Embed Size (px)
Citation preview
1
Rapid Results for USA Jobs, Health & Wealth: Restoring Our Futures With Low-‐Cost Strategies Funded by Repatriated Overseas Corporate Funds
Prepared by: Dennis D. Embry, Ph.D. President/Senior Scientist, PAXIS Institute, Tucson, AZ • 1-‐520-‐299-‐6770 • [email protected]
Abstract
Reuters News Service estimates that $1.5 trillion in profits are held overseas. Pressure has been increasing to repatriate those funds, but not to repeat the failure of the 2004 repatriation that experts claim did not lead to an increase in domestic investment, employment or R&D.
Existing law plus innovations in “Pay for Success Contracts” (aka Social Impact Bonds), however, provides a pathway for repatriating those pent up profits as USA investments. In turn, those funds can be used to increase employment by the nation’s 4.6 million small businesses (<25 employees) plus rapidly reduce major costly health, educational, and safety problems harming the global competitiveness of the United States.
Current law allows American businesses to repatriate overseas profits by purchasing US investments (e.g., T-‐bills), and only paying tax on the interest. This is already happening, in part because of the instability of the European Union. By tweaking this law, we can create a new investment mechanism, tentatively called: “Our Futures Fund: An American Families & Employment Impact Bond.”
The Our Futures Fund would then invest in staking “no-‐risk” hires of unemployed by qualified small businesses (<25 employees) to ramp up products, services, marketing and sales.
Additionally, the Our Futures Fund would invest in expanding the implementation across the country of previously proven and tested, very cost-‐efficient strategies that can significantly reduce current Medicaid and healthcare costs, future health-‐care, improve public safety, and improve our global competitiveness.
Individual, business, organizational and government beneficiary entities will have a contract to pay back the Our Futures Fund based on careful measures of success and principles established by previous successful experiments in the US and other countries involving Social Impact Bonds. Thus, the success of new employees, businesses, and reductions of crushing costs to local, state and federal governments (e.g., Medicaid, unemployment payments, crime, etc.) would payback the Our Futures Fund and its investors both principle and interest—the companies repatriating overseas corporate profits. A sweetener could be added to the existing law: Interest payments from the Our Futures Fund would be non-‐taxable.
In theory, if US corporations repatriated the same profits as they did in 2004 of $360 billion to the Our Futures Fund, millions of new, sustainable jobs could be created across every American community; and hundreds of billions of dollars of crushing health, welfare, and prison costs would be averted at a local, state and federal level. The US economy would rebound, and our global competitiveness would be increased for all our futures.
2
Predicting America’s Future from Current Facts
Unless current FACTS are altered, multiple adverse trends can be predicted for America. Current FACTS predict a perfect storm of worsening problems for our economy, our public safety, our health, our economy, our global competitiveness, and our national security. Fortunately, the United States actually possesses the best science to alter these trends. Applying this world-‐class science can save Our Futures in America.
FACT: Unemployment has profound physical and behavioral impact on adults, their current children, and their future children
Unemployment has one of the most devastating impacts on persistent mental and physical health on adults and their dependent children. Consider a few examples:
• The US National Longitudinal Survey of Youth shows girls tend to become obese in periods of local and national unemployment,1 which then predicts future disability pension status2 and long-‐term health costs for both young woman, lower fertility, and unhealthy future offspring.3-‐6
• The US National Longitudinal Survey of Youth shows that unemployment increases risky sexual behavior and risk of sexually transmitted diseases.7 The same survey shows higher risk of serious lifetime substance abuse or alcohol abuse.8 Parental
job loss increases youth smoking, forecasting many lifetime health problems.9
• A longitudinal study of 9,500 persons shows that unemployment most adversely affects the most conscientious, good employees for future employment.10
• Two population-‐based longitudinal studies of U. S. workers show that involuntary job loss causes serious cognitive depression and poorer overall health.11 Another longitudinal study of unemployed workers shows that symptoms of common mental disorders then cause greater time in unemployment over four years.12 Increased psychiatric hospitalization follows unemployment in another 12-‐year study.13 The mental health effects of unemployment cause many more persons to migrate to disability benefits.14
• Poor mental health caused by becoming unemployed cause parents to be more negative and punishing to their children.15 Becoming unemployed as mothers increases ADHD among dependent children,16 which in turn predicts unemployment for those children as they age.17
• Losing employment causes subsequent infants born to be more premature and unhealthy.18
• Fathers’ job loss increases suicide among their dependent children.19
• Increases in community unemployment, mortgage delinquency, and foreclosure predict future hospitalizations for serious child maltreatment,20 including traumatic brain injuries.21 In turn, this predicts lifetime employment problems by the child.22
Re-‐employment, however, typically improves health indicators quickly.23 And a warm family environment protects a child from future unemployment as an adult.24-‐26
3
FACT: American Children Have the Highest Rate of Mental, Emotional, Behavioral and Related Physical Illnesses Among Rich Democracies.
The evidence for this sorry state comes from multiple studies, sources and indicators cited in the 2009 Institute of Medicine Report.27 The trends have been worsen for at least the past 20 years, and now it appears that our current children may have a short lifespan than current adults as a consequence of multiple underlying connected factors from adverse childhood experiences, violence, suicide, injuries, plus related metabolic disorders.
