Embed Size (px)
Citation preview

1
STROKE AND CONSTRAINT-INDUCED MOVEMENT THERAPY: USE OF ESHKOL-WACHMAN MOVEMENT NOTATION TO EXAMINE QUALITY OF MOVEMENT
By
YI-PO CHIU
A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT
OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY
UNIVERSITY OF FLORIDA
2007

2
© 2007 Yi-Po Chiu

3
To my family, mentors, and friends.
4
ACKNOWLEDGMENTS
When I look back over the past five years, I am extremely amazed and grateful that on the
road of pursuing my doctoral degree at University of Florida, there have been so many people
that have supported and encouraged me. The care and love that I have received from the
following people have not only helped me to reach my goals, but have also made me a better
person. First, I acknowledge my family. My parents have financially and spiritually supported
my graduate studies from day one. Although the whole study process took much longer than
they expected, my family, including my two sisters, their husbands and my cutest nephew Sean,
have strong faith in me.
Second, I would like to express my greatest gratitude to my mentors. Dr. Kathye Light is
an extraordinary mentor for my master and doctoral study at the University of Florida. During
my eight years at UF, she has always supported my research direction.. I truly admire her
knowledge and understanding of cultural differences. She has shown me how to become a great
mentor, educator and scientist for my future career in rehabilitation science. I will always miss
our beneficial discussions about science and life. Dr. Philip Teitelbaum and Osnat Teitelbaum
have been two important persons in my doctoral study. Dr. Teitelbaum is the most
knowledgeable and distinguished scholar I have ever met. Because of their kindness and
acceptance, I am able to experience the powerfulness of the Eshkol-Wachman Movement
Notation. Their unconditional support and teaching have deeply touched my heart. I am
thankful they don’t treat education as a trading business, or else I could never repay them for
their numerous time spent on me. They also shared with me their invaluable Jewish culture
during several holiday events. The honor is always mine to study with them. Dr. Craig Velozo
has been a role model to me. He has taught me how cautiously we should deal with scientific
data. Our previous collaboration with Rasch has shown me the essence of teamwork. His
5
constructive suggestions and feedback always help me to better myself. Dr. Andrea Behrman
has been supportive during my study. I thank her for her continuing support and guidance.
Without the support and assistance from my fellow graduate students, colleagues and
friends, I would not be able to smoothly finish my study. I would like to thank the people in the
stroke laboratories, including Stacy, Sandy, Dr. Lorie Richards, Matt, Tara, Vicky, Fran, Sarah,
and all volunteers for their assistance in my study. Stacy has been helping me with my writing
since day one of my study. I truly appreciate how she treats me as her family. The most
precious thing is that she opens her arms and heart to a foreigner like me. The two-week stay at
her and Candy’s home at Columbia, SC meant so much to me, not only giving me a homey
environment but also a booster shot on my dissertation writing. Being able to visit Stacy’s
family during the vacation of Independence Day in the past also tremendously alleviated my
homesickness. Sandy is my wonderful American mother. I truly appreciate her care, assistance,
encouragement and kindness. I also acknowledge the following people. They have been my
wonderful friends that have assisted me in many different ways. They are Robert, Shin-Yi, Pey-
Shan, Tiffany, Tseng-Tien, Rick and Stephanie, Zoe and Kang-Uei, Kai-Jen and Tzu-Yi, Kevin
and Caley, Andrea, Illy, Ruud’s family, Stacy’s family, Matt’s family and Sandy’s family.
Robert has been a supportive friend for the past two years. He has shown me different aspects of
life, such as humanity, politics, history and nature. I have learned a lot from him. Shin-Yi and
Pey-Shan have been my loyal statistics consultants for my study. Tiffany is my wonderful gal
and best jogging partner. I miss the time we spent together. Rick and Stephanie allowed me to
help in their kitchen, so I was able to experience the reality of restaurant business. Kevin and
Caley, Zoe and Kang-Uei, and Kai-Jen and Tzu-Yi are the three couples of friends that have
been provided valuable supports and assistance. When I feel stressful and need a place to retreat,
6
the doors of their homes are always open for me. I really appreciate their wonderful friendship
and hospitality. The last but not the least appreciation is given to my two cats: Latte and
Mimosa. Because of their company, my time at Gainesville can be more joyful.
7
TABLE OF CONTENTS page
ACKNOWLEDGMENTS ...............................................................................................................4
LIST OF TABLES.........................................................................................................................10
LIST OF FIGURES .......................................................................................................................11
ABSTRACT...................................................................................................................................12
CHAPTER
1 INTRODUCTION ..................................................................................................................14
Background and Significance .................................................................................................14 Movement Disorders in Stroke........................................................................................14 Current Methodology of Movement Analysis.................................................................17 Quality of Movement in Constraint-Induced Movement Therapy..................................21 Definition of Quality of Movement Used for People Post-Stroke ..................................23 Generalized Motor Program Theory: The Research Framework ....................................25 A Comprehensive Approach of Movement Analysis: Using Eshkol-Wachman
Movement Notation .....................................................................................................26 Research Aims and Hypotheses..............................................................................................29
Experiment I ....................................................................................................................30 Experiment II...................................................................................................................30 Experiment III .................................................................................................................31
Summary.................................................................................................................................32
2 DEVELOPMENT AND RELIABILITY OF THE ESSENTIAL MOVEMENT COMPONENT EVALUATION FORM USING ESHKOL-WACHMAN MOVEMENT NOTATION............................................................................................................................35
Introduction.............................................................................................................................35 Methods ..................................................................................................................................37
Development of The Essential-Movement Component Evaluation Form Using EWMN.........................................................................................................................37
“Lift Basket” task .....................................................................................................38 Eshkol-Wachman Movement Notation....................................................................39 Participants ...............................................................................................................40 Essential-Movement Component Evaluation form ..................................................40
Intra-Rater and Inter-Rater Reliability of The EMCE Form...........................................42 Participants ...............................................................................................................42 Procedure..................................................................................................................44
Data Analysis..........................................................................................................................45 Results.....................................................................................................................................47
Intra-Rater Reliability......................................................................................................47
8
Inter-Rater Reliability......................................................................................................47 Discussion...............................................................................................................................48
Rater Reliability of The EMCE Form .............................................................................48 Limitations.......................................................................................................................50
Conclusions.............................................................................................................................51
3 ASSESSING MOVEMENT QUALITY AFTER STROKE..................................................59
Introduction.............................................................................................................................59 Method....................................................................................................................................61
Participants ......................................................................................................................61 Procedure.........................................................................................................................63
Data Analysis..........................................................................................................................66 Results.....................................................................................................................................66 Discussion...............................................................................................................................67 Conclusions.............................................................................................................................70
4 EFFECTS OF CONSTRAINT-INDUCED MOVEMENT THERAPY ON QUALITY OF MOVEMENT POST-STROKE .......................................................................................74
Introduction.............................................................................................................................74 Methods ..................................................................................................................................75
Participants ......................................................................................................................75 Procedure.........................................................................................................................77
“Lift Basket” task .....................................................................................................78 Essential-Movement Component Evaluation form ..................................................79
Data Analysis...................................................................................................................80 Results.....................................................................................................................................81 Discussion...............................................................................................................................82
Essential-Movement Component ....................................................................................82 Compensatory Movement ...............................................................................................84 Limitation ........................................................................................................................87
Conclusions.............................................................................................................................88
5 GENERAL SUMMARY AND CONCLUSIONS .................................................................94
Overview.................................................................................................................................94 Experiment I Summary...........................................................................................................94 Experiment II Summary .........................................................................................................96 Experiment III Summary ......................................................................................................100 General Conclusions.............................................................................................................103
APPENDIX
A PILOT DATA.......................................................................................................................106
Pilot Study 1 .........................................................................................................................106 Purpose ..........................................................................................................................106
9
Aim:...............................................................................................................................106 Participants ....................................................................................................................106 Method/Data Analysis ...................................................................................................106 Results and Conclusion .................................................................................................107
Pilot Study 2 .........................................................................................................................107 Purpose ..........................................................................................................................107 Participants ....................................................................................................................107 Method/Data Analysis ...................................................................................................107 Results and Conclusion .................................................................................................108
Pilot Study 3 .........................................................................................................................109 Purpose ..........................................................................................................................109 Participants ....................................................................................................................109 Method/Data Analysis ...................................................................................................109 Results and Conclusion .................................................................................................109
B ESSENTIAL-MOVEMENT COMPONENT EVELUATION FORM................................114
C FUGL-MEYER ASSESSMENT..........................................................................................115
LIST OF REFERENCES.............................................................................................................120
BIOGRAPHICAL SKETCH .......................................................................................................132
10
LIST OF TABLES
Table page 1-1 Atypical synergy movement patterns of extremities observed in people with stroke .......33
1-2 Wolf Motor Function Test: Functional Ability Scale ........................................................33
2-1 Functional Ability Scale ....................................................................................................53
2-2 Demographic information of raters....................................................................................53
2-3 Demographic information of participants..........................................................................53
2-4 Intra-rater reliability (ICC) for individual essential-movement component and total score of essential-movement component ...........................................................................53
2-5 Intra-rater reliability (ICC) for magnitude of essential-movement components ...............54
2-6 Inter-rater reliability for individual and total score of essential-movement component ...54
2-7 Inter-rater reliability (ICC) for magnitude of four essential-movement components........54
2-8 Standard error of measurement (SEM) and minimally detectable change (MDC) ...........54
3-1 Demographic information of subjects................................................................................71
3-2 One-way ANOVA results for total score of essential-movement component and compensatory movement, and movement magnitude of four movement components .....71
3-3 Percentage of observed essential-movement components and compensatory movements of Lift Basket task in control, high- and low-functioning stroke groups .......72
4-1 Demographic information of participants..........................................................................89
4-2 Repeated measure ANOVA results for composite scores of essential-movement component and compensatory movement, and movement magnitude of three movement components ......................................................................................................89
4-3 Percentage of observed essential-movement components and compensatory movements of Lift Basket task in high- and low-functioning stroke groups.....................90
4-4 Corresponding compensatory movement of the Lift Basket task observed in individuals with stroke.......................................................................................................90
A-1 Demographic information of control group participants of Pilot Study 1 .......................111
A-2 Results of Pilot Study 3....................................................................................................111
11
LIST OF FIGURES
Figure page 1-1 Two fundamental planes of EW sphere .............................................................................34
1-2 The 26 positions on SoR when one unit of movement is 45° ............................................34
2-1 Lift Basket task ..................................................................................................................55
2-2 Fundamental planes of EWMN sphere ..............................................................................56
2-3 Positions on SoR................................................................................................................56
2-4 Example of original EWMN page for the “Lift Basket” task in WMFT...........................57
2-5 Essential-Movement Component Evaluation form based on EWMN...............................58
3-1 Set-up for the Lift Basket task ...........................................................................................73
4-1 Starting and ending positions of the Lift Basket task ........................................................91
4-3 Mean composite scores of essential-movement component for high-functioning and low-functioning stroke groups before and after receiving CIMT......................................93
A-1 EWMN page for the “Lift Basket” task in WMFT (example).........................................112
A-2 Essential-Movement Components Evaluation Form (Prototype: without compensatory movement)................................................................................................113
B-1 EMCE form (with compensatory movement)..................................................................114
12
Abstract of Dissertation Presented to the Graduate School of the University of Florida in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy
STROKE AND CONSTRAINT-INDUCED MOVEMENT THERAPY: USE OF ESHKOL-
WACHMAN MOVEMENT NOTATION TO EXAMINE QUALITY OF MOVEMENT
By
Yi-Po Chiu
December 2007 Chair: Kathye E. Light Major: Rehabilitation Science
Quality of movement is an important indicator of post-stroke recovery, but has often been
ignored by rehabilitation professionals. In addition, limited measures of movement quality are
available in clinical and research settings. Constraint-Induced Movement Therapy (CIMT) has
been a beneficial stroke intervention during the past two decades, but its effects on quality of
movement has not been explored. In this study, the author developed an evaluation form, the
Essential-Movement Component Evaluation (EMCE) form, based on a combined application of
the Generalized Motor Program and Eshkol-Wachman Movement Notation (EWMN), measuring
quality of movement that investigates invariant features for a reaching-grasping-lifting-placing
task. For Experiment I, the results showed the EMCE form based on the EWMN method had
excellent intra- and inter-rater reliability with high intraclass correlation coefficients and low
standard error of measurement, when three raters graded 20 participants. With a short training
and practice session, the raters, even novice investigators, can reliably document movement
quality using the EMCE form. For Experiment II, the one-way analysis of variance (ANOVA)
results demonstrated that people with stroke had less normal movement components and more
compensatory movements than normal participants. Among people with stroke, the low-

13
functioning group (n= 20; upper-extremity Fugl-Meyer motor scores ≤ 33) utilized less essential
movement components than the high-functioning group (n= 20; upper-extremity Fugl-Meyer
motor scores > 33). Both stroke groups significantly adopted more compensatory movement
than the normal group (n= 10), but no difference was found between the two stroke groups.
Underutilized essential-movement components and dominance of compensatory movement can
provide rehabilitation professional useful information on developing tailored therapeutic
programs to restore disrupted movement patterns post-stroke. For Experiment III, after 2-week
CIMT, the two-group x two-time ANOVA results showed the low-functioning group (n= 30)
significantly regained more essential movement components than the high-functioning group (n=
30). There was no statistically significant treatment effect on compensatory movement. In
order to improve movement quality post-stroke, the goals of CIMT training, therefore, need to be
expanded to increase the function of underused essential-movement components, re-establish
normal movement sequences, and prevent compensatory movements.
14
CHAPTER 1 INTRODUCTION
Background and Significance
Stroke is the leading cause of long-term disability in the United States.1, 2 Of those
individuals who sustain a stroke, 66% lose long-term functional ability in their affected arm.3-5
About 700,000 Americans experience a first or recurrent stroke each year,6 resulting in annual
direct and indirect costs that are expected to reach $62.7 billion nationwide in 2007.2 Persons
who sustain a stroke often require an enormous amount of medical care involving acute,
rehabilitative, and other maintenance types of treatment. Furthermore, 84% of those who return
to their homes following treatment are unable to resume work.7 Strokes not only affect the
person who has had the stroke, but also those who live and work with the individual. Changes in
role function, self-perception, quality of life, as well as basic capabilities are apparent after
stroke. In light of the foregoing statistics, the widespread occurrence of upper-extremity paresis
following stroke presents an important challenge for rehabilitation research.
In this chapter, the author reviews the relevant literature of important topics in stroke
relevant to this dissertation. The topics include common movement disorders post-stroke,
current methodology of movement analysis, quality of movement in Constraint-Induced
Movement Therapy (CIMT), the Generalized Motor Program theory (GMP), and the Eshkol-
Wachman Movement Notation (EWMN).
Movement Disorders in Stroke
The most common impairments contributing to movement dysfunction after stroke are
muscle weakness,8-11 abnormal muscle tone,9, 11 atypical movement synergy,9, 12, 13, and impaired
inter-joint coordination. 14-17
15
Muscle weakness. Muscle weakness is one of the negative signs of CNS injury after an
individual suffers a stroke.18 Eighty to ninety percent of people with stroke demonstrate
weakness of muscles.11, 19 Possible factors contributing to muscle weakness post-stroke include
alterations in the physiology of motor units, notably changes in firing rates and muscle-fiber
atrophy.8
Overall, muscle weakness may develop after stroke as a result of deconditioning. In
particular, muscle weakness related to stroke paresis may affect one half of the body, including
the trunk and the extremities.9 In the trunk, muscle weakness can interfere with postural control,
balance, and the ability to perform movement sequences.20, 21 Weakness in the extremities can
impede functional use in activities, such as weight bearing and activities of daily living.9, 21
Abnormal muscle tone. After stroke, alterations in muscle tone are observed.9, 21 Muscle
tone changes may be leading to flaccidity or spasticity. Flaccidity or complete loss of muscle
tone is usually present immediately after the stroke. Duration of flaccidity is generally short-
lived, lasting hours, days, or weeks. Prolonged muscular flaccidity post-stroke, however, is
regarded as a negative indicator for functional prognosis.22
Spasticity emerges in about 90% of stroke cases and can occur in all muscles.23 Lance
offered a definition of spasticity that has been generally accepted by physiologists: ‘Spasticity is
a motor disorder characterized by a velocity-dependent increase in tonic stretch reflexes (muscle
tone) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex, as one
component of the upper-motor neuron syndrome’11, 24 In other words, spasticity is a state of
hypereflexia after suffering upper-motor neuron lesions.25, 26
The existence of spasticity, which arises from injury to corticospinal pathways and occurs
as part of an upper-motoneuron syndrome usually includes other components, resulting in the
16
term, spasticity syndromes.23 Clinically, spasticity syndromes18, 23, 27-30 contain increased
resistance to passive movement, clasp-knife response, ankle clonus, flexor/extensor spasms, and
excessive muscle cocontraction. The effects of spasticity include restricted voluntary
movement and static posturing of the limbs.31 Individuals with persistent spasticity post-stroke
tend to have less functional recovery32-34 and spend longer time in rehabilitation18 than the
persons without spasticity.
Atypical or pathological movement synergy. Synergy is defined as the action of
muscles working together in a fixed spatial and temporal relationship producing a coordinated
and functional movement.35 Injury to the central-nervous system, such as stroke may affect
synergistic organization of movement.
Following stroke, movements are often limited to patterns of stereotyped atypical or
pathological movement synergy. There are two distinct atypical synergy patterns for each
extremity: flexion synergy and extension synergy (Table 1-1).12, 36 Performing a dynamic
activity, such as reaching for an object and walking may elicit these pathological synergy
patterns. Muscles involved in pathological synergy patterns are often so closely connected that
selective movements outside the synergistic patterns become impossible. For instance, bending
the elbow to touch the chin may result in shoulder flexion, abduction, and external rotation.
According to Brunnstrom’s clinical observation, however, recovery of stroke may follow a
stereotyped sequence, which includes six stages.12 As recovery progresses, the atypical
movement synergies begin to dissipate and lose their dominance over actions after individuals
have learned more voluntary movement. Active selective control of the affected body parts then
become achievable.9, 12, 13 For example, an individual with a stroke moves the arm from 0° to
90° of shoulder flexion when keeping the elbow straight and the forearm fully pronated. An
17
indication of synergy-free movement is that the elbow and forearm shall be able to maintain their
required positions while the arm is moving to 90° of shoulder flexion.
Impaired inter-joint coordination. Inter-limb incoordination is a major impairment of
motor control following a stroke. Coordination is defined as “ability to control one’s movement
properly,”37 “a behavior of two or more degrees of freedom in relation to each other to produce
skilled activity,”38 and “accurate timing of activity onset in different muscles.”39
The common manifestations of impaired inter-limb coordination reported in previous
studies of individuals with stroke include incorrect timing of muscle activation,14, 21, 40, 41
slowness of movement,15, 42-44 segmented movement,15, 42, 43 variable arm movement,42, 44 larger
movement errors,42 and recruitment of extra degrees of freedom (i.e. compensatory movements
from other body parts).15, 42, 43, 45
Current Methodology of Movement Analysis
Scientists, clinicians, and engineers have developed various methods and equipment to
study movement deficits and functional recovery post-stroke. In this section, the relevant
literature concerning contemporary methodology of movement analysis used for stroke research
will be reviewed. The advantages and disadvantages of these methodologies will be discussed.
The methodology for investigating movement deficits after stroke can be divided into two main
categories: qualitative and quantitative methods.46
Qualitative methods. These are defined as nonnumeric evaluations of motion using visual
observation and video analysis.
Observation. Therapists typically use observation to evaluate movement of stroke patients
in clinical rehabilitation settings.12, 13, 21 Common parameters of observation include atypical
synergy patterns, postural symmetry, static/dynamic balance, and gait patterns.36 For instance,
post-stroke atypical synergy is an abnormal stereotyped movement pattern. There are two major
18
types of pathological synergy patterns in the extremities (Table 1-1): flexion synergy and
extension synergy.47 Brunnstrom12 suggested that the recovery of motor function after stroke
follows characteristic stages. In the later stages, patients are able to make movements out of
synergy.12 Out of synergy indicates increased selective/voluntary control of the paretic body.
Clinicians document the progress of synergy movement patterns as an indicator of improvement.
Video/photographic analysis. Video or photographic analysis is a common research
method of motion analysis used in rehabilitation clinics and research facilities. After videotaping
or taking pictures of patient’s movements, therapists or researchers can further evaluate quality
of movement. Reflective markers on specific anatomical landmarks, for instance joint and bone
prominences, can assist the observation of body parts and positions. Recently, Bukowski48
developed a movement analysis procedure, analyzing the range-of-motion and the muscles
involved in daily activities. The procedure requires participants to expose the region of interest
and to repeatedly perform an activity to determine appropriate body landmarks. After placing
body markers on each subject, evaluators can measure range-of-motion and infer involved
muscles from changes of joint position in video clips. Bukowski’s method finely integrates
kinesiology with representative activities of daily life, but the procedure of analysis can be time-
consuming. In addition, requiring repetitive performance and physical exposure may cause
inconvenience and subject fatigue, thus hindering clinical feasibility.
Quantitative methods. These are defined as numeric evaluations of motion, based on data
collected during the performance46, such as biomechanics and motor function scales.
Biomechanical analysis. Biomechanists apply the theory of mechanics and physics to a
biological system to analyze the movement of an organism and the effect of forces on the
organism.46 Biomechanical analysis includes two main aspects: kinematics and kinetics.
19
Kinematics is a study that focuses on movement characteristics and spatial/temporal perspectives
of movement without considering the forces involved in the movement. A kinematic analysis
involves describing a movement in terms of its position, velocity, and acceleration. Kinetics is
concerned with forces acting on a system. The common research parameters in biomechanics
can include speed, direction, force, moment, and torque.46 Biomechanical methods are heavily
dependent on data collection using laboratory equipment. Electro-goniometers, accelerometers,
and imaging techniques are frequently used for kinematic analysis.49 Kinetic analysis
necessitates use of force transducers and force plates.49 Furthermore, processing the collected
data often requires sophisticated algorithms, mechanical models, or computer software.
Motor function scales. In order to quantify human movement, numerous motor function
scales have been developed, for example, the Functional Ability Scale(FAS) in the Wolf Motor
Function Test (WMFT),50 the Quality of Movement Scale in the Motor Activity Log,1 Chedoke
Arm and Hand Activity Inventory,51-53 and the Reaching Performance Scale.54 Motor function
scales are designed using ordinal rating categories, which assign scores from low to high with
specific descriptions to indicate increase or decrease of motor function. For instance, the
Functional Ability Scale in the Wolf Motor Function Test is a 6-point scale ranging from 0 (Does
not attempt with the involved arm) to 5 (Does attempt with the involved arm and the movement
appears to be normal). Ordinal motor function scales are used extensively in studies of stroke
intervention effectiveness.54-58
Qualitative methods have some advantages over quantitative methods for describing post-
stroke movement. Qualitative methods are more flexible, feasible, convenient and less costly
than quantitative methods.59 The limitations of qualitative methods, however, include lack of
precision, reliability, and validity.60, 61 Moreover, subjective, narrative information from
20
qualitative analysis is typically obtained under less controlled, and less structured conditions than
those for quantitative analysis.62 Many of the conventional quality of movement measurements
focus on a specific aspect of impairment rather than the wide range of issues which arise from
compromised movement. For instance, both Brunnstrom’s notion of hemiplegic limb synergies12
and Bobath’s concept of abnormal movement patterns combined with abnormal postural tone13
have a tendency to emphasize specific movement impairment. Their specification of movement
impairment mainly targets the affected limbs, without considering associated compensatory
movements of the body. There is, therefore, a need for further research to develop a more
comprehensive and clinically feasible measurement method to systematically analyze quality of
movement.
Quantitative methods, such as biomechanics for example, can have greater accuracy, but
their cost and time consuming nature make these methods only feasible in a laboratory
environment. The sophisticated systems of movement analysis can be used to identify
parameters of normal movement, and are sometimes used in research. The required equipment,
however, is expensive, needs considerable expertise for its operation, and the volume of data
produced can often be overwhelming.63 The derivatives from advanced calculations of
biomechanical parameters can actually generate great confusion and difficulty for clinicians
without providing sufficient direct information about the movement. Most of the stroke
intervention studies focus mainly on aspects of movement deficits as measured by movement
speed and accuracy. 1, 50, 64-71 These aspects do not give insight into the interaction of body parts
that produce them. Motor function scales are feasible and helpful for healthcare providers, but a
statistically significant change of averaged scores can merely indicate an incremental change
along that scale72 and provide limited information about improvement in function and quality of
21
movement. For example, evaluators are unable to explain what the actual movement
improvement is when there is a statistically significant change in averaged FAS score of WMFT
from 2.5 to 3.6.
Developing a measurement template to measure quality of movement, therefore, is
beneficial to our understanding of post-stroke movement after intervention. In the next section,
this need in stroke assessment is further illustrated by using examples from Constraint-Induced
Movement Therapy (CIMT) research. CIMT has been acknowledged as an effective stroke
intervention during the last two decades.
Quality of Movement in Constraint-Induced Movement Therapy
During the past two decades, Constraint-Induced Movement Therapy (CIMT)1, 67, 68 has
been developed by Taub, Wolf and others. CIMT is mainly used in the post-stroke population.
The hypothesis of CIMT is that restraint of the less-affected upper-extremity will force the more-
affected extremity to overcome the phenomenon of “learned nonuse.”66, 67 Based on animal
studies in which primates received surgical deafferentation of one upper-extremity, “learned
nonuse” was defined as “an adverse learning cycle caused by unsuccessful motor attempts with
the deafferented arm that resulted in pain, failure or uncoordinated movements.”1 The ultimate
goals of CIMT are to break the adverse “learned nonuse” cycle and to improve functional use of
the affected upper-extremity.
Constraint-Induced Movement Therapy has two main components: 1) restraint of the less-
affected upper-extremity for 90% of waking hours to force the use of the affected upper-
extremity, and 2) extensive practice with the affected upper-extremity. To date, the effectiveness
of CIMT intervention and its promising results have been widely discussed in the literature.1, 50,
64-70 No studies, however, directly address the impact of CIMT on quality of movement.
22
Assessment of quality of movement: Wolf Motor Function Test. The Wolf Motor
Function Test (WMFT)50 is one of the primary outcome measurements reported in CIMT studies.
Originally, the 15 timed tasks of the WMFT are arranged in an order based upon biomechanical
complexity and progress from proximal to distal joint involvement. A recent pilot study of the
WMFT using Rasch measurement, conducted by Wen and Velozo (unpublished) in 2003,
however, has shown a different order of task difficulty. This indicates that Wolf’s conceptual
task complexity is not reflected in participants’ responses. For example, the last task, Lift Basket,
which was supposed to be the most difficult task of WMFT became the second difficult task.
The WMFT quantifies upper-extremity movement ability through timed single- or multiple-joint
motions and functional tasks. The results of the WMFT are reported on two forms: average time
and average functional-ability scores (Table 1-2). Researchers report CIMT as effective and
clinically meaningful when individuals post-stroke significantly decrease average time or
increase average functional-ability scores.50, 64, 65, 67, 68, 71-74 Decreased time to perform a task
tends to indicate improved efficiency of movement according to CIMT literature.1, 50, 64-71 Recent
biomechanical studies of reaching/grasping movement in stroke populations,42, 43, 45, 75 however,
raise some controversial questions: Is a faster movement a better movement? Do patients with
stroke recover their pre-stroke movement after CIMT? Do patients with stroke adopt
compensatory strategies to perform tasks more efficiently after CIMT? In the study by Cirstea,
Ptito and Levin, decreased movement time after training in moderate-to-severe hemiparesis may
be ascribed to adopting compensatory movements as the optimal solution to improve movement-
outcome measurements.75 There is, however, minimal information available regarding using
compensatory strategies to improve performance during CIMT.
23
Moreover, regarding improved functional-activity scores of the WMFT after CIMT,
averaged ordinal-scale scores of the 15 tasks provide very limited information about actual
improvement of movement.76 If the scores change from rating category 2 to 4 after CIMT, does
it mean the improvement is doubled? What are the factors that contribute to the improvement of
scores? Interpreting scores changing from 2 to 4 as a 100% functional improvement would be
erroneous. Inappropriately interpreting results from the ordinal motor-function scales may cause
potential distortion or bias of inference. Bonifer et al.72 suggested that future CIMT studies
should evaluate the relationships between changes on standardized assessments of motor
function and improvements in everyday function.
In the present research, the questions raised above about CIMT intervention regarding
quality of movement were investigated by analyzing a complex movement selected from the
WMFT. Quality of movement is clearly defined and the results are clearly presented.
Definition of Quality of Movement Used for People Post-Stroke
Both rehabilitation professionals and individuals post-stroke want to work towards and
accomplish well-controlled, normal looking movements. Studying quality of movement,
therefore, is important to clinicians and researchers. Quality of movement, however, has not
been systemically measured, and in fact, the definition of quality of movement continues to be
controversial. The common indicators of quality of movement in the literature include:
coordination of inter-limb movements, movement time, linear displacement, linear velocity,
linear acceleration, angular displacement, angular velocity, angular acceleration, force, and
moment of force. 17, 44, 45, 75, 77 In addition, some researchers consider that efficiency of
movement is a representation of quality of movement.78 An efficient movement with high
movement quality is the one that fulfills a specific purpose with movement economy at the
required speed and with the least energy expenditure.79-81 The description of quality of
24
movement, therefore, appears to differ widely among professionals. In Pomeroy’s study, ten
experienced physical therapists were asked to grade the quality of movements of people with and
without stroke, based on their performance of six standardized functional tasks, using a 100-mm
visual-analogue scale. Their intriguing results suggested that substantial disagreement existed
among therapists in grading movement quality. In contrast, no significant discrepancy was
found between the grading scores of the same therapist at two separate viewing times. The
meaning of movement quality, therefore, may be consistent within an individual therapist but
discrepant between therapists.
Definition of quality of movement. Prior to investigating post-stroke movement quality,
establishing a reference point for quality is necessary. Generally speaking, the consensus of
rehabilitation professionals in regard to this reference point is “normal movement.”82 Normal
movement is the movement observed in people with no previous neurological disorders that may
affect movement execution.83 Moreover, normal movement has been a basis for treating
neurologically-injured individuals.13, 14, 47 Assessing impairment and designing its appropriate
intervention, therefore, depends on a thorough understanding of normal movement.
In the current research, this author defines quality of movement as movement component
and strategy. Through direct observation coupled with the use of a coherent movement analysis
system, clinicians and researchers can then identify the movement composition (i.e. movement
components) and sequence. When therapists recognize specific aspects of a particular skill and
movement sequence of a task,84 the information will assist clinicians and researchers in assessing
progress of recovery and developing rehabilitation programs.
After defining quality of movement, the following sections focus on 1) the essentials of
normal human movement based on the Generalized Motor Program theory, which was the
25
central framework of this research, and 2) the Eshkol-Wachman Movement Notation (EWMN),
an assessment tool used in this research to develop a movement quality analysis form.
Generalized Motor Program Theory: The Research Framework
In order to study quality of movement in normal people and people with stroke, the GMP
theory was employed throughout this research. The clarity of this theory allows us to establish
the essentials of human movement.
The GMP theory,38, 85 a theory that provides an explanation for the motor control and
motor learning of both rapid and slow movements, was proposed by Schmidt in 1975. Since
then the GMP theory has been extensively discussed in the studies of cognitive psychology,
neuroscience, motor development, physical therapy, and occupational therapy.86 The GMP
theory was proposed as a theoretical structure to explain various responses of a movement that
share invariant features, such as the sequencing of submovements, relative timing, and relative
forces. Actions controlled by the same GMP differ from each other in the assignment of variant
movement parameters, for instance absolute time, absolute force, and selection of effectors.38, 85,
86 In light of the GMP theory, invariant submovements in a fixed movement sequence can be
identified when different individuals execute the same activity.
For instance, the reach/grasp action is a task frequently investigated in studies of upper-
extremity motor function. The essential invariant features have been extensively discussed. In
order to accomplish the reach/grasp action, an individual has to execute a sequence of
submovements. These include eye/head movement that responds to the location of a targeted
object, hand reaching out, hand opening, and grasping. These submovements are invariant
among different individuals. According to GMP theory, what makes movement look different is
how fast or how forcibly people move.
26
Another classic example of the GMP theory demonstrated by Lashley is handwriting.38, 87
Two right-handed, blindfolded individuals were asked to write the words “motor equivalence”
with their right hand (the dominant hand), their left hand (the non-dominant hand) and their teeth.
The results showed that even when writing with different effectors or in different speed and size,
certain aspects of the written words appeared to be invariant, for instance, the shapes of the
letters.
The invariant features of the GMP theory, therefore, can serve as a research framework in
studying quality of movement. When the invariant features of movement in people without
stroke can be distinguished, healthcare providers will be able to clearly and effectively pinpoint
the impairment of motor control in people with stroke.
A Comprehensive Approach of Movement Analysis: Using Eshkol-Wachman Movement Notation
Understanding the fundamental deficits of movement in individuals post stroke is crucial
for the development of effective rehabilitative interventions. In the present research, the author
examined post-stroke movement deficit using a comprehensive approach that contained two
modes of assessment.
First, the author considered the whole body as one functional unit. Therefore, by using
whole-body movement analysis, affected and less affected body parts will be considered at the
same time. Knowing the limitations of upper-extremity function in an impaired limb is central
but knowing the influence of the less-affected body parts is also beneficial to understand the
interactions between different body parts. Second, the author analyzed post-stroke movement as
a multifaceted process, which took into account the sequence of submovements. Examination of
a movement included a beginning, middle, and end point in its discrete parts and overall sum.
27
This approach provided further insight about the conditions and challenges facing patients post-
stroke when executing an activity.
As of today few systematic methods of whole-body motion analysis are available for
clinicians or researchers in stroke rehabilitation. Existing systems may be able to define,
describe, and distinguish the different types of movement, but these standardized methodologies
apply to only the body segment most affected by the stroke. In addition, these analyses are most
often end-point measurements. When studying movement deficits following stroke,
biomechanical researchers mainly give attention to partial views of a movement, without
considering involvement of other body parts.17, 43, 45, 75, 77, 88, 89 Analyzing movements for the
changing interrelationship of whole-body parts, hence, can yield an increased understanding of
human movement. A comprehensive view of movement could help identification of the often
dysfunctional movement parameters seen post-stroke. In order to implement this comprehensive
approach, the author chose the EWMN90-92 method as the evaluation tool.
Eshkol-Wachman Movement Notation (EWMN). EWMN90-92 is a movement language
developed in Israel by professors Noa Eshkol and Avraham Wachman. In the literature of
human and animal behavior, EWMN has been shown to effectively describe various aspects of
movement, such as time, speed, direction, magnitude, limb position, inter-limb spatial
relations/coordination, sequence and trajectory.93-97 Although EWMN is not currently a widely
known or accepted method to analyze movement in stroke rehabilitation, some research
scientists have pointed out the benefits of utilizing this useful tool. Teitelbaum94, 97 and
Whishaw93, 96 have utilized EWMN in their research, with the understanding that observing and
noting movement as a multifaceted sequence can bring forth helpful insights about brain function
and recovery.
