Embed Size (px)
DESCRIPTION
STRATEGIC AND BUSINESS ANALYSIS OF THE WESTERN CAPE DEPARTMENT OF HEALTH AND THE STRATEGIC PARTNERSHIPS FUNCTION IN CONTEXT OF THE HEALTHCARE SECTOR IN SOUTH AFRICA AN ANALYSIS OF THE POTENTIAL COMPETITIVE ADVANTAGES AND STRATEGIC IMPERATIVES AND DIRECTIONS REQUIRED TO ACHIEVE THE STRATEGIC OBJECTIVES OF THE WESTERN CAPE GOVERNMENT AND SPECIFICALLY OF THE Western Cape DEPARTMENT OF HEALTH HEALTH, WELLNESS and SOCIAL DEVELOPMENT AS DRIVERS OF ECONOMIC GROWTH, DEVELOPMENT, POVERTY ALLEVIATION AND REDUCTION OF INEQUALITY PARTNERSHIPS, COLLABORATION, CO-CREATION, CO-PRODUCTION: CREATING AN ENABLING ENVIRONMENT TOWARDS ACHIEVING NATIONAL, PROVINCIAL, LOCAL AND SOCIETAL STRATEGIC OBJECTIVES AND OUTCOMES WITHIN RESTRICTED BUDGETARY ENVIRONMENT
Citation preview
ASSIGNMENT COVER PAGE
SURNAME: Brinkmann
INITIALS: A
STUDENT NUMBER: 17573602
TELEPHONE NUMBER: 0828900663
PROGRAMME NAME: EDP 2012
MODULE: Strategic Management
FACILITATOR: Prof Westwood
DUE DATE: 8 October 2012
17 excluding references, Appendices and Attachment
NUMBER OF PAGES:
CERTIFICATION
I certify the content of the assignment to be my own and original work and that all sources have been accurately reported and acknowledged, and that this document has not previously been submitted in its entirety or in part at any educational establishment.
_________________________
SIGNATURE
OR
6701130018085
_________________________
ID number for assignments submitted via e-mail
FOR OFFICE USE
DATE RECEIVED:
2
REPORT AND RECOMMENDATIONS
PREPARED FOR CONSIDERATION BY THE EXECUTIVE MANAGEMENT COMMITTEE: Western Cape
DEPARTMENT OF HEALTH
[WCDOH]
8 OCTOBER 2012
STRATEGIC AND BUSINESS ANALYSIS OF THE WESTERN CAPE DEPARTMENT OF HEALTH AND THE
STRATEGIC PARTNERSHIPS FUNCTION IN CONTEXT OF THE HEALTHCARE SECTOR IN SOUTH AFRICA
AN ANALYSIS OF THE POTENTIAL COMPETITIVE ADVANTAGES AND STRATEGIC IMPERATIVES AND
DIRECTIONS REQUIRED TO ACHIEVE THE STRATEGIC OBJECTIVES OF THE WESTERN CAPE GOVERNMENT
AND SPECIFICALLY OF THE Western Cape DEPARTMENT OF HEALTH
HEALTH, WELLNESS and SOCIAL DEVELOPMENT AS DRIVERS OF ECONOMIC GROWTH, DEVELOPMENT,
POVERTY ALLEVIATION AND REDUCTION OF INEQUALITY
PARTNERSHIPS, COLLABORATION, CO-CREATION, CO-PRODUCTION: CREATING AN ENABLING ENVIRONMENT
TOWARDS ACHIEVING NATIONAL, PROVINCIAL, LOCAL AND SOCIETAL STRATEGIC OBJECTIVES AND
OUTCOMES WITHIN RESTRICTED BUDGETARY ENVIRONMENT
PREPARED BY:
AMANDA BRINKMANN
ADVISER TO THE MINISTER OF HEALTH: WESTERN CAPE GOVERNMENT
HEAD OF STRATEGIC PARTNERSHIPS: WESTERN CAPE GOVERNMENT
3
TABLE OF CONTENTS
1. WESTERN CAPE GOVERNMENT: STRATEGIC OBJECTIVES
1.1 ACHIEVING THE WELLNESS OBJECTIVE
1.1.1 DEFININING WELLNESS AND HEALTH
1.1.2 THE SOCIAL DETERMINANTS OF HEALTH AND WELLNESS IN CONTEXT OF POVERTY
ALLEVIATION, ECONOMIC DEVELOPMENT AND GROWTH OUTCOMES
1.1.3 THE COST TO GOVERNMENT AND SOCIETY OF CONTINUING WITH A „ BUSINESS-AS-USUAL‟
APPROACH
1.1.4 PROVINCIAL TRANSVERSAL MANAGEMENT SYSTEM [ PTMS]
2. WCDOH VISION 2020 – PARTNERING AND PARTNERSHIP AS A STRATEGIC PRIORITY
3. WCDOH: CONSTRAINTS – RATIONALISING THE NEED FOR INNOVATION AND PARTNERSHIPS
4. STRATEGIC PARTNERSHIPS: WESTERN CAPE GOVERNMENT: A vision of an ideal future of
health and wellness: 2020 and beyond
5. SPACE MODEL MATRIX ANALYSIS: WESTERN CAPE DEPARTMENT OF HEALTH AND STRATEGIC
PARTNERSHIPS
5.1 CONTEXT
5.2 ENVIRONMENTAL STABILITY
5.2.1 RATIONALISING THE RATINGS
5.3 INDUSTRY ATTRACTIVENESS
5.3.1 RATIONALISING THE RATINGS
5.4 COMPETITIVE ATTRACTIVENESS
5.4.1 RATIONALISING THE RATINGS
5.5 FINANCIAL STRENGTH
5.5.1 RATIONALISING THE RATING
5.6 THE OUTCOME – WHERE IT ALL COMES TOGETHER – CONCLUSIONS AND
RECOMMENDATIONS
6. CONCLUSION
7. REFERENCES
4
1. WESTERN CAPE GOVERNMENT: STRATEGIC OBJECTIVES
The Western Cape Provincial Government has developed a Provincial Strategic Plan with eleven
provincial strategic objectives in order to effectively pursue the vision of creating an „open
opportunity society for all‟. [WCDOH. March 2012]
The provincial strategic objectives are closely aligned with the national outcomes particularly in
relation to concurrent functions such as health.
The provincial strategic objectives are:
1) Creating opportunities for growth and jobs
2) Improving education outcomes
3) Increasing access to safe and efficient transport
4) Increasing wellness
5) Increasing safety
6) Developing integrated and sustainable human settlements
7) Mainstreaming sustainability and optimising resource use efficiency
8) Promoting social inclusion and reducing poverty [SO8 and 9 are being combined)
Increasing social cohesion [SO8]
Poverty reduction and alleviation [SO9]
9) Integrating service delivery for maximum impact
10) Increasing opportunities for growth and development in rural areas
11) Building the best-run provincial government in the world.
The Western Cape Department of Health is responsible for the implementation and stewardship of
Strategic Objective 4: Increasing Wellness
1.1 ACHIEVING THE WELLNESS OBJECTIVE
1.1.1 DEFININING WELLNESS AND HEALTH
Dictionary.com [Accessed September 2012] defines health as follows:
• The general condition of the body or mind with reference to soundness and vigour: good
health; poor health.
• Soundness of body or mind; freedom from disease or ailment: to have one's health; to lose
one's health.
• Vigour; vitality: economic health.
Earthzense.com [Accessed September 2012] defines and described wellness as follows:
Wellness is a term that has become extremely popular in recent years, so much so that the
definition of wellness has also rendered different meanings to different people. Most define
wellness as simply “being physically well” most of the time.
All inclusive, the generally accepted definition of wellness is:
To stay in good condition physically, mentally, and spiritually, especially through healthy choices in
those areas – a balance in all of these areas indicates wellness in an individual. This definition of
wellness seems to imply that wellness is a lifestyle choice.
And it defines wellness to include not just being healthy physically, but embraces a holistic concept
of health that encompasses our whole being - body, mind and spirit. Wellness is a natural human
condition that has become negatively conditioned throughout the passages of time by the lifestyle
choices we make.
5
1.1.2 THE SOCIAL DETERMINANTS OF HEALTH AND WELLNESS IN CONTEXT OF POVERTY ALLEVIATION,
ECONOMIC DEVELOPMENT AND GROWTH OUTCOMES
In its Burden of Disease Study [Myers, Naledi, et al.2007] the Western Cape Department of Health
[WCDOH] identified the upstream, socio-cultural factors that impact downstream health outcomes.
The upstream risk factors touch on issues of development, such as: inequity, poverty, low income
and unemployment, homelessness, social inclusion, and justice. These determinants fall outside of
the direct ambit and control of the WCDOH‟s primary mandate.
The findings of this report are further supported by the Rio Declaration on the Social Determinants of
health [World Health Organisation. 21 October 2011], which was in turn an outflow of the World
Health Organisation [ WHO] Conference on the Social Determinants of Health, which was held in
Brazil in 2011. The Rio Declaration reached the following agreements:
Social and health equity can be achieved through action on the social determinants of
health and well-being. This should be attainable via a comprehensive, inter-sectoral
approach.
It was agreed that health equity is a shared responsibility that requires engagement of all
sectors of government, all sectors of society and all members of the international
community in an „ all for equity‟ and „health for all‟ global action.
Three overarching recommendations were adopted: * to tackle the inequitable distribution
of power, money and resources; * to improve daily living conditions * to measure and
understand the problem and assess the impact of action.
In the WHO report titled, Macroeconomics and Health: Investing in Health for Economic
Development [Sachs, J, D. 20 December 2001] it is further confirmed that health is a developmental
outcome.
“Whilst it is accepted that health is a developmental outcome, the opposite view that health can
be a driving force for development and economic upliftment has not been fully recognised. The
Commission on Macroeconomics and Health asserts that, if upstream risk factors were controlled in
conjunction with improved health services to address the downstream risk factors,
… impoverished families could not only enjoy lives that are longer, healthier, and more productive,
but they would also choose to have fewer children, secure in the knowledge that their children
would survive, and could thereby invest more in the education and health of each child…the
improvements in health would translate into higher incomes, higher economic growth, and
reduced population growth [Sachs, 2001].”
To address the burden of disease, one needs to understand that determinants of health
encompass both downstream biological and behavioural risk factors, and upstream societal and
structural risk factors.
The importance of the MDGs in health is, in one sense, self-evident. Improving the health and
longevity of the poor is an end in itself, a fundamental goal of economic development. But it is also
a means to achieving the other development goals relating to poverty reduction. The linkages of
health to poverty reduction and to long-term economic growth are powerful, much stronger than is
generally understood.
1.1.3 THE COST TO GOVERNMENT AND SOCIETY OF CONTINUING WITH A „ BUSINESS-AS-USUAL‟
APPROACH
The Western Cape Government is essentially caught in the proverbial „Catch 22‟ situation, where it
is compelled to spend the majority of the available budget on things that are entirely preventable.
The list is nearly never-ending: * Crime * School drop-out * Substance and alcohol abuse *
Teenaged pregnancies * Welfare * HIV/AIDS * Burden of Disease * Unemployment * Inter-personal
violence * Collective Depression – and so the list continues. Governing is effectively reactive.
6
Government resources are stretched to the limit to fulfil its mandate of dealing with the
consequences of societal decay and the resultant un-wellness of its citizens. The cycle of
government spending can be likened to constantly putting Band-Aids on gaping wounds. In some
instances, 90% of available budget and resources are spent on the things that could be prevented,
if only systemic, future-focused interventions were implemented in partnership with the whole-of-
society.
The private sector, philanthropic and global donors have been funding a plethora of NGO‟s and
programmes and yet, outcomes are, at the very least moderate. This can be ascribed to the fact
that there is no strategic model that seeks to address the systemic causes of the cycle of poverty,
despair and hopelessness that continues to perpetuate itself in a ubiquitous cycle of behavioural
and socialisation repetition. Government, funders, NGO‟s and researchers are all working in
isolation of one another, rather than to collaborate and partner to amplify outcomes. Such
collaboration would more than likely lead to duplications in funding and programmes being
eradicated as well as to improve overall outcomes, whilst using fewer resources.
By imaging that by putting more resources into health and education any of the developmental
outcomes will change, we are fooling ourselves and doing nothing more than to assuage our
conscience that we are at least doing SOMETHING.
The answer to creating societal wellness, breaking the cycle of poverty and all of the
consequences that are ultimately dealt with mainly by departments of Health and society as a
whole, lies in an implementation model that seeks to disrupt the circumstances that children are
born into as well as the socialisation process that nearly pre-determines their future by virtue of
these circumstances. Just on 16 million patient contacts at Primary Health Care sites in the Western
Cape alone, provides an indication of the un-wellness of our citizens. Add to that the fact that
estimates put undiagnosed mental illness, such as depression as high as 17% and one starts
understanding that a great many patients that are presenting at state facility may indeed be
somatising. If they were correctly diagnosed and treated, but moreover, if the cycle of depression
and despair were interrupted at an early and systemic stage, the savings to the health care system
and society would be immense.
The Strategic Partnerships Portfolio within the Western Cape Government was given the freedom to
define the scope and boundaries of its work and to find transversal solutions to societal challenges.
In the course of the 3 year process of working across all three spheres of government, with civil
society, the private sector, academia, research institutions, philanthropic donors and the citizens of
the country and province, the writer has developed and piloted a model and methodology called:
A PASSPORT TO WELLNESS© A roadmap out of poverty, towards growth and development
[Brinkmann, A. February 2010 onwards]. [Appended]
This model disrupts and intervenes within the socialization process to move from current future to
ideal future in a practical and pragmatic manner. This strategy has been adopted by the Western
Cape Government, has support from civil society and donors and will, over time, have the effect of
freeing up capacity within health facilities, release funds spent on all of the issues that are
preventable, so that in five, ten and fifteen years from now, government and society are able to
spend more of their resources on growth and development outcomes.
1.1.4 PROVINCIAL TRANSVERSAL MANAGEMENT SYSTEM [ PTMS]
The PTMS provides a structured opportunity to mobilise role players outside of health to address
these upstream determinants of health and wellness. The Provincial Transversal Management
System is a priority of the Western Cape Government, providing political support for effective inter-
sectoral collaboration within the provincial government.
This is informed by the philosophy that acting in a united manner around a common set of
objectives as a “whole of society” and a “whole of government” will promote delivery. This further
evidenced and demonstrated within the PASSPORT TO WELLNESS model [Brinkmann, A. February
2010 onwards].
7
The strategic objectives are clustered into three sectors i.e. human development, economic and
infrastructure, and administration and inter-governmental. Each of the strategic objectives has a
steering group to co-ordinate the working groups within the strategic objective.
2 WCDOH VISION 2020 – PARTNERING AND PARTNERSHIP AS A STRATEGIC PRIORITY
In November 2011, WCDOH released its Vision 2020 – The Future of Health care in the Western
Cape: A Draft Framework for Dialogue [WCDOH. November 2011]
“Seven guiding principles have been identified to guide the 2020 strategy:
1. Patient-centred quality of care
2. A move towards an outcomes-based approach
3. The retention of a Primary Health Care philosophy
4. Strengthening the District Health Services model
5. Equity
6. Affordability
7. Building Strategic Partnerships “
The document deals very expressly with what should be done differently and what the case for
change is. Some of the compelling motivations for change include: * changes in the provincial
demography * socio-economic determinants of health and the burden of disease * advances in
technology * global, national and provincial environments * extreme tightening of the fiscal
envelope, necessitating innovation and different ways of doing things * sustaining existing good
practice and improving on others * cost effective interventions within limited resources * prevention
of disease and promotion of wellness.
Building Strategic Partnerships
It is essential that the provincial government seeks out and builds creative partnerships with role-
players in the private sector, civil society, higher education, labour movement, other spheres of
government and internationally. There is a realisation that improving the health status of the
population requires a whole-of-society approach and that the capacity and resources within the
private sector need to be engaged, given the disparity between what is spent versus the
population coverage in the public and private sectors.
The provincial Ministry of Health, via its Head of Strategic Partnerships has already started an
exciting engagement with the private sector, which has shown a willingness to invest in the public
sector. Commercial opportunities are being investigated that can be mutually beneficial. A public
– private health forum exists which provides a structured opportunity for engagement with the
private sector. The Health Foundation was also recently established by the private sector, on a
similar basis as the Red Cross Children‟s Trust, with the intent of assisting the Strategic Partnerships
Portfolio and WCDOH in achieving its objectives and outcomes via a range of partnerships and
collaborations.
A range of diverse partnerships have already been realised and the benefits and outcomes for all
parties involved have surpassed expectations. This provides a strong foundation upon which to
build. One of the key differentiators in respect of how the private sector and partners are engaged
is that it is done with business, economic growth and mutually beneficial outcomes in mind. The
Strategic Partnership Portfolio functions as though it is a private sector entity and has therefore
developed a common and understandable language between the public and private sector.
3 WCDOH: CONSTRAINTS – RATIONALISING THE NEED FOR INNOVATION AND PARTNERSHIPS
3.1 The Western Cape accounts for 10.4% of population or 5. 287 million citizens of which an
estimated 80%+ are served by the public health system.
3.2 In 2012/13, it is projected that 16 348 182 patient contacts will be managed at Primary Health
Care [PHC] level, 511 367 patients admitted to the department‟s hospitals, 135 018 patients
treated with anti-retroviral therapy, 487 781 patients transported in ambulances, 98 500 babies
8
delivered in the maternity services and 6 909 cataract operations performed [Western Cape
Department of Health. March 2012].
3.3 Both Gauteng and the Western Cape will continue to experience shifts in demography and
population distribution related to inward migration from the Eastern Cape and Limpopo – this
inward migration places additional stress and pressure on already over-burdened state
3.4 An asset/equipment backlog exists generally within the WCDOH, but specifically at the three [3]
Tertiary, Central Hospitals: Groote Schuur Hospital, Tygerberg Hospital and Red Cross Hospital.
3.5 Some, or all, of the facilities managed by the WCDOH have a shortage of equipment and/or
ageing or obsolete equipment that need to be upgraded or replaced.
3.6 There are real costs, financial and non-financial, associated with the lack of necessary
equipment in certain facilities.
3.7 The budget allocated by Treasury to the WCDOH is currently not sufficient to meet the annual
equipment demands of all facilities, and by inference, insufficient to reduce and/or eliminate
the existing backlog. [Botha, T. 26 March 2012]
3.8 There are significant maintenance and infrastructure backlogs, which despite the accelerated
infrastructure spend over the past 3 years, will not be dealt with within the constrained budget
as allocated by National Treasury.
3.9 Strategic Partnerships, efficiency, innovation, stretching the healthcare rand and patient-
centricity are all at the very heart of achieving the objectives of the WCDOH. [ Botha, T. 26
March 2012]
3.10 National Treasury has issued a notice indicating a tightening of the budgetary envelope.
The estimated time horizon is anticipated to be three to five years. [National Treasury
Department: South Africa. August 2012]
3.11 Notwithstanding the above, negative impact on service delivery is not an option as is
evidenced by the Strategic Objective Four of the WCDOH as set out within the Annual
Performance Plan 2012/13[Appendix F:Western Cape Department of Health. March 2012] as
well as with the spirit, content and objectives of Vision 2020 [WCDOH. November 2011]. This is
reiterated within the content of the WCDOH Budget Speech 2012 [Botha, T. 26 March 2012].
It is therefore vital, now, more than ever, to engage in mutually beneficial partnerships and
collaborations with a deep and broad range of role players so as to deliver on the objectives of the
WCDOH and society as a whole.
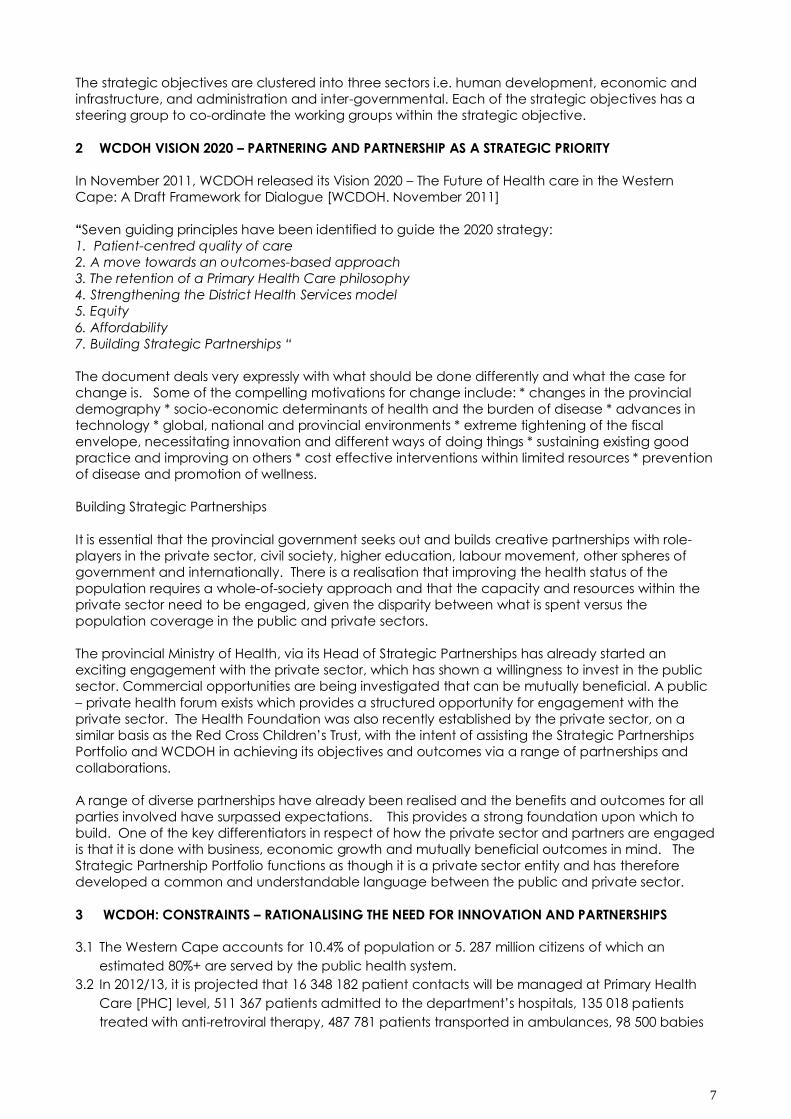
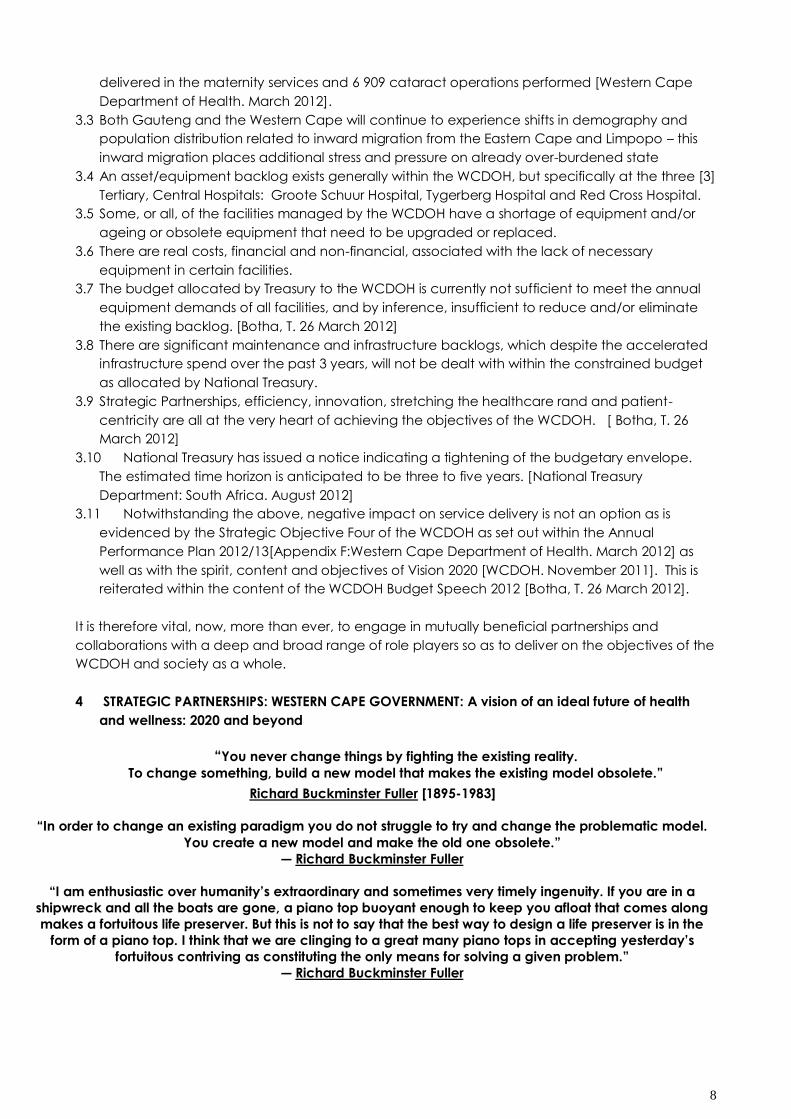
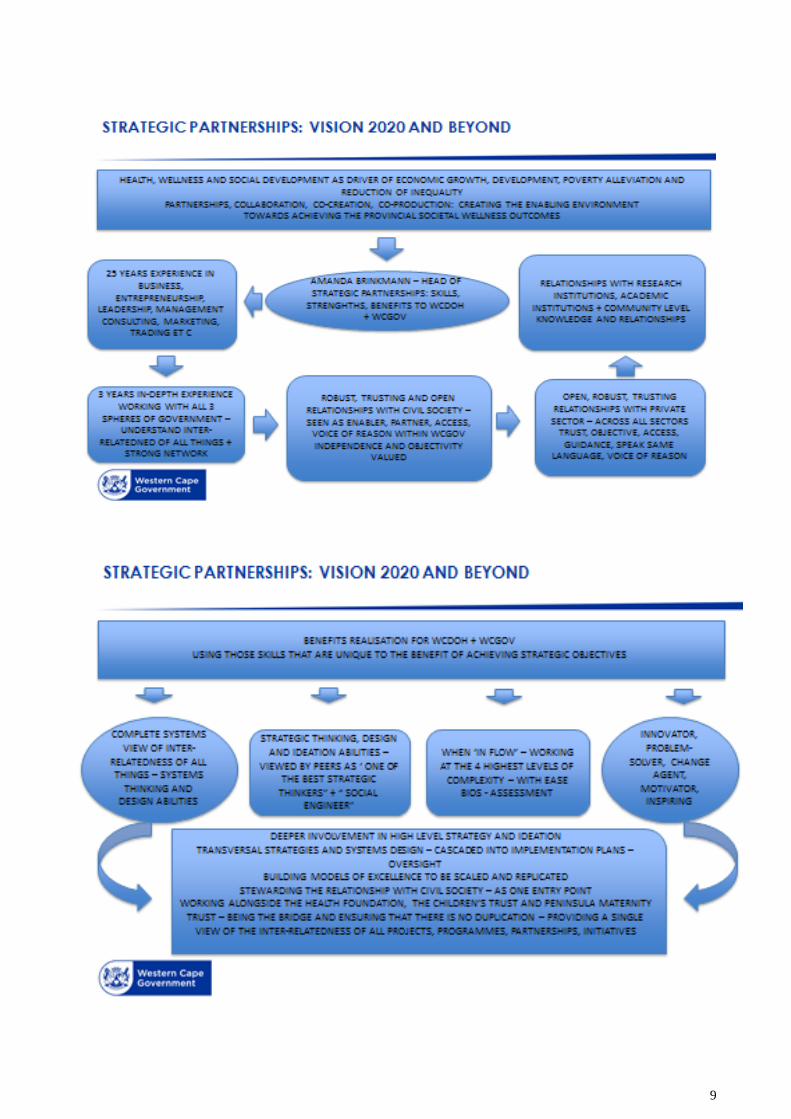
4 STRATEGIC PARTNERSHIPS: WESTERN CAPE GOVERNMENT: A vision of an ideal future of health
and wellness: 2020 and beyond
“You never change things by fighting the existing reality.
To change something, build a new model that makes the existing model obsolete.”
Richard Buckminster Fuller [1895-1983]
“In order to change an existing paradigm you do not struggle to try and change the problematic model.
You create a new model and make the old one obsolete.”
― Richard Buckminster Fuller
“I am enthusiastic over humanity‟s extraordinary and sometimes very timely ingenuity. If you are in a
shipwreck and all the boats are gone, a piano top buoyant enough to keep you afloat that comes along
makes a fortuitous life preserver. But this is not to say that the best way to design a life preserver is in the
form of a piano top. I think that we are clinging to a great many piano tops in accepting yesterday‟s
fortuitous contriving as constituting the only means for solving a given problem.”
― Richard Buckminster Fuller
9
10
5 SPACE MODEL MATRIX ANALYSIS: WESTERN CAPE DEPARTMENT OF HEALTH AND STRATEGIC
PARTNERSHIPS
5.1 CONTEXT
It is generally considered to be unusual to apply the Space Matrix analysis to a government entity.
In this case, I have taken up the challenge that was laid down, given that I have spent the majority
of my career in the private sector as an entrepreneur, in advertising, marketing, business consulting,
construction, forex trading, importing and exporting and management consulting. I was
specifically approached to give life, shape and form to the Strategic Partnership Portfolio because
of my commercial and entrepreneurial bent, my ability to work at the highest levels of complexity
with ease and to therefore understand the inter-relatedness and inter-connectedness of all things.
I also speak the language of business, whilst having a strong social bent and am motivated by a
strong sense of purpose and meaning to be part of the positive change in the world. The role and
work that I do is not about me, but rather about what I can contribute to the overall benefit of
society. In my opinion, there is always a way to ensure that benefits accrue to all parties involved –
such mutual benefits are found by structuring wants, needs, expectations, boundaries and
limitations up-front and being honest and forthright about what each party desires and what they
are prepared to contribute and/or concede to reach their objectives. Innovation, often moving
into the realm of blue-skying, lies at the core of imaging all that could be – without limitations or
restrictions. I am yet to encounter a challenge or problem for which there are not multiple possible
solutions. It is with this mind-set, years of evidence-based experience and a need to be the
change in this world, that I am tackling this analysis – essentially using a hybridised version of the
Space Matrix Modelling – so as to accommodate the unique idiosyncrasies of a portfolio that
ensure that I am not a government official, do not tow any party lines and no interest or objectives
other than to improve quality and access to services, quality of life, wealth, health and prosperity
for all involved. Bearing this brief background in mind, let us proceed to the unpacking of the
various elements of the Space Model Analysis:
11
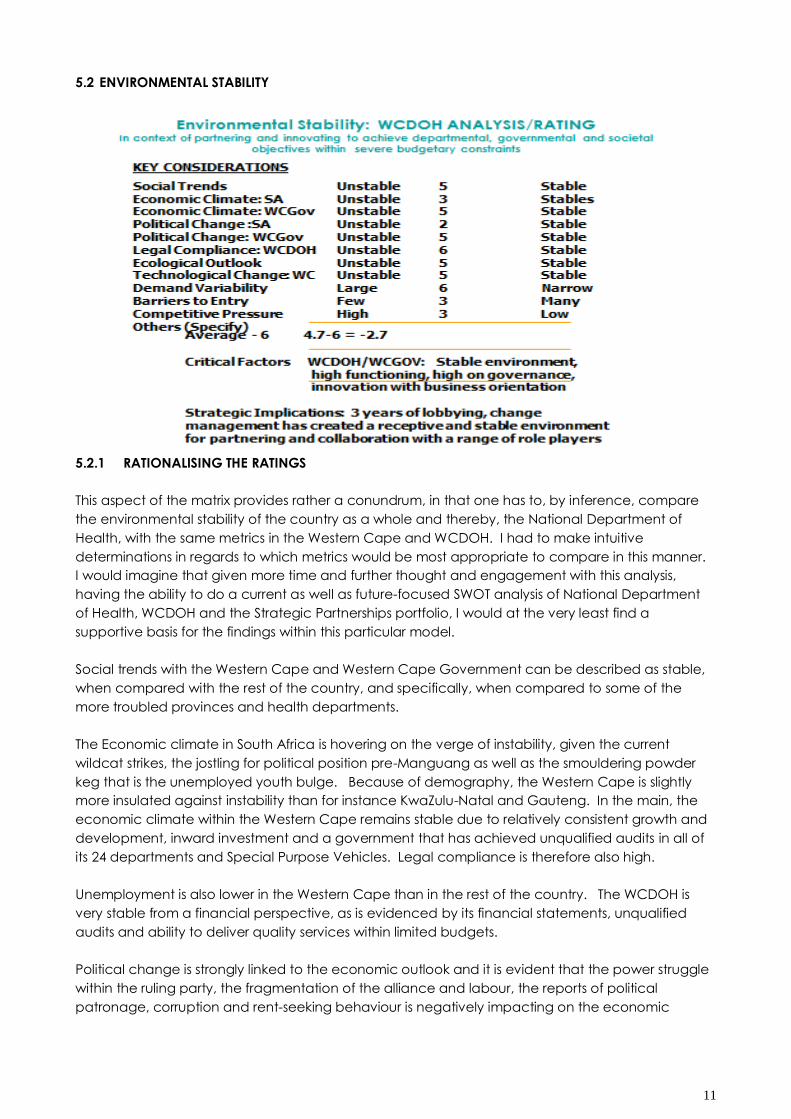
5.2 ENVIRONMENTAL STABILITY
5.2.1 RATIONALISING THE RATINGS
This aspect of the matrix provides rather a conundrum, in that one has to, by inference, compare
the environmental stability of the country as a whole and thereby, the National Department of
Health, with the same metrics in the Western Cape and WCDOH. I had to make intuitive
determinations in regards to which metrics would be most appropriate to compare in this manner.
I would imagine that given more time and further thought and engagement with this analysis,
having the ability to do a current as well as future-focused SWOT analysis of National Department
of Health, WCDOH and the Strategic Partnerships portfolio, I would at the very least find a
supportive basis for the findings within this particular model.
Social trends with the Western Cape and Western Cape Government can be described as stable,
when compared with the rest of the country, and specifically, when compared to some of the
more troubled provinces and health departments.
The Economic climate in South Africa is hovering on the verge of instability, given the current
wildcat strikes, the jostling for political position pre-Manguang as well as the smouldering powder
keg that is the unemployed youth bulge. Because of demography, the Western Cape is slightly
more insulated against instability than for instance KwaZulu-Natal and Gauteng. In the main, the
economic climate within the Western Cape remains stable due to relatively consistent growth and
development, inward investment and a government that has achieved unqualified audits in all of
its 24 departments and Special Purpose Vehicles. Legal compliance is therefore also high.
Unemployment is also lower in the Western Cape than in the rest of the country. The WCDOH is
very stable from a financial perspective, as is evidenced by its financial statements, unqualified
audits and ability to deliver quality services within limited budgets.
Political change is strongly linked to the economic outlook and it is evident that the power struggle
within the ruling party, the fragmentation of the alliance and labour, the reports of political
patronage, corruption and rent-seeking behaviour is negatively impacting on the economic
12
outlook and sentiment for South Africa. We have just recently seen a downgrading of by Standards
and Poors.
In contrast and in comparison, even when taking the alleged “Project Reclaim” that seeks to
destabilise the province into account, it would seem that the political landscape is, for now,
relatively stable with little chance of significant change on the cards.
The province has embarked on a phased project to ensure technological advances in the
knowledge economy, but specifically, in connectivity for all of its citizens over the next 5 years. The
government itself has had to deal with a legacy ICT system that was less than satisfactory and so a
comprehensive Microsoft migration is in process, thereby improving business efficiencies
significantly. Statistics show that there is a direct link between connectivity and technological
advances and growth in GDP and development.
On the metrics of demand variability, barriers to entry and competitive pressure, I have chosen to
focus on the unique value proposition that my portfolio, open door approach as well as access to
the Executive of the province, city and national government offers prospective partners. I do not
perceive rank or file, have built a supportive shadow network within the structures and together, we
are able to keep the end goal of societal benefit in mind so as to find new and innovative ways of
doing things. In fact, one of the maxims by which I work with all of my colleagues, is to remind
them that we are here to serve the people of this province, that it is by their grace and tax money
that we wake up every morning and have a purpose and that when we look at any piece of
legislation, regulation or policy, we must not only look at what is in front of us, if what is in front of us
seems to hamper the achievement of the desired outcomes. We must rather look at what we
should change, adapt or alter, in order to make such outcomes possible. Any barriers to entry are
dealt with by employing the „break it to fix it‟ and „find the ONE way in which this can happen‟
approach.
No other province seems to have established a portfolio with the scope, mandate and access that
the Strategic Partnerships portfolio has and in fact, there have been advances to assist in setting
similar structures up in other provinces, due to the perceived competitive advantage that this
conveys on WCDOH and the province as a whole.
It is important to note that the appointment is non-political, non-partisan and on a contractual
basis, meaning that no agendas other than the improvement of the lives of the people of the
provinces are in play. This is vital to the success and credibility of the portfolio and its work and
outcomes.
