Embed Size (px)
Citation preview

Baby is blue ..What to do ?
Approach to a cyanotic newbornDr Bharathi
Case Scenario 1
• B/o X
• Term / male /AGA born to primi mother by vaginal delivery .
• Baby cried immediately after birth and is otherwise well .
• There is cyanosis of peripheries alone….
Acrocyanosis
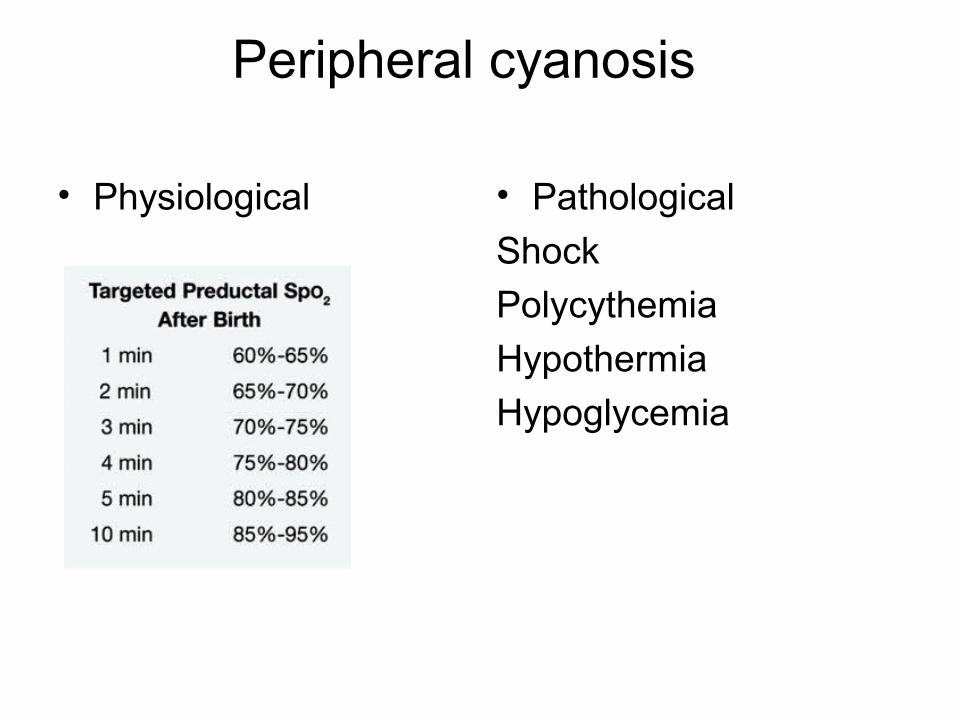
Peripheral cyanosis
• Physiological • Pathological
Shock
Polycythemia
Hypothermia
Hypoglycemia
Although peripheral cyanosis is seen in conditions in which the infant is exposed to a cold environment, it could also be the presenting sign of serious conditions such as
• sepsis, • hypoglycemia, • hypoplastic left-heart syndrome
Peripheral cyanosis should not be ignored unless other conditions have been ruled out.

Case scenario 2
• A concerned mother brings her newborn to you
“ One side of my baby is blue and the other side is red . What is this ?”
Harlequin skin change
• One quadrant or one half of the body may become cyanotic or pale while the rest of the body remains pink.
• Hands and feet remain warm.
• Exact reason not known
• Thought to be - vasomotor instability
What would you call it if the upper half is pink and the lower half is blue ?
• Differential cyanosis
• Seen in PDA with R – L shunting
Case scenario 3
• Term / AGA baby born to primi mother by SVD . Cried well at birth . Was well for 1st 3 days.
• On day 4 child develops lethargy , poor feeding , cold extremities and is blue over face , tongue , hands and feet .
• How will you approach ?
Cyanosis
• Cyanosis (from the Greek word meaning ‘‘dark blue’’) is a blue to dusky hue in the newborn
• Colour of the reduced hemoglobin gives rise to the colour seen in cyanosis.
• Lees reported that cyanosis would be visible if the deoxygenated hemoglobin content is greater than 3 g% (3 g per 100 mL).
Sasidharan P. An approach to diagnosis and management of cyanosis and tachypnea in term infants. Pediatr. Clin. North Am. 2004 Aug;51(4):999–1021, ix.
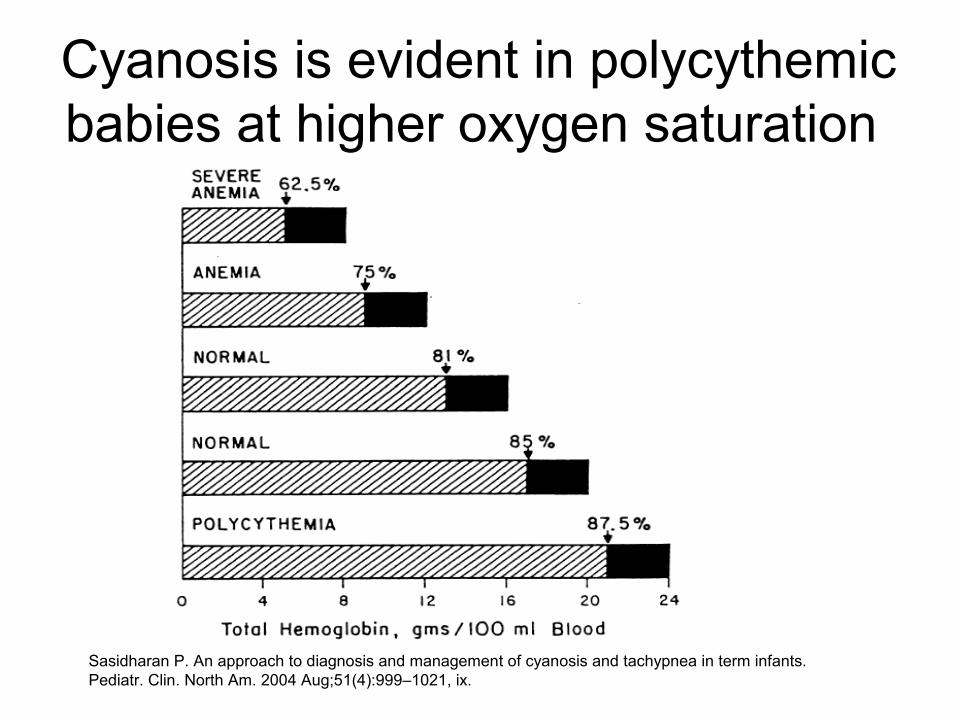
Cyanosis is evident in polycythemic babies at higher oxygen saturation
Sasidharan P. An approach to diagnosis and management of cyanosis and tachypnea in term infants. Pediatr. Clin. North Am. 2004 Aug;51(4):999–1021, ix.
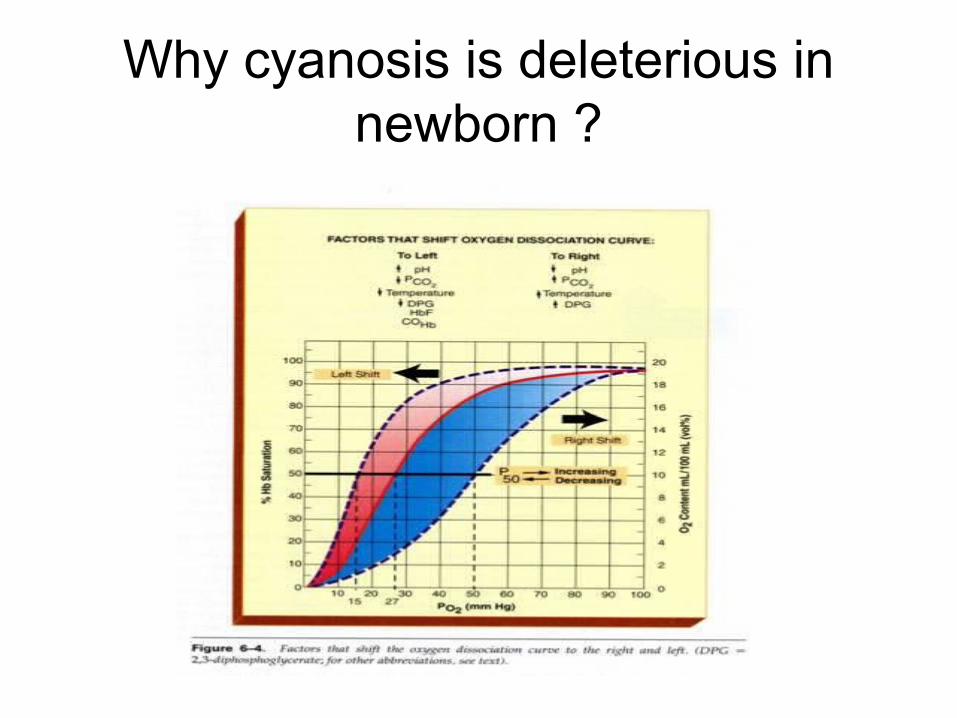
Why cyanosis is deleterious in newborn ?