28
EWMN is a simple geometrical model, which is compatible with the structure and function
of the human body in motion. In EWMN, each limb is reduced to its longitudinal axis, an
imaginary straight line of unchanging length. A “limb” doesn’t refer to merely arms and legs,
but to any part of the body, which lies between two joints or is a mobile extremity attached to a
joint. Thus, the head, neck, trunk, pelvis and the fingers each consider as a “limb.” The
movements of a single axis of constant length, which is free to move about its fixed end, are
always enclosed by a sphere. Therefore, when a limb moves, it follows curved paths on the
surface of such a sphere. In order to define such data, coordinates are ascribed to the sphere in a
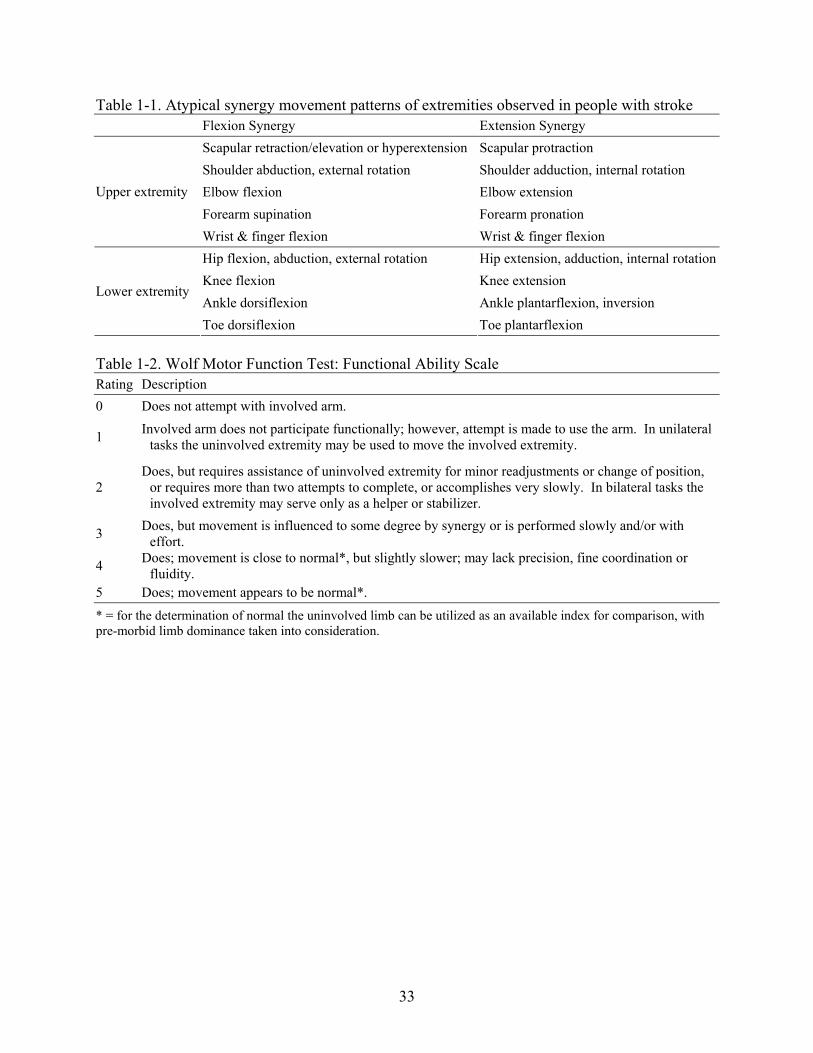
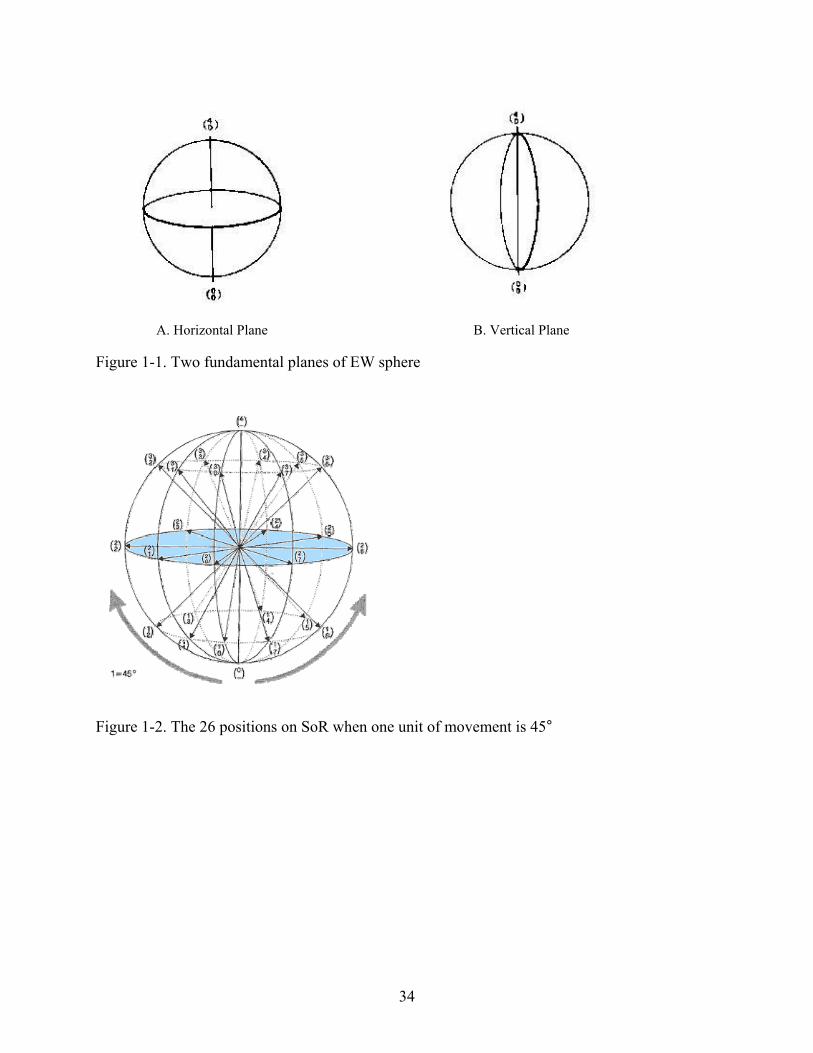
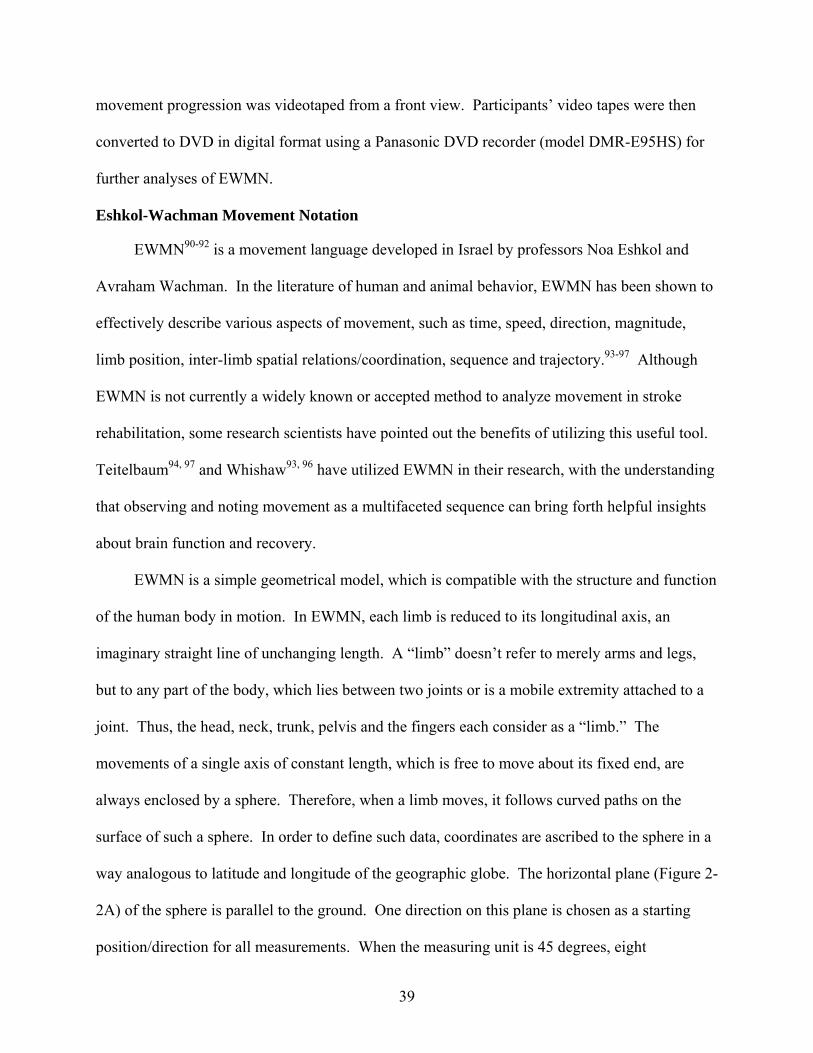
way analogous to latitude and longitude of the geographic globe. The horizontal plane (Figure 1-
1A) of the sphere is parallel to the ground. One direction on this plane is chosen as a starting
position/direction for all measurements. When the measuring unit is 45 degrees, eight
positions/directions are obtained. Vertical planes (Figure 1-1B) are perpendicular to, and
intersect with these horizontal directions. The intersections of horizontal and vertical planes are
defined as positions on the EW sphere. The EW sphere is referred to as the System of Reference
(SoR).90-92 When one unit of movement is 45 degrees, 26 positions are defined on the
SoR.(Figure 1-2) In EWMN, all movements are reduced to three types: plane, conical and
rotatory movements according to the angular relationship between the axis of movement and the
initial position of the limb.90, 92 The advantages of using the EWMN method include:
1. EWMN can systematically record and measure whole body movements, without
depending on expensive equipment and complicated computer software analyses. The
equipment needed for EWMN analysis are a video camera, TV monitor, VCR, or DVD recorder
and DVD player.
29
2. EWMN can directly investigate the prime mover of any movement. In any movement
the limbs of the body are characterized as either “active” or “being carried”. In EWMN, the
movements of passively carried limbs (“light limb”) are influenced by the actual active moving
limbs (“heavy limb”). The spatial changes of the light limb are simply secondary products of the
heavy limb’s movement. Researchers often pay attention to the light limb although the heavy
limb is doing the movement. For instance, when an individual with stroke reaches for a target on
the table, the major research interest is often about whether the hand can touch the target as fast
as possible. Which body part actually moves (heavy limb) seems less important than completion
of the task. The patient can just use the trunk (heavy limb) to carry the hand (light limb) to the
target and still succeed in the task. Examining the movements of the heavy limb can readily
show actual body parts that are recruited for execution of an activity. The movement of the
heavy limb (prime mover), therefore, was the focus of this investigation.
3. In EWMN the exact sequence of human movement pattern can be analyzed by frame-
by-frame analysis. The essential components of a movement can then be readily determined.
Although EWMN has been shown to be an effective and efficient method to study human
movement, its reliability has not been quantitatively determined. In order to justify the
reproducibility and dependability of the EWMN method in the field of movement analysis, the
tests of its intra-rater and inter-rater reliability are required. .
Research Aims and Hypotheses
The overall aims of this research were: 1) to determine, for the first time, the reliability of a
movement analysis chart using the EWMN90-92 method, 2) to investigate invariant features of a
reaching-grasping-lifting-placing task for those with and without stroke, 3) to examine the
change in movement quality of a reaching-grasping-lifting-placing task following CIMT
intervention in terms of invariant features, including movement sequences, components and
30
strategies, and 4) to systematically characterize the compensatory movements observed in people
with stroke while performing a reaching-grasping-lifting-placing task.
Experiment I
General aim 1. Development of a movement analysis form using the Eshkol-Wachman
Movement Notation method and establishment of its reliability
Specific aim 1. To develop a movement analysis form, the Essential-Movement
Component Evaluation (EMCE) form, to measure movement quality of the “Lift Basket” task
Specific aim 2. To establish, for the first time, intra-rater and inter-rater reliability of the
EWMN method when using the EMCE Form.” (see Appendix B)
Hypothesis 1. All the three raters in the intra-rater reliability test will show an excellent
intraclass correlation coefficient (ICC) value, which exceeds .75,98-100 between two separate
testing times.
Hypothesis 2. The result of the inter-rater reliability test will show an excellent ICC
value, which exceeds .75,98-100 among the three raters.
Experiment II
General aim 2. Comparison of movement between persons with and without stroke in
terms of movement components, sequence and strategy
Specific aim 3. To determine the differences between the control and two stroke groups in
terms of the score of essential-movement components and movement sequence identified by the
EMCE form in a reaching-grasping-lifting-placing task. The essential-movement components
identified in persons without stroke are the ten consecutive actions required for accomplishing
the “Lift Basket” task. (See Appendix A: Pilot Study 2 for the details of how the ten essential-
movement components were identified.)
31
Hypothesis 3. Ten essential-movement components of the “Lift Basket” task in the
WMFT 1, 50, 64, 65, 101 that were previously identified by EWMN will appear among all control
group participants, but will be observed less in participants with stroke.
Hypothesis 4. For participants with stroke, the high-functioning group will preserve
greater scores of essential-movement components than the low-functioning group in the “Lift
Basket” task.
Hypothesis 5. The control group participants will initiate the “Lift Basket” task with
proximal body parts progressing to distal body parts; whereas, participants post-stroke will
initiate the task with proximal body parts and only recruit proximal body parts to complete the
task.
Experiment III
General aim 3. Determination of quality of movement changes after the intervention of
Constraint-Induced Movement Therapy
Specific aim 4. To examine the “Lift Basket” task after CIMT in terms of essential-
movement components, movement sequence, and strategy.
Hypothesis 6. During the pre-test evaluation the high-functioning stroke group will
preserve more essential-movement components of the “Lift Basket” task than the low-
functioning stroke group.
Hypothesis 7. After receiving the 2-week CIMT intervention, both the high-functioning
and low-functioning stroke groups will show significant improvement in the scores of essential-
movement components.
Hypothesis 8. After receiving the 2-week CIMT intervention, the low-functioning stroke
group will show more movement improvement in terms of total scores of essential-movement
components, as compared with the high-functioning stroke group.
32
General aim 4. Characterization of compensatory movement in persons with stroke
Specific aim 5. To systematically categorize compensatory movements observed from the
“Lift Basket” task in people with stroke.
Hypothesis 9. After 2-week CIMT intervention, the stroke groups will have less
compensatory movement as compared with pre-test while performing the “Lift Basket” task.
(See Appendix B. EMCE form for explanation of compensatory movement.)
Summary
The rationale of CIMT suggests that the “learned nonuse” developed in people with stroke
may be reversed by stressing the interaction between the affected and less affected upper-
extremity. Constraint on using the less affected upper-extremity may force the use of the
affected upper-extremity and promote its function. The manner in which CIMT examines
quality of movement, however, has yet to consider movement sequence, movement strategy and
whole-body movement analysis. Instead, the outcome measures used reveal limited information
about post-stroke movement, opting to measure quality of movement in terms of how patients
score on a 6-point ordinal scale of the Wolf Motor Function Test (WMFT).102
In the current research, therefore, the author sought to have a more inclusive understanding
of a complex movement in the WMFT through analyses of invariant movement features as
defined in the GMP theory. In addition, the author took a comprehensive approach using
EWMN that emphasized the whole-body movement analysis and whole procedure of movement
to investigate the changes of movement quality after the CIMT intervention.
33
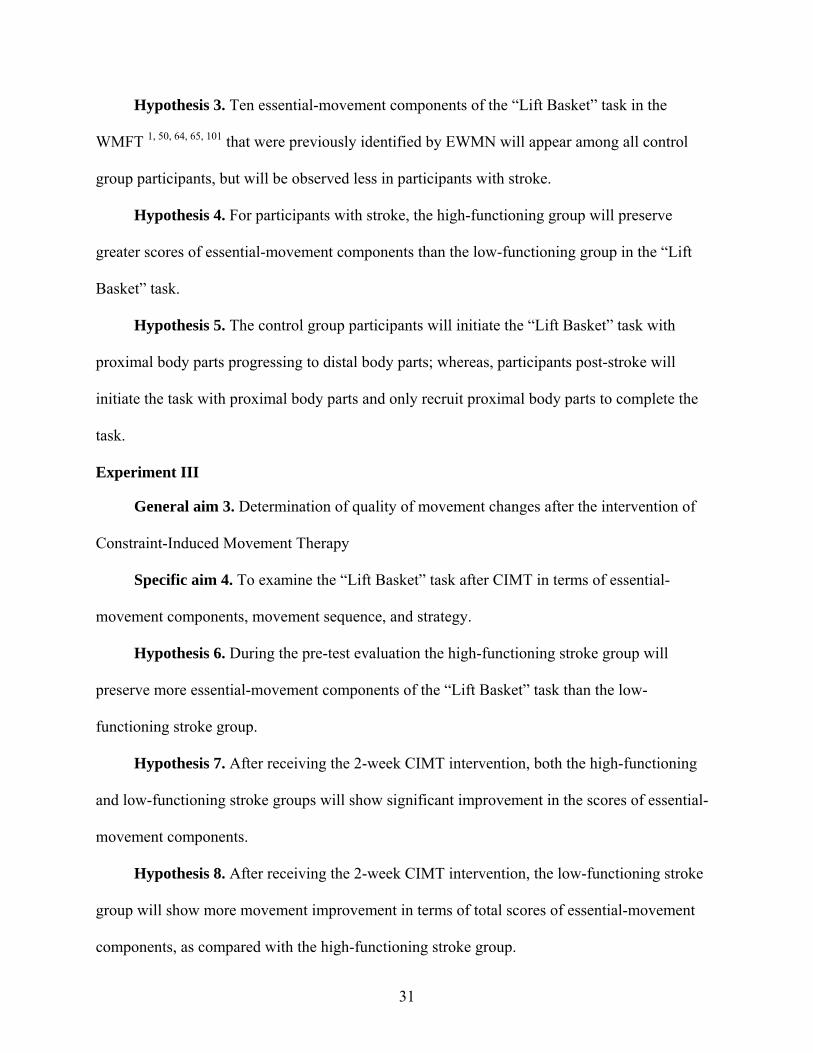
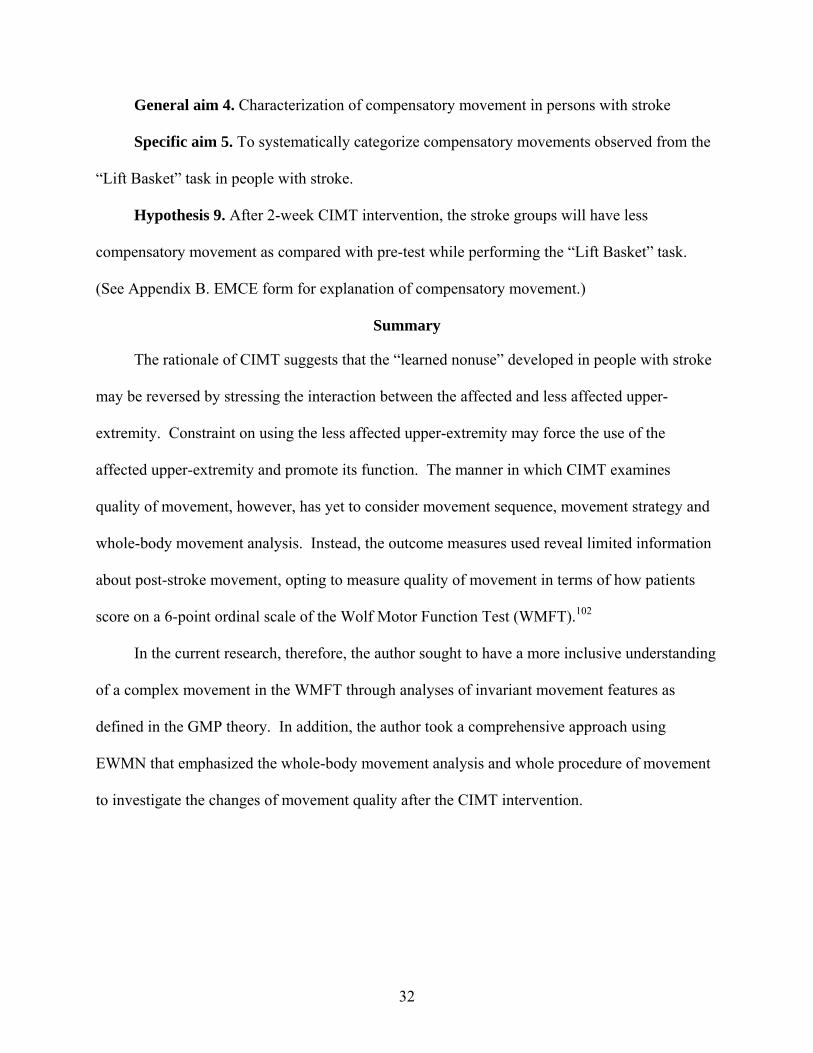
Table 1-1. Atypical synergy movement patterns of extremities observed in people with stroke Flexion Synergy Extension Synergy
Scapular retraction/elevation or hyperextension Scapular protraction Shoulder abduction, external rotation Shoulder adduction, internal rotation Elbow flexion Elbow extension Forearm supination Forearm pronation
Upper extremity
Wrist & finger flexion Wrist & finger flexion Hip flexion, abduction, external rotation Hip extension, adduction, internal rotationKnee flexion Knee extension Ankle dorsiflexion Ankle plantarflexion, inversion
Lower extremity
Toe dorsiflexion Toe plantarflexion Table 1-2. Wolf Motor Function Test: Functional Ability Scale Rating Description 0 Does not attempt with involved arm.
1 Involved arm does not participate functionally; however, attempt is made to use the arm. In unilateral tasks the uninvolved extremity may be used to move the involved extremity.
2 Does, but requires assistance of uninvolved extremity for minor readjustments or change of position,
or requires more than two attempts to complete, or accomplishes very slowly. In bilateral tasks the involved extremity may serve only as a helper or stabilizer.
3 Does, but movement is influenced to some degree by synergy or is performed slowly and/or with effort.
4 Does; movement is close to normal*, but slightly slower; may lack precision, fine coordination or fluidity.
5 Does; movement appears to be normal*. * = for the determination of normal the uninvolved limb can be utilized as an available index for comparison, with pre-morbid limb dominance taken into consideration.
34
Figure 1-1. Two fundamental planes of EW sphere
Figure 1-2. The 26 positions on SoR when one unit of movement is 45°
A. Horizontal Plane B. Vertical Plane
35
CHAPTER 2 DEVELOPMENT AND RELIABILITY OF THE ESSENTIAL MOVEMENT COMPONENT
EVALUATION FORM USING ESHKOL-WACHMAN MOVEMENT NOTATION
Introduction
Movement quality is an important aspect in our daily life.103 Physical education teachers
use quality of movement to evaluate student performance. Athletes rely on the analysis of
movement quality to improve their technique and pursue perfect performance. Dancers strive for
a smooth and coordinated movement based on the qualitative performance. So do people
following a stroke. After our clients can perform certain representative functional activities,
such as walking and reaching, improvement in quality of these movements becomes their next
ultimate goal. A movement with poor quality may impede the use of the affected extremities,
and may adversely affect self image and further hamper social participation.104
Quality of movement, nevertheless, is an aspect that has not been extensively explored in
stroke rehabilitation. Possible reasons for ignoring movement quality assessment can be the
current emphasis on a functional treatment approach,17, 75, 88, 105 lack of agreement on the
definition of movement quality,63 and the lack of measurements available to describe changes of
movement quality.106, 107 Currently, therapists and researchers may pay more attention to
successful and fast performance of a task rather than to how the movement is executed.108 In
addition, a functional treatment approach can lead to greater improvement in quantitative
measures than a traditional neuromuscular approach, which emphasizes normality of
movement.109 Clinicians and researchers seem to have an implicit knowledge about quality of
movement.63 Generally speaking, the consensus of rehabilitation professionals in regard to this
reference point is “normal movement.”82 Normal movement is the movement observed in
people with no previous neurological disorders that may affect movement execution.83
36
Moreover, normal movement has been a basis for treating neurologically-injured individuals.13, 14,
47
In order to investigate post-stroke quality of movement, the invariant features of the
Generalized Motor Program (GMP) theory can serve as the research framework in this study
since the clarity of this theory allows us to establish the essentials of human movement. The
GMP theory,38, 85 a theory that provides an explanation for the motor control and motor learning
of both rapid and slow movements, was proposed by Schmidt in 1975. Since then the GMP
theory has been extensively discussed in the studies of cognitive psychology, neuroscience,
motor development, physical therapy, and occupational therapy.86 The GMP theory was
proposed as a theoretical structure to explain various responses of a movement that share
invariant features, such as the sequencing of submovements, relative timing, and relative forces.
Actions controlled by the same GMP differ from each other in the assignment of variant
movement parameters, for instance absolute time, absolute force, and selection of effectors.38, 85,
86 Invariant submovements, in a fixed movement sequence, can be identified when different
individuals execute the same activity. According to the GMP theory, quality of movement in
this study is defined as specific aspects of movement, including movement components,
sequence, and strategy.84 A movement of good quality is one that approximates normal
movement.82, 83 Studying invariant features (i.e. movement component, sequence and strategy) of
post-stroke movements can provide important information regarding the impact of stroke on
motor programming.
Biomechanical methods may be useful to explore quality of movement, but the
requirement of expensive equipment and complicated computer software analyses can make this
application very difficult in clinical settings. Developing a clinically feasible and reliable
37
method to measure quality of movement would, therefore, provide a means for clinicians to
report valuable information. In this study, the Eshkol-Wachman Movement Notation (EWMN)
was introduced to provide an effective and economical method. EWMN90-92 is a movement
language developed in Israel by professors Noa Eshkol and Avraham Wachman. In the literature
of human and animal behavior, EWMN has been shown to effectively describe various aspects
of movement, such as time, speed, direction, magnitude, limb position, inter-limb spatial
relations/coordination, sequence and trajectory.93-97 EWMN was the assessment tool used in this
study to develop an evaluation form based on a combined application of GMP38, 85 and
EWMN,90-92 measuring quality of movement that investigates invariant features for a reaching-
grasping-lifting-placing task..
The aims of this study were to 1) develop the Essential-Movement Component Evaluation
(EMCE) form for a reaching-grasping-lifting-placing task in WMFT using the EWMN method,
and 2) to determine the intra- and inter-rater reliability of the EMCE form for a reaching-
grasping-lifting-placing task.
Methods
Development of The Essential-Movement Component Evaluation Form Using EWMN
The movement task selected for this study was the “Lift Basket” task of the WMFT. The
WMFT is a standardized test and one of the primary outcomes in the CIMT studies.1, 50, 57, 58, 64,
67, 68, 74, 101 The WMFT consists of a series of 15 timed tasks and two strength tasks that are
performed in either a sitting or standing position. The 15 tasks are arranged in order of
biomechanical complexity according to the joints involved and the level of difficulty. The tasks
progress from proximal to distal joint involvement and from gross to fine motor skills.50 A
recent pilot study of the WMFT using Rasch measurement, conducted by Wen and Velozo
(unpublished) in 2003, however, has shown a different order of task difficulty. This indicates
38
that Wolf’s conceptual task complexity is not reflected in participants’ responses. For example,
the last task, Lift Basket, which was supposed to be the most difficult task of WMFT became the
second difficult task. The WMFT quantifies upper-extremity movement ability through timed
single- or multiple-joint motions and functional tasks.50
The last task in the WMFT, “Lift Basket,” is regarded as a complex task that demands
efforts from multiple body systems, such as muscle strength, dynamic/standing balance, and
inter-limb coordination. As compared with a simple activity, such as reaching for an object on a
table, “Lift Basket” is a representative activity with greater difficulty in our daily life. This task
requires involvement from the whole body. Studying this task, therefore, can show how one
body part interacts with others during movement. Moreover, the “Lift Basket” task is an “out of
synergy” movement that can target the limitation people with stroke have when performing a
reaching and lifting task.88
“Lift Basket” task
The set-up of the “Lift Basket” task included a basket, a desk (29” high) located in front of
the participant and a bedside table (44” high) located on the participant’s side to be tested. (see
Figure 2-1) The bedside table extended along the width of the desk. The basket was placed on
the desk and lined up with the center of the participants’ body. A three-pound weight was placed
in the basket. Participants were tested in a standing position while facing the desk. The set-up of
the “Lift Basket” task is illustrated with its starting position (Figure 2-1A) and ending position
(Figure 2-1B). The task description was “Patient attempts to pick up basket by grasping handle
(from underneath the handle) and placing the basket on far edge of the rolling bedside table.”
All participants were asked to “Pick up the basket with your hand and place the basket on the
rolling table. The far edge of the basket should go past the far edge of the bedside table. Try not
to move your feet while you do this task. Do this as quickly as you can.”102 The subject’s
39
movement progression was videotaped from a front view. Participants’ video tapes were then
converted to DVD in digital format using a Panasonic DVD recorder (model DMR-E95HS) for
further analyses of EWMN.
Eshkol-Wachman Movement Notation
EWMN90-92 is a movement language developed in Israel by professors Noa Eshkol and
Avraham Wachman. In the literature of human and animal behavior, EWMN has been shown to
effectively describe various aspects of movement, such as time, speed, direction, magnitude,
limb position, inter-limb spatial relations/coordination, sequence and trajectory.93-97 Although
EWMN is not currently a widely known or accepted method to analyze movement in stroke
rehabilitation, some research scientists have pointed out the benefits of utilizing this useful tool.
Teitelbaum94, 97 and Whishaw93, 96 have utilized EWMN in their research, with the understanding
that observing and noting movement as a multifaceted sequence can bring forth helpful insights
about brain function and recovery.
EWMN is a simple geometrical model, which is compatible with the structure and function
of the human body in motion. In EWMN, each limb is reduced to its longitudinal axis, an
imaginary straight line of unchanging length. A “limb” doesn’t refer to merely arms and legs,
but to any part of the body, which lies between two joints or is a mobile extremity attached to a
joint. Thus, the head, neck, trunk, pelvis and the fingers each consider as a “limb.” The
movements of a single axis of constant length, which is free to move about its fixed end, are
always enclosed by a sphere. Therefore, when a limb moves, it follows curved paths on the
surface of such a sphere. In order to define such data, coordinates are ascribed to the sphere in a
way analogous to latitude and longitude of the geographic globe. The horizontal plane (Figure 2-
2A) of the sphere is parallel to the ground. One direction on this plane is chosen as a starting
position/direction for all measurements. When the measuring unit is 45 degrees, eight
40
positions/directions are obtained. Vertical planes (Figure 2-2B) are perpendicular to, and
intersect with these horizontal directions. The intersections of horizontal and vertical planes are
defined as positions on the EW sphere. The EW sphere is referred to as the System of Reference
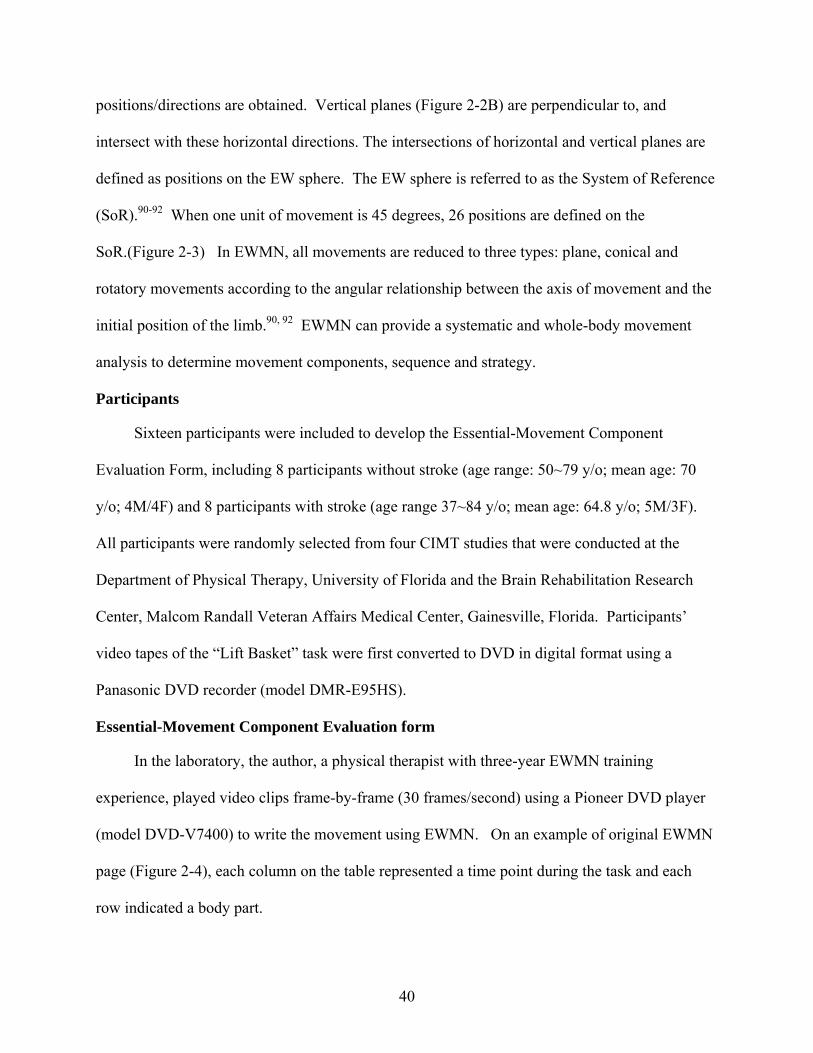
(SoR).90-92 When one unit of movement is 45 degrees, 26 positions are defined on the
SoR.(Figure 2-3) In EWMN, all movements are reduced to three types: plane, conical and
rotatory movements according to the angular relationship between the axis of movement and the
initial position of the limb.90, 92 EWMN can provide a systematic and whole-body movement
analysis to determine movement components, sequence and strategy.
Participants
Sixteen participants were included to develop the Essential-Movement Component
Evaluation Form, including 8 participants without stroke (age range: 50~79 y/o; mean age: 70
y/o; 4M/4F) and 8 participants with stroke (age range 37~84 y/o; mean age: 64.8 y/o; 5M/3F).
All participants were randomly selected from four CIMT studies that were conducted at the
Department of Physical Therapy, University of Florida and the Brain Rehabilitation Research
Center, Malcom Randall Veteran Affairs Medical Center, Gainesville, Florida. Participants’
video tapes of the “Lift Basket” task were first converted to DVD in digital format using a
Panasonic DVD recorder (model DMR-E95HS).
