Embed Size (px)
Citation preview

© 2009
On the CUSP: STOP BSIOn the CUSP: STOP BSIThe Science of Improving Patient The Science of Improving Patient
SafetySafety

© 2009
Learning ObjectivesLearning Objectives
• To understand that every system is designed to achieve the results it gets
• To know the basic principles of safe design of both technical and teamwork
• To understand how teams make wise decisions


© 2009
The Problem is LargeThe Problem is Large
• In U.S. Healthcare system
– 7% of patients suffer a medication error
– Every patients admitted to an ICU suffer adverse
event
– 44,000- 98,000 deaths
– Nearly 100,000 deaths from HAI
– Approximately 30,000 deaths from CLABSI
– $50 billion in total costs
• Similar results in UK and AustraliaKohn To err is human

© 2009
10.5Alcohol dependence
22.8Hip fracture
40.7Urinary tract infection
45.2Headaches
45.4Diabetes mellitus
48.6Hyperlipidemia
53.0Benign prostatic hyperplasia
53.5Asthma
53.9Colorectal cancer
57.2Orthopedic conditions
57.7Depression
64.7Hypertension
68.0Coronary artery disease
68.5Low back pain
Percentage of Recommended Care Received Condition
McGlynn et al, NEJM 2003; 348(26):2635-2645
RAND Study Confirms Continued RAND Study Confirms Continued Quality Gap Quality Gap

© 2009
How Can This Happen?How Can This Happen?
Need to view the delivery of healthcare as a science

© 2009
How Can We Improve?How Can We Improve?Understand the Science of SafetyUnderstand the Science of Safety
• Every system is perfectly designed to achieve the results it gets
• Understand principles of safe design – standardize, create checklists, learn when things go wrong
• Recognize these principles apply to technical and team work
• Teams make wise decision when there is diverse and independent input
Caregivers are not to blameCaregivers are not to blame

© 2009
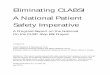
SystemSystem FailureFailure LeadingLeading toto ThisThis ErrorError
Catheter pulled withPatient sitting
Communication betweenresident and nurse
Lack of protocol For catheter removal
Inadequate trainingand supervision
Pronovost Annals IM 2004; Reason
Patient suffers
Venous air embolism

© 2009
System Factors Impact System Factors Impact SafetySafety
HospitalHospital
Departmental FactorsDepartmental Factors
Work EnvironmentWork Environment
Team FactorsTeam Factors
Individual ProviderIndividual Provider
Task FactorsTask Factors
Patient CharacteristicsPatient Characteristics
InstitutionInstitutionalal
Adopted from VincentAdopted from Vincent


© 2009
Evidence Regarding the Impact of Evidence Regarding the Impact of ICU Organization on PerformanceICU Organization on Performance
• Physicians
• Nurses
• Pharmacists
Pronovost JAMA 1999, 2002; Pronovost ECP 2001

© 2009
Aviation Accidents Aviation Accidents per Million Departuresper Million Departures

© 2009
Systems Systems
• Every system is designed to achieve the results it gets
• To improve performance we need to change systems
• Start with pilot test one patient, one day, one physician, one room

© 2009
Principles of Safe DesignPrinciples of Safe Design
• Standardize – Eliminate steps if possible
• Create independent checks
• Learn when things go wrong– What happened– Why– What did you do to reduce risk– How do you know it worked

© 2009
StandardizeStandardize

© 2009
Line Cart Contents – 4 Line Cart Contents – 4 DrawersDrawers

© 2009
Eliminate StepsEliminate Steps

© 2009
Create Independent Create Independent ChecksChecks

© 2009
2 Year Results from 103 2 Year Results from 103 ICUsICUs
Time period Median CRBSI rate Incidence rate ratio
Baseline 2.7 1
Peri intervention 1.6 0.76
0-3 months 0 0.62
4-6 months 0 0.56
7-9 months 0 0.47
10-12 months 0 0.42
13-15 months 0 0.37
16-18 months 0 0.34
Pronovost NEJM 2006

© 2009
Principles of Safe Design Principles of Safe Design Apply to Technical and Apply to Technical and
TeamworkTeamwork

© 2009
Basic Components and Process of Basic Components and Process of CommunicationCommunication
Elizabeth Dayton, Joint Commission Journal, Jan. 2007


© 2009
% o
f res
pond
ents
repo
rting
abo
ve a
dequ
ate
team
work
ICUSRS Data
ICU Physicians and ICU RN ICU Physicians and ICU RN CollaborationCollaboration

© 2009
Teamwork ToolsTeamwork Tools
• Daily goals
• AM briefing
• Shadowing

© 2009
Teams Make Wise Decisions When Teams Make Wise Decisions When There is Diverse and Independent There is Diverse and Independent
InputInput
• Wisdom of Crowds
• Alternate between convergent and divergent thinking– Get from OR to balcony


© 2009
Don’t Play Man DownDon’t Play Man Down
When you feel something say somethingWhen you feel something say something

© 2009
Action ItemsAction Items
• Pick one area and reflect on the systems that predict performance– Walk and observe the process
• Work to standardize one process such as central line cart
• Pilot test it
• Ensure all staff know the science for improving patient safety


© 2009
ReferencesReferences
• Berwick DM. A primer on leading the improvement of systems. BMJ 1996;132:619-22.
• Langley G, Nolan K. The improvement guide: a practical approach to enhancing organizational performance. Hoboken, NJ: Jossey-Bass Publishers 1996.
• Needham DM, Thompson DM, et al. A system factors analysis of airway events from the Intensive Care Unit Safety Reporting System (ICUSRS). Crit Care Med 2004;32:2227-33.
• Pronovost PJ, Wu Aw, et al. Acute decompensation after removing a central line: practical approaches to increasing safety in the intensive care unit. Ann Int Med 2004;140(12):1025-1033.
• Pronovost PJ, Angus DC, et al. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA 2002;288(17):2151-2162.
• Reason J. Managing the risks of organizational accidents. Burlington, VT: Ashgate Publishing Company, 2000.