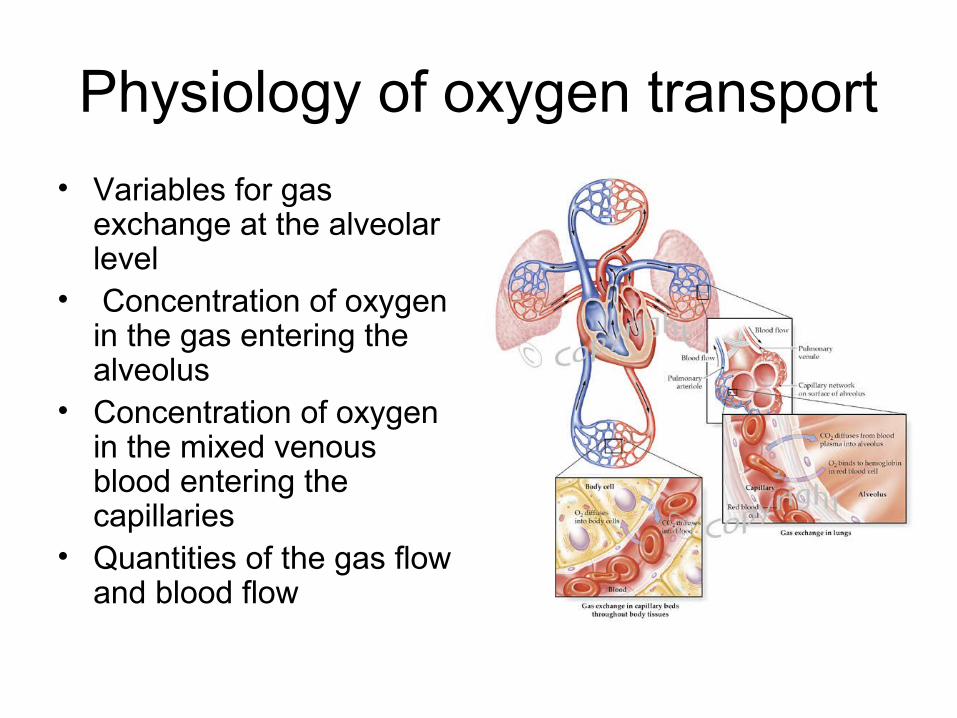
Physiology of oxygen transport
• Variables for gas exchange at the alveolar level
• Concentration of oxygen in the gas entering the alveolus
• Concentration of oxygen in the mixed venous blood entering the capillaries
• Quantities of the gas flow and blood flow
Causes of cyanosis - pathophysiology
• Hypoventilation
• Significant right-to-left intracardiac or intrapulmonary shunting
• Ventilation perfusion unevenness
• Inadequate transport of oxygen by the hemoglobin.
Sasidharan P. An approach to diagnosis and management of cyanosis and tachypnea in term infants.
Pediatr. Clin. North Am. 2004 Aug;51(4):999–1021, ix.
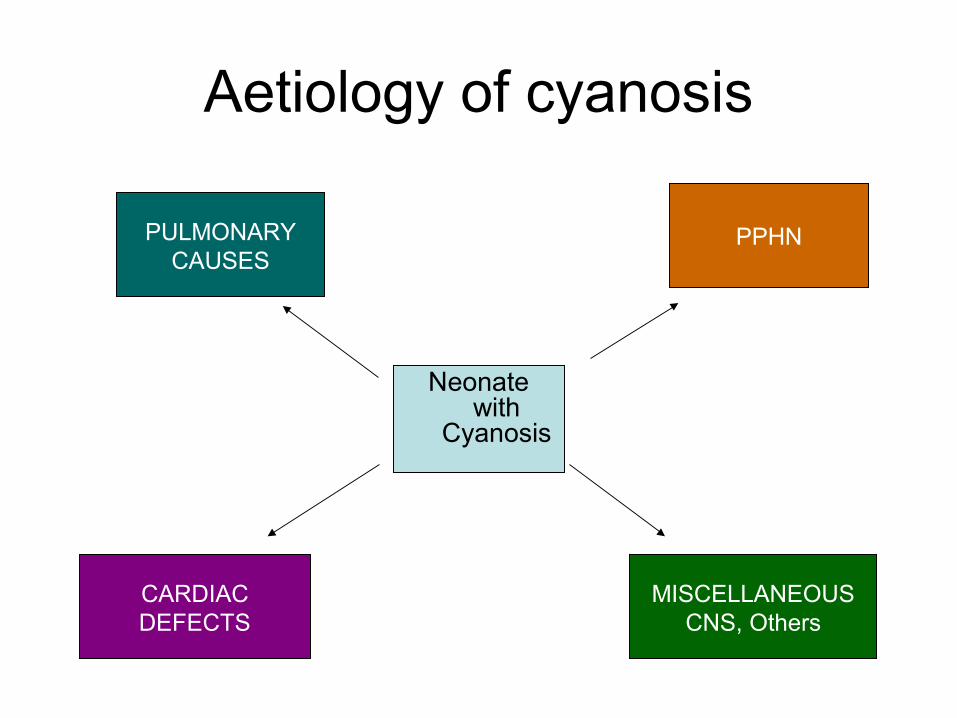
Aetiology of cyanosis
PULMONARYCAUSES
PPHN
CARDIACDEFECTS
MISCELLANEOUSCNS, Others
Neonate with
Cyanosis
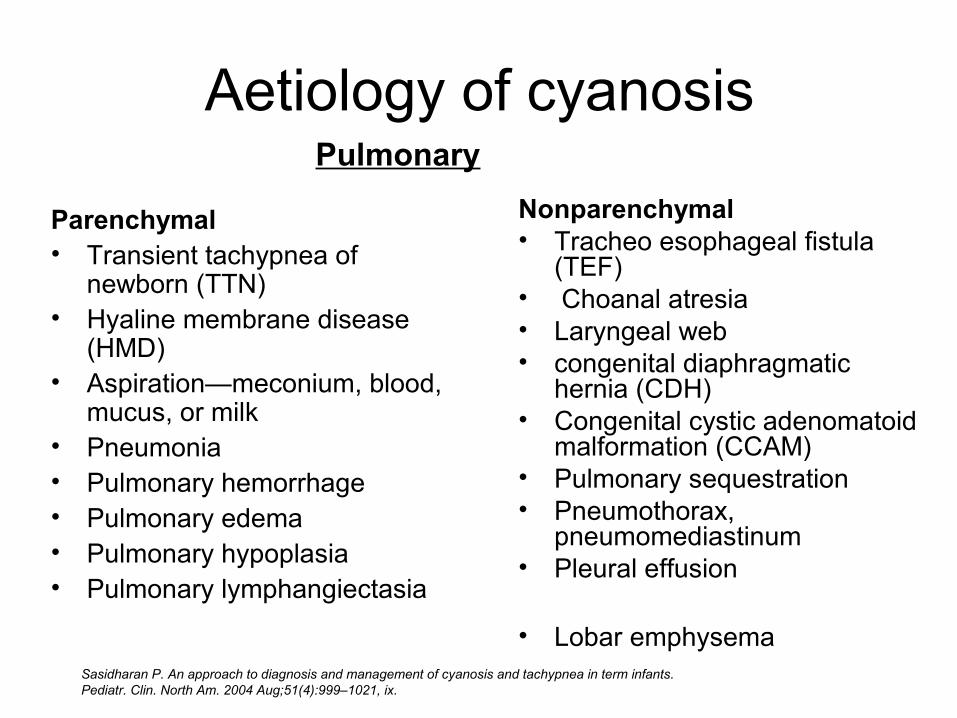
Aetiology of cyanosis
Parenchymal• Transient tachypnea of
newborn (TTN)• Hyaline membrane disease
(HMD)• Aspiration—meconium, blood,
mucus, or milk• Pneumonia• Pulmonary hemorrhage• Pulmonary edema• Pulmonary hypoplasia• Pulmonary lymphangiectasia
Nonparenchymal• Tracheo esophageal fistula
(TEF)• Choanal atresia• Laryngeal web• congenital diaphragmatic
hernia (CDH)• Congenital cystic adenomatoid
malformation (CCAM)• Pulmonary sequestration• Pneumothorax,
pneumomediastinum• Pleural effusion
• Lobar emphysema
Pulmonary
Sasidharan P. An approach to diagnosis and management of cyanosis and tachypnea in term infants. Pediatr. Clin. North Am. 2004 Aug;51(4):999–1021, ix.
