Embed Size (px)
Citation preview
Major Rail Occurrence
ForumSydney – 28-29 April 2015
Tony SimesManager - Rail
ATSB
Rail Accident Investigations –The ATSB Approach
• Accident Investigations
– Aviation
– Marine
– Rail
• Research
– Aviation / Marine / Rail
Australian Transport Safety Bureau (ATSB)
• ATSB Rail Investigators
– Perth
– Adelaide
– Canberra
• Agreements with
– OTSI (Sydney)
– CITS (Melbourne)
• ATSB Rail jurisdiction
– NSW
– Vic
– SA
– NT
– Tas
– WA (DIRN)
– QLD (DIRN)
• Punitive (breaches of law)
– Criminal / Civil
– Regulatory (in some cases)
• Just Cause (recognises that errors occur)
– Coronial (mostly)
– Internal organisation (preferably)
• No Blame
– ATSB
Investigation Types
• Not only ‘What’ happened, but ‘Why’
– Why did it occur
– Why did people behave the way they did
– Why did the environment/system allow it
• What factors and issues contributed to the accident
• How can the system be made more error tolerant
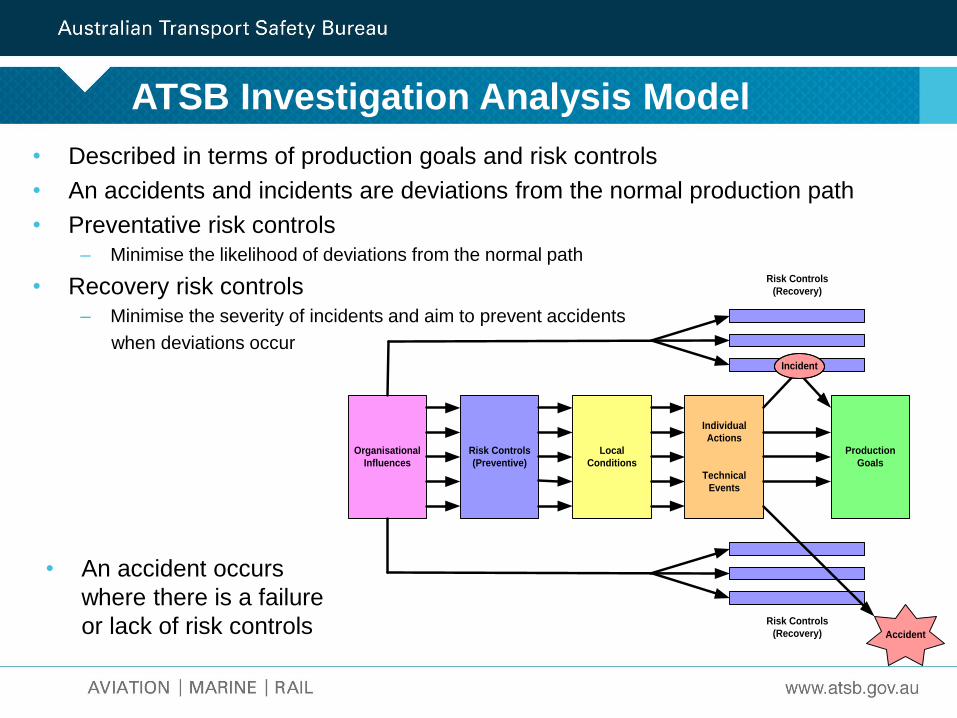
ATSB Investigation Analysis Model
Risk Controls
(Recovery)
Risk Controls
(Recovery)
Risk Controls
(Preventive)
Local
Conditions
Individual
Actions
Technical
Events
Production
Goals
Accident
Organisational
Influences