Essential-Movement Component Evaluation form
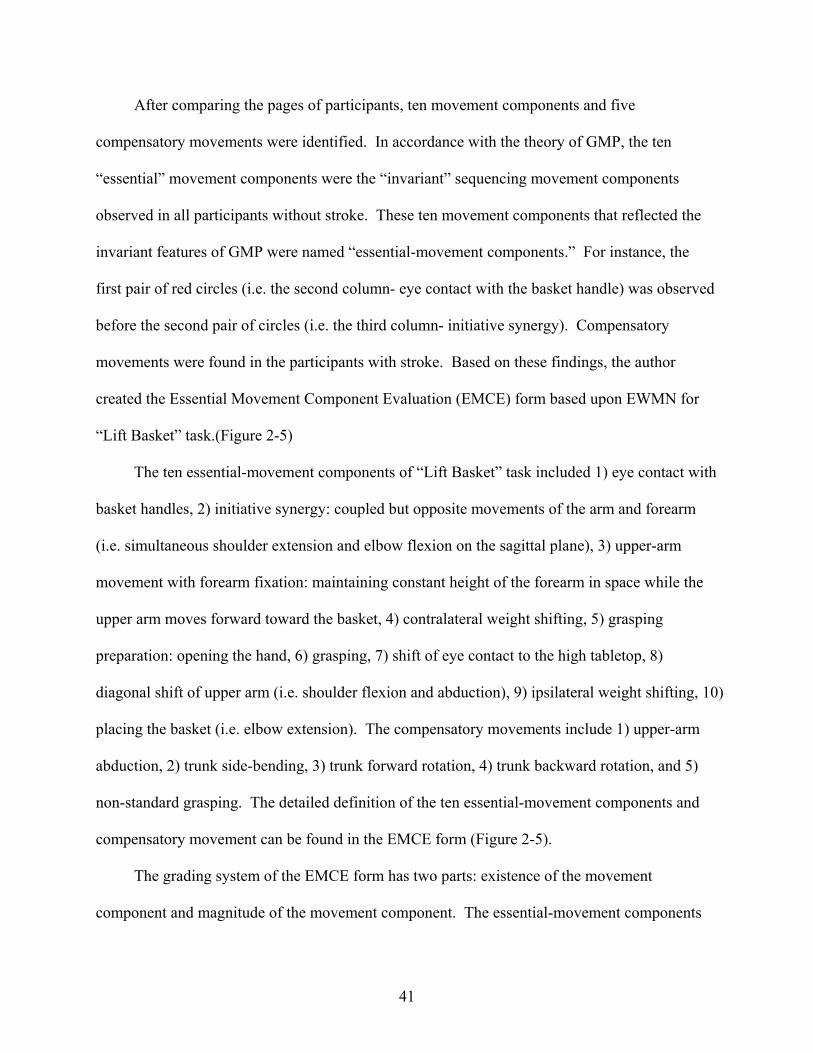
In the laboratory, the author, a physical therapist with three-year EWMN training
experience, played video clips frame-by-frame (30 frames/second) using a Pioneer DVD player
(model DVD-V7400) to write the movement using EWMN. On an example of original EWMN
page (Figure 2-4), each column on the table represented a time point during the task and each
row indicated a body part.
41
After comparing the pages of participants, ten movement components and five
compensatory movements were identified. In accordance with the theory of GMP, the ten
“essential” movement components were the “invariant” sequencing movement components
observed in all participants without stroke. These ten movement components that reflected the
invariant features of GMP were named “essential-movement components.” For instance, the
first pair of red circles (i.e. the second column- eye contact with the basket handle) was observed
before the second pair of circles (i.e. the third column- initiative synergy). Compensatory
movements were found in the participants with stroke. Based on these findings, the author
created the Essential Movement Component Evaluation (EMCE) form based upon EWMN for
“Lift Basket” task.(Figure 2-5)
The ten essential-movement components of “Lift Basket” task included 1) eye contact with
basket handles, 2) initiative synergy: coupled but opposite movements of the arm and forearm
(i.e. simultaneous shoulder extension and elbow flexion on the sagittal plane), 3) upper-arm
movement with forearm fixation: maintaining constant height of the forearm in space while the
upper arm moves forward toward the basket, 4) contralateral weight shifting, 5) grasping
preparation: opening the hand, 6) grasping, 7) shift of eye contact to the high tabletop, 8)
diagonal shift of upper arm (i.e. shoulder flexion and abduction), 9) ipsilateral weight shifting, 10)
placing the basket (i.e. elbow extension). The compensatory movements include 1) upper-arm
abduction, 2) trunk side-bending, 3) trunk forward rotation, 4) trunk backward rotation, and 5)
non-standard grasping. The detailed definition of the ten essential-movement components and
compensatory movement can be found in the EMCE form (Figure 2-5).
The grading system of the EMCE form has two parts: existence of the movement
component and magnitude of the movement component. The essential-movement components
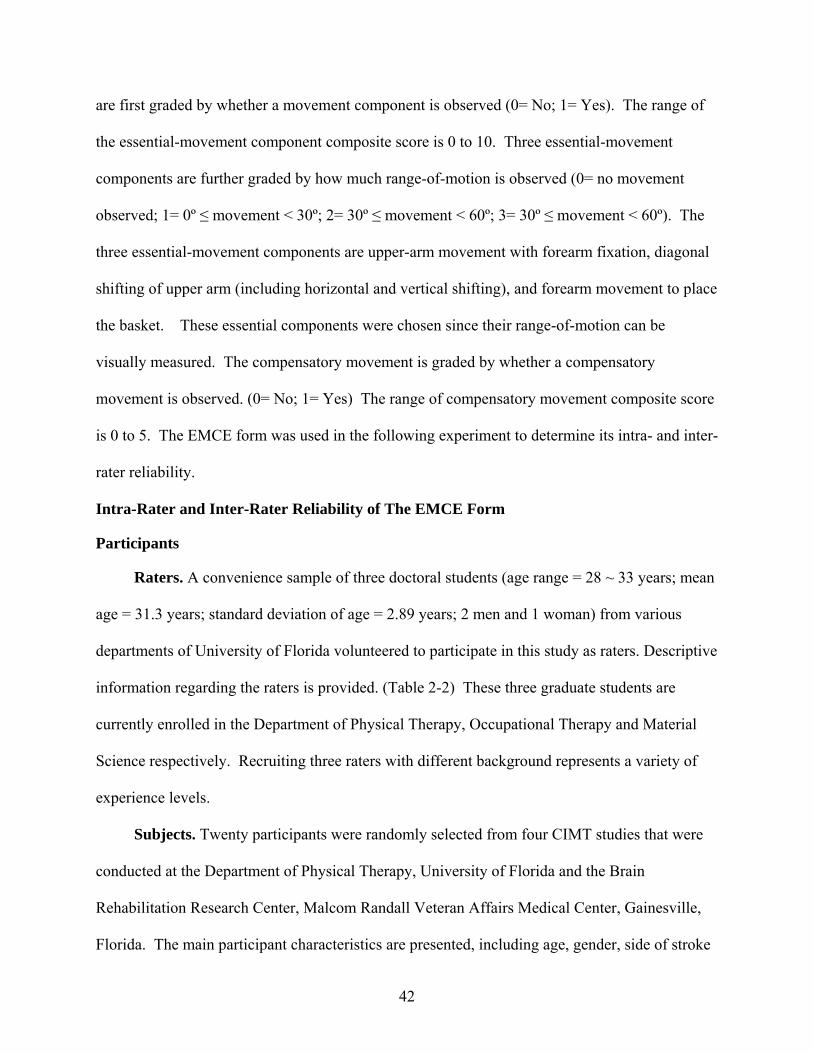
42
are first graded by whether a movement component is observed (0= No; 1= Yes). The range of
the essential-movement component composite score is 0 to 10. Three essential-movement
components are further graded by how much range-of-motion is observed (0= no movement
observed; 1= 0º ≤ movement < 30º; 2= 30º ≤ movement < 60º; 3= 30º ≤ movement < 60º). The
three essential-movement components are upper-arm movement with forearm fixation, diagonal
shifting of upper arm (including horizontal and vertical shifting), and forearm movement to place
the basket. These essential components were chosen since their range-of-motion can be
visually measured. The compensatory movement is graded by whether a compensatory
movement is observed. (0= No; 1= Yes) The range of compensatory movement composite score
is 0 to 5. The EMCE form was used in the following experiment to determine its intra- and inter-
rater reliability.
Intra-Rater and Inter-Rater Reliability of The EMCE Form
Participants
Raters. A convenience sample of three doctoral students (age range = 28 ~ 33 years; mean
age = 31.3 years; standard deviation of age = 2.89 years; 2 men and 1 woman) from various
departments of University of Florida volunteered to participate in this study as raters. Descriptive
information regarding the raters is provided. (Table 2-2) These three graduate students are
currently enrolled in the Department of Physical Therapy, Occupational Therapy and Material
Science respectively. Recruiting three raters with different background represents a variety of
experience levels.
Subjects. Twenty participants were randomly selected from four CIMT studies that were
conducted at the Department of Physical Therapy, University of Florida and the Brain
Rehabilitation Research Center, Malcom Randall Veteran Affairs Medical Center, Gainesville,
Florida. The main participant characteristics are presented, including age, gender, side of stroke
43
and time since stroke.(Table 2-3) Three groups of participants were included in this experiment:
participants without stroke (normal group; n= 4), high-functioning participants with stroke (n= 8),
and low-functioning participants with stroke (n= 8).
The participants with stroke were divided into two groups using their upper-extremity
Fugl-Meyer motor scores: high-functioning (scores > 33) and low-functioning group (scores ≤
33). The Fugl-Meyer Assessment110 (see Appendix C) is regarded as an objective and
quantifiable assessment of motor impairment. The Fugl-Meyer Assessment is also a
standardized assessment to measure recovery after stroke. The upper-extremity Fugl-Meyer
motor component (total score = 66) assesses the ability to move in/out of synergy, reflexes, wrist
stability, grasping ability and coordination. In stroke rehabilitation research, the Fugl-Meyer
Assessment is frequently used as a primary outcome measure of impairment,74, 111 and has been
shown to be predictive of dependency, functional level and recovery after stroke.58, 112-114
The inclusion criterion for the control group was that they had no prior history of
neurological disorders. All participants with stroke in this experiment met the following
inclusion criteria: 1) the diagnosis of at least one stroke, but not more than three strokes on the
same side of the brain, 2) stroke at least three months prior to study participation, 3) ability to
follow simple instructions, 4) a score of 20 or higher on the Mini Mental-State Exam,115 5) the
ability to sit independently without back or arm support for two minutes, 6) the ability to stand
with support of a straight cane, quad cane or hemi-walker for two minutes, 7) the ability to
actively participate for six hours of therapy without long rests or nap periods, 8) passive range-
of-motion of all upper-extremity motions of at least half the normal range, 9) traditional CIMT
minimal motor criteria.1, 67, 116-118 Minimal motor criteria were defined as active movement of
the wrist through at least 20 degrees of extension from a relaxed flexed position, and active
44
movement of at least three fingers (the thumb and two fingers) 20 degrees of extension at the
metacarpal-phalangeal and proximal interphalangeal joints.
Exclusion criteria for both stroke groups included 1) any health problems that put the
individual at significant risk of harm during the study, 2) any other neurological conditions such
as multiple sclerosis or Parkinson’s disease, 3) taking drugs for spasticity, 4) pain that is scored
greater than 5/10 on the McGill Pain Scale119. Furthermore, the participants were excluded if
they could not independently reach the handle of the basket for the “Lift Basket” task of the
WMFT in a standing position with or without support of a straight cane, quad cane or hemi-
walker within two minutes.
Procedure
All data used in this experiment were retrospectively retrieved from four previously
completed studies. All participants signed a consent form that was pre-approved by the
Institutional Review Board of University of Florida for permission to be videotaped and have
their videotapes analyzed for movement control. The participants without stroke were recruited
from the local community and only received one test, the Wolf Motor Function Test (WMFT),1,
50, 64, 65, 101 which is a standardized evaluation in traditional CIMT.1, 65 The participants with
stroke received a series of pre-test evaluations that included the WMFT.1, 50, 64, 65, 101
To examine inter-rater and intra-rater reliability, all three raters were provided with the
EMCE Form of EWMN and written instructions for administering the evaluation. The raters
were then given a one-hour training session by the primary investigator to review the movement
components, grading criteria, and instructions for administering the evaluation. Applied
examples of grading were also provided using sample video clips of Lift Basket task, along with
feedback and discussion regarding the choice of the appropriate ratings. After training, the raters
were instructed not to discuss the grading criteria or the evaluation with other raters. A DVD
45
disc that contained the twenty participants’ video clips was then given to each rater. In the
laboratory, the raters played video clips frame-by-frame (30 frames/second) at separate times to
grade participants’ movement, using a Pioneer DVD player (model DVD-V7400). To
investigate intra-rater reliability, one week after this viewing session, the same raters were asked
to grade the same participants’ movement.
A one-week time period was chosen to minimize the possibility of recall. The order of
appearance of each participant’s video clip was randomly altered by the primary investigator for
the second viewing of the DVD. The same guidelines used in the first viewing session were
followed in the second viewing session. In addition, raters were blind to the groups to which the
participants were assigned, his or her first viewing results, and other raters’ results. The above
precautions were taken in order to minimize possible rater bias caused by raters’ memory of the
results of the first viewing session.62
Data Analysis
For the reliability tests in this study, three statistical methods were chosen, including the
intraclass correlation coefficient (ICC),98-100 standard error of measurement (SEM),120, 121 and
minimal detectable change (MDC).122, 123 ICC is a reliability index that measures the strength of
reliability.62 ICC ranges from 0 to 1. SEM is a common method that measures the consistency
or stability of repeated responses over time.62 A measure with stable responses can separate out
errors due to the rater or instrument. SEM can reflect the range of scores that can be expected on
retesting or the extent of expected error in different raters’ scores. MDC is an index to measure
how much change of specific score is necessary to be confident that “true change” has
occurred.124 A small MDC indicates that the changes measured by an instrument are not caused
by error.
46
The scores graded by the raters using the EMCE form included number of essential-
movement components (essential-movement component composite score) and movement
magnitude of the three movement components. For statistical evaluation of inter-rater and intra-
rater reliability, ICC(2,1)98-100 was used to determine the reliability of 1) the essential-movement
component composite scores, 2) movement magnitude of three movement components (upper-
arm movement with forearm fixation, horizontal and vertical shifting movement of upper arm,
and placing basket), and 3) individual essential-movement components. The standards of
interpreting magnitude of the ICC were based on Fleiss’ categories: ≤ .40= poor, .40-.75= fair to
good, >.75= excellent.100, 125
SEM and MDC was calculated for the total score of essential-movement components for
inter-rater and intra-rater reliability. The SEM is expressed in the units of the measure and is
estimated as follows: ICCSD −× 1 , where SD is the standard deviation of the pooled measures
of the scores. The MDC was calculated using the following formula:
296.1 ××= SEMMDC ,126 where 1.96 reflects the 95% confidence intervals and 2 accounts
for the additional uncertainty introduced by measurements obtained at two different time points.
SEM estimates how repeated measures of a person on the same instrument tend to be
distributed around his or her “true” score. SEM is directly related to the reliability of a test. The
larger the SEM, the lower the reliability of the test and the less precision there is in the measures
taken and scores obtained. MDC reflects the smallest detectable difference that can be
considered “actual change” that exceeds measurement error. A change in an observed value that
is less than the MDC would be considered indistinguishable from measurement error.
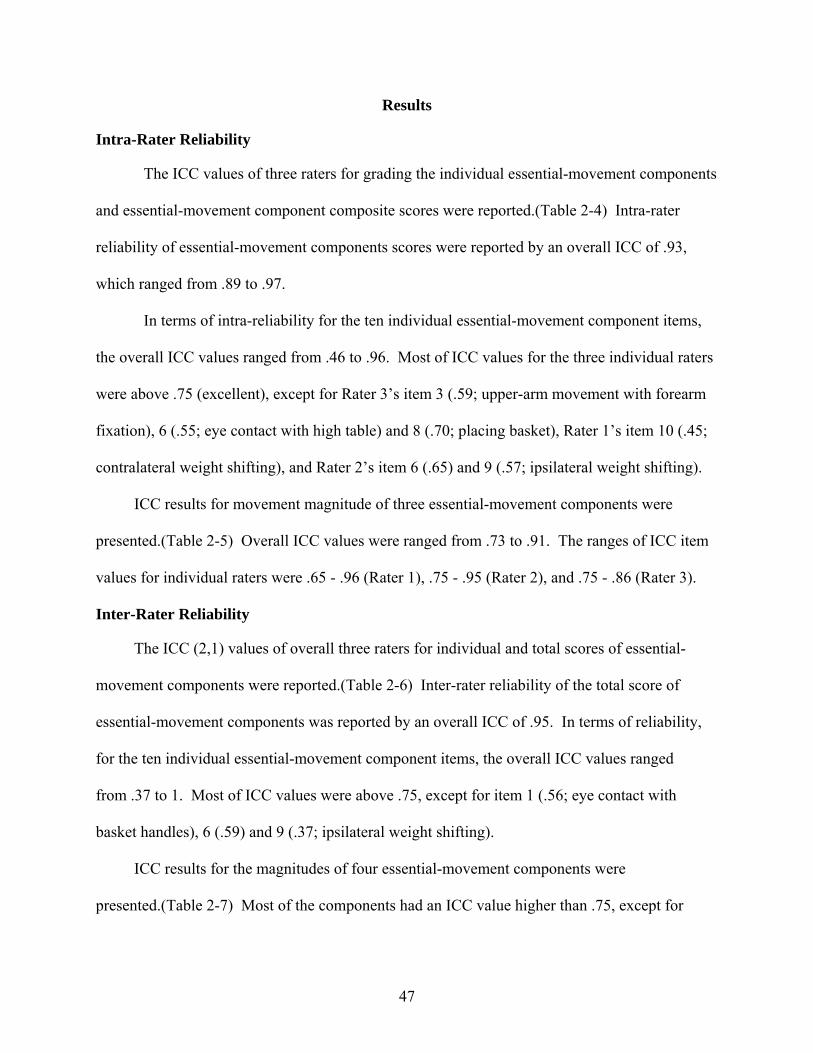
47
Results
Intra-Rater Reliability
The ICC values of three raters for grading the individual essential-movement components
and essential-movement component composite scores were reported.(Table 2-4) Intra-rater
reliability of essential-movement components scores were reported by an overall ICC of .93,
which ranged from .89 to .97.
In terms of intra-reliability for the ten individual essential-movement component items,
the overall ICC values ranged from .46 to .96. Most of ICC values for the three individual raters
were above .75 (excellent), except for Rater 3’s item 3 (.59; upper-arm movement with forearm
fixation), 6 (.55; eye contact with high table) and 8 (.70; placing basket), Rater 1’s item 10 (.45;
contralateral weight shifting), and Rater 2’s item 6 (.65) and 9 (.57; ipsilateral weight shifting).
ICC results for movement magnitude of three essential-movement components were
presented.(Table 2-5) Overall ICC values were ranged from .73 to .91. The ranges of ICC item
values for individual raters were .65 - .96 (Rater 1), .75 - .95 (Rater 2), and .75 - .86 (Rater 3).
Inter-Rater Reliability
The ICC (2,1) values of overall three raters for individual and total scores of essential-
movement components were reported.(Table 2-6) Inter-rater reliability of the total score of
essential-movement components was reported by an overall ICC of .95. In terms of reliability,
for the ten individual essential-movement component items, the overall ICC values ranged
from .37 to 1. Most of ICC values were above .75, except for item 1 (.56; eye contact with
basket handles), 6 (.59) and 9 (.37; ipsilateral weight shifting).
ICC results for the magnitudes of four essential-movement components were
presented.(Table 2-7) Most of the components had an ICC value higher than .75, except for
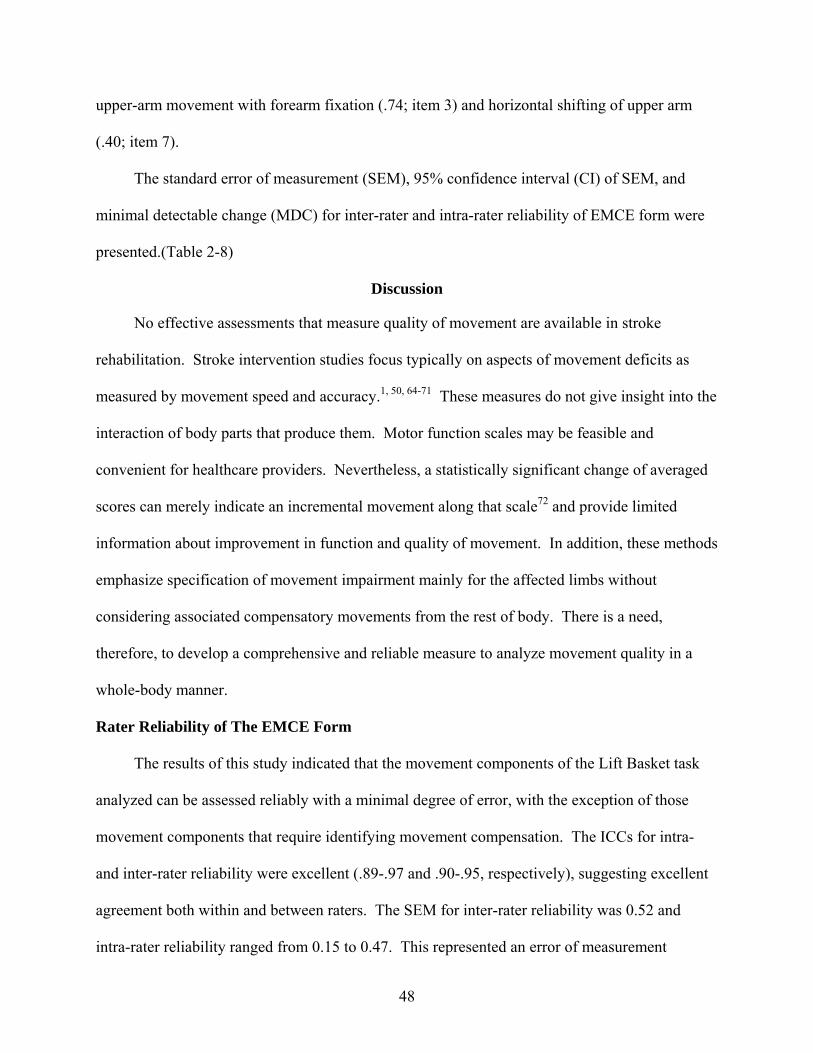
48
upper-arm movement with forearm fixation (.74; item 3) and horizontal shifting of upper arm
(.40; item 7).
The standard error of measurement (SEM), 95% confidence interval (CI) of SEM, and
minimal detectable change (MDC) for inter-rater and intra-rater reliability of EMCE form were
presented.(Table 2-8)
Discussion
No effective assessments that measure quality of movement are available in stroke
rehabilitation. Stroke intervention studies focus typically on aspects of movement deficits as
measured by movement speed and accuracy.1, 50, 64-71 These measures do not give insight into the
interaction of body parts that produce them. Motor function scales may be feasible and
convenient for healthcare providers. Nevertheless, a statistically significant change of averaged
scores can merely indicate an incremental movement along that scale72 and provide limited
information about improvement in function and quality of movement. In addition, these methods
emphasize specification of movement impairment mainly for the affected limbs without
considering associated compensatory movements from the rest of body. There is a need,
therefore, to develop a comprehensive and reliable measure to analyze movement quality in a
whole-body manner.
Rater Reliability of The EMCE Form
The results of this study indicated that the movement components of the Lift Basket task
analyzed can be assessed reliably with a minimal degree of error, with the exception of those
movement components that require identifying movement compensation. The ICCs for intra-
and inter-rater reliability were excellent (.89-.97 and .90-.95, respectively), suggesting excellent
agreement both within and between raters. The SEM for inter-rater reliability was 0.52 and
intra-rater reliability ranged from 0.15 to 0.47. This represented an error of measurement
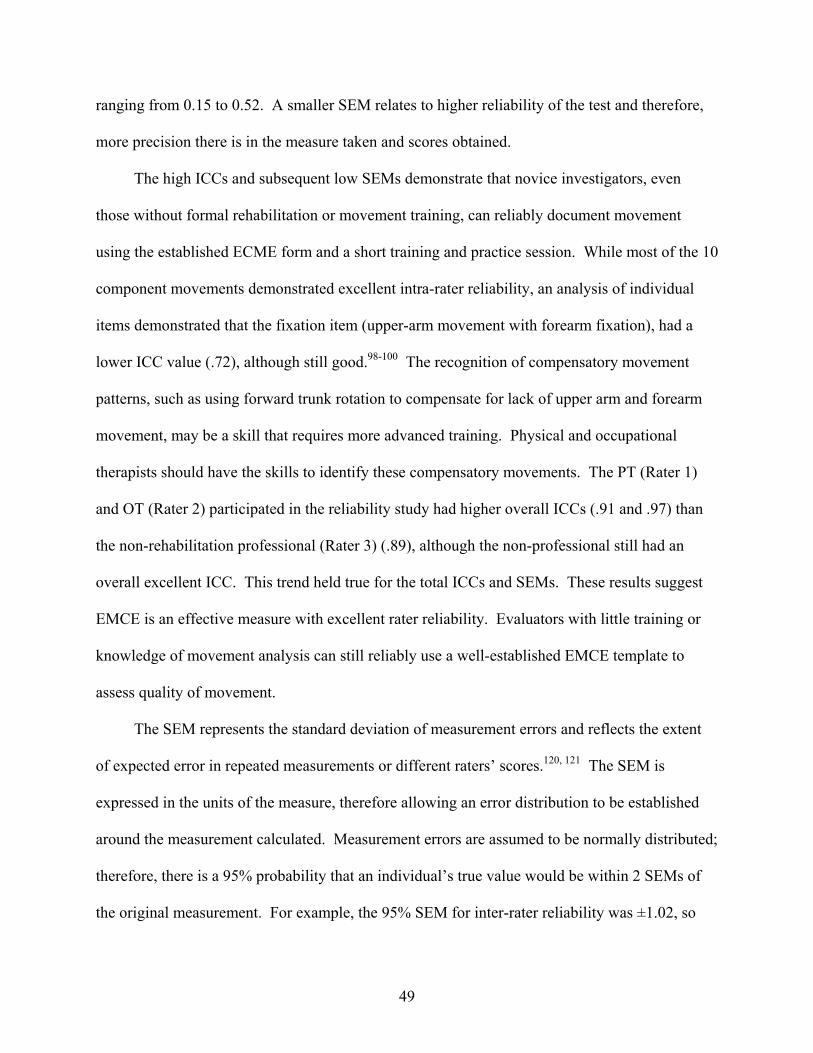
49
ranging from 0.15 to 0.52. A smaller SEM relates to higher reliability of the test and therefore,
more precision there is in the measure taken and scores obtained.
The high ICCs and subsequent low SEMs demonstrate that novice investigators, even
those without formal rehabilitation or movement training, can reliably document movement
using the established ECME form and a short training and practice session. While most of the 10
component movements demonstrated excellent intra-rater reliability, an analysis of individual
items demonstrated that the fixation item (upper-arm movement with forearm fixation), had a
lower ICC value (.72), although still good.98-100 The recognition of compensatory movement
patterns, such as using forward trunk rotation to compensate for lack of upper arm and forearm
movement, may be a skill that requires more advanced training. Physical and occupational
therapists should have the skills to identify these compensatory movements. The PT (Rater 1)
and OT (Rater 2) participated in the reliability study had higher overall ICCs (.91 and .97) than
the non-rehabilitation professional (Rater 3) (.89), although the non-professional still had an
overall excellent ICC. This trend held true for the total ICCs and SEMs. These results suggest
EMCE is an effective measure with excellent rater reliability. Evaluators with little training or
knowledge of movement analysis can still reliably use a well-established EMCE template to
assess quality of movement.
The SEM represents the standard deviation of measurement errors and reflects the extent
of expected error in repeated measurements or different raters’ scores.120, 121 The SEM is
expressed in the units of the measure, therefore allowing an error distribution to be established
around the measurement calculated. Measurement errors are assumed to be normally distributed;
therefore, there is a 95% probability that an individual’s true value would be within 2 SEMs of
the original measurement. For example, the 95% SEM for inter-rater reliability was ±1.02, so
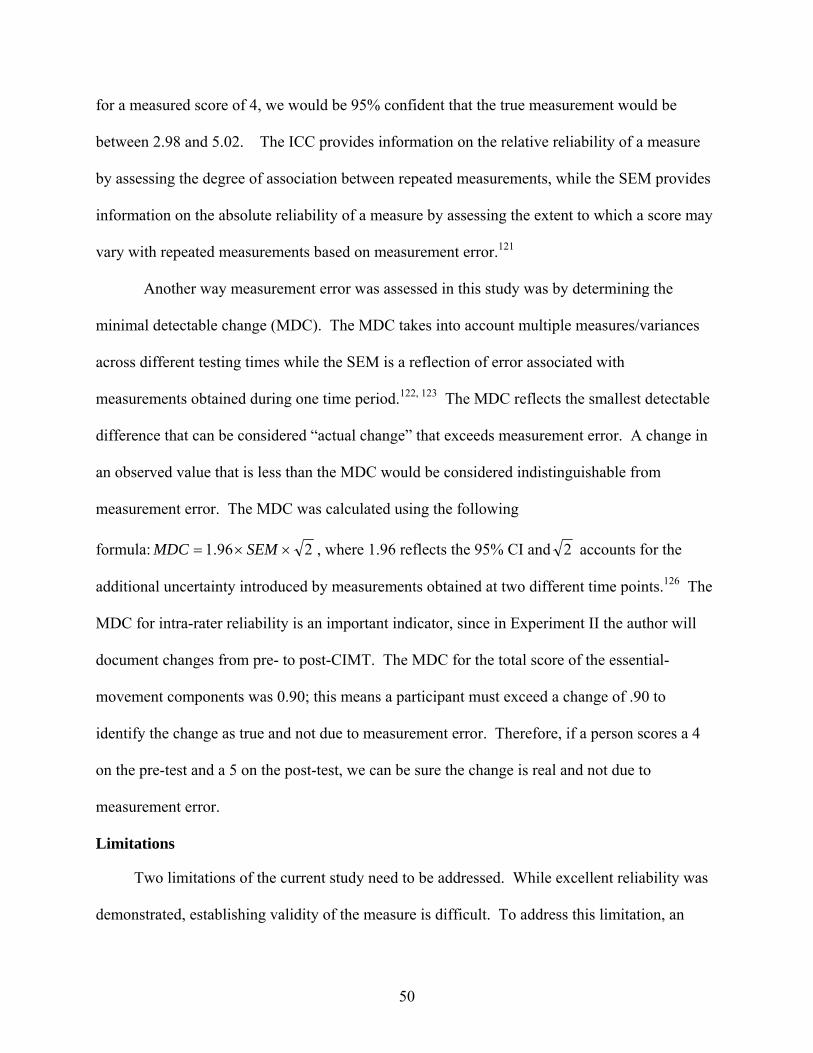
50
for a measured score of 4, we would be 95% confident that the true measurement would be
between 2.98 and 5.02. The ICC provides information on the relative reliability of a measure
by assessing the degree of association between repeated measurements, while the SEM provides
information on the absolute reliability of a measure by assessing the extent to which a score may
vary with repeated measurements based on measurement error.121
Another way measurement error was assessed in this study was by determining the
minimal detectable change (MDC). The MDC takes into account multiple measures/variances
across different testing times while the SEM is a reflection of error associated with
measurements obtained during one time period.122, 123 The MDC reflects the smallest detectable
difference that can be considered “actual change” that exceeds measurement error. A change in
an observed value that is less than the MDC would be considered indistinguishable from
measurement error. The MDC was calculated using the following
formula: 296.1 ××= SEMMDC , where 1.96 reflects the 95% CI and 2 accounts for the
additional uncertainty introduced by measurements obtained at two different time points.126 The
MDC for intra-rater reliability is an important indicator, since in Experiment II the author will
document changes from pre- to post-CIMT. The MDC for the total score of the essential-
movement components was 0.90; this means a participant must exceed a change of .90 to
identify the change as true and not due to measurement error. Therefore, if a person scores a 4
on the pre-test and a 5 on the post-test, we can be sure the change is real and not due to
measurement error.
Limitations
Two limitations of the current study need to be addressed. While excellent reliability was
demonstrated, establishing validity of the measure is difficult. To address this limitation, an
51
attempt was made to demonstrate validity in Experiment II by comparing the movements of a
person with stroke to “normal” movements in individuals without stroke, where normal
movement is considered the gold standard for validity purposes. Nevertheless, determination of
the validity of the current template in this study may be accomplished by future collaboration
with adequate biomechanical methods. Second, although utilization of the EMCE form showed
excellent inter-rater and intra-rater reliability, even for a non-rehabilitation professional, the
generalization of the EMCE method for functional activities of daily life can be limited. Future
study is necessary to develop the EMCE forms for other representative daily activities,127 such as
walking, eating and ascending/descending stairs. Researchers with appropriate training in
EWMN could develop EMCE forms for other key movements to effectively measure quality of
movement.
Conclusions
Quality of movement is an important indicator of post-stroke recovery, but has often been
ignored by rehabilitation professionals. In order to investigate post-stroke quality of movement,
the invariant features of the Generalized Motor Program (GMP) theory can serve as the research
framework in this study since the clarity of this theory allows us to establish the essentials of
human movement. Biomechanical methods may be useful to explore quality of movement, but
the requirement of expensive equipment and complicated computer software analyses can make
their application very difficult in clinical settings. The Eshkol-Wachman Movement Notation
(EWMN), therefore, was introduced to provide an effective and economical method. In this
study, the author developed an evaluation form based on a combined application of the GMP38, 85
and EWMN,90-92 measuring quality of movement that investigates invariant features for a
reaching-grasping-lifting-placing task.
52
Overall an excellent ICC value was established for this new outcome measure (the
Essential-Movement Component Evaluation form) that provides a systematic whole-body
movement analysis in a feasible manner. The combination of invariant features of the GMP and
EWMN method to study quality of movement in people with stroke is effective and reliable.
This measurement template does more than traditional assessments by evaluating the
contributions of the whole body to the activity, thus providing an additional means to assess
quality of movement. Novice investigators, even those without formal rehabilitation or
movement training, can reliably document movement using the established ECME form with
minimal training and practice.
