Embed Size (px)
Citation preview

© 2014 Direct One Communications, Inc. All rights reserved. 1
One Size Does Not Fit All:Personalized Treatment of Patients with Epilepsy
Vikram R. Rao, MD, PhD
University of California, San Francisco, Epilepsy Center, San Francisco, California
A REPORT FROM THE 67TH ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY (AES 2013)

© 2014 Direct One Communications, Inc. All rights reserved. 2
Personalized Treatment in Epilepsy
Epilepsy: enduring tendency for recurrent seizures
4th most common neurological disorder; lifetime prevalence is 1 in 26 individuals.
Evidence for superiority of one antiepileptic drug (AED) over another is often lacking.
AEDs are chosen based on patient-specific factors:» Genetic information» Physical characteristics and comorbid conditions» Concurrent medications
Individualizing treatment may maximize tolerability, adherence, and efficacy
Chang BS, Lowenstein DH. N Engl J Med. 2003;349:1257; Fisher RS et al. Epilepsia. 2005;46:470; Institute of Medicine, 2012; Glauser T et al. Epilepsia. 2013;54:551; French JA, Gazzola DM. Continuum. 2013;19:643

© 2014 Direct One Communications, Inc. All rights reserved. 3
Pharmacogenomics in Epilepsy

© 2014 Direct One Communications, Inc. All rights reserved. 4
Pharmacogenomics:Overview
Pharmacogenomics: use of biomarkers related to a patient’s genome to guide drug therapy
Chan A et al. Ann Neurol. 2011;70:684

© 2014 Direct One Communications, Inc. All rights reserved. 5
Pharmacogenomics:To Avoid Adverse Drug Reactions
HLA-B*1502 allele predicts carbamazepine (CBZ)-induced Stevens-Johnson syndrome in patients of Han Chinese and South Asian ancestry; pre-treatment testing recommended in these patients.
HLA-A*3101 allele may be a marker of CBZ-induced drug reactions in other patient populations.
Avoid sodium channel blockers, such as lamotrigine (LTG), in syndromes with SCN1A mutation (eg, Dravet syndrome).
Research is ongoing for markers of valproate (VPA)-induced weight gain and vigabatrin retinopathy.
Chung WH et al. Nature. 2004;428:486; McCormack M et al. N Engl J Med. 2011;364:1134; Ozeki T et al. Hum Mol Genet. 2011;20:1034; Belcastro V et al. Epilepsy Res. 2013;107:1; Kinirons P et al. Epilepsy Res. 2006;70:144

© 2014 Direct One Communications, Inc. All rights reserved. 6
Pharmacogenomics:To Predict Favorable Treatment Responses
Some previously medically refractory patients can achieve seizure freedom with levetiracetam (LEV).» Genetic basis of these “dramatic responders” is
elusive.
Functional variants of cytochrome P-450 enzymes affect phenytoin (PHT) metabolism.
SCN1A polymorphisms may influence maximum dose and serum levels of CBZ and PHT.
A patient’s genetic profile may eventually be used to determine optimal medical therapy, but ethical, financial, and legal issues abound.
Nicolson A et al. Neurology. 2004;63:568; Lynch JM et al. Epilepsy Res. 2009;83:44; Dibbens et al. Epilepsy Res. 2012;101:277; Aynacioglu AS et al. Br J Clin Pharmacol. 1999;48:409; Chaudhry AS et al. J Pharmacol Exp Ther. 2010;332:599; Tate SK et al. Proc Natl Acad Sci U S A. 2005;102:5507; Tate SK et al. Pharmacogenet Genomics. 2006;16:721; Zimprich F et al. Epilepsia. 2008;49:1108

© 2014 Direct One Communications, Inc. All rights reserved. 7
Personalizing Drug Delivery