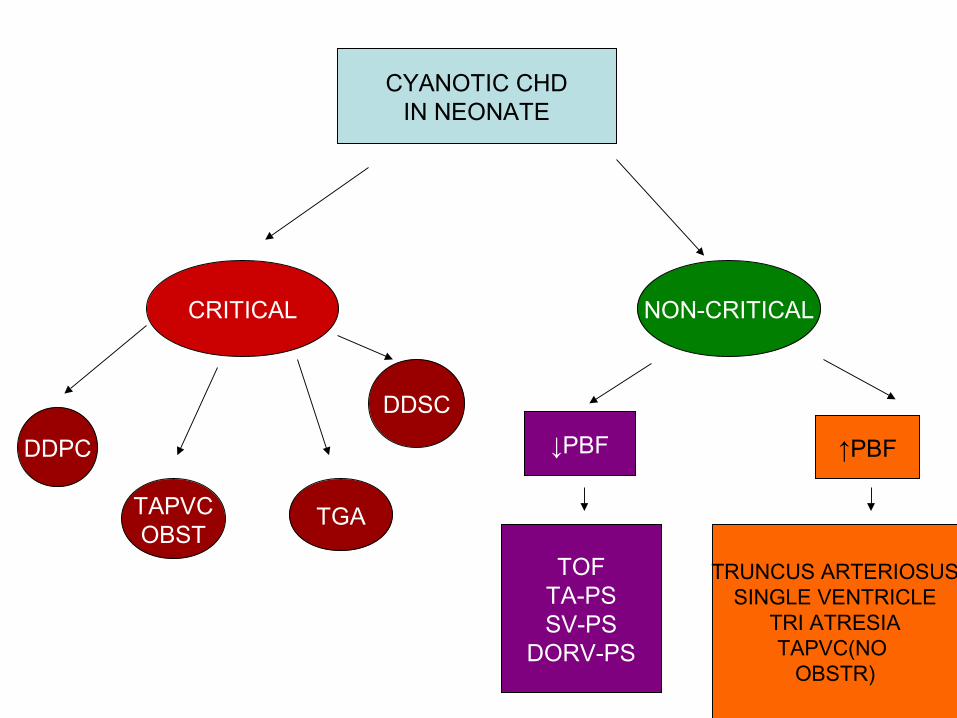
CYANOTIC CHDIN NEONATE
CRITICAL NON-CRITICAL
↓PBF ↑PBF
TOFTA-PSSV-PS
DORV-PS
TRUNCUS ARTERIOSUSSINGLE VENTRICLE
TRI ATRESIATAPVC(NO
OBSTR)
DDSC
TGATAPVCOBST
DDPC
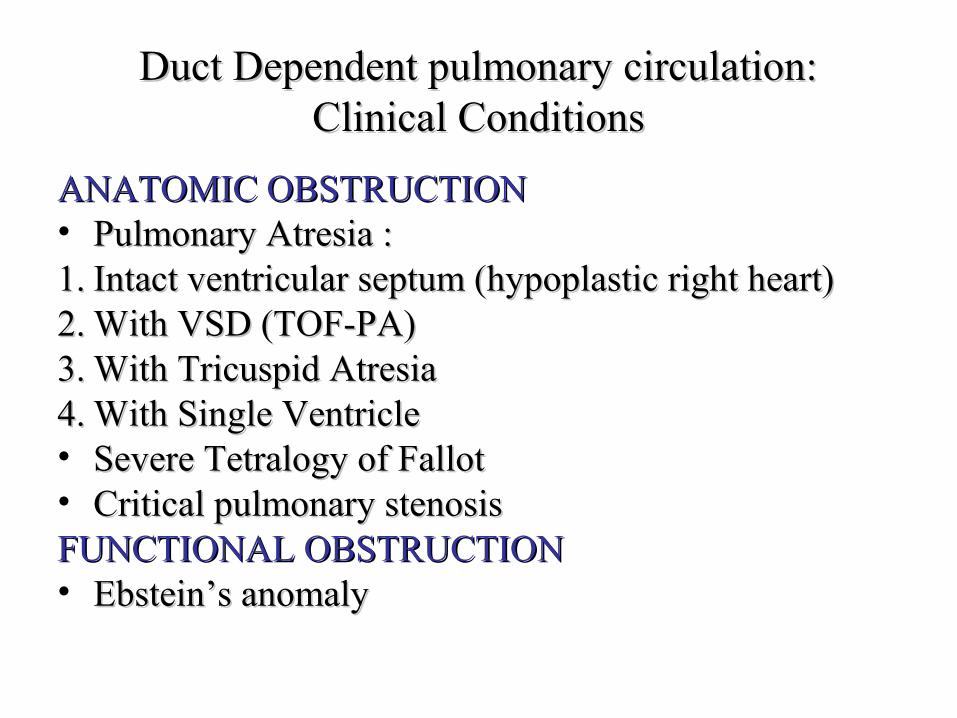
Duct Dependent pulmonary circulation:Duct Dependent pulmonary circulation:Clinical ConditionsClinical Conditions
ANATOMIC OBSTRUCTIONANATOMIC OBSTRUCTION• Pulmonary Atresia : Pulmonary Atresia : 1.1. Intact ventricular septum (hypoplastic right heart)Intact ventricular septum (hypoplastic right heart)2.2. With VSD (TOF-PA)With VSD (TOF-PA)3.3. With Tricuspid AtresiaWith Tricuspid Atresia4.4. With Single VentricleWith Single Ventricle• Severe Tetralogy of FallotSevere Tetralogy of Fallot• Critical pulmonary stenosisCritical pulmonary stenosisFUNCTIONAL OBSTRUCTIONFUNCTIONAL OBSTRUCTION• Ebstein’s anomalyEbstein’s anomaly

Duct Dependent Systemic circulation:Duct Dependent Systemic circulation:Clinical ConditionsClinical Conditions
• Critical aortic stenosis
• Coarctation of aorta
• Interrupted aortic arch
• Hypoplastic left heart
Manual of neonatalogy – John P Cloherty – 17 th edition
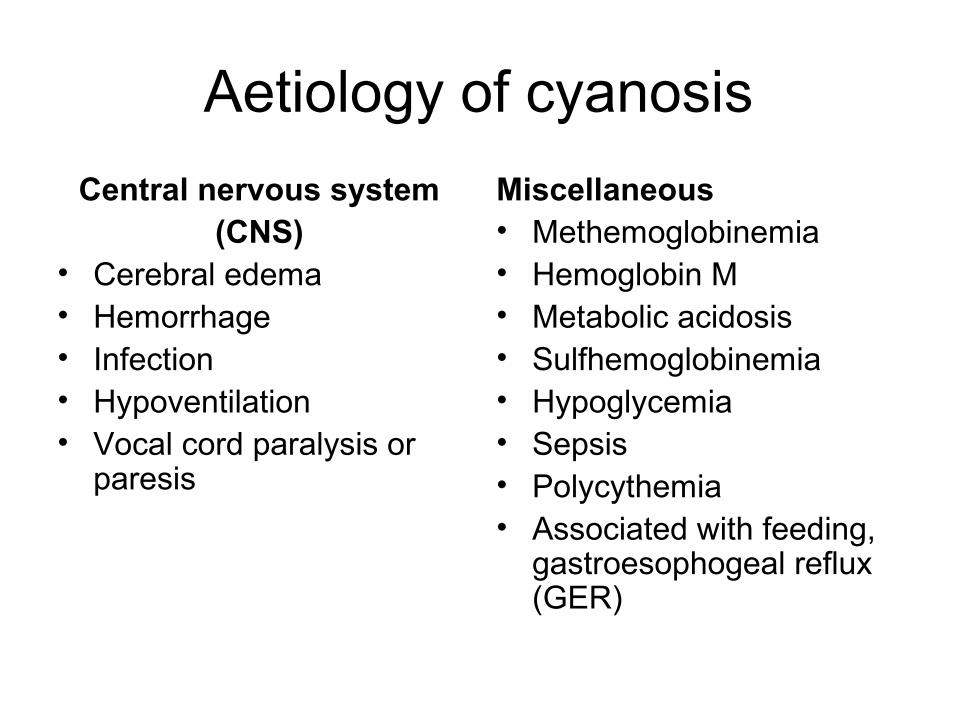
Aetiology of cyanosis
Central nervous system(CNS)