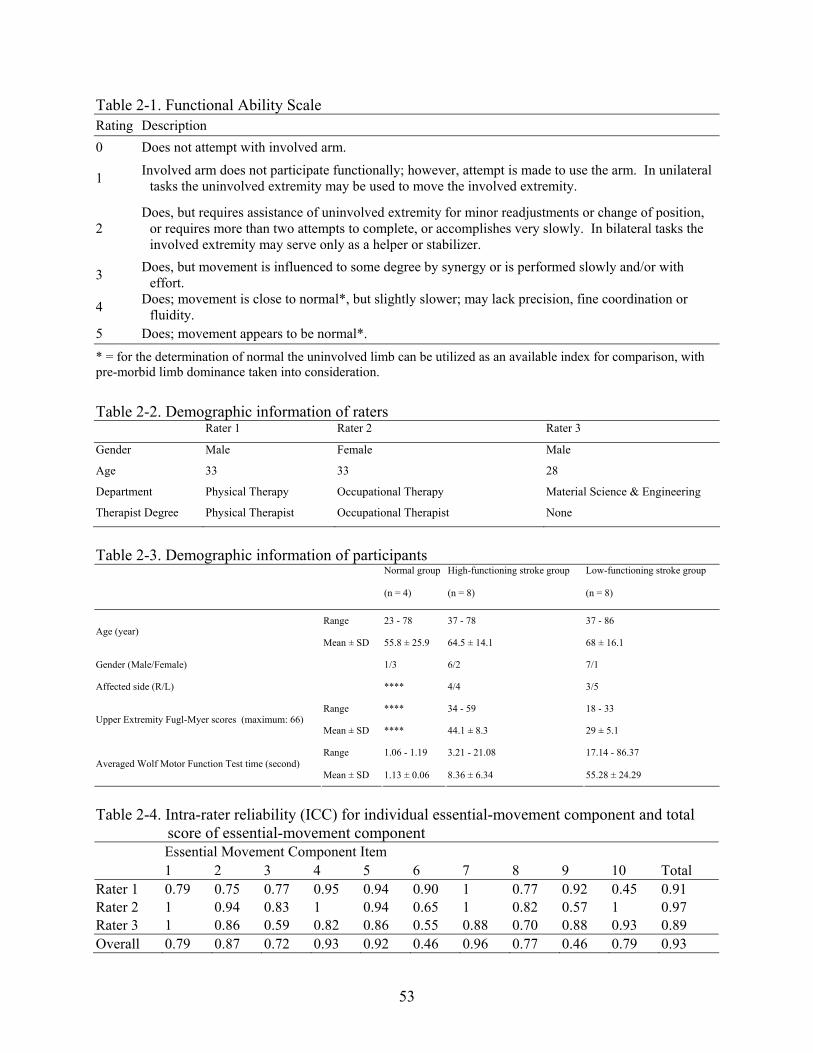
53
Table 2-1. Functional Ability Scale Rating Description 0 Does not attempt with involved arm.
1 Involved arm does not participate functionally; however, attempt is made to use the arm. In unilateral tasks the uninvolved extremity may be used to move the involved extremity.
2 Does, but requires assistance of uninvolved extremity for minor readjustments or change of position,
or requires more than two attempts to complete, or accomplishes very slowly. In bilateral tasks the involved extremity may serve only as a helper or stabilizer.
3 Does, but movement is influenced to some degree by synergy or is performed slowly and/or with effort.
4 Does; movement is close to normal*, but slightly slower; may lack precision, fine coordination or fluidity.
5 Does; movement appears to be normal*. * = for the determination of normal the uninvolved limb can be utilized as an available index for comparison, with pre-morbid limb dominance taken into consideration.
Table 2-2. Demographic information of raters Rater 1 Rater 2 Rater 3
Gender Male Female Male
Age 33 33 28
Department Physical Therapy Occupational Therapy Material Science & Engineering
Therapist Degree Physical Therapist Occupational Therapist None
Table 2-3. Demographic information of participants
Normal group High-functioning stroke group Low-functioning stroke group
(n = 4) (n = 8) (n = 8)
Range 23 - 78 37 - 78 37 - 86 Age (year)
Mean ± SD 55.8 ± 25.9 64.5 ± 14.1 68 ± 16.1
Gender (Male/Female) 1/3 6/2 7/1
Affected side (R/L) **** 4/4 3/5
Range **** 34 - 59 18 - 33 Upper Extremity Fugl-Myer scores (maximum: 66)
Mean ± SD **** 44.1 ± 8.3 29 ± 5.1
Range 1.06 - 1.19 3.21 - 21.08 17.14 - 86.37 Averaged Wolf Motor Function Test time (second)
Mean ± SD 1.13 ± 0.06 8.36 ± 6.34 55.28 ± 24.29
Table 2-4. Intra-rater reliability (ICC) for individual essential-movement component and total
score of essential-movement component Essential Movement Component Item 1 2 3 4 5 6 7 8 9 10 Total
Rater 1 0.79 0.75 0.77 0.95 0.94 0.90 1 0.77 0.92 0.45 0.91 Rater 2 1 0.94 0.83 1 0.94 0.65 1 0.82 0.57 1 0.97 Rater 3 1 0.86 0.59 0.82 0.86 0.55 0.88 0.70 0.88 0.93 0.89 Overall 0.79 0.87 0.72 0.93 0.92 0.46 0.96 0.77 0.46 0.79 0.93
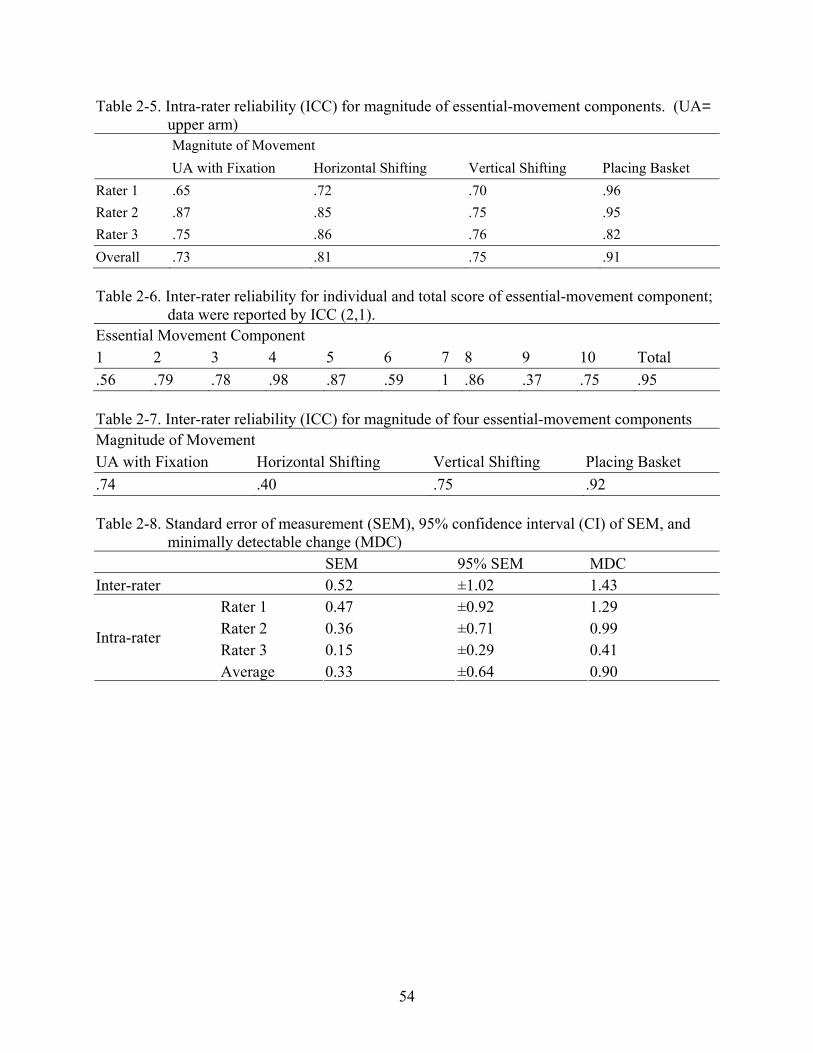
54
Table 2-5. Intra-rater reliability (ICC) for magnitude of essential-movement components. (UA= upper arm) Magnitute of Movement
UA with Fixation Horizontal Shifting Vertical Shifting Placing Basket
Rater 1 .65 .72 .70 .96 Rater 2 .87 .85 .75 .95 Rater 3 .75 .86 .76 .82 Overall .73 .81 .75 .91 Table 2-6. Inter-rater reliability for individual and total score of essential-movement component;
data were reported by ICC (2,1). Essential Movement Component 1 2 3 4 5 6 7 8 9 10 Total .56 .79 .78 .98 .87 .59 1 .86 .37 .75 .95 Table 2-7. Inter-rater reliability (ICC) for magnitude of four essential-movement components Magnitude of Movement UA with Fixation Horizontal Shifting Vertical Shifting Placing Basket .74 .40 .75 .92 Table 2-8. Standard error of measurement (SEM), 95% confidence interval (CI) of SEM, and
minimally detectable change (MDC) SEM 95% SEM MDC Inter-rater 0.52 ±1.02 1.43
Rater 1 0.47 ±0.92 1.29 Rater 2 0.36 ±0.71 0.99 Rater 3 0.15 ±0.29 0.41
Intra-rater
Average 0.33 ±0.64 0.90
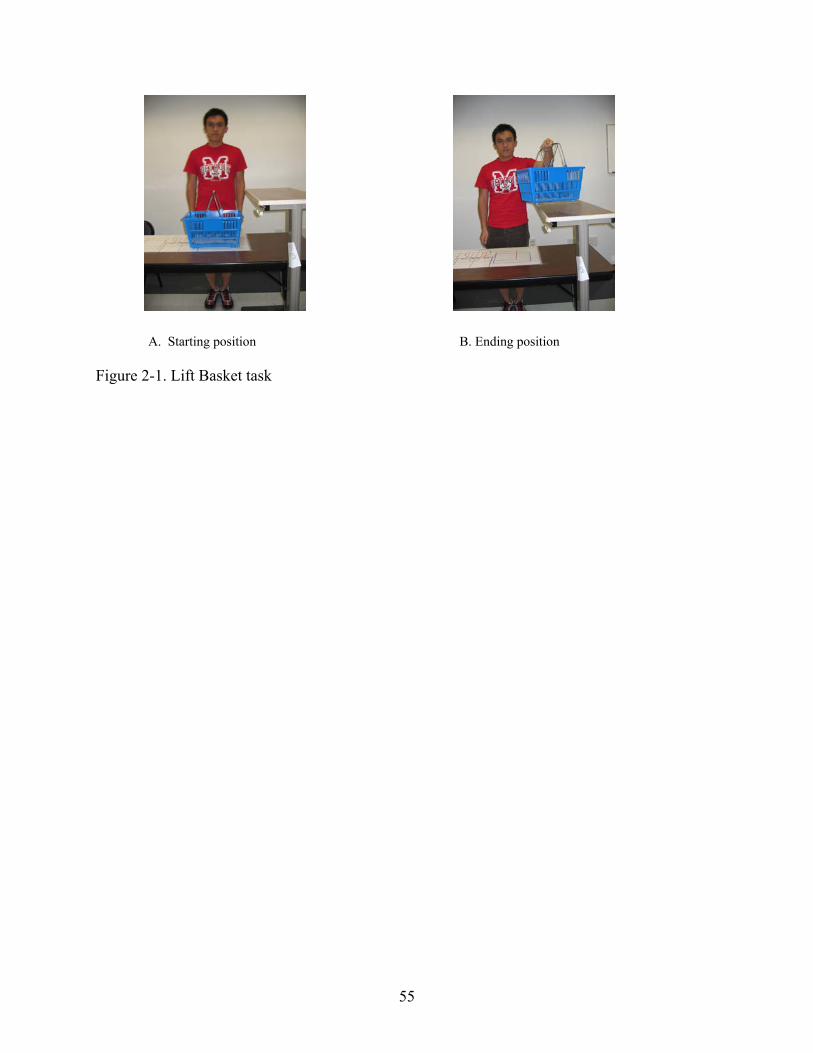
55
Figure 2-1. Lift Basket task
A. Starting position B. Ending position
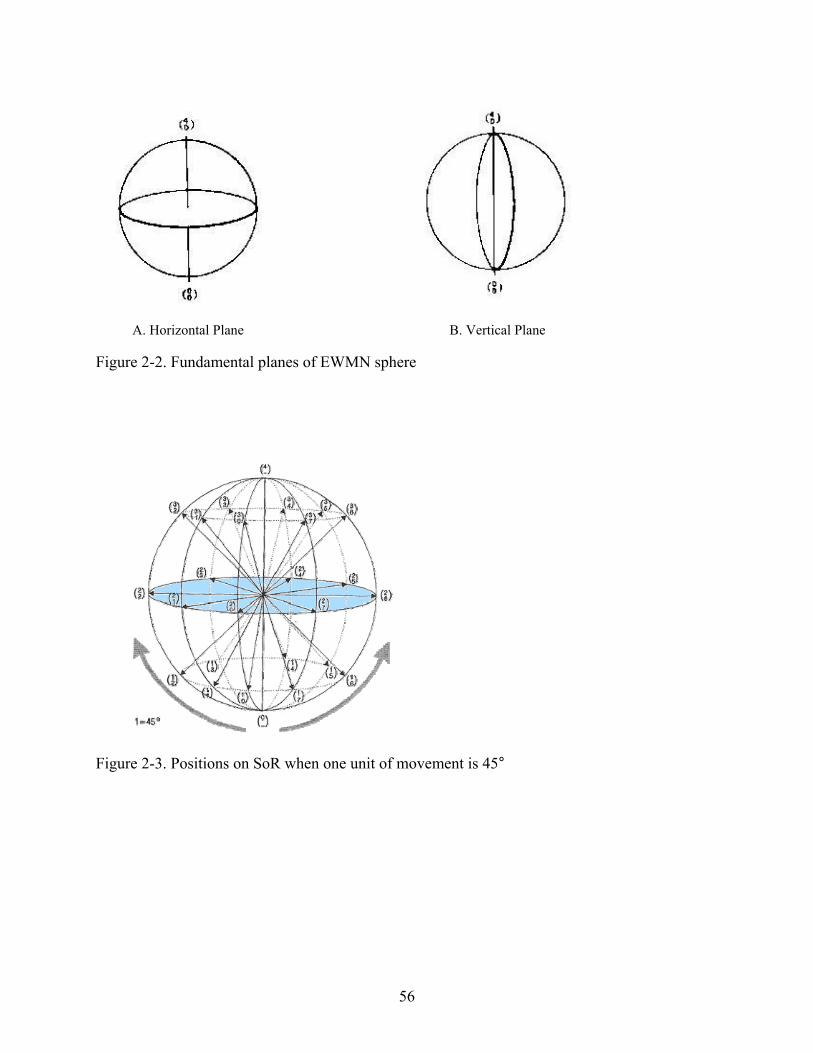
56
Figure 2-2. Fundamental planes of EWMN sphere
Figure 2-3. Positions on SoR when one unit of movement is 45°
A. Horizontal Plane B. Vertical Plane
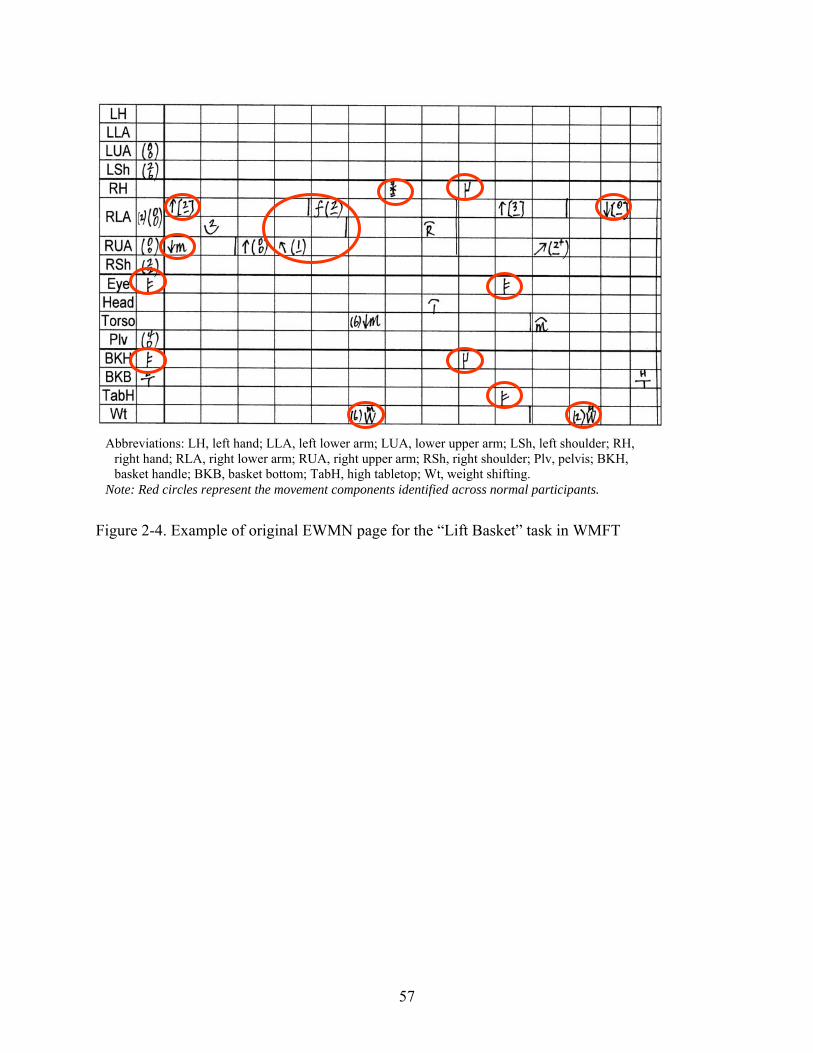
57
Figure 2-4. Example of original EWMN page for the “Lift Basket” task in WMFT
Abbreviations: LH, left hand; LLA, left lower arm; LUA, lower upper arm; LSh, left shoulder; RH, right hand; RLA, right lower arm; RUA, right upper arm; RSh, right shoulder; Plv, pelvis; BKH, basket handle; BKB, basket bottom; TabH, high tabletop; Wt, weight shifting.
Note: Red circles represent the movement components identified across normal participants.
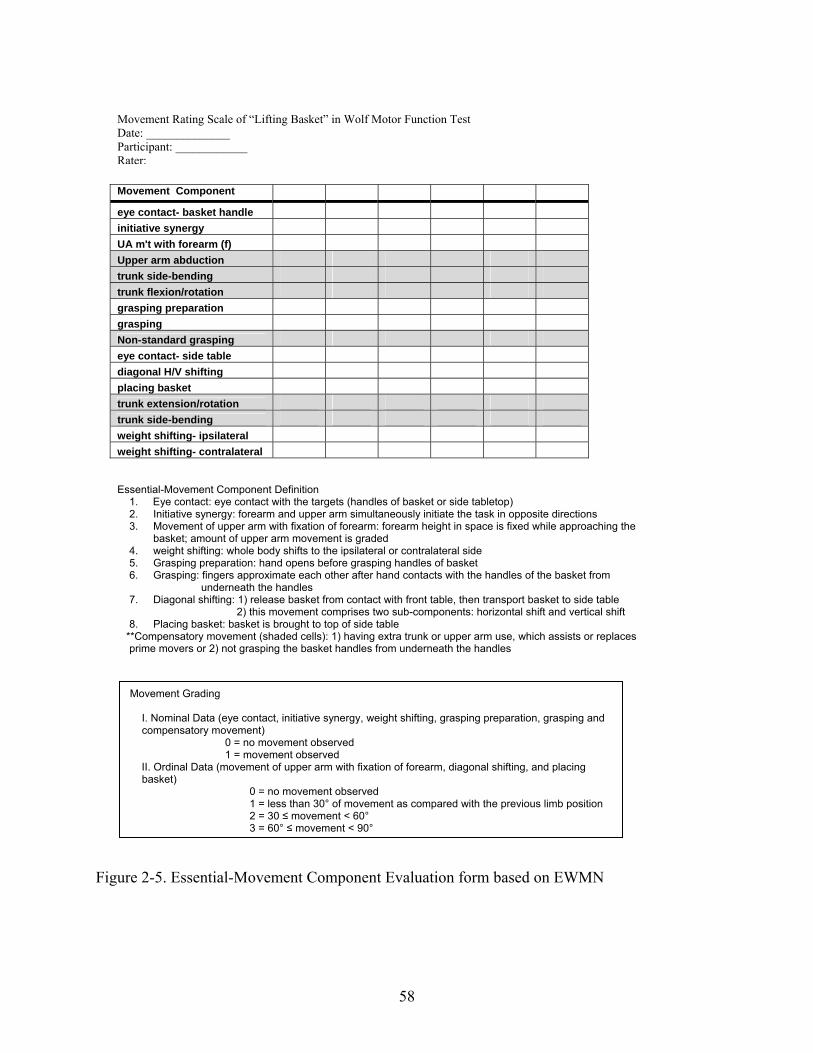
58
Figure 2-5. Essential-Movement Component Evaluation form based on EWMN
Movement Grading
I. Nominal Data (eye contact, initiative synergy, weight shifting, grasping preparation, grasping and compensatory movement)
0 = no movement observed 1 = movement observed
II. Ordinal Data (movement of upper arm with fixation of forearm, diagonal shifting, and placing basket)
0 = no movement observed 1 = less than 30° of movement as compared with the previous limb position 2 = 30 ≤ movement < 60° 3 = 60° ≤ movement < 90°
Movement Component eye contact- basket handle initiative synergy UA m't with forearm (f) Upper arm abduction trunk side-bending trunk flexion/rotation grasping preparation grasping Non-standard grasping eye contact- side table diagonal H/V shifting placing basket trunk extension/rotation trunk side-bending weight shifting- ipsilateral weight shifting- contralateral
Essential-Movement Component Definition 1. Eye contact: eye contact with the targets (handles of basket or side tabletop) 2. Initiative synergy: forearm and upper arm simultaneously initiate the task in opposite directions 3. Movement of upper arm with fixation of forearm: forearm height in space is fixed while approaching the
basket; amount of upper arm movement is graded 4. weight shifting: whole body shifts to the ipsilateral or contralateral side 5. Grasping preparation: hand opens before grasping handles of basket 6. Grasping: fingers approximate each other after hand contacts with the handles of the basket from
underneath the handles 7. Diagonal shifting: 1) release basket from contact with front table, then transport basket to side table
2) this movement comprises two sub-components: horizontal shift and vertical shift 8. Placing basket: basket is brought to top of side table
**Compensatory movement (shaded cells): 1) having extra trunk or upper arm use, which assists or replaces prime movers or 2) not grasping the basket handles from underneath the handles
Movement Rating Scale of “Lifting Basket” in Wolf Motor Function Test Date: ______________ Participant: ____________ Rater:
59
CHAPTER 3 ASSESSING MOVEMENT QUALITY AFTER STROKE
Introduction
Human movements reflect an individual’s personality, styles and culture. Movement is
used to manipulate our external environment and an expression of self emotion.128 There is a
natural “quality” to our movement. When movement capability is altered by a stroke, clients not
only lose motor function, but also their natural quality of movement.42, 45, 105, 107 Rehabilitation
therapists have always been concerned with attempting to recover movement quality. By
applying various strategies, therapists aim to enable the recovery process and facilitate the
movement restoration. For example, neuromuscular facilitation approaches were developed with
treatment oriented to improving movement patterns toward normality of movement.13, 129
In this day of insurance driven medicine, the concern of cost containment often causes
therapists to alter their expectations for clients to that of simply reaching task accomplishment
goals within a limited period of time, regardless of movement quality. Instead of focusing on
true recovery and normal movement restoration, compensatory strategies have played a dominant
role in current rehabilitation intervention. Quality of movement, nevertheless, does matter in our
daily life.103 Dancers strive for a smooth and coordinated move. Athletes pursue perfect
performance. So do people following a stroke. After our clients can perform certain
representative functional activities, such as walking and reaching, improvement in quality of
these movements becomes their next ultimate goal. A movement with poor quality may impede
their use of the affected extremities, especially in the public, and may further hamper social
participation.104
Clinicians and researchers have developed several instruments to measure movement
quality after stroke, but their attempts often focus on general functional ability of specific
60
affected body parts rather than quality of movement in a whole-body view. Examples of these
measurements include the Functional Activity Scale (FAS) in the Wolf Motor Function Test
(WMFT),50, 102 the Quality of Movement Scale (QoM) in the Motor Activity Log,1 the Motor
Evaluation Scale for Upper Extremity in Stroke Patients (MESUPES),106 and movement pattern
analyses.13, 107 Ordinal motor function scales, such as FAS and QoM, are used extensively in
studies of stroke intervention effectiveness.54-58 Motor function scales are feasible and helpful
for healthcare providers, but a statistically significant change of averaged scores can merely
indicate an incremental change along that scale72 and provide limited information about
improvement in function and quality of movement. MESUPES is a scale of movement quality
that encompasses eight arm function items with six rating categories and nine hand function
items with three rating categories.106 The grading system does not have a uniform definition
across the items. In addition, the composite score generated may simply indicate the level of
assistance required while performing the tasks, rather than quality of the movement. Two
examples of movement pattern analysis include Bobath’s test for quality of movement patterns13
and Cirstea’s biomechanical movement variable analysis.17, 42, 75, 107 The tasks used by Bobath
mainly examine the ability of active selective control of the affected body parts and are not
directly related to functional movement. As for Cirstea’s biomechanical method, the derivatives
from advanced calculations of biomechanical parameters can actually generate great confusion
and difficulty for clinicians without providing sufficient direct information about the
movement.130, 131 Developing a clinically feasible and reliable method to measure post-stroke
movement quality, therefore, becomes necessary for advancing evaluation skills of clinicians to
determine effectiveness of stroke interventions.
61
Recently, Chiu has developed an evaluation template, the Essential-Movement Component
Evaluation (EMCE) form to measure quality of movement.132 The development of EMCE was
based on a combined application of the Generalized Motor Program (GMP) theory38, 85 and the
Eshkol-Wachman Movement Notation (EWMN) method.90-92 The EMCE form had an excellent
overall intra-rater [ICC(2,1)= .93; 95% CI= .88-.96; p< 0.001 ] and inter-rater reliability
[ICC(2,1)= .95; 95% CI= .89-.98; p< 0.001].132 In addition, the EMCE form had a small
standard error of measurement (SEM= .33) and minimally detectable change (MDC= ±0.9).132
The high ICCs and subsequent low SEMs indicated that novice investigators, even those without
formal rehabilitation training, can reliably document movement using the established ECME
form and a short training and practice session. Evaluators with little training or knowledge of
movement analysis can still reliably use a well-established EMCE template to assess quality of
movement in terms of movement components, sequence and strategy.
The effectiveness, reliable, economical, and user-friendly features of EMCE have made
its future use feasible in clinical and research settings. The objective of this research was to
present a method of measuring movement quality and to explore if this method can distinguish
problematic movement patterns observed in people with stroke.
Method
Participants
Fifty participants were randomly selected from four CIMT studies that were conducted at
the Department of Physical Therapy, University of Florida and the Brain Rehabilitation Research
Center, Malcom Randall Veteran Affairs Medical Center, Gainesville, Florida. Participant
characteristics were presented, including age, gender, side of stroke and time since stroke.(Table
3-1) Three groups were included in this experiment: participants without stroke (normal group;
62
n= 10), high-functioning participants with stroke (n= 20) and low-functioning participants with
stroke (n= 20).
The participants with stroke were divided into two groups using their upper-extremity
Fugl-Meyer motor scores: high-functioning (scores > 33) and low-functioning group (scores ≤
33). The Fugl-Meyer Assessment110 (see Appendix C) is regarded as an objective and
quantifiable assessment of motor impairment. The Fugl-Meyer Assessment is also a
standardized assessment to measure recovery after stroke. The upper-extremity Fugl-Meyer
motor component (total score = 66) assesses the ability to move in/out of synergy, reflexes, wrist
stability, grasping ability, and coordination. In stroke rehabilitation research, the Fugl-Meyer
Assessment is frequently used as a primary outcome measure of impairment,74, 111 and has been
shown to be predictive of dependency, functional level and recovery after stroke.58, 112-114
The inclusion criterion for the control group was that they had no prior history of
neurological disorders. All participants with stroke in this experiment met the following
inclusion criteria: 1) the diagnosis of at least one stroke, but not more than three strokes on the
same side of the brain, 2) stroke at least three months prior to study participation, 3) ability to
follow simple instructions, 4) a score of 20 or higher on the Mini Mental-State Exam,115 5) the
ability to sit independently without back or arm support for two minutes, 6) the ability to stand
with support of a straight cane, quad cane or hemi-walker for two minutes, 7) the ability to
actively participate for six hours of therapy without long rests or nap periods, 8) passive range-
of-motion of all upper-extremity motions of at least half the normal range, 9) traditional CIMT
minimal motor criteria.1, 67, 116-118 Minimal motor criteria were defined as active movement of
the wrist through at least 20 degrees of extension from a relaxed flexed position, and active
63
movement of at least three fingers (the thumb and two fingers) 20 degrees of extension at the
metacarpal-phalangeal and proximal interphalangeal joints.
Exclusion criteria for both stroke groups included 1) any health problems that put the
individual at significant risk of harm during the study, 2) any other neurological conditions such
as multiple sclerosis or Parkinson’s disease, 3) taking drugs for spasticity, 4) pain that is scored
greater than 5/10 on the McGill Pain Scale119. Furthermore, the participants were excluded if
they could not independently reach the handle of the basket for the “Lift Basket” task of the
WMFT in a standing position with or without support of a straight cane, quad cane or hemi-
walker within two minutes.
Procedure
All data used in this experiment were retrospectively retrieved from four previously
completed studies. All participants signed a consent form that was pre-approved by the
Institutional Review Board of University of Florida for permission to be tested and to have their
videotapes analyzed for movement control. The participants without stroke were recruited from
the local community and only received one test, the Wolf Motor Function Test (WMFT),1, 50, 64,
65, 101 which is a standardized evaluation tool in traditional CIMT.1, 65 The participants with
stroke first received a series of pre-test evaluations that included the WMFT.1, 50, 64, 65, 101
The movement task selected for this study was the “Lift Basket” task of the WMFT. The
WMFT is a standardized test and one of the primary outcomes in the CIMT studies.1, 50, 57, 58, 64,
67, 68, 74, 101 The WMFT consists of a series of 15 timed tasks and two strength tasks that are
performed in either a sitting or standing position. The 15 tasks are arranged in order of
biomechanical complexity according to the joints involved and the level of difficulty. The tasks
progress from proximal to distal joint involvement and from gross to fine motor skills.50 A
recent pilot study of Rasch measurement conducted by Wen and Velozo (unpublished) in 2003,
64
however, has shown a different order of task difficulty. This indicates that Wolf’s conceptual
task complexity is not reflected in participants’ responses. For example, the last task, Lift Basket,
which was supposed to be the most difficult task of WMFT became the second difficult task.
The WMFT quantifies upper-extremity movement ability through timed single- or multiple-joint
motions and functional tasks.50
The last task in the WMFT, “Lift Basket,” is regarded as a complex task that demands
efforts from multiple body systems, such as muscle strength, dynamic/standing balance, and
inter-limb coordination. The Rasch pilot study of Wen and Velozo (unpublished) demonstrated
the “Lift Basket” task to be the second most difficult task of the WMFT in terms of item
difficulty analysis. As compared with a simple activity, such as reaching for an object on a table,
“Lift Basket” is a representative activity with greater difficulty in our daily life. This task
requires involvement from the whole body. Studying this task, therefore, can show how one
body part interacts with others during movement. Moreover, the “Lift Basket” task is an “out of
synergy” movement that can target the limitations people with stroke have when performing a
reaching and lifting task.88
“Lift Basket” task. The set-up of the “Lift Basket” task included a basket, a desk (29”
high) located in front of the participant and a bedside table (44” high) located on the participant’s
side to be tested. (see Figure 3-1A and 3-1B) The bedside table extended along the width of the
desk. The basket was placed on the desk and lined up with the center of the participants’ body.
A three-pound weight was placed in the basket. Participants are tested in a standing position
while facing the desk. The set-up of the “Lift Basket” task is illustrated with its starting position
(Figure 3-1A) and ending position (Figure 3-1B). The task description was “Patient attempts to
pick up basket by grasping handle (from underneath the handle) and placing the basket on far
65
edge of the rolling bedside table.” All participants were asked to “Pick up the basket with your
hand and place the basket on the rolling table. The far edge of the basket should go past the far
edge of the bedside table. Try not to move your feet while you do this task. Do this as quickly
as you can.”102 The subject’s movement progression was videotaped from a front view.
Participants’ video tapes were then converted to DVD in digital format using a Panasonic DVD
recorder (model DMR-E95HS) for further analyses of EWMN.
In this study, the motion videos of the “Lift Basket” task of WMFT pre-test were randomly
selected from the three groups. The fifty videos tapes were converted to DVD in digital format
using a Panasonic DVD recorder (model DMR-E95HS) for further analyses of EWMN. In the
laboratory, a physical therapist with three-year EWMN training experience played video clips
frame-by-frame (30 frames/second) to grade participants’ movement using a Pioneer DVD
player (model DVD-V7400). The EMCE form (see Appendix B) was used to analyze
participants’ movement quality in terms of movement component, sequence, and strategy.
The essential-movement components were first graded by whether a movement component
was observed (0= No; 1= Yes). The range of essential-movement component composite score is
0 to 10. Three essential-movement components were further graded by how much range-of-
motion is observed (0= no movement observed; 1= 0º ≤ movement < 30º; 2= 30º ≤ movement <
60º; 3= 30º ≤ movement < 60º). The three essential-movement components were upper-arm
movement with forearm fixation, diagonal shifting of upper arm (including horizontal and
vertical shifting), and forearm movement to place the basket. These essential components were
chosen since their range-of-motion can be visually measured. The compensatory movement was
graded by whether a compensatory movement is observed. (0= No; 1= Yes) The range of
compensatory movement composite score is 0 to 5.
66
Data Analysis
One-way analysis of variance (ANOVA) was used to determine if there were any
statistically significant differences in essential-movement component composite scores,
compensatory movement composite scores and movement magnitude of three essential-
movement components between three groups (normal, high-functioning and low-functioning).
The significant level was set at .05. In addition, the Scheffe post-hoc multiple comparison
analysis was used to determine pair-wise significance. The prevalence for each essential-
movement component and compensatory movement was reported in percentage.
Results
The one-way ANOVA results are presented. (Table 3-2) All p values of the dependent
variables were less than .001, including the essential-movement component total score, the
compensatory movement total score, and the movement magnitude of the three essential-
movement components. Most of the Scheffe post-hoc multiple comparison analyses were
statistically significant, except for upper-arm diagonal shifting (high-functioning vs. normal),
total score of compensatory movement (high-functioning vs. low-functioning), and upper-arm
movement with forearm fixation (high-functioning vs. low-functioning). Percentages of
observed movement component and compensatory movement from the three groups were
reported. (Table 3-3) The percentage of every essential-movement components observed from
the three groups decreased as impairment level increased, except for the contralateral weight
shifting which was the same for three groups. Percentages of observed compensatory movement
increased as impairment level increased. A small percentage of compensatory movement was
noticed in the normal group as well.
67
Discussion
The results from the ANOVAs showed there were statistically significant differences
between the means of the groups for total score of essential-movement components, the total
score of compensatory movements, and the movement magnitude of the three essential-
movement components. In accordance with the hypothesis, the results suggested that the EMCE
form for the Lift Basket task was able to effectively distinguish the differences between normal
individuals and the two different stroke groups. As for the post-hoc analyses, no significant
differences were found in the movement magnitude of the upper-arm horizontal and vertical
shifting between the high-functioning and normal group. These non-significant results suggest
that in the high-functioning stroke group the movement of the upper-arm was not significantly
different during this lifting component than the normal group. No significant differences were
noted, however, between the high- and low-functioning groups in the total score of
compensatory movements or in the magnitude of upper-arm movement with forearm fixation.
Unlike the lifting component, during the early phase of reaching (i.e. upper-arm movement with
fixation) the high-functioning group was not statistically different than that of the low-
functioning group. A possible explanation can be that the high-functioning stroke group adopted
compensatory movement during reaching even when their function was improved. The
compensatory movements observed included movement initiation with upper-arm abduction,
trunk side-bending, and trunk forward rotation. Adopting these compensatory movements in the
high-functioning stroke group can be an indication of the habitual movement strategy that
followed the previous atypical synergy while their upper extremity function was still limited.