© 2014 Direct One Communications, Inc. All rights reserved. 8
Personalizing Drug Delivery:Formulation Extended-release (ER) AED formulations allow
more gradual systemic absorption vs immediate-release
ER formulations offer several advantages:» Less variability in serum drug levels» Lower incidence of peak-dose toxicity» Increased patient convenience (may favor
compliance)
Benefit directly demonstrated for LTG vs ER CBZ
Potential disadvantages of ER formulations:» Higher cost» High peak serum levels may be desired when
treating seizures with predictable diurnal variation» Shorter “forgiveness period”
Bialer M. CNS Drugs. 2007;21:765; Canger R et al. Acta Neurol Scand. 1990;82:9; Brodie MJ et al. Epilepsy Res. 1999;37:81; Saetre E et al. Epilepsia. 2007;48:1292; Guilhoto LM et al. Epilepsy Behav. 2011;20:334

© 2014 Direct One Communications, Inc. All rights reserved. 9
Rectal diazepam in solution leads to a more rapid increase in serum drug levels than rectal suppositories (basis for Diastat®)
RAMPART study: Intramuscular midazolam is superior to intravenous (IV) lorazepam for pre-hospital treatment of status epilepticus
Higher rate of seizure freedom on arrival to hospital:» Lower rates of hospital/ICU admission
» Issues: difficulty obtaining IV access; shorter half-life of lorazepam out of refrigeration
Sublingual lorazepam associated with higher rates of treatment failure compared with rectal diazepam
Personalizing Drug Delivery:Route of Administration
Knudsen FU. Acta Paediatr Scand. 1977;66:563; Kriel RL et al. Pediatr Neurol. 1999;20:282; Silbergleit R et al. N Engl J Med. 2012;366:591; Silbergleit R et al. Epilepsia. 2013;54(suppl 6):74; Malu CK et al. J Child Neurol. 2013

© 2014 Direct One Communications, Inc. All rights reserved. 10
Setting (eg, pre-hospital vs hospital; household vs ambulance)
Clinical urgency (eg, status epilepticus vs self-limited seizure)
Ease of obtaining IV access Logistical considerations of particular
medications and formulations (eg, availability, storage requirements, cost)
Regulatory approval status and extent of data supporting clinical efficacy
Personalizing Drug Delivery:Dosing Considerations

© 2014 Direct One Communications, Inc. All rights reserved. 11
Cutaneous Drug Reactions

© 2014 Direct One Communications, Inc. All rights reserved. 12
Cutaneous Drug Reactions:Epidemiology
Among treatment-related side effects underlying AED intolerance, rash is one of the most common.
Adverse cutaneous drug reactions (ACDRs) affect 2% of hospitalized patients.» With AEDs, 15% of patients will develop a rash
within 4 weeks of drug initiation.
Risk factors for ACDRs:» Age» Number of comorbid conditions» Polypharmacy» Immunosuppression» Female gender (?)
Chung S et al. J Br Epilepsy Assoc. 2007;16:296; Arndt KA, Jick H. JAMA. 1976;235:918; Porter J, Jick H. JAMA. 1977;237:879; Blaszczyk B et al. Pharmacol Rep. 2013;65:399; Liao PJ et al. Int J Clin Pract. 2013;67:576; Todd G. Dermatol Clin. 2006;24:459

© 2014 Direct One Communications, Inc. All rights reserved. 13
Broad spectrum of severity: » Mild, diffuse, morbiliform rash life-
threatening multisystem illness
Key factors for initial evaluation:» Need to determine chronicity, distribution, pattern,
organization, morphology, probable anatomic depth, and mucosal membrane involvement
Reactions that are likely immunologic:» Activated T lymphocytes and macrophages can be
found in areas of damaged skin.
Cutaneous Drug Reactions:Clinical Manifestations
Caproni M et al. Br J Dermatol. 2006;154:319