Incident
• Described in terms of production goals and risk controls
• An accidents and incidents are deviations from the normal production path
• Preventative risk controls– Minimise the likelihood of deviations from the normal path
• Recovery risk controls– Minimise the severity of incidents and aim to prevent accidents
when deviations occur
• An accident occurs
where there is a failure
or lack of risk controls
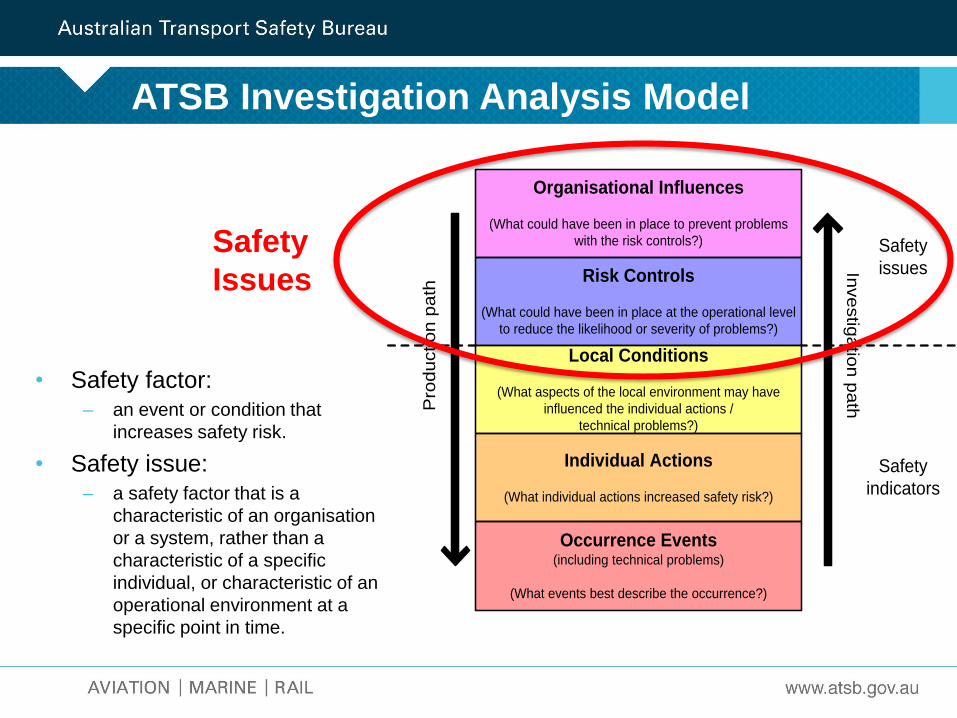
ATSB Investigation Analysis Model
• Safety factor:– an event or condition that
increases safety risk.
• Safety issue:– a safety factor that is a
characteristic of an organisation
or a system, rather than a
characteristic of a specific
individual, or characteristic of an
operational environment at a
specific point in time.
Organisational Influences
(What could have been in place to prevent problems
with the risk controls?)
Risk Controls
(What could have been in place at the operational level
to reduce the likelihood or severity of problems?)
Local Conditions
(What aspects of the local environment may have
influenced the individual actions /
technical problems?)
Individual Actions
(What individual actions increased safety risk?)