• Cerebral edema• Hemorrhage• Infection• Hypoventilation• Vocal cord paralysis or
paresis
Miscellaneous• Methemoglobinemia• Hemoglobin M• Metabolic acidosis• Sulfhemoglobinemia• Hypoglycemia• Sepsis• Polycythemia• Associated with feeding,
gastroesophogeal reflux (GER)
Initial assessment of infants who have cyanosis
•History•Physical examination•Chest radiograph•CBC with differential count•Blood glucose, calcium•Arterial blood gas (ABG)/hyperoxia test•Blood culture/sepsis screen•EKG and echocardiogram
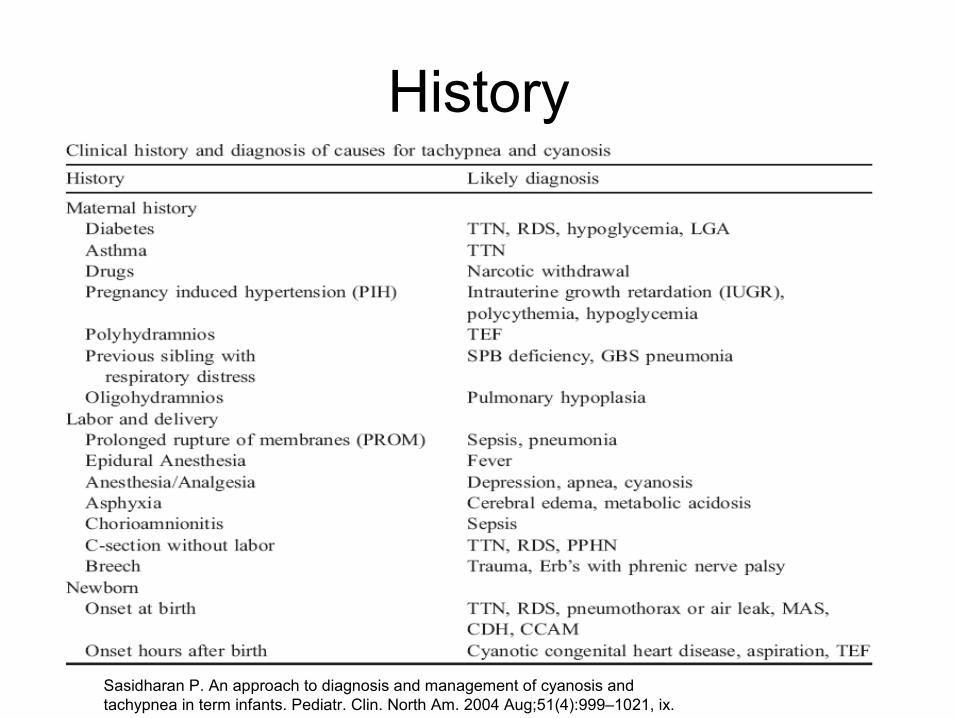
History
Sasidharan P. An approach to diagnosis and management of cyanosis and tachypnea in term infants. Pediatr. Clin. North Am. 2004 Aug;51(4):999–1021, ix.
Physical examination• Examined in neutral thermal environment• Away from blue phototherapy lights• Asses capillary refill time- <3 sec• Temperature , pallor, polycythemia, femoral pulses, BP of all 4
limbs• Barrel shaped chest –post term-MAS• Bell shaped thorax – neurologic abnormalities• Scaphoid abdomen-CDH• Look for nasal flaring,grunting & retractions• Airway – choanal atresia.• Pulse oximetry.
Sasidharan P. An approach to diagnosis and management of cyanosis and tachypnea in term infants. Pediatr. Clin. North Am. 2004 Aug;51(4):999–1021, ix.
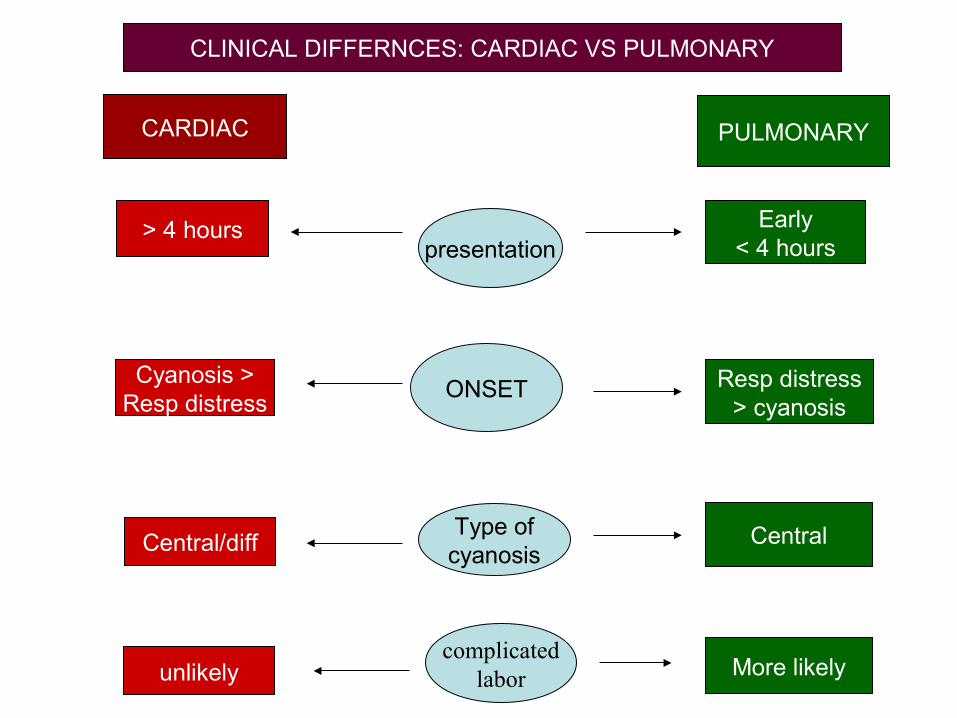