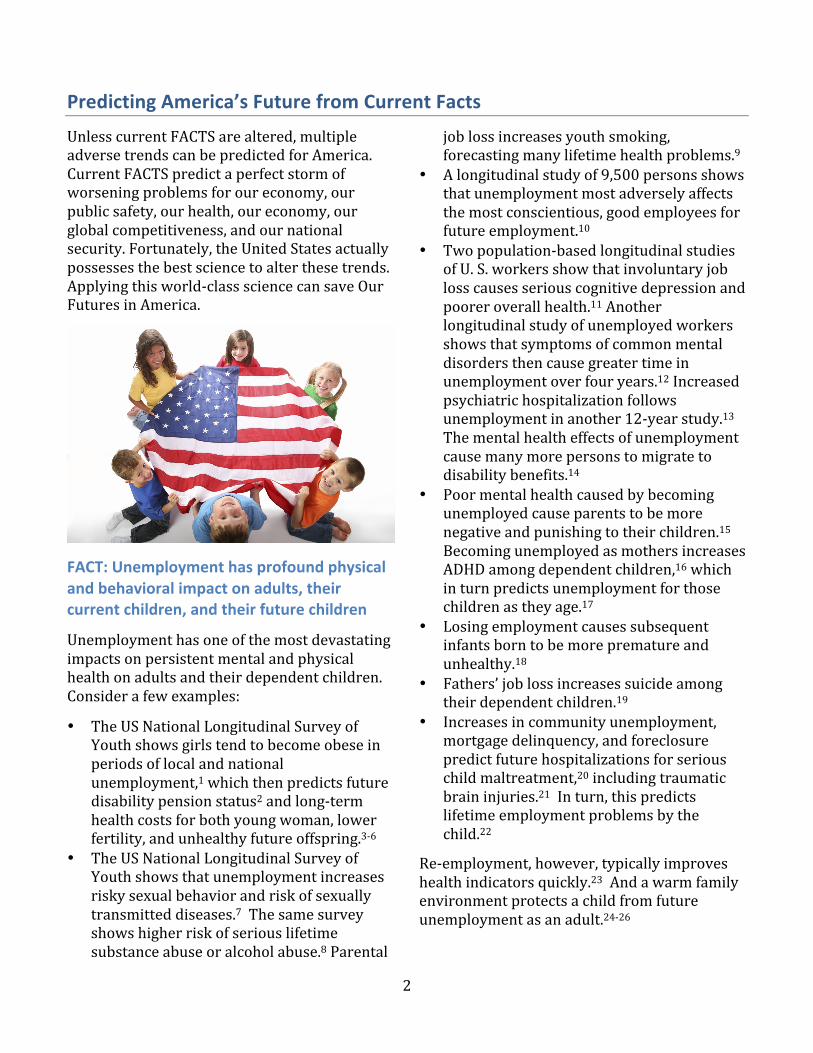
For example, the National Longitudinal Study of Adolescence (see below) shows that one-‐out-‐of-‐two 18 year olds in America will meet an objective diagnoses of one major mental health problem that impair work performance, educational attainment, compromise health, and increase risk of criminal offenses.
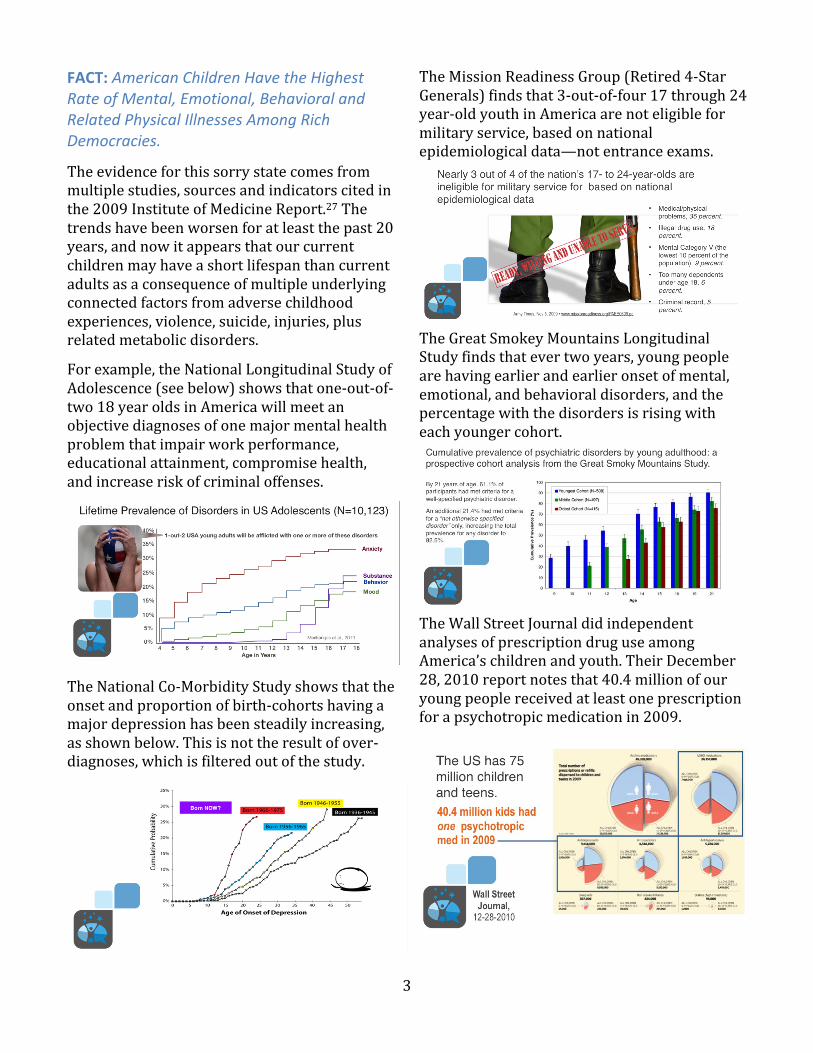
The National Co-‐Morbidity Study shows that the onset and proportion of birth-‐cohorts having a major depression has been steadily increasing, as shown below. This is not the result of over-‐diagnoses, which is filtered out of the study.