Pro
du
ctio
n p
ath
Safety
issues
Safety
indicators
Inve
stig
atio
n p
ath
Occurrence Events(including technical problems)
(What events best describe the occurrence?)
Safety
Issues
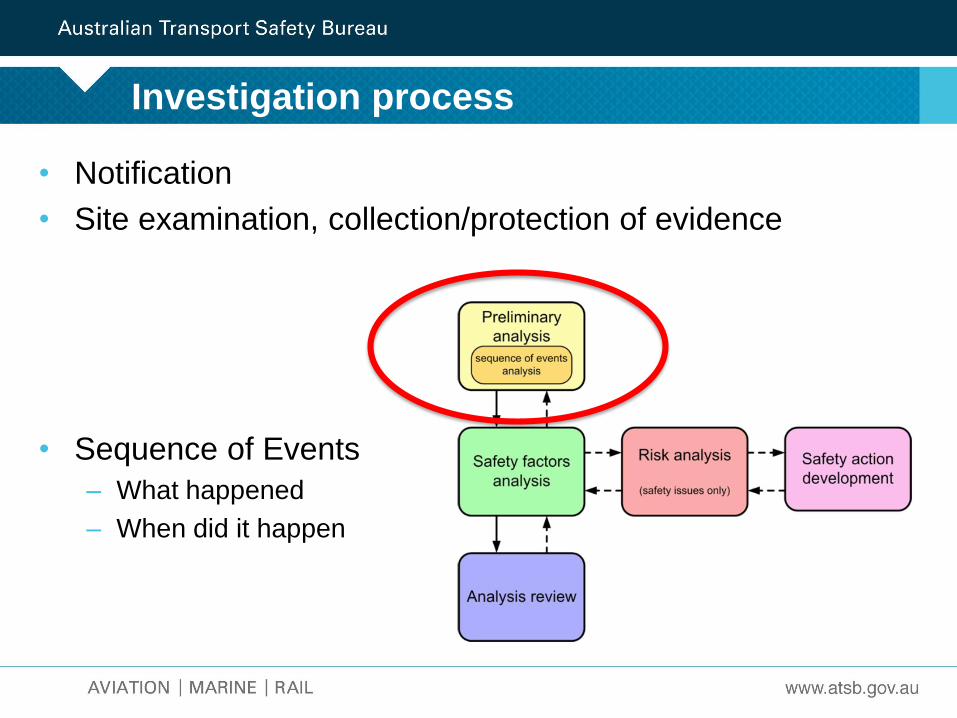
• Notification
• Site examination, collection/protection of evidence
• Sequence of Events
– What happened
– When did it happen
Investigation process
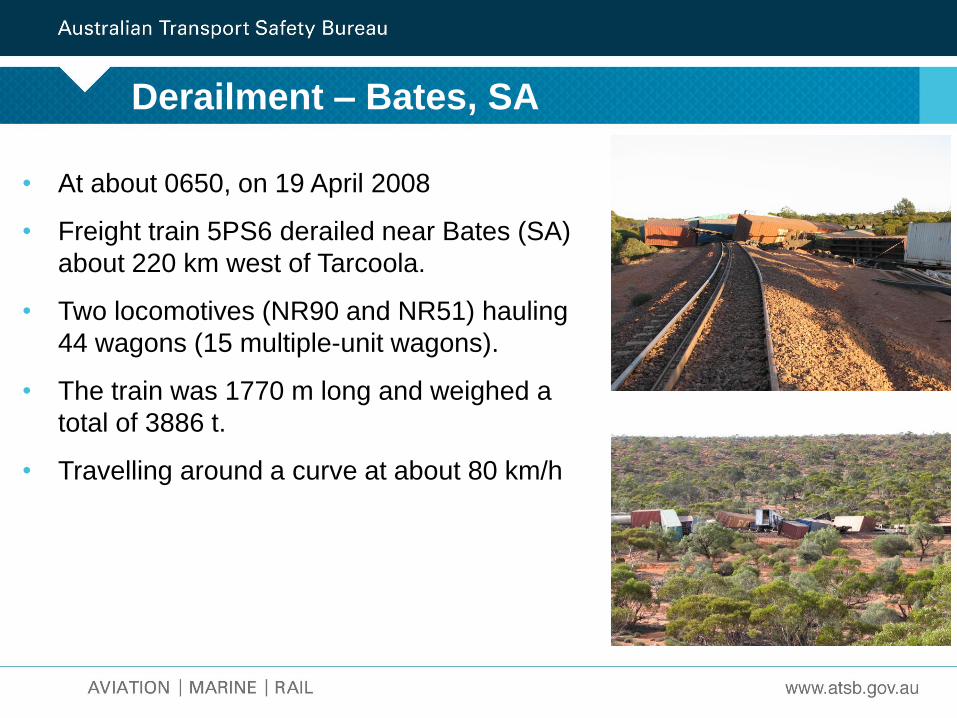
Derailment – Bates, SA
• At about 0650, on 19 April 2008
• Freight train 5PS6 derailed near Bates (SA)
about 220 km west of Tarcoola.
• Two locomotives (NR90 and NR51) hauling
44 wagons (15 multiple-unit wagons).
• The train was 1770 m long and weighed a
total of 3886 t.
• Travelling around a curve at about 80 km/h
• Locomotive drivers recalled hearing ‘crack, crack, crack’
• The driver eased off the throttle before noticing a
reduction of brake pipe pressure
• Train brakes automatically applied and 5PS6 came to a
stop
• Train had derailed and a significant portion of track had
been destroyed
• Dangerous goods (resin solution and various chemicals)
• Exclusion zone around the derailment site until an
appropriate assessment could be conducted by
hazardous materials assessors.