CARDIAC PULMONARY
Early< 4 hours
> 4 hourspresentation
Resp distress> cyanosis
Cyanosis >Resp distress
Type ofcyanosis
CentralCentral/diff
complicatedlabor More likelyunlikely
CLINICAL DIFFERNCES: CARDIAC VS PULMONARY
ONSET
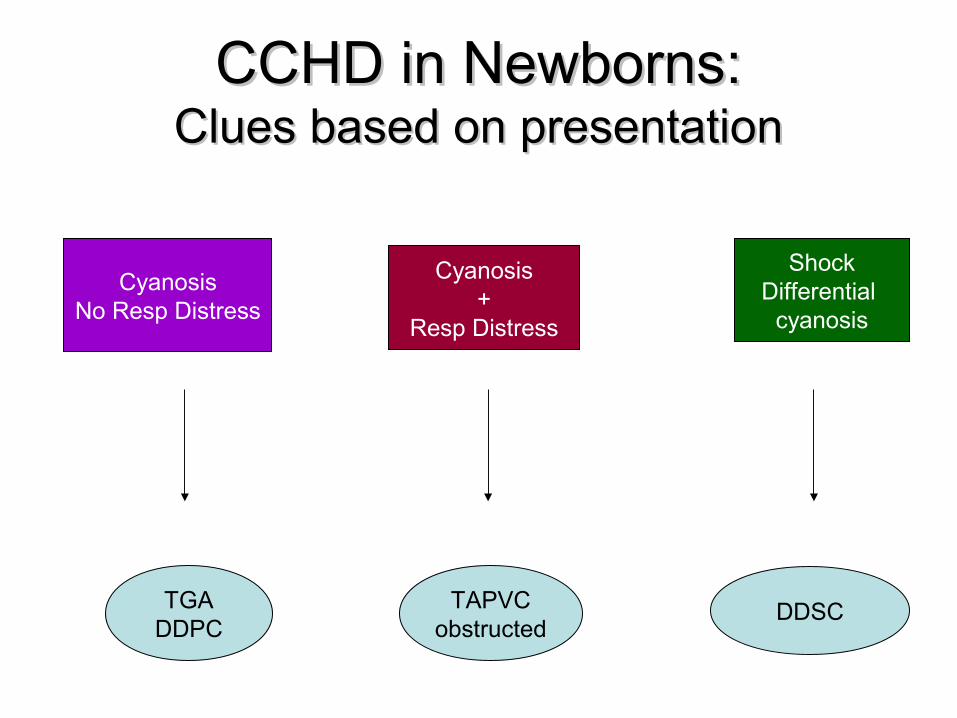
CCHD in Newborns:CCHD in Newborns:Clues based on presentationClues based on presentation
CyanosisNo Resp Distress
Cyanosis+
Resp Distress
ShockDifferential
cyanosis
TGADDPC
TAPVCobstructed
DDSC
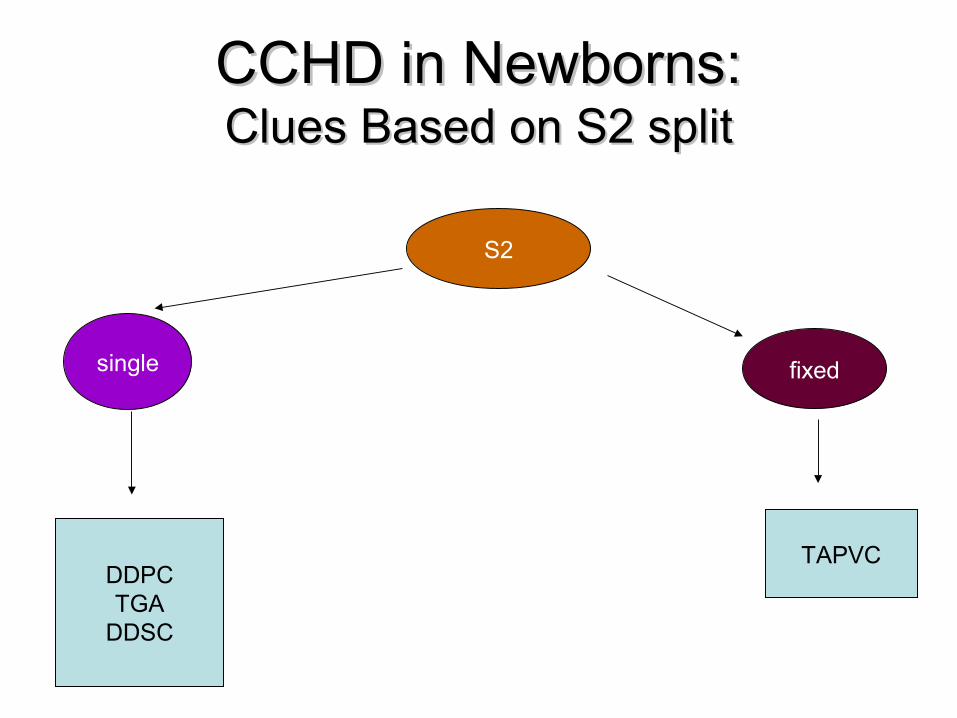
CCHD in Newborns:CCHD in Newborns:Clues Based on S2 splitClues Based on S2 split
S2
single fixed
DDPCTGA
DDSC
TAPVC
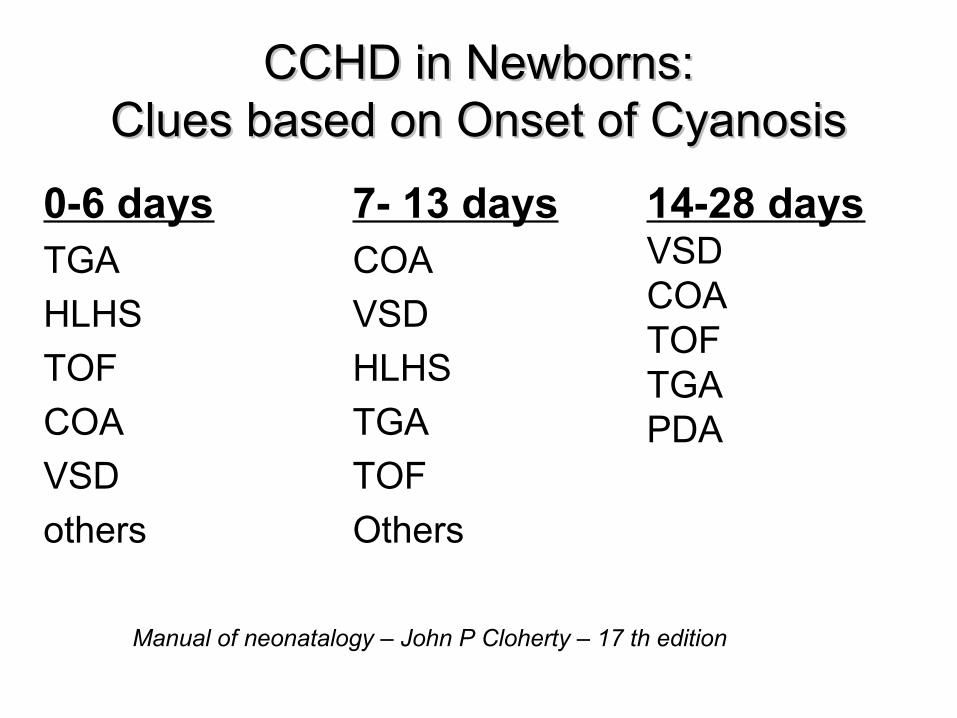
CCHD in Newborns:CCHD in Newborns:Clues based on Onset of CyanosisClues based on Onset of Cyanosis
0-6 daysTGA
HLHS
TOF
COA
VSD
others
7- 13 daysCOA
VSD
HLHS
TGA
TOF
Others
14-28 daysVSDCOATOFTGAPDA
Manual of neonatalogy – John P Cloherty – 17 th edition
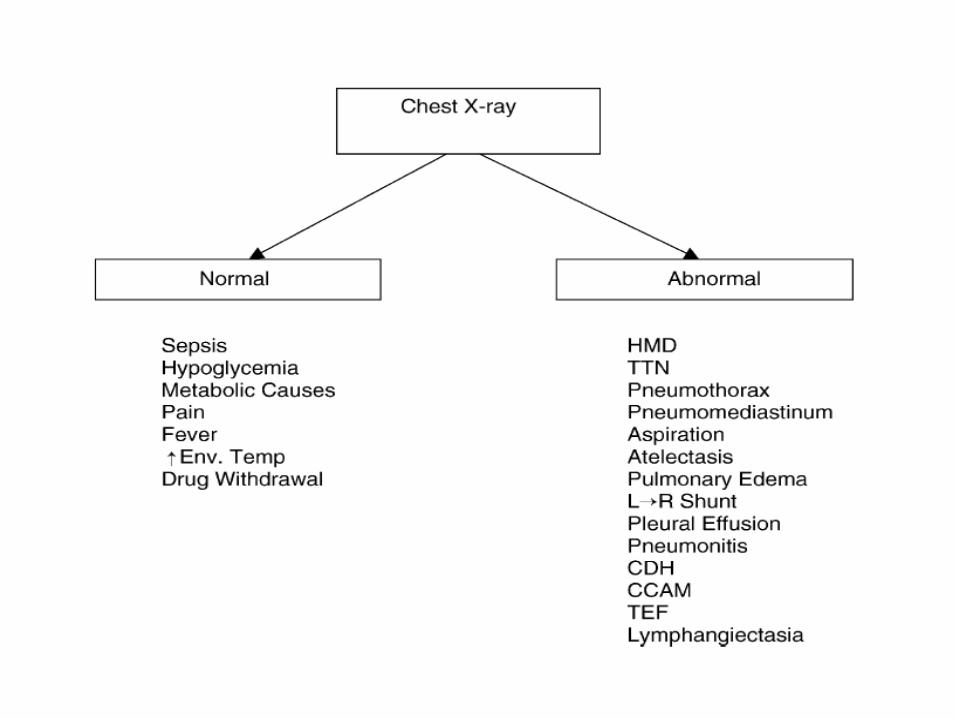
Chest xray
• Situs – locate stomach , liver, heart
• Cardiac position
• Chamber enlargement
• Arch sidedness
• Lung vasculature
• Lung parenchyma
• Bony cage and diaphragm
• Small heart- hypovolemia, adrenal insufficiency, pulmonary interstitial emphysema, congenital lobar emphysema.