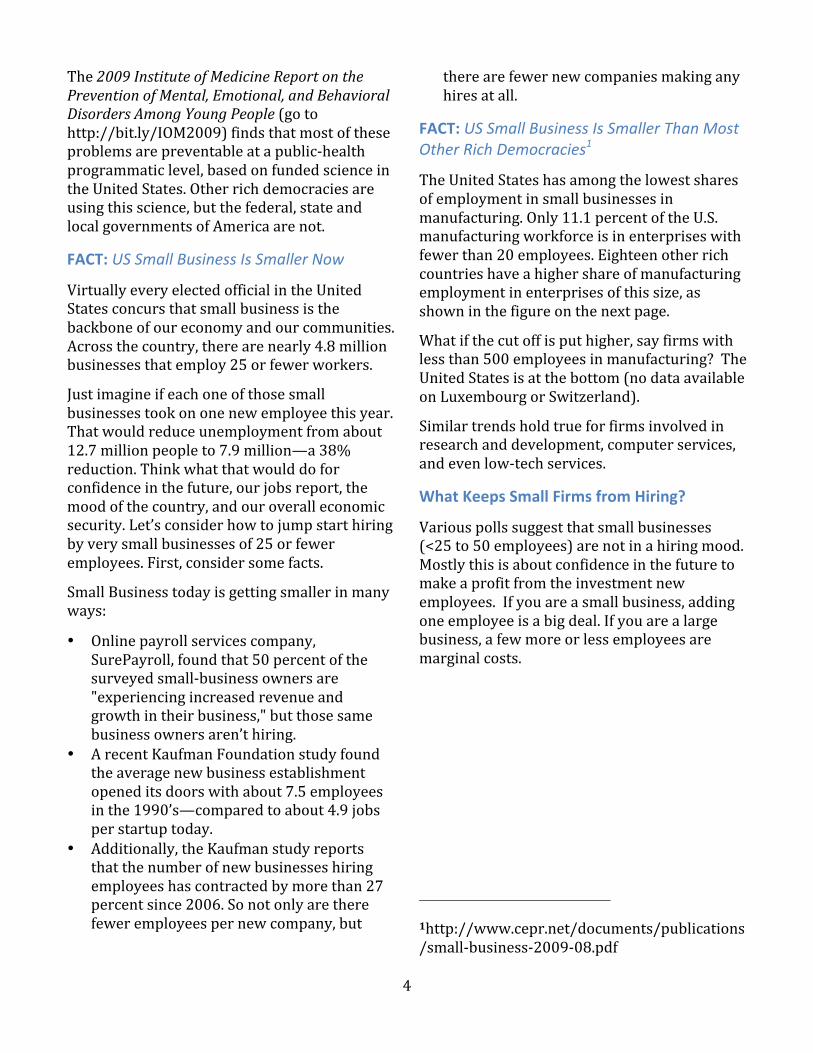
The Mission Readiness Group (Retired 4-‐Star Generals) finds that 3-‐out-‐of-‐four 17 through 24 year-‐old youth in America are not eligible for military service, based on national epidemiological data—not entrance exams.
The Great Smokey Mountains Longitudinal Study finds that ever two years, young people are having earlier and earlier onset of mental, emotional, and behavioral disorders, and the percentage with the disorders is rising with each younger cohort.
The Wall Street Journal did independent analyses of prescription drug use among America’s children and youth. Their December 28, 2010 report notes that 40.4 million of our young people received at least one prescription for a psychotropic medication in 2009.
4
The 2009 Institute of Medicine Report on the Prevention of Mental, Emotional, and Behavioral Disorders Among Young People (go to http://bit.ly/IOM2009) finds that most of these problems are preventable at a public-‐health programmatic level, based on funded science in the United States. Other rich democracies are using this science, but the federal, state and local governments of America are not.
FACT: US Small Business Is Smaller Now
Virtually every elected official in the United States concurs that small business is the backbone of our economy and our communities. Across the country, there are nearly 4.8 million businesses that employ 25 or fewer workers.
Just imagine if each one of those small businesses took on one new employee this year. That would reduce unemployment from about 12.7 million people to 7.9 million—a 38% reduction. Think what that would do for confidence in the future, our jobs report, the mood of the country, and our overall economic security. Let’s consider how to jump start hiring by very small businesses of 25 or fewer employees. First, consider some facts.