© 2014 Direct One Communications, Inc. All rights reserved. 14
Drug reaction with eosinophilia and systemic symptoms (DRESS): » Morbiliform cutaneous eruption involving the face,
trunk, and limbs, along with fever, lymphadenopathy, hematologic abnormalities, and organ dysfunction (especially the liver)
» Mortality ~ 10%
Aromatic AEDs, particularly CBZ, and sulfonamides are the most common inciting agents.
Typically develops 2–6 weeks after treatment initiation
Several formal diagnostic criteria existHusain Z, et al. J Am Acad Dermatol. 2013;68:693; Kardaun SH et al. Br J Dermatol. 2013;169:1071; Bocquet H et al. Sem Cutan Med Surg. 1996;15:250; Kelly JP et al. J Clin Epidemiol. 1995;48:1099
Cutaneous Drug Reactions:DRESS

© 2014 Direct One Communications, Inc. All rights reserved. 15
Stevens-Johnson syndrome (SJS): less than 10% body surface area (BSA) skin detachment
Toxic epidermal necrolysis (TEN): differs from SJS only in severity; greater than 30% of BSA involvement, higher mortality
Usually 1–3 weeks after drug initiation, prodromal phase of flu-like symptoms
PHT, PHB, CBZ, and LTG are most often associated with SJS/TEN; estimated incidence: 1–10/10,000 new users; case reports exist of other AEDs causing SJS/TEN
Tartarone A, Lerose R. Ther Drug Monit. 2010;32:669; Mockenhaupt M et al. Neurology. 2005;64:1134; Zou LP et al. Seizure. 2012;21:823; Duong TA et al. JAMA Dermatol. 2013;149:113; Naveen K et al. Int J Crit Illness Injury Sci. 2012;2:44
Cutaneous Drug Reactions:SJS/TEN

© 2014 Direct One Communications, Inc. All rights reserved. 16
Prompt withdrawal of the offending agent and initiation of aggressive supportive care remain the mainstays of treatment
Topical corticosteroid therapy is common. Systemic corticosteroids and other
immunosuppressive agents are controversial. Intensive care or burn unit needed for
management of systemic complications and to optimize fluid status, nutrition, analgesia, and infection control
Cutaneous Drug Reactions:Treatment
Husain Z et al. J Am Acad Dermatol. 2013;68:709; Tas S, Simonart T. Dermatology. 2003;206:353

© 2014 Direct One Communications, Inc. All rights reserved. 17
Epilepsy in Women

© 2014 Direct One Communications, Inc. All rights reserved. 18
Epilepsy in Women:Catamenial Epilepsy
Estrogen: proconvulsant Progesterone: neuroinhibitory One-third of women with focal epilepsy
demonstrate a catamenial pattern.» Seizures occur at times during menstrual cycle
when estrogen level exceeds progesterone level or when levels of either hormone are changing rapidly.
Cyclic progesterone therapy may be beneficial for a subset of women with catamenial epilepsy.» Less robust evidence for acetazolamide and
clobazamPennell PB. Continuum. 2013;19:697; Herzog AG et al. Neurology. 2012;78:1959; Harden CL, Pennell PB. Lancet Neurol. 2013;12:72

© 2014 Direct One Communications, Inc. All rights reserved. 19
Enzyme-inducing AEDs lead to increased clearance—and thus decreased contraceptive efficacy—of sex hormones.
Estrogen-containing contraceptives induce hepatic enzymes and may decrease the serum concentration of certain AEDs such as LTG.
Best options for women with epilepsy are long-acting reversible contraceptives:» Progestin implants
» Intrauterine devices (IUDs)
Epilepsy in Women:Contraception
Davis AR et al. Epilepsia. 2011;52:243; Reimers A et al. Epilepsia. 2005;46:1414.