13
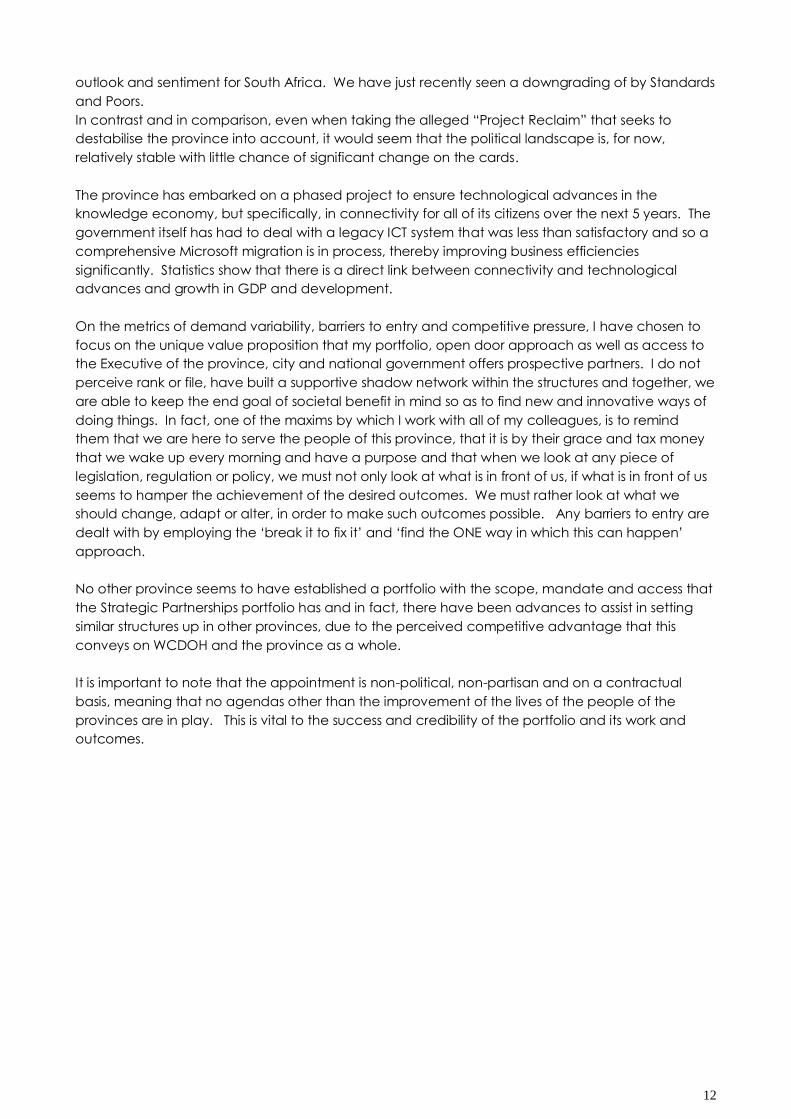
5.3 INDUSTRY ATTRACTIVENESS
5.3.1 RATIONALISING THE RATINGS
Health and Education are rated as the top priorities not only for government spending, but by a
great many corporate and philanthropic donors, as well as Non-Governmental Organisations
[NGO‟s]. Both of these areas are key drivers of growth and development.
In general, growth and investment in the Western Cape has remained stable with growth in certain
sectors, such as for instance Green Manufacturing and Health Biotechnology. The WCDOH is mid-
life-cycle, from the perspective that it has made significant advances over the past decade, is the
highest functioning health system in South Africa and has already achieved most of the objectives
that the NDOH has set out to be achieved in the rest of the country over the next decade.
There is however more work to be done to improve on best practice, work on staff morale,
upgrade infrastructure in collaboration with a range of partners and enter into innovative
transactional partnerships that would have the net effect of increasing service access points for
state patients, whilst assisting in generating annuity revenue for WCDOH over time, so as to
become less reliant on the fiscus as its sole source of income.
The WCDOH and WCGOV is perceived as being differentiated from the other provinces by virtue of
its geographic location, its unique demographic and psychographic profile, its cultural and
religious diversity, its natural beauty and of course, the high functioning nature of the state
institutions in regards to service delivery.
14
More and more donors, partners, corporates, NGO‟s and organisations are approaching the
Strategic Partnerships portfolio via referrals and word-of-mouth. In fact, it is fair to say that I have
not had to make one pro-active appointment in three years. This is both a good and bad thing of
course. Good, in the sense that we have been over-run with proposals and offers of pilot projects,
partnerships and collaborative engagements; bad – because a great many opportunities may
have been lost due to not having the luxury and time to take a breath and plan pro-actively and
capitalise on existing as well as pre-existing relationships. This situation has now however been
addressed by the narrowing of the scope of the portfolio and by agreeing very specific
performance indicators and objectives.
By nature, the „profit‟ potential for government and WCDOH is generally high within the partnership
space, specifically when working within the CSI space. But even then, we try to innovate by for
instance making a fully equipped, state-of-the-art theatre complex, donated and funded for the
most part by a range of partners, available as their showroom in South Africa and Africa. By
exposing surgeons and registrars in training to the new technology, it is common knowledge that
there is some influence on future purchase decisions and specifications, if said equipment show
real benefit and value in terms of clinical and patient outcomes. We also ensure that we provide
as many publicity opportunities as possible to our partners, so that they reap the benefit of the
goodwill with their prospective customers.
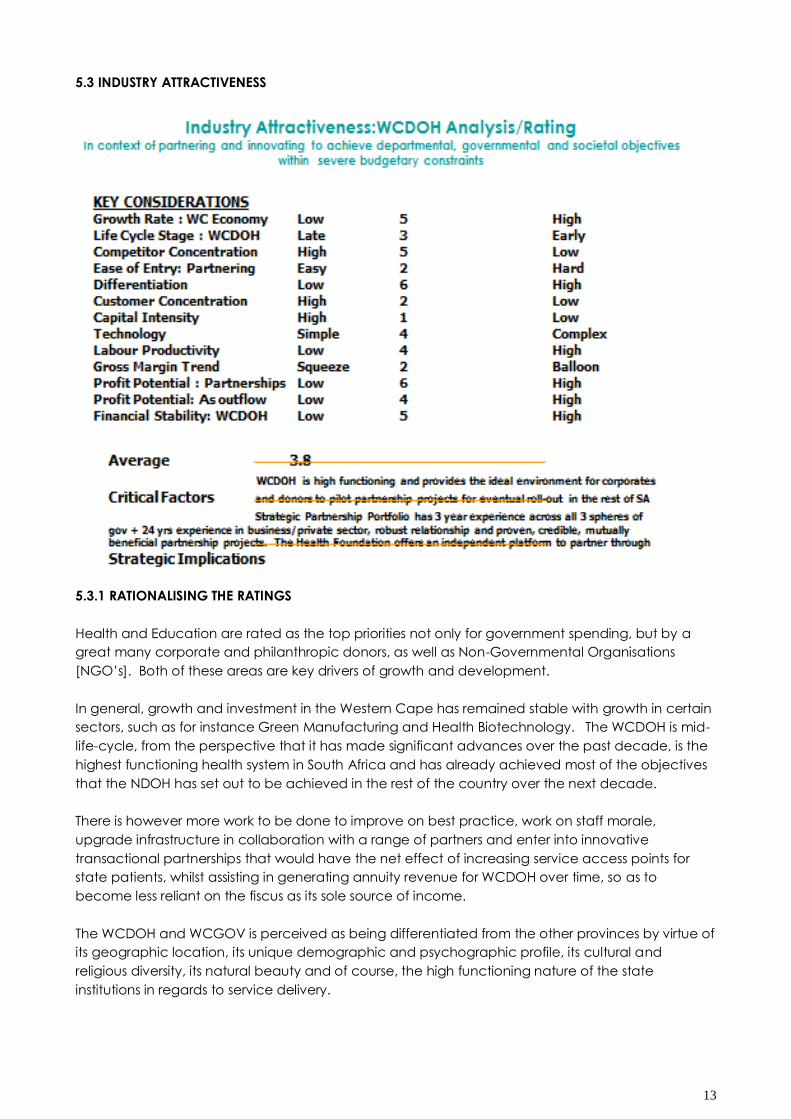
5.4 COMPETITIVE ATTRACTIVENESS
5.4.1 RATIONALISING THE RATINGS
The WCDOH serves approximately 75-80% of the population in the Western Cape – which pretty
much ensure market dominance in the health care industry. Having said that, the Western Cape
has one of the highest concentrations of private health facilities in the country and is also the
destination of choice for clinicians to settle with their families, due to the quality of life issues
attached to living in the province. The province also benefits from semi- and retired clinicians how
offer their services to mentor and train clinicians across the province.
15
Given that the Strategic Partnerships portfolio has had the privilege of building robust relationships
across all three spheres of government and with a myriad of role players and partners, its position is
currently relatively uncontested.
In terms of product quality, one always pushes towards improvement and excellence, so as to
surpass your best efforts of the day before. WCDOH certainly feels the pressure of improving on
and strengthening the foundation it has laid over the past decade and is making a paradigm shift
from curative to preventative health, as well as patient-centricity.
The product quality of the Strategic Partnership portfolio is evidenced through daily written and
verbal feedback related to the speed of service, the level of innovation, the passion and energy
for the task at hand, the grasping of a plethora of options and opportunities and the conversion
into real action and implementation in the shortest time possible. The role is also known for
unlocking and unblocking red tape and clearing speed bumps with some haste, when these issues
are holding up positive momentum. In my humble opinion, the quality of service, guidance,
assistance, counsel and relationships are held in high esteem by most of the „ partners‟ that I have
had the honour and privilege to engage with. Customer and partner loyalty is therefore very high
and trusting relationships exist.
WCDOH has a 4.1% staff vacancy rate - far lower than all other provinces. There are challenges
related to absenteeism due to stress and staff churns of about 14%. WCDOH is however working on
staff retention strategies as well as succession planning, aligned with improved performance
management.
Given that infrastructure and maintenance backlogs are estimated at R 1 billion and given that this
funding is not on budget, there is a high level of investment required from a range of partners in
order to achieve modernisation of infrastructure and equipment. We have however identified 16
potential areas of partnership – from straight forward cause marketing, adopt-a-facility or ward to
transactional relationships involving the possibility of exploring co-locations and co-ownership of
niche medical facilities adjacent to state health facilities, the availability of for instance mini
supermarkets at health facilities – rendering a service to communities, staff and patients, whilst
creating annuity revenue for the facility and department so as to expand and/or maintain levels of
service delivery during fiscally constrained periods. The notion of selling the „naming or
commercial‟ rights to key facilities to brands is also not out of the question. A range of innovative
options are currently in exploration and/or pilot phases.
It goes without saying that asset utilisation is high – and will continue to be so in the foreseeable
future, as the demand for services grow in the short term, but hopefully start declining in the mid- to
longer-term as the preventative and wellness outcomes start realising. The level of investment has
to be relatively high so as to convert the WCDOH into the most modern public health system on the
continent so that we are able to attract, train and retain the best possible clinical skills in our
province, country and continent.
Level of control is a contradictory term and perhaps begs exploration – there are mechanisms put
in place that allows our partners control in terms of where their funding is spent, what the outcomes
are and how transparent processes are. At the same time, the WCDOH is highly governed and
therefore controls and manages efficiencies. From the perspective of Strategic Partnerships, the
control is more subtle and involves using a strong and committed internal shadow network to
monitor the progress of projects and to ensure that they move through the system as swiftly as
possible towards implementation.
16
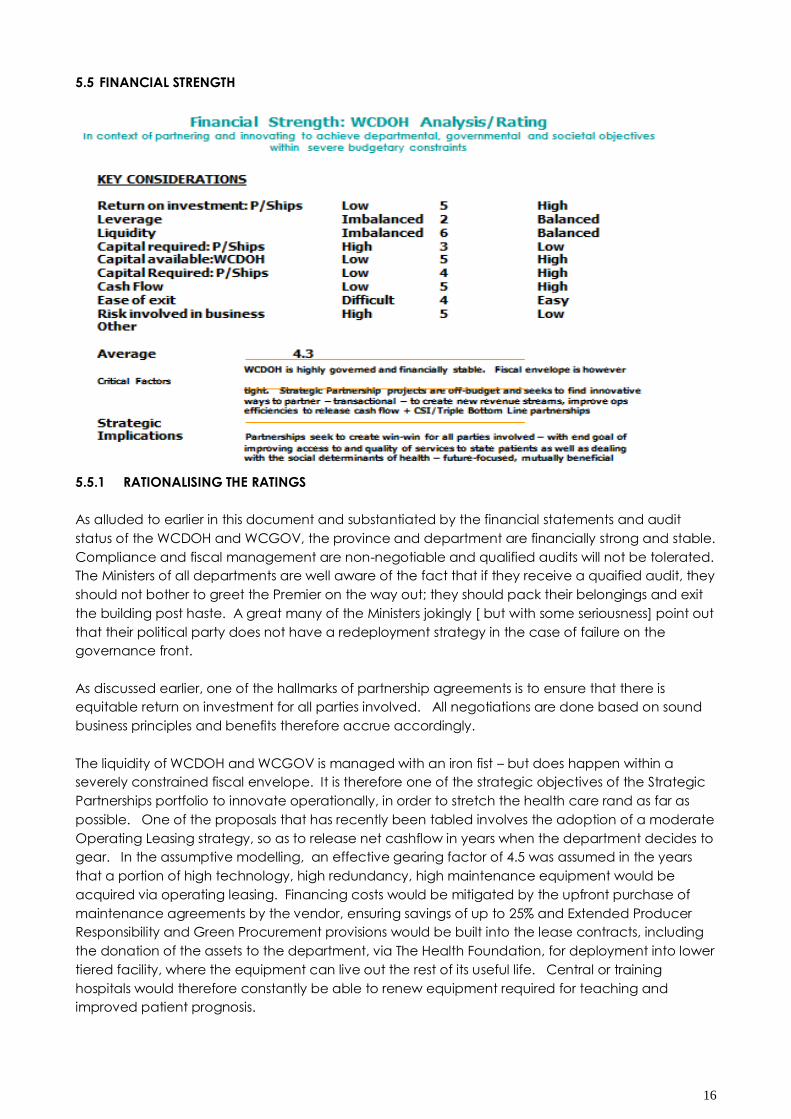
5.5 FINANCIAL STRENGTH
5.5.1 RATIONALISING THE RATINGS
As alluded to earlier in this document and substantiated by the financial statements and audit
status of the WCDOH and WCGOV, the province and department are financially strong and stable.
Compliance and fiscal management are non-negotiable and qualified audits will not be tolerated.
The Ministers of all departments are well aware of the fact that if they receive a quaified audit, they
should not bother to greet the Premier on the way out; they should pack their belongings and exit
the building post haste. A great many of the Ministers jokingly [ but with some seriousness] point out
that their political party does not have a redeployment strategy in the case of failure on the
governance front.
As discussed earlier, one of the hallmarks of partnership agreements is to ensure that there is
equitable return on investment for all parties involved. All negotiations are done based on sound
business principles and benefits therefore accrue accordingly.
The liquidity of WCDOH and WCGOV is managed with an iron fist – but does happen within a
severely constrained fiscal envelope. It is therefore one of the strategic objectives of the Strategic
Partnerships portfolio to innovate operationally, in order to stretch the health care rand as far as
possible. One of the proposals that has recently been tabled involves the adoption of a moderate
Operating Leasing strategy, so as to release net cashflow in years when the department decides to
gear. In the assumptive modelling, an effective gearing factor of 4.5 was assumed in the years
that a portion of high technology, high redundancy, high maintenance equipment would be
acquired via operating leasing. Financing costs would be mitigated by the upfront purchase of
maintenance agreements by the vendor, ensuring savings of up to 25% and Extended Producer
Responsibility and Green Procurement provisions would be built into the lease contracts, including
the donation of the assets to the department, via The Health Foundation, for deployment into lower
tiered facility, where the equipment can live out the rest of its useful life. Central or training
hospitals would therefore constantly be able to renew equipment required for teaching and
improved patient prognosis.

17
Cash flow is well managed and when entering into any form of partnership, a clear exit strategy is
agreed up-front so as to ensure that the department can plan over the Medium-Term Expenditure
Framework to bring operational and any other related costs into the budget. This ensures
sustainability of services.
Given the level of governance, quality of management and professional, business-like approach of
WCDOH and Strategic Partnerships the risks involved in doing business with WCDOH are low – if not
non-existent.
5.6 THE OUTCOME – WHERE IT ALL COMES TOGETHER – CONCLUSIONS AND RECOMMENDATIONS
From the graph above, it is evident that doing business with and partnering with the
WCDOH through its Strategic Partnerships Portfolio is highly desirable.
The department and portfolio both rank highly on all four quadrants of the matrix – which
provides a fair amount of comfort to potential partners and investors.
The scope of this particular report does not allow for a comprehensive and in-depth
discussion and analysis of all of the competitive dimensions that I would ideally like to
analyse in order to plot a clear and comprehensive strategy.
In an ideal world, I would have started the process with a current as well as future SWOT
analysis of NDOH, WCDOH and Strategic Partnerships. This would be the first phase of my
base analysis.
These analyses would complement Porter‟s Five Forces Model – which would look at the
industry growth overall.
The BCG Analysis would confirm the direction of the marketing orientation and strategy and
provide a clear direction on which projects and priority areas most of the resources should
be directed at and also, our market share and growth relative to our largest competitor.
I would then have proceeded to an Internal Factor Evaluation [IFE] to educate myself as to
the strengths and weaknesses in the functional areas of the business and the relationships
between these areas.
18
Thereafter, it follows that I would do an External Factor Evaluation [EFE], so as to confirm and
evaluate the current business and trading conditions that I am functioning within, visualise
and prioritise opportunities and threats facing the organisations and portfolio and of course,
include a comprehensive PESTEL analysis for good measure, as further benchmark and
baseline.
What makes these two models attractive from a multi-basing perspective, is the fact that
one is able to add a great many relevant elements, weight them and therefore bring a
more factual and numeric measure into the mix.
The natural progression for me would be to move to the Internal-External Model, which
combines the IFE and EFE, so as to assess the available strategic options.
If there are multiple strategy options, I would proceed to the Quantitative Strategic Planning
Matrix [QSFM] to establish where the real competitive „edge‟ is located.
I would more than likely end with the Balanced Scorecard to ensure that a performance
framework is put in place to ensure that that right decisions are taken and that there is
constant monitoring of the achievements against the strategic objectives of the
organisation – internally and externally.
All of these analyses, read together with the Space Matrix Model would provide the multiple
dimensions required so as to move forward with confidence and comfort.
It must of course be said that one is also led by your instinct and intuition in issues of strategy
and so common sense would still prevail in the midst of the potential analysis paralysis.
6 CONCLUSION
I have found this exercise interesting, informative, instructive and thought-provoking and have
already started the process as described above, against a range of strategic objectives, so as to
trial various combinations of methodologies and to compare their outcomes.
It has been satisfying to use the Space Matrix Model within the public sphere. The caveat in this
instance is of course that this is not necessarily „government-as-usual‟ in the traditional sense. The
structure, mandate, scope and business-like approach demonstrated by the WCDOH and
Strategic Partnerships may have skewed the outcome of the analysis and it would be extremely
interesting to in fact complete a comprehensive analysis as described within the section before –
by analysing and comparing NDOH, WCDOH, ECDOH and Strategic Partnerships and its successes
and innovations as part of the Unique Value Proposition of WCDOH and WCGOV.
In the final analysis, the Space Matrix Analysis process did however provide sufficient proof or
ratification that we are on the right track and that we should continue to explore, exploit and grow
our competitive advantage – not only in the interest of the people of our province, but with the
intent of building best practice models that could be scaled and replicated where it is most
needed, in the rest of the country.
19
7. REFERENCES: STRATEGIC MANAGEMENT ASSIGNMENT: EDP 2012
Anderson B, Phillips, H. 2006. Adult mortality (age 15‐64) based on death notification data in South
Africa: Statistics South Africa. Report No. 03‐09‐05. Pretoria: Statistics South Africa
Andrews G, Pillay, Y. 2005. Strategic Priorities for the National Health System 2004‐2009. In Ijumba P,
Barron P [Eds]. South African Health Review, 2005. Durban: Health Systems Trust.
Badri, M. Cleary, S. Maartens, G. Pitt. J. Bekker, L.G. Orrell, C. Wood, R. 2006. When to initiate highly active antiretroviral therapy in Sub‐Saharan Africa? A South African cost‐effectiveness study.
Antiviral Therapy 11(1):63‐72
Barron P (2008). A fifteen year review of the health sector in South Africa. Prepared for the
Department of Health, unpublished (December 2008)/ Barron P, Strachan K (1997). The Year in
Review. In Barron P (ed). South African Health Review 1997. Health Systems Trust.
http://www.hst.org.za/uploads/files/sahr2007.pdf [Accessed September 2012]
Biermann, J. 2006. South Africa‟s Health Care under Threat. International Policy Framework and
Free market Foundation
http://www.healthpolicyunit.org/downloads/Health_Care_under_Threat.pdf [Accessed October
2012] [Appendix E]
Botha, T. 26 March 2012. Western Cape Health Budget Speech 2012 by Mr Theuns Botha, Minister of
Health at Western Cape Provincial Legislature
Bradshaw D (2008). Chapter 4: Determinants of health and their trends. In Barron P, Roma‐Reardon
J (Eds). South African Health Review 2008. Health Systems Trust.
http://www.hst.org.za/uploads/files/sahr2008.pdf [Accessed September 2012]
Bradshaw D, Norman R, Lewin, S et al (2007). Strengthening public health in South Africa: Building a
stronger evidence base for improving the health of the nation. South African Medical Journal 97: 643 ‐ 649
Bradshaw, D. Groenewald, P. Laubscher. R. Nannan, N. Nojilana, B. Norman. R. Pieterse, D.
Schneider, M. 2003. Initial burden of disease estimates for South Africa, 2000. Burden of Disease
Research Unit, Medical Research Council.
http://www.mrc.ac.za/bod/bodestimates.pdf [Accessed October 2012]
Brinkmann, A. February 2010 onwards. A PASSPORT TO WELLNESS© A roadmap out of poverty,
towards growth and development. [Attached]
Centre for Scientific and Industrial Research (1996). National Health Facilities Audit. Division of
Building Technology, CSIR, in association with Department of Health and Raubenheimer & Partners.
Boutek research Report Bouc 5a, April 1996
Chopra, M. Lawn, J. Sanders, D. Barron, P et al. 2009. Achieving the health Millennium Development Goals for South Africa: challenges and priorities. The Lancet 374: 1023 ‐ 1031
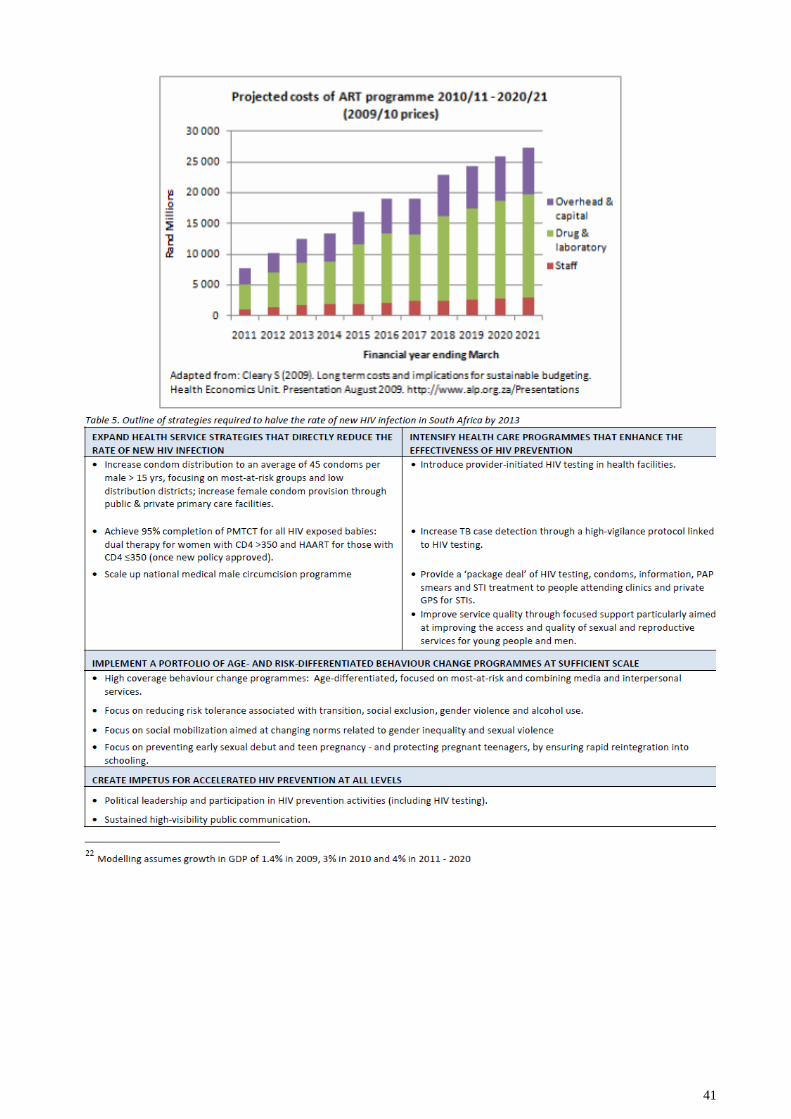
Cleary, S. 2009. Long term costs and implications for sustainable budgeting. Health Economics Unit.
Presentation August 2009. http://www.alp.org.za/Presentations [Accessed August 2012]
Cleary, S. McIntyre, D. Boulle, A. 2006. The cost‐effectiveness of antiretroviral treatment in
Khayelitsha, South Africa – a primary data analysis. Cost Effectiveness and Resource Allocation
4:20. Doi:10.1186 1478‐7547‐4‐20. http://www.resourceallocation.
com/content/4/1/20 [Accessed April 2011]
Daviaud, E. Chopra, M. 2008. How much is not enough? Human resources requirements for primary health care: a case study from South Africa. Bull World Health Organ. 2008 Jan; 86(1):46‐51.
http://www.who.int/bulletin/volumes/86/1/07‐042283.pdf [Accessed July 2011]
20
Day, C. Barron. P. Montecelli, F. Sello, E. [editors] 2009. The District Health Barometer 2007/8. Durban:
Health Systems Trust 35
Day, C. Gray, A. 2008. Health & Related Indicators. In Barron P, Roma‐Reardon J (Eds). South
African Health Review 2008. Health Systems Trust. http://www.hst.org.za/uploads/files/sahr2008.pdf
[Accessed November 2009]
Development Bank of Southern Africa. 2008. A Roadmap for the Reform of the South African Health
System. A process convened and facilitated by the Development Bank of Southern Africa.
Dorrington, R. Johnson, L. Bradshaw, D. Daniel, T. 2007. The Demographic Impact of HIV/AIDS in
South Africa: National and Provincial Indicators for 2006. Cape Town: Centre for Actuarial Research,
Medical Research Council and Actuarial Society of SA.
Harrison,D. December 2009. An Overview of Health and Health Care in South Africa 1994-2010:
Priorities, Progress and Prospects for New Gains. A Discussion Document Commissioned by the
Henry J. Kaiser Family Foundation to Help Inform the National Health Leaders‟ Retreat, Muldersdrift,
January 24-26 2010 [Appendix B]
Harrison, D. 2009. Rationale for the National Operational Plan for HIV Prevention. Pretoria:
Department of Health. http://www.doh.gov.za/ [Accessed July 2012]
Hirschowitz, R. Orkin, M. 1995]). A national household survey of health inequalities in South Africa.
The Community Agency for Social Enquiry (CASE) for the Henry J. Kaiser Family Foundation, Menlo
Park, CA.
http://dictionary.reference.com/browse/health. Define: Health. Accessed September 2012
Kevany, S. Meintjies, G. Rebe, K. Maartens, G. Cleary, S. 2009. Clinical and financial burdens of
secondary level care in a public sector antiretroviral setting (G F Jooste Hospital). South African Medical Journal 99: 320 ‐ 325
Lawn, S. Churchyard, G. 2009. Epidemiology of HIV‐associated tuberculosis. Current Opinion in HIV
and AIDS 4:325‐333
Lawn, S. Wood, R. 2007. When should antiretroviral treatment be started in patients with HIV‐associated tuberculosis in South Africa? South African Medical Journal 97: 414 ‐ 415
Lewin, S. Norman, R. Nannan, N. Thomas, E. Bradshaw, D and the South African Comparative Risk
Assessment Collaborating Group. 2007. Estimating the burden of disease attributable to unsafe
water and lack of sanitation and hygiene in South Africa in 2000. South African Medical Journal 97:
755 – 762
Mayosi, B. Flischer, A. Lalloo, U. Sitas, F. Tollman, S. Bradshaw, D. 2009. Health in South Africa 4: The
burden of non‐communicable diseases in South Africa. The Lancet 374: 934‐47
McIntyre, D. Bloom, G. Doherty, J. Brijlal, P. 1995. Health Expenditure and Finance in South Africa.
Durban: Health Systems Trust and World Bank
Myers, J. Naledi, T. et al. 2007. Western Cape Burden of Disease Reduction Project: Report
National Department of Health Strategic Plan 2010 – 2013.
Nannan, N. Norman, R. Hendricks, M. Dhansay, M. Bradshaw, D and the South African Comparative
Risk Assessment Collaborating Group. 2007. Estimating the burden of disease attributable to
childhood and maternal under nutrition in South Africa in 2000. South African Medical Journal 97:
733 ‐ 739
21
National Committee on Confidential Enquiries into Maternal Deaths. 2008. Saving mothers 2005‐2007. Fourth Report on Confidential Enquiries into Maternal Deaths (Expanded Executive
Summary). http://www.doh.gov.za/docs/reports‐f.html. [Accessed February 2010]
National Department of Health. 24 May 2012. Strategic Plan for Maternal, New-born, Child and
Women‟s Health [MNCWH] and Nutrition in South Africa 2012-2016
National Department of Health. 4 March 2012. Annual Performance Plan 2012/13 – 2014/15.
APPENDIX A: EXCERPTS
National Department of Health .2009a. Annual Report 2008/9. Pretoria.
http://www.doh.gov.za/docs/reports/annual/2009 [Accessed September 2012]
National Department of Health. 2009b. Strategic Plan 2009/10 – 2011/12. Pretoria. http://www.doh.gov.za/docs/strategic09‐11‐f.htm [Accessed September 2012]
(Accessed November 2009)
National Department of Health .2009c. Operational Plan for HIV Prevention (in final draft,
December 2009). Pretoria
National Department of Health and Medical Research Council. 2008. South Africa Demographic
and Health Survey 2003. http://www.doh.gov.za/docs/reports‐f.html
National Department of Health. 2008. Annual Report 2007/8. Pretoria.
http://www.doh.gov.za/docs/reports/annual/2008 [Accessed October 2012]
National Department of Health. 2007. A policy on quality of health care in South Africa. Pretoria.
http://www.doh.gov.za/docs/policy/qhc.pdf
National Department of Health. 2006. A National Human Resources Plan for Health to provide skilled
human resources for healthcare adequate to take care of all South Africans; 2006.
URL: http://www.doh.gov.za/docs/discuss/2006/hrh_plan/index.html
National Department of Health. 2005. The Charter of the Health Sector of the Republic of South
Africa (Draft revised 28 October 2005). http://www.doh.gov.za/docs/misc‐f.html
National Department of Health. 1997. White Paper for the Transformation of the Health System.
Pretoria: Government Printer
National Treasury South Africa. 22 February 2012. 2012 Budget Speech Minister of Finance Pravin
Gordhan
National Treasury Department: South Africa. August 2012. Medium Term Expenditure Framework
Guidelines. Preparation of Expenditure Estimates for the 2012 Medium Term Expenditure Framework.
Norman, R. Bradshaw, D. Schneider, M et al. 2007. A comparative risk assessment for South Africa in 2000: towards promoting health and preventing disease. South African Medical Journal 97: 637 ‐ 641
Sachs, J, D. 20 December 2001. Macroeconomics and Health: Investing in Health for Economic
Development. Report of the Commission on Macroeconomics and Health
Scott, R. Harrison, D. 2009. A gauge of HIV prevention in South Africa. Johannesburg: loveLife Trust.
http://www.lovelife.org.za/prevention_gauge
Seedat, M. van Niekerk, A. Jewkes, R. Suffla, S. Ratele, K. 2009. Violence and injuries in South Africa: Prioritizing an agenda for prevention. The Lancet 374: 1011‐ 1022
22
Segall, M. May 1999. “The Bottle Is Half Full”: Policy Oriented Overview of The Main Findings of a
Review of Public Health Service Delivery
Statistics South Africa. Statistical Release P0302. 27 July 2011. Mid-year Population Estimates 2011.
http://www.statssa.gov.za/
Statistics South Africa. 2005. Mortality and causes of death in South Africa, 1997 – 2003. Statistical
release PO309.3.
http://www.statssa.gov.za/publications/P03093/P03093.pdf. [Accessed February 2012]
Statistics South Africa. 2009a. Mortality and causes of death in South Africa, 2007. Findings from
death notification. Statistical release PO309.3.
http://www.statssa.gov.za/publications/P03093/P030932007.pdf. [ Accessed March 2011]
Statistics South Africa .2009b. Road traffic accident deaths in South Africa, 2001 – 2006: Evidence from death notification. Report no. 03‐09‐07. Pretoria:
http://www.statssa.gov.za/publications/Report‐03‐09‐07/Report‐03‐09‐07.pdf
Statistics South Africa .2009c. Gross Domestic Product Annual Estimates 1993 – 2008: Third Quarter
2009. Statistical release PO441.
http://www.statssa.gov.za/publications/P0441/P04413rdQuarter2009.pdf
Taylor, B. 2007. Rationing of Medicines and Health Care Technology. In Harrison, S. Bhana, R. Ntuli,
A. (Eds). South African Health Review 2007. Health Systems Trust.
http://www.hst.org.za/uploads/files/sahr2007.pdf [Accessed September 2012]
Van Holdt, K. Murphy, M. 2007. Public hospitals in South Africa: stressed institutions, disempowered
management. In Buhlungu, S. Daniel, J. Southall, R. Lutchman, J. State of the Nation: South Africa
2007. Cape Town: HSRC Press
Van den Heever, A. 2009. The determinants of medical scheme membership. In CMS News. Issue
No. 2 of 2009 – 2010. Pretoria: Council for Medical Schemes. http://www.medicalschemes.com
Western Cape Department of Health. November 2011. Vision 2020 – The future of health care in the
Western Cape: A Draft Framework for Dialogue [Appendix G]
Western Cape Department of Health. March 2012. Annual Performance Plan 2012-2013
Western Cape Department of Health. August 2012. Annual Report 2011-2012
Western Cape Department of Health. 8 November 2011. The Cape Town Declaration on Wellness:
Wellness Summit [Appendix H]
World Development Report (2006). Equity and Development. Washington DC: The World Bank.
http://www.worldbank.org
World Health Organisation. 4 April 2011. South Africa Health profile. www.doh.gov.za.[ Accessed
September 2012]
World Health Organisation. 21 October 2011. Rio Political Declaration on the Determinants of
Health. http://www.who.int/sdhconference/declaration/en/. [Accessed September 2012]
www.earthzense.com/Definition-of-wellness. Define: Wellness: Accessed September 2012
23
APPENDIX A: NATIONAL DEPARTMENT OF HEALTH: ANNUAL PERFORMANCE PLAN: HIGHLIGHTS
[National Department of Health. March 2012.]
In its Annual Performance Plan 2012/13 – 2014/15, [National Department of Health. 7 March 2012]
the following highlights and priorities are iterated: 7.1.1 One of the focal areas remains dealing with the Quadruple Burden of Disease [BOD]:
HIV/AIDS, TB, Violence & Injury and Non-Communicable Diseases [NCD].
7.1.2 The focus on dealing with NCD will be: * Reducing tobacco smoking * Reducing of
harmful alcohol consumption * Promoting physical activity * Addressing unhealthy diets.
7.1.3 It is recognised that to deal with inter-personal, gender-based violence and injury, a
broader, inter-sectoral, societal approach will be required.
7.1.4 Infrastructure continues to crumble and there are huge backlogs in maintenance,
upgrades, equipment that need to be dealt with in order to strengthen the healthcare
system.
7.1.5 Primary Healthcare [PHC] re-engineering, district health, PHC outreach programmes
and school health will be put in place.
Human Resources for Health [HRH] strategy and plan have been put into place to deal
with the shortage of clinical staff in South Africa. 7.1.6 After the national audit of all health facilities, it has been determined that there is an
urgent need to train and up skill the management at health facilities.
7.1.7 There is also an urgent requirement to strengthen health information systems.
7.1.8 Furthermore, there is a need to accelerate collaboration with other government
departments so as to expedite the national turnaround strategy.
7.1.9 All efforts are focused on the eventual roll-out of the National Health Insurance [NHI]
and Universal Healthcare for all.
7.1.10 In terms of refocusing on the re-engineering of the PHC system, the social determinants
of health must be dealt with; this was agreed at the World Health Organisation [WHO]
Conference on the Social Determinants of Health, held in Brazil in October 2011. This led
to the Rio Declaration on the Social Determinants of Health [World Health Organisation.
21 October 2011].
7.1.11 It is anticipated that this Declaration will be the basis for the development of a
framework and plan that would seek to deal with the social determinants of disease –
the starting point being to firstly establish and agree what these determinants are and
how they should be dealt with.
7.1.12 NDOH plans to deploy at least 5000 Community-based Healthcare Workers to assist
District Teams.
7.1.13 There will be a renewed focus on school health with nurses being deployed to the 8000
schools in the lowest quintiles and supplementation with mobile health units to provide
packages of health screening and treatment – including oral, dental,
7.1.14 In Grades 8-10 there will be a focus on HIV/AIDS prevention and education, prevention
of teenaged pregnancies and drug abuse; the focus will be on prevention and health
promotion.
7.1.15 Public Private Partnerships are viewed as one of the ways in which the delivery of health
infrastructure could be accelerated.
7.1.16 The Baseline for Under Five Infant Mortality is currently 56 in 1000 live births; a target of 50
in 1000 live births has been set for 2014/15.