Small Business today is getting smaller in many ways:
• Online payroll services company, SurePayroll, found that 50 percent of the surveyed small-‐business owners are "experiencing increased revenue and growth in their business," but those same business owners aren’t hiring.
• A recent Kaufman Foundation study found the average new business establishment opened its doors with about 7.5 employees in the 1990’s—compared to about 4.9 jobs per startup today.
• Additionally, the Kaufman study reports that the number of new businesses hiring employees has contracted by more than 27 percent since 2006. So not only are there fewer employees per new company, but
there are fewer new companies making any hires at all.
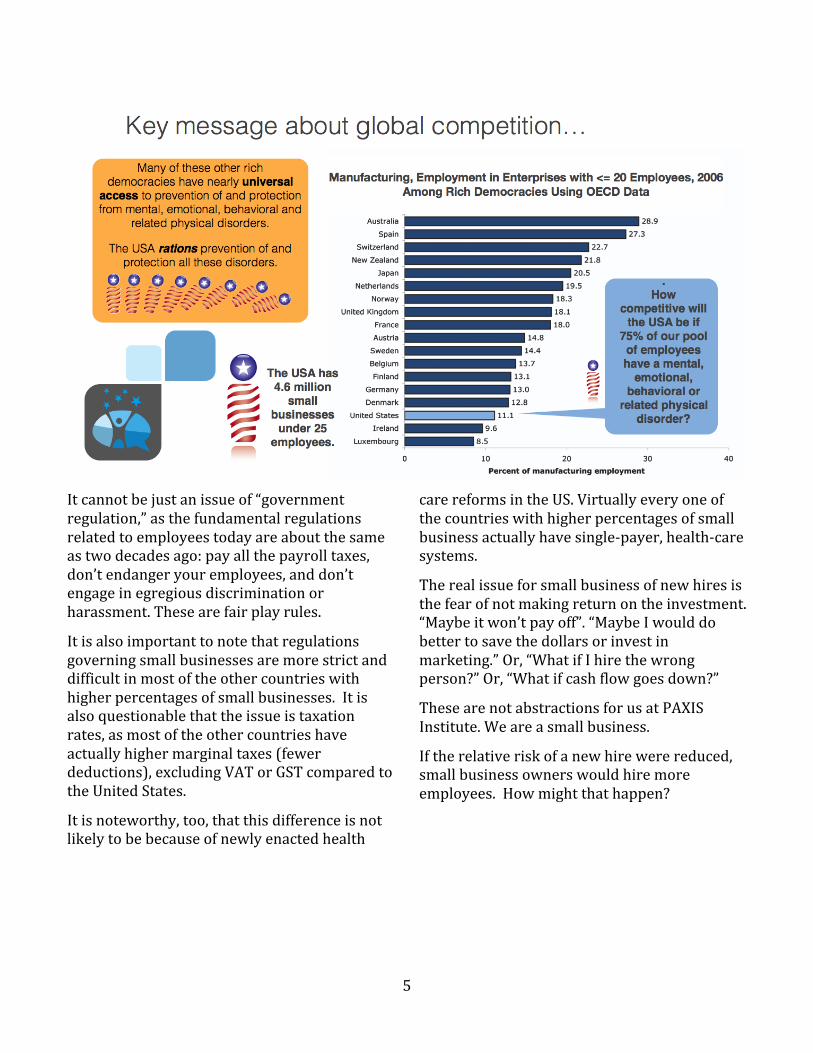
FACT: US Small Business Is Smaller Than Most Other Rich Democracies1
The United States has among the lowest shares of employment in small businesses in manufacturing. Only 11.1 percent of the U.S. manufacturing workforce is in enterprises with fewer than 20 employees. Eighteen other rich countries have a higher share of manufacturing employment in enterprises of this size, as shown in the figure on the next page.
What if the cut off is put higher, say firms with less than 500 employees in manufacturing? The United States is at the bottom (no data available on Luxembourg or Switzerland).
Similar trends hold true for firms involved in research and development, computer services, and even low-‐tech services.
What Keeps Small Firms from Hiring?
Various polls suggest that small businesses (<25 to 50 employees) are not in a hiring mood. Mostly this is about confidence in the future to make a profit from the investment new employees. If you are a small business, adding one employee is a big deal. If you are a large business, a few more or less employees are marginal costs.
1http://www.cepr.net/documents/publications/small-‐business-‐2009-‐08.pdf
5
It cannot be just an issue of “government regulation,” as the fundamental regulations related to employees today are about the same as two decades ago: pay all the payroll taxes, don’t endanger your employees, and don’t engage in egregious discrimination or harassment. These are fair play rules.
It is also important to note that regulations governing small businesses are more strict and difficult in most of the other countries with higher percentages of small businesses. It is also questionable that the issue is taxation rates, as most of the other countries have actually higher marginal taxes (fewer deductions), excluding VAT or GST compared to the United States.
It is noteworthy, too, that this difference is not likely to be because of newly enacted health
care reforms in the US. Virtually every one of the countries with higher percentages of small business actually have single-‐payer, health-‐care systems.