Sequence
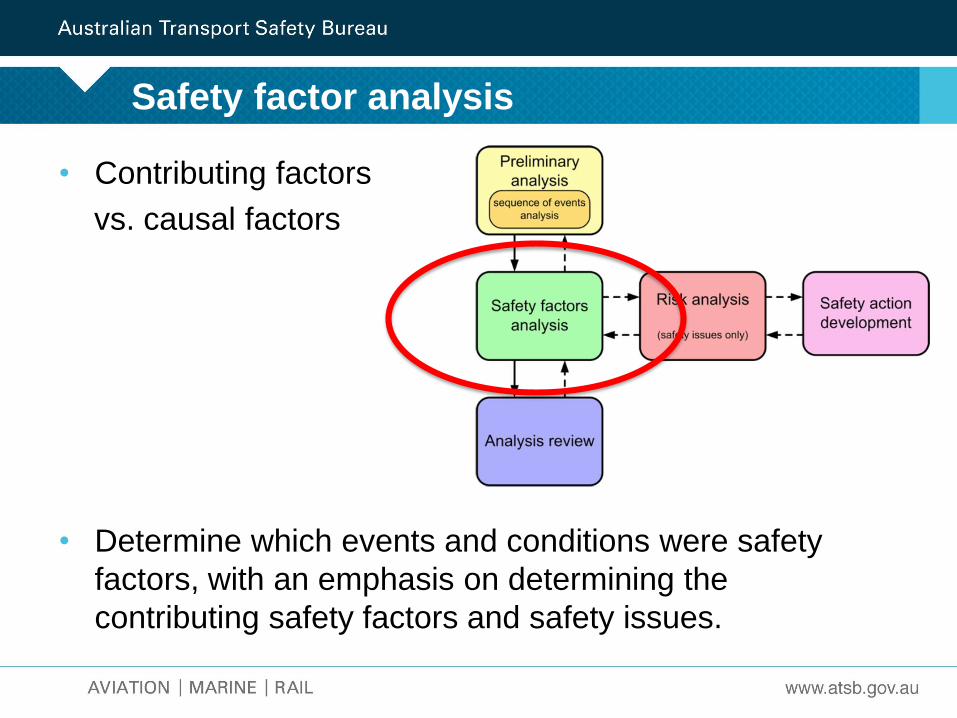
• Contributing factors
vs. causal factors
• Determine which events and conditions were safety
factors, with an emphasis on determining the
contributing safety factors and safety issues.
Safety factor analysis
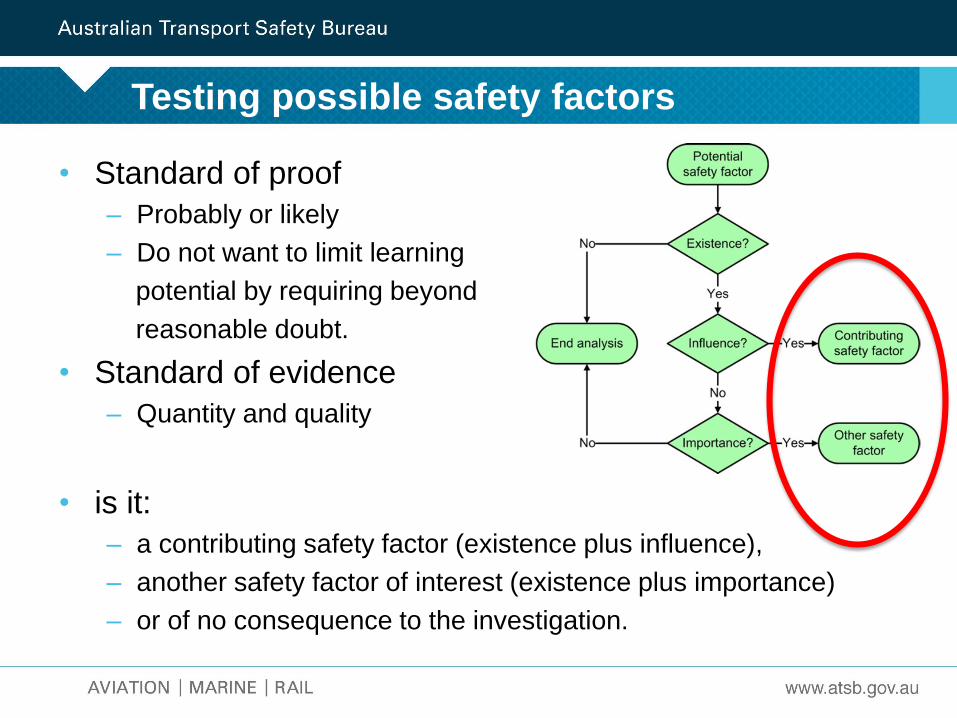
• Standard of proof
– Probably or likely
– Do not want to limit learning
potential by requiring beyond
reasonable doubt.
• Standard of evidence
– Quantity and quality
• is it:
– a contributing safety factor (existence plus influence),
– another safety factor of interest (existence plus importance)
– or of no consequence to the investigation.
