOBSERVANT research group. Immediate and in-termediate outcome after transapical versustransfemoral transcatheter aortic valvereplacement. Am J Cardiol 2016;117:245–51.
64. Gaasch WH, Meyer TE. Left ventricularresponse to mitral regurgitation. Implications formanagement. Circulation 2008;118:2298–303.
65. Hansson NC, Grove EL, Andersen HR, et al.Transcatheter aortic valve thrombosis, incidence,predisposing factors, and clinical implications.J Am Coll Cardiol 2016;8:2059–69.
66. Edwards Life Sciences, Corp. Edwards pausesenrollment in early stage mitral program. EdwardsLifesciences Corp. May 19, 2016. Available at: http://www.edwards.com/fr/newsroom/Pages/ShowPR.aspx?PageGuid¼%7B61d40c10-d690-45fa-b541-ab1f4806b975%7D. Accessed March 1, 2017.
67. Nishimura RA, Otto CM, Bonow RO, et al. 2014AHA/ACC guideline for the management of pa-tients with valvular heart disease: a report of theAmerican College of Cardiology/American HeartAssociation Task Force on Practice Guidelines.J Am Coll Cardiol 2014;63:e57–185.
68. Vahanian A, Alfieri O, et al., for the taskforcemembers. Guidelines on the management ofvalvular heart disease (version 2012): the jointtask force on the management of valvular heartdisease of the European Society of Cardiology(ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2012;33:2451–96.
69. De Backer O, Piazza N, Banai S, et al. Percu-taneous transcatheter mitral valve replacement:an overview of devices in preclinical and earlyclinical evaluation. Circ Cardiovasc Interv 2014;7:400–9.
KEY WORDS mitral regurgitation, mitralvalve surgery, transcatheter cardiactherapeutics