The real issue for small business of new hires is the fear of not making return on the investment. “Maybe it won’t pay off”. “Maybe I would do better to save the dollars or invest in marketing.” Or, “What if I hire the wrong person?” Or, “What if cash flow goes down?”
These are not abstractions for us at PAXIS Institute. We are a small business.
If the relative risk of a new hire were reduced, small business owners would hire more employees. How might that happen?
6
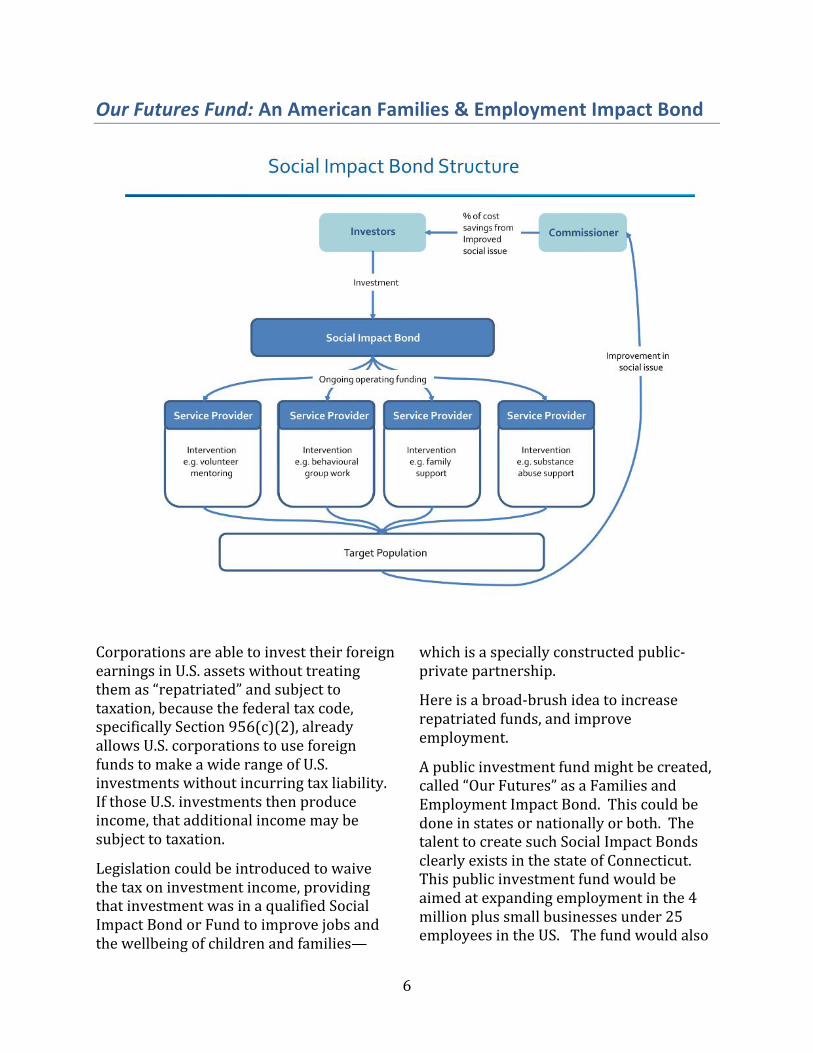
Our Futures Fund: An American Families & Employment Impact Bond
Corporations are able to invest their foreign earnings in U.S. assets without treating them as “repatriated” and subject to taxation, because the federal tax code, specifically Section 956(c)(2), already allows U.S. corporations to use foreign funds to make a wide range of U.S. investments without incurring tax liability. If those U.S. investments then produce income, that additional income may be subject to taxation.
Legislation could be introduced to waive the tax on investment income, providing that investment was in a qualified Social Impact Bond or Fund to improve jobs and the wellbeing of children and families—
which is a specially constructed public-‐private partnership.
Here is a broad-‐brush idea to increase repatriated funds, and improve employment.
A public investment fund might be created, called “Our Futures” as a Families and Employment Impact Bond. This could be done in states or nationally or both. The talent to create such Social Impact Bonds clearly exists in the state of Connecticut. This public investment fund would be aimed at expanding employment in the 4 million plus small businesses under 25 employees in the US. The fund would also

7
be aimed at reduce mental, emotional, behavioral and related physical illnesses among children and families.
Local public entities and local small businesses will form an Our Futures partnership, and local folks seeking employment may become members of this effort. They will prepare a charter that embraces specific actions in their settings to become beneficiary partners in local or regional American Employment Impact Bonds
This investment fund—The American Families and Employment Impact Bonds—would do several types of investments in increasing health and wellbeing for the population of children and families as well as employment in targeted political jurisdictions—e.g., municipalities, counties, and states.
Example Children and Families Investments:
The fund would invest in two of the most highlighted strategies in the IOM Report with a potential to rapidly improve health and safety indicators among children and families at a population, public-‐health level: Triple P and the Good Behavior Game. These two interventions have evidence for being population level approaches with cost effective outcomes across many problems.
Proven Triple P Outcomes Triple P is a system of parenting supports from which parents can choose. Various studies show that these parenting supports can be delivered by many different types of people and via many different media, all with proven effects via many randomized-‐control trials around the world, including the US. Many of those studies can be seen at: http://bit.ly/TRIPLE-‐P-‐CITES .