© 2014 Direct One Communications, Inc. All rights reserved. 20
Epilepsy in Women: Risk of Congenital Malformations
~3.5% of women in their reproductive years may be taking an AED for epilepsy or other indications (eg, headache, pain, or a mood disorder).
AED use increases the risk of major congenital malformations to 3%–9%, about two- to threefold higher than the risk in the general population.
Fetal exposure to valproate has been associated with dose-dependent impairment in cognitive abilities during childhood.
LTG is often considered the drug of choice during pregnancy.Pennell PB. Continuum. 2013;19:697; Meador KJ et al. Neurology. 2008;71:1109; Harden CL et al.
Neurology. 2009;73:133; Holmes LB et al. N Engl J Med. 2001;344:1132; Tomson T, Battino D. Lancet Neurol. 2012;11:803; Meador KJ et al. Lancet Neurol. 2013;12:244

© 2014 Direct One Communications, Inc. All rights reserved. 21
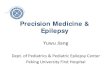
Rates of major congenital malformations at one year after birth in relation to exposure to AED monotherapy
Epilepsy in Women: Risk of Congenital Malformations
Tomson T, Battino D. Lancet Neurol. 2012;11:803; Tomson T et al. Lancet Neurol. 2011;10:609

© 2014 Direct One Communications, Inc. All rights reserved. 22
20%–33% of women with epilepsy experience an increase in seizure frequency during pregnancy.
Optimize seizure control before pregnancy; seizure freedom for at least 9 months prior to pregnancy is associated with an 84%–92% chance of remaining seizure-free during pregnancy.
Avoid polytherapy if possible Monitor therapeutic drug levels, especially of
LTG and LEV, monthly. Folic acid supplementation, 0.4–5.0 mg/d
Epilepsy in Women: Managing Epilepsy During Pregnancy
Anon. Neurology. 2006;66:354; Harden CL et al. Neurology. 2009;73:126; Pennell PB et al. Neurology. 2008;70:2130; Pennell PB, Hovinga CA. Int Rev Neurobiol. 2008;83:227; Harden CL et al. Neurology. 2009;73:142; Thomas SV. Neurol India. 2011;59:59

© 2014 Direct One Communications, Inc. All rights reserved. 23
Epilepsy in Patients with HIV

© 2014 Direct One Communications, Inc. All rights reserved. 24
Multiple considerations in the personalized treatment of epilepsy in patients infected with human immunodeficiency virusARV = antiretroviral therapyAED = antiepileptic drug
Epilepsy and HIV: Treatment Issues in Patients with HIV
From a presentation made by Gretchen L. Birbeck, MD, PhD, at AES 2013

© 2014 Direct One Communications, Inc. All rights reserved. 25
Epilepsy and HIV: Drug Interactions
Concurrent use of AEDs with antiretroviral medications (ARVs) is common, and the potential interactions between these drug types are extensive, for example:» Avoid saquinavir in patients on potentially
arrhythmogenic AEDs, such as ezogabine or lacosamide
» Rilpivirine and etravirine are contraindicated with CBZ, oxcarbazepine, PHB, and PHT
» Avoid enzyme-inducing AEDs in patients taking protease inhibitors or non-nucleoside reverse transcriptase inhibitors
» Most benzodiazepines are contraindicated with ARVs due to the risk of prolonged sedation.
AED/ARV interactions have clinical implications for disease progression and emergence of ARV resistance.
Birbeck GL et al. Neurology. 2012;78:139; Siddiqi O, Birbeck GL. Curr Treat Options Neurol. 2013;15:529

© 2014 Direct One Communications, Inc. All rights reserved. 26
Treatment with ARVs is recommended for all HIV-positive patients, so potential drug-drug interactions should be anticipated before starting AEDs in an HIV-positive patient
The AED of choice in HIV-positive patients is LEV, due to its broad-spectrum activity, ease of use, minimal drug interactions, and favorable side-effect profile.» Alternatives: pregabalin, gabapentin, lacosamide
» Valproate is also favorable because it will not induce ARV metabolism, but its side-effect profile may be somewhat worse than that of other therapeutic options.
Siddiqi O, Birbeck GL. Curr Treat Options Neurol. 2013;15:529
Epilepsy and HIV: Management of Epilepsy