• Egg-on-end - transposition of the great vessels
• Snowman sign – TAPVC
• Boot-shaped heart - tetralogy of Fallot.
• Severe cardiomegaly -Ebstein’s anomaly
• Moderate cardiomegaly - Infants of diabetic mothers (hyperinsulinemia), cardiomyopathy (caused by infections,metabolic disorders or asphyxia)
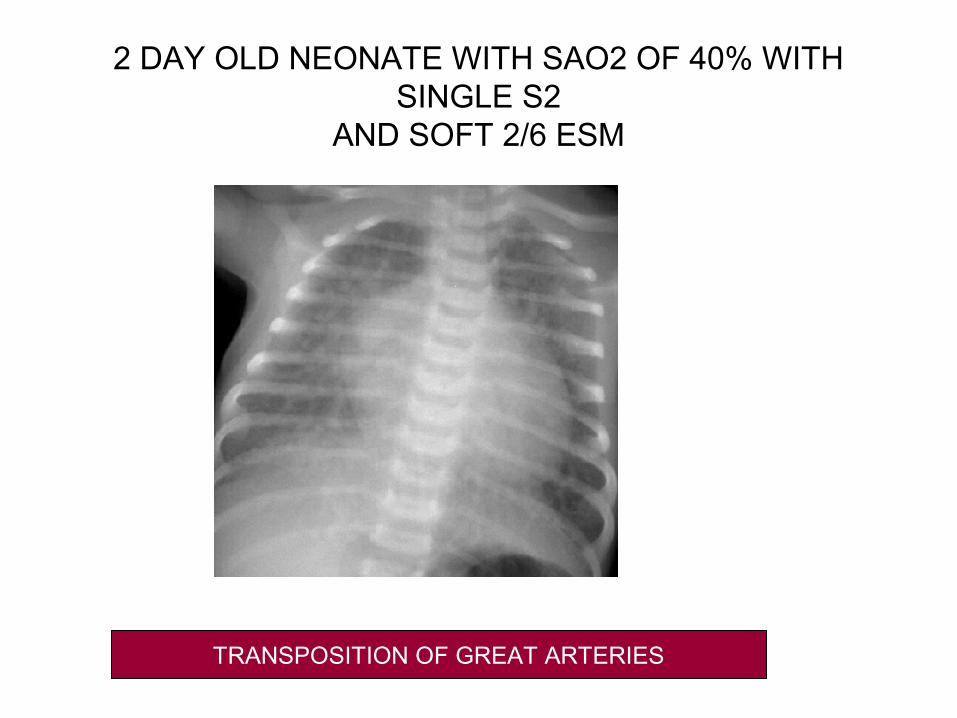
2 DAY OLD NEONATE WITH SAO2 OF 40% WITH SINGLE S2
AND SOFT 2/6 ESM
TRANSPOSITION OF GREAT ARTERIES
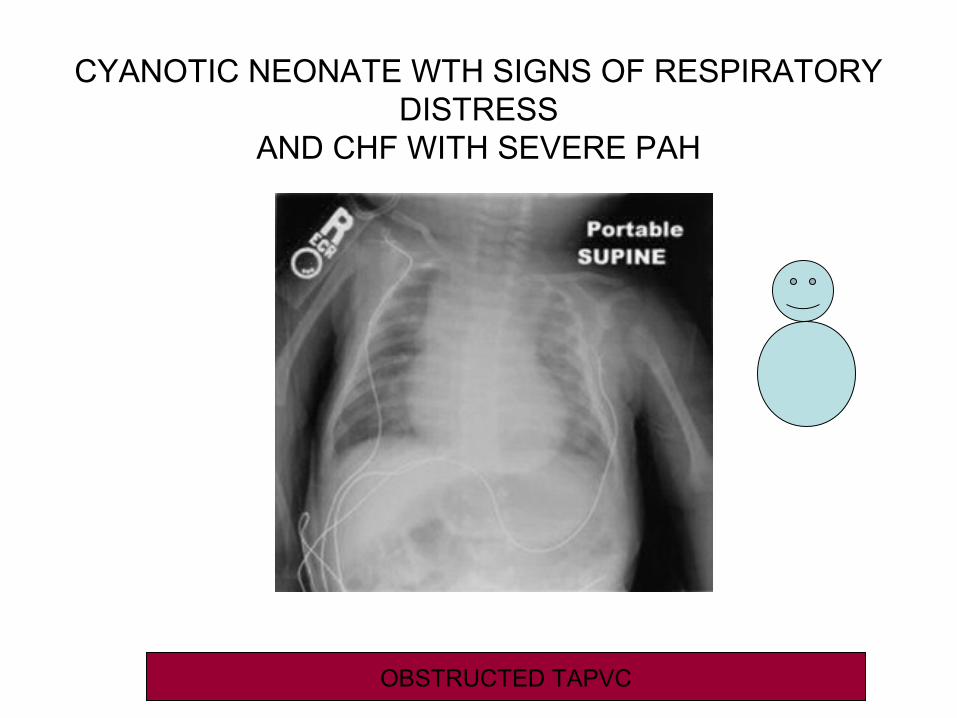
CYANOTIC NEONATE WTH SIGNS OF RESPIRATORY DISTRESS
AND CHF WITH SEVERE PAH
OBSTRUCTED TAPVC
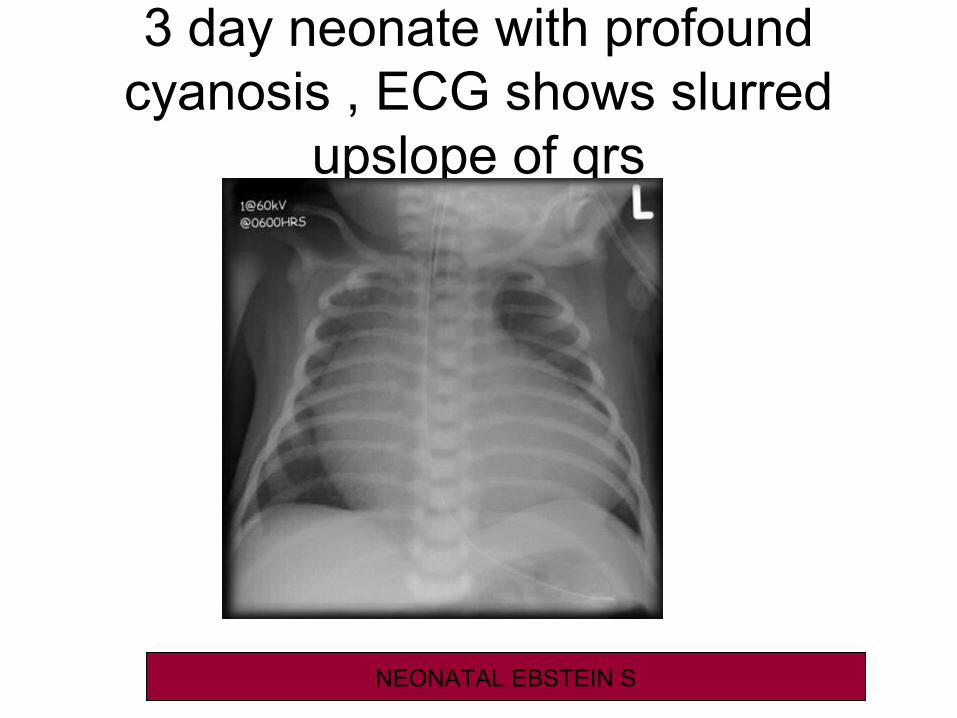
3 day neonate with profound cyanosis , ECG shows slurred
upslope of qrs
NEONATAL EBSTEIN S
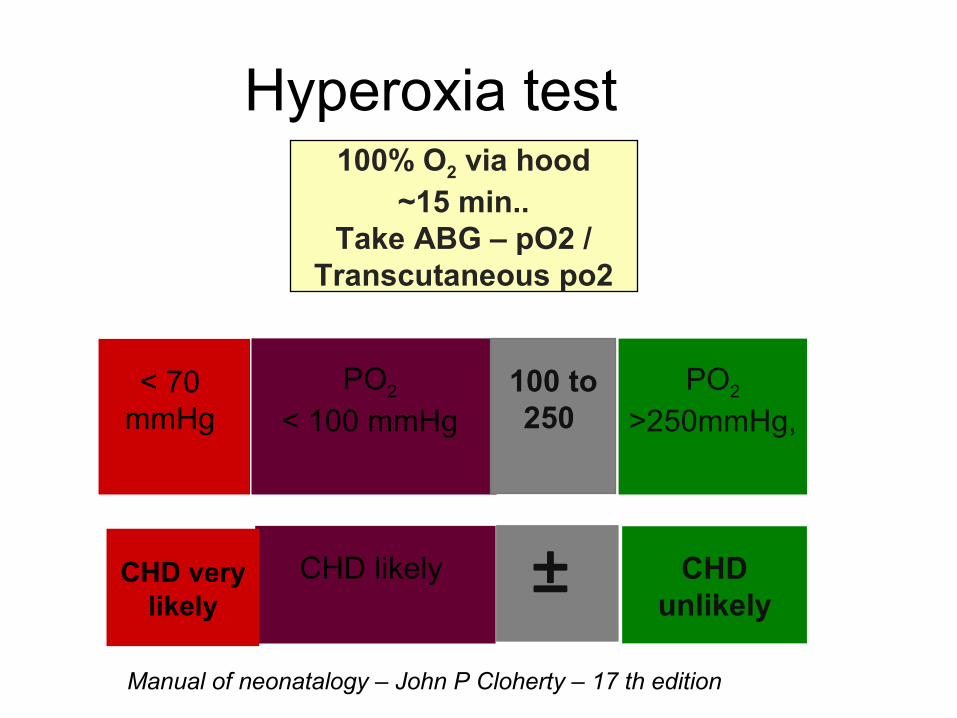
Hyperoxia test100% O2 via hood
~15 min..Take ABG – pO2 /
Transcutaneous po2
PO2 < 100 mmHg
CHD likely
PO2
>250mmHg,
CHDunlikely
100 to250
±
< 70 mmHg
CHD very likely
Manual of neonatalogy – John P Cloherty – 17 th edition
ECG