Testing possible safety factors
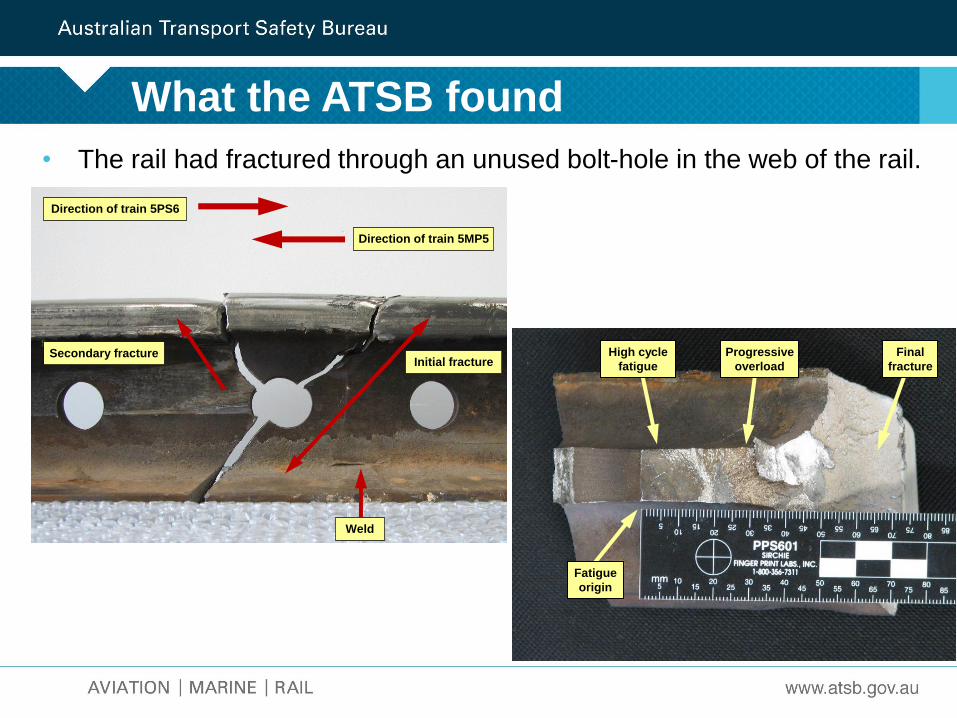
What the ATSB found
• The rail had fractured through an unused bolt-hole in the web of the rail.
High cycle
fatigue
Progressive
overload
Final
fracture
Fatigue
origin
Initial fractureSecondary fracture
Direction of train 5PS6
Direction of train 5MP5
Weld
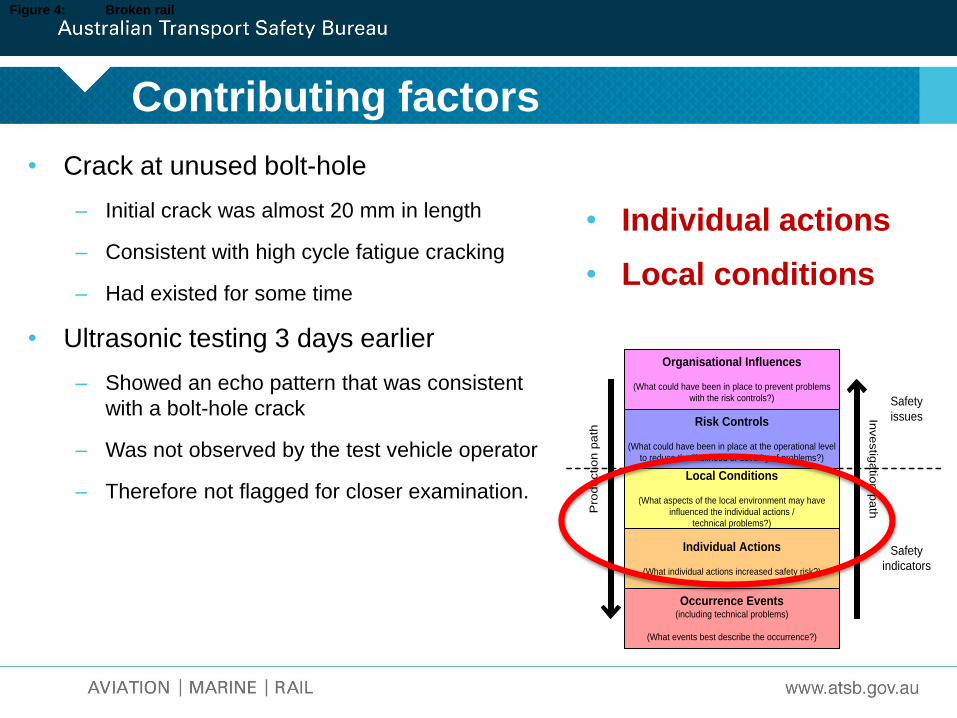
Contributing factors
• Crack at unused bolt-hole
– Initial crack was almost 20 mm in length
– Consistent with high cycle fatigue cracking
– Had existed for some time
• Ultrasonic testing 3 days earlier
– Showed an echo pattern that was consistent
with a bolt-hole crack
– Was not observed by the test vehicle operator
– Therefore not flagged for closer examination.