7.1.17 The Baseline for Infant Mortality is currently 40 in 1000 live births; a target of 36 in 1000 live
births has been set for 2014/15.
7.1.18 The Baseline for Maternal Mortality is currently 310 per 100 000 births; the target for
2014/15 has been set at 270 per 100 000 births.

24
n general, NDOH has agreed to the Health Sector Negotiated Delivery Agreement, which has 12
outcomes in total. NDOH is responsible for the achievement of Outcome 2 namely: A long and
healthy life for all South Africans.
NDOH has furthermore committed to the delivery of the Health-related Millennium Development
Goals: * to eradicate extreme poverty and hunger * Promote gender equality and empower
women * Reduce child mortality * Improve maternal health
25
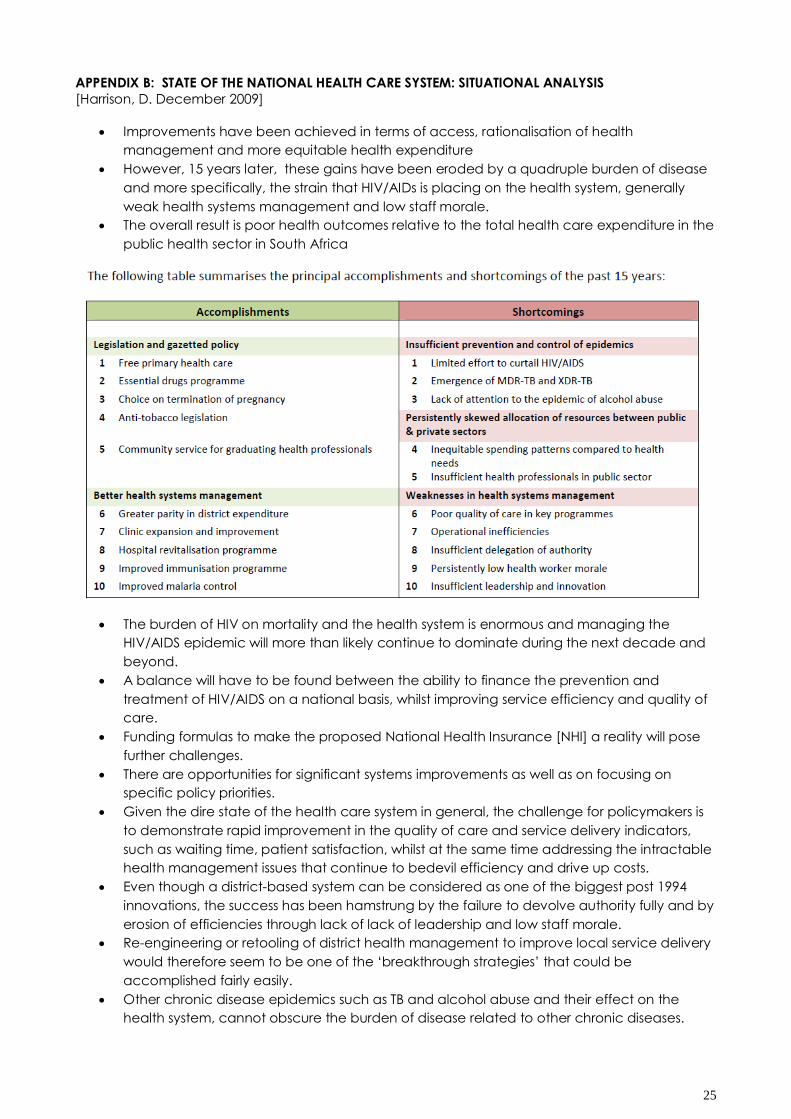
APPENDIX B: STATE OF THE NATIONAL HEALTH CARE SYSTEM: SITUATIONAL ANALYSIS
[Harrison, D. December 2009]
Improvements have been achieved in terms of access, rationalisation of health
management and more equitable health expenditure
However, 15 years later, these gains have been eroded by a quadruple burden of disease
and more specifically, the strain that HIV/AIDs is placing on the health system, generally
weak health systems management and low staff morale.
The overall result is poor health outcomes relative to the total health care expenditure in the
public health sector in South Africa
The burden of HIV on mortality and the health system is enormous and managing the
HIV/AIDS epidemic will more than likely continue to dominate during the next decade and
beyond.
A balance will have to be found between the ability to finance the prevention and
treatment of HIV/AIDS on a national basis, whilst improving service efficiency and quality of
care.
Funding formulas to make the proposed National Health Insurance [NHI] a reality will pose
further challenges.
There are opportunities for significant systems improvements as well as on focusing on
specific policy priorities.
Given the dire state of the health care system in general, the challenge for policymakers is
to demonstrate rapid improvement in the quality of care and service delivery indicators,
such as waiting time, patient satisfaction, whilst at the same time addressing the intractable
health management issues that continue to bedevil efficiency and drive up costs.
Even though a district-based system can be considered as one of the biggest post 1994
innovations, the success has been hamstrung by the failure to devolve authority fully and by
erosion of efficiencies through lack of lack of leadership and low staff morale.
Re-engineering or retooling of district health management to improve local service delivery
would therefore seem to be one of the „breakthrough strategies‟ that could be
accomplished fairly easily.
Other chronic disease epidemics such as TB and alcohol abuse and their effect on the
health system, cannot obscure the burden of disease related to other chronic diseases.
26
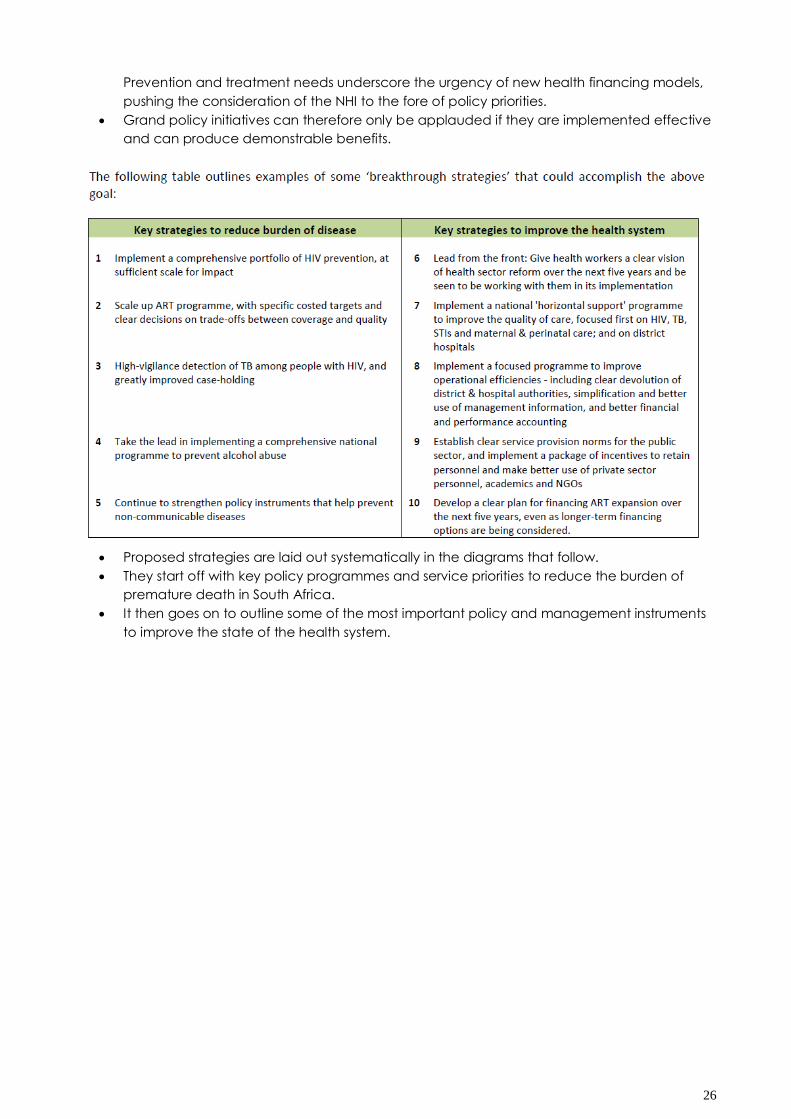
Prevention and treatment needs underscore the urgency of new health financing models,
pushing the consideration of the NHI to the fore of policy priorities.
Grand policy initiatives can therefore only be applauded if they are implemented effective
and can produce demonstrable benefits.
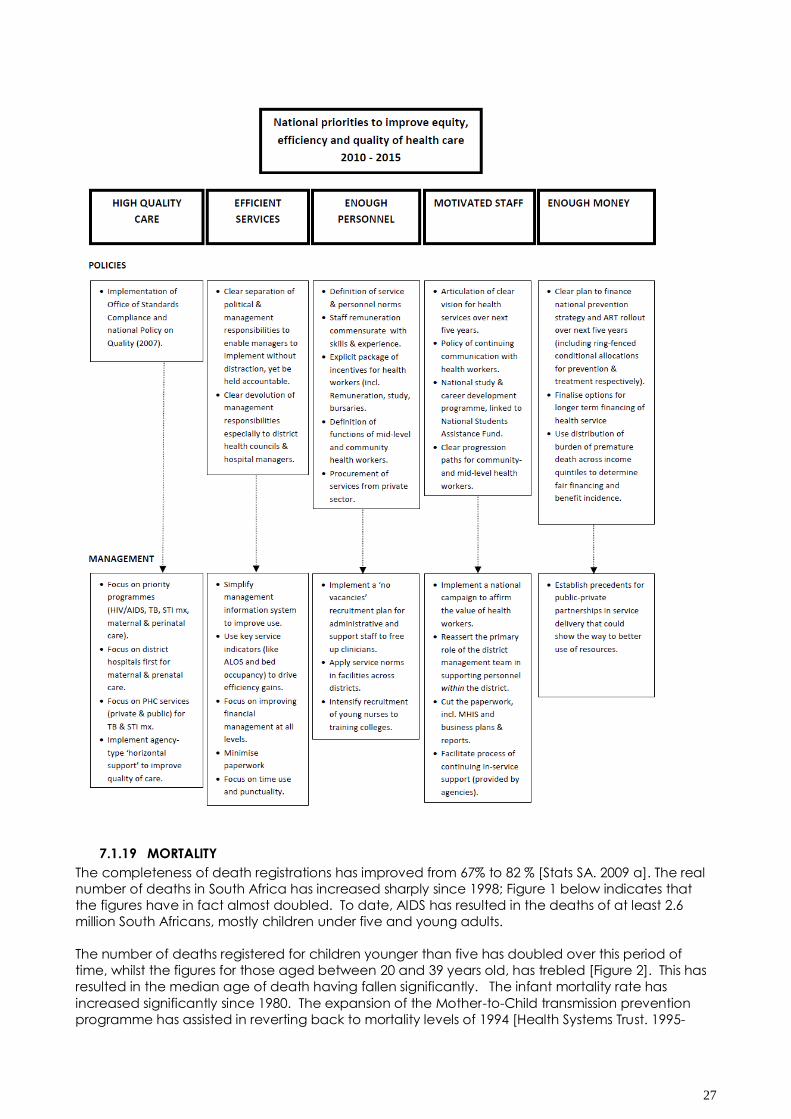
Proposed strategies are laid out systematically in the diagrams that follow.
They start off with key policy programmes and service priorities to reduce the burden of
premature death in South Africa.
It then goes on to outline some of the most important policy and management instruments
to improve the state of the health system.
27
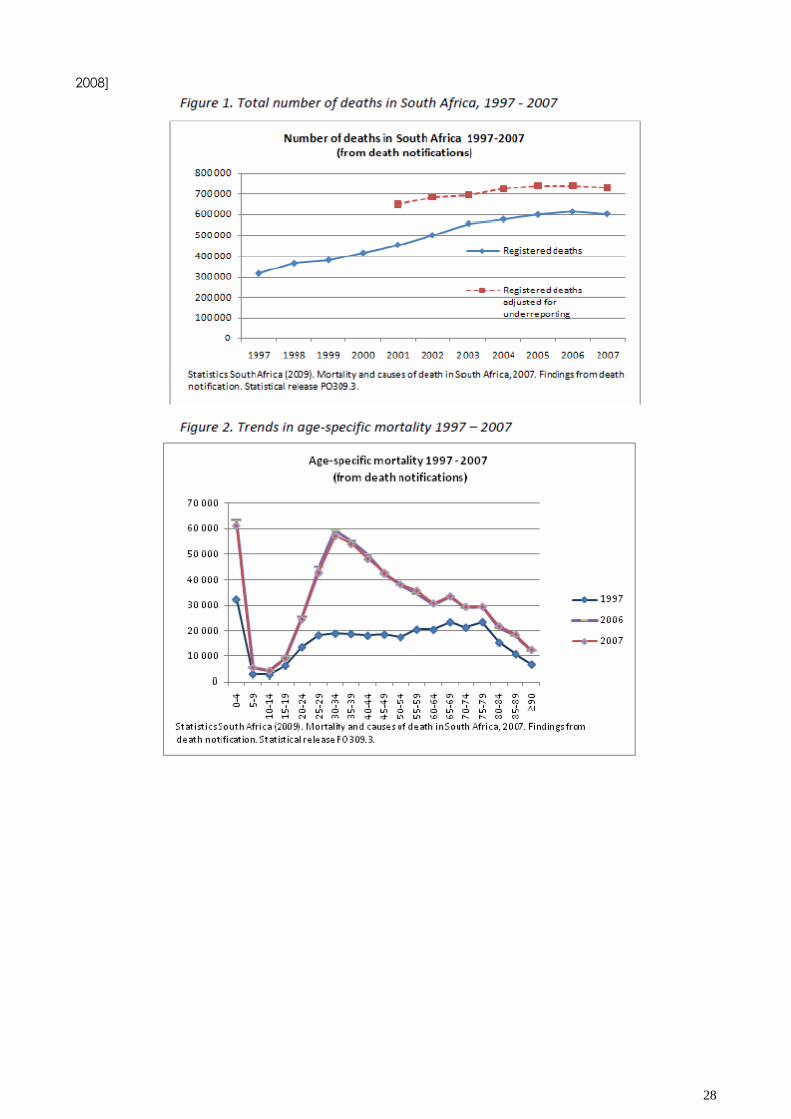
7.1.19 MORTALITY
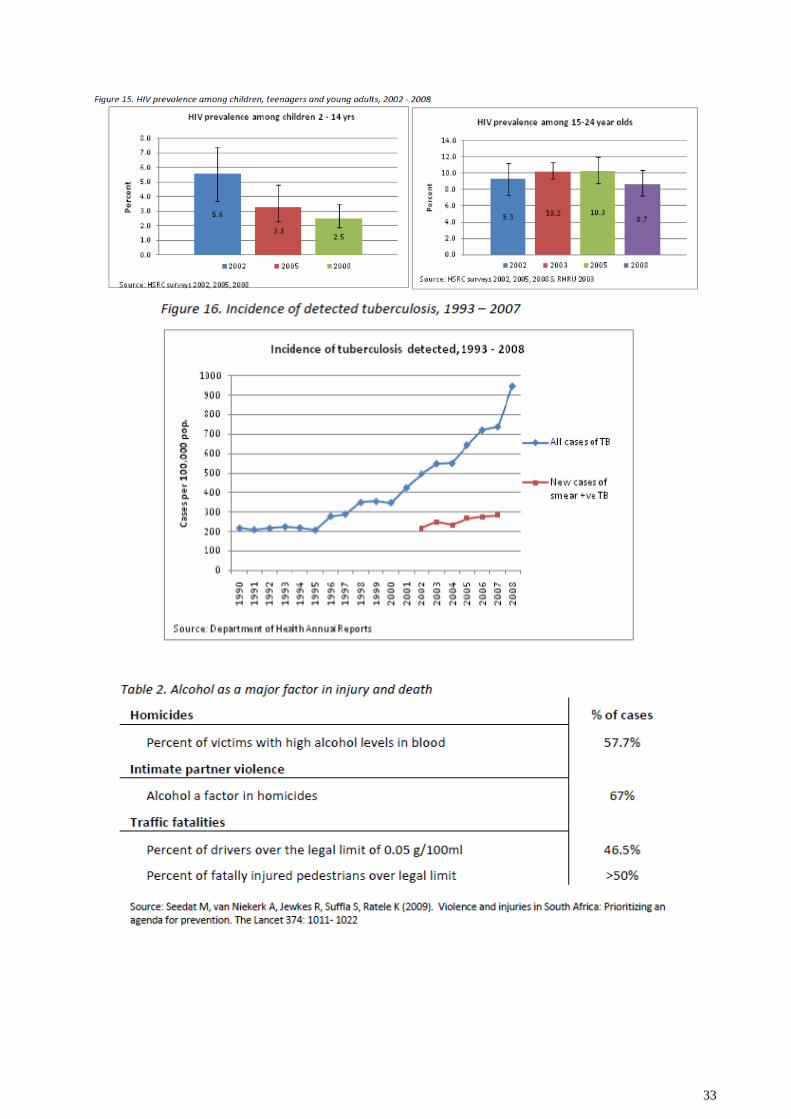
The completeness of death registrations has improved from 67% to 82 % [Stats SA. 2009 a]. The real
number of deaths in South Africa has increased sharply since 1998; Figure 1 below indicates that
the figures have in fact almost doubled. To date, AIDS has resulted in the deaths of at least 2.6
million South Africans, mostly children under five and young adults.
The number of deaths registered for children younger than five has doubled over this period of
time, whilst the figures for those aged between 20 and 39 years old, has trebled [Figure 2]. This has
resulted in the median age of death having fallen significantly. The infant mortality rate has
increased significantly since 1980. The expansion of the Mother-to-Child transmission prevention
programme has assisted in reverting back to mortality levels of 1994 [Health Systems Trust. 1995-
28
2008]
29
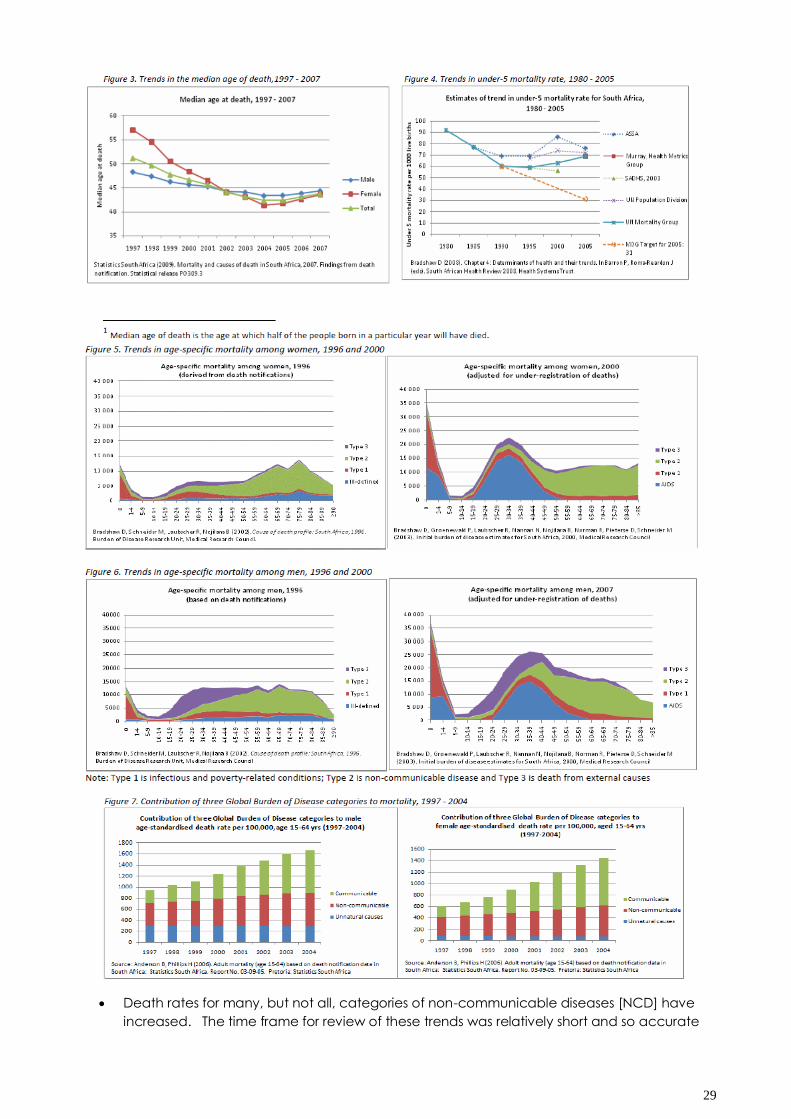
Death rates for many, but not all, categories of non-communicable diseases [NCD] have
increased. The time frame for review of these trends was relatively short and so accurate
30
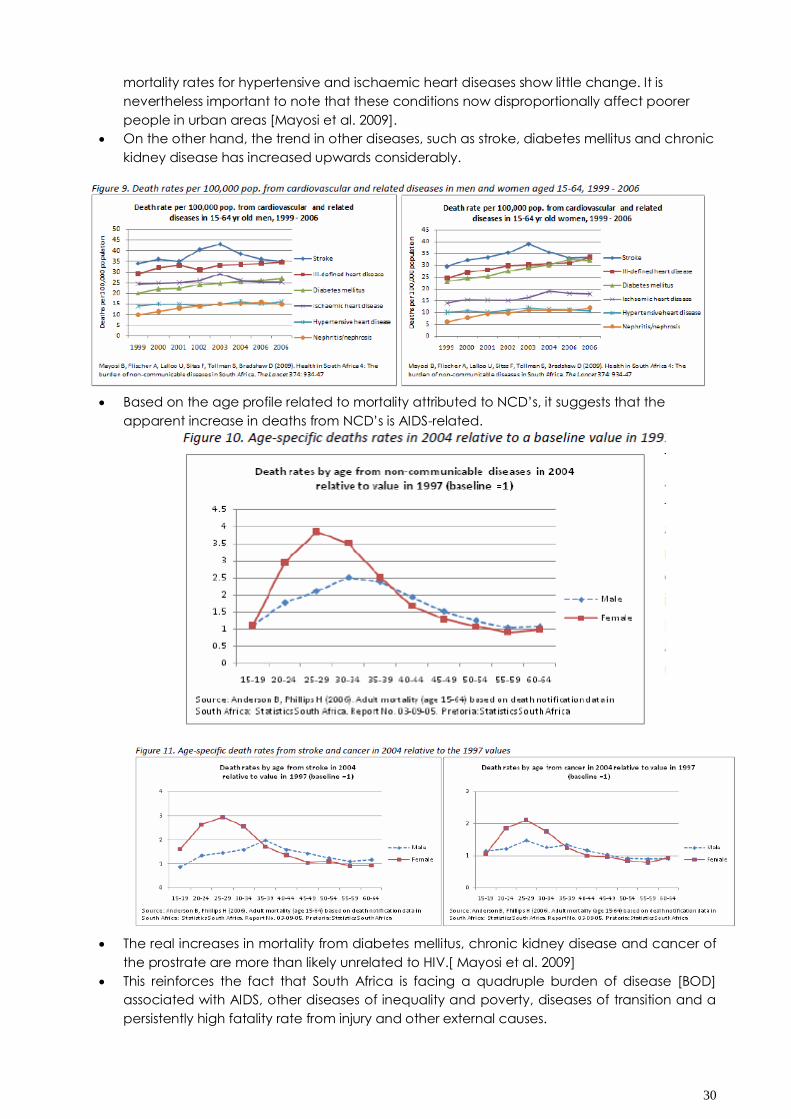
mortality rates for hypertensive and ischaemic heart diseases show little change. It is
nevertheless important to note that these conditions now disproportionally affect poorer
people in urban areas [Mayosi et al. 2009].
On the other hand, the trend in other diseases, such as stroke, diabetes mellitus and chronic
kidney disease has increased upwards considerably.
Based on the age profile related to mortality attributed to NCD‟s, it suggests that the
apparent increase in deaths from NCD‟s is AIDS-related.
The real increases in mortality from diabetes mellitus, chronic kidney disease and cancer of
the prostrate are more than likely unrelated to HIV.[ Mayosi et al. 2009]
This reinforces the fact that South Africa is facing a quadruple burden of disease [BOD]
associated with AIDS, other diseases of inequality and poverty, diseases of transition and a
persistently high fatality rate from injury and other external causes.
31
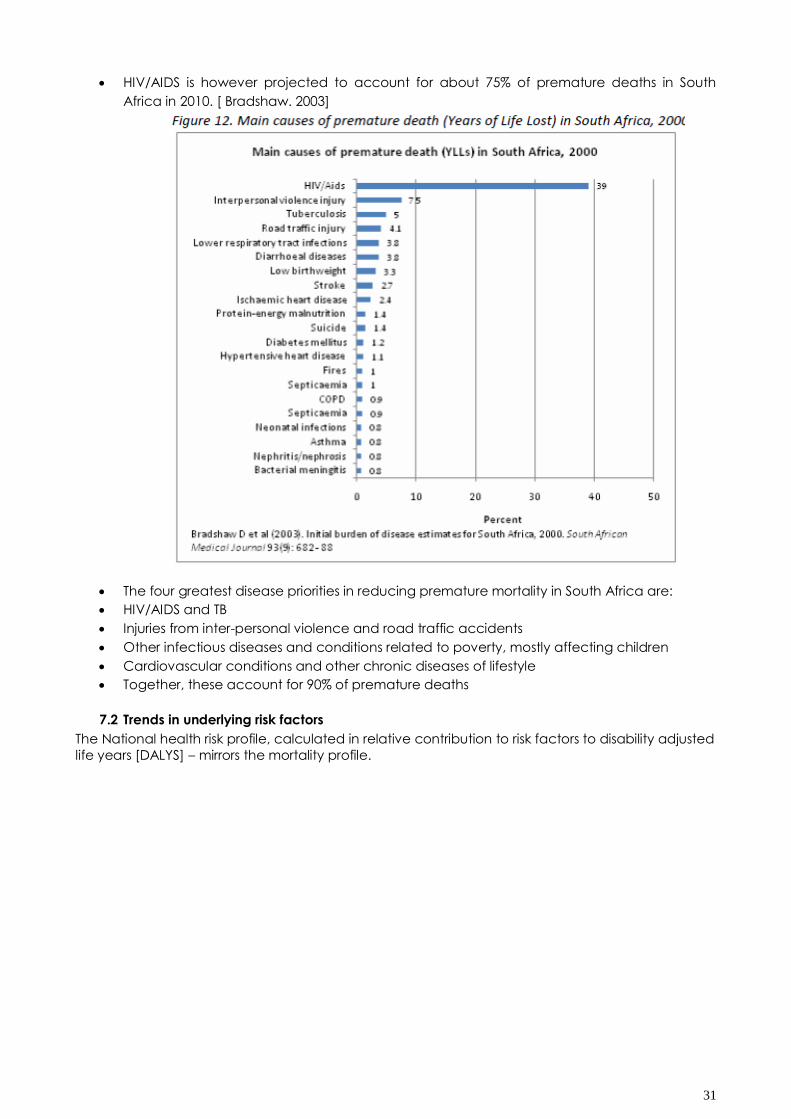
HIV/AIDS is however projected to account for about 75% of premature deaths in South
Africa in 2010. [ Bradshaw. 2003]
The four greatest disease priorities in reducing premature mortality in South Africa are:
HIV/AIDS and TB
Injuries from inter-personal violence and road traffic accidents
Other infectious diseases and conditions related to poverty, mostly affecting children
Cardiovascular conditions and other chronic diseases of lifestyle
Together, these account for 90% of premature deaths
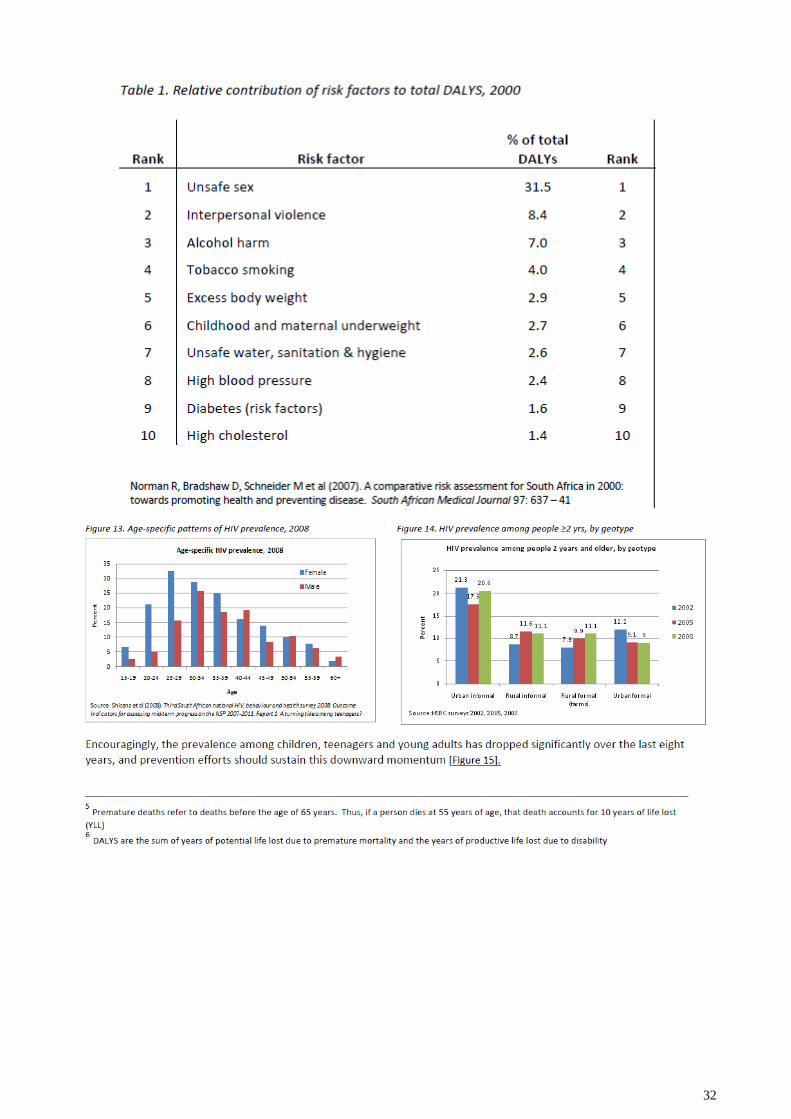
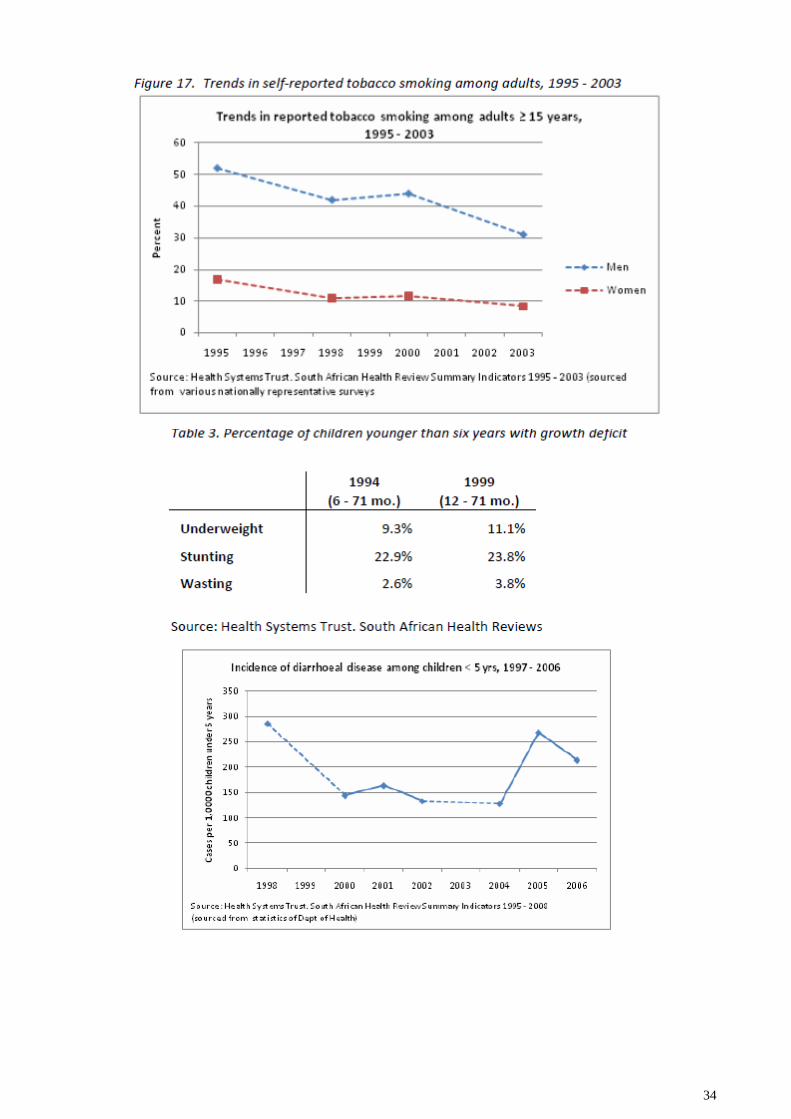
7.2 Trends in underlying risk factors
The National health risk profile, calculated in relative contribution to risk factors to disability adjusted
life years [DALYS] – mirrors the mortality profile.
32
33
34
35
36
37
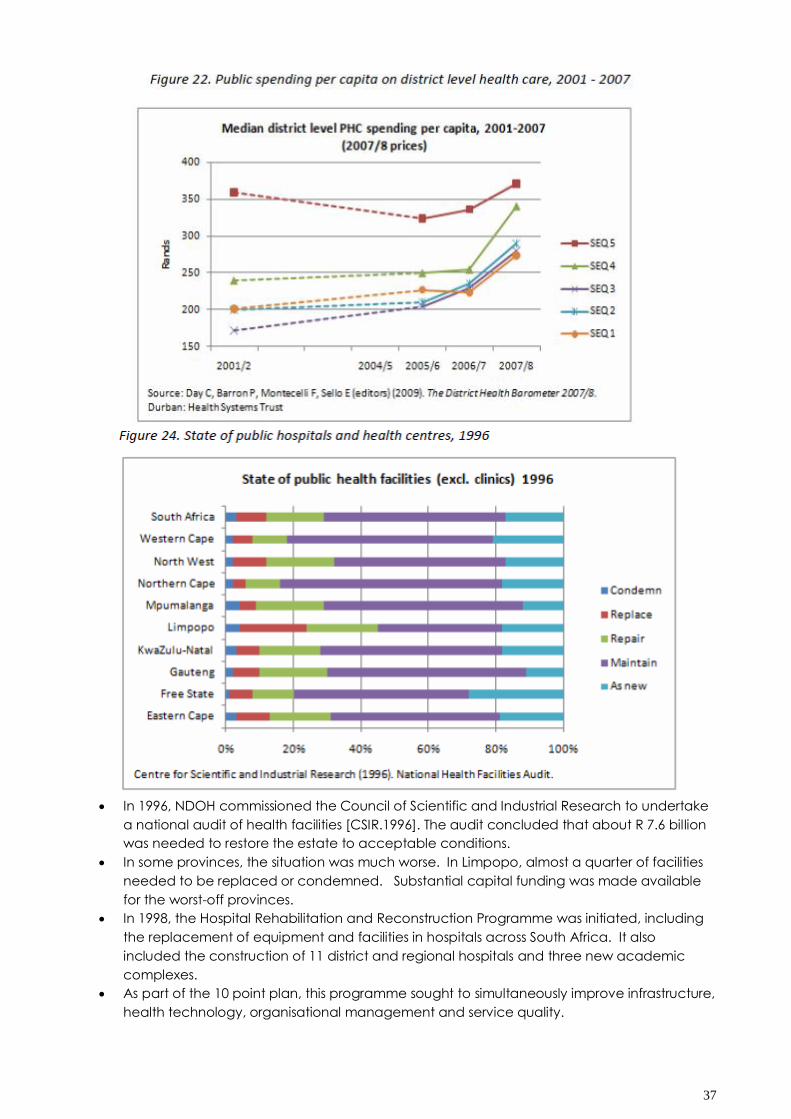
In 1996, NDOH commissioned the Council of Scientific and Industrial Research to undertake
a national audit of health facilities [CSIR.1996]. The audit concluded that about R 7.6 billion
was needed to restore the estate to acceptable conditions.
In some provinces, the situation was much worse. In Limpopo, almost a quarter of facilities
needed to be replaced or condemned. Substantial capital funding was made available
for the worst-off provinces.
In 1998, the Hospital Rehabilitation and Reconstruction Programme was initiated, including
the replacement of equipment and facilities in hospitals across South Africa. It also
included the construction of 11 district and regional hospitals and three new academic
complexes.
As part of the 10 point plan, this programme sought to simultaneously improve infrastructure,
health technology, organisational management and service quality.