The percentage of every essential-movement component in the two stroke groups was
observed less as impairment level increased, except for contralateral weight shifting which was
the same for both the high and low functioning groups. People with stroke have the tendency to
68
bear their weight on the less affected side, but have difficulty in shifting the weight to the
affected side.44, 133 The inability to shift body weight from one side to another may cause
decreased ability to engage in dynamic activities, such as reaching or walking.134 The most
impaired essential-movement components found in the low-functioning stroke group included
initiative synergy (preparation for reaching), forearm fixation (aiming), grasp preparation (hand
opening), grasp, eye contact to high table (estimation for height of lifting), upper-arm diagonal
shifting (upper-arm strength), and placing basket (elbow extension). The initiative synergy is an
essential-movement component that acted as a preparatory step of reaching. Instead of moving
the upper arm directly to the target, the forearm and upper arm simultaneously initiated the task
in opposite directions (i.e. a couple movement of shoulder extension and elbow flexion on the
sagittal plane). Then the forearm and upper arm move forward toward the basket handle. This
short time delay caused by the initiative synergy provides the forearm an opportunity to prepare
its appropriate position for later reaching. Forearm fixation is an aiming movement that keeps
the forearm in a fixed height until the hand reaches to the target.
According to the GMP theory, actions controlled by the same GMP share the same
invariant features, such as the sequencing of submovements, relative timing and relative forces.
Movements governed by the same GMP differ from each other in the assignment of variant
movement parameters, for instance absolute time, absolute force, and selection of effectors.38, 85,
86 In line with the GMP theory, invariant submovements in a fixed movement sequence can be
identified when different individuals execute the same activity. In this experiment, decreased
use of essential-movement component with the increase of compensatory movements was found
as impairment level increased. These results indicated that the motor programming may be
altered in people with stroke. Having less essential-movement components forced individuals
69
with stroke to adopt more compensatory movements. Underutilized essential-movement
components in stroke groups provide clinicians a useful direction of treatment. Instead of simply
emphasizing repetition and speed, an effective training program may also focus on restoring
underutilized essential-movement components in a sequencing manner.
Compensatory movements were found in all three groups, but the prevalence increased as
impairment levels increased from normal, to high-functioning, to low-functioning. Possible
reasons for the normal group adopting compensatory movements were inaccurate basket
placement, short body structure, or muscle weakness. When these conditions exist, the upper
arm and trunk may need to compensate for the discrepancy in the position of the basket. For the
low-functioning stroke group, however, compensatory movements were often substituted for
essential-movement components, which may indicate the inability to recruit certain body parts17,
42, 45, 75, 89, 135, 136 or muscle weakness.8, 10, 11, 18, 19 Additionally, the proximal body parts, which
include upper arm and trunk, often dominated the movement or incorrectly initiated the
movement, for example, the movement was initiated by trunk side-bending or upper arm
abduction. For the high-functioning group, while the essential-movement components were
observed, compensatory movements still appeared, but functioned as assistance for the essential-
movement components.
Whether compensatory movement is a necessary post-stroke adaptation, which should not
be corrected remains controversial.137-139 Some recent studies, however, have shown that
emphasis on training certain underutilized movement components during reaching, such as
elbow and shoulder range-of-motion can significantly improve movement quality.107, 140 On the
other hand, restraint of the trunk to prevent its compensatory contribution toward a reaching or
pointing task, while training, can actually induce more upper extremity movement89, 135, 136, 141

70
Trunk restraint allows patients with stroke to make use of arm joint ranges that are present but
not normally recruited during unrestrained arm-reaching tasks. Thus, the underlying "normal"
patterns of movement coordination may not be entirely lost after a stroke and underutilized
essential-movement component may be restorable.135 In order to improve quality of movement,
therefore, restoration of underused essential-movement component and reduction or inhibition of
compensatory movements may be two priority goals for treatment.
Limitations. Improper experiment set-up for videotaping was noticed during reviewing
movement clips. Different locations where the basket was placed or different starting position of
the task may induce unnecessary compensatory movements that were observed in normal
individuals. The EMCE has shown to be a reliable research template to investigate quality of
movement, but the generalization of the results from this experiment can be limited due to
specificity of task nature. Future development of EMCE for other representative activities of
daily life is necessary to improve external validity.
Conclusions
The EMCE form for the Lift Basket task was able to effectively distinguish the differences
between normal individuals and the two different stroke groups. Statistically significant
differences in quality of movement were found between normal individuals and people with
stroke. The percentage of essential-movement component observed from the two stroke groups
decreased as impairment level increased. Compensatory movements were found in all three
groups, but prevalence increased as impairment level increased from normal, to high-
functioning, to low-functioning. Underutilized movement components and dominance of
compensatory movements can provide rehabilitation professional useful information on
developing tailored therapeutic programs to restore disrupted movement patterns in the stroke
population.
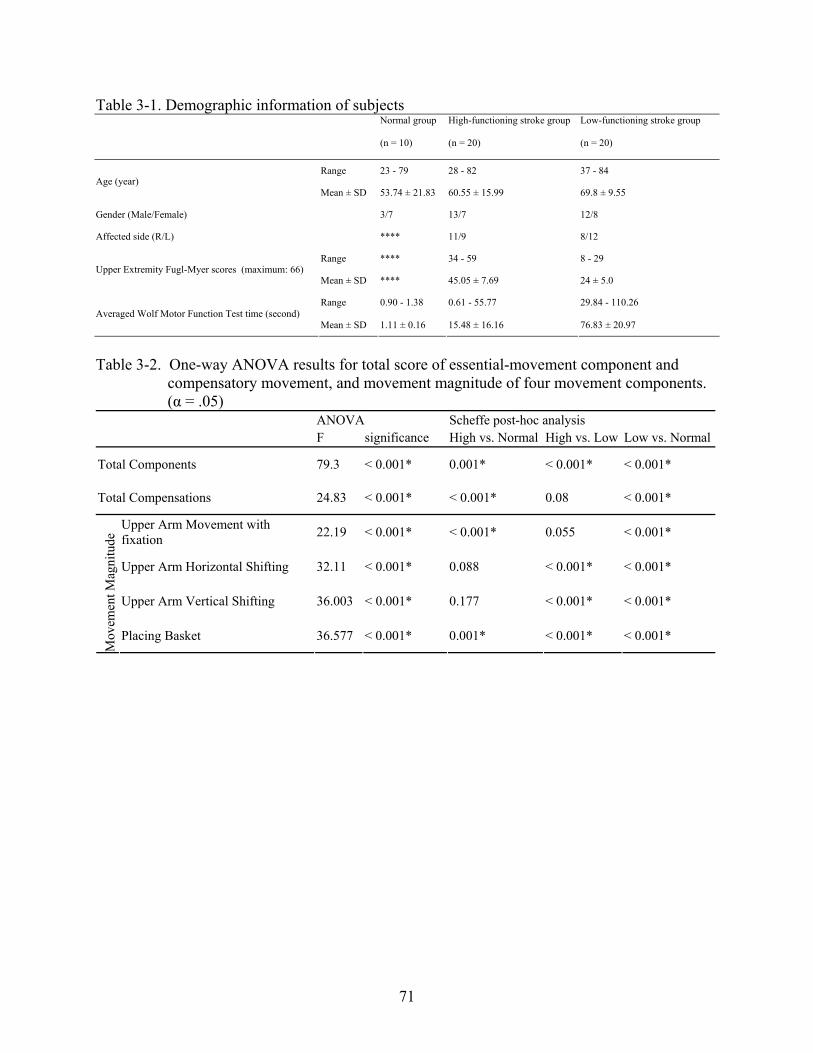
71
Table 3-1. Demographic information of subjects Normal group High-functioning stroke group Low-functioning stroke group
(n = 10) (n = 20) (n = 20)
Range 23 - 79 28 - 82 37 - 84 Age (year)
Mean ± SD 53.74 ± 21.83 60.55 ± 15.99 69.8 ± 9.55
Gender (Male/Female) 3/7 13/7 12/8
Affected side (R/L) **** 11/9 8/12
Range **** 34 - 59 8 - 29 Upper Extremity Fugl-Myer scores (maximum: 66)
Mean ± SD **** 45.05 ± 7.69 24 ± 5.0
Range 0.90 - 1.38 0.61 - 55.77 29.84 - 110.26 Averaged Wolf Motor Function Test time (second)
Mean ± SD 1.11 ± 0.16 15.48 ± 16.16 76.83 ± 20.97
Table 3-2. One-way ANOVA results for total score of essential-movement component and
compensatory movement, and movement magnitude of four movement components. (α = .05)
ANOVA Scheffe post-hoc analysis F significance High vs. Normal High vs. Low Low vs. Normal
Total Components 79.3 < 0.001* 0.001* < 0.001* < 0.001*
Total Compensations 24.83 < 0.001* < 0.001* 0.08 < 0.001*
Upper Arm Movement with fixation 22.19 < 0.001* < 0.001* 0.055 < 0.001*
Upper Arm Horizontal Shifting 32.11 < 0.001* 0.088 < 0.001* < 0.001*
Upper Arm Vertical Shifting 36.003 < 0.001* 0.177 < 0.001* < 0.001*
Mov
emen
t Mag
nitu
de
Placing Basket 36.577 < 0.001* 0.001* < 0.001* < 0.001*
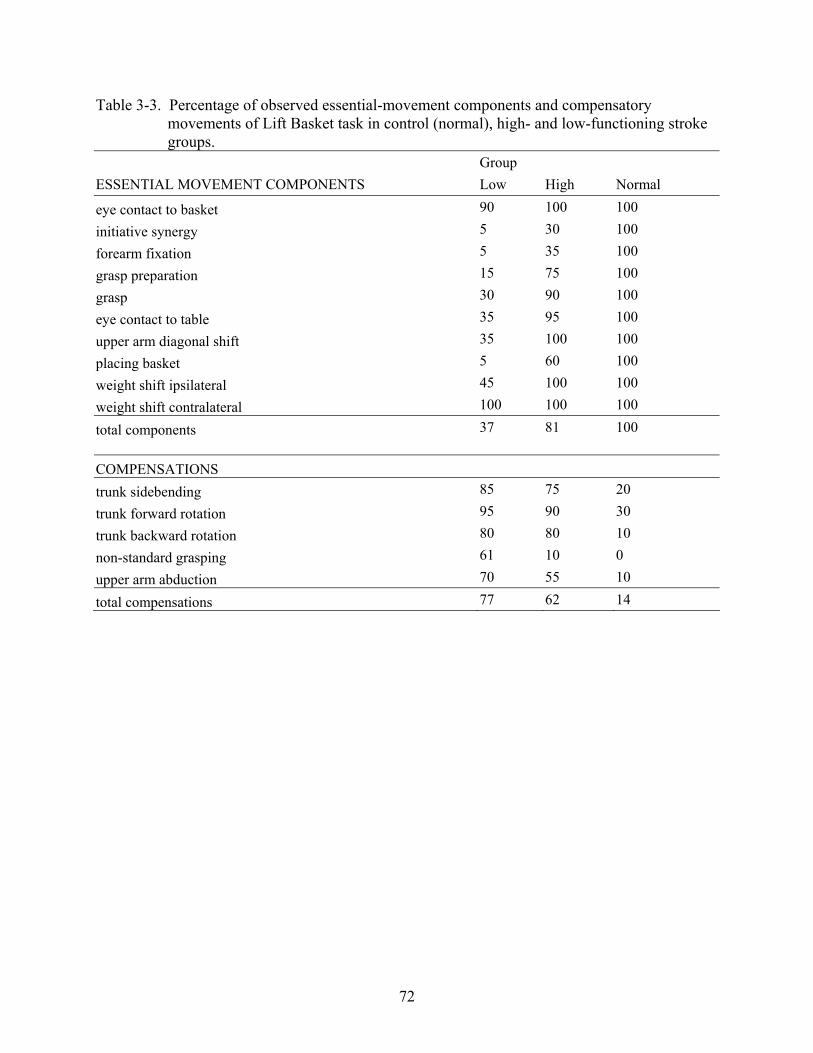
72
Table 3-3. Percentage of observed essential-movement components and compensatory movements of Lift Basket task in control (normal), high- and low-functioning stroke groups.
Group ESSENTIAL MOVEMENT COMPONENTS Low High Normal
eye contact to basket 90 100 100
initiative synergy 5 30 100
forearm fixation 5 35 100
grasp preparation 15 75 100
grasp 30 90 100
eye contact to table 35 95 100
upper arm diagonal shift 35 100 100
placing basket 5 60 100
weight shift ipsilateral 45 100 100
weight shift contralateral 100 100 100
total components 37 81 100 COMPENSATIONS
trunk sidebending 85 75 20
trunk forward rotation 95 90 30
trunk backward rotation 80 80 10
non-standard grasping 61 10 0
upper arm abduction 70 55 10
total compensations 77 62 14
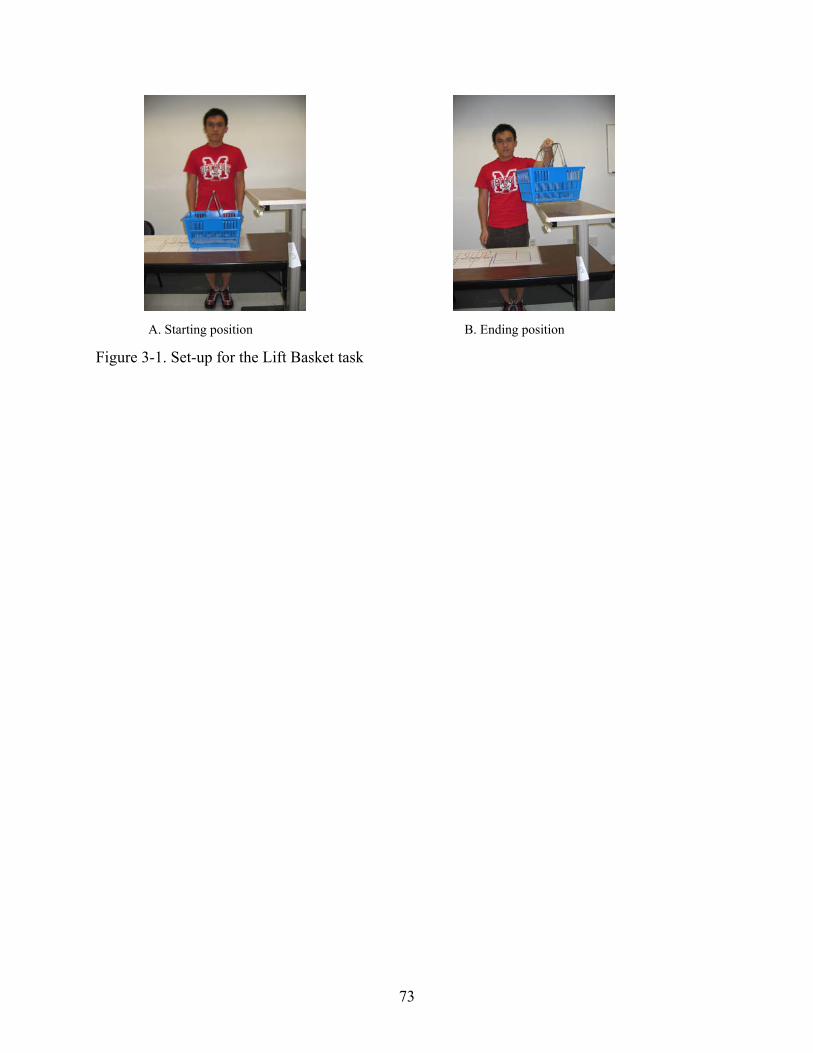
73
Figure 3-1. Set-up for the Lift Basket task
A. Starting position B. Ending position
74
CHAPTER 4 EFFECTS OF CONSTRAINT-INDUCED MOVEMENT THERAPY ON QUALITY OF
MOVEMENT POST-STROKE
Introduction
Constraint-Induced Movement Therapy (CIMT)1, 67, 68 has been a promising rehabilitation
strategy during the past two decades. CIMT is mainly used in the post-stroke population The
hypothesis of CIMT is that restraint of the less-affected upper-extremity will force the more-
affected extremity to overcome the phenomenon of “learned nonuse.”66, 67 Based on animal
studies in which primates received surgical deafferentation of one upper-extremity, “learned
nonuse” was defined as “an adverse learning cycle caused by unsuccessful motor attempts with
the deafferented arm that resulted in pain, failure or uncoordinated movements.”1 The ultimate
goals of CIMT are to break the adverse “learned nonuse” cycle and to further improve functional
use of the affected upper-extremity.
While substantial research evidence supports benefits of CIMT,1, 67, 68, 71, 105, 114, 118, 142, 143
limited evidence is available regarding the underlying mechanisms that account for improved
motor function.143 One of the most common reported outcomes is the Wolf Motor Function Test
(WMFT).1, 50, 57, 67, 68, 102 Outcomes of WMFT have two parts: time to complete a task and score
on an ordinal scale (Functional Ability Scale). The resultant data indicate changes in movement
efficiency and use of affected extremity. This information, however, does not allow
investigators to address direct changes in quality of movement. Is a faster movement a better
movement? Do patients with stroke recover their pre-stroke movement after CIMT? Do patients
with stroke adopt compensatory strategies to perform tasks more efficiently after CIMT?
In order to answer these questions, the author has developed the Essential-Movement
Component Evaluation (EMCE) form, a research template to evaluate quality of movement. The
development of EMCE was based on a combined application of the Generalized Motor Program
75
(GMP) theory38, 85 and the Eshkol-Wachman Movement Notation (EWMN) method.90-92 EMCE
can provide crucial information about composition of a movement (i.e. movement component,
sequence and strategy) and influence of compensatory movement. In addition, EMCE was
shown to have an excellent inter-rater [ICC(2,1)= .95; 95% CI= .89-.98; p< 0.001] and intra-rater
reliability [ICC(2,1)= .93; 95% CI= .88-.96; p< 0.001] according to our previous study.132 In
addition, the EMCE form had a small standard error of measurement (SEM= .33) and minimally
detectable change (MDC= ±0.9).132 The high ICCs and subsequent low SEMs indicated that
novice investigators, even those without formal rehabilitation training, can reliably document
movement using the established ECME form and a short training and practice session.
Evaluators with little training or knowledge of movement analysis can still reliably use a well-
established EMCE template to assess quality of movement in terms of movement components,
sequence and strategy. The aims of this study were 1) to determine the effects of CIMT on
quality of movement measured by EMCE, and 2) to systematically categorize compensatory
movement used in persons with stroke pre- and post-CIMT.
Methods
Participants
Sixty participants were randomly selected from four CIMT studies that were conducted at
the Department of Physical Therapy, University of Florida and the Brain Rehabilitation Research
Center, Malcom Randall Veteran Affairs Medical Center, Gainesville, Florida. Primary
participant characteristics were presented, including age, gender, side of stroke and time since
stroke.(Table 4-1) Two groups of participants were included in this experiment: high-
functioning participants with stroke (n= 30), and low-functioning participants with stroke (n= 30).
The participants with stroke were divided into two groups using their upper-extremity
Fugl-Meyer motor scores: high-functioning (scores > 33) and low-functioning group (scores ≤
76
33). The Fugl-Meyer Assessment110 (see Appendix C) is regarded as an objective and
quantifiable assessment of motor impairment. The Fugl-Meyer Assessment is also a
standardized assessment to measure recovery after stroke. The upper-extremity Fugl-Meyer
motor component (total score = 66) assesses the ability to move in/out of synergy, reflexes, wrist
stability, grasping ability and coordination. In stroke rehabilitation research, the Fugl-Meyer
Assessment is frequently used as a primary outcome measure of impairment,74, 111 and has been
shown to be predictive of dependency, functional level and recovery after stroke.58, 112-114
All participants with stroke in this experiment met the following inclusion criteria: 1) the
diagnosis of at least one stroke, but not more than three strokes on the same side of the brain, 2)
stroke at least three months prior to study participation, 3) ability to follow simple instructions,
4) a score of 20 or higher on the Mini Mental-State Exam,115 5) the ability to sit independently
without back or arm support for two minutes, 6) the ability to stand with support of a straight
cane, quad cane or hemi-walker for two minutes, 7) the ability to actively participate for six
hours of therapy without long rests or nap periods, 8) passive range-of-motion of all upper-
extremity motions of at least half the normal range, 9) traditional CIMT minimal motor criteria.1,
67, 116-118 Minimal motor criteria were defined as active movement of the wrist through at least 20
degrees of extension from a relaxed flexed position, and active movement of at least three fingers
(the thumb and two fingers) 20 degrees of extension at the metacarpal-phalangeal and proximal
interphalangeal joints.
Exclusion criteria for both stroke groups include 1) any health problems that put the
individual at significant risk of harm during the study, 2) any other neurological conditions such
as multiple sclerosis or Parkinson’s disease, 3) taking drugs for spasticity, 4) pain that is scored
greater than 5/10 on the McGill Pain Scale119. Furthermore, the participants were excluded if
77
they could not independently reach the handle of the basket for the “Lift Basket” task of the
WMFT with or without support of a walking assistive device within the two-minute time period.
Procedure
All data used in this experiment were retrospectively retrieved from four previously
completed studies. All participants signed a consent form that was pre-approved by the
Institutional Review Board of University of Florida for permission to be videotaped and have
their videotapes analyzed for movement control. The participants with stroke first received a
series of pre-test evaluations that included the WMFT,1, 50, 64, 65, 101 which is a standardized
evaluation in traditional CIMT.1, 65
After completing the pre-test evaluations, the participants with stroke received two weeks
(ten consecutive weekdays) of CIMT. During the two-week intervention, the less-affected hand
was immobilized in a padded mitt for 90% of the waking hours. The mitt was to be worn at all
times except when performing a minimal amount of agreed upon activities (e.g. bathroom
activities, naps, when the less-affected limb is used for an assistive device in walking, and other
circumstances where safety may be compromised). During the ten consecutive weekdays, the
participants with stroke received supervised task practice, using only their affected upper-
extremity for six hours a day. The tasks included items such as: meal preparation, eating,
grooming, home maintenance, games and hobbies. The CIMT intervention emphasized
substantial movement repetitions while performing functional activities of daily life. After the 2-
week treatment, the participants with stroke received a series of post-test evaluations, which
were the same as the pre-test evaluations.
The movement task selected for this study was the “Lift Basket” task of the WMFT. The
WMFT is a standardized test and one of the primary outcomes in the CIMT studies.1, 50, 57, 58, 64,
67, 68, 74, 101 The WMFT consists of a series of 15 timed tasks and two strength tasks that are
78
performed in either a sitting or standing position. The 15 tasks are arranged in order of
biomechanical complexity according to the joints involved and the level of difficulty. The tasks
progress from proximal to distal joint involvement and from gross to fine motor skills.50 A
recent pilot study of Rasch measurement conducted by Wen and Velozo (unpublished) in 2003,
however, has shown a different order of task difficulty. This indicates that Wolf’s conceptual
task complexity is not reflected in participants’ responses. For example, the last task, Lift Basket,
which was supposed to be the most difficult task of WMFT became the second difficult task.
The WMFT quantifies upper-extremity movement ability through timed single- or multiple-joint
motions and functional tasks.50
The last task in the WMFT, “Lift Basket,” is regarded as a complex task that demands
efforts from multiple body systems, such as muscle strength, dynamic/standing balance, and
inter-limb coordination. The Rasch pilot study of Wen and Velozo (unpublished) demonstrated
the “Lift Basket” task to be the second most difficult task of the WMFT in terms of item
difficulty analysis. As compared with a simple activity, such as reaching for an object on a table,
“Lift Basket” is a representative activity with greater difficulty in our daily life. This task
requires involvement from the whole body. Studying this task, therefore, can show how one
body part interacts with others during movement. Moreover, the “Lift Basket” task is an “out of
synergy” movement that can target the limitations people with stroke have when performing a
reaching and lifting task.88
“Lift Basket” task
The set-up of the “Lift Basket” task included a basket, a desk (29” high) located in front of
the participant and a bedside table (44” high) located on the participant’s side to be tested.
(Figure 4-1A and 4-1B) The bedside table extended along the width of the desk. The basket was
placed on the desk and lined up with the center of the participants’ body. A three-pound weight
79
was placed in the basket. Participants were tested in a standing position while facing the desk.
The set-up of the “Lift Basket” task is illustrated with its starting position (Figure 4-1A) and
ending position (Figure 4-1B). The task description was “Patient attempts to pick up basket by
grasping handle (from underneath the handle) and placing the basket on far edge of the rolling
bedside table.” All participants were asked to “Pick up the basket with your hand and place the
basket on the rolling table. The far edge of the basket should go past the far edge of the bedside
table. Try not to move your feet while you do this task. Do this as quickly as you can.”102 The
subject’s movement progression was videotaped from a front view. Participants’ video tapes
were then converted to DVD in digital format using a Panasonic DVD recorder (model DMR-
E95HS) for further analyses of the Eshkol-Wachman Movement Notation (EWMN). EWMN90-
92 is a movement language developed in Israel by professors Noa Eshkol and Avraham
Wachman. In the literature of human and animal behavior, EWMN has been shown to
effectively describe various aspects of movement, such as time, speed, direction, magnitude,
limb position, inter-limb spatial relations/coordination, sequence and trajectory.93-97
Essential-Movement Component Evaluation form
The Essential-Movement Component Evaluation (EMCE) Form (see Figure 4-2) was used
to evaluate and document participants’ movement quality. The EMCE form of EWMN
encompasses ten sequencing movement components identified from participants without stroke,
and compensatory trunk movements identified from the participants with stroke. The ten
essential-movement components of “Lift Basket” task include 1) eye contact with basket handles,
2) initiative synergy: coupled but opposite movements of the arm and forearm, 3) forearm
fixation: maintaining constant height of forearm in space while arm moves toward the basket, 4)
contralateral weight shifting, 5) hand preparation for grasping, 6) grasping, 7) shift of eye contact
to side tabletop, 8) diagonal shift of upper arm, 9) ipsilateral weight shifting, 10) forearm
80
movement of placing the basket. The compensatory movements include 1) upper-arm abduction,
2) trunk side-bending, 3) trunk forward rotation, 4) trunk backward rotation, and 5) non-standard
grasping. The detailed definition of the ten essential-movement components and compensatory
movement can be found in Appendix A or the EMCE form (Figure 4-2).
In this experiment, the one hundred and twenty video clips were converted to DVD in
digital format using a Panasonic DVD recorder (model DMR-E95HS) for further analyses of
EWMN. In the laboratory, a physical therapist with three-year EWMN training experience
played video clips frame-by-frame (30 frames/second) to grade participants’ movement using a
Pioneer DVD player (model DVD-V7400). The EMCE form based on EWMN was used to
analyze participants’ movement quality in terms of movement component, sequence, and
strategy.132
The essential-movement components are first graded by whether a movement component
is observed (0= No; 1= Yes). The range of essential-movement component composite score is 0
to 10. Three essential-movement components are further graded by how much range-of-motion
is observed (0= no movement observed; 1= 0º ≤ movement < 30º; 2= 30º ≤ movement < 60º; 3=
30º ≤ movement < 60º). The three essential-movement components are upper-arm movement
with forearm fixation, diagonal shifting of upper arm (including horizontal and vertical shifting),
and forearm movement to place the basket. The compensatory movement is graded by whether
a compensatory movement is observed. (0= No; 1= Yes) The range of compensatory movement
composite score is 0 to 5.
Data Analysis
A two-group (high-functioning and low-functioning stroke groups) x two-time (pre-CIMT
and post-CIMT) analysis of variance (ANOVA) with repeated measures were conducted to
analyze the six dependent variables in this study. The dependent variables included essential-
81
movement component composite scores and compensatory movement composite scores, and
movement magnitude of the four movement components. The significant level was set at .05. In
addition, the use of t-test was to determine pair-wise significance when the interaction (group x
time) was statistically significant. The prevalence of each essential-movement component and
compensatory movement was also reported in percentage.
Results
Results of the 2(group) x 2 (testing times) ANOVAs with repeated measures conducted in
this experiment are presented (Table 4-2). Statistically significant differences existed between
pre-CIMT and post-CIMT in upper-arm movement with forearm fixation and upper-arm
horizontal shifting. Between the two stroke groups, statistically significant differences were
found in compensatory composite scores and all four movement magnitude variables.
Results revealed a statistically significant group (high-functioning, low-functioning) x time
(pre-CIMT, post-CIMT) interaction for essential-movement component composite scores (F(1, 58)
= 7.05, p < 0.01). Fig 4-3 was the interaction plot of two groups’ mean composite scores of
essential-movement component. Specifically, essential-movement component composite scores
increased in the low functioning group from pre-CIMT to post-CIMT (t = -3.47, p < 0.01), but
not in the high-functioning group (t = 0.28, p = 0.78). A statistically significant group effect was
found, indicating the low-functioning group adopted more compensatory movements than the
high-functioning group. (F(1, 58) = 5.84, p < 0.05) Percentages of observed movement component
and compensatory movement from the three groups were reported. (Table 4-3) For the
percentage of compensatory movement, although both groups showed increased use of
compensatory movement after CIMT, the changes were not statistically significant.
82
Discussion
CIMT leads to improvement in upper-extremity motor function post-stroke.1, 67, 68, 71, 105,
114, 118, 142, 143 The underlying movement strategies that account for the functional improvement
from CIMT remain unknown.143 In a recent article, Wolf defined clinically meaningful
improvements of CIMT as a reduction in the numbers of the 15 timed WMFT tasks that could
not be completed.109 His inference may be appropriate in terms of movement efficiency, but
there was no indication how the individuals with stroke altered their movement quality. The
Essential-Movement Component Evaluation (EMCE) is a reliable, effective and economical
method to examine quality of movement in terms of movement components, sequence, and
strategy.132 The goal of this experiment was to use the EMCE method to study the effects of
CIMT on the movement quality of a reaching-grasping-lifting-placing task (i.e. Lift Basket) in
WMFT.
Essential-Movement Component
The statistically significant interaction between time and group for the essential-movement
component composite scores indicates the impact of treatment depended on the groups. The
interpretation of the main effects (group or time) was incomplete and misleading. Treatment
effects of CIMT on the essential-movement component, therefore, depended on the severity or
level of the impairment. Post hoc analyses indicated that the composite scores were
significantly increased after CIMT in the low-functioning group, but not in the high-functioning
group. CIMT seemed to have more effect on restoring essential-movement components in the
low-functioning group than in the high-functioning group. A possible explanation may be that
the low-functioning group had fewer movement components pre-CIMT than the high-
functioning group. In the low-functioning group six out of the ten essential-movement
components were lower than 50 percent on the pre-test. These underutilized components in the
83
low-functioning group included initiative synergy, forearm fixation, grasping preparation,
grasping, upper-arm diagonal shifting, and placing basket. The high-functioning group did not
show statistically significant change in the essential-movement component total score after the
intervention. On the prevalence table (Table 4-3), two underutilized components were found:
initiative synergy and forearm fixation. Regarding movement magnitude, two components
(upper-arm movement forearm fixation and upper-arm horizontal shifting) showed statistically
significant treatment effects. Those treatment effects indicated that CIMT promoted range-of-
motion of shoulder flexion and horizontal abduction.
The initiative synergy is an essential-movement component that acted as a preparatory step
of reaching. Instead of moving the upper arm directly to the target, the forearm and upper arm
simultaneously initiate the task in opposite directions (i.e. a couple movement of shoulder
extension and elbow flexion on the sagittal plane). Then the forearm and upper arm move
forward toward the basket handle. This short time delay caused by the initiative synergy
provides the forearm an opportunity to prepare its appropriate position for later reaching.
Forearm fixation is a subsequent aiming movement that keeps the forearm in a fixed height until
the hand reaches to the target. Without this aiming movement, the process of reaching requires
more adjustments and the movement becomes unsmooth and segmental. Grasping preparation is
a crucial component to have a successful grasp. An inappropriate hand opening can impede
formation of a secure grasp.45, 77, 144 Upper-arm diagonal shifting (shoulder flexion and
abduction) and placing basket (elbow extension) are two “out of synergy” movements.
According to Brunnstrom, these movements are often difficult to regain for people post-stroke.12
Except for forearm fixation showing decreased use, after receiving CIMT, most of the
underutilized components in the low-functioning group increased or maintained their pre-CIMT
84
use,. In addition to forearm fixation, the high-functioning group had more declining components
than the low-functioning group, including grasping preparation and grasping. The allowance of
compensatory movement during CIMT training may have lead to the decline in essential-
movement components. The limitations in movement control may be different for high- and low
functioning groups. Forced use of the affected extremity possibly encouraged and elicited the
exploration of underutilized essential-movement components in the low-functioning group.
When having more pre-existing essential-movement components, the same training, however,
may encourage the use of compensatory movement in the high-functioning group in order to
meet the speed command of the task.
Compensatory Movement
There was no statistically significant treatment effect on the total compensatory movement
score, indicating CIMT did not increase the use of compensatory movements. A possible
explanation was that increased use of certain compensatory movements was offset by decreased
use of others, such as trunk side-bending and non-standard grasping. In addition, a statistically
significant group effect was found, indicating the low-functioning group adopted more
compensatory movements than the high-functioning group. (F(1, 58) = 5.84, p < 0.05)
Most of the compensatory movements were frequently observed in both groups pre- and
post-CIMT. Initiative synergy was often substituted by the trunk side-bending to the
contralateral side along with shoulder abduction. Instead of moving the upper arm forward with
forearm fixation, the elbow joint was locked at 90 degree of flexion during the whole reaching
part of the task. In order to reach for the basket, therefore, the trunk had to forward rotate so that
the hand could perform the subsequent grasping movement. Two non-standard grasping
compensatory movements were observed: wrist and reversed maneuvers. In the wrist maneuver
the hand went under and passed the basket handle, and then the wrist lifted the basket. The
85
reversed maneuver was that the hand grasped the basket handle with the thumb pointing toward
the individual. The compensatory grasping maneuvers appeared to occur for individuals who
could not perform grasping preparation (hand opening) and forearm supination. When the upper
arm shifted diagonally to lift the basket, trunk backward rotation often assisted the lifting.
Elbow extension was necessary for placing the basket onto the high table. Ipsilateral weight
shifting, however, took the place of elbow movement, and the elbow often remained at 90 degree
of flexion. Generally speaking, the low-functioning group often substituted compensatory
movements for the essential-movement components, which may indicate the inability to recruit
certain body parts17, 42, 45, 75, 89, 135, 136 or muscle weakness.8, 10, 11, 18, 19 Additionally, the proximal
body parts, which include the upper arm and trunk, often dominated the movement or incorrectly
initiated the movement. Although the high-functioning group used the essential-movement
components, compensatory movements still appeared, but functioned as assistance. A table is
presented to summarize the aforementioned compensatory movements. (Table 4-4)
CIMT is a rehabilitative approach based on the task-oriented model.25, 109 The task-oriented
model assumes that “control of movement is organized around goal-directed, functional
behaviors rather than on muscles or movement patterns.”145 The task-oriented model also
encourages the individual to actively participate in solving motor challenges.146 In
rehabilitation, practicing a motor task or activity should be functionally based and practiced in a
variety of contexts. Thus, the patient can develop and implement the strategies learned for future
tasks after discharge from therapy. The two training modes of CIMT are repetitive task practice
and adaptive task practice.109 Repetitive task practice emphasizes continuous attempts to
execute movements of a repeated nature, such as dusting, eating, or combing. The practice is
designed to enhance problem-solving skills. Adaptive task practice uses the principles of operant
86
or instrumental conditioning to repeatedly perform a defined task in a series of trials. During
each trial, the task has a defined duration. The goal of adaptive task practice is either to increase
the successful repetitions or to use less time to complete the task. From the standpoint of the
task-oriented model, both practice modes imply that compensatory movement is acceptable and
should be encouraged if function is improved.137, 147 The allowance of compensatory movement
during CIMT training may be based on some controversial assumptions: 1) movement
impairment is not reversible; 2) improvement on goal-directed functional tasks is more
meaningful to patient’s recovery than improvement on movement quality; or 3) faster movement
or more completions indicates better motor control or coordination.