• A study funded by the Centers for Disease Control and Prevention proved that Triple P can prevent multiple indicators of child maltreatment for whole counties, at the cost of $15 per child in the county.28
• Triple P can be delivered effectively via mass media.29-‐31
• Triple P can be delivered via phone to remote areas.32
• Triple P averts or prevents serious problems like oppositional defiance or conduct disorders.33
• Triple P reduces parental depression.34 35
• Triple P improves marital and step-‐family relationships.36
• Triple P reduces obesity.37 38
Multiple projects and studies show that Triple P works well in America.
A recently published cost-‐savings estimator shows how many cases of child maltreatment might be saved in each state and how much money would be saved as a consequence.39 The estimator may be downloaded at http://paxis.org/triplep/Default.aspx
A video about the study and results may be viewed http://slidesha.re/triplepvideo
Proven Good Behavior Outcomes The Good Behavior Game40 is a “behavioral vaccine” used everyday in a classroom, and can be implemented in a public-‐health model.39
The Game is used during any instructional activity, by dividing the class into teams who may work together to earn simple, brief activity rewards like a “giggle fest.” The Game teaches children how to pay attention voluntarily, and ignore the misbehaviors of other students. The
8
children learn that they can “better their world, and better themselves.”
One can view videos about the province-‐wide launch of the Good Behavior Game (commercially branded as PAX GBG) in Manitoba and an earlier pilot here:
http://bit.ly/ManitobaPAXLaunch
http://bit.ly/ManitobaPAXGBGPilot
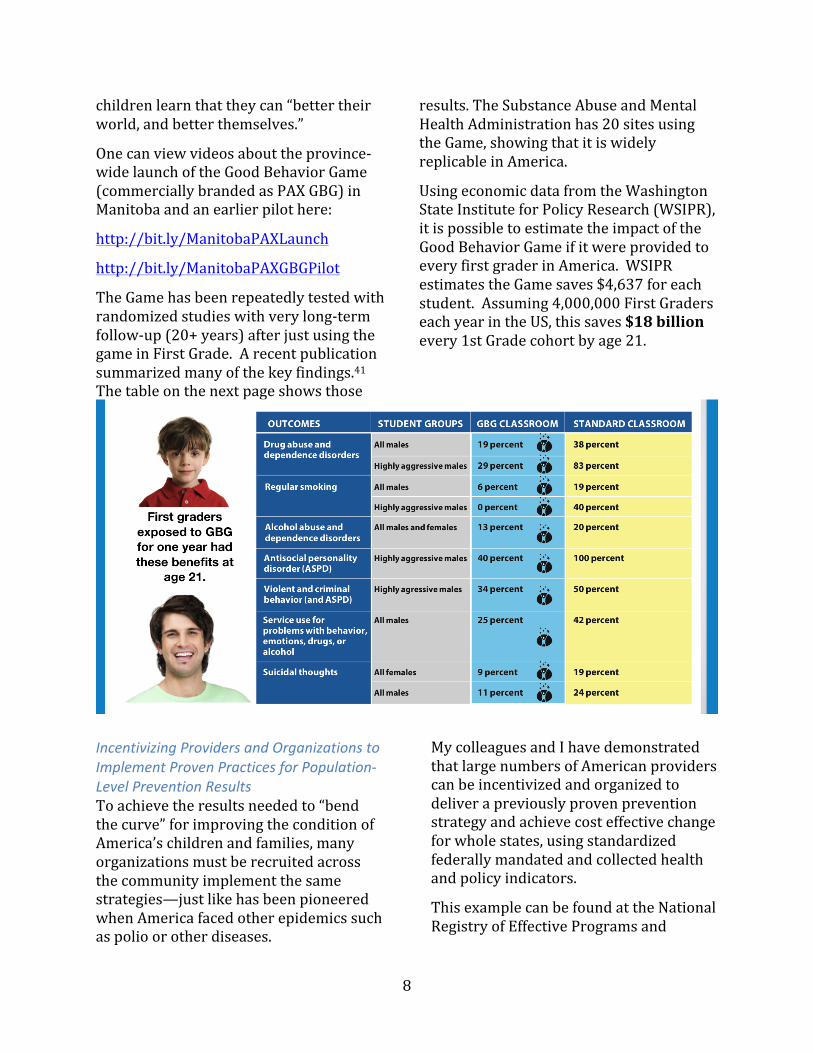
The Game has been repeatedly tested with randomized studies with very long-‐term follow-‐up (20+ years) after just using the game in First Grade. A recent publication summarized many of the key findings.41 The table on the next page shows those
results. The Substance Abuse and Mental Health Administration has 20 sites using the Game, showing that it is widely replicable in America.
Using economic data from the Washington State Institute for Policy Research (WSIPR), it is possible to estimate the impact of the Good Behavior Game if it were provided to every first grader in America. WSIPR estimates the Game saves $4,637 for each student. Assuming 4,000,000 First Graders each year in the US, this saves $18 billion every 1st Grade cohort by age 21.
