Embed Size (px)
Citation preview

1
General wound care
1.Cleaning &debridement
2.Antimicrobial Agents
3. Biologicaldressings
4. Biosynthetic &Synthetic dressing
5.Excision & grafting

2
Excision and Grafting

33
Excision & Grafting the burn woundExcision & Grafting the burn wound
Full thickness or extensive burn-spontaneous Full thickness or extensive burn-spontaneous reepithelialization is not possible.reepithelialization is not possible.
Skin transplant or a graft of the patient`s own Skin transplant or a graft of the patient`s own skin (autograft) is required.skin (autograft) is required.
Main area for grafting-face for cosmetic and Main area for grafting-face for cosmetic and psychologic reasons, and joint, for movementpsychologic reasons, and joint, for movement
If the burn is extensive, chest and abdomen is If the burn is extensive, chest and abdomen is grafted to reduce surface area.grafted to reduce surface area.

44
Excision & Grafting the burn woundExcision & Grafting the burn wound
During the procedure of excision and During the procedure of excision and grafting, eschar is removed.grafting, eschar is removed.
A graft is placed on clean, viable tissue.A graft is placed on clean, viable tissue.
With early excision, function is restore and With early excision, function is restore and scar tissue formation is minimized.scar tissue formation is minimized.
Extensive bleeding may be expected.Extensive bleeding may be expected.
Burn wound can be cover by patient`s skin Burn wound can be cover by patient`s skin (autograft) (autograft)

55
Cultured epithelial autograftsCultured epithelial autografts
Pt with large body surface area burns, Pt with large body surface area burns, limited unburned skin available as a donor limited unburned skin available as a donor site for grafting.site for grafting.
Cultured epithelial autograft (CEA) is one Cultured epithelial autograft (CEA) is one method to obtain skin tissue from a person method to obtain skin tissue from a person with limited available skin for harvesting.with limited available skin for harvesting.
CEA is grown for biopsies obtained from CEA is grown for biopsies obtained from the patient`s own skin.the patient`s own skin.

66
Cultured epithelial autograftsCultured epithelial autografts
Taking one or two small (2 to 3 cm long by Taking one or two small (2 to 3 cm long by 1cm wide) biopsy specimens from 1cm wide) biopsy specimens from unburned skin.( usually the groin or axilla)unburned skin.( usually the groin or axilla)Performed as soon as possible when the Performed as soon as possible when the pt has been identified.pt has been identified.Specimen is sent to lab.Specimen is sent to lab.Skin specimen are cultivated in the Skin specimen are cultivated in the culture medium that contain epidermal culture medium that contain epidermal growth factor.growth factor.

77
Cultured epithelial autograftsCultured epithelial autografts
18 – 25 days cultivated keratinocytes expand 18 – 25 days cultivated keratinocytes expand up to 10,000 and form a sheet that can be used up to 10,000 and form a sheet that can be used as skin graft.as skin graft.
The cultured skin placed on the patient`s The cultured skin placed on the patient`s excised burn wounds.excised burn wounds.
CEA grafts are only epidermal cells, good care CEA grafts are only epidermal cells, good care is required to prevent injury or infection.is required to prevent injury or infection.

88
Cultured epithelial autograftsCultured epithelial autografts
CEA grafts generate permanent skin coverage CEA grafts generate permanent skin coverage because they generate from pt`s own cells.because they generate from pt`s own cells.
This type of skin graft has played an important role in This type of skin graft has played an important role in the survival of the pt with major burns with limited the survival of the pt with major burns with limited skin for donor harvesting.skin for donor harvesting.
Problems related to CEA include thin, friable skin Problems related to CEA include thin, friable skin (lack of dermal cells) and contracture development.(lack of dermal cells) and contracture development.

99
Wound closureWound closure Skin grafting is usually required or preferred with Skin grafting is usually required or preferred with
full-thickness or deep partial thickness.full-thickness or deep partial thickness.
After eshar removed and development of a base of After eshar removed and development of a base of granulating tissue, graft`s of patient`s own skin granulating tissue, graft`s of patient`s own skin (autograft) are applied.(autograft) are applied.
Blood flow is established by 3Blood flow is established by 3rd rd or or 4 4thth , and by 7 , and by 7thth and 10and 10thth day postgrafting, vascularity continuity and day postgrafting, vascularity continuity and wound closure have been established.wound closure have been established.

1010
TransCyteTransCyte The most recent temporary skin substitute.The most recent temporary skin substitute.
This bioengineered substance is derived form This bioengineered substance is derived form human fibroblast cells grown within mesh.human fibroblast cells grown within mesh.
This product is also a bilayer skin substitute This product is also a bilayer skin substitute
The outer epidermal analog is a thin nonporous The outer epidermal analog is a thin nonporous silicone film with barrier functions comparable to silicone film with barrier functions comparable to skin. skin.

1111
TransCyteTransCyte The inner dermal analog is layered with neonatal The inner dermal analog is layered with neonatal
fibroblasts which produce products mainly collagen type fibroblasts which produce products mainly collagen type I, fibronectin and glycosaminoglycans.I, fibronectin and glycosaminoglycans.
Cryo-preservation destroys the fibroblasts but preserves Cryo-preservation destroys the fibroblasts but preserves the activity of fibroblast.-the activity of fibroblast.-
These products do stimulate the wound healing process. These products do stimulate the wound healing process. A thin water layer is maintained at the wound surface for A thin water layer is maintained at the wound surface for
epidermal cell migration.epidermal cell migration.