Recent studies suggest that impaired movement components may be reversible and not
normally just recruited post-stroke.89, 135, 136, 141 Trunk restraint to prevent its compensatory
contribution toward a reaching or pointing task while training can induce more upper extremity
movement. For instance, Michaelsen, Dannenbaum and Levin, reported that for the control
group (no trunk restraint) after one-month of arm training, trunk compensatory movement
increased, but for the experimental group decreased trunk movement and increased elbow
extension were found.135 Trunk restraint allowed patients with stroke to make use of arm joint
ranges that were present but not normally recruited during unrestrained arm-reaching tasks.
Thus, the underlying "normal" patterns of movement coordination may not be entirely lost after
stroke.135 Changing movement pattern, including restoration of essential-movement component
and inhibition of compensatory movement can be beneficial to improve quality of movement.138,
139
Whether functional recovery is simply goal attainment, or improved movement control
while accomplishing the goal, still remains debatable.146 Task-oriented intervention, such as
87
CIMT, focuses on task completion as fast or as many times as possible, without consideration of
compensatory movements. Moving faster with greater numbers of repetitions appears to indicate
improved function in the laboratory, but when individuals return to the community, the less
coordinated or awkward movement may adversely affect self image, especially in the public.
Allowance of compensatory movement can be detrimental to the recovery process. For example,
if a client with stroke can not walk, and they choose to use a powered wheelchair in order to
compensate the impaired function and to attain the goal of independent mobility. The ability of
walking would never be restored. Quality of movement does matter in our daily life.107, 140 After
our clients can perform certain representative functional activities, such as walking and reaching,
improvement in quality of these movements becomes their next ultimate goal.
In this study, movement quality is defined as movement that approximates normal
movement. Normal movement is that observed in people without disorders that affect movement
execution.82, 83 In addition, normal movement encompasses movement components that are
required for executing a movement (i.e. essential-movement component) in a sequencing manner
without using compensatory movement. EMCE method can effectively pinpoint the missing
essential-movement components and compensatory movement. The beneficial information
gathered from the EMCE form can assist clinicians to design appropriate and tailored training
programs for their clients if movement quality is a treatment goal. The goals of CIMT training
can then be further clarified to improve the essential-movement components, re-establishment of
normal movement sequence, and prevention of compensatory movement.
Limitation
Evaluation of the Lift Basket task was under the condition that tested participants’
maximal capacity. The participants were asked to execute the task as quickly as possible.
Adoption of compensatory movement under this situation, however, may not indicate this
88
strategy will be seen when participants performs the task at a self-paced comfortable speed. For
future study, investigation of compensatory movement while performing at a self-paced speed
may be necessary.
Conclusions
A statistically significant interaction between time and group for essential-movement
component composite scores was found, indicating treatment effects of CIMT on essential-
movement component depended on the severity level of impairment. The composite scores
significantly increased only in the low-functioning group, but no significant changes were found
in the high-functioning group. Although there was no statistically significant treatment effect on
compensatory movement scores, increased use of compensatory movement was found in both
groups. In order to improve movement quality post-stroke, the goals of CIMT training,
therefore, need to be expanded to increase the function of underused essential-movement
components, re-establish normal movement sequences, and prevent compensatory movements.
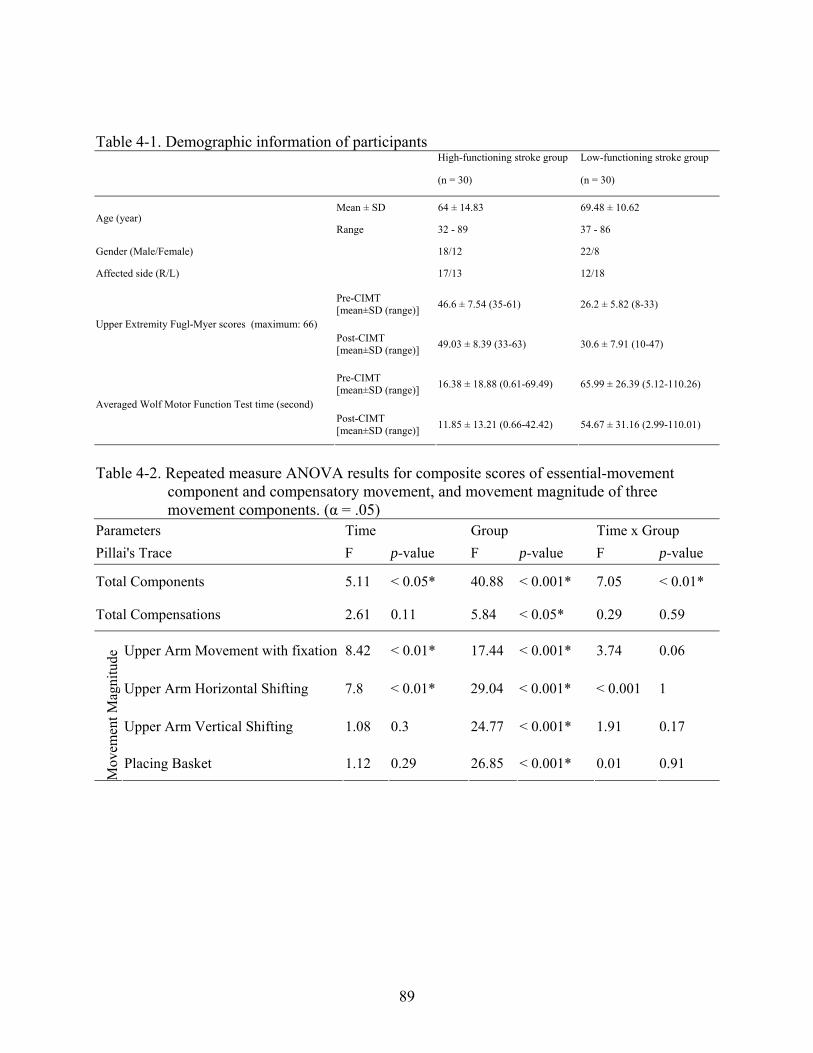
89
Table 4-1. Demographic information of participants High-functioning stroke group Low-functioning stroke group
(n = 30) (n = 30)
Mean ± SD 64 ± 14.83 69.48 ± 10.62 Age (year)
Range 32 - 89 37 - 86
Gender (Male/Female) 18/12 22/8
Affected side (R/L) 17/13 12/18
Pre-CIMT [mean±SD (range)] 46.6 ± 7.54 (35-61) 26.2 ± 5.82 (8-33)
Upper Extremity Fugl-Myer scores (maximum: 66) Post-CIMT [mean±SD (range)] 49.03 ± 8.39 (33-63) 30.6 ± 7.91 (10-47)
Pre-CIMT [mean±SD (range)] 16.38 ± 18.88 (0.61-69.49) 65.99 ± 26.39 (5.12-110.26)
Averaged Wolf Motor Function Test time (second) Post-CIMT [mean±SD (range)] 11.85 ± 13.21 (0.66-42.42) 54.67 ± 31.16 (2.99-110.01)
Table 4-2. Repeated measure ANOVA results for composite scores of essential-movement
component and compensatory movement, and movement magnitude of three movement components. (α = .05)
Parameters Time Group Time x Group Pillai's Trace F p-value F p-value F p-value
Total Components 5.11 < 0.05* 40.88 < 0.001* 7.05 < 0.01*
Total Compensations 2.61 0.11 5.84 < 0.05* 0.29 0.59
Upper Arm Movement with fixation 8.42 < 0.01* 17.44 < 0.001* 3.74 0.06
Upper Arm Horizontal Shifting 7.8 < 0.01* 29.04 < 0.001* < 0.001 1
Upper Arm Vertical Shifting 1.08 0.3 24.77 < 0.001* 1.91 0.17
Mov
emen
t Mag
nitu
de
Placing Basket 1.12 0.29 26.85 < 0.001* 0.01 0.91
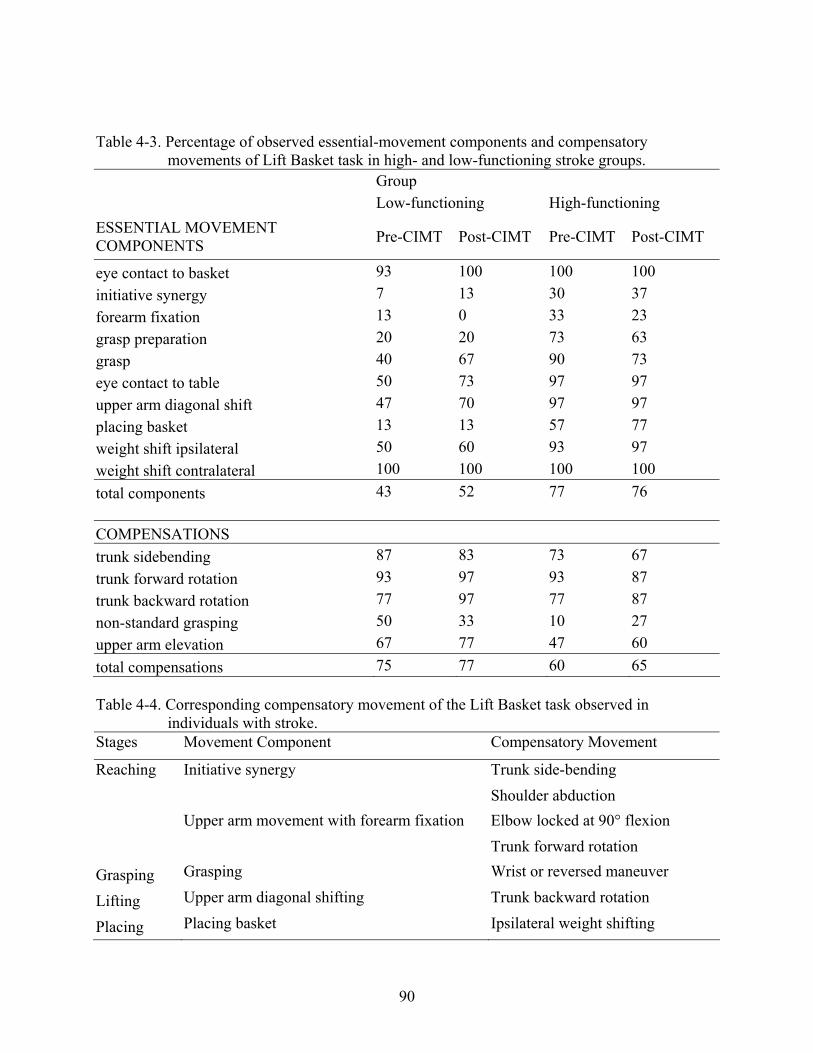
90
Table 4-3. Percentage of observed essential-movement components and compensatory movements of Lift Basket task in high- and low-functioning stroke groups.
Group Low-functioning High-functioning ESSENTIAL MOVEMENT COMPONENTS Pre-CIMT Post-CIMT Pre-CIMT Post-CIMT
eye contact to basket 93 100 100 100 initiative synergy 7 13 30 37 forearm fixation 13 0 33 23 grasp preparation 20 20 73 63 grasp 40 67 90 73 eye contact to table 50 73 97 97 upper arm diagonal shift 47 70 97 97 placing basket 13 13 57 77 weight shift ipsilateral 50 60 93 97 weight shift contralateral 100 100 100 100 total components 43 52 77 76 COMPENSATIONS trunk sidebending 87 83 73 67 trunk forward rotation 93 97 93 87 trunk backward rotation 77 97 77 87 non-standard grasping 50 33 10 27 upper arm elevation 67 77 47 60 total compensations 75 77 60 65 Table 4-4. Corresponding compensatory movement of the Lift Basket task observed in
individuals with stroke. Stages Movement Component Compensatory Movement
Trunk side-bending Initiative synergy Shoulder abduction Elbow locked at 90° flexion
Reaching
Upper arm movement with forearm fixation Trunk forward rotation
Grasping Grasping Wrist or reversed maneuver
Lifting Upper arm diagonal shifting Trunk backward rotation
Placing Placing basket Ipsilateral weight shifting
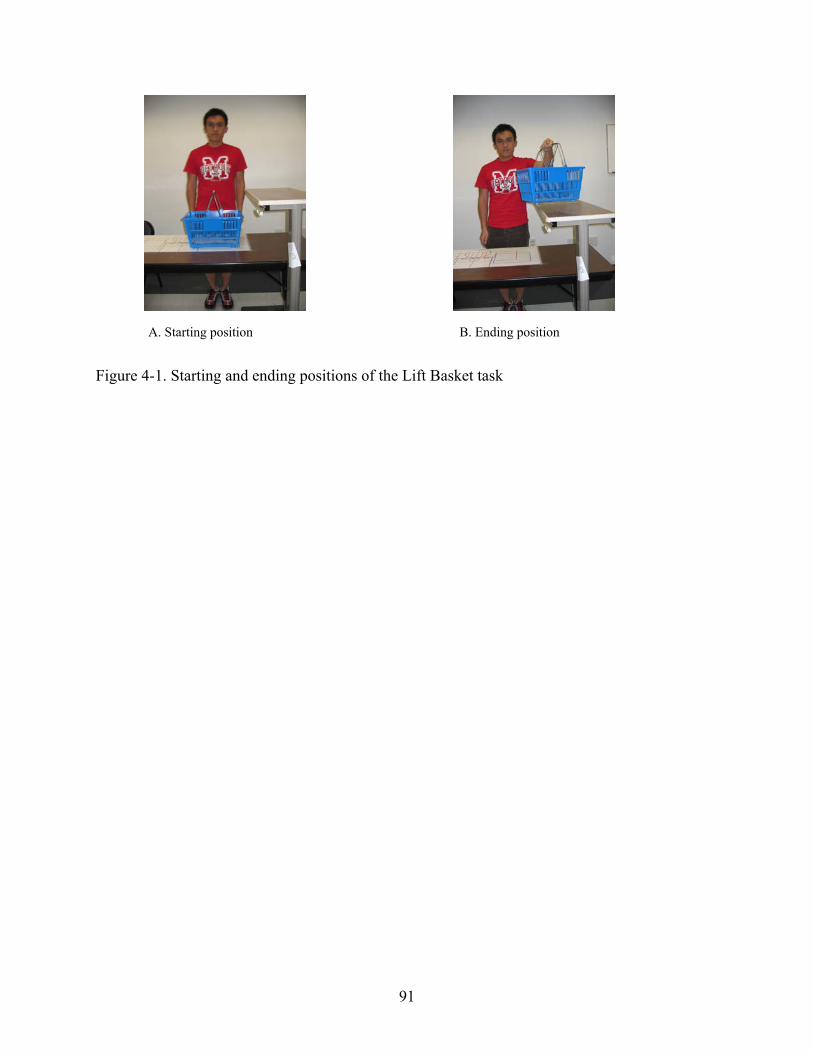
91
Figure 4-1. Starting and ending positions of the Lift Basket task
A. Starting position B. Ending position
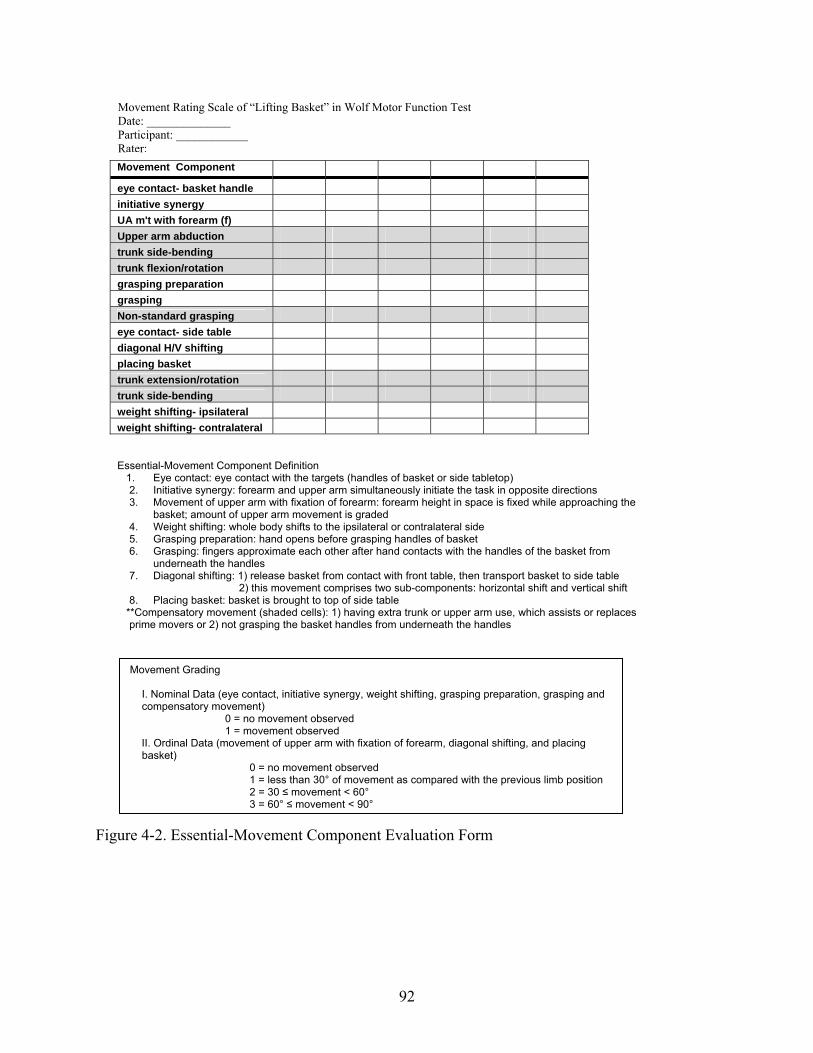
92
Figure 4-2. Essential-Movement Component Evaluation Form
Movement Rating Scale of “Lifting Basket” in Wolf Motor Function Test Date: ______________ Participant: ____________ Rater: Movement Component eye contact- basket handle initiative synergy UA m't with forearm (f) Upper arm abduction trunk side-bending trunk flexion/rotation grasping preparation grasping Non-standard grasping eye contact- side table diagonal H/V shifting placing basket trunk extension/rotation trunk side-bending weight shifting- ipsilateral weight shifting- contralateral
Essential-Movement Component Definition 1. Eye contact: eye contact with the targets (handles of basket or side tabletop) 2. Initiative synergy: forearm and upper arm simultaneously initiate the task in opposite directions 3. Movement of upper arm with fixation of forearm: forearm height in space is fixed while approaching the
basket; amount of upper arm movement is graded 4. Weight shifting: whole body shifts to the ipsilateral or contralateral side 5. Grasping preparation: hand opens before grasping handles of basket 6. Grasping: fingers approximate each other after hand contacts with the handles of the basket from
underneath the handles 7. Diagonal shifting: 1) release basket from contact with front table, then transport basket to side table
2) this movement comprises two sub-components: horizontal shift and vertical shift 8. Placing basket: basket is brought to top of side table
**Compensatory movement (shaded cells): 1) having extra trunk or upper arm use, which assists or replaces prime movers or 2) not grasping the basket handles from underneath the handles
Movement Grading
I. Nominal Data (eye contact, initiative synergy, weight shifting, grasping preparation, grasping and compensatory movement)
0 = no movement observed 1 = movement observed
II. Ordinal Data (movement of upper arm with fixation of forearm, diagonal shifting, and placing basket)
0 = no movement observed 1 = less than 30° of movement as compared with the previous limb position 2 = 30 ≤ movement < 60° 3 = 60° ≤ movement < 90°
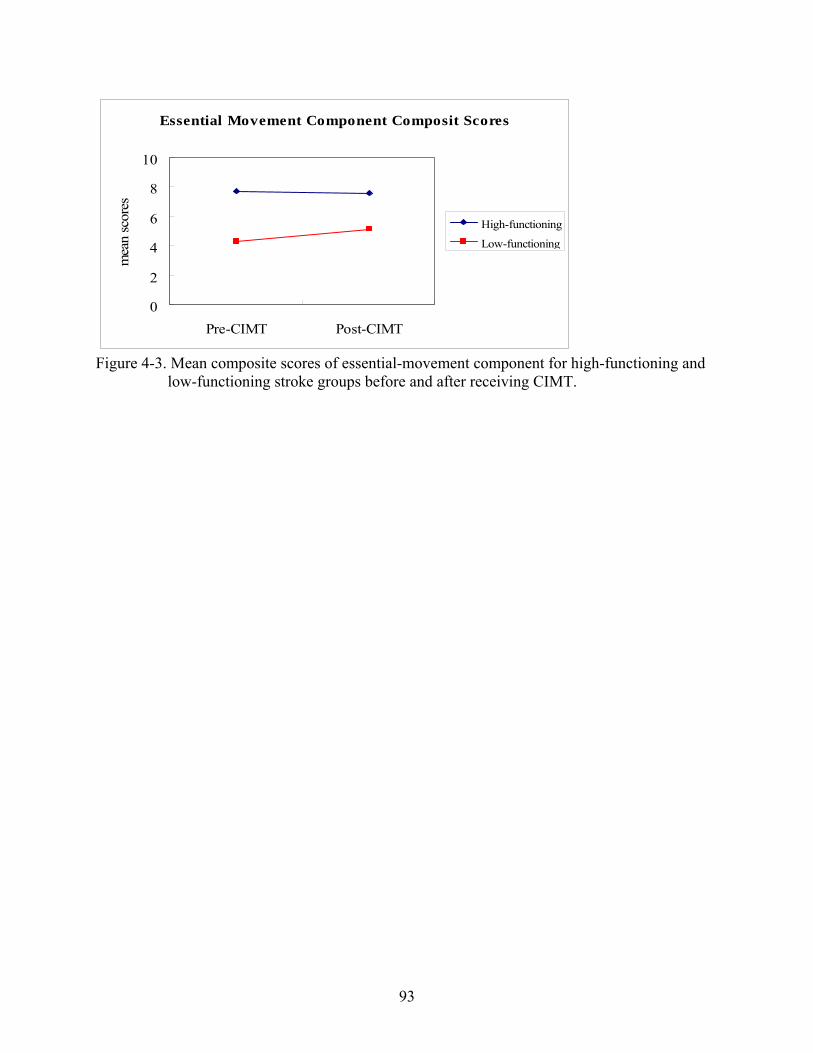
93
Essential Movement Component Composit Scores
0
2
4
6
8
10
Pre-CIMT Post-CIMT
mea
n sc
ores
High-functioning
Low-functioning
Figure 4-3. Mean composite scores of essential-movement component for high-functioning and
low-functioning stroke groups before and after receiving CIMT.
94
CHAPTER 5 GENERAL SUMMARY AND CONCLUSIONS
Specific and detailed discussions have been provided in the previous chapters regarding the
three studies using the Essential-Movement Component Evaluation (EMCE) form to examine
quality of movement for CIMT intervention and stroke rehabilitation. The purpose of this
chapter is to summarize and integrate the major findings for each experiment.
Overview
Scientists and clinicians have developed numerous methods to measure movement
impairment following stroke. Quality of movement, however, has not been objectively measured
in clinical or research settings. The Functional Ability Scale (FAS; see Table 2-1) is a measure
of movement quality currently used in Constraint-Induced Movement Therapy research, but its
outcomes provide limited information about functional improvement and quality of movement.72
Three experiments were included in this dissertation. The first experiment (Chapter 2) was
to develop a clinically feasible template, EMCE, to measure quality of movement post-stroke
based on a combined application of the Generalized Motor Program (GMP) theory38, 85 and the
Eshkol-Wachman Movement Notation (EWMN) method.90-92 In addition, the inter- and intra-
rater reliability of the EMCE form were established. The second experiment (Chapter 3) was to
present a method of measuring movement quality (i.e. EMCE) and to explore if this method can
distinguish problematic movement patterns observed in people with stroke. Finally, the third
experiment (Chapter 4) was to use the EMCE to investigate the effect of CIMT on movement
quality in terms of essential-movement components, sequence and strategy.
Experiment I Summary
The goals of this study were to develop a quality of movement evaluation form and to
further determine the inter- and intra-rater reliability of this evaluation form. Using the EWMN
95
method, ten movement components and five compensatory movements were identified and
included on the EMCE form for the “Lift Basket” task of WMFT. The ten essential-movement
components of the task include 1) eye contact with basket handles, 2) initiative synergy: coupled
but opposite movements of the arm and forearm (i.e. simultaneous shoulder extension and elbow
flexion on the sagittal plane), 3) upper-arm movement with forearm fixation: maintaining
constant height of the forearm in space while the upper arm moves forward toward the basket, 4)
contralateral weight shifting, 5) grasping preparation: opening the hand, 6) grasping, 7) shift of
eye contact to the high tabletop, 8) diagonal shift of upper arm (i.e. shoulder flexion and
abduction), 9) ipsilateral weight shifting, 10) placing the basket (i.e. elbow extension). The
compensatory movements include 1) upper-arm abduction, 2) trunk side-bending, 3) trunk
forward rotation, 4) trunk backward rotation, and 5) non-standard grasping.
The results of this study indicated that the movement components of the Lift Basket task
analyzed can be assessed reliably with a minimal degree of error. The ICCs for intra- and inter-
rater reliability were excellent (.89-.97 and .90-.95, respectively), suggesting excellent agreement
both within and between raters. The SEM for inter-rater reliability was 0.52 and intra-rater
reliability ranged from 0.15 to 0.47. This represented an error of measurement ranging from
0.15 to 0.52. A smaller SEM relates to higher reliability of the test and therefore, more precision
in the measure.
The high ICCs and subsequent low SEMs demonstrate that novice investigators, even
those without formal rehabilitation or movement training, can reliably document movement
using the established ECME form and a short training and practice session. The SEM represents
the standard deviation of measurement errors and reflects the extent of expected error in repeated
measurements or different raters’ scores.120, 121 SEM is directly related to the reliability of a test.
96
The larger the SEM, the lower the reliability of the test and the less precision there is in the
measures taken and scores obtained. The MDC reflects the smallest detectable difference that
can be considered “actual change” that exceeds measurement error. The MDC for the total score
of the essential-movement components was 0.90; this means a participant must exceed a change
of .90 in the essential-movement component total score to identify the change as true and not due
to measurement error. Therefore, if a person scores a 4 on the pre-test and a 5 on the post-test,
we can be sure the change is real and not due to measurement error.
While most of the 10 component movements demonstrated excellent intra-reliability, an
analysis of individual items demonstrated that the fixation item (upper-arm movement with
forearm fixation), had a lower ICC value (.72), although still good.98-100 The recognition of
compensatory movement patterns, such as using forward trunk rotation to compensate for lack of
upper-arm and forearm movement, may be a skill that requires more advanced training. Physical
and occupational therapists should have the skills to identify these compensatory movements.
The PT (Rater 1) and OT (Rater 2) participated in the reliability study had higher overall ICCs
(.91 and .97) than the non-rehabilitation professional (Rater 3) (.89), although the non-
professional still had an overall excellent ICC. This trend held true for the total ICCs and SEMs.
These results suggest EMCE is an effective measure with excellent rater reliability. Evaluators
with little training or knowledge of movement analysis can still reliably use a well-established
EMCE template to assess quality of movement.
Experiment II Summary
The goal of this study was to apply the EMCE form to a larger sample to examine the
differences between people with and without stroke in terms of quality of movement. The results
from the ANOVAs showed there were statistically significant differences between the means of
the groups for total score of essential-movement components, the total score of compensatory
97
movements, and the movement magnitude of the three essential-movement components. In
accordance with the hypothesis, the results suggested that the EMCE form for the Lift Basket
task was able to effectively distinguish the differences between normal individuals and the two
different stroke groups. As for the post-hoc analyses, no significant differences were found in
the movement magnitude of the upper-arm horizontal and vertical shifting between the high-
functioning and normal group. These non-significant results suggest that in the high-functioning
stroke group the movement of the upper-arm was not significantly different during this lifting
component than the normal group. No significant differences were noted, however, between the
high- and low-functioning groups in the total score of compensatory movements or in the
magnitude of upper-arm movement with forearm fixation. Unlike the lifting component, during
the early phase of reaching (i.e. upper-arm movement with fixation) the high-functioning group
was not statistically different than that of the low-functioning group. A possible explanation can
be that the high-functioning stroke group adopted compensatory movement during reaching even
when their function was improved. The compensatory movements observed included movement
initiation with upper-arm abduction, trunk side-bending, and trunk forward rotation. Adopting
these compensatory movements in the high-functioning stroke group can be an indication of the
habitual movement strategy that followed the previous atypical synergy while their upper
extremity function was still limited.
The percentage of every essential-movement component in the two stroke groups was
observed less as impairment level increased, except for contralateral weight shifting which was
the same for both the high and low functioning groups. People with stroke have the tendency to
bear their weight on the less affected side, but have difficulty in shifting the weight to the
affected side.44, 133 The inability to shift body weight from one side to another may cause
98
decreased ability to engage in dynamic activities, such as reaching or walking.134 The most
impaired essential-movement components found in the low-functioning stroke group included
initiative synergy (preparation for reaching), forearm fixation (aiming), grasp preparation (hand
opening), grasp, eye contact to high table (estimation for height of lifting), upper-arm diagonal
shifting (upper-arm strength), and placing basket (elbow extension). The initiative synergy is an
essential-movement component that acted as a preparatory step of reaching. Instead of moving
the upper arm directly to the target, the forearm and upper arm simultaneously initiated the task
in opposite directions (i.e. a couple movement of shoulder extension and elbow flexion on the
sagittal plane). Then the forearm and upper arm move forward toward the basket handle. This
short time delay caused by the initiative synergy provides the forearm an opportunity to prepare
its appropriate position for later reaching. Forearm fixation is an aiming movement that keeps
the forearm in a fixed height until the hand reaches to the target.
According to the GMP theory, actions controlled by the same GMP share the same
invariant features, such as the sequencing of submovements, relative timing and relative forces.
Movements governed by the same GMP differ from each other in the assignment of variant
movement parameters, for instance absolute time, absolute force, and selection of effectors.38, 85,
86 In line with the GMP theory, invariant submovements in a fixed movement sequence can be
identified when different individuals execute the same activity. In this experiment, decreased
use of essential-movement component with the increase of compensatory movements was found
as impairment level increased. These results indicated that the motor programming may be
altered in people with stroke. Having less essential-movement components forced individuals
with stroke to adopt more compensatory movements. Underutilized essential-movement
components in stroke groups provide clinicians a useful direction of treatment. Instead of simply
99
emphasizing repetition and speed, an effective training program may also focus on restoring
underutilized essential-movement components in a sequencing manner.
Compensatory movements were found in all three groups, but the prevalence increased as
impairment levels increased from normal, to high-functioning, to low-functioning. Possible
reasons for the normal group adopting compensatory movements were inaccurate basket
placement, short body structure, or muscle weakness. When these conditions exist, the upper
arm and trunk may need to compensate for the discrepancy in the position of the basket. For the
low-functioning stroke group, however, compensatory movements were often substituted for
essential-movement components, which may indicate the inability to recruit certain body parts17,
42, 45, 75, 89, 135, 136 or muscle weakness.8, 10, 11, 18, 19 Additionally, the proximal body parts, which
include upper arm and trunk, often dominated the movement or incorrectly initiated the
movement, for example, the movement was initiated by trunk side-bending or upper arm
abduction. For the high-functioning group, while the essential-movement components were
observed, compensatory movements still appeared, but functioned as assistance for the essential-
movement components.
Whether compensatory movement is a necessary post-stroke adaptation, which should not
be corrected remains controversial.137-139 Some recent studies, however, have shown that
emphasis on training certain underutilized movement components during reaching, such as
elbow and shoulder range-of-motion can significantly improve movement quality.107, 140 On the
other hand, restraint of the trunk to prevent its compensatory contribution toward a reaching or
pointing task, while training, can actually induce more upper extremity movement89, 135, 136, 141
Trunk restraint allows patients with stroke to make use of arm joint ranges that are present but
not normally recruited during unrestrained arm-reaching tasks. Thus, the underlying "normal"
100
patterns of movement coordination may not be entirely lost after a stroke and underutilized
essential-movement component may be restorable.135 In order to improve quality of movement,
therefore, restoration of underused essential-movement component and reduction or inhibition of
compensatory movements may be two priority goals for treatment.
Experiment III Summary
The goals of the third experiment were to determine the effects of CIMT on quality of
movement as measured by EMCE, and to systematically categorize compensatory movements
used by persons with stroke pre- and post-CIMT. The results revealed a statistically significant
interaction between time and group for the essential-movement component composite scores
indicates the impact of treatment depended on the groups. The interpretation of the main effects
(group or time) was incomplete and misleading. Treatment effects of CIMT on the essential-
movement component, therefore, depended on the severity or level of the impairment. Post hoc
analyses indicated that the composite scores were significantly increased after CIMT in the low-
functioning group, but not in the high-functioning group. CIMT seemed to have more effect on
restoring essential-movement components in the low-functioning group than in the high-
functioning group. A possible explanation may be that the low-functioning group had fewer
movement components pre-CIMT than the high-functioning group. In the low-functioning group
six out of the ten essential-movement components were lower than 50 percent on the pre-test.
These underutilized components in the low-functioning group included initiative synergy,
forearm fixation, grasping preparation, grasping, upper-arm diagonal shifting, and placing
basket. The high-functioning group did not show statistically significant change in the essential-
movement component total score after the intervention. On the prevalence table (Table 4-3), two
underutilized components were found: initiative synergy and forearm fixation. Regarding
movement magnitude, two components (upper-arm movement forearm fixation and upper-arm
101
horizontal shifting) showed statistically significant treatment effects. Those treatment effects
indicated that CIMT promoted range-of-motion of shoulder flexion and horizontal abduction.
The initiative synergy is an essential-movement component that acted as a preparatory step
of reaching. Instead of moving the upper arm directly to the target, the forearm and upper arm
simultaneously initiate the task in opposite directions (i.e. a couple movement of shoulder
extension and elbow flexion on the sagittal plane). Then the forearm and upper arm move
forward toward the basket handle. This short time delay caused by the initiative synergy
provides the forearm an opportunity to prepare its appropriate position for later reaching.
Forearm fixation is a subsequent aiming movement that keeps the forearm in a fixed height until
the hand reaches to the target. Without this aiming movement, the process of reaching requires
more adjustments and the movement becomes unsmooth and segmental. Grasping preparation is
a crucial component to have a successful grasp. An inappropriate hand opening can impede
formation of a secure grasp.45, 77, 144 Upper-arm diagonal shifting (shoulder flexion and
abduction) and placing basket (elbow extension) are two “out of synergy” movements.