• Most conditions cause right axis deviation Most conditions cause right axis deviation with RVHwith RVH
• Cyanotic infant with left axis deviation and Cyanotic infant with left axis deviation and LVH: LVH:
1.Tricuspid atresia1.Tricuspid atresia
2 Pulmonary atresia with intact ventricular 2 Pulmonary atresia with intact ventricular septum.septum.
• ArrhythmiaArrhythmia
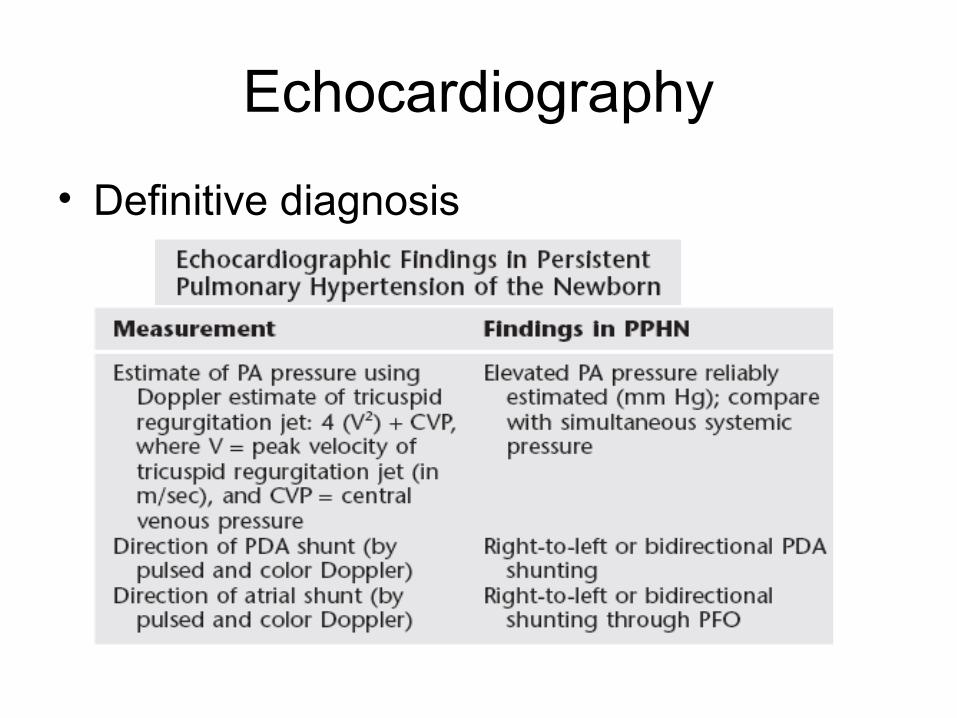
Echocardiography
• Definitive diagnosis
Management
• Thermo-neutral environmentThermo-neutral environment• Airway , breathing , circulationAirway , breathing , circulation• Correct hypovolemia, metabolic Correct hypovolemia, metabolic
derangements, treat sepsis.derangements, treat sepsis.• Particular care of IV lines and infusions – Particular care of IV lines and infusions –
avoid flushing of air bubbles into IV lines.avoid flushing of air bubbles into IV lines.• Feeding may be withheld in neonates with Feeding may be withheld in neonates with
duct dependent states if prostaglandin is duct dependent states if prostaglandin is anticipated.anticipated.