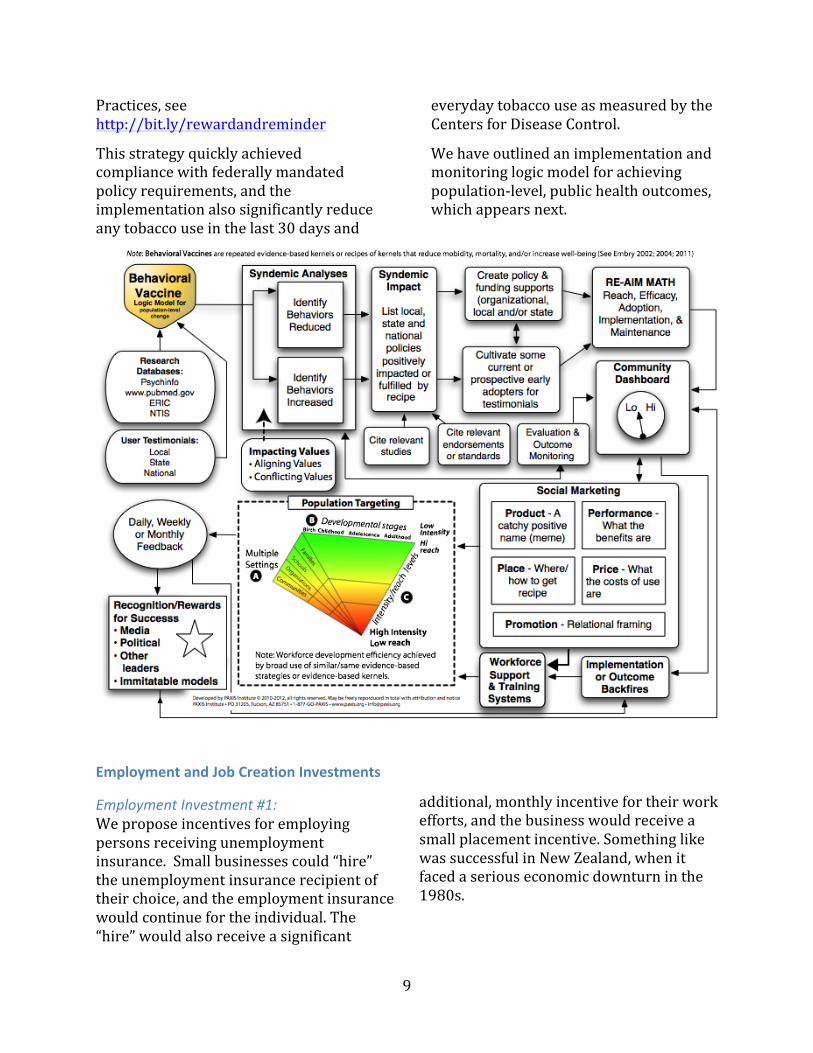
Incentivizing Providers and Organizations to Implement Proven Practices for Population-‐Level Prevention Results To achieve the results needed to “bend the curve” for improving the condition of America’s children and families, many organizations must be recruited across the community implement the same strategies—just like has been pioneered when America faced other epidemics such as polio or other diseases.
My colleagues and I have demonstrated that large numbers of American providers can be incentivized and organized to deliver a previously proven prevention strategy and achieve cost effective change for whole states, using standardized federally mandated and collected health and policy indicators.
This example can be found at the National Registry of Effective Programs and
9
Practices, see http://bit.ly/rewardandreminder
This strategy quickly achieved compliance with federally mandated policy requirements, and the implementation also significantly reduce any tobacco use in the last 30 days and
everyday tobacco use as measured by the Centers for Disease Control.
We have outlined an implementation and monitoring logic model for achieving population-‐level, public health outcomes, which appears next.
Employment and Job Creation Investments
Employment Investment #1: We propose incentives for employing persons receiving unemployment insurance. Small businesses could “hire” the unemployment insurance recipient of their choice, and the employment insurance would continue for the individual. The “hire” would also receive a significant
additional, monthly incentive for their work efforts, and the business would receive a small placement incentive. Something like was successful in New Zealand, when it faced a serious economic downturn in the 1980s.
10
Employment Investment #2: In this track, an existing, credit worthy small businesses would submit a brief business plan to expand their business for a subsidized new hire who is no longer eligible for unemployment yet wish to get employment. The small business would have to commit to providing health insurance for the new employee, the space, etc. The investment for such an employee would be for 12 months to jumpstart business expansion.
Repayment of Investors
As significant beneficiaries, municipal, county and/or and state governments would have a binding agreement to payback pro-‐rata funds to the Social Impact Bond based on designed criteria related to reduced mental, emotional, behavioral, and related physical health outcomes as well as unemployment, using economic modeling.
Also as beneficiaries, contracted businesses would agree to pay pro-‐rata funds into the Social Impact Fund, based on a reasonable formula of impact on their increased business (if any) over a specified time.
Finally, the hired person would agree to make pro-‐rata payments back to the Impact Fund based on federally reported taxes over a period of time, for W2 wages.
Fund Integrity
A series of checks and balances would be established for this fund, based on the well proven principles from the Nobel Prize in Economics for Common Pool Resources to Elinor Ostrum and colleagues. There proven principles include:
1. Group Identity: all parties have a strong sense of group identity and know the rights and obligations of membership,
along with the boundaries of the funds or resources being managed.