Figure 4: Broken rail
• Individual actions
• Local conditions
Organisational Influences
(What could have been in place to prevent problems
with the risk controls?)
Risk Controls
(What could have been in place at the operational level
to reduce the likelihood or severity of problems?)
Local Conditions
(What aspects of the local environment may have
influenced the individual actions /
technical problems?)
Individual Actions
(What individual actions increased safety risk?)
Pro
du
ctio
n p
ath
Safety
issues
Safety
indicators
Inve
stig
atio
n p
ath
Occurrence Events(including technical problems)
(What events best describe the occurrence?)
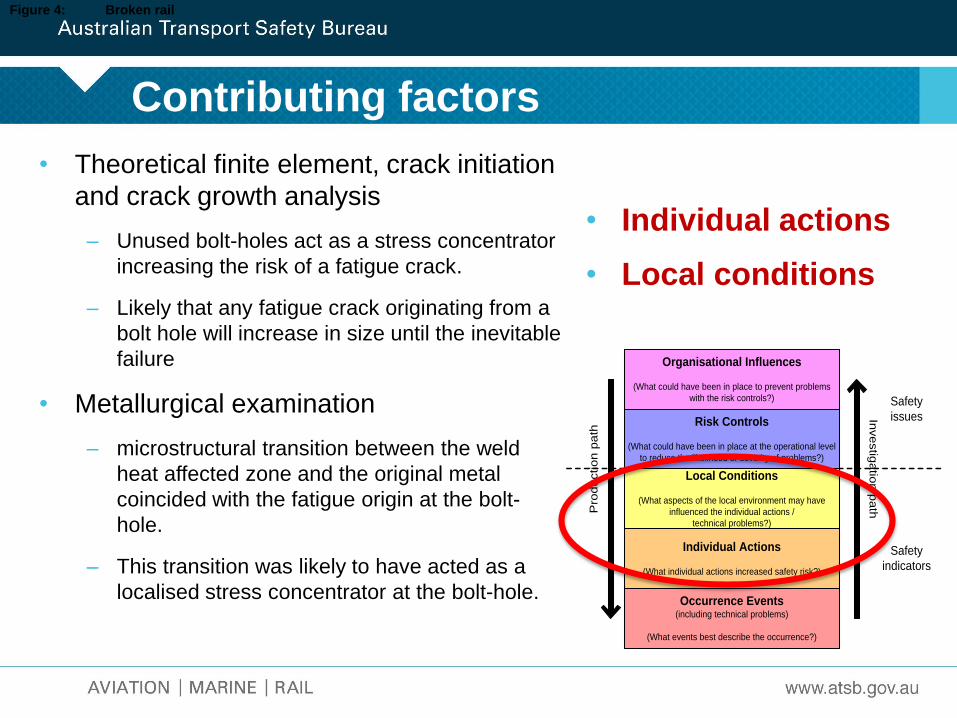
Contributing factors
• Theoretical finite element, crack initiation
and crack growth analysis
– Unused bolt-holes act as a stress concentrator
increasing the risk of a fatigue crack.
– Likely that any fatigue crack originating from a
bolt hole will increase in size until the inevitable
failure
• Metallurgical examination
– microstructural transition between the weld
heat affected zone and the original metal
coincided with the fatigue origin at the bolt-
hole.
– This transition was likely to have acted as a
localised stress concentrator at the bolt-hole.
Figure 4: Broken rail
• Individual actions
• Local conditions
Organisational Influences
(What could have been in place to prevent problems
with the risk controls?)
Risk Controls
(What could have been in place at the operational level
to reduce the likelihood or severity of problems?)
Local Conditions
(What aspects of the local environment may have
influenced the individual actions /
technical problems?)
Individual Actions
(What individual actions increased safety risk?)
Pro
du
ctio
n p
ath
Safety
issues
Safety
indicators
Inve
stig
atio
n p
ath
Occurrence Events(including technical problems)
(What events best describe the occurrence?)