According to Brunnstrom, these movements are often difficult to regain for people post-stroke.12
Except for forearm fixation showing decreased use, after receiving CIMT, most of the
underutilized components in the low-functioning group increased or maintained their pre-CIMT
use,. In addition to forearm fixation, the high-functioning group had more declining components
than the low-functioning group, including grasping preparation and grasping. The allowance of
compensatory movement during CIMT training may have lead to the decline in essential-
movement components. The limitations in movement control may be different for high- and low
functioning groups. Forced use of the affected extremity possibly encouraged and elicited the
exploration of underutilized essential-movement components in the low-functioning group.
102
When having more pre-existing essential-movement components, the same training, however,
may encourage the use of compensatory movement in the high-functioning group in order to
meet the speed command of the task. There was no statistically significant treatment effect on
the total compensatory movement score, indicating CIMT did not increase the use of
compensatory movements. A possible explanation was that increased use of certain
compensatory movements was offset by decreased use of others, such as trunk side-bending and
non-standard grasping. In addition, a statistically significant group effect was found, indicating
the low-functioning group adopted more compensatory movements than the high-functioning
group.
Most of the compensatory movements were frequently observed in both groups pre- and
post-CIMT. Initiative synergy was often substituted by the trunk side-bending to the
contralateral side along with shoulder abduction. Instead of moving the upper arm forward with
forearm fixation, the elbow joint was locked at 90 degree of flexion during the whole reaching
part of the task. In order to reach for the basket, therefore, the trunk had to forward rotate so that
the hand could perform the subsequent grasping movement. Two non-standard grasping
compensatory movements were observed: wrist and reversed maneuvers. In the wrist maneuver
the hand went under and passed the basket handle, and then the wrist lifted the basket. The
reversed maneuver was that the hand grasped the basket handle with the thumb pointing toward
the individual. The compensatory grasping maneuvers appeared to occur for individuals who
could not perform grasping preparation (hand opening) and forearm supination. When the upper
arm shifted diagonally to lift the basket, trunk backward rotation often assisted the lifting.
Elbow extension was necessary for placing the basket onto the high table. Ipsilateral weight
shifting, however, took the place of elbow movement, and the elbow often remained at 90 degree
103
of flexion. Generally speaking, the low-functioning group often substituted compensatory
movements for the essential-movement components, which may indicate the inability to recruit
certain body parts17, 42, 45, 75, 89, 135, 136 or muscle weakness.8, 10, 11, 18, 19 Additionally, the proximal
body parts, which include the upper arm and trunk, often dominated the movement or incorrectly
initiated the movement. Although the high-functioning group used the essential-movement
components, compensatory movements still appeared, but functioned as assistance.
General Conclusions
The EMCE method can effectively pinpoint missing essential-movement component and
compensatory movement. With appropriate training of EWMN, researchers could develop
EMCE forms to evaluate movement quality for representative activities of daily living. The
beneficial information gathered from the EMCE form will assist clinicians to design appropriate
and tailored training programs for their clients.
CIMT is a rehabilitative approach based on the task-oriented model.25, 109 The task-oriented
model assumes that “control of movement is organized around goal-directed, functional
behaviors rather than on muscles or movement patterns.”145 The task-oriented model also
encourages the individual to actively participate in solving motor challenges.146 In
rehabilitation, practicing a motor task or activity should be functionally based and practiced in a
variety of contexts. Thus, the patient can develop and implement the strategies learned for future
tasks after discharge from therapy. The two training modes of CIMT are repetitive task practice
and adaptive task practice.109 Repetitive task practice emphasizes continuous attempts to
execute movements of a repeated nature, such as dusting, eating, or combing. The practice is
designed to enhance problem-solving skills. Adaptive task practice uses the principles of operant
or instrumental conditioning to repeatedly perform a defined task in a series of trials. During
each trial, the task has a defined duration. The goal of adaptive task practice is either to increase
104
the successful repetitions or to use less time to complete the task. From the standpoint of the
task-oriented model, both practice modes imply that compensatory movement is acceptable and
should be encouraged if function is improved.137, 147 According to the results of this study, the
methodology of CIMT did not improve quality of movement in terms of compensatory
movements (Table 4-3), which were not seen in people without neurological disorders. Most of
the compensatory movements, however, were frequently observed in both groups pre- and post-
CIMT.
Why do individuals with stroke choose compensatory movements in the “Lift Basket”
task? A potential explanation can be the speed required to perform the task. The subjects were
asked to execute the Lift Basket task as fast as possible, which tested individuals’ maximal
capacity. In order to reach for the target at the fastest speed, use of compensatory movements
may be just a representation of the trade-off between speed and movement quality. This
argument seems legitimate, but several recent studies have reported that individuals post-stroke
also use compensatory movements when reaching at a self-paced or comfortable speed.45, 135, 148
Whether functional recovery is simply goal attainment or improved movement pattern in
accomplishing the goal still remains debatable.146 Achieving good movement quality is an
important goal for people recovering from a stroke. A movement of good quality is one that
approximates normal movement.82, 83 Normal movement encompasses movement components
that are required for executing a movement (i.e. essential-movement components) in a
sequencing manner without using compensatory movements. The goals of CIMT training,
therefore, need to be expanded to increase the function of underused essential-movement
components, re-establish normal movement sequences, and prevent compensatory movements.
In order to improve movement quality and motor relearning, the incorporation of appropriate

105
guidance that emphasizes normal movement component, sequence, and strategy may be
necessary for future CIMT.30, 38
106
APPENDIX A PILOT DATA
Pilot Study 1
Purpose
The purpose of Pilot Study 1 was to conduct the proposed project with a small number of
participants to determine the feasibility of utilizing the planned methodology in reliability tests
for EWMN.
Aim: To determine the feasibility of conducting the inter-rater reliability and intra-rater
reliability for EWMN.
Hypothesis 1. The preliminary result of intra-rater reliability test will show a high
percentage of agreement, which will exceed 90 percent, between two separate testing times.
Hypothesis 2. The preliminary result of inter-rater reliability test will show a high
percentage of agreement, which will exceed 90 percent, among three different raters.
Participants
Three participants without stroke were randomly selected from a control group for this
study. All participants were voluntarily recruited from the local community. Their demographic
information is listed (Table A-1).
Method/Data Analysis
Three participants’ video tapes of the “Lift Basket” task were first converted to DVD in
digital format using a Panasonic DVD recorder (model DMR-E95HS). In the laboratory, three
raters with at least three-years EWMN training experience, then played video clips frame-by-
frame (30 frames/second) to grade participants’ movement using EWMN at separate times, using
a Pioneer DVD player (model DVD-V7400). One week after this viewing session, the same
107
raters were asked to grade the same participants’ movement. Percent of agreement was
calculated for inter-rater and intra-rater reliability.
Results and Conclusion
For the intra-rater reliability test, the percentage of agreement was 98%. For the inter-rater
reliability test, the percentage of agreement was 96%. Both intra-rater reliability and inter-rater
reliability showed values higher than 90%. The results indicate that after adequate training in
EWMN, raters can perform the evaluations reliably.
Pilot Study 2
Purpose
The purpose of Pilot Study 2 was to conduct the proposed project with a small number of
participants to determine feasibility of utilizing the planned methodology in determining
invariant features of the “Lift Basket” task using the EWMN method.
Participants
Eight participants without stroke (age range: 50~79 y/o; mean age: 70 y/o; 4M/4F) were
randomly selected from a control group for this study. All participants were voluntarily recruited
from the local community.
Method/Data Analysis
Participants’ video tapes of the “Lift Basket” task were first converted to DVD in digital
format using a Panasonic DVD recorder (model DMR-E95HS). In the laboratory, the author, a
physical therapist with three-years EWMN training experience, played video clips frame-by-
frame (30 frames/second) to grade participants’ movement using EWMN, using a Pioneer DVD
player (model DVD-V7400). Figure A-1 was an example of original EWMN page. Each
column on the table represented a time point during the task. For instance, the first pair of red
108
circles (i.e. the second column- eye contact with the basket handle) was observed before the
second pair of circles (i.e. the third column- initiative synergy).
Results and Conclusion
Using EWMN, ten essential movement components were identified in sequence from
control group participants:
1. Eye contact with basket handles
2. Initiative synergy: coupled but opposite movements of the arm and forearm
3. Forearm fixation: maintaining constant height of forearm in space while arm moves
toward the basket
4. Contralateral weight shifting
5. Hand preparation for grasping
6. Grasping
7. Shift of eye contact to side tabletop
8. Diagonal shift of arm
9. Ipsilateral weight shifting
10. Forearm movement of placing the basket.
The ten “essential-movement components” indicate that all participants not suffering from
stroke demonstrate these “invariant” components in their movement control for the “Lift Basket”
task. The study of essential-movement component follows the theory of Generalized Motor
Programs.38, 85
Normal movement strategy is recognized as recruiting first a proximal body part and then a
distal one. According to the above findings, an “Essential-Movement Components Evaluation
Form (EMCE)” for the “Lift Basket” task in the WMFT was created (Figure A-2). Among the
109
ten essential-movement components, “initiative synergy” and “forearm fixation” were two
movements that have never been reported in the literature of reaching.
Pilot Study 3
Purpose
The two purposes of Pilot Study 3 were 1) to modify the original “Essential-Movement
Components Evaluation Form” (Table A-3) for use in participants with stroke, and 2) to show
differences in essential-movement components among the three groups (control, low-functioning
stroke pre-test and high-functioning stroke pre-test).
Participants
Six participants (two participants from each group) were randomly selected from the three
groups for this study.
Method/Data Analysis
Participants’ video tapes of the “Lift Basket” task were first converted to DVD in digital
format using a Panasonic DVD recorder (model DMR-E95HS). In the laboratory, the author, a
physical therapist with three-years EWMN training experience, played video clips frame-by-
frame (30 frames/second) to grade participants’ movement using EWMN, using a Pioneer DVD
player (model DVD-V7400). The total essential-movement component scores were calculated.
Results and Conclusion
After using EWMN in examining the movements of the “Lift Basket” task in the
participants with stroke, five compensatory movements were observed. The compensatory
movement included upper-arm elevation, trunk side-bending, trunk forward rotation, trunk
backward rotation, and non-standard grasping. The original EMCE form was modified as seen
in Appendix B, which was used for this current project to record both essential-movement
components and compensatory movements. The differences of essential-movement components
110
among the three groups were shown.(Table A-2) As severity of stroke increased, the numbers of
essential-movement components decreased.(Table A-4) The high-functioning stroke group
preserved more essential-movement components than the low-functioning stroke group.
Compensatory movements were found (excessive trunk use and alternative grasping) in the
participants with stroke. In conclusion, the findings of Pilot Study 3 suggest that 1) there were
missing essential-movement components in participants with stroke while performing the “Lift
Basket” task; 2) the degree of missing essential-movement components appeared proportional to
the severity of stroke, and 3) compensatory movements were substituted for missing essential-
movement components of the “Lift Basket” task in participants with stroke. Completion of the
pilot study demonstrated that developing the template and using it to assess movement during the
“Lift Basket” task is feasible.
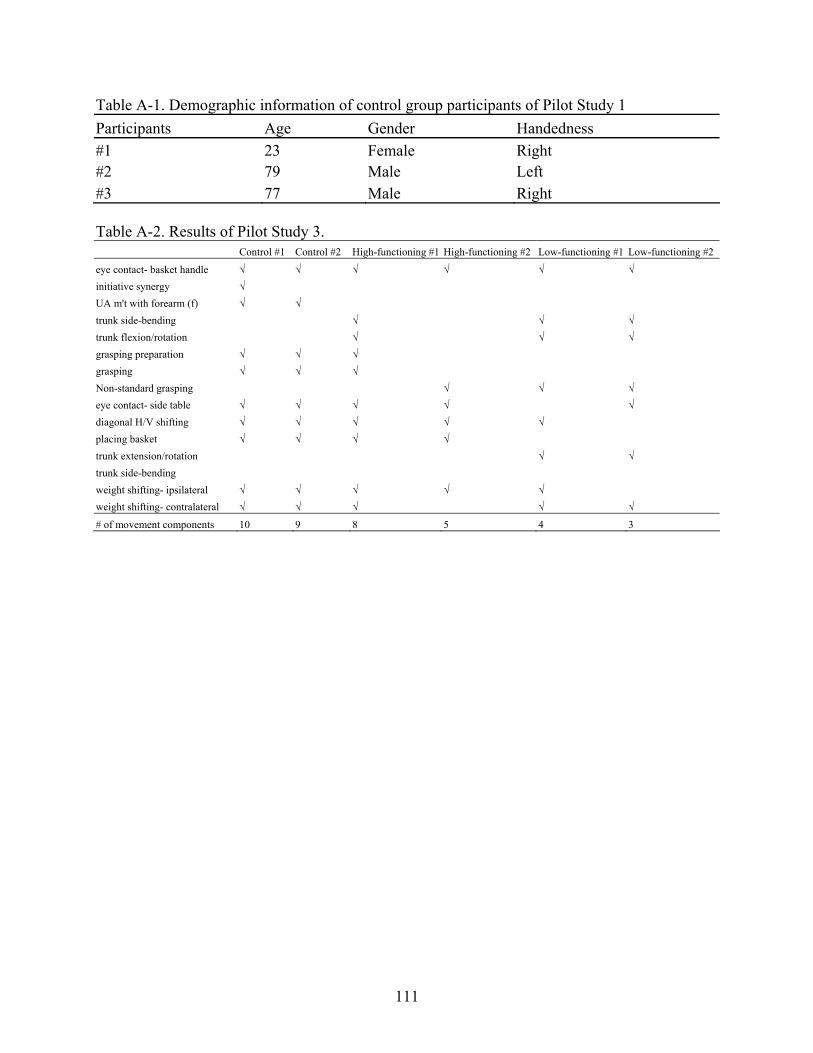
111
Table A-1. Demographic information of control group participants of Pilot Study 1 Participants Age Gender Handedness #1 23 Female Right #2 79 Male Left #3 77 Male Right Table A-2. Results of Pilot Study 3. Control #1 Control #2 High-functioning #1 High-functioning #2 Low-functioning #1 Low-functioning #2
eye contact- basket handle √ √ √ √ √ √ initiative synergy √ UA m't with forearm (f) √ √ trunk side-bending √ √ √ trunk flexion/rotation √ √ √ grasping preparation √ √ √ grasping √ √ √ Non-standard grasping √ √ √ eye contact- side table √ √ √ √ √ diagonal H/V shifting √ √ √ √ √ placing basket √ √ √ √ trunk extension/rotation √ √ trunk side-bending weight shifting- ipsilateral √ √ √ √ √ weight shifting- contralateral √ √ √ √ √
# of movement components 10 9 8 5 4 3
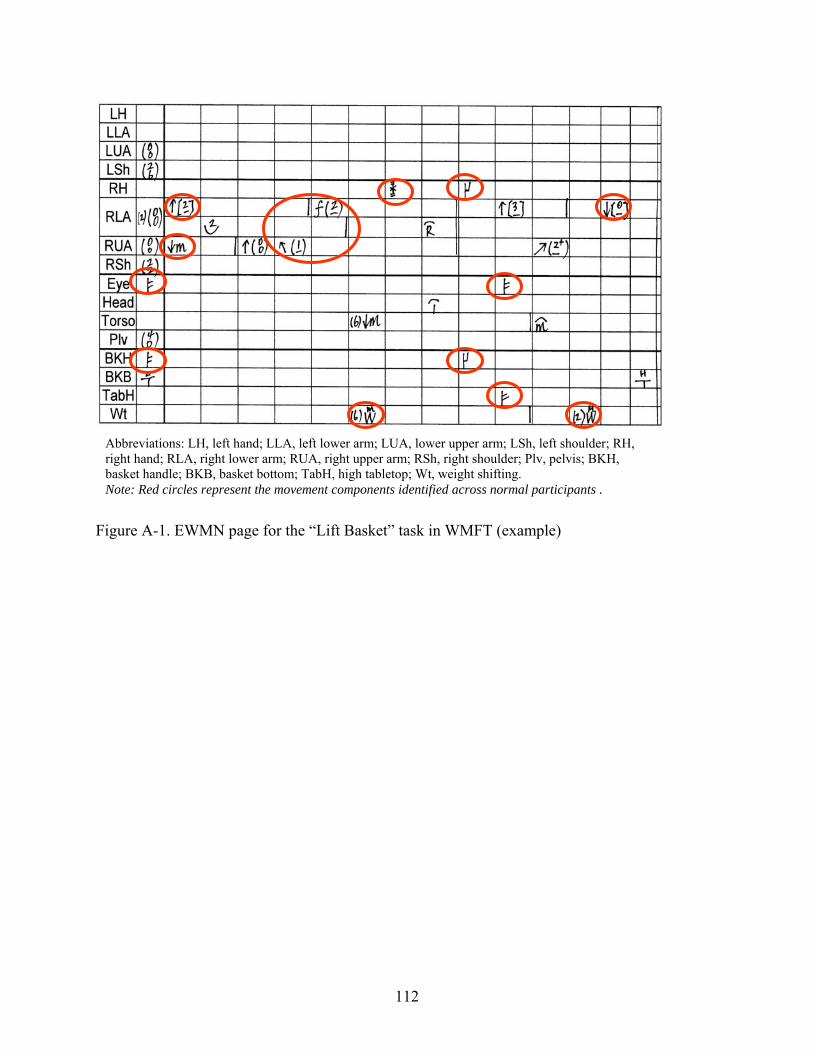
112
Figure A-1. EWMN page for the “Lift Basket” task in WMFT (example)
Abbreviations: LH, left hand; LLA, left lower arm; LUA, lower upper arm; LSh, left shoulder; RH, right hand; RLA, right lower arm; RUA, right upper arm; RSh, right shoulder; Plv, pelvis; BKH, basket handle; BKB, basket bottom; TabH, high tabletop; Wt, weight shifting. Note: Red circles represent the movement components identified across normal participants .
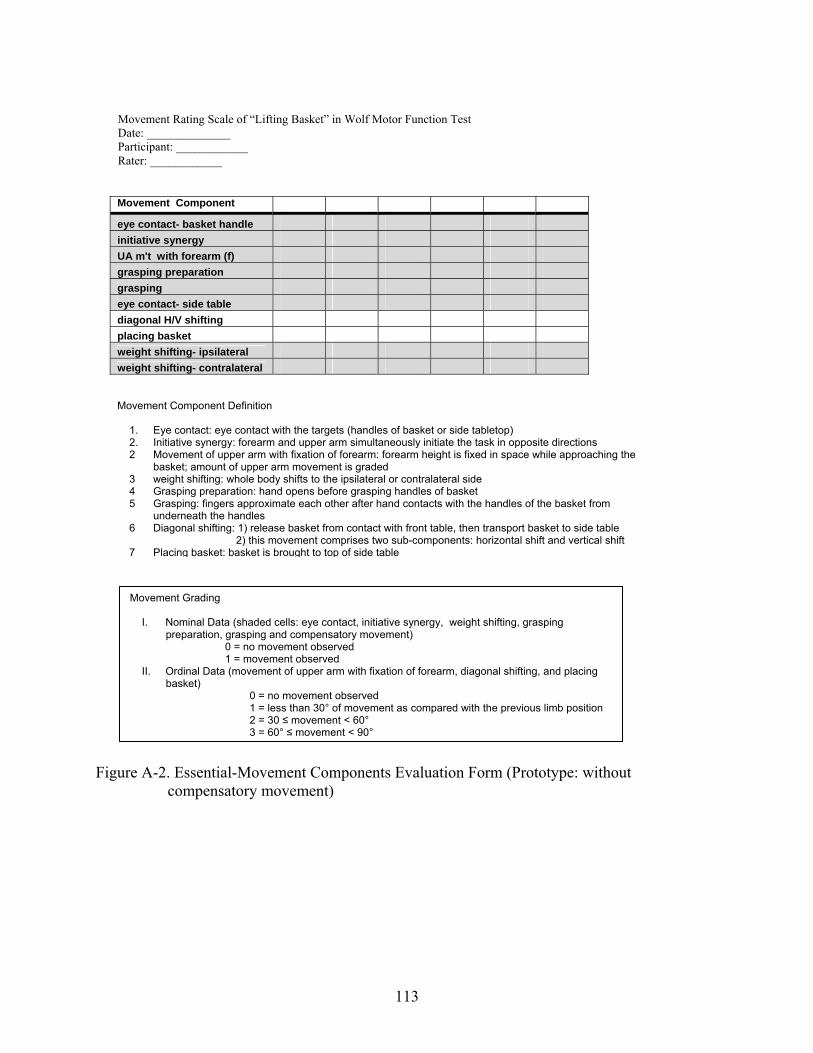
113
Figure A-2. Essential-Movement Components Evaluation Form (Prototype: without
compensatory movement)
Movement Rating Scale of “Lifting Basket” in Wolf Motor Function Test Date: ______________ Participant: ____________ Rater: ____________
Movement Component eye contact- basket handle initiative synergy UA m't with forearm (f) grasping preparation grasping eye contact- side table diagonal H/V shifting placing basket weight shifting- ipsilateral weight shifting- contralateral Movement Component Definition
1. Eye contact: eye contact with the targets (handles of basket or side tabletop) 2. Initiative synergy: forearm and upper arm simultaneously initiate the task in opposite directions 2 Movement of upper arm with fixation of forearm: forearm height is fixed in space while approaching the
basket; amount of upper arm movement is graded 3 weight shifting: whole body shifts to the ipsilateral or contralateral side 4 Grasping preparation: hand opens before grasping handles of basket 5 Grasping: fingers approximate each other after hand contacts with the handles of the basket from
underneath the handles 6 Diagonal shifting: 1) release basket from contact with front table, then transport basket to side table
2) this movement comprises two sub-components: horizontal shift and vertical shift 7 Placing basket: basket is brought to top of side table
Movement Grading
I. Nominal Data (shaded cells: eye contact, initiative synergy, weight shifting, grasping preparation, grasping and compensatory movement)
0 = no movement observed 1 = movement observed
II. Ordinal Data (movement of upper arm with fixation of forearm, diagonal shifting, and placing basket)
0 = no movement observed 1 = less than 30° of movement as compared with the previous limb position 2 = 30 ≤ movement < 60° 3 = 60° ≤ movement < 90°
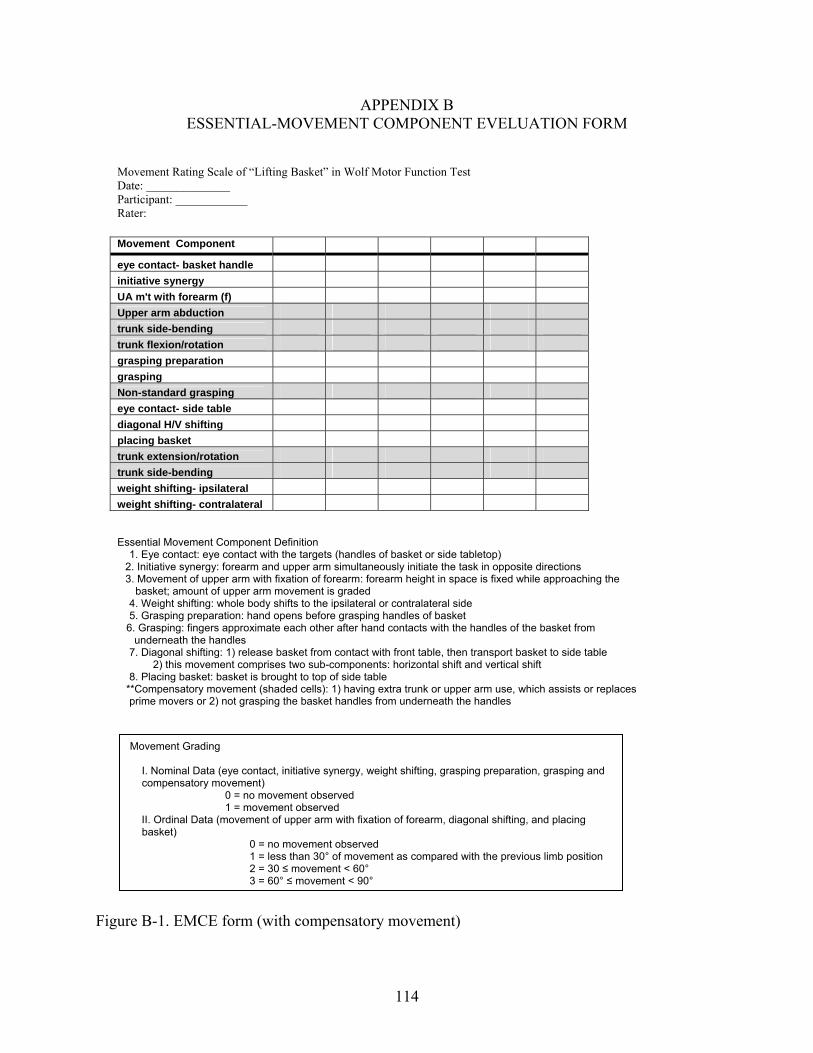
114
APPENDIX B ESSENTIAL-MOVEMENT COMPONENT EVELUATION FORM
Figure B-1. EMCE form (with compensatory movement)
Movement Grading
I. Nominal Data (eye contact, initiative synergy, weight shifting, grasping preparation, grasping and compensatory movement)
0 = no movement observed 1 = movement observed
II. Ordinal Data (movement of upper arm with fixation of forearm, diagonal shifting, and placing basket)
0 = no movement observed 1 = less than 30° of movement as compared with the previous limb position 2 = 30 ≤ movement < 60° 3 = 60° ≤ movement < 90°
Movement Component eye contact- basket handle initiative synergy UA m't with forearm (f) Upper arm abduction trunk side-bending trunk flexion/rotation grasping preparation grasping Non-standard grasping eye contact- side table diagonal H/V shifting placing basket trunk extension/rotation trunk side-bending weight shifting- ipsilateral weight shifting- contralateral
Essential Movement Component Definition 1. Eye contact: eye contact with the targets (handles of basket or side tabletop)
2. Initiative synergy: forearm and upper arm simultaneously initiate the task in opposite directions 3. Movement of upper arm with fixation of forearm: forearm height in space is fixed while approaching the
basket; amount of upper arm movement is graded 4. Weight shifting: whole body shifts to the ipsilateral or contralateral side 5. Grasping preparation: hand opens before grasping handles of basket 6. Grasping: fingers approximate each other after hand contacts with the handles of the basket from
underneath the handles 7. Diagonal shifting: 1) release basket from contact with front table, then transport basket to side table 2) this movement comprises two sub-components: horizontal shift and vertical shift 8. Placing basket: basket is brought to top of side table
**Compensatory movement (shaded cells): 1) having extra trunk or upper arm use, which assists or replaces prime movers or 2) not grasping the basket handles from underneath the handles
Movement Rating Scale of “Lifting Basket” in Wolf Motor Function Test Date: ______________ Participant: ____________ Rater:
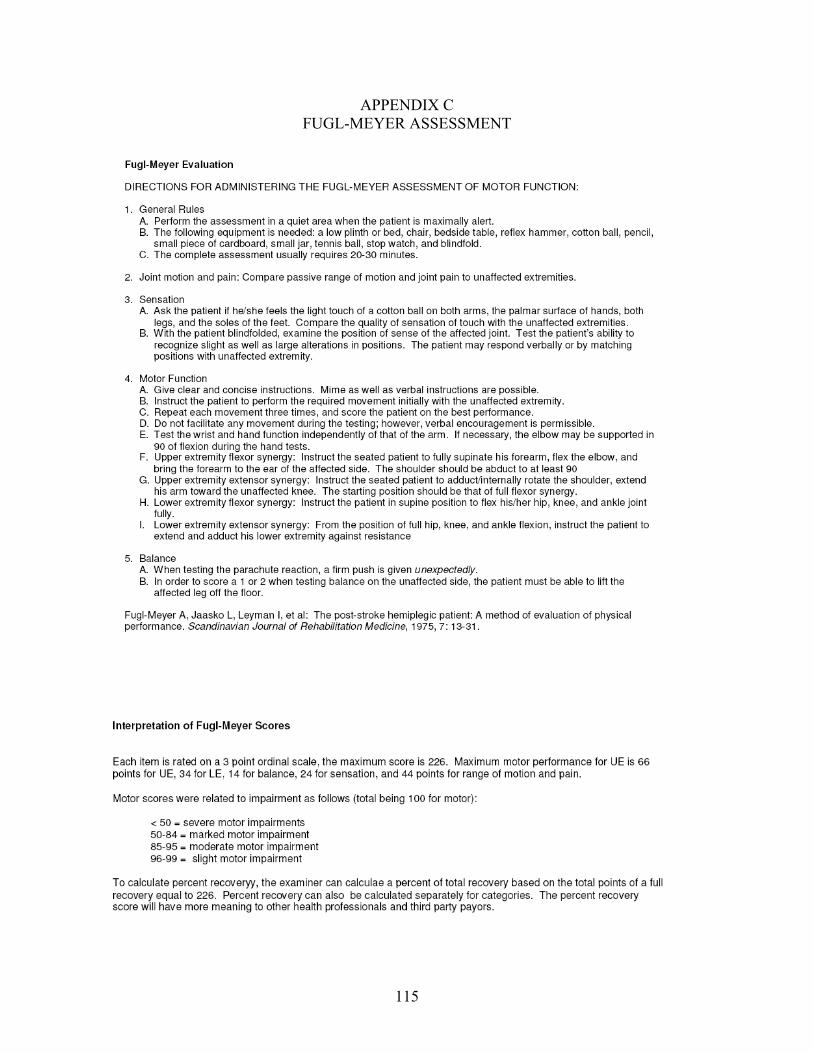
115
APPENDIX C FUGL-MEYER ASSESSMENT
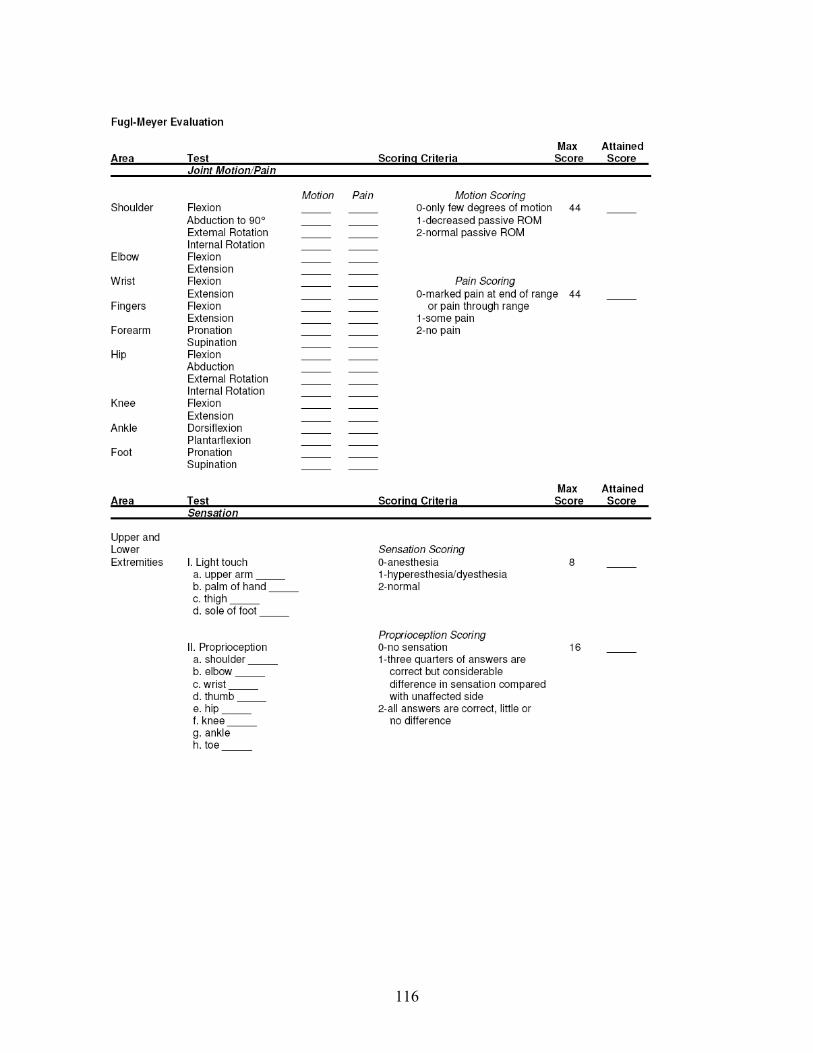
116
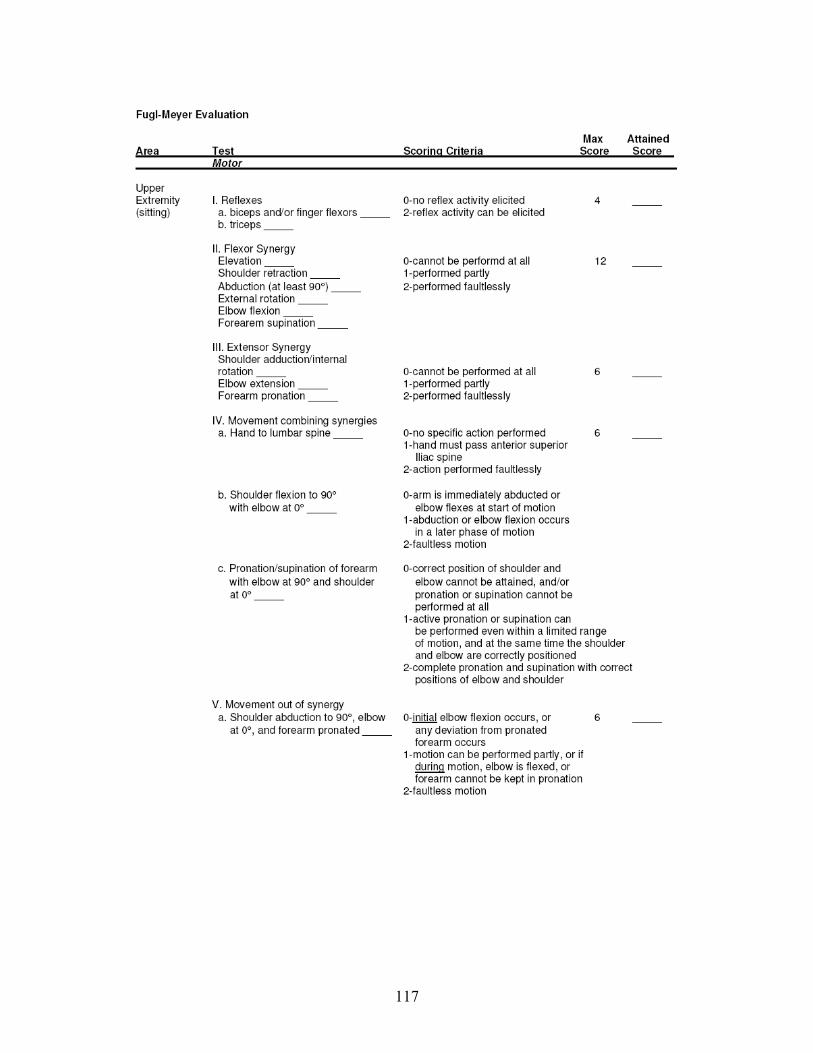
117
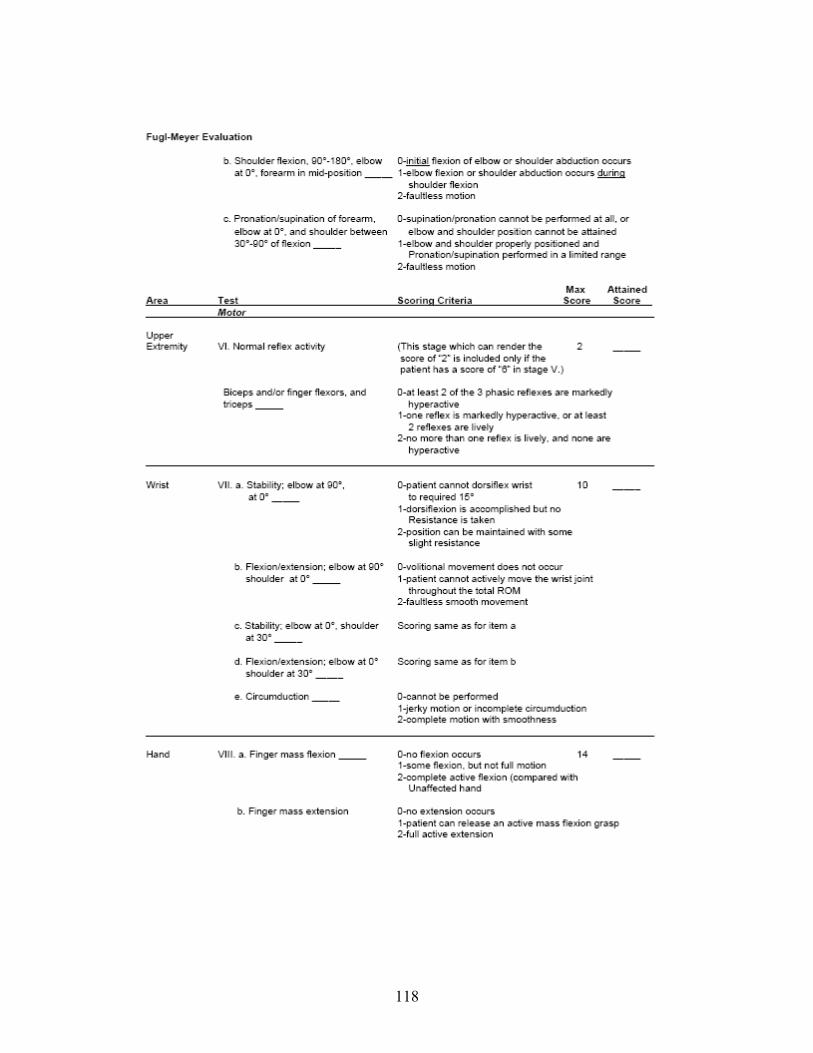
118
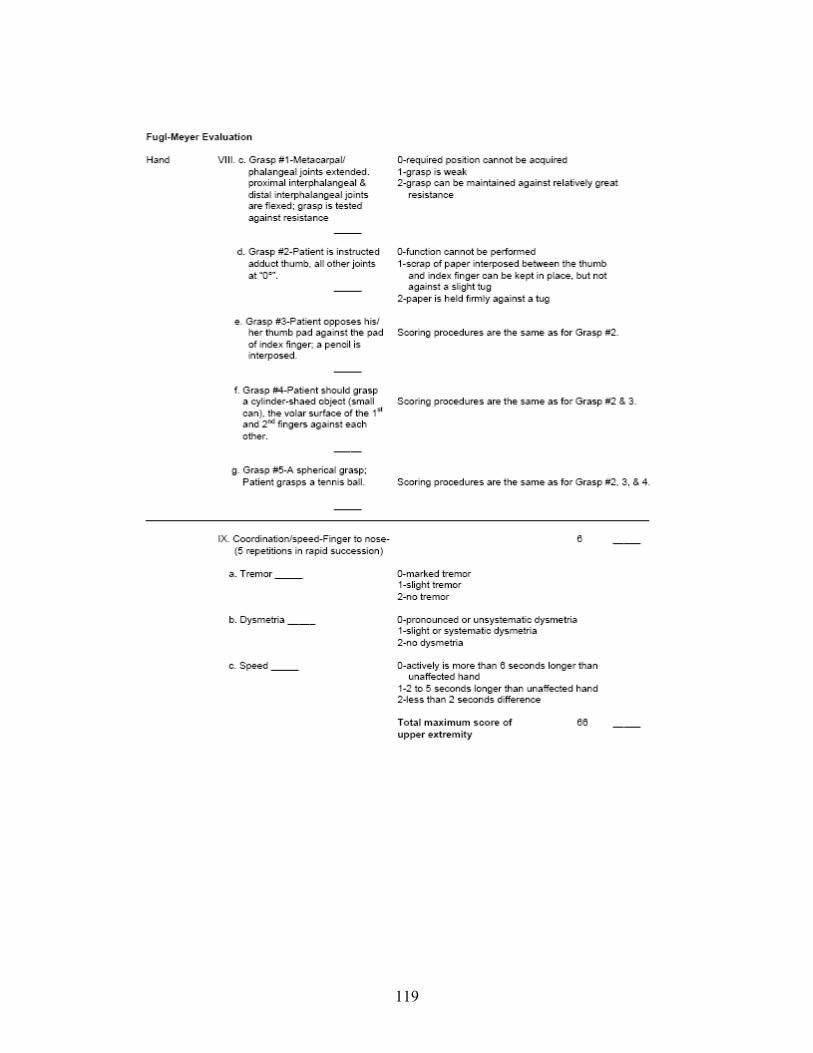
119
120
LIST OF REFERENCES
1. Taub E, Miller NE, Novack TA, et al. Technique to improve chronic motor deficit after stroke. Arch Phys Med Rehabil. Apr 1993;74(4):347-354.
2. Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics--2007 update:
a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. Feb 6 2007;115(5):e69-171.
3. Kwakkel G, Kollen B, Wagenaar R. Therapy impact on functional recovery in stroke
rehabilitation: a critical review of the literature. Physiotherapy. 1999;85(7):377-391. 4. Sunderland A, Tinson D, Bradley L, Hewer RL. Arm function after stroke. An evaluation
of grip strength as a measure of recovery and a prognostic indicator. J Neurol Neurosurg Psychiatry. Nov 1989;52(11):1267-1272.
5. Wade DT, Langton-Hewer R, Wood VA, Skilbeck CE, Ismail HM. The hemiplegic arm
after stroke: measurement and recovery. J Neurol Neurosurg Psychiatry. Jun 1983;46(6):521-524.
6. American Heart Association. Heart disease and stroke statistics-2005 update. Dallas,
TX: American Heart Association; 2004. 7. Ernst E. A review of stroke rehabilitation and physiotherapy. Stroke. Jul
1990;21(7):1081-1085. 8. Bourbonnais D, Vanden Noven S. Weakness in patients with hemiparesis. Am J Occup
Ther. May 1989;43(5):313-319. 9. Ryerson SD. Hemiplegia. In: Umphred D, ed. Neurological rehabilitation. 4th ed. St.
Louis, MO: Mosby; 2001:741-789. 10. Chae J, Yang G, Park BK, Labatia I. Muscle weakness and cocontraction in upper limb
hemiparesis: relationship to motor impairment and physical disability. Neurorehabil Neural Repair. Sep 2002;16(3):241-248.
11. Sheean G. Neurophysiology of spasticity. In: Barnes M, Johnson, GR, ed. Upper motor
neuron syndrome and spasticity. New York, NY: Cambridge University Press; 2000:12-78.
12. Brunnstrom S. Movement therapy in hemiplegia: a neurophysiological approach. New
York, NY: Harper & Row; 1970. 13. Bobath B. Adult hemiplgia: evaluation and treatment. 3rd ed. Oxford: Heinemann
Medical; 1990.
121
14. Carr J, Shepherd R. A motor learning model for rehabilitation. In: Carr J, Shepherd R, Gordon J, Gentile A, Held J, eds. Movement science: foundations for physical therapy in rehabilitation. Rockville, MD: Aspen; 1987:31-91.
15. Archambault P, Pigeon P, Feldman AG, Levin MF. Recruitment and sequencing of
different degrees of freedom during pointing movements involving the trunk in healthy and hemiparetic subjects. Exp Brain Res. May 1999;126(1):55-67.
16. Reisman DS, Scholz JP. Aspects of joint coordination are preserved during pointing in
persons with post-stroke hemiparesis. Brain. Nov 2003;126(Pt 11):2510-2527. 17. Cirstea MC, Mitnitski AB, Feldman AG, Levin MF. Interjoint coordination dynamics
during reaching in stroke. Exp Brain Res. Aug 2003;151(3):289-300. 18. Gillen G. Upper Extremity Function and Management. In: Gillen G, Burkhardt A, eds.
Stroke Rehabilitation: A Functional-Based Approach. St. Louis: Mosby; 1998:109-151. 19. Bogousslavsky J, Van Melle G, Regli F. The Lausanne Stroke Registry: analysis of 1,000
consecutive patients with first stroke. Stroke. Sep 1988;19(9):1083-1092. 20. Karatas M, Cetin N, Bayramoglu M, Dilek A. Trunk muscle strength in relation to
balance and functional disability in unihemispheric stroke patients. Am J Phys Med Rehabil. Feb 2004;83(2):81-87.
21. Ryerson SD, Levit K. Functional movement reeducation: a contemporary model for
stroke rehabilitation. New York: Churchill Livingstone; 1997. 22. Twitchell TE. The restoration of motor function following hemiplegia in man. Brain. Dec
1951;74(4):443-480. 23. O'Sullivan SB. Examination of motor function: motor control and motor learning. In:
O'Sullivan SB, Schmitz TJ, eds. Physical Rehabilitation. 5th ed. Philadephia: F.A. Davis; 2007:227-272.
24. Lance JW. Symposium synopsis. In: Feldman RG, Young RR, Koella WP, eds.
Spasticity: disorder of motor control. Chicago: Year Book Medical Publishers; 1980:485-494.
25. Bennett SE, Karnes JL. Neurological Disability: Assessment and Treatment. Philadephia:
Lippincott; 1998. 26. Shepherd R. Training motor control in individuals with movement dysfunction following
brain lesions. Paper presented at: Conference at Rehabilitation Institute of Chicago, 1994; Chicago.
122
27. Magoun HW, Rhines R. Spasticity: the stretch-reflex and extrapyramidal systems. Springfield, IL: Charles C Thomas; 1947.
28. Boyd RN, Ada L. Physiotherapy management of spasticity. In: Barnes M, Johnson G, eds. Upper motor neuron syndrome and spasticity. Cambridge: Cambridge; 2000:96-121.
29. Good DC. Measurement of spasticity. In: Gelber DA, Jeffery DR, eds. Clinical
evaluation and management of spasticity. Totowa, NJ: Humana Press; 2002:27-46. 30. Shumway-Cook A, Woollacott MH. Motor Control : Theory and Practical Applications.
1st ed. Philadelphia: Lippincott Williams & Wilkins; 1995. 31. O'Sullivan SB. Stroke. In: O'Sullivan SB, Schmitz TJ, eds. Physical Rehabilitation:
Assessment and Treatment. Philadelphia: F. A. Davis Company; 1988:327-360. 32. Welmer AK, von Arbin M, Widen Holmqvist L, Sommerfeld DK. Spasticity and its
association with functioning and health-related quality of life 18 months after stroke. Cerebrovasc Dis. 2006;21(4):247-253.
33. Sommerfeld DK, Eek EU, Svensson AK, Holmqvist LW, von Arbin MH. Spasticity after
stroke: its occurrence and association with motor impairments and activity limitations. Stroke. Jan 2004;35(1):134-139.
34. Watkins CL, Leathley MJ, Gregson JM, Moore AP, Smith TL, Sharma AK. Prevalence
of spasticity post stroke. Clin Rehabil. Aug 2002;16(5):515-522. 35. O'Sullivan SB. Motor Control Assessment. In: O'Sullivan SB, Schmitz TJ, eds. Physical
Rehabilitation: Assessment and Treatment. 3rd ed. Philadelphia: F. A. Davis Company; 1988:111-131.
36. O'Sullivan SB. Stroke. In: O'Sullivan SB, Schmitz TJ, eds. Physical Rehabilitation. 5th
ed. Philadephia: F.A. Davis; 2007:705-776. 37. Cowie AS. Oxford advanced learner's dictionary of current English. 4th ed. Oxford:
Oxford University Press; 1989. 38. Schmidt RA, Lee TD. Motor control and learning: a behavioral emphasis. 3rd ed.
Champaign, IL: Human Kinetics; 1999. 39. Matsuo Y, Asai Y, Nomura T, et al. Intralimb incoordination in patients with ataxia.
Neuroreport. Nov 14 2003;14(16):2057-2059. 40. Nakamura R, Taniguchi R. Reaction time in patients with cerebral hemiparesis.
Neuropsychologia. 1977;15(6):845-848. 41. Sahrmann SA, Norton BJ. The relationship of voluntary movement to spasticity in the
upper motor neuron syndrome. Ann Neurol. Dec 1977;2(6):460-465.
123
42. Cirstea MC, Levin MF. Compensatory strategies for reaching in stroke. Brain. May
2000;123 ( Pt 5):940-953. 43. Roby-Brami A, Feydy A, Combeaud M, Biryukova EV, Bussel B, Levin MF. Motor
compensation and recovery for reaching in stroke patients. Acta Neurol Scand. May 2003;107(5):369-381.
44. Kusoffsky A, Apel I, Hirschfeld H. Reaching-lifting-placing task during standing after
stroke: Coordination among ground forces, ankle muscle activity, and hand movement. Arch Phys Med Rehabil. May 2001;82(5):650-660.
45. Michaelsen SM, Jacobs S, Roby-Brami A, Levin MF. Compensation for distal
impairments of grasping in adults with hemiparesis. Exp Brain Res. Jul 2004;157(2):162-173.
46. Hamill J, Knutzen K. Biomechanical basis of human movement. Baltimore, MD:
Lippincott Williams & Wilkins; 2003. 47. Davies P. Steps to follow: a guide to the treatment of adult hemiplegia. Berlin: Springer-
Verlag; 1993. 48. Bukowski E. Muscular analysis of everyday activities. Thorofare, NJ: Slack; 2000. 49. Winter DA. Biomechanics and Motor Control of Human Movement. 3rd ed. Hoboken,
NJ: John Wiley & Sons, Inc.; 2005. 50. Wolf SL, Lecraw DE, Barton LA, Jann BB. Forced use of hemiplegic upper extremities
to reverse the effect of learned nonuse among chronic stroke and head-injured patients. Exp Neurol. May 1989;104(2):125-132.
51. Barreca S, Gowland CK, Stratford P, et al. Development of the Chedoke Arm and Hand
Activity Inventory: theoretical constructs, item generation, and selection. Top Stroke Rehabil. Fall 2004;11(4):31-42.
52. Barreca SR, Stratford PW, Lambert CL, Masters LM, Streiner DL. Test-retest reliability,
validity, and sensitivity of the Chedoke arm and hand activity inventory: a new measure of upper-limb function for survivors of stroke. Arch Phys Med Rehabil. Aug 2005;86(8):1616-1622.
53. Barreca SR, Stratford PW, Masters LM, Lambert CL, Griffiths J. Comparing 2 versions
of the chedoke arm and hand activity inventory with the action research arm test. Phys Ther. Feb 2006;86(2):245-253.

124
54. Levin MF, Desrosiers J, Beauchemin D, Bergeron N, Rochette A. Development and validation of a scale for rating motor compensations used for reaching in patients with hemiparesis: the reaching performance scale. Phys Ther. Jan 2004;84(1):8-22.
55. Pang MY, Harris JE, Eng JJ. A community-based upper-extremity group exercise program improves motor function and performance of functional activities in chronic stroke: a randomized controlled trial. Arch Phys Med Rehabil. Jan 2006;87(1):1-9.
56. McCombe Waller S, Whitall J. Hand dominance and side of stroke affect rehabilitation in
chronic stroke. Clin Rehabil. Aug 2005;19(5):544-551. 57. Wolf SL, Thompson PA, Morris DM, et al. The EXCITE trial: attributes of the Wolf
Motor Function Test in patients with subacute stroke. Neurorehabil Neural Repair. Sep 2005;19(3):194-205.
58. Fritz SL, Light KE, Patterson TS, Behrman AL, Davis SB. Active finger extension
predicts outcomes after constraint-induced movement therapy for individuals with hemiparesis after stroke. Stroke. Jun 2005;36(6):1172-1177.
59. Liamputtong P, Ezzy D. Qualitative Research Methods. 2nd ed. South Melbourne,
Australia: Oxford University Press; 2005. 60. Baum F. Researching public health: behind the qualitative-quantitative methodological
debate. Soc Sci Med. Feb 1995;40(4):459-468. 61. Denzin NK, Lincoln YS. Handbook of Qualitative Research. 2nd ed. Thousand Oaks,
CA: Sage Publication; 2000. 62. Portney LG, Watkins MP. Foundations of clinical research: Applications to practice.
Upper Saddle River, NJ: Prentice Hall Health; 2000. 63. Pomeroy VM, Pramanik A, Sykes L, Richards J, Hill E. Agreement between
physiotherapists on quality of movement rated via videotape. Clin Rehabil. May 2003;17(3):264-272.
64. Miltner WH, Bauder H, Sommer M, Dettmers C, Taub E. Effects of constraint-induced
movement therapy on patients with chronic motor deficits after stroke: a replication. Stroke. Mar 1999;30(3):586-592.
65. Kunkel A, Kopp B, Muller G, et al. Constraint-induced movement therapy for motor
recovery in chronic stroke patients. Arch Phys Med Rehabil. Jun 1999;80(6):624-628. 66. Morris D, Crago J, DeLuca S, Pidikiti R, Taub E. Constraint-Induced Movement Therapy
for motor recovery after stroke. Neurorehabilitation. 1997;9:29-43.
125
67. Taub E, Uswatte G, Pidikiti R. Constraint-Induced Movement Therapy: a new family of techniques with broad application to physical rehabilitation- a clinical review. J Rehabil Res Dev. 1999;36(3):237-251.
68. Taub E, Wolf S. Constraint induced movement techniques to facilitate upper extremity
use in stroke patients. Topics in Rehabil. 1997;3(4):38-61. 69. Blanton S, Wolf SL. An application of upper-extremity constraint-induced movement
therapy in a patient with subacute stroke. Phys Ther. Sep 1999;79(9):847-853. 70. Tarkka IM, Pitkanen K, Sivenius J. Paretic hand rehabilitation with constraint-induced
movement therapy after stroke. Am J Phys Med Rehabil. Jul 2005;84(7):501-505. 71. Bonifer NM, Anderson KM, Arciniegas DB. Constraint-induced movement therapy after
stroke: efficacy for patients with minimal upper-extremity motor ability. Arch Phys Med Rehabil. Sep 2005;86(9):1867-1873.
72. Bonifer NM, Anderson KM, Arciniegas DB. Constraint-induced therapy for moderate
chronic upper extremity impairment after stroke. Brain Inj. May 2005;19(5):323-330. 73. Bonifer N, Anderson KM. Application of constraint-induced movement therapy for an
individual with severe chronic upper-extremity hemiplegia. Phys Ther. Apr 2003;83(4):384-398.
74. Wolf SL, Blanton S, Baer H, Breshears J, Butler AJ. Repetitive task practice: a critical
review of constraint-induced movement therapy in stroke. Neurologist. Nov 2002;8(6):325-338.
75. Cirstea MC, Ptito A, Levin MF. Arm reaching improvements with short-term practice
depend on the severity of the motor deficit in stroke. Exp Brain Res. Oct 2003;152(4):476-488.
76. Bond T, CM F. Applying the rasch model: fundamental measurement in the human
sciences. Mahwah, NJ: Lawrence Erlbaum Associates; 2001. 77. Roby-Brami A, Jacobs S, Bennis N, Levin MF. Hand orientation for grasping and arm
joint rotation patterns in healthy subjects and hemiparetic stroke patients. Brain Res. Apr 18 2003;969(1-2):217-229.
78. Galley PM, Forster AC. Human movement: an introductory text for physiotherapy
studies. 2nd ed. Melbourne: Churchill Livingstone; 1987. 79. Piccinini L, Cimolin V, Galli M, Berti M, Crivellini M, Turconi AC. Quantification of
energy expenditure during gait in children affected by cerebral palsy. Eura Medicophys. Oct 3 2006.
126
80. Platts MM, Rafferty D, Paul L. Metabolic cost of over ground gait in younger stroke patients and healthy controls. Med Sci Sports Exerc. Jun 2006;38(6):1041-1046.
81. David D, Regnaux JP, Lejaille M, Louis A, Bussel B, Lofaso F. Oxygen consumption during machine-assisted and unassisted walking: a pilot study in hemiplegic and healthy humans. Arch Phys Med Rehabil. Apr 2006;87(4):482-489.
82. Ashburn A, Partridge C, DrSouza L. Physiotherapy in the rehabilitation of stroke. Clin
Rehabil. 1993;7:337-345. 83. Edwards S. An analysis of normal movement as the basis for the development of
treatment techniques. In: Edwards S, ed. Neurological Physiotherapy. A Problem Solving Approach. New York: Churchill Livingstone; 1996:15-40.
84. Higgins JR. Human Movement: An integrated approach. St. Louis, MO: The C. V.
Mosby Company; 1977. 85. Schmidt RA. A schema theory of discrete motor skill learning. Psychological Review.
1975;82(4):225-260. 86. Shea CH, Wulf G. Schema theory: a critical appraisal and reevaluation. J Mot Behav.
Mar 2005;37(2):85-101. 87. Lashley KS. The problem of cerebral organization in vision. In: Cattell J, ed. Biological
symposia. Vol VII. Lancaster, PA: Jaques Cattell Press; 1942:301-322. 88. Levin MF. Interjoint coordination during pointing movements is disrupted in spastic
hemiparesis. Brain. Feb 1996;119 ( Pt 1):281-293. 89. Michaelsen SM, Levin MF. Short-term effects of practice with trunk restraint on reaching
movements in patients with chronic stroke: a controlled trial. Stroke. Aug 2004;35(8):1914-1919.
90. Eshkol N, Wachman A. Movement notation. London: Weidenfeld and Wicolson; 1958. 91. Eshkol N. The hand book. Tel Aviv, Israel: The Movement Notation Society; 1971. 92. Eshkol N. Twenty-five lessons by Dr. Moshe Feldenkrais. Tel Aviv, Israel: The
Movement Notation Society; 1976. 93. Whishaw IQ, Pellis SM, Gorny BP, Pellis VC. The impairments in reaching and the
movements of compensation in rats with motor cortex lesions: an endpoint, videorecording, and movement notation analysis. Behav Brain Res. Jan 31 1991;42(1):77-91.
127
94. Teitelbaum P, Teitelbaum O, Nye J, Fryman J, Maurer RG. Movement analysis in infancy may be useful for early diagnosis of autism. Proc Natl Acad Sci U S A. Nov 10 1998;95(23):13982-13987.
95. Farr TD, Whishaw IQ. Quantitative and qualitative impairments in skilled reaching in the mouse (Mus musculus) after a focal motor cortex stroke. Stroke. Jul 2002;33(7):1869-1875.
96. Whishaw IQ, Suchowersky O, Davis L, Sarna J, Metz GA, Pellis SM. Impairment of
pronation, supination, and body co-ordination in reach-to-grasp tasks in human Parkinson's disease (PD) reveals homology to deficits in animal models. Behav Brain Res. Jul 18 2002;133(2):165-176.
97. Teitelbaum O, Benton T, Shah PK, Prince A, Kelly JL, Teitelbaum P. Eshkol-Wachman
movement notation in diagnosis: the early detection of Asperger's syndrome. Proc Natl Acad Sci U S A. Aug 10 2004;101(32):11909-11914.
98. McGraw KO, Wong SP. Forming inferences about some intraclass correlation
coefficients. Psychological Method. 1996(1):30-46. 99. Shrout PE, Fleiss JL. Intraclass correlations: use in assessing rater reliability.
Psychological Bulletin. 1979;86(2):420-428. 100. Stevens EM, Jr., Vos GA, Stephens JP, Moore JS. Inter-rater reliability of the strain
index. J Occup Environ Hyg. Nov 2004;1(11):745-751. 101. Winstein CJ, Miller JP, Blanton S, et al. Methods for a multisite randomized trial to
investigate the effect of constraint-induced movement therapy in improving upper extremity function among adults recovering from a cerebrovascular stroke. Neurorehabil Neural Repair. Sep 2003;17(3):137-152.
102. Wolf SL. Wolf Motor Function Test. Extremity Constraint-Induced Therapy Evaluation
(EXCITE) Manual of Procedures. Atlanta: Emory University School of Medicine; 2001. 103. Knudson D, Morrison C. Qualitative analysis of human movement. 2nd ed. Champaign,
IL: Human Kinetics; 2002. 104. Mukherjee D, Levin RL, Heller W. The cognitive, emotional, and social sequelae of
stroke: psychological and ethical concerns in post-stroke adaptation. Top Stroke Rehabil. Fall 2006;13(4):26-35.
105. Wolf SL, Winstein CJ, Miller JP, et al. Effect of constraint-induced movement therapy on
upper extremity function 3 to 9 months after stroke: the EXCITE randomized clinical trial. Jama. Nov 1 2006;296(17):2095-2104.
106. Van de Winckel A, Feys H, van der Knaap S, et al. Can quality of movement be
measured? Rasch analysis and inter-rater reliability of the Motor Evaluation Scale for
128
Upper Extremity in Stroke Patients (MESUPES). Clin Rehabil. Oct 2006;20(10):871-884.
107. Cirstea MC, Levin MF. Improvement of arm movement patterns and endpoint control depends on type of feedback during practice in stroke survivors. Neurorehabil Neural Repair. Sep-Oct 2007;21(5):398-411.
108. Desrosiers J, Hebert R, Bravo G, Dutil E. Upper extremity performance test for the
elderly (TEMPA): normative data and correlates with sensorimotor parameters. Test d'Evaluation des Membres Superieurs de Personnes Agees. Arch Phys Med Rehabil. Dec 1995;76(12):1125-1129.
109. Wolf SL. Revisiting Constraint-Induced Movement Therapy: Are We Too Smitten With
the Mitten? Is All Nonuse "Learned"? and Other Quandaries. Phys Ther. Sep 2007;87(9):1212-1223.
110. Sanford J, Moreland J, Swanson LR, Stratford PW, Gowland C. Reliability of the Fugl-
Meyer assessment for testing motor performance in patients following stroke. Phys Ther. Jul 1993;73(7):447-454.
111. Nadeau SE, Behrman AL, Davis SE, et al. Donepezil as an adjuvant to constraint-induced
therapy for upper-limb dysfunction after stroke: An exploratory randomized clinical trial. J Rehabil Res Dev. Jul 2004;41(4):525-534.
112. Fritz SL. Functional and Descriptive Predictors of Outcomes Following Constraint-
Induced Movement Therapy for Individuals with Post-Stroke Hemiparesis. Gainesville: Rehabilitation Science, University of Florida; 2004.
113. Hsieh CL, Sheu CF, Hsueh IP, Wang CH. Trunk control as an early predictor of
comprehensive activities of daily living function in stroke patients. Stroke. Nov 2002;33(11):2626-2630.
114. Page SJ, Sisto S, Levine P, McGrath RE. Efficacy of modified constraint-induced
movement therapy in chronic stroke: a single-blinded randomized controlled trial. Arch Phys Med Rehabil. Jan 2004;85(1):14-18.
115. Gimenez-Roldan S, Novillo MJ, Navarro E, Dobato JL, Gimenez-Zuccarelli M. [Mini-
mental state examination: proposal of protocol to be used]. Rev Neurol. Apr 1997;25(140):576-583.
116. Wolf SL, Binder-MacLeod SA. Electromyographic biofeedback applications to the
hemiplegic patient. Changes in upper extremity neuromuscular and functional status. Phys Ther. Sep 1983;63(9):1393-1403.
117. Wolf SL. Electromyographic biofeedback applications to stroke patients. A critical
review. Phys Ther. Sep 1983;63(9):1448-1459.
129
118. Wolf SL, Miller JP, Clark PC, Woinstein CJ. The EXCITE trial: formulation, implementation, and results. Paper presented at: American Physical Therapy Association Combined Section Meeting 2006, 2006; San Diego, CA.
119. Katz J, Melzack R. Measurement of pain. Surg Clin North Am. Apr 1999;79(2):231-252. 120. Harris KD, Heer DM, Roy TC, Santos DM, Whitman JM, Wainner RS. Reliability of a
measurement of neck flexor muscle endurance. Phys Ther. Dec 2005;85(12):1349-1355. 121. Domholdt E. Rehabilitation research: Principles and applications. 3rd ed. St Louis:
Elsevier; 2005. 122. Michener LA, Boardman ND, Pidcoe PE, Frith AM. Scapular muscle tests in subjects
with shoulder pain and functional loss: reliability and construct validity. Phys Ther. Nov 2005;85(11):1128-1138.
123. Nunnally JC, Bernstein IH. Psychometric theory. New York: McGraw-Hill; 1994. 124. Leggin BG, Michener LA, Shaffer MA, Brenneman SK, Iannotti JP, Williams GR, Jr.
The Penn shoulder score: reliability and validity. J Orthop Sports Phys Ther. Mar 2006;36(3):138-151.
125. Fleiss JL. The design and analysis of clinical experiement. New York: John Wiley &
Sons, Inc.; 1986. 126. Beaton DE. Understanding the relevance of measured change through studies of
responsiveness. Spine. Dec 15 2000;25(24):3192-3199. 127. Cech DJ, Martin ST. Functional movement development: across the life span. 2nd ed.
Philadephia: W.B. Saunders; 2002. 128. Brownstein B. Movement Biomechanics and Control. In: Brownstein B, Bronner S, eds.
Functional Movement in Orthopardic and Sports Physical Therapy: Evaluation, treatment, and outcomes. New York: Churchill Livingstone; 1997:1-42.
129. Voss DE, Ionta MK, Myers BJ. Proprioceptive neuromuscular facilitation : patterns and
techniques. 3rd ed. Philadelphia: Harper & Row; 1985. 130. Salbach NM, Jaglal SB, Korner-Bitensky N, Rappolt S, Davis D. Practitioner and
organizational barriers to evidence-based practice of physical therapists for people with stroke. Phys Ther. Oct 2007;87(10):1284-1303; discussion 1304-1286.
131. Duncan PW. Barriers to evidence-based physical therapist practice for people with
stroke. Phys Ther. 2007;87(10):1304-1305.
130
132. Chiu Y-P. Examining the Invariant Features of a Complex Task in Individuals Post-Stroke who Received Constraint-Induced Movement Therapy. [Dissertation]. Gainesville: Physical Therapy, University of Florida; 2007.
133. Tessem S, Hagstrom N, Fallang B. Weight distribution in standing and sitting positions,
and weight transfer during reaching tasks, in seated stroke subjects and healthy subjects. Physiother Res Int. Jun 2007;12(2):82-94.
134. Reisman DS, Scholz JP. Deficits in surface force production during seated reaching in
people after stroke. Phys Ther. Mar 2007;87(3):326-336. 135. Michaelsen SM, Luta A, Roby-Brami A, Levin MF. Effect of trunk restraint on the
recovery of reaching movements in hemiparetic patients. Stroke. Aug 2001;32(8):1875-1883.
136. Michaelsen SM, Dannenbaum R, Levin MF. Task-specific training with trunk restraint on
arm recovery in stroke: randomized control trial. Stroke. Jan 2006;37(1):186-192. 137. Latash ML, Anson JG. What are ''normal movements'' in atypical populations?
Behavioral and Brain Sciences. Mar 1996;19(1):55-&. 138. Konczak J, Dichgans J. The concept of "normal" movement and its consequence for
therapy. Behavioral and Brain Sciences. 1996;19(1):79. 139. Levin MF. Should stereotypic movement synergies in hemiparetic patients be considered
adaptive? Behavioral and Brain Sciences. 1996;19(1):79-80. 140. Cirstea CM, Ptito A, Levin MF. Feedback and cognition in arm motor skill reacquisition
after stroke. Stroke. May 2006;37(5):1237-1242. 141. de Oliveira R, Cacho EW, Borges G. Improvements in the upper limb of hemiparetic
patients after reaching movements training. Int J Rehabil Res. Mar 2007;30(1):67-70. 142. Page SJ, Sisto S, Johnston MV, Levine P. Modified constraint-induced therapy after
subacute stroke: A preliminary study. Neurorehabilitation and Neural Repair. Sep 2002;16(3):290-295.
143. Alberts JL, Butler AJ, Wolf SL. The effects of constraint-induced therapy on precision
grip: a preliminary study. Neurorehabil Neural Repair. Dec 2004;18(4):250-258. 144. Roby-Brami A, Bennis N, Mokhtari M, Baraduc P. Hand orientation for grasping
depends on the direction of the reaching movement. Brain Res. Jun 30 2000;869(1-2):121-129.
145. Horak F. Assumptions underlying motor control for neurologic rehabilitation. Paper
presented at: Proceedings of the II-Step Conference, 1992; Alexandria, VA.
131
146. Carr JH, Shepherd RB. Movement Science: Foundations for Physical Therapy Rehabilitation. Rockville, MD: Aspen; 1987.
147. Kwakkel G. Impact of intensity of practice after stroke: issues for consideration. Disabil
Rehabil. Jul 15-30 2006;28(13-14):823-830. 148. Thielman GT, Dean CM, Gentile AM. Rehabilitation of reaching after stroke: task-
related training versus progressive resistive exercise. Arch Phys Med Rehabil. Oct 2004;85(10):1613-1618.
132
BIOGRAPHICAL SKETCH
I received my Bachelor of Science in Physical Therapy from the National Cheng Kung
University (NCKU), Tainan, Taiwan in 1995. After fulfilling a 2-year mandatory military
service, I returned to NCKU in 1997 and worked as a teaching assistant at the Department of
Physical Therapy for 2 years. To accumulate clinical experience, I also worked as a physical
therapist in a variety of settings, including outpatient and home care, on a part-time basis. Based
on these valuable experiences, I noticed therapeutic techniques that physical therapists use can
mostly rely on personal clinical observations. The lack of evidence and support for neurological
physical therapy led me to the University of Florida in 1999, where I pursued a Master Degree in
Health Science and a Doctoral Degree in Rehabilitation Science. I received my Master of Health
Science in Physical Therapy at the University of Florida in 2001.
My main research concentration in the Rehabilitation Science Doctoral program was
movement dysfunction and my minor concentration was gerontology. I have been involved in
numerous research projects, especially in stroke rehabilitation. Under the supervision of my
mentor, Dr. Kathye E. Light, I have been working on a series of studies of Constraint-Induced
Movement Therapy (CIMT) to improve upper-extremity function in stroke population. During
the first half of my doctoral study, I used electromyography to study muscle activation patterns
of upper extremity post-stroke. However, a chance of research collaboration with Dr. Philip
Teitelbaum at the Department of Psychology determined the direction of my dissertation. My
focus of the study was using the Eshkol-Wachman Movement Notation to develop a movement
evaluation template for measuring quality of movement post-stroke.