38
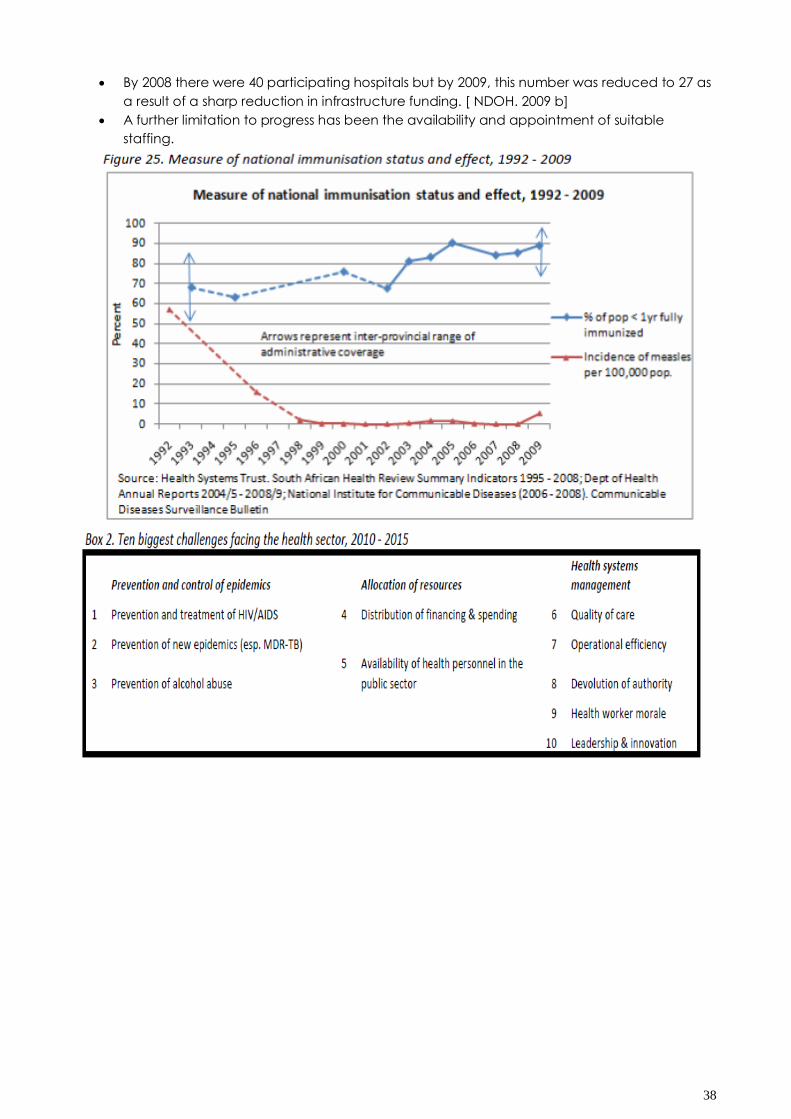
By 2008 there were 40 participating hospitals but by 2009, this number was reduced to 27 as
a result of a sharp reduction in infrastructure funding. [ NDOH. 2009 b]
A further limitation to progress has been the availability and appointment of suitable
staffing.
39
40
41
42
43
44
45
46
47
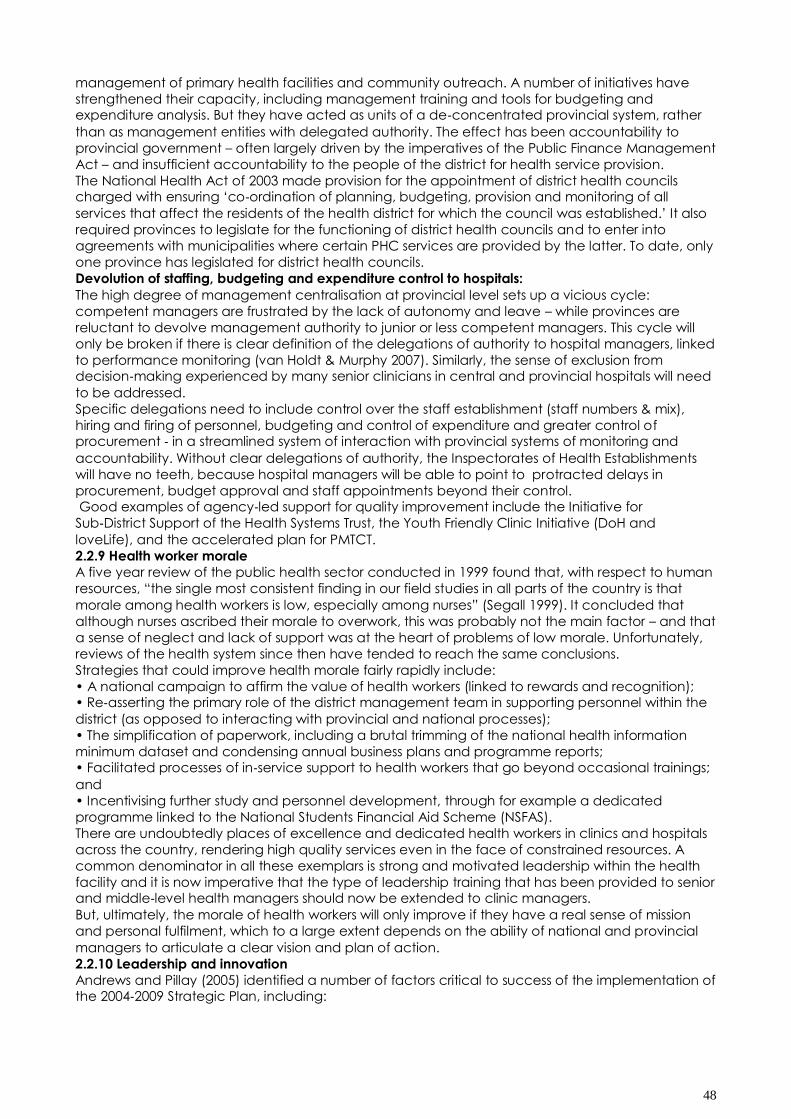
Devolution of management authority
There are two urgent priorities with respect to devolution of authority, namely the institutionalisation
of the district health system and devolution of staffing, budgeting and expenditure control of
hospitals to hospital management.
Some of the key challenges are described below:
District health system:
Since 1994, the district health system has been recognised as the main mechanism for
implementation of primary health care (Owen 1995). Yet it has failed to be properly institutionalised. District management teams have been appointed and are responsible for day‐to‐day
48
management of primary health facilities and community outreach. A number of initiatives have
strengthened their capacity, including management training and tools for budgeting and expenditure analysis. But they have acted as units of a de‐concentrated provincial system, rather
than as management entities with delegated authority. The effect has been accountability to
provincial government – often largely driven by the imperatives of the Public Finance Management
Act – and insufficient accountability to the people of the district for health service provision.
The National Health Act of 2003 made provision for the appointment of district health councils charged with ensuring „co‐ordination of planning, budgeting, provision and monitoring of all
services that affect the residents of the health district for which the council was established.‟ It also
required provinces to legislate for the functioning of district health councils and to enter into
agreements with municipalities where certain PHC services are provided by the latter. To date, only
one province has legislated for district health councils.
Devolution of staffing, budgeting and expenditure control to hospitals:
The high degree of management centralisation at provincial level sets up a vicious cycle:
competent managers are frustrated by the lack of autonomy and leave – while provinces are
reluctant to devolve management authority to junior or less competent managers. This cycle will
only be broken if there is clear definition of the delegations of authority to hospital managers, linked
to performance monitoring (van Holdt & Murphy 2007). Similarly, the sense of exclusion from decision‐making experienced by many senior clinicians in central and provincial hospitals will need
to be addressed.
Specific delegations need to include control over the staff establishment (staff numbers & mix),
hiring and firing of personnel, budgeting and control of expenditure and greater control of procurement ‐ in a streamlined system of interaction with provincial systems of monitoring and
accountability. Without clear delegations of authority, the Inspectorates of Health Establishments
will have no teeth, because hospital managers will be able to point to protracted delays in
procurement, budget approval and staff appointments beyond their control. Good examples of agency‐led support for quality improvement include the Initiative for
Sub‐District Support of the Health Systems Trust, the Youth Friendly Clinic Initiative (DoH and
loveLife), and the accelerated plan for PMTCT.
2.2.9 Health worker morale
A five year review of the public health sector conducted in 1999 found that, with respect to human
resources, “the single most consistent finding in our field studies in all parts of the country is that
morale among health workers is low, especially among nurses” (Segall 1999). It concluded that
although nurses ascribed their morale to overwork, this was probably not the main factor – and that
a sense of neglect and lack of support was at the heart of problems of low morale. Unfortunately,
reviews of the health system since then have tended to reach the same conclusions.
Strategies that could improve health morale fairly rapidly include:
• A national campaign to affirm the value of health workers (linked to rewards and recognition); • Re‐asserting the primary role of the district management team in supporting personnel within the
district (as opposed to interacting with provincial and national processes);
• The simplification of paperwork, including a brutal trimming of the national health information
minimum dataset and condensing annual business plans and programme reports; • Facilitated processes of in‐service support to health workers that go beyond occasional trainings;
and
• Incentivising further study and personnel development, through for example a dedicated
programme linked to the National Students Financial Aid Scheme (NSFAS).
There are undoubtedly places of excellence and dedicated health workers in clinics and hospitals
across the country, rendering high quality services even in the face of constrained resources. A
common denominator in all these exemplars is strong and motivated leadership within the health
facility and it is now imperative that the type of leadership training that has been provided to senior and middle‐level health managers should now be extended to clinic managers.
But, ultimately, the morale of health workers will only improve if they have a real sense of mission
and personal fulfilment, which to a large extent depends on the ability of national and provincial
managers to articulate a clear vision and plan of action.
2.2.10 Leadership and innovation
Andrews and Pillay (2005) identified a number of factors critical to success of the implementation of the 2004‐2009 Strategic Plan, including:
49
• Leadership, and in particular, political leaders as well as managers in the health system, must
clearly articulate and communicate a vision and a mission that will resonate with front line health
workers.
• A programme of action that is developed with, and that captures the imagination of, those
charged with its implementation. This would require greater empowerment of leaders at the local
level to drive the change agenda.
These critical success factors are just as relevant today. To these, a third should be added – namely
a mechanism for leadership development and public innovation in the health sector. This mechanism – an agency (or agencies), working with provincial and district managers ‐ would be
able to provide „horizontal support to the district management team and health workers at facility
level.
In this way, an agenda of change would remain on the front burner, even as pressing concerns
and management crises inevitably take up the time of senior health service managers. But neither
should the latter abdicate responsibility: a mechanism of „horizontal support‟ will only work if it
enjoys the backing of senior management. A commitment by senior management to visit health
facilities at least once a month to share the vision and provide encouragement could rebuild a
sense of common purpose.
PROSPECTS FOR NEW GAINS
The review of successes presented in section 2.1 above shows that many of the breakthroughs
were achieved through bold policy initiatives. Not surprisingly, many of them were accomplished in
the first five years of democratic government, which presented a singular window of opportunity for
policy development and implementation.
The squeeze on public spending in the late nineties knocked the wind out of the sails of health
systems transformation. But the loss of momentum was not only the result of financial constraints:
Failure to regulate the private sector properly, coupled with the inability to motivate staff across the
public sector, accelerated the drain of health professionals in the first few years of the new
millennium.
The advent of the mortality phase of the AIDS epidemic – noticeable from about 1998 – signalled a
period of growing pressure on the health system, and growing frustration from both health workers
and civil society alike at the apparent ambivalence of Government to deal with it effectively.
Nevertheless, it should be noted that, even during this phase, there were some important breakthroughs in health policy, including anti‐tobacco legislation and community service for
graduating health professionals. There were also incremental improvements in health systems
management and rationalisation in a number of provinces, which received little media attention.
The time and effort taken to unravel and restructure the fragmented health services of apartheid
should not be underestimated. But now, the South African public health system stands on the edge
of a chasm, which can only be bridged by new resources and decisive leadership. There is no way
that the public health system will be able to be sustained at current levels of funding – if the rollout
of the ART programme is to continue.
To some extent, the resources may be obtained by better use of the public resources and services
of the private sector. To a large extent, it will require new funding.
This is the intent of the proposed national health insurance (NHI) system. There is however the risk
that the NHI will be viewed as the panacea for both financing shortfalls and health service
deficiencies, and sight should not be lost of the fact that the NHI is essentially a financing
mechanism. In this regard, it would be injudicious to rule out the option of sourcing new funding
through general taxation – as opposed to a dedicated payroll tax – until the implications of the
latter are fully understood.
The pressures on the health system over the next five years imply that there will be little margin for
trial‐and‐error. Some of important factors to consider in decisions about an NHI are presented in
Appendix 1, but the key point is that an NHI (and/or other financing mechanisms) will enable the
implementation of policies and programmes that address national health priorities. Of itself, it is not
a national health priority. These are described below.
HIV prevention:
If health planning is informed by an analysis of the burden of disease, there is no doubt that the
greatest health priority is to prevent new HIV infection. This will require the full and urgent
implementation of the comprehensive strategies outlined in section 2.1. An urgent priority for the
financial year 2010/11 is to saturate the demand for condoms in high prevalence districts and most‐at‐risk groups. The big gaps in coverage of community‐level behaviour change programme
will need to be urgently addressed – requiring additional funding from Government and its bilateral
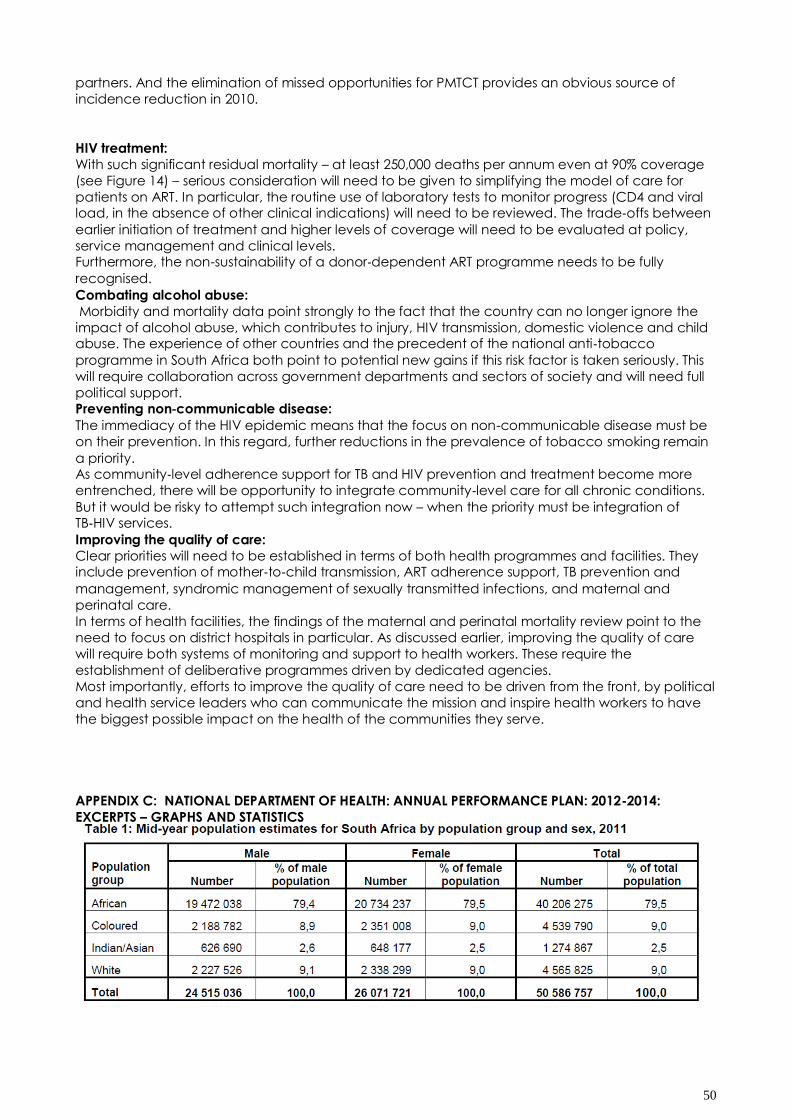
50
partners. And the elimination of missed opportunities for PMTCT provides an obvious source of
incidence reduction in 2010.
HIV treatment:
With such significant residual mortality – at least 250,000 deaths per annum even at 90% coverage
(see Figure 14) – serious consideration will need to be given to simplifying the model of care for
patients on ART. In particular, the routine use of laboratory tests to monitor progress (CD4 and viral load, in the absence of other clinical indications) will need to be reviewed. The trade‐offs between
earlier initiation of treatment and higher levels of coverage will need to be evaluated at policy,
service management and clinical levels. Furthermore, the non-sustainability of a donor‐dependent ART programme needs to be fully
recognised.
Combating alcohol abuse:
Morbidity and mortality data point strongly to the fact that the country can no longer ignore the
impact of alcohol abuse, which contributes to injury, HIV transmission, domestic violence and child abuse. The experience of other countries and the precedent of the national anti‐tobacco
programme in South Africa both point to potential new gains if this risk factor is taken seriously. This
will require collaboration across government departments and sectors of society and will need full
political support. Preventing non‐communicable disease:
The immediacy of the HIV epidemic means that the focus on non-communicable disease must be
on their prevention. In this regard, further reductions in the prevalence of tobacco smoking remain
a priority. As community‐level adherence support for TB and HIV prevention and treatment become more
entrenched, there will be opportunity to integrate community‐level care for all chronic conditions.
But it would be risky to attempt such integration now – when the priority must be integration of TB‐HIV services.
Improving the quality of care:
Clear priorities will need to be established in terms of both health programmes and facilities. They include prevention of mother‐to‐child transmission, ART adherence support, TB prevention and
management, syndromic management of sexually transmitted infections, and maternal and
perinatal care.
In terms of health facilities, the findings of the maternal and perinatal mortality review point to the
need to focus on district hospitals in particular. As discussed earlier, improving the quality of care
will require both systems of monitoring and support to health workers. These require the
establishment of deliberative programmes driven by dedicated agencies.
Most importantly, efforts to improve the quality of care need to be driven from the front, by political
and health service leaders who can communicate the mission and inspire health workers to have
the biggest possible impact on the health of the communities they serve.
APPENDIX C: NATIONAL DEPARTMENT OF HEALTH: ANNUAL PERFORMANCE PLAN: 2012-2014:
EXCERPTS – GRAPHS AND STATISTICS
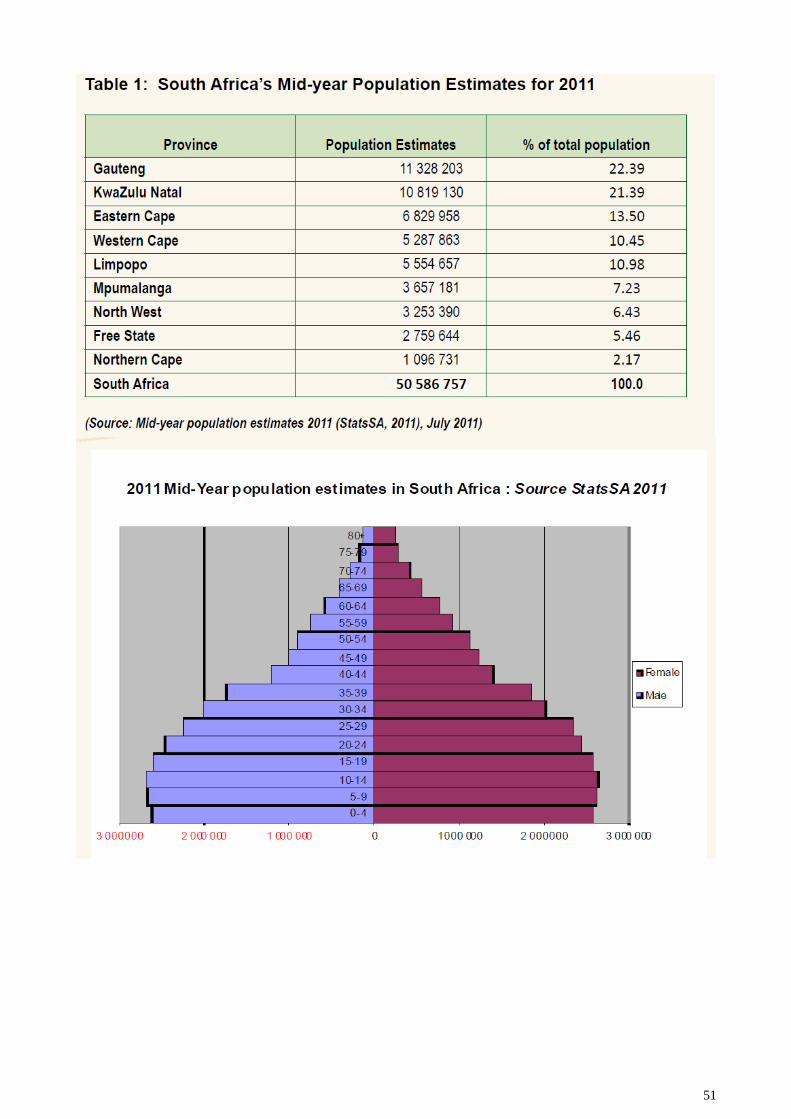
51
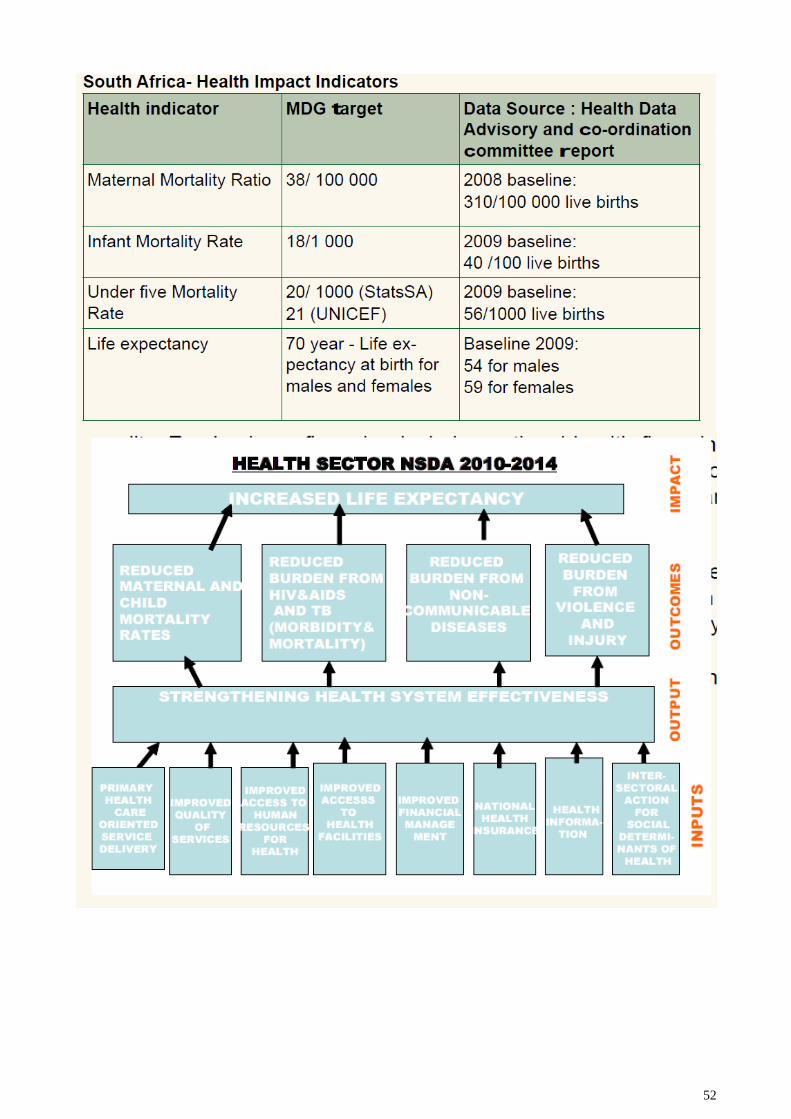
52
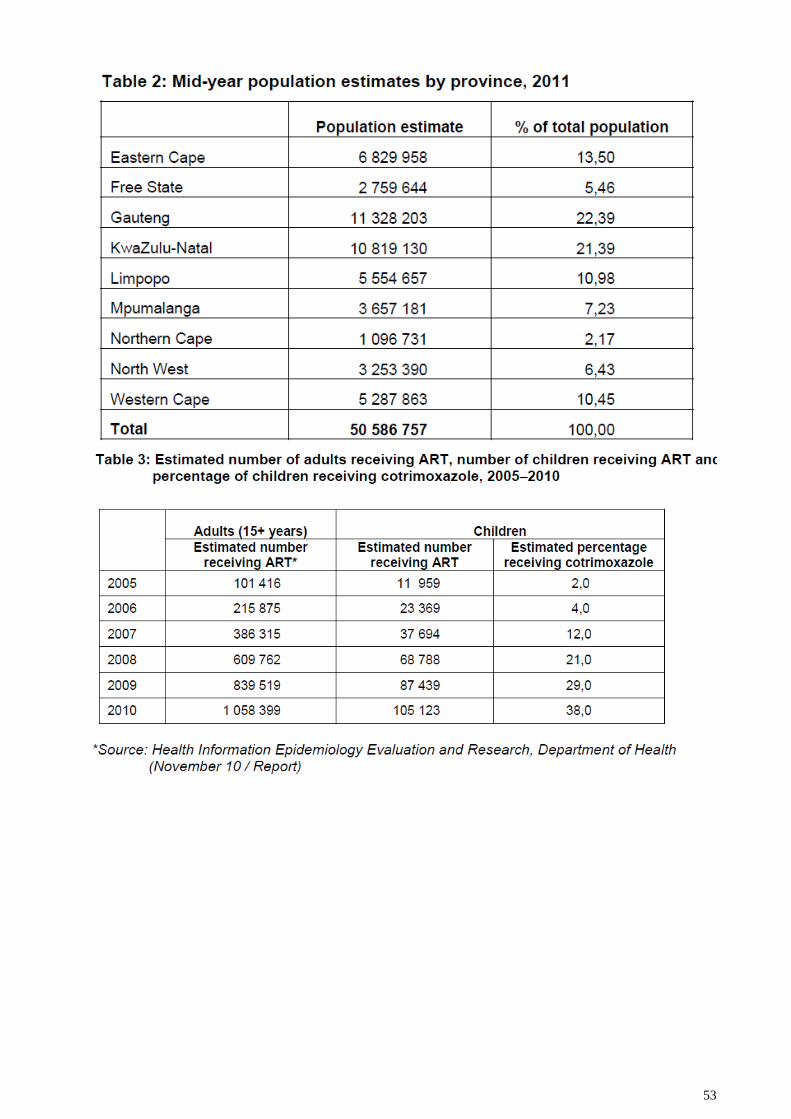
53
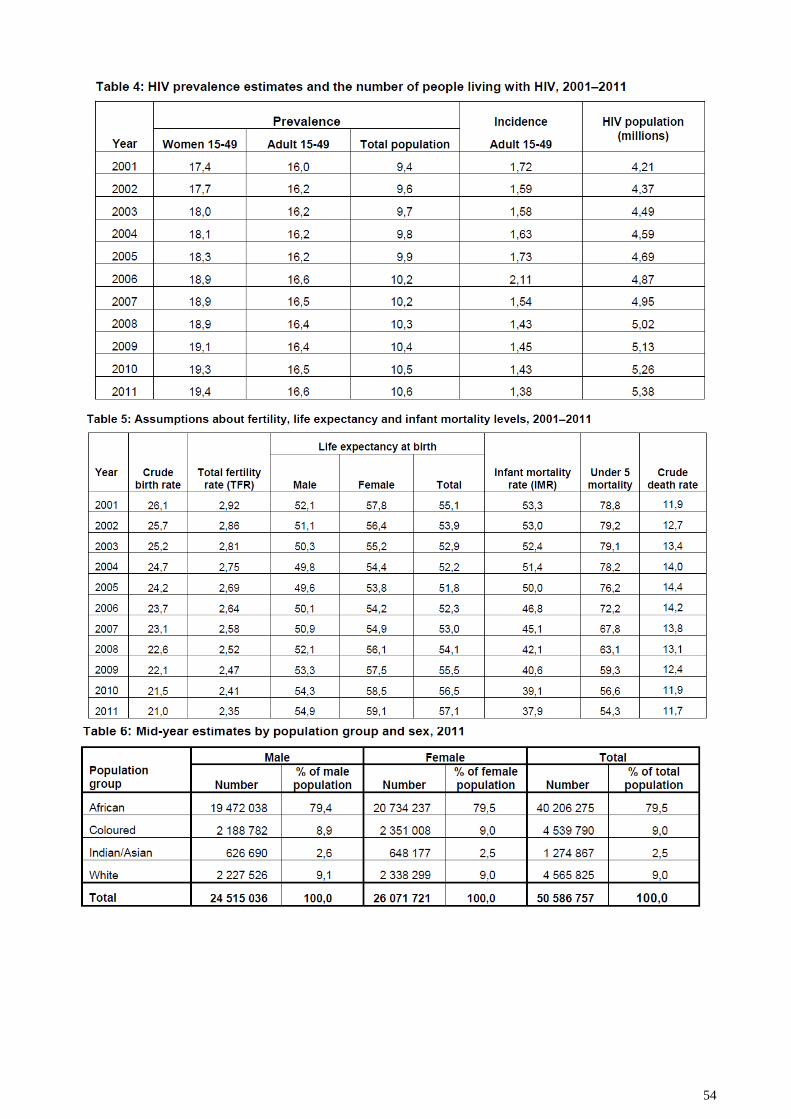
54
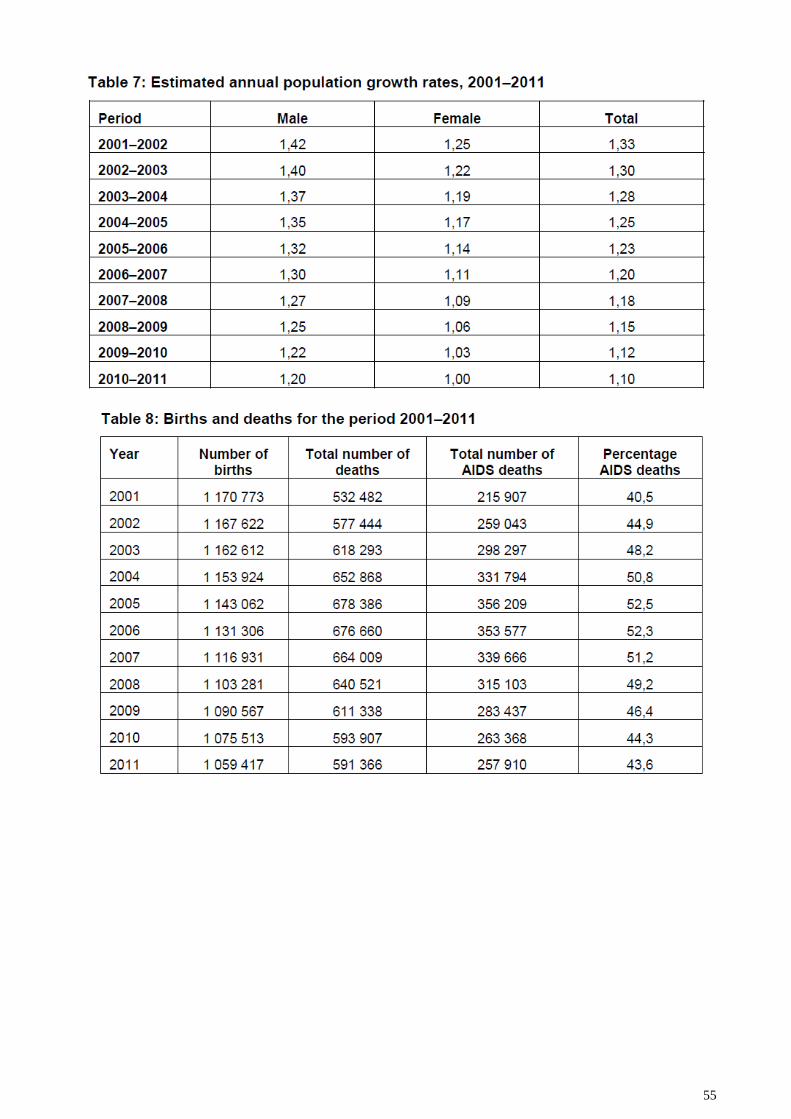
55
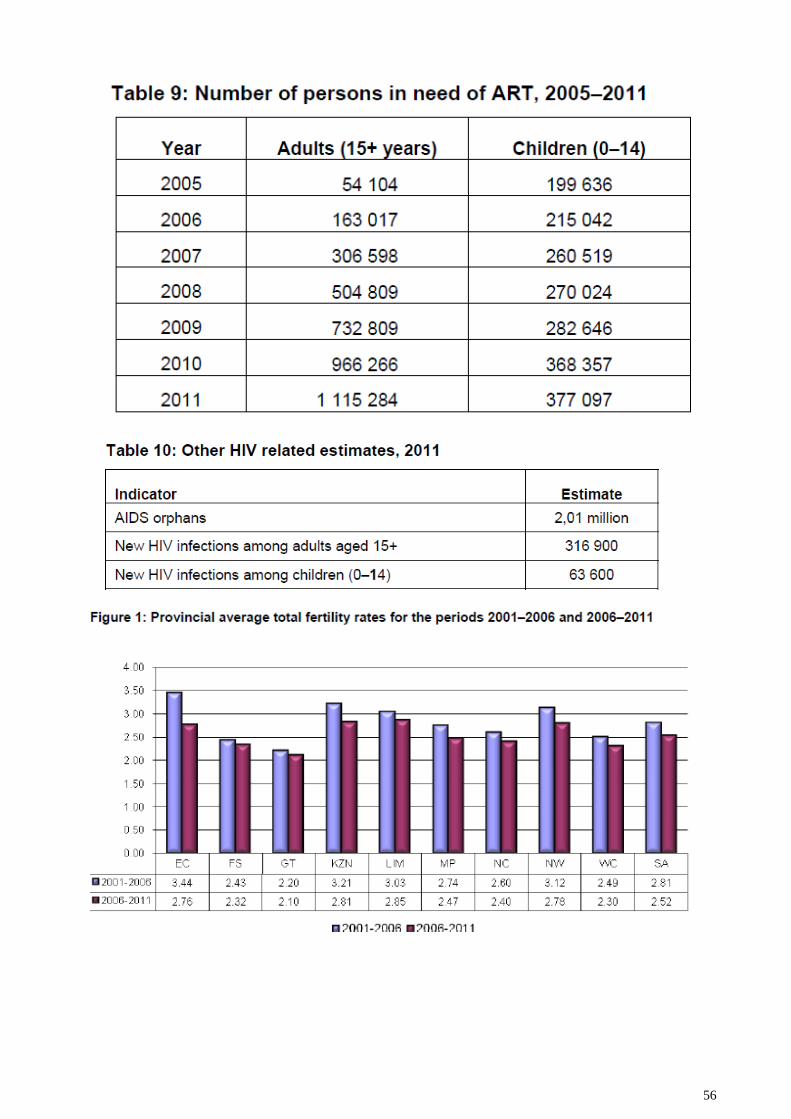
56
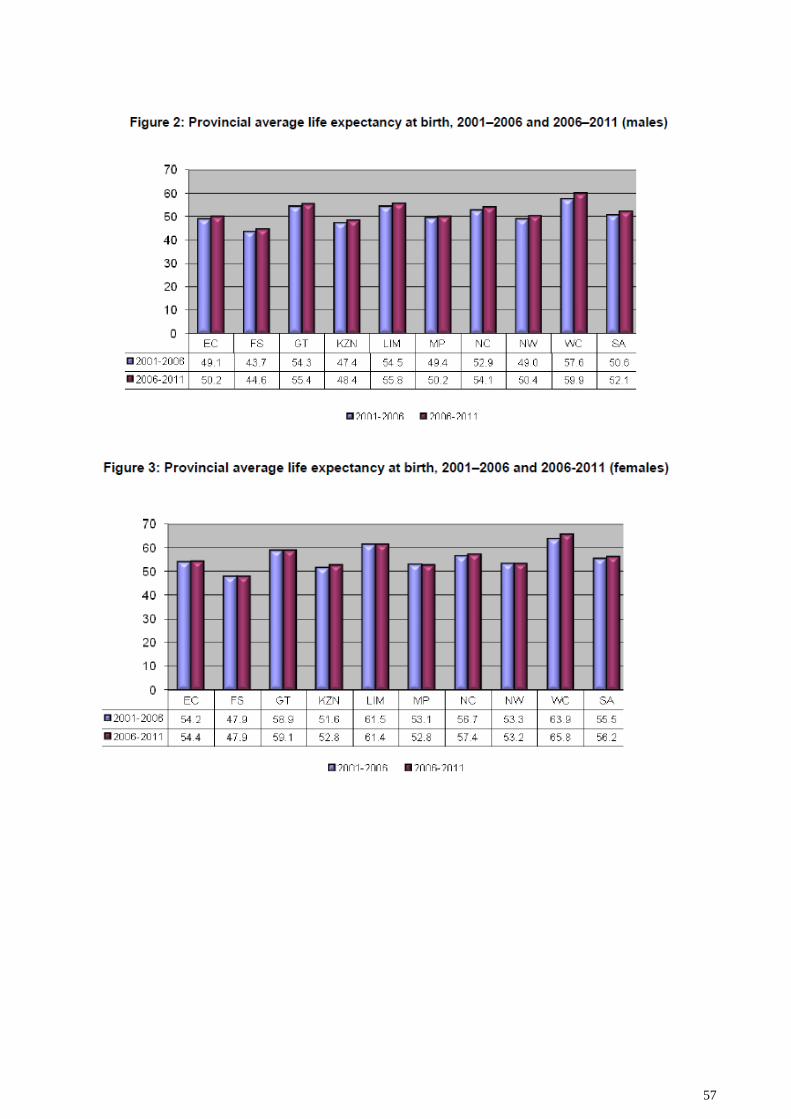
57
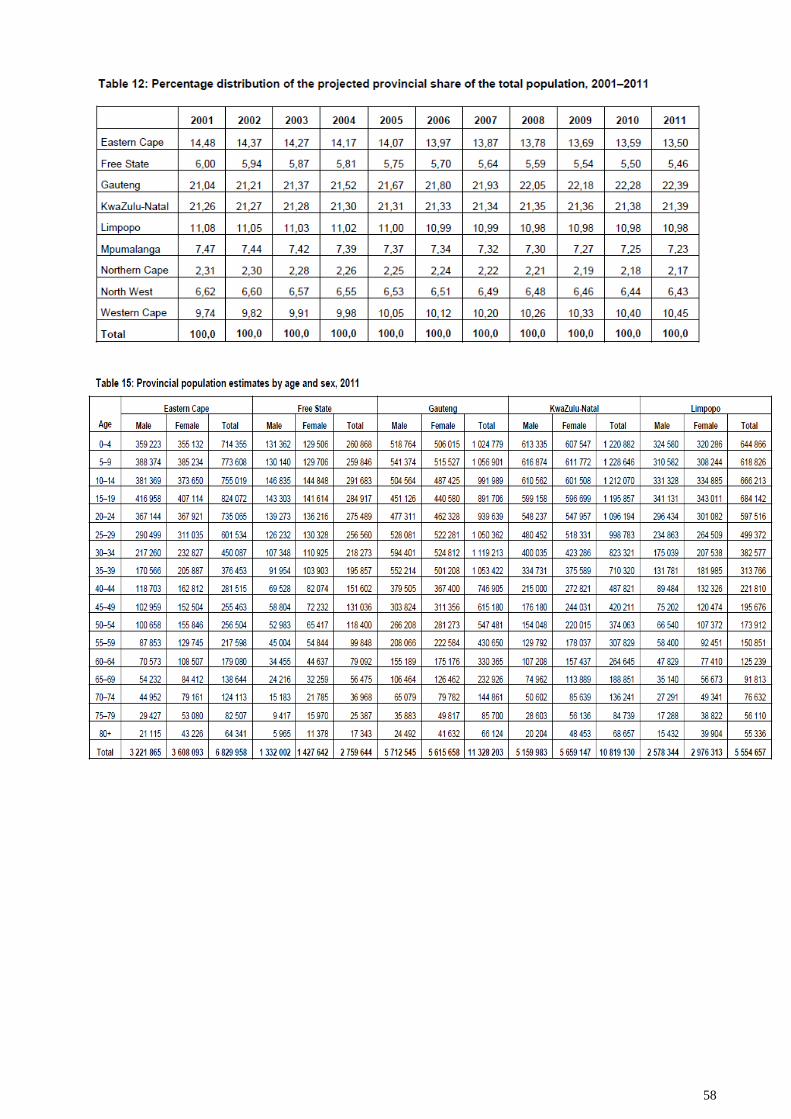
58
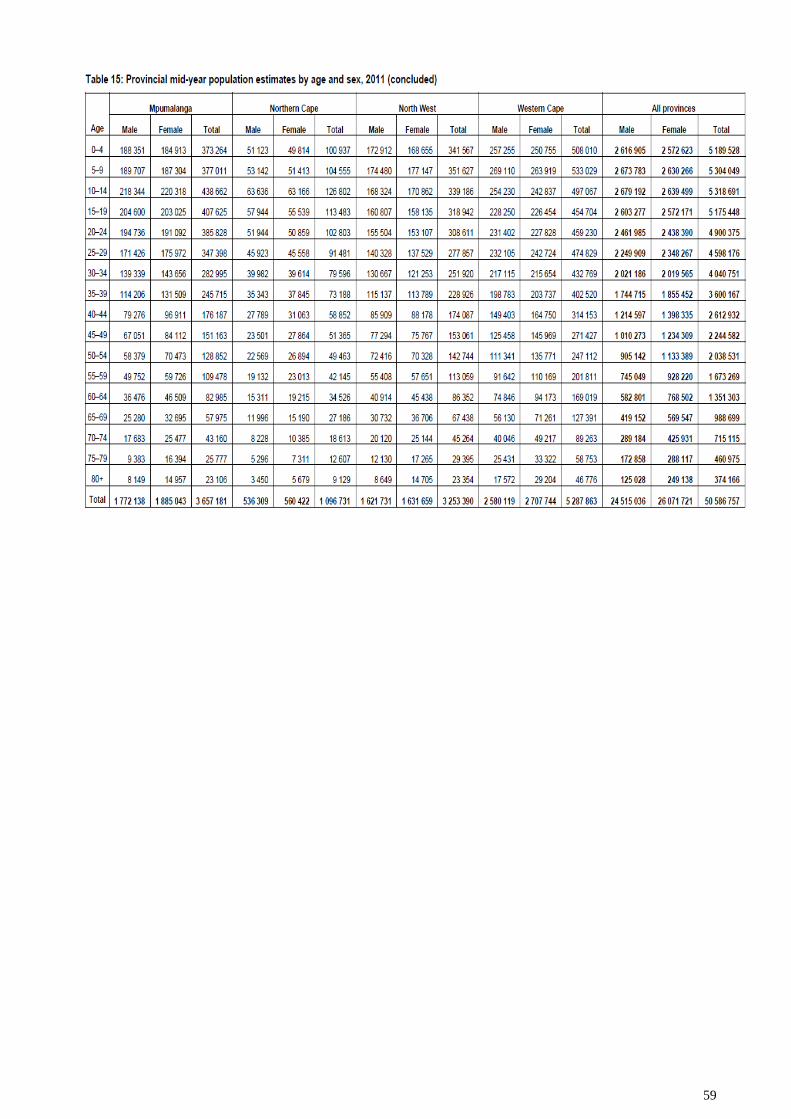
59
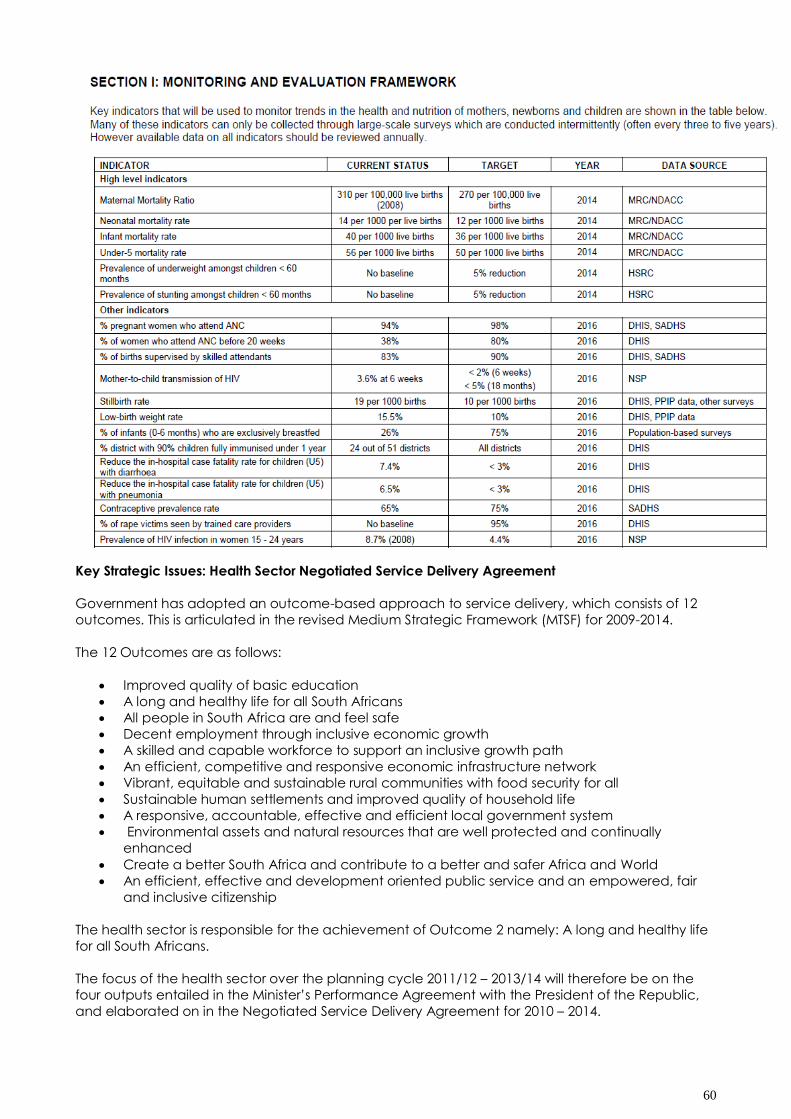
60
Key Strategic Issues: Health Sector Negotiated Service Delivery Agreement
Government has adopted an outcome-based approach to service delivery, which consists of 12
outcomes. This is articulated in the revised Medium Strategic Framework (MTSF) for 2009-2014.