12
TransCyte
• The nylon mesh provides flexibility and excellent adherence properties.
• The product is peeled off after the wound has re-epithelialized.
• TransCyte must be stored at –70 C° in order to preserve the bioactivity of the dermal matrix products.
• TransCyte is also indicated for the temporary closure of the excised wound prior to grafting.

13
TransCyte
Advantages• Bilayer analog • Excellent adherence to a superficial to
mid-dermal burn • Decreases pain • Provides bioactive dermal components • Maintains flexibility • Good outer barrier function

14
TransCyteDisadvantages
• Need to store frozen till use
• Relatively expensive

15
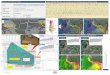
The two-layer structure, the inner layer being bioactive

16
TransCyte in Sealed Cassette
Stored at -70°Centigrade

17
TransCyte for Partial Thickness Hand
Burn
Cutting the sheet to fit with a small overlap followed by initial immobilization until adherent

18
TransCyte on Foot Burn (3 days)
Note flexibility of the dressing

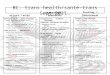
19
TransCyte on Leg Burn (10 days)
Opaque appearance indicating re-epithelialization beneath dressing for removal

20
TransCyte (Day 12)
Skin substitute being removed

21
Escharotomy
• Full thickness deep dermal burns which are nearly circumferential on the limbs, neck, thorax.
• Act like tourniquets with the development of edema.
• All extremity burns at risk should be monitored with at least hourly vascular checks of pulse or Doppler signal.
• Escharotomies are longitudinal or crisscross incisions through such deep burns.
• Done without analgesia and on the ward.• Does not bleed much.

22
Escharotomy

23
General wound care
1.Cleaning &debridement
2.Antimicrobial Agents
3. Biologicaldressings
4. Biosynthetic &Synthetic dressing
5.Excision & grafting

24
ACUTE PHASE
Other medicationNutrition
Relievinganxiety
WoundCleansing anddebridement

2525
RehabilitationRehabilitationPHASEPHASE

26
Physical & Occupational therapy
• Rigorous physical therapy with the physical therapist
• To maintain optimal joint function.• A good time for exercise is during and after
hydrotherapy • Skin is softer and bulky dressings are removed.• The patient with neck burns should sleep without
pillows • Head hanging slightly over the top of the
mattress to encourage hyperextension

27
Positioning
• During this phase, patient must be maintained in positions that prevent contractures.
• Contracture= abnormal flexion and fixition of a join cause by muscle atrophy and shortening
• Minimizes formation of edema. • Prevents tissue destruction, and maintains soft
tissues to facilitate recovery. • Patients should be positioned in a direction of
comfort, especially around joints and flexor surfaces.

2828
PositioningPositioning
Extremities should be elevated above the Extremities should be elevated above the level of the heart using pillows, blankets, level of the heart using pillows, blankets, and towels. and towels.
Lower extremities should be elevated Lower extremities should be elevated when the patient is sitting. when the patient is sitting.
Patients who do not have endotracheal Patients who do not have endotracheal tubes or central lines may be placed prone tubes or central lines may be placed prone to avoid pressure to posterior areasto avoid pressure to posterior areas

2929
Position and splintingPosition and splinting
Turned from side to side to prevent the Turned from side to side to prevent the development of sacral pressure sores and development of sacral pressure sores and to minimize discomfort from pressure on to minimize discomfort from pressure on burns to these areas. burns to these areas. Burns to the upper extremities or hands Burns to the upper extremities or hands should be evaluated by an occupational should be evaluated by an occupational therapist.therapist.Splints immobilize body parts and prevent Splints immobilize body parts and prevent contracture of the joint.contracture of the joint.

3030
ExercisesExercises
Physical therapists work in conjunction with Physical therapists work in conjunction with occupational therapists.occupational therapists.
Assessment by the physical therapist to assist Assessment by the physical therapist to assist with ambulation, range of motion exercises with ambulation, range of motion exercises necessary splintsnecessary splints
Exercises are begun early, active and passive.Exercises are begun early, active and passive.
Range of motion (R0M), performed every 2 Range of motion (R0M), performed every 2 hours at bedside.hours at bedside.
Early ambulationEarly ambulation

31

32

3333
Pressure garment.Pressure garment.
• Fitting of pressure garment, can prevent or reduce hyperthropic scarring.
• Customade elastic pressure garments for 6 months and 1 year postgraft.
• The psychologist plays an integral part in facilitating the psychological recovery of burn patients, and should be consulted for every patient admitted to the burn unit.

34
SPLINT




![CartemotoneigeSagLac2014-15 [Unlocked by ] sentier lac st-jean.pdf · 6.6 trans-quÉbec 83 trans-quÉbec 93 trans-quÉbec 93 trans-quÉbec 93 trans-quÉbec 93 trans-quÉbec 93 trans-quÉbec](https://img.pdfslide.us/doc/110x75/5b2cb5eb7f8b9ac06e8b5a01/cartemotoneigesaglac2014-15-unlocked-by-sentier-lac-st-jeanpdf-66-trans-quebec.jpg)