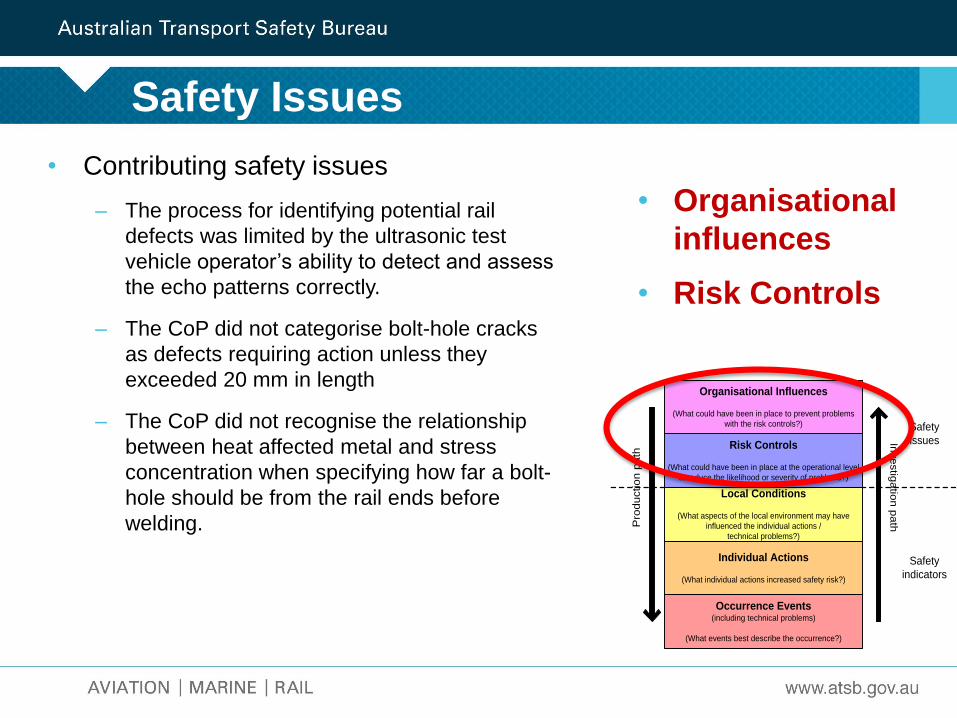
Safety Issues
• Contributing safety issues
– The process for identifying potential rail
defects was limited by the ultrasonic test
vehicle operator’s ability to detect and assess
the echo patterns correctly.
– The CoP did not categorise bolt-hole cracks
as defects requiring action unless they
exceeded 20 mm in length
– The CoP did not recognise the relationship
between heat affected metal and stress
concentration when specifying how far a bolt-
hole should be from the rail ends before
welding.
• Organisational
influences
• Risk Controls
Organisational Influences
(What could have been in place to prevent problems
with the risk controls?)
Risk Controls
(What could have been in place at the operational level
to reduce the likelihood or severity of problems?)
Local Conditions
(What aspects of the local environment may have
influenced the individual actions /
technical problems?)
Individual Actions
(What individual actions increased safety risk?)
Pro
du
ctio
n p
ath
Safety
issues
Safety
indicators
Inve
stig
atio
n p
ath
Occurrence Events(including technical problems)
(What events best describe the occurrence?)
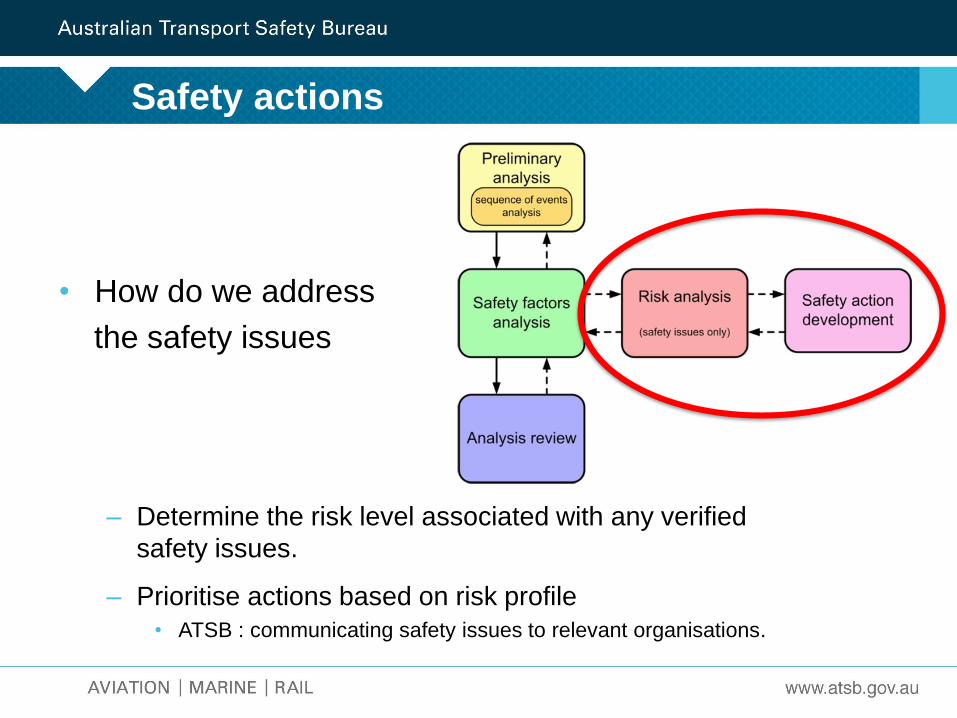
• How do we address
the safety issues
– Determine the risk level associated with any verified
safety issues.