PGE 1
• Neonate failing hyperoxia test
• Shock within 1st 3 weeks of life
• Start at 0.05 µg/kg/mt – 0.1mcg/kg/mt
• Anticipate apnea
• Can worsen TAPVC
• Available as 500 μg vialAvailable as 500 μg vial
Manual of neonatalogy – John P Cloherty – 17 th edition
Oxygen TherapyOxygen Therapy
• Can be dangerous in certain statesCan be dangerous in certain states• Ductus dependent systemic lesions Ductus dependent systemic lesions • Pulmonary blood flow can increase at the Pulmonary blood flow can increase at the
cost of systemic blood flow(DDSC)cost of systemic blood flow(DDSC)• Tailor the FiO2, a Tailor the FiO2, a SaO2 of 80-85% may SaO2 of 80-85% may
be adequate to balance systemic and be adequate to balance systemic and pulmonary circulationspulmonary circulations
• Cyanosis not associated with acidosis Cyanosis not associated with acidosis need not be correctedneed not be corrected
Manual of neonatalogy – John P Cloherty – 17 th edition
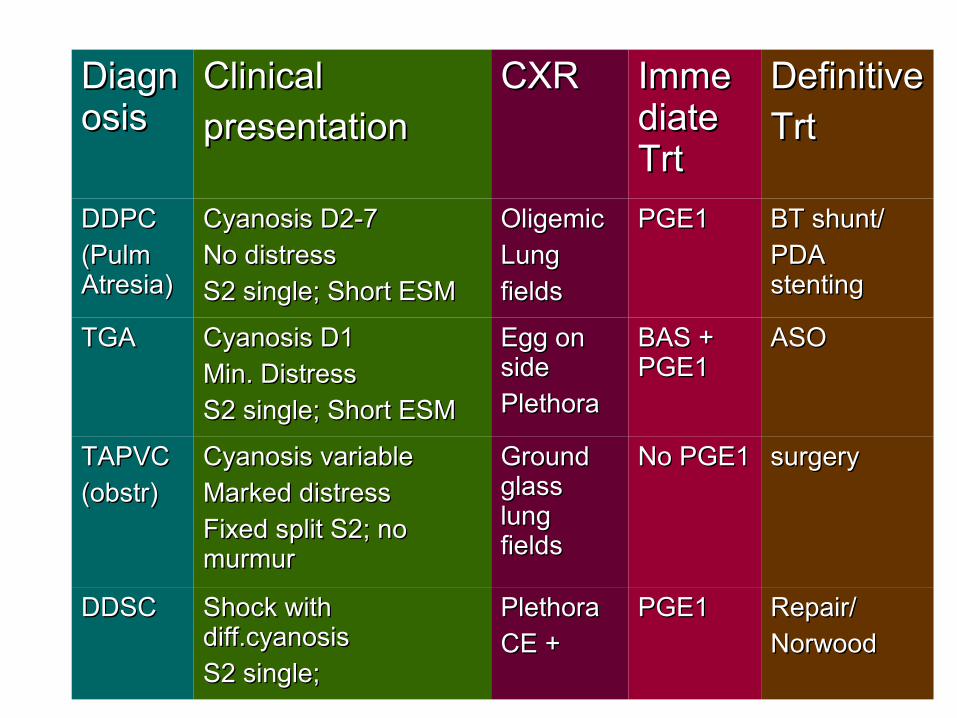
DiagnDiagnosisosis
ClinicalClinical
presentationpresentationCXRCXR ImmeImme
diate diate TrtTrt
DefinitiveDefinitive
TrtTrt
DDPCDDPC
(Pulm (Pulm Atresia)Atresia)
Cyanosis D2-7Cyanosis D2-7
No distressNo distress
S2 single; Short ESMS2 single; Short ESM
OligemicOligemic
Lung Lung
fieldsfields
PGE1PGE1 BT shunt/BT shunt/
PDA PDA stentingstenting
TGATGA Cyanosis D1Cyanosis D1
Min. Distress Min. Distress
S2 single; Short ESMS2 single; Short ESM
Egg on Egg on sideside
Plethora Plethora
BAS + BAS + PGE1PGE1
ASOASO
TAPVCTAPVC
(obstr)(obstr)Cyanosis variableCyanosis variable
Marked distressMarked distress
Fixed split S2; no Fixed split S2; no murmurmurmur
Ground Ground glass glass lung lung fieldsfields
No PGE1No PGE1 surgerysurgery
DDSCDDSC Shock with Shock with diff.cyanosisdiff.cyanosis
S2 single; S2 single;
PlethoraPlethora
CE +CE +PGE1PGE1 Repair/Repair/
NorwoodNorwood
Strategies to manage PPHN
• Avoid hyperoxemia (spo2 90 – 98)• HFV• iNO• ECMO• Sedation• Hemodynamic support• Correct acidosis ,polycythemia• Drugs – sildenafil, mag sulph , adenosine,CCB, tolazoline, prostacycline,inhaled ethyl
nitriteManual of neonatalogy – John P Cloherty – 17 th edition
Met hemoglobinemia
• Iron molecule in hemoglobin- normally in the ferrous state (Fe2.
• The ferric (Fe3+) form combines with water producing methemoglobin (MetHb).
• The predominant intracellular mechanism for the reduction of MetHb is cytochrome 5b.
• MetHb may be increased in the red cell owing to exposure to toxic substances or to absence of reductive pathways
Nelson textbook of pediatrics – 19 th edition

Treatment
• Methylene blue given IV (1-2 mg/kg initially) is used to treat toxic methemoglobinemia.
• An oral dose can be administered (100-300 mg PO per day) as maintenance therapy.
Nelson textbook of pediatrics – 19 th edition
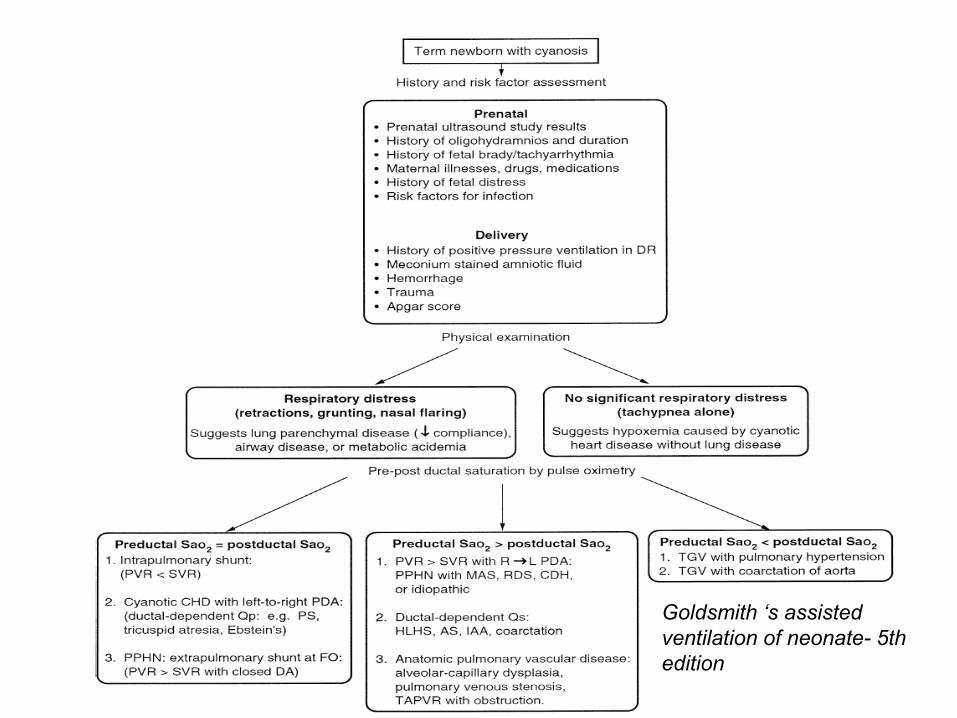
Goldsmith ‘s assisted ventilation of neonate- 5th edition

Goldsmith ‘s assisted ventilation of neonate- 5th edition
• Thank You



























![Winchester Uke Jam Songbook Vol 2 iPad · PDF fileWinchester Uke Jam Songbook Volume 2 ... Well It`s a blue blue, blue suede shoes baby, blue blue, blue suede shoes baby, [F] Blue](https://img.pdfslide.us/doc/110x75/5ab688e97f8b9a156d8de025/winchester-uke-jam-songbook-vol-2-ipad-uke-jam-songbook-volume-2-well-its-a.jpg)