The 12 Outcomes are as follows:
Improved quality of basic education
A long and healthy life for all South Africans
All people in South Africa are and feel safe
Decent employment through inclusive economic growth
A skilled and capable workforce to support an inclusive growth path
An efficient, competitive and responsive economic infrastructure network
Vibrant, equitable and sustainable rural communities with food security for all
Sustainable human settlements and improved quality of household life
A responsive, accountable, effective and efficient local government system
Environmental assets and natural resources that are well protected and continually
enhanced
Create a better South Africa and contribute to a better and safer Africa and World
An efficient, effective and development oriented public service and an empowered, fair
and inclusive citizenship
The health sector is responsible for the achievement of Outcome 2 namely: A long and healthy life
for all South Africans.
The focus of the health sector over the planning cycle 2011/12 – 2013/14 will therefore be on the
four outputs entailed in the Minister‟s Performance Agreement with the President of the Republic,
and elaborated on in the Negotiated Service Delivery Agreement for 2010 – 2014.
61
These are (1) Increasing Life Expectancy; (2) Reducing Maternal and Child Mortality Rates; (3)
Combating HIV and AIDS and decreasing the burden of diseases from Tuberculosis and (4)
Strengthening Health System Effectiveness. Strategies for achieving these are reflected in the
relevant medium term plans of the National and Provincial Departments of Health.
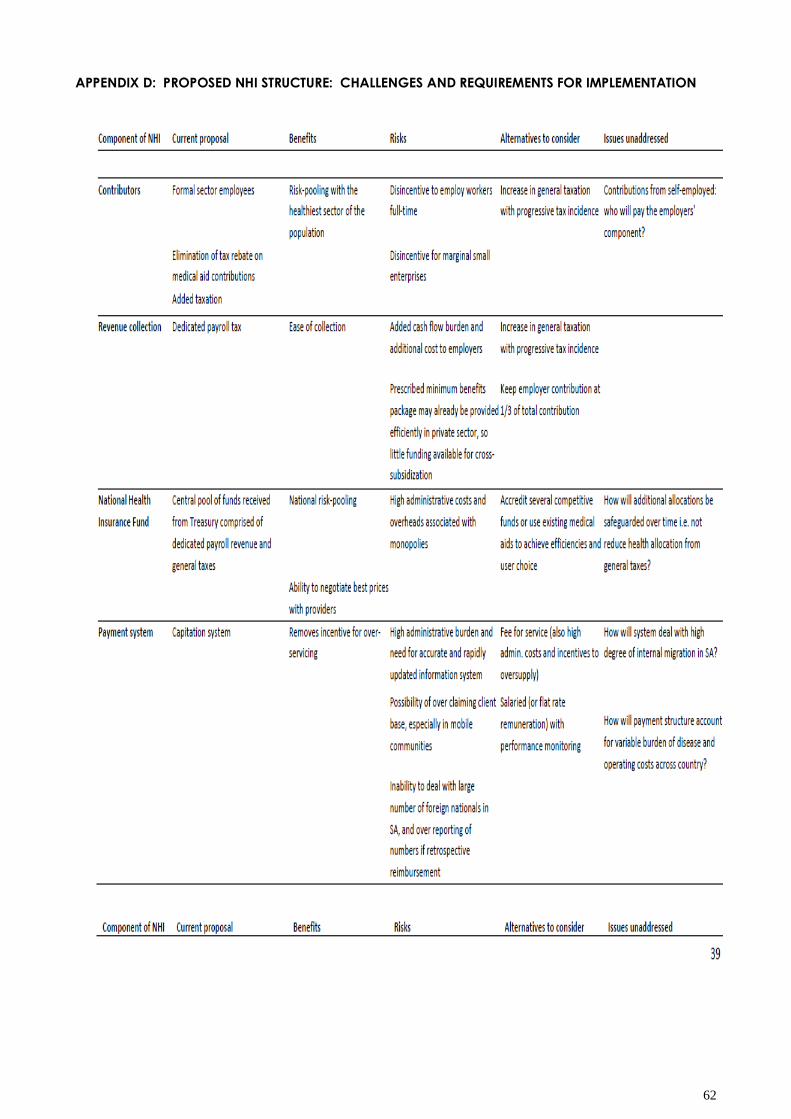
62
APPENDIX D: PROPOSED NHI STRUCTURE: CHALLENGES AND REQUIREMENTS FOR IMPLEMENTATION
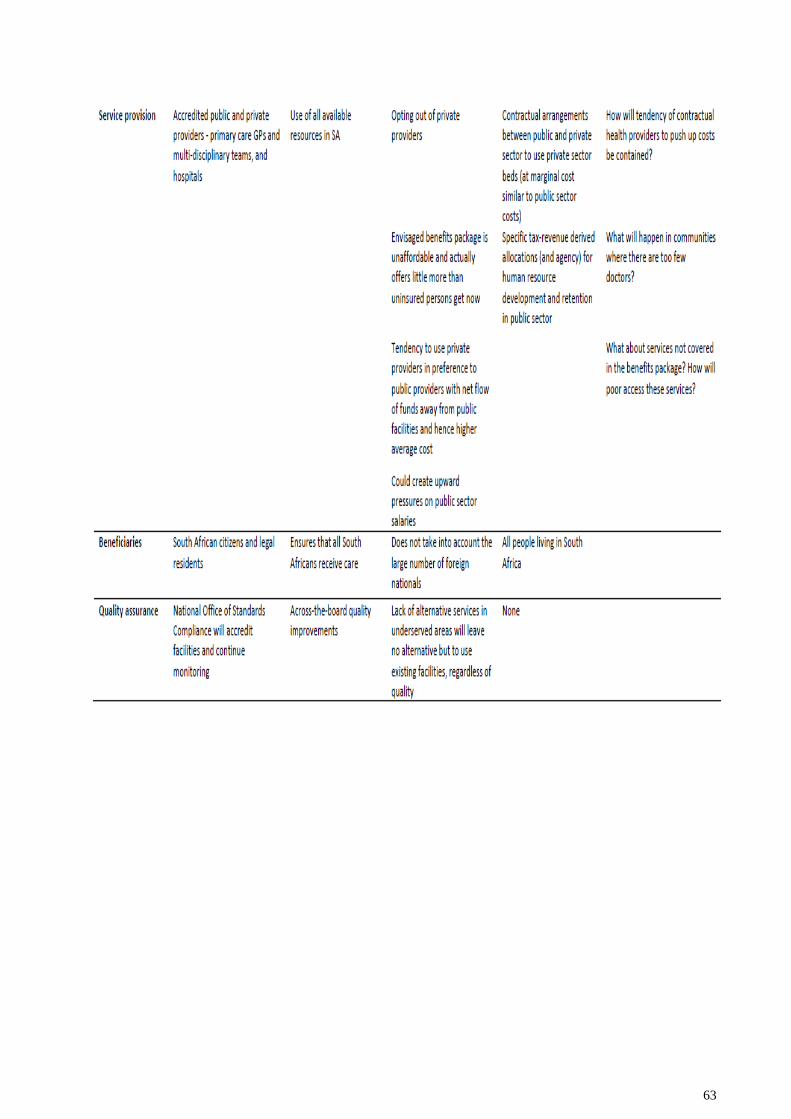
63
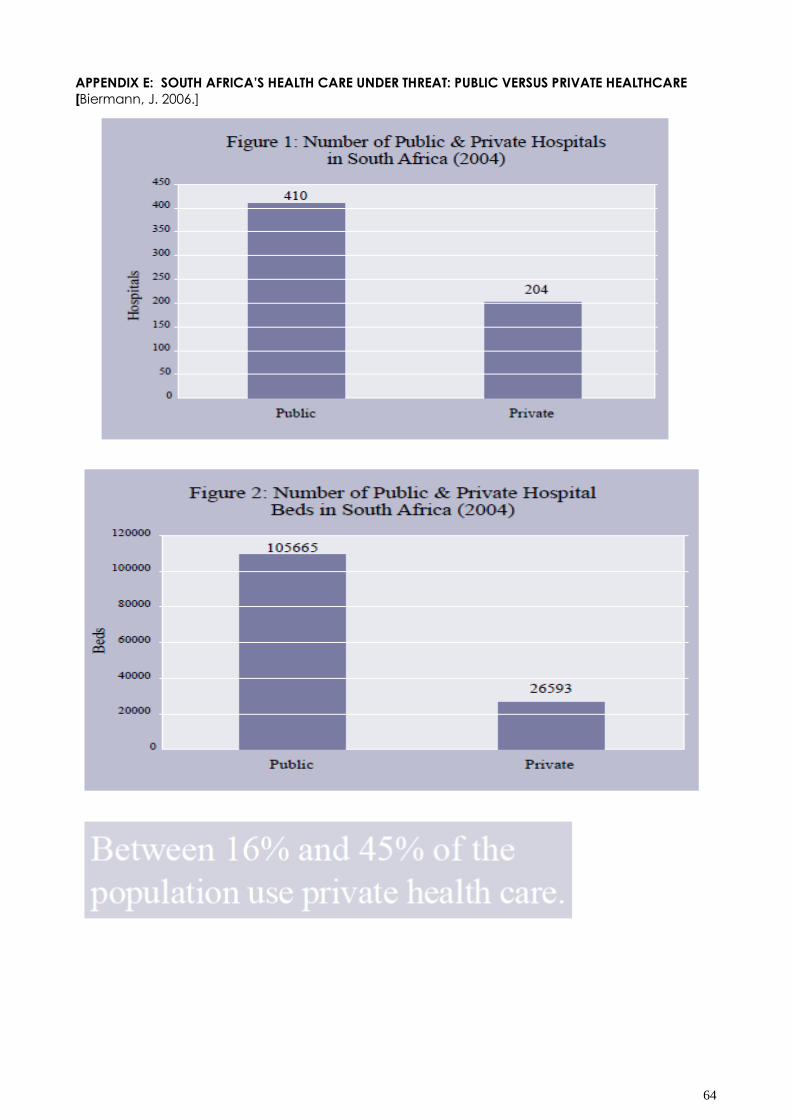
64
APPENDIX E: SOUTH AFRICA‟S HEALTH CARE UNDER THREAT: PUBLIC VERSUS PRIVATE HEALTHCARE
[Biermann, J. 2006.]
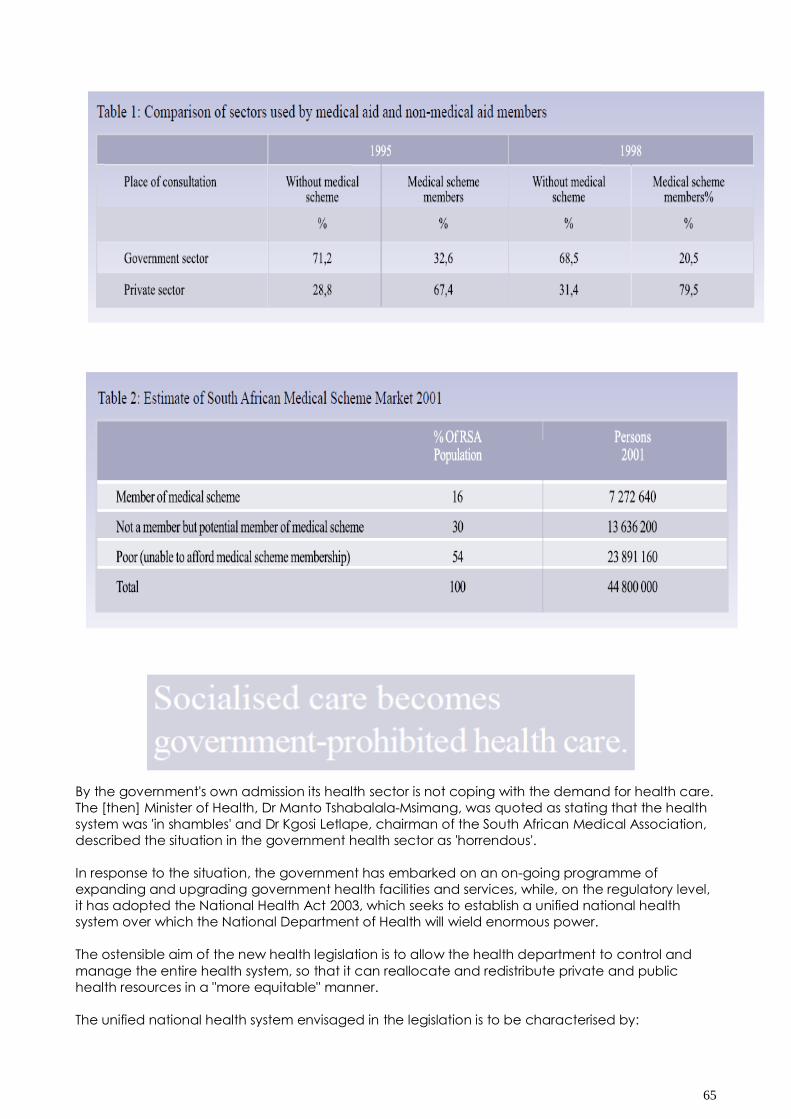
65
By the government's own admission its health sector is not coping with the demand for health care.
The [then] Minister of Health, Dr Manto Tshabalala-Msimang, was quoted as stating that the health
system was 'in shambles' and Dr Kgosi Letlape, chairman of the South African Medical Association,
described the situation in the government health sector as 'horrendous'.
In response to the situation, the government has embarked on an on-going programme of
expanding and upgrading government health facilities and services, while, on the regulatory level,
it has adopted the National Health Act 2003, which seeks to establish a unified national health
system over which the National Department of Health will wield enormous power.
The ostensible aim of the new health legislation is to allow the health department to control and
manage the entire health system, so that it can reallocate and redistribute private and public
health resources in a "more equitable" manner.
The unified national health system envisaged in the legislation is to be characterised by:
66
Planning interventions in the form of national, provincial and district health plans.
Economic interventions in the form of price controls, compulsory minimum benefit
requirements for medical schemes, limitations on risk rating of patients by medical schemes,
prohibitions on re-insurance by medical schemes, and the establishment of a system of
social health insurance.
Licensing in the form of certificates of need (CON) requirements for the establishment or
expansion of facilities and the introduction of new technologies, enabling the Minister of
Health to control the number of private hospitals and beds, the location of new hospitals,
where doctors may practise, and the dispensing of medicines by general practitioners.
Compulsory public service for medical graduates, prescribed medical education curricula
emphasising primary health care over specialist care, prohibition of insurance policies that
cover medical expenses, compulsory acceptance of members by medical aid funds,
compulsory membership of medical aid schemes and limitations on medical aid funds and
insurers, restricting their ability to introduce innovative and more cost-effective services.
The Act introduces South Africa's own version of a centrally planned, socialised health
system, in which the facilities, the equipment, the doctors, nurses and other medical
professionals, and services, whether in the public or private sector, have been regulated,
licensed, certified, approved and price-controlled by the government.
A Critique of the Recent Legislation
The unified national health system envisaged in the National Health Act 2003 ignores the failures of
the country's existing government health sector and the evidence from other countries with
government (socialist) health systems which shows that these systems are inefficient, expensive,
lack sophisticated medical equipment, have long waiting lists for medical procedures and
appointments with specialists, do not provide equal access to and equal treatment for all citizens,
provide lower quality health care than private systems, control costs by rationing care and medical
technology, and fall far short of attaining their lofty ideals. The experience in the countries that
serve as role models for South Africa's health-care plans, such as the United Kingdom and Canada,
is particularly relevant.
In a fully socialised health system everything is centrally planned, controlled and co-ordinated. The
government owns all the hospitals and medical facilities and government health planners
determine how many hospitals and beds there should be, where they should be located, the type
and quantity of services and medicines that will be available, the salaries health-care professionals
may earn, the amount of money that may be spent on particular procedures and technologies,
the type of equipment that may be installed at hospitals and clinics, and the prices that will be
charged for health-care procedures and medicines.
South Africa's new National Health Act subjects its private health-care providers to the same
controls applied in a socialised health system. Private care, from now on, will thus be private only
insofar as health establishments will be privately owned. The government will be planning the entire
health-care system, with dire consequences for all patients, rich and poor.
A government attempting to plan and/or provide health care to an entire nation is confronted by
the insurmountable obstacles faced by centrally planned and co-ordinated systems: the
impossibility of knowing everything necessary to ensure effective, efficient and equitable delivery of
goods and services, the misallocation of resources that result from the ignoring or obliteration of
signals provided by prices, the complexity of centralised planning, the difficulty of forecasting the
future, and the inefficiency of governments in general.
Centrally prohibited health care
When governments impose plans on their citizens, whatever does not fit in with those plans
becomes illegal. This observation led the economist Murray N Rothbard to remark that a centrally
planned economy is a centrally prohibited economy. Socialised care becomes government
prohibited health care: nothing may be done without prior government approval.

67
So, for example, South African doctors will be prohibited from opening medical practices in areas
that government health-care planners believe are adequately served. The planners will somehow
know exactly where all doctors should practise and what procedures and equipment they should
use in order to meet the needs of all patients.
Government health systems are inefficient
Compared to its private health-care providers, South Africa's government health sector is slow,
unwieldy and inefficient because it is not subject to the discipline entailed in making profits,
avoiding losses, and earning an adequate return on capital invested.
The government sector can always obtain more funds from taxpayers, or, if government health
costs and demands for service get really out of hand, ration health care.
The proponents of government health care regard the economic rationing of health care as
inequitable, but regard rationing of health care by governments as justifiable, notwithstanding the
promises to provide health-care services to all who need them. A health department discussion
document makes this admission:
In the government health-care sector, therefore, it is said to be for reasons of equity that health
services are either limited or not available. However, when economic rationing occurs in the
private health sector the proponents of socialised health care describe such rationing as
inequitable.
Government health systems, like all government activities world-wide, are encumbered by
bureaucratic procedures and are consequently unavoidably inefficient. They cannot compete
with private providers. The contracts awarded to private health-care providers by the British
National Health Service (NHS), which is under severe pressure to speed up the provision of medical
care for the more than one million NHS patients who are on waiting lists for surgical procedures,
provides an illustration of the greater efficiency of private providers.
South African private hospital groups, Netcare and Life Healthcare are among the companies to
whom contracts have been awarded.24 The contracts require the performance of thousands of
medical procedures annually, such as cataract procedures, orthopaedic surgery (including hip
and knee replacements), ambulatory surgical procedures (including arthroscopies), general
surgical procedures, and ear, nose, throat and oral procedures.
Life Healthcare, in a joint venture with Care UK PLC, has been contracted to construct and operate
three Diagnostic Treatment Centres in England, which include consulting rooms, radiology
(including X-ray, CT scanner, MRI and ultrasound), pathology laboratories, theatres, ICU beds,
general beds ,and a rehabilitation gymnasium.
The contracts awarded confirm the superiority of private care over government care as well as the
competency of South African companies in providing world-class medical care. It is unfortunate for
government sector patients that these resources are not being used locally to alleviate the pressure
on the government sector.
The quality of care and the competitive cost of private health care have made South Africa a
destination for medical tourism. Patients come to South Africa from the United Kingdom, where
they are entitled to free health care, and pay for medical treatment out of their own resources to
avoid the long waiting times for medical care in the British National Health Service (NHS).25
The knowledge problem
Proponents of government health systems argue that such systems ensure the optimal and
productive utilisation of the country's health-care resources. Their arguments are based on the
fallacy that there is someone who actually knows how to allocate health-care resources in an
equitable manner and what optimal utilisation of health resources would comprise.
68
However, as explained by Nobel laureate Friedrich Hayek, such a person or organisation cannot
exist. Hayek's writings teach us that government planning cannot achieve the efficiency in the use
of resources which market processes make possible because the knowledge required to do so is
dispersed among thousands or millions of individuals.26
All government enterprises and state controlled economies fall prey to what has become known as
"the knowledge problem" and South Africa is no exception.
In a market economy the task of "fixing" prices is undertaken by hundreds of millions of people
individually keeping track of the relatively few prices they need to know for their own decision-
making.
In a health-care system under political and bureaucratic domination, price controls are invariably
introduced, supposedly to make care affordable and to contain costs.
This obliterates the very price information system that would allow health-care resources to be
utilised most efficiently. By ignoring prices, politicians, health-care planners and policy makers have
no means of knowing what the optimal allocation of health resources should be and the fact that
they are generally driven by non-economic motives makes matters worse.
As a result, health-care delivery becomes a product of political and bureaucratic expediency
rather than a response to real health-care needs.
Equity, efficiency and effective delivery become the casualties of the absence of market prices to
co-ordinate production, supply and delivery of health care to consumers.
This is what South Africa's citizens will face if its health department continues on its current course.

69
The "free health care" myth
Government health policy entitles certain categories of patients, including pregnant women and
children younger than six years of age, to receive "free" general care, while "free" primary health
care is available to every citizen.38
However, the health care is not free. It is provided to patients at the expense of the taxpayer.
The day after Nelson Mandela, during his presidency, announced that "all pregnant women and
children under the age of 6 years" would be entitled to "free" health care; some public hospitals
could not cope with the large number of women and children who arrived on their doorstep
seeking medical care.
The event dramatically demonstrated that if the cost is reduced, especially if it is reduced to zero,
the demand increases exponentially. To cope with this demand, government health-care providers
have no option but to reduce availability or deny health care to patients.
However, the difficulties that arise as a result of the introduction of so-called "free" care are not
limited to rationing - it also means less efficient and more expensive health care.39 A large
bureaucracy is needed to administer a socialised health system, which together with the built in
bureaucratic inefficiencies, add even more to the costs of so-called "free" health care.
To control costs, officials oppose the introduction of advances in medical technology. Advanced
technologies and procedures such as MRI scanners and the implantation of artificial hearts, are a
major threat to their budgets.40
"Free" health care is therefore not only, not free, it is expensive, it inevitably denies patients access
to the latest medical procedures and technologies, and it is not freely accessible.
70
THE ALTERNATIVE
Quality Health Care for All
There are two very different approaches to the problem of ensuring that people have adequate
access to health care.
One approach is for the government to attempt to gradually nationalise all health-care services,
ultimately ending with fully taxpayer-funded state-owned health services. This is the apparent aim
of the National Health Act of 2003 and also of the recently proposed "Health Charter".
But economics and world experience tell us that nationalised health care does not work, for three
major reasons. The first is that national health systems do not respond to the day-to-day decisions of
consumers and therefore fail totally to supply their needs. The second is that they invite unlimited
demand, which cannot be met with limited resources. The third is that a relatively poor South Africa
cannot hope to achieve success at implementing a system that some of the wealthiest countries,
such as the United Kingdom and Canada, have for decades been trying vainly to make succeed.
The other approach is to establish a health-care environment in which private health-care funding
and provision can grow rapidly, serving an increasing percentage of the population to the point
where all health services are privately provided. This option will work, as the quality and efficiency
of the existing private health-care providers have ably demonstrated, as long as they are not
burdened with government demands that detrimentally affect their efficiency.
Whichever approach is chosen, one aspect will not change, one hundred per cent of the funding
will be from private sources, firstly through taxes, and secondly through voluntary medical aid or
insurance schemes and voluntary out-of-pocket payments.
Citizens have the right to expect that the taxes they pay to fund the health care of the poor will be
used in a cost effective, efficient and equitable manner. They can rightly demand that
government health policy be conducive to the continued growth and development of private
healthcare.
South Africa's health-care challenge will be best met if government exchanges its role in health-
care provision for that of funder of health care for the poor, purchasing care from competing
private health-care providers.
The most effective mechanism to achieve the empowerment of the poor is to provide them with
resources to purchase health care directly from service providers of their choice.
The implications for health-care reform are that government should:
Refrain from unnecessarily interfering with and micromanaging private health-care provision
and encourage those who can afford to pay for their own health care to do so.
Direct its resources to ensuring that the poor receive adequate care from providers of their
own choice.
Fund the needy directly through appropriate means such as vouchers, smart cards, or
contributions on their behalf to competing medical aid funds, to allow poor patients to
purchase quality health care.
Encourage the development of health-care insurance products for the emerging market.20
Remove controls that increase health-care costs or prevent the provision of care by
scrapping all requirements for certificates of need, price controls, compulsory community
service, registration requirements for medicines already approved in the European Union,
the United States, Canada, Australia and New Zealand, and such other countries that meet
certain defined standards.
Implementing the above measures would relieve government of the burden of providing health
care and would enable it to put substantial financial resources directly in the hands of those who
need them most. The essence of the reform programme would be to maximise the role of the
private health sector and for government to relieve itself of the liability of providing health care.
71
The main beneficiaries of such a reform programme would be the poor, who would be given a
wide range of healthcare choices. Benefits to the taxpayers would be a more efficient use of
taxpayer funds and certainty that tax monies earmarked for funding health care for the poor
reaches them directly so that poor South Africans would get more and better health care for the
same or less money.
State assistance to those who should be self-supporting would be eliminated, allowing greater
assistance to those who really need it. A further benefit is that over time, those people who prosper
sufficiently to take care of their own health care would be removed from the health-care support
list.
The government would have responsibility for a thriving, growing, health-care sector that would be
the envy of the developing and the developed world. Health professionals would start returning to
South Africa instead of leaving.21
Government's policy and discussion documents do not explain how South Africa, a relatively poor
country, will succeed in providing equitable health care to all through the envisaged national
health system, when wealthy countries have failed in their attempts to do this.
If government's health-care plans continue in the direction of nationalisation, which appears to be
the ultimate goal, South Africans will lose their world-class private healthcare firms. Patients will lose
the freedom to choose their own health care, which is such a vital and personal service, and
bureaucratic health-care planners will be making decisions for them. This happens in Canada, the
United Kingdom and other countries that have national health systems.
The whole national health system will function badly, just as it does in those countries.
The health of the whole South African nation is threatened by the centrally planned health system
envisaged in the Health Act 2003.
activities are so
72
APPENDIX F: WESTERN CAPE DEPARTMENT OF HEALTH: ANNUAL PERFORMANCE PLAN 2012-2013:
EXCERPTS AND SITUATIONAL ANALYSIS
Western Cape Government‟s role is to make the vision of an open opportunity society for all an
everyday reality. This we cannot achieve alone, but in partnership with each and every citizen, with
civil society, with business and with other institutions and spheres of government. We are better
together.
The Department of Health leads the way on the road to SO4 – Increasing Wellness with the strategic
plan based on patient-centeredness, a move towards an outcomes-based approach, the
retention of a primary healthcare philosophy, strengthening the district health services model, and
building strategic partnerships.
The key service delivery priorities in this year‟s annual performance plan include:
· Focusing on quality of care initiatives
· The long-awaited commissioning of the Khayelitsha District Hospital
· Commissioning the Mitchells Plain District Hospital
· Implementing a saving-mothers-and-children plan
· Implementing the integrated TB/HIV plan
· Rolling out key prevention strategies in communities with relevant stakeholders
· Strengthening general specialist service and training
A particular focal point is Healthcare 2020, the Department‟s strategic vision and comprehensive
service plan leading up to 2020, with client-centred quality care at the core.
Particularly in the eyes of the patient, the patient experience is as important as the outcome of the
treatment, and the respectful treatment of the patient. The Department will put multilevel
interventions in place to address staff behaviour and approach towards patients.
It remains a challenge to achieve these performance targets within limited financial constraints.
2012 is in addition a landmark year as the Department will finalise the 2020 strategic framework,
which will provide a roadmap for public sector health services in the Western Cape for the next
decade.
The 2020 framework builds on the Healthcare 2010 Comprehensive Service Plan (CSP) and yet
heralds some important policy shifts.
2020 continues to strengthen the Primary Health Care philosophy, the District Health Service model
and institutionalises good corporate practices such as operating with the budget and an
unqualified audit.
However, 2020 places emphasis on improving the quality of care and the patient experience. There
is a values-based approach to strengthen commitment of staff towards improving the patient
experience and clinical outcomes. There is also a conceptual shift towards wellness, strengthening
prevention and promotion both within the health service as well as upstream within broader
society.
2012 will be year of challenges and opportunities that calls for a united resolve to focus on
developing the vision for 2020 and to take the first systematic steps in this direction. I am convinced
that the Western Cape Department of Health has the people with skills, dedication and talent to
make this vision a reality.
During 2012 the Department will finalize the 2020 strategy. The principles, vision and values and a
generic approach to planning for the health service platform embodied in the strategy have been
developed and endorsed by a critical mass of senior and middle management within the
Department.
Following approval of the strategic direction for public health services in the Western Cape by the
Provincial Cabinet a discussion document was released in December 2011 for public comment.
73
Staff within the health service as well as external stakeholders such as the universities, organized
labour, the private sector and NPOs will be engaged to build consensus around the strategic
direction of the Department for the next decade.
The draft strategy for 2020 has two main thrusts, as described in the Strategic Objective: Improving
Wellness (SO 4) that forms part of provincial strategic plan.
Firstly, at the heart of the vision of 2020 is a renewed commitment to a caring, quality, patient-
centric health service.
The district health service, supported by all levels and sections of the service is the key vehicle to
deliver this quality health service. The PHC philosophy implies a comprehensive health service
across levels of care and the various sectors allowing for meaningful and active participation by
communities.
The limited resource base compared to the need for health services demands a more focused
approach to improve health outcomes in the most efficient and productive manner possible.
The Department acknowledges that addressing these challenges requires strong partnerships with
a range of role players.
Secondly, there is an important conceptual shift from managing the consequences of the burden
of disease to improving wellness.