– Prioritise actions based on risk profile
• ATSB : communicating safety issues to relevant organisations.
Safety actions
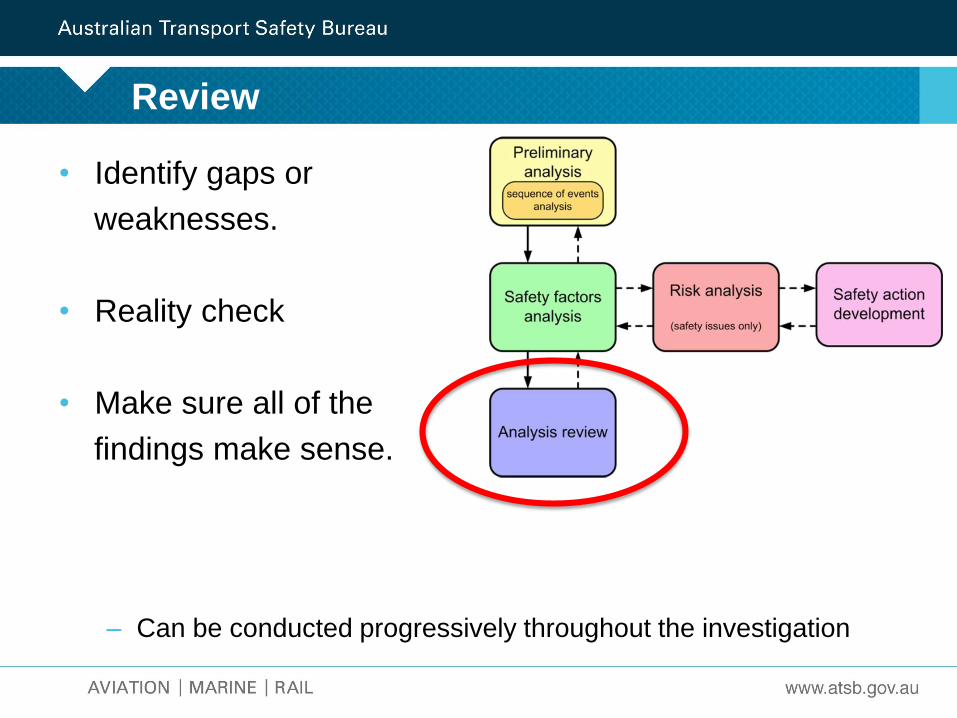
• Identify gaps or
weaknesses.
• Reality check
• Make sure all of the
findings make sense.
– Can be conducted progressively throughout the investigation
Review
What has been done
• Review of standards
– all bolt-hole cracks are recorded as defects and require removal,
irrespective of the crack size.
• Further development of the ultrasonic testing process
– Reduce reliance on the operator to recognise defects
• software solution to identify ultrasonic reflection patterns
– Re-analysis of data to identify defects that
may have been missed
Conclusion
• Identify ‘What’ happened, but also ask the
question ‘Why’ did it happen.
– Why did people behaved the way they did
– Why did the environment allow it to occur
• Adopt a framework designed to encourage
quality analysis techniques
• What factors contributed to the incident
• Aim is to enhance safety, not to apportion
blame or liability.
• Look for:
– Organisational influences
– Risk control measures
Thankyou





