2. Proportional costs and benefits. Everyone is expected do their fair share and those who go beyond the call of duty are appropriately recognized.
3. Consensus decision-‐making: Participants will work hard to implement a consensus decision—to do what “we” in the group want, not what they want. In addition, the best decisions often require knowledge of local circumstances that we have and they lack, making consensus decision-‐making doubly important.
4. Monitoring: Since individuals, groups businesses, or public beneficiaries might try to actively game the system, a system of monitoring desired outcomes and transgressions would agreed upon
5. Graduated sanctions: The local groups often can be self-‐correcting, but stronger sanctions need to be provided from punishments to exclusion.
6. Fast and fair conflict resolution: When conflicts arise, they must be resolved quickly and in a manner that all parties consider fair. This typically involves a hearing in which respected members of the group, who can be expected to be impartial, and make an equitable decisions.
7. Local autonomy: Many smaller groups of beneficiaries will be nested in larger groups. They will need to have some powers to make local decisions.
8. Nested governances: When a group beneficiaries is nested with a larger society, relationships among groups and higher-‐level entities (such as state and federal regulatory agencies) must reflect the same principles outlined above for single groups.
11
Next Steps
Soon, there needs to be discussion with various elected officials and other experts to refine this plan.
These discussions would identify major partners, timelines, and mechanisms to refine and promote the plan.
References Cited
1. Arkes J. How the economy affects teenage weight. Social
Science & Medicine 2009;68(11):1943-‐47. 2. Neovius K, Johansson K, Rossner S, Neovius M. Disability
pension, employment and obesity status: a systematic review. Obes Rev 2008;9(6):572-‐81.
3. Jokela M, Elovainio M, Kivimaki M. Lower fertility associated with obesity and underweight: the US National Longitudinal Survey of Youth. Am J Clin Nutr 2008;88(4):886-‐93.
4. Olshansky SJ, Passaro DJ, Hershow RC, Layden J, Carnes BA, Brody J, et al. A potential decline in life expectancy in the United States in the 21st century.[see comment]. New England Journal of Medicine 2005;352(11):1138-‐45.
5. Krassas GE, Tzotzas T. Do obese children become obese adults: childhood predictors of adult disease. Pediatr Endocrinol Rev 2004;1 Suppl 3:455-‐9.
6. Gavard JA. Health care costs of obesity in women. Obstet Gynecol Clin North Am 2009;36(2):213-‐26, xii.
7. Davis MJ. The effects of unemployment and poverty on sexual appetite and sexual risk in emerging and young adults. Sexual Addiction & Compulsivity 2009;16(4):267-‐88.
8. Mossakowski KN. Is the duration of poverty and unemployment a risk factor for heavy drinking? Social Science & Medicine 2008;67(6):947-‐55.
9. Unger JB, Hamilton JE, Sussman S. A family member's job loss as a risk factor for smoking among adolescents. Health Psychol 2004;23(3):308-‐13.
10. Boyce CJ, Wood AM, Brown GDA. The dark side of conscientiousness: Conscientious people experience greater drops in life satisfaction following unemployment. Journal of Research in Personality 2010;44(4):535-‐39.
11. Burgard SA, Brand JE, House JS. Toward a better estimation of the effect of job loss on health. Journal of Health and Social Behavior 2007;48(4):369-‐84.
12. Butterworth P, Leach LS, Pirkis J, Kelaher M. Poor mental health influences risk and duration of unemployment: A prospective study. Social Psychiatry and Psychiatric Epidemiology 2012;47(6):1013-‐21.
13. Eriksson T, Agerbo E, Mortensen PB, Westergaard-‐Nielsen N. Unemployment and mental disorders: Evidence from Danish panel data. International Journal of Mental Health 2010;39(2):56-‐73.
14. Lamberg T, Virtanen P, Vahtera J, Luukkaala T, Koskenvuo M. Unemployment, depressiveness and disability retirement: A follow-‐up study of the Finnish HeSSup population sample. Social Psychiatry and Psychiatric Epidemiology 2010;45(2):259-‐64.
15. McLoyd VC, Jayaratne TE, Ceballo R, Borquez J. Unemployment and work interruption among African American single mothers: effects on parenting and adolescent socioemotional functioning. Child Dev 1994;65(2 Spec No):562-‐89.
16. Harvey E. Parental employment and conduct problems among children with attention-‐deficit/hyperactivity disorder: An examination of child care workload and parenting well-‐being as mediating variables. Journal of Social and Clinical Psychology 1998;17(4):476-‐90.
17. Zwaan M, Gru√ü B, M√ºller A, Graap H, Martin A, Glaesmer H, et al. The estimated prevalence and correlates of adult ADHD in a German community sample. European Archives of Psychiatry and Clinical Neuroscience 2012;262(1):79-‐86.
18. Lindo JM. Parental job loss and infant health. J Health Econ 2011;30(5):869-‐79.
19. Aleck O, Stefania M, James T, James D, Ruth H, Lisa C, et al. The impact of fathers' physical and psychosocial work conditions on attempted and completed suicide among their children. BMC Public Health 2006;6:77.
20. Ben-‐Arieh A. Socioeconomic correlates of rates of child