Central to this approach is an increased emphasis on prevention and promotion by addressing the
upstream risk factors that impact on health and wellness in the whole of society. The endorsement
at the Western Cape Health Summit held in November 2011 of the Cape Town Declaration on
Wellness by approximately 250 delegates from all sectors of society in the Western Cape was an
important milestone in this regard.
There are six focus areas that have been identified and work is underway to identify, plan and
implement projects in these areas.
A summary of progress has been included in Part A of the APP. These are the promotion of safety
and reduction of injuries, women‟s health, child health, mental health, healthy lifestyles and HIV/TB.
These focus areas are aligned with the Millennium Development Goals (MDG) and the quadruple
burden of disease that afflicts the provincial population.
The Department will embark upon a structured process to engage staff around creating a
heightened values consciousness. The departmental values are caring, competency,
accountability, integrity, responsiveness and respect.
There is increasing international evidence that a values-based approach impacts positively on the
quality of the health service and productivity of the workforce. Annual Barrett‟s values survey results
have and will be used as a basis for this dialogue with staff, which will drive a change management
process in the Department.
The Department‟s strategic goals as outlined in the Annual Performance Plan and the 2020 strategy
are aligned with the goals of the National Service Delivery Agreement of the National Minister as
well as the MDGs.
Improvement in the quality of health services and strengthening the district and primary health
care services are common to both the 2020 strategy and the discussion document on National
Health Insurance. The provincial government while differing with the national government on
certain aspects of the NHI proposals supports the general thrust toward improving the quality of
health services and as outlined in the APP is strengthening general specialist outreach in health
districts and school health services to this end.

74
In 2012/13, it is projected that 16 348 182 patients will be managed at PHC level, 511 367 patients
admitted to the department‟s hospitals, 135 018 patients treated with anti-retroviral therapy,
487 781 patients transported in ambulances, 98 500 babies delivered in the maternity services and
6 909 cataract operations performed.
The aim is to achieve a TB cure rate of 82 per cent, immunization coverage of 95 per cent, reduce
mother to child transmission of the AIDS virus to 1.8 per cent and reduce maternal mortality within
our institutions to 65 per 100 000 live births.
Another important development in 2012 will be the implementation of the new contract for the
Chronic Dispensing Unit (CDU). The service from the CDU will be expanded from the Cape Metro to
cover all areas of the province in a phased manner and ultimately home delivery of medication to
patients who are stable on chronic medication and have a fixed home address.
The overall reduction in real terms of the provincial equitable share of the budget has meant that
additional funds could not be allocated specifically to national priority areas such as school health
services, district specialist teams and community-based services. However, these priorities will be
addressed within the available budget.
It is noteworthy that the Western Cape Department of Health has already progressed some way to
address these priorities over the last two years.
The need for good quality, auditable data to manage a complex health service requires a further
investment of resources. The process to strengthen information management capacity
commenced in 2011 will continue. In addition to the appointment of new staff and further in-house
training will increase the capacity to address shortcomings in the system.
The Primary Health Care Information System (PHCIS) that was developed by the department will be
further rolled out in 2012/13 to cover all the 126 PHC facilities in the province. The increased
automation will also reduce the strain that manual processes exert on the staff, improve the quality
of the data for better management and reduce the audit risk.
The improvement of response times within EMS remains an important priority within the health
service and the envisaged new communication system will seek to augment initiatives in this
regard.
A pharmacy information system is being implemented at hospitals to improve inventory
management and controls.
Baseline quality audits were conducted at all facilities to assess compliance with the set of national
core quality standards in 2011. These findings will be used as the basis to develop quality
improvement plans at institutional level. An initiative to improve the patient experience within PHC
and district hospitals will commence with a focus on reception services, clinical governance and
continuity of care.
In conclusion it can be seen from this executive summary that the Western Cape Department of
Health is making significant progress toward its vision of Quality Health for All. The Department has
taken seriously the Premier‟s call for all departments to contribute to the provincial government‟s
efforts to become the best regional government in the world!
VISION
Quality health for all.
The vision statement is in the process of being reviewed as part of the consultation of the 2020
framework.
75
MISSION
We undertake to provide equitable access to quality health services in partnership with the
relevant stakeholders within a balanced and well managed health system to the people of the
Western Cape and beyond.
VALUES
The core values of the Department are:
1) Caring
2) Competence
3) Accountability
4) Integrity
5) Responsiveness
The Top Management of the Department undertook a 360-degree leadership evaluation to identify
areas that can be improved within their specific sphere of influence. Approximately
350 managers have participated in Barrett Survey Values workshops to create awareness of the
importance of values and their impact on service delivery.
The workshops have orientated senior and middle management to the core values of the
Provincial Government and the Department.
The second annual Barrett Survey was undertaken in July 2011 and was broadened to increase the
depth of engagement around building a values based approach. This process will be further
deepened during the 2012/13 financial year.
STRATEGIC GOALS
The strategic goals of the Western Cape Department of Health are aligned with:
The provincial government‟s vision to increase wellness in the Province.
The Millennium Development Goals [MDGs].
The national government‟s vision for health: “A long and healthy life for all South Africans”, as
reflected in the Negotiated Service Delivery Agreement [NSDA] between the President and the
National Minister of Health.
The wording of the strategic goal titles and statements has been refined. The changes that have
been made are underlined in the table below and included in Annexure A where changes to the
2009/10 five-year Strategic Plan, are recorded. The strategic goals will be substantially reviewed
once the 2020 framework has been adopted in the first half of 2012.
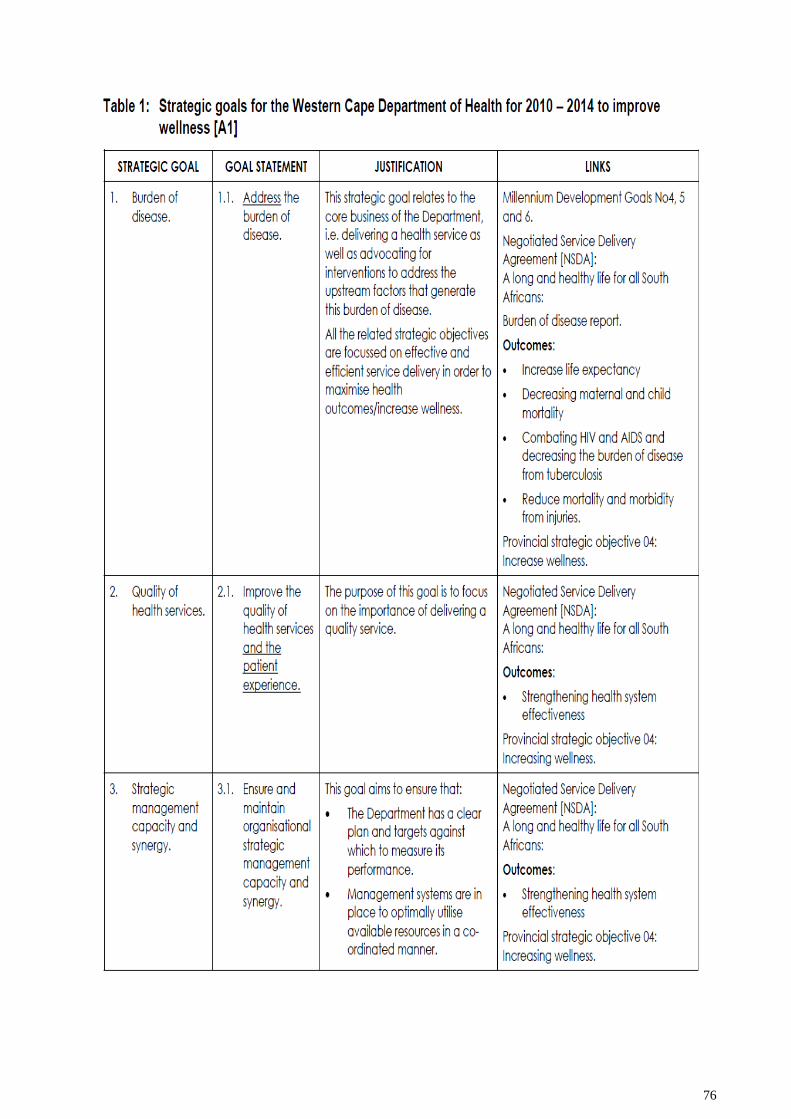
76
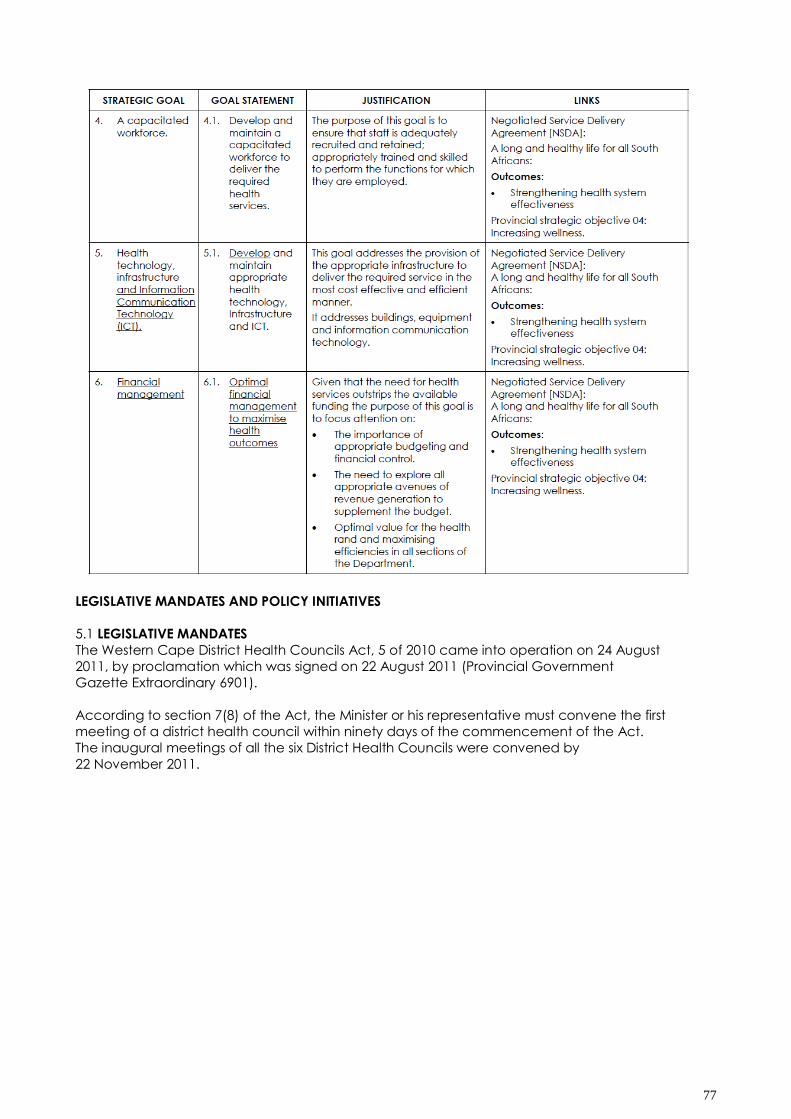
77
LEGISLATIVE MANDATES AND POLICY INITIATIVES
5.1 LEGISLATIVE MANDATES
The Western Cape District Health Councils Act, 5 of 2010 came into operation on 24 August
2011, by proclamation which was signed on 22 August 2011 (Provincial Government
Gazette Extraordinary 6901).
According to section 7(8) of the Act, the Minister or his representative must convene the first
meeting of a district health council within ninety days of the commencement of the Act.
The inaugural meetings of all the six District Health Councils were convened by
22 November 2011.
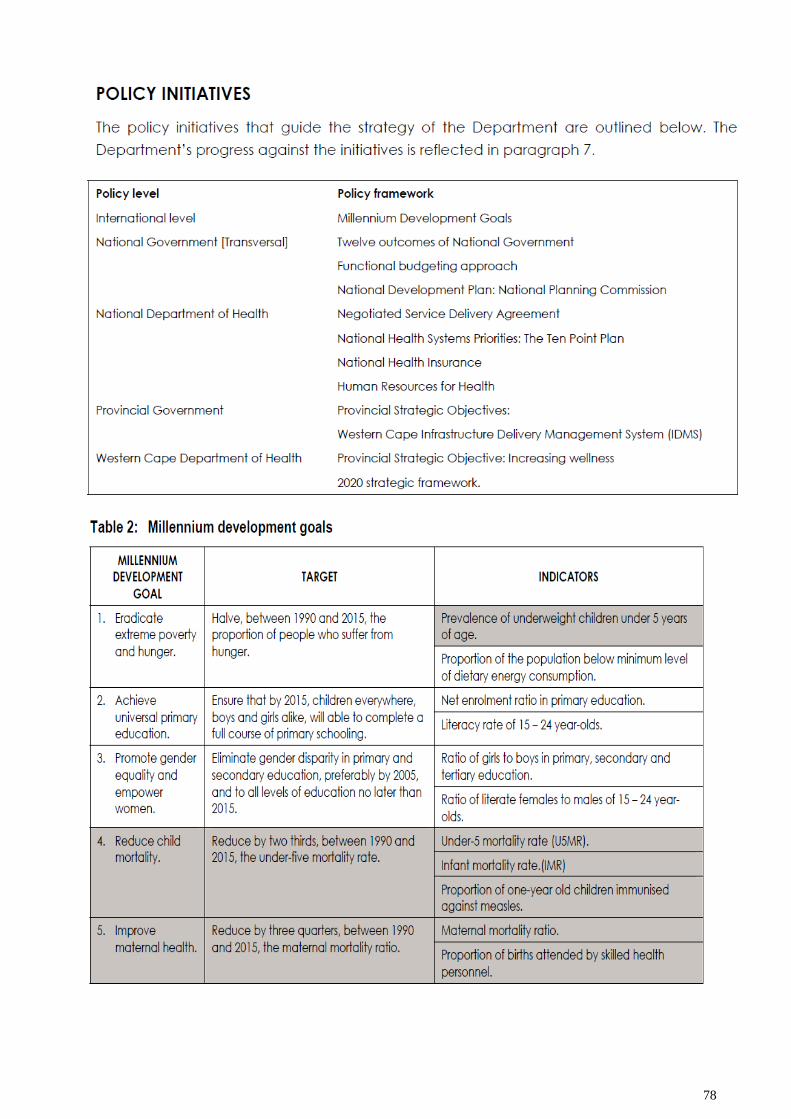
78
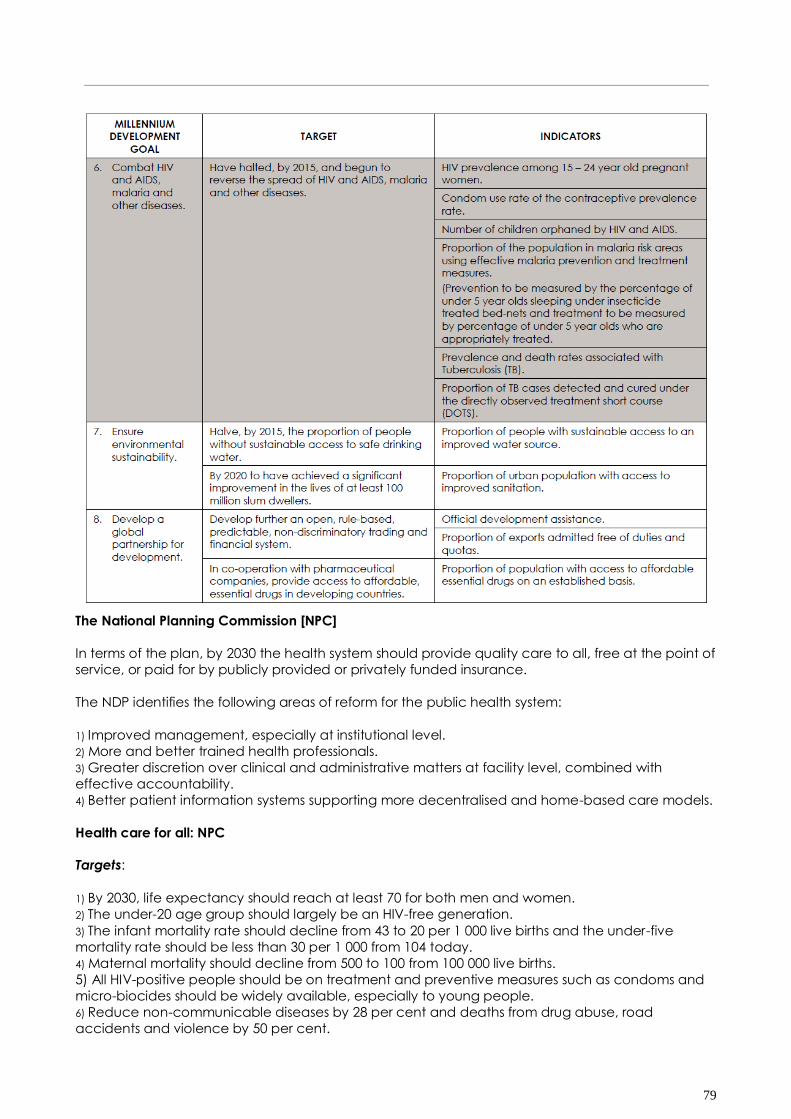
79
The National Planning Commission [NPC]
In terms of the plan, by 2030 the health system should provide quality care to all, free at the point of
service, or paid for by publicly provided or privately funded insurance.
The NDP identifies the following areas of reform for the public health system:
1) Improved management, especially at institutional level.
2) More and better trained health professionals.
3) Greater discretion over clinical and administrative matters at facility level, combined with
effective accountability.
4) Better patient information systems supporting more decentralised and home-based care models.
Health care for all: NPC
Targets:
1) By 2030, life expectancy should reach at least 70 for both men and women.
2) The under-20 age group should largely be an HIV-free generation.
3) The infant mortality rate should decline from 43 to 20 per 1 000 live births and the under-five
mortality rate should be less than 30 per 1 000 from 104 today.
4) Maternal mortality should decline from 500 to 100 from 100 000 live births.
5) All HIV-positive people should be on treatment and preventive measures such as condoms and
micro-biocides should be widely available, especially to young people.
6) Reduce non-communicable diseases by 28 per cent and deaths from drug abuse, road
accidents and violence by 50 per cent.
80
7) Everyone has access to an equal standard of basic health care regardless of their income.
Actions:
1) Address social determinants of health: Promote active lifestyles and balanced diets, control
alcohol abuse and health awareness to reduce non-communicable diseases.
2) Reduce burden of disease to manageable levels: Broaden coverage of anti-retroviral (ARV)
treatment to all HIV-positive people, provide ARVs to high-risk HIV negative people and provide
effective micro-biocides routinely to all women 16 years and older.
3) Build human resources for the health sector of the future:
Accelerate production of community specialists in the five main specialist areas (medicine,
surgery, including anaesthetics, obstetrics, paediatrics and psychiatry)
Recruit, train and deploy between 700 000 and 1.3 million community health workers to
implement community-based health care.
4) Strengthen the national health system: Determine minimum qualifications for hospital managers
and ensure that all managers have the necessary qualifications.
5) Implement national health insurance (NHI):
Implement the scheme in a phased manner, focussing on:
Improving the quality and care at public facilities.
reducing the relative cost of private medical care.
Increasing the number of medical professionals.
Introducing a patient record system and supporting information technology systems.
6.2.3.2 Education
Another focus area of the NDP is improving education, training and innovation. In order to achieve
this, a target has been set to eradicate child under-nutrition and vitamin A deficiency among
children by 2030. By 2030 the feeding schemes in schools should cover all children in need and
provide food that is high in nutritional content.
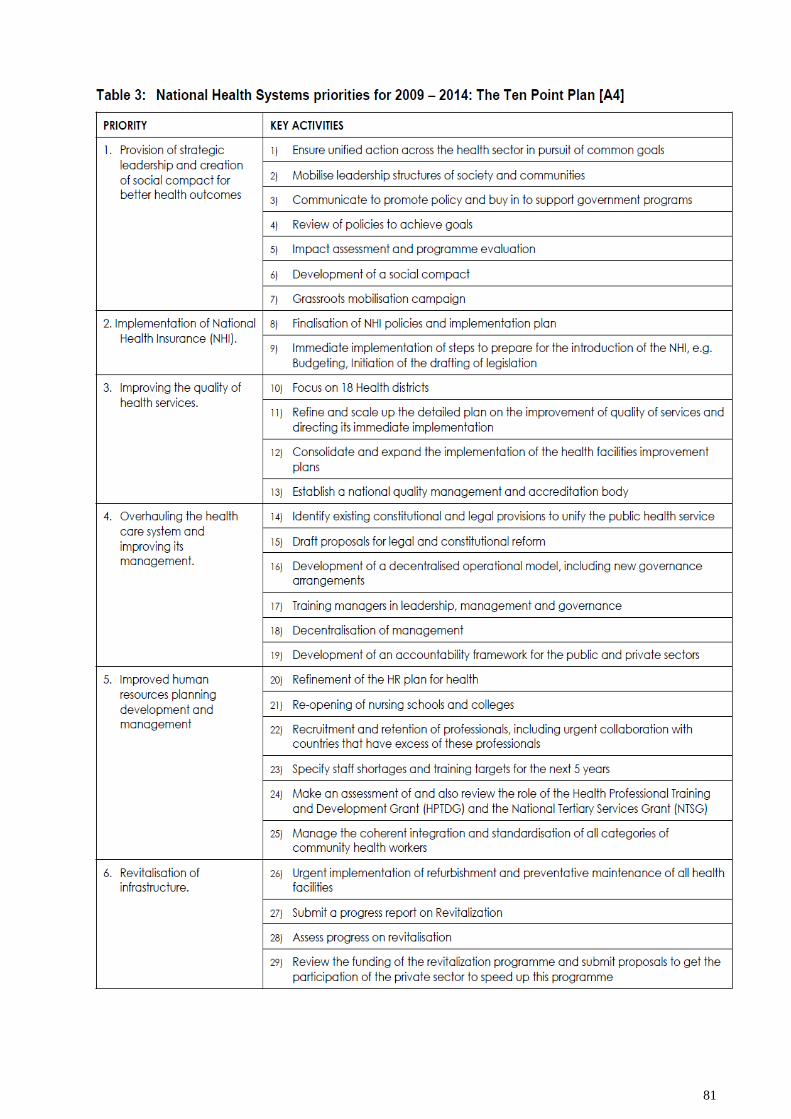
81
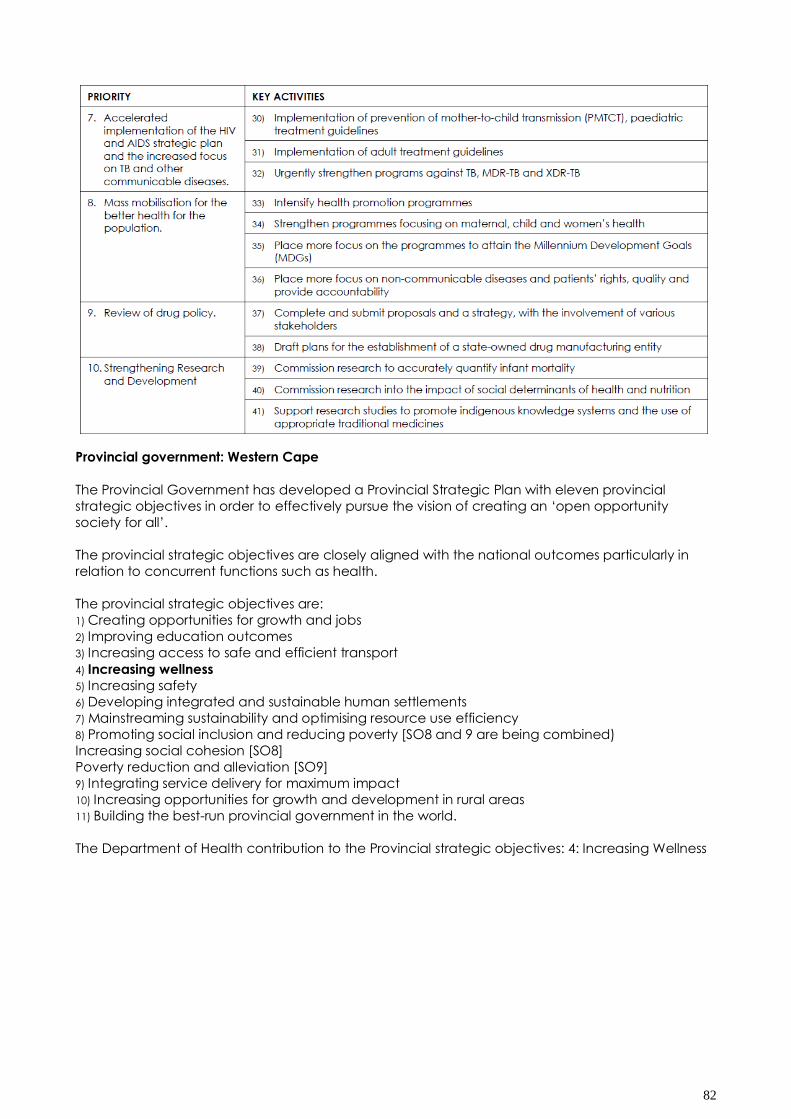
82
Provincial government: Western Cape
The Provincial Government has developed a Provincial Strategic Plan with eleven provincial
strategic objectives in order to effectively pursue the vision of creating an „open opportunity
society for all‟.
The provincial strategic objectives are closely aligned with the national outcomes particularly in
relation to concurrent functions such as health.
The provincial strategic objectives are:
1) Creating opportunities for growth and jobs
2) Improving education outcomes
3) Increasing access to safe and efficient transport
4) Increasing wellness
5) Increasing safety
6) Developing integrated and sustainable human settlements
7) Mainstreaming sustainability and optimising resource use efficiency
8) Promoting social inclusion and reducing poverty [SO8 and 9 are being combined)
Increasing social cohesion [SO8]
Poverty reduction and alleviation [SO9]
9) Integrating service delivery for maximum impact
10) Increasing opportunities for growth and development in rural areas
11) Building the best-run provincial government in the world.
The Department of Health contribution to the Provincial strategic objectives: 4: Increasing Wellness
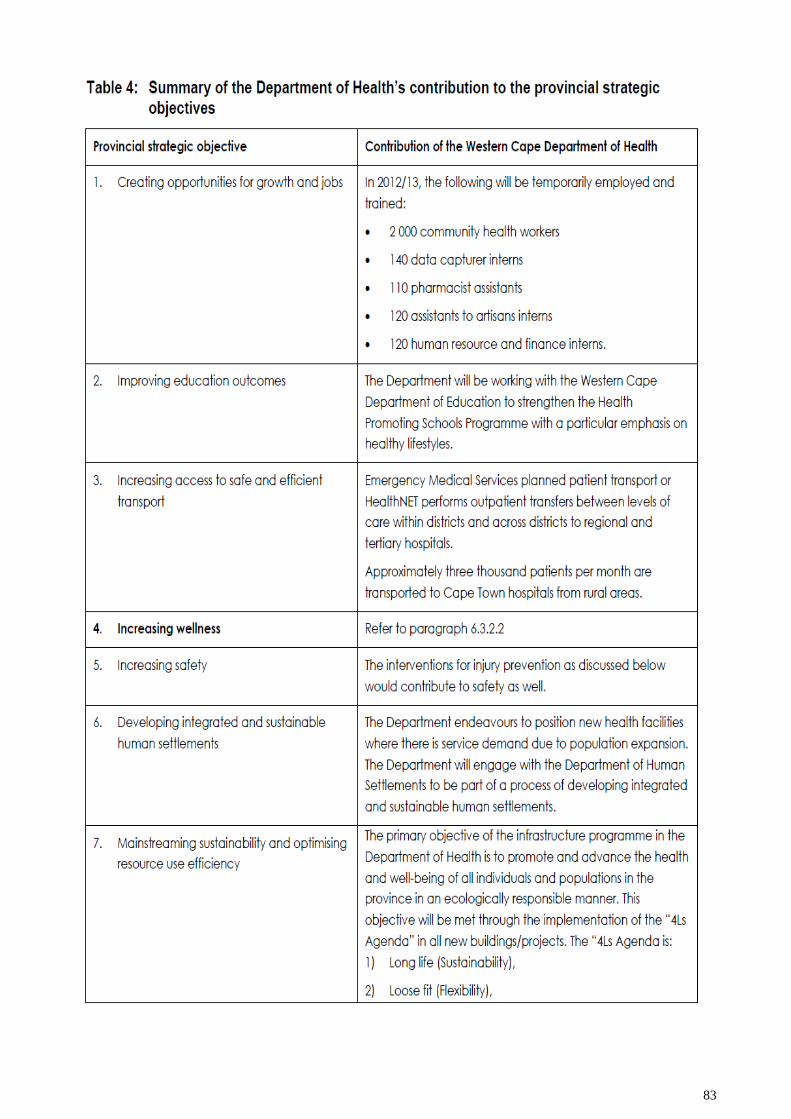
83
84
85
Provincial Transversal Management System [PTMS]
It is well documented that much of the burden of disease that confronts the Department on a daily
basis is caused by upstream factors in society that are outside the mandate of the Department.
The PTMS provides a structured opportunity to mobilise role players outside of health to address
these upstream factors. These factors have been systematically identified in the burden of disease
report undertaken by the Department in partnership with the universities and the Medical Research
Council (MRC).
The Provincial Transversal Management System is a priority of the Western Cape Government
providing political support for effective inter-sectoral collaboration within the provincial
government.
This is informed by the philosophy that acting in a united manner around a common set of
objectives as a “whole of society” and a “whole of government” will promote delivery.
The strategic objectives are clustered into three sectors i.e. human development, economic and
infrastructure, and administration and inter-governmental. Each of the strategic objectives has a
steering group that co-ordinate the working groups within the strategic objective.
In line with the quadruple burden of disease and the MDGs, the Department has formed six
workgroups:
1) Violence and road injuries prevention
2) Healthy lifestyles
3) Women‟s health
4) Maternal and child health
5) Infectious diseases (HIV and TB)
6) Mental Health
86
APPENDIX G: PROVINCIAL STRATEGIC OBJECTIVE 4: INCREASING WELLNESS: WESTERN CAPE
DEPARTMENT OF HEALTH: AN OVERVIEW [Western Cape Department of Health. November 2011.]
87
88
89
90
91
92
93
From a patient‟s perspective the health service is perceived to be a single service regardless of the
component parts and management structures. Similarly from the perspective of stakeholders such
as suppliers who need to be paid for services rendered, the Department is perceived as a single
entity.
A realisation of this challenge led to the adoption of the concept geographic service areas (GSA),
which is a functional arrangement to facilitate better cohesion and coordination of health services
for a defined population within a specified geographic area.
There are six districts in the Western Cape but currently five GSAs:
1) The Cape Town Metro District is divided into Metro West and Metro East GSAs.
2) Central Karoo and Eden are combined into the Eden/Central Karoo GSA.
This has been done to address the difficulty of recruiting and retaining staff and effectively
managing the Central Karoo District, which is a geographically large, sparsely populated area, as
an independent entity.
3) Winelands and Overberg have been combined into a single GSA for operational and logistical
reasons.
4) West Coast:
The boundaries for the West Coast GSA are co-terminous with the districts except in the
Sub-districts of Drakenstein and Stellenbosch which are formally part of the Winelands
District and which fall within the West Coast GSA as patients from these communities are referred to
Paarl Hospital in the West Coast GSA due to the topography and road links.
District managers co-ordinate the services within the GSA, and working closely with the chief
executive officer of the regional hospital, other managers and clinicians within the GSA assume
responsibility for service delivery within that area. The GSAs are functional arrangements to
enhance service delivery and will not impinge on the statutory structures and powers of the districts
and the management teams.
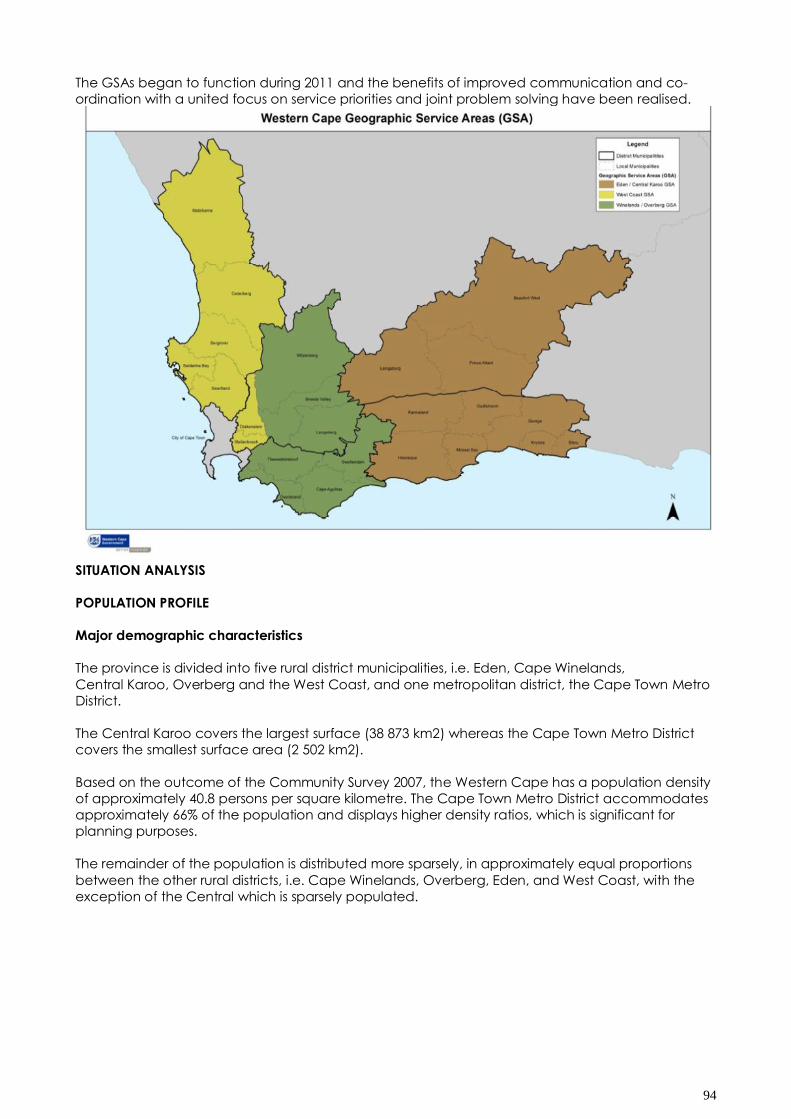
94
The GSAs began to function during 2011 and the benefits of improved communication and co-
ordination with a united focus on service priorities and joint problem solving have been realised.
SITUATION ANALYSIS
POPULATION PROFILE
Major demographic characteristics
The province is divided into five rural district municipalities, i.e. Eden, Cape Winelands,
Central Karoo, Overberg and the West Coast, and one metropolitan district, the Cape Town Metro
District.
The Central Karoo covers the largest surface (38 873 km2) whereas the Cape Town Metro District
covers the smallest surface area (2 502 km2).
Based on the outcome of the Community Survey 2007, the Western Cape has a population density
of approximately 40.8 persons per square kilometre. The Cape Town Metro District accommodates
approximately 66% of the population and displays higher density ratios, which is significant for
planning purposes.
The remainder of the population is distributed more sparsely, in approximately equal proportions
between the other rural districts, i.e. Cape Winelands, Overberg, Eden, and West Coast, with the
exception of the Central which is sparsely populated.
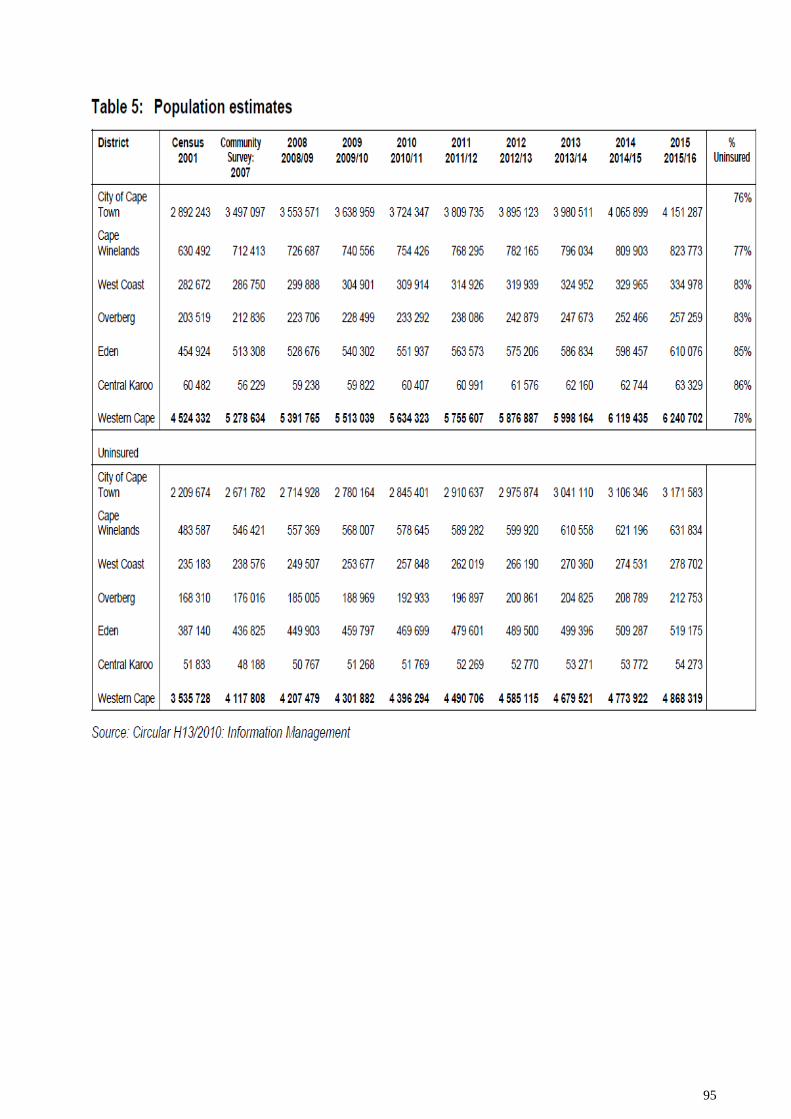
95
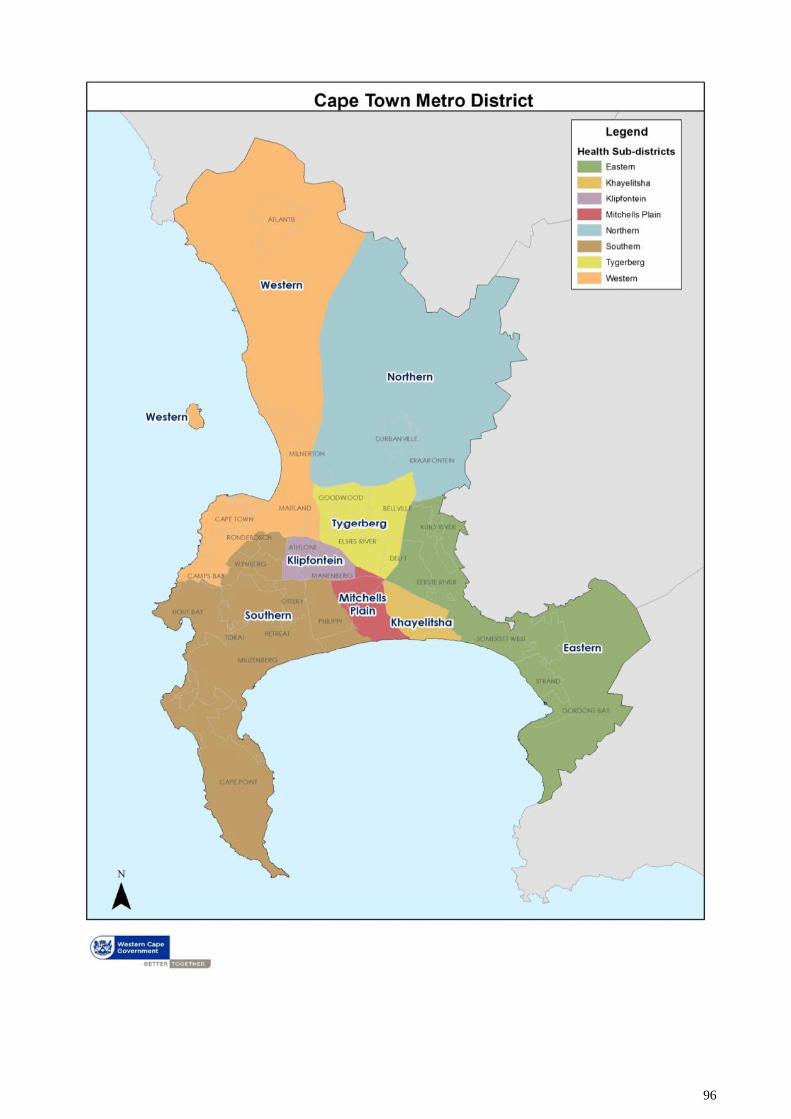
96
97
SOCIO-ECONOMIC PROFILE
Although the South African economy has shown a positive year-on-year growth in real gross
domestic product (GDP) since the first quarter of 2010, the labour market shows no real sign of
recovery.
Nationally the number of unemployed individuals, according to the expanded definition of
unemployment, has grown by nearly 7 per cent per annum since 2008.
In the third quarter of 2011/12 the unemployment rate, in terms of the narrow definition of
unemployment, which does not take discouraged work seekers into account, was 23.3 percent in
the Western Cape against the national rate of 25.0 per cent.
In terms of the broad definition of unemployment the rate in the Western Cape for the same period
was 24.3 percent in comparison to the national rate of 33.3 per cent.
The national patterns of labour market disadvantage are also evident in the provincial labour
market where there are biases in terms of youth, gender, race and level of education. (Medium
Term Budget Policy Statement 2012-2015).
The deprivation index measures the relative deprivation of populations across districts within
South Africa and is derived from a set of demographic and socio-economic variables from the
2007 Community Survey and the 2005 and 2006 General Household Survey.
A high value for the deprivation index denotes higher levels of deprivation. Furthermore, districts
that fall into socio-economic quintile 5 are the least deprived (best off), whereas those that fall into
quintile 1 are most deprived (worst off).
All the districts within the Western Cape are ranked amongst the least deprived in the country
(District Health Barometer 2008/09).
Province-specific deprivation indices (Stats SA) show that the most deprived wards within the
Western Cape are within the City of Cape Town municipality, particularly the townships on the
Cape Flats alongside the N2, and in the Karoo.
The Central Karoo comprises approximately one per cent of the total population. More detailed
analysis also suggests that approximately half of the fifty most deprived wards in the Province are
most deprived in four or more of the following domains: income and material deprivation,
employment deprivation, health deprivation, education deprivation, and living environment
deprivation.
The following Table outlines that poverty and socio-demographic data obtained from the General
Household Survey of 2010.
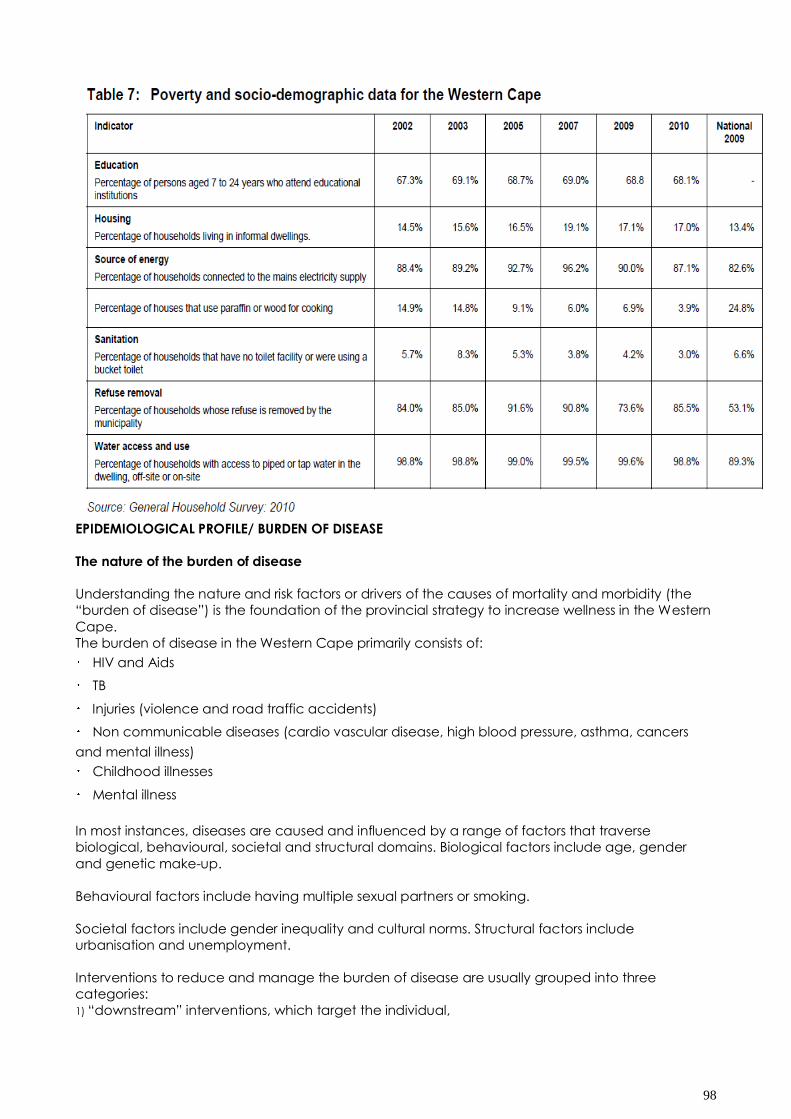
98
EPIDEMIOLOGICAL PROFILE/ BURDEN OF DISEASE
The nature of the burden of disease
Understanding the nature and risk factors or drivers of the causes of mortality and morbidity (the
“burden of disease”) is the foundation of the provincial strategy to increase wellness in the Western
Cape.
The burden of disease in the Western Cape primarily consists of:
HIV and Aids
TB
Injuries (violence and road traffic accidents)
Non communicable diseases (cardio vascular disease, high blood pressure, asthma, cancers
and mental illness)
Childhood illnesses
Mental illness
In most instances, diseases are caused and influenced by a range of factors that traverse
biological, behavioural, societal and structural domains. Biological factors include age, gender
and genetic make-up.
Behavioural factors include having multiple sexual partners or smoking.
Societal factors include gender inequality and cultural norms. Structural factors include
urbanisation and unemployment.
Interventions to reduce and manage the burden of disease are usually grouped into three
categories:
1) “downstream” interventions, which target the individual,
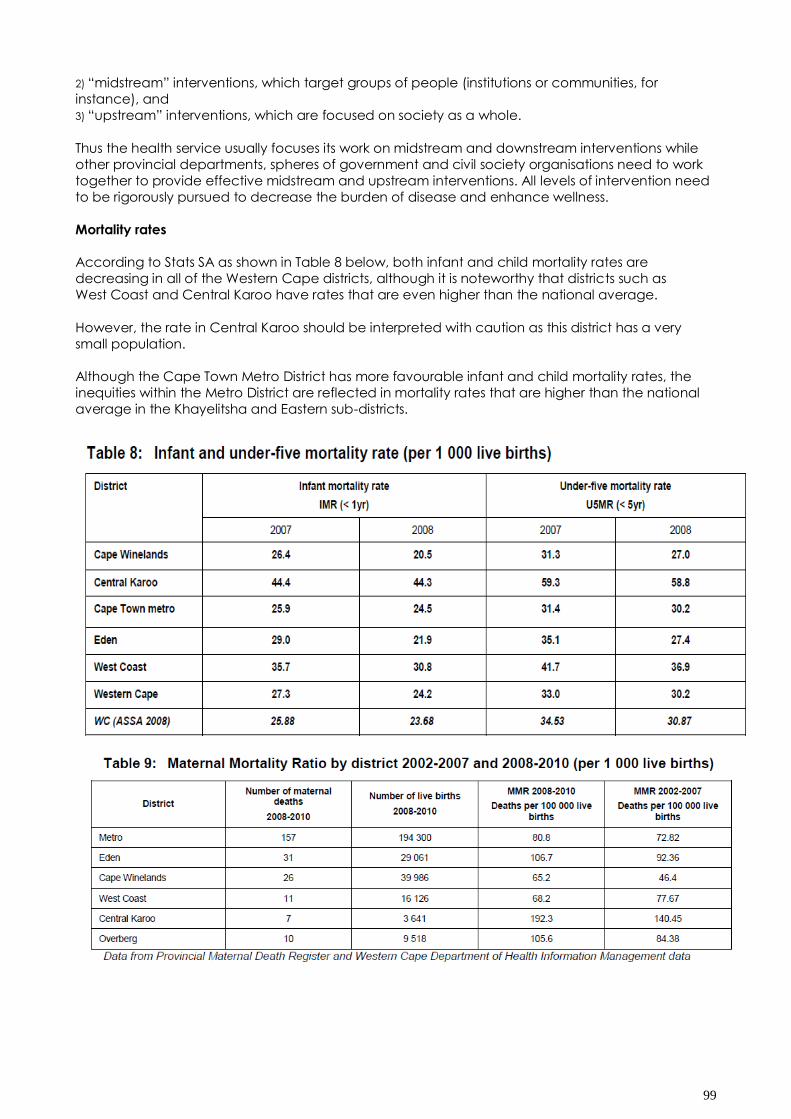
99
2) “midstream” interventions, which target groups of people (institutions or communities, for
instance), and
3) “upstream” interventions, which are focused on society as a whole.
Thus the health service usually focuses its work on midstream and downstream interventions while
other provincial departments, spheres of government and civil society organisations need to work
together to provide effective midstream and upstream interventions. All levels of intervention need
to be rigorously pursued to decrease the burden of disease and enhance wellness.
Mortality rates
According to Stats SA as shown in Table 8 below, both infant and child mortality rates are
decreasing in all of the Western Cape districts, although it is noteworthy that districts such as
West Coast and Central Karoo have rates that are even higher than the national average.
However, the rate in Central Karoo should be interpreted with caution as this district has a very
small population.
Although the Cape Town Metro District has more favourable infant and child mortality rates, the
inequities within the Metro District are reflected in mortality rates that are higher than the national
average in the Khayelitsha and Eastern sub-districts.
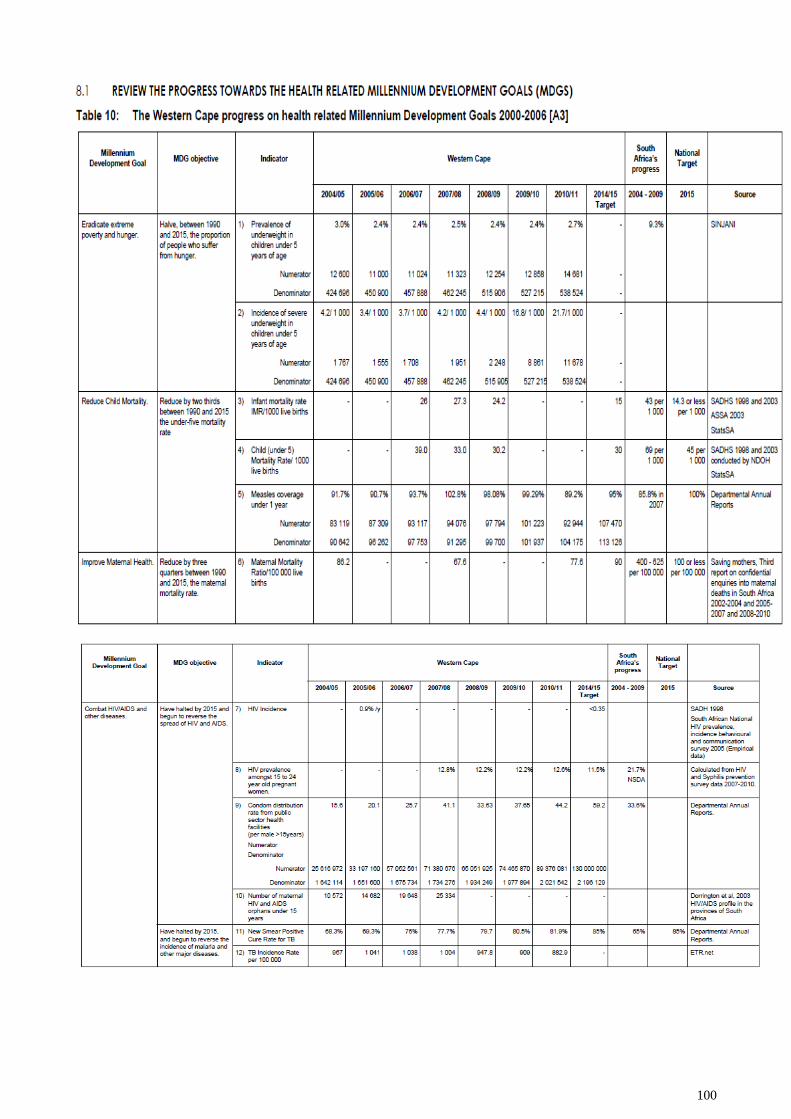
100
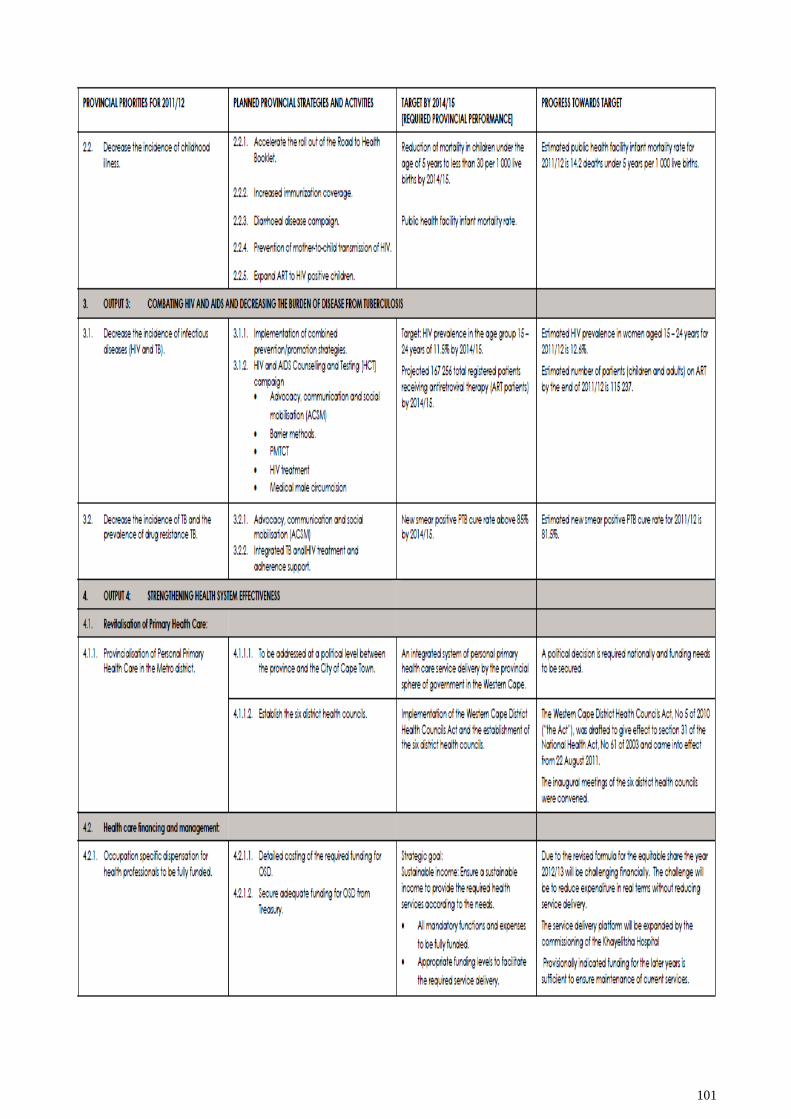
101
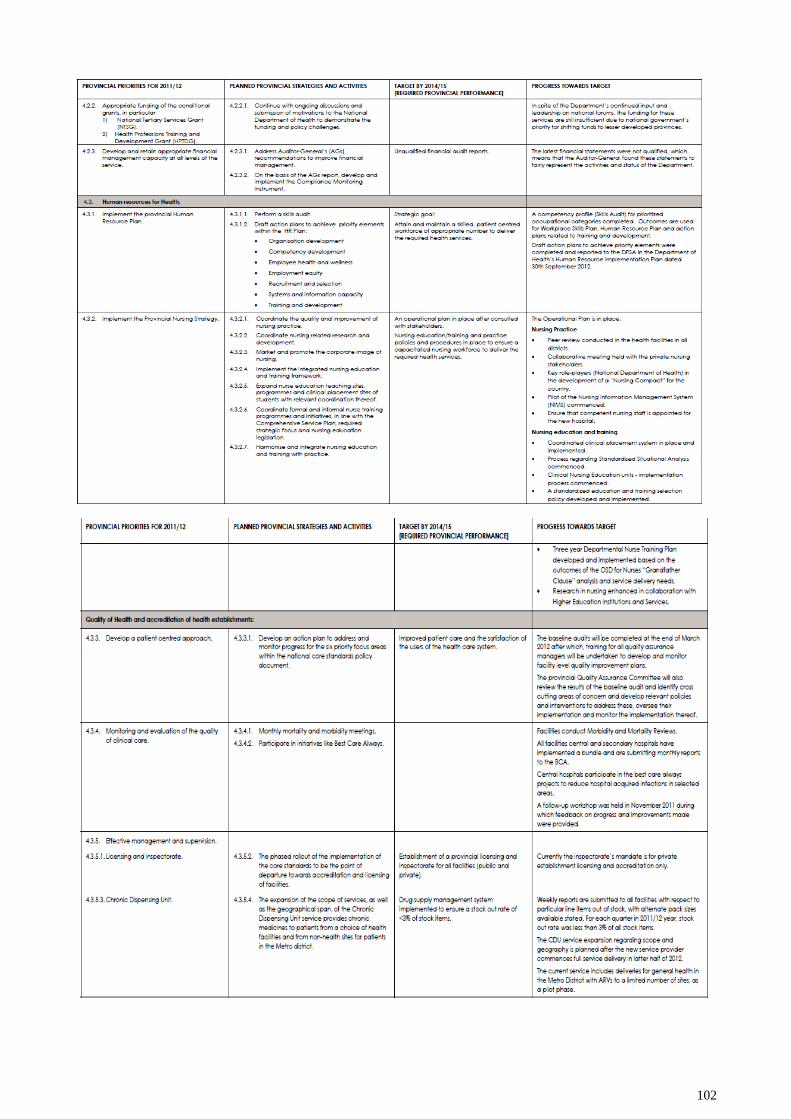
102
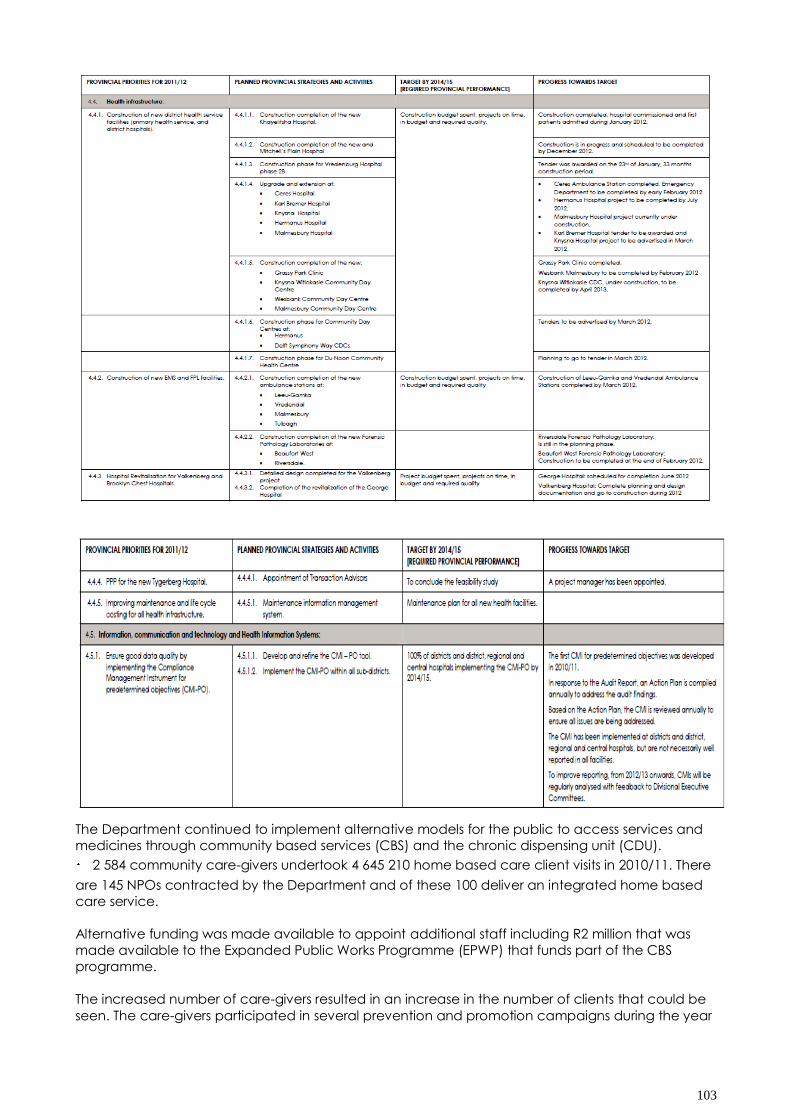
103
The Department continued to implement alternative models for the public to access services and
medicines through community based services (CBS) and the chronic dispensing unit (CDU).
2 584 community care-givers undertook 4 645 210 home based care client visits in 2010/11. There
are 145 NPOs contracted by the Department and of these 100 deliver an integrated home based
care service.
Alternative funding was made available to appoint additional staff including R2 million that was
made available to the Expanded Public Works Programme (EPWP) that funds part of the CBS
programme.
The increased number of care-givers resulted in an increase in the number of clients that could be
seen. The care-givers participated in several prevention and promotion campaigns during the year
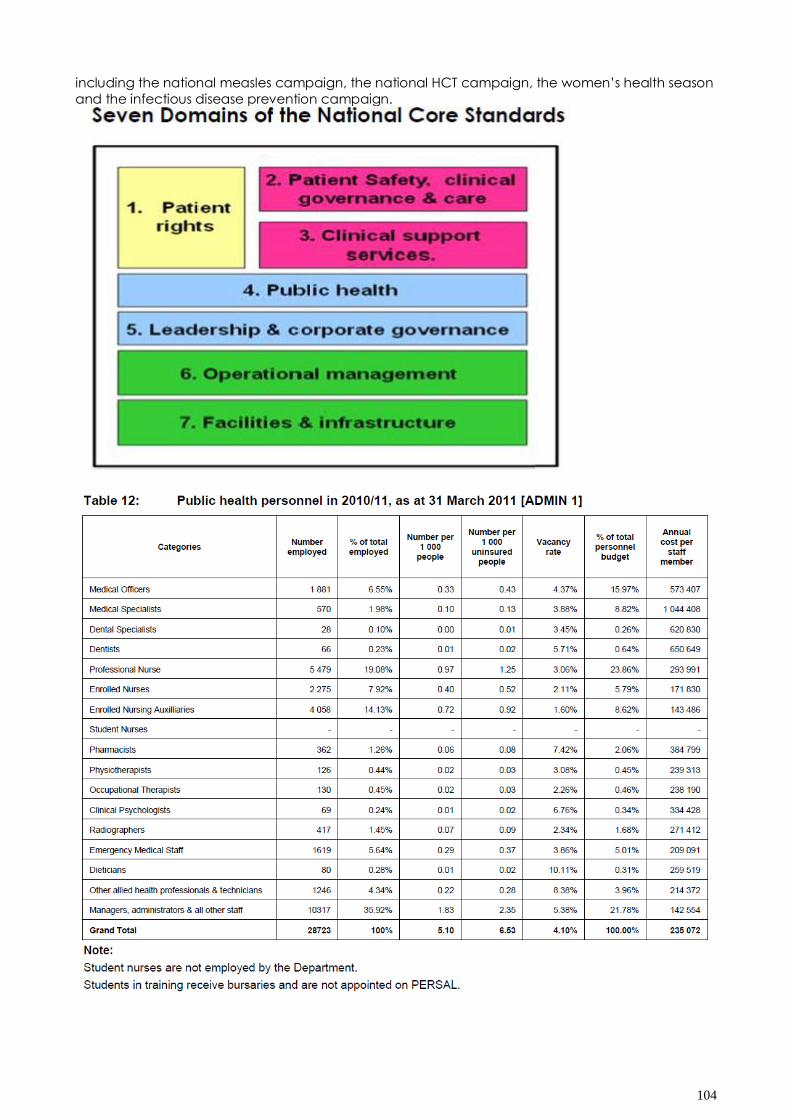
104
including the national measles campaign, the national HCT campaign, the women‟s health season
and the infectious disease prevention campaign.
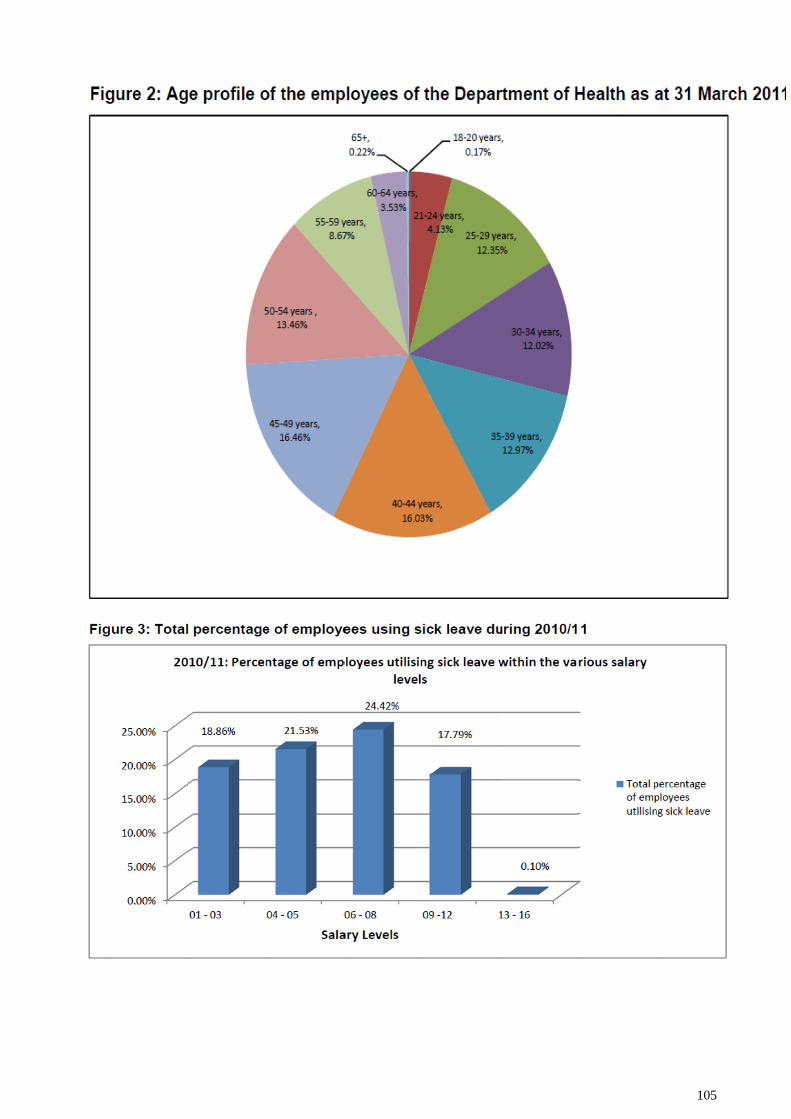
105
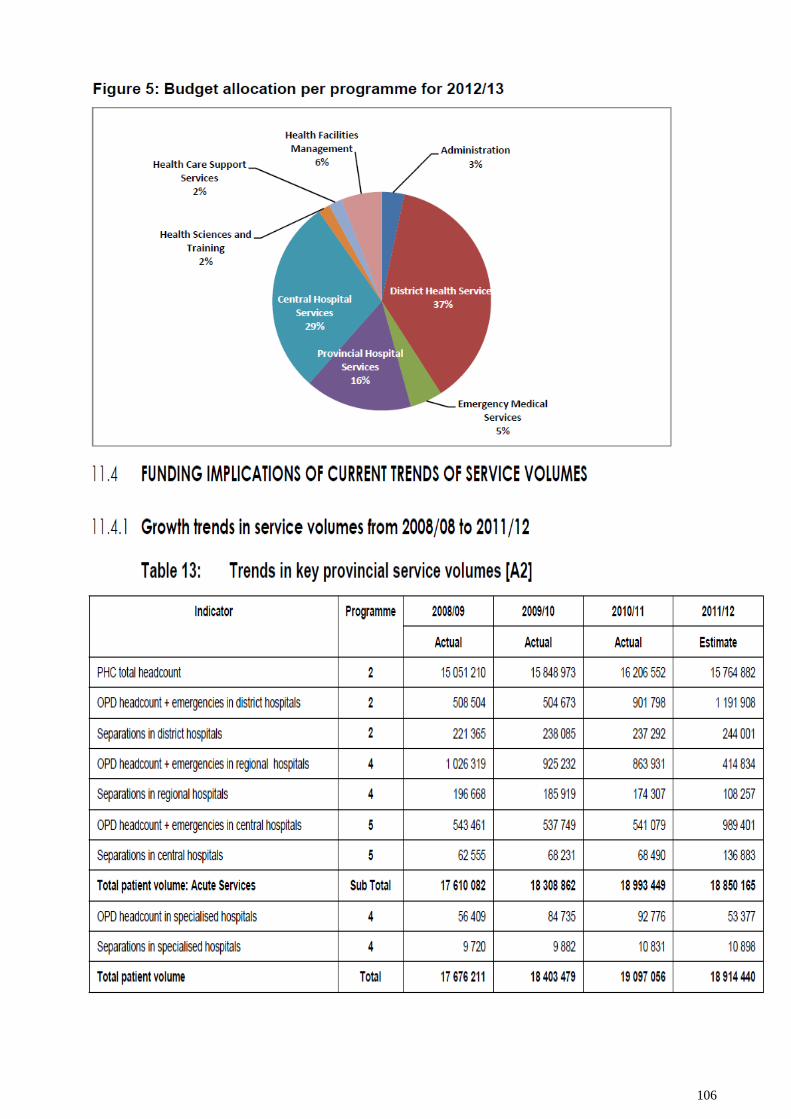
106
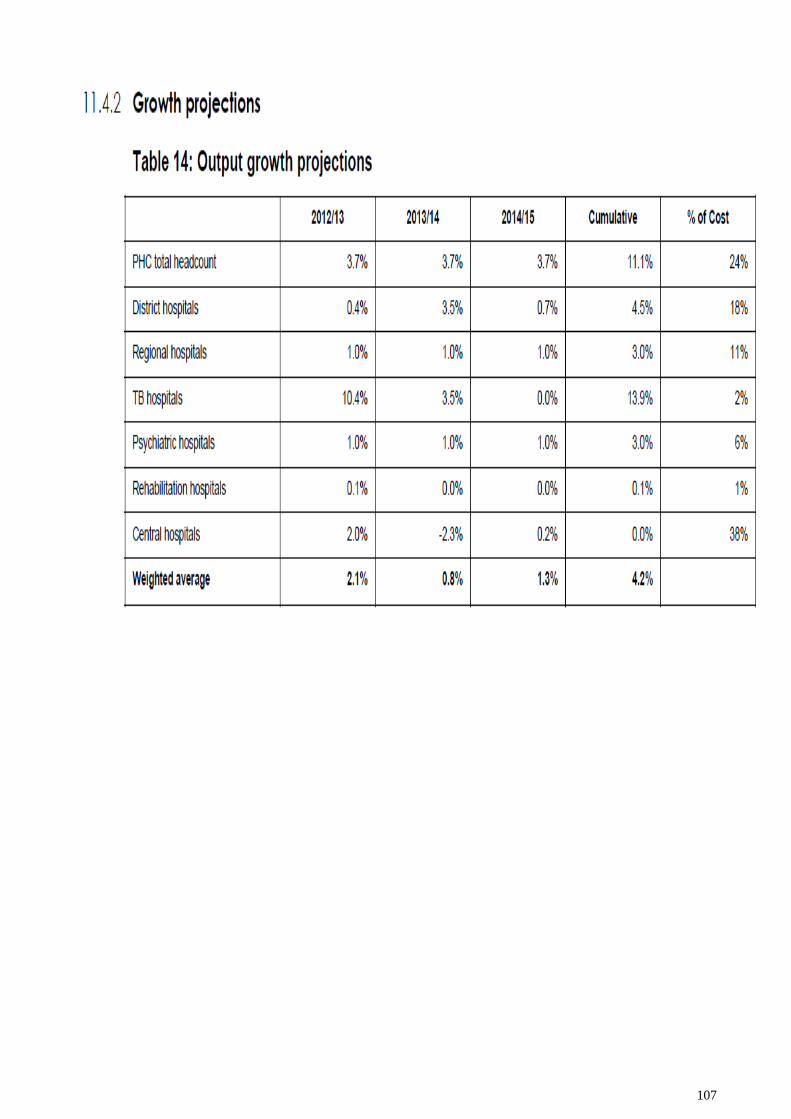
107
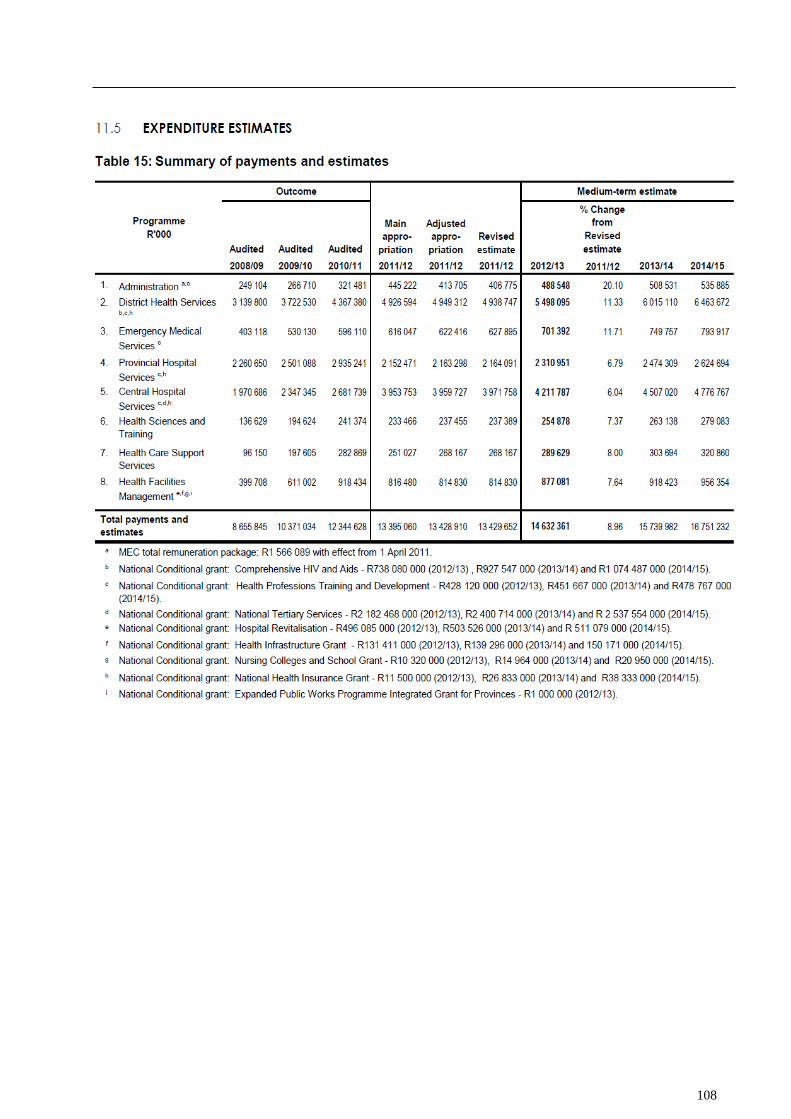
108
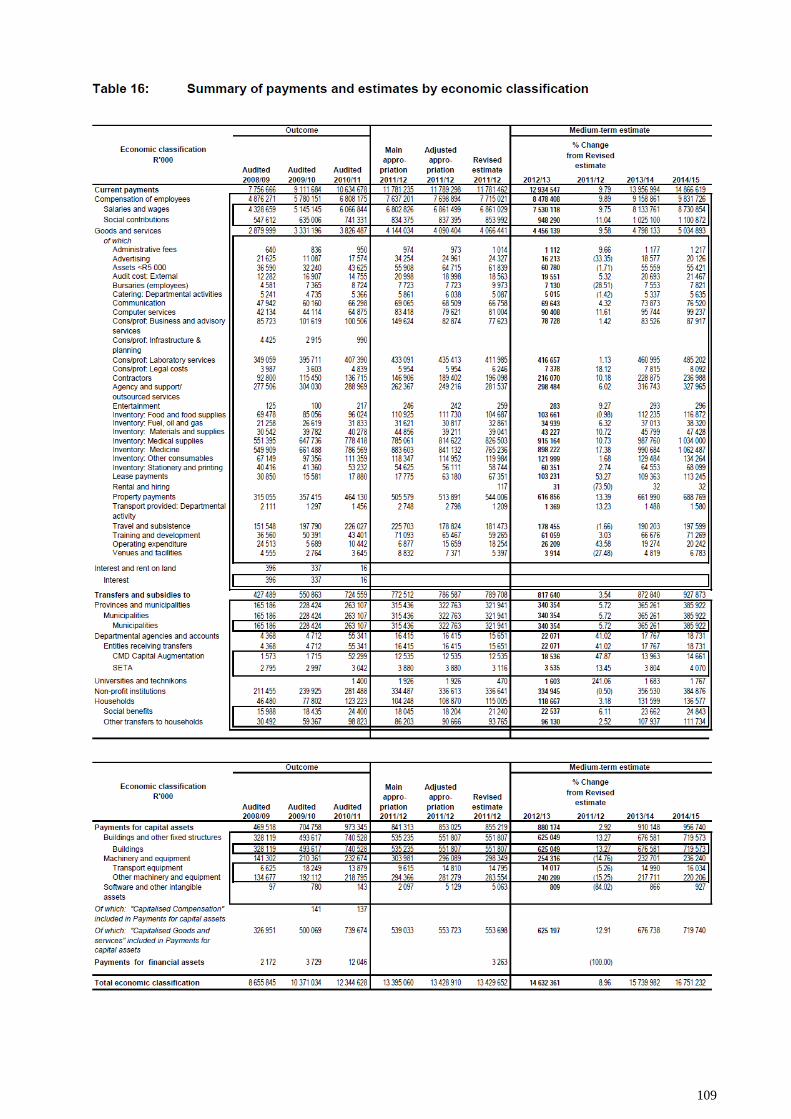
109
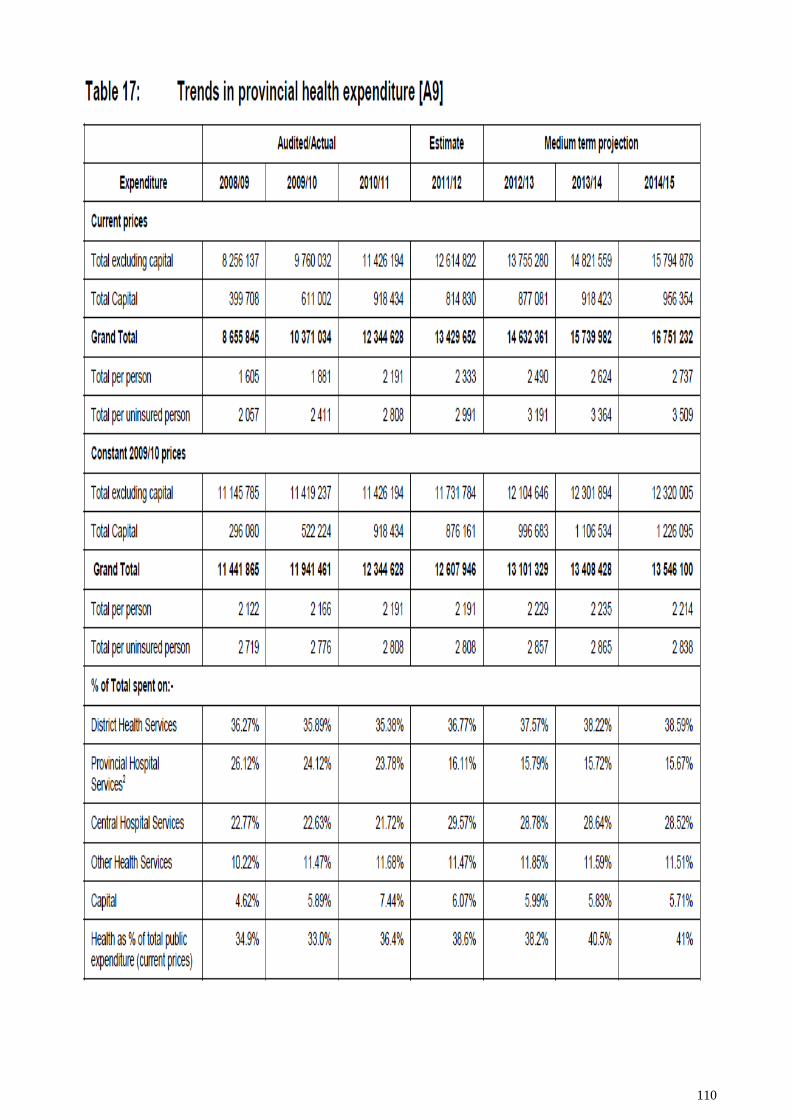
110

111
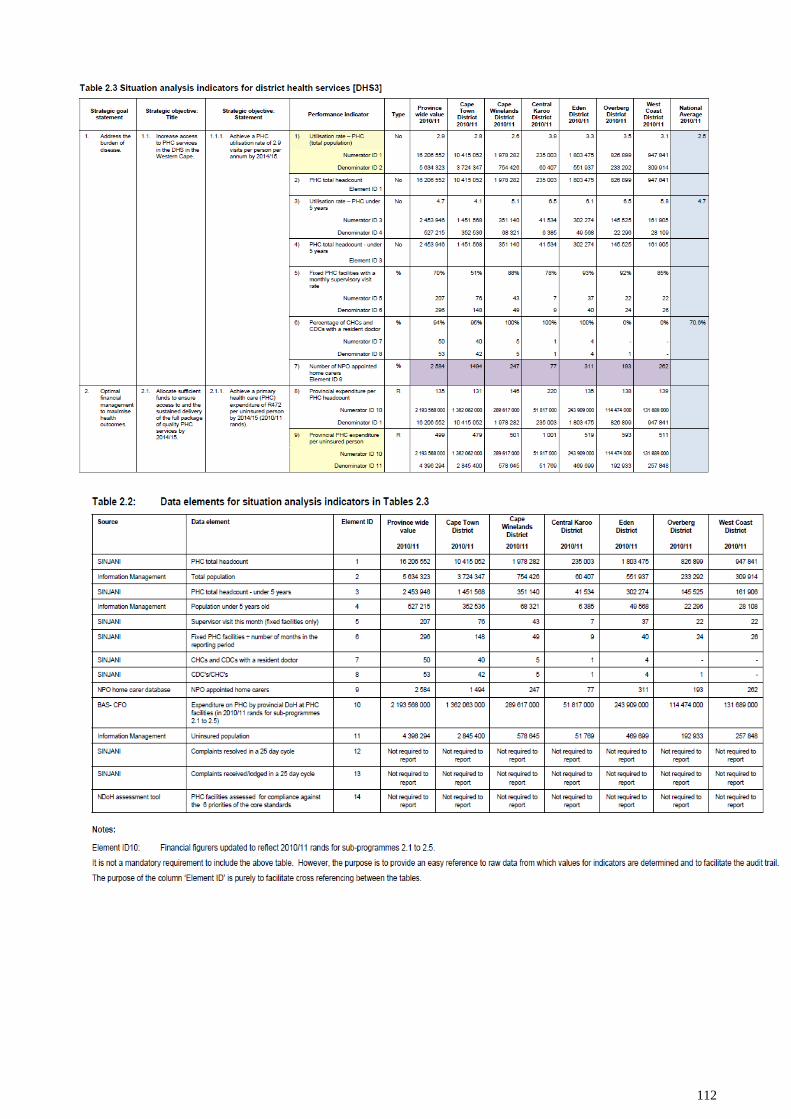
112
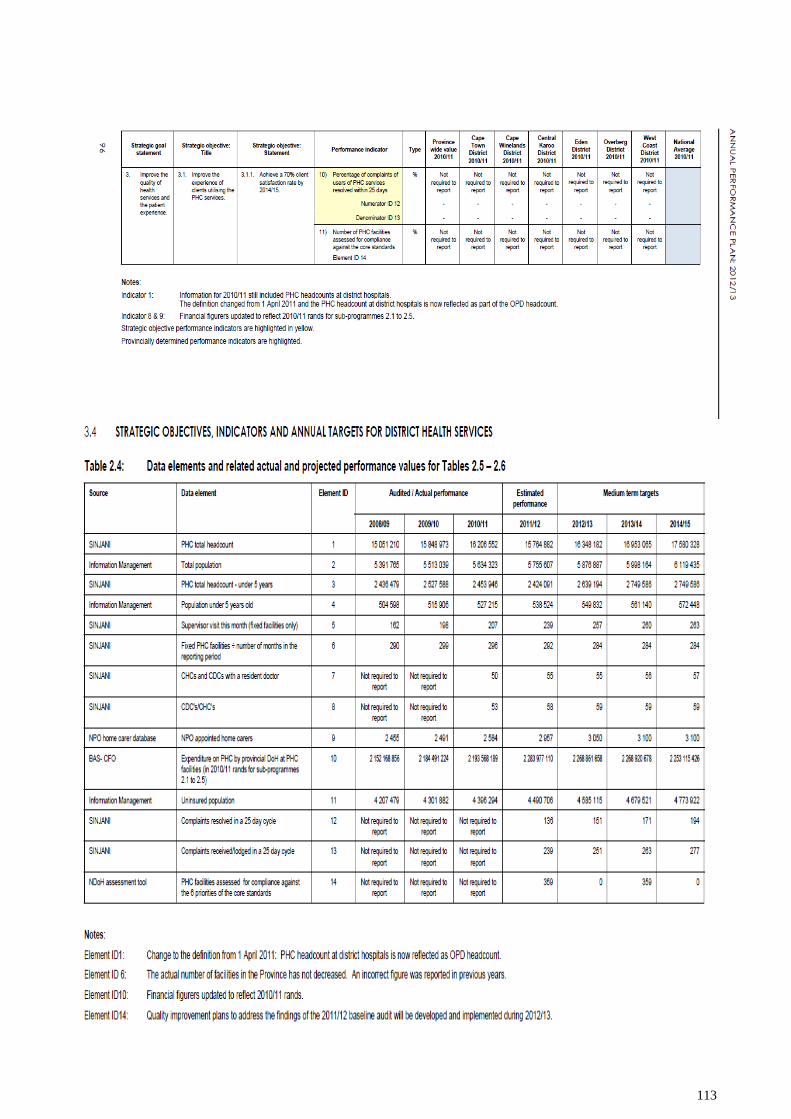
113
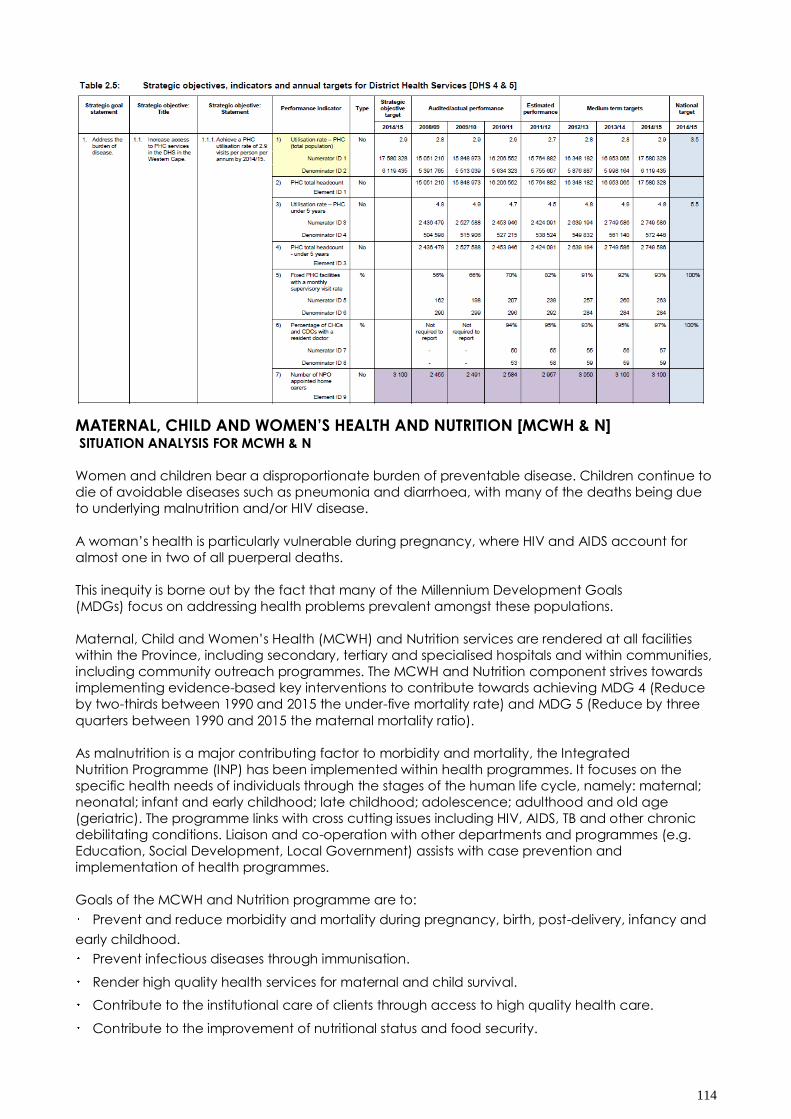
114
MATERNAL, CHILD AND WOMEN‟S HEALTH AND NUTRITION [MCWH & N] SITUATION ANALYSIS FOR MCWH & N
Women and children bear a disproportionate burden of preventable disease. Children continue to
die of avoidable diseases such as pneumonia and diarrhoea, with many of the deaths being due
to underlying malnutrition and/or HIV disease.
A woman‟s health is particularly vulnerable during pregnancy, where HIV and AIDS account for
almost one in two of all puerperal deaths.
This inequity is borne out by the fact that many of the Millennium Development Goals
(MDGs) focus on addressing health problems prevalent amongst these populations.
Maternal, Child and Women‟s Health (MCWH) and Nutrition services are rendered at all facilities
within the Province, including secondary, tertiary and specialised hospitals and within communities,
including community outreach programmes. The MCWH and Nutrition component strives towards
implementing evidence-based key interventions to contribute towards achieving MDG 4 (Reduce
by two-thirds between 1990 and 2015 the under-five mortality rate) and MDG 5 (Reduce by three
quarters between 1990 and 2015 the maternal mortality ratio).
As malnutrition is a major contributing factor to morbidity and mortality, the Integrated
Nutrition Programme (INP) has been implemented within health programmes. It focuses on the
specific health needs of individuals through the stages of the human life cycle, namely: maternal;
neonatal; infant and early childhood; late childhood; adolescence; adulthood and old age
(geriatric). The programme links with cross cutting issues including HIV, AIDS, TB and other chronic
debilitating conditions. Liaison and co-operation with other departments and programmes (e.g.
Education, Social Development, Local Government) assists with case prevention and
implementation of health programmes.
Goals of the MCWH and Nutrition programme are to:
Prevent and reduce morbidity and mortality during pregnancy, birth, post-delivery, infancy and
early childhood.
Prevent infectious diseases through immunisation.
Render high quality health services for maternal and child survival.
Contribute to the institutional care of clients through access to high quality health care.
Contribute to the improvement of nutritional status and food security.
115
APPENDIX H: WELLNESS SUMMIT DECLARATION: WESTERN CAPE GOVERNMENT AND PARTNERS
THE CAPE TOWN DECLARATION ON WELLNESS
8 NOVEMBER 2011
We, the participants in the first summit on wellness of the Premier of the Western Cape gathered in
Cape Town on 8 November 2011:
1. Recognising that: -
1.1. Wellness is a key requirement for development
1.2. The Western Cape, as the other provinces of South Africa, principally suffers from a quadruple
burden of disease consisting of high levels of:
1.2.1. HIV and AIDS and TB;
1.2.2. Maternal and childhood illnesses;
1.2.3. Intentional and non-intentional injuries;
1.2.4. Non-communicable diseases such as diabetes, cardio vascular, respiratory, cancers, mental
diseases.
1.3. Wellness is built on a foundation of the health of children which starts at birth and is initiated
and sustained with breastfeeding.
1.4. Ill health is strongly influenced by behavioural, socio - economic, structural and societal factors.
1.5. Inequity is strongly associated with increased ill health.
1.6. Achieving an increased state of wellness for all requires concerted interventions based on
sound evidence and is best implemented through partnerships in an integrated whole of society
approach.
2. Noting that: -
2.1. There are unacceptably high levels of risk factors and ill health, violence and road injuries in the
Western Cape.
2.2. Ill health impacts on every stratum of the population in the province.
2.3. The most deprived are disproportionately affected by ill health and have unequal access to
health care and this further exacerbates their vulnerability.
2.4. Most at - risk populations require specialised targeted interventions.
3. Affirm that: -
3.1. The province is committed to achieving the Millennium Development Goals related to
infectious diseases, maternal and child health, gender equality, education, environmental
sustainability and poverty as well as non - communicable diseases, violence and traffic injuries.
3.2. The province is committed to engage with the population, community and non -governmental
organisations.
3.3. A shift towards a “whole of government” and a “whole of society” approach is imperative
because government in South Africa cannot succeed without mobilising the ideas and energy of
civil society and communities.
3.4. The prevention of risk factors, disease and its complications before it occurs must be the priority.
4. Realize that: -
4.1. To address infectious diseases
a. HIV prevention strategies including those addressing social, behaviour change and biomedical
prevention strategies promoting safer sex is not at sufficient levels to stop new infections.
b. The increasing trend of multi-and extreme drug resistant TB suggests the need to identify cases of
TB earlier and effect a first time cure.
c. HIV /AIDS and TB should be managed in an integrated manner.
4.2. To address child health
a. Important causes of death such as perinatal conditions, infectious disease, especially
pneumonia, diarrhoea, TB and HIV / AIDS; violence and road injuries and non-communicable
diseases must be tackled.
b. Poor nutrition, which is the underlying cause and the exacerbating risk factor of ill health in
childhood, must be improved.
116
c. Effective early childhood development is required to reduce vulnerabilities during childhood,
adolescence and adulthood.
d. The wellness of adolescents also needs to be addressed.
e. Improving the wellness and development of mothers, parents and families will advance the
health of their children.
4.3. To address woman‟s health
a. Gender equality, reducing poverty, combating infectious diseases and reducing gender based
violence is important.
b. It is essential to work with men and young boys to reduce and prevent gender-based violence
and promote gender equality and women‟s wellness.
c. Quality and coverage of health services for women must be improved.
d. Awareness and management of sexual and reproductive health, cancers affecting women and
mental health must be addressed.
4.4. To address violence and road injuries
a. It is necessary to accept that violence and road traffic injuries afflicting the province‟s citizens
have reached epidemic proportions.
b. Men need to be included as an important focus group as they comprise a majority of injury
deaths.
c. Alcohol, physical and social infrastructure are key risk factors for the burden of violence and
road injuries and it is necessary to develop and implement strategies to reduce alcohol
consumption and improve physical and social infrastructure.
4.5. To address non communicable diseases and associated risk factors
a. Greater attention and focus must be given to non-communicable diseases which affect a large
proportion of society.
b. Adequate attention to be given to mental disease, which contributes significantly to the burden
of ill health, and places an undue strain on individuals, families, communities and social services.
c. Healthy choices related to healthy eating, physical activity, stopping smoking and the use of
harmful drugs and the safe use of alcohol must be prioritised.
d. Efforts must be made to facilitate the right health choices which are not always the easiest or
most affordable choice and often determined by the social and built environment.
e. Increase the availability of affordable healthy foods.
f. Synergies between the management of NCDs and chronic infectious diseases should be
addressed.
5. Hereby commit to:-
5.1. Ensure sustainable long-term, inter-sectoral action to address the root causes of ill health,
injuries and inequity.
5.2. Ensure gender equality and the education of all children as well as adult education.
5.3. Create environments in communities, schools and public and private institutions that reduce
stigma and increase health literacy, are safe and stimulating for children and adults and that
promote their wellness.
5.4. Address the structural, legislative and behavioural constraints and mobilise all members of
society particularly in schools, workplaces communities and government to facilitate making the
right choice to:
*eat healthy foods *promote breastfeeding
*increase physical activity * stop smoking and not smoke in the first place
*not do harmful drugs *test for HIV and have safe sex
*drink alcohol safely *drive safely
* stop violence *responsibly use medicines
*immunise against infectious diseases.
5.5. Take responsibility for the wellness of our children.
5.6. Maximise the wellness of pregnant women and give special attention to the care of new born
babies
5.7. Promote early childhood nutrition through breastfeeding and effective early childhood
development.
117
5.8. Support long-term adherence to medication and chronic disease management at individual
and community level.
5.9. Interventions are informed by evidence and appropriate research.
5.10. Ensure a strong health system to detect and manage disease and their risk factors early and
treat it effectively.
6. To fulfil these commitments
6.1. Develop policies and multi-sectoral interventions informed by evidence and provide resources
to reduce the burden of disease and increase wellness.
6.2. Establish a robust surveillance (that includes both an estimation of mortality and morbidity),
monitoring, evaluation and research capacity to support inter sectoral policy development and
service delivery.
6.3. Establish / maintain/strengthen inter-sectoral working groups (that include infectious diseases,
violence and traffic injuries prevention, women‟s health, maternal and child health, healthy
lifestyles, mental health) to plan, co-ordinate, and monitor and evaluate meaningful collaborative
action towards specified health outcomes.
6.4. Engage Communities and build community capacity including the use of community
agents/workers.
6.5. Establish information sharing, inter-sectoral fora of all parties including PPP interested in ensuring
increased wellness in the province.
6.6. Determine and monitor targets to increase wellness.
7. Concluding statement
We acknowledge that this is the beginning of an important process for the whole of society to
impact on the wellness of our people in the Western Cape.
118
APPENDIX G: RIO POLITICAL DECLARATION ON SOCIAL DETERMINANTS OF HEALTH
Rio de Janeiro, Brazil, 21 October 2011
1. Invited by the World Health Organization, we, Heads of Government, Ministers and
government representatives came together on the 21st day of October 2011 in Rio de
Janeiro to express our determination to achieve social and health equity through action on
social determinants of health and well-being by a comprehensive intersectoral approach.
2. We understand that health equity is a shared responsibility and requires the engagement of
all sectors of government, of all segments of society, and of all members of the international
community, in an "all for equity" and “health for all" global action.
3. We underscore the principles and provisions set out in the World Health Organization
Constitution and in the 1978 Declaration of Alma-Ata as well as in the 1986 Ottawa Charter
and in the series of international health promotion conferences, which reaffirmed the
essential value of equity in health and recognized that "the enjoyment of the highest
attainable standard of health is one of the fundamental rights of every human being
without distinction of race, religion, political belief, economic or social condition". We
recognize that governments have a responsibility for the health of their peoples, which can
be fulfilled only by the provision of adequate health and social measures and that national
efforts need to be supported by an enabling international environment.
4. We reaffirm that health inequities within and between countries are politically, socially and
economically unacceptable, as well as unfair and largely avoidable, and that the
promotion of health equity is essential to sustainable development and to a better quality of
life and well-being for all, which in turn can contribute to peace and security.
5. We reiterate our determination to take action on social determinants of health as
collectively agreed by the World Health Assembly and reflected in resolution WHA62.14
(“Reducing health inequities through action on the social determinants of health”), which
notes the three overarching recommendations of the Commission on Social Determinants of
Health: to improve daily living conditions; to tackle the inequitable distribution of power,
money and resources; and to measure and understand the problem and assess the impact
of action.
6. Health inequities arise from the societal conditions in which people are born, grow, live,
work and age, referred to as social determinants of health. These include early years'
experiences, education, economic status, employment and decent work, housing and
environment, and effective systems of preventing and treating ill health. We are convinced
that action on these determinants, both for vulnerable groups and the entire population, is
essential to create inclusive, equitable, economically productive and healthy societies.
Positioning human health and well-being as one of the key features of what constitutes a
successful, inclusive and fair society in the 21st century is consistent with our commitment to
human rights at national and international levels.
7. Good health requires a universal, comprehensive, equitable, effective, responsive and
accessible quality health system. But it is also dependent on the involvement of and
dialogue with other sectors and actors, as their performance has significant health impacts.
Collaboration in coordinated and intersectoral policy actions has proven to be effective.
Health in All Policies, together with intersectoral cooperation and action, is one promising
approach to enhance accountability in other sectors for health, as well as the promotion of
health equity and more inclusive and productive societies. As collective goals, good health
and well-being for all should be given high priority at local, national, regional and
international levels.
8. We recognize that we need to do more to accelerate progress in addressing the unequal
distribution of health resources as well as conditions damaging to health at all levels. Based
on the experiences shared at this Conference, we express our political will to make health
equity a national, regional and global goal and to address current challenges, such as
eradicating hunger and poverty, ensuring food and nutritional security, access to safe
drinking water and sanitation, employment and decent work and social protection,
protecting environments and delivering equitable economic growth, through resolute
action on social determinants of health across all sectors and at all levels. We also
acknowledge that by addressing social determinants we can contribute to the
achievement of the Millennium Development Goals.
119
9. The current global economic and financial crisis urgently requires the adoption of actions to
reduce increasing health inequities and prevent worsening of living conditions and the
deterioration of universal health care and social protection systems.
10. We acknowledge that action on social determinants of health is called for both within
countries and at the global level. We underscore that increasing the ability of global actors,
through better global governance, promotion of international cooperation and
development, participation in policy-making and monitoring progress, is essential to
contribute to national and local efforts on social determinants of health.
11. Action on social determinants of health should be adapted to the national and sub-
national contexts of individual countries and regions to take into account different social,
cultural and economic systems. Evidence from research and experiences in implementing
policies on social determinants of health, however, shows common features of successful
action. There are five key action areas critical to addressing health inequities: (i) to adopt
better governance for health and development; (ii) promote participation in policy-making
and implementation; (iii) to further reorient the health sector towards reducing health
inequities; (iv) to strengthen global governance and collaboration; and (v) to monitor
progress and increase accountability. Action on social determinants of health therefore
means that we, the representatives of Governments, will strive individually and collectively
to develop and support policies, strategies, programmes and action plans, which address
social determinants of health, with the support of the international community, that include:
(xii) Promote access to affordable, safe, efficacious and quality medicines, including through the
full implementation of the WHO Global Strategy and Plan of Action on Public Health, Innovation
and Intellectual Property;
(xiii) Strengthen international cooperation with a view to promoting health equity in all countries
through facilitating transfer on mutually agreed terms of expertise, technologies and scientific data
in the field of social determinants of health, as well as exchange of good practices for managing
intersectoral policy development.
12. To promote participation in policy-making and implementation
12.1 Acknowledging the importance of participatory processes in policy-making and
implementation for effective governance to act on social determinants of health; 4
12.2 We pledge to:
(i) Promote and enhance inclusive and transparent decision-making, implementation and
accountability for health and health governance at all levels, including through enhancing access
to information, access to justice and public participation;
(ii) Empower the role of communities and strengthen civil society contribution to policy-making and
implementation by adopting measures to enable their effective participation for the public interest
in decision-making;
(iii) Promote inclusive and transparent governance approaches, which engage early with affected
sectors at all levels of governments, as well as support social participation and involve civil society
and the private sector, safeguarding against conflict of interests;
(iv) Consider the particular social determinants resulting in persistent health inequities for indigenous
people, in the spirit of the United Nations Declaration on the Rights of Indigenous Peoples, and their
specific needs and promote meaningful collaboration with them in the development and delivery
of related policies and programmes;
(v) Consider the contributions and capacities of civil society to take action in advocacy, social
mobilization and implementation on social determinants of health;
(vi) Promote health equity in all countries particularly through the exchange of good practices
regarding increased participation in policy development and implementation;
(vii) Promote the full and effective participation of developed and developing countries in the
formulation and implementation of policies and measures to address social determinants of health
at the international level.
120
13. To further reorient the health sector towards reducing health inequities
13.1 Acknowledging that accessibility, availability, acceptability, affordability and quality of health
care and public health services are essential to the enjoyment of the highest attainable standard
of health, one of the fundamental rights of every human being, and that the health sector should
firmly act to reduce health inequities;
13.2 We pledge to:
(i) Maintain and develop effective public health policies which address the social, economic,
environmental and behavioural determinants of health with a particular focus on reducing health
inequities;
(ii) Strengthen health systems towards the provision of equitable universal coverage and promote
access to high quality, promotive, preventive, curative and rehabilitative health services
throughout the life-cycle, with a particular focus on comprehensive and integrated primary health
care;
(iii) Build, strengthen and maintain public health capacity, including capacity for intersectoral
action, on social determinants of health;
(iv) Build, strengthen and maintain health financing and risk pooling systems that prevent people
from becoming impoverished when they seek medical treatment;
(v) Promote mechanisms for supporting and strengthening community initiatives for health
financing and risk pooling systems;
(vi) Promote changes within the health sector, as appropriate, to provide the capacities and tools
to act to reduce health inequities including through collaborative action;
(vii) Integrate equity, as a priority within health systems, as well as in the design and delivery of
health services and public health programmes;
(viii) Reach out and work across and within all levels and sectors of government by promoting
mechanisms for dialogue, problem-solving and health impact assessment with an equity focus to
identify and promote policies, programmes, practices and legislative measures that may be
instrumental for the goal pursued by this Political Declaration and to adapt or reform those harmful
to health and health equity;
(ix) Exchange good practices and successful experiences with regard to policies, strategies and
measures to further reorient the health sector towards reducing health inequities.
14. To strengthen global governance and collaboration
14.1 Acknowledging the importance of international cooperation and solidarity for the equitable
benefit of all people and the important role the multilateral organizations have in articulating norms
and guidelines and identifying good practices for supporting actions on social determinants, and in
facilitating access to financial resources and technical cooperation, as well as in reviewing and,
where appropriate, strategically modifying policies and practices that have a negative impact on
people's health and well-being;
14.2 We pledge to:
(i) Adopt coherent policy approaches that are based on the right to the enjoyment of the highest
attainable standard of health, taking into account the right to development as referred to, inter
alia, by the 1993 Vienna Declaration and Programme of Action, that will strengthen the focus on
social determinants of health, towards achieving the Millennium Development Goals;
(ii) Support social protection floors as defined by countries to address their specific needs and the
ongoing work on social protection within the United Nations system, including the work of the
International Labour Organization;
(iii) Support national governments, international organizations, nongovernmental entities and others
to tackle social determinants of health as well as to strive to ensure that efforts to advance
international development goals and objectives to improve health equity are mutually supportive;
(iv) Accelerate the implementation by the State Parties of the WHO Framework Convention on
Tobacco Control (FCTC), recognizing the full range of measures including measures to reduce
consumption and availability, and encourage countries that have not yet done so to consider
acceding to the FCTC as we recognize that substantially reducing tobacco consumption is an
important contribution to addressing social determinants of health and vice versa;
121
(v) Take forward the actions set out in the political declaration of the United Nations General
Assembly High-Level Meeting on the Prevention and Control Non-communicable Diseases at local,
national and international levels – ensuring a focus on reducing health inequities;
(vi) Support the leading role of the World Health Organization in global health governance, and in
promoting alignment in policies, plans and activities on social determinants of health with its
partner United Nations agencies, development banks and other key international organizations,
including in joint advocacy, and in facilitating access to the provision of financial and technical
assistance to countries and regions;
(vii) Support the efforts of governments to promote capacity and establish incentives to create a
sustainable workforce in health and in other fields, especially in areas of greatest need;
(viii) Build capacity of national governments to address social determinants of health by facilitating
expertise and access to resources through appropriate United Nations agencies‟ support,
particularly the World Health Organization;
(ix) Foster North-South and South-South cooperation in showcasing initiatives, building capacity and
facilitating the transfer of technology on mutually agreed terms for integrated action on health
inequities, in line with national priorities and needs, including on health services and
pharmaceutical production, as appropriate.
15. To monitor progress and increase accountability
15.1 Acknowledging that monitoring of trends in health inequities and of impacts of actions to
tackle them is critical to achieving meaningful progress, that information systems should facilitate
the establishment of relationships between health outcomes and social stratification variables and
that accountability mechanisms to guide policy-making in all sectors are essential, taking into
account different national contexts;
15.2 We pledge to:
(i) Establish, strengthen and maintain monitoring systems that provide disaggregated data to assess
inequities in health outcomes as well as in allocations and use of resources;
(ii) Develop and implement robust, evidence-based, reliable measures of societal well-being,
building where possible on existing indicators, standards and programmes and across the social
gradient, that go beyond economic growth;
(iii) To promote research on the relationships between social determinants and health equity
outcomes with a particular focus on evaluation of effectiveness of interventions;
(iv) Systematically share relevant evidence and trends among different sectors to inform policy and
action;
(v) Improve access to the results of monitoring and research for all sectors in society;
(vi) Assess the impacts of policies on health and other societal goals, and take these into account
in policy-making;
(vii) Use intersectoral mechanisms such as a Health in All Policies approach for addressing inequities
and social determinants of health; enhance access to justice and ensure accountability, which
can be followed up;
(viii) Support the leading role of the World Health Organization in its collaboration with other United
Nations agencies in strengthening the monitoring of progress in the field of social determinants of
health and in providing guidance and support to Member States in implementing a Health in All
Policies approach to tackling inequities in health;
(ix) Support the World Health Organization on the follow-up to the recommendations of the
Commission on Information and Accountability for Women's and Children's Health;
122
(x) Promote appropriate monitoring systems that take into consideration the role of all relevant
stakeholders including civil society, nongovernmental organizations as well as the private sector,
with appropriate safeguard against conflict of interests, in the monitoring and evaluation process;
(xi) Promote health equity in and among countries, monitoring progress at the international level
and increasing collective accountability in the field of social determinants of health, particularly
through the exchange of good practices in this field;
(xii) Improve universal access to and use of inclusive information technologies and innovation in key
social determinants of health.
16. Call for global action
16.1 We, Heads of Government, Ministers and government representatives, solemnly reaffirm our
resolve to take action on social determinants of health to create vibrant, inclusive, equitable,
economically productive and healthy societies, and to overcome national, regional and global
challenges to sustainable development. We offer our solid support for these common objectives
and our determination to achieve them.
16.2 We call upon the World Health Organization, United Nations agencies and other international
organizations to advocate for, coordinate and collaborate with us in the implementation of these
actions. We recognize that global action on social determinants will need increased capacity and
knowledge within the World Health Organization and other multilateral organizations for the
development and sharing of norms, standards and good practices. Our common values and
responsibilities towards humanity move us to fulfil our pledge to act on social determinants of
health. We firmly believe that doing so is not only a moral and human rights imperative but also
indispensable to promote human well-being, peace, prosperity and sustainable development. We
call upon the international community to support developing countries in the implementation of
these actions through the exchange of best practices, the provision of technical assistance and in
facilitating access to financial resources, while reaffirming the provisions of the United Nations
Millennium Declaration as well as the Monterrey Consensus of the International Conference on
Financing for Development.
16.3 We urge those developed countries which have pledged to achieve the target of 0.7 percent
of GNP for official development assistance by 2015, and those developed countries that have not
yet done so, to make additional concrete efforts to fulfil their commitments in this regard. We also
urge developing countries to build on progress achieved in ensuring that official development
assistance is used effectively to help achieve development goals and targets.
16.4 World leaders will soon gather again here in Rio de Janeiro to consider how to meet the
challenge of sustainable development laid down twenty years ago. This Political Declaration
recognizes the important policies needed to achieve both sustainable development and health
equity through acting on social determinants.
16.5 We recommend that the social determinants approach is duly considered in the on-going
reform process of the World Health Organization. We also recommend that the 65th World Health
Assembly adopts a resolution endorsing this Political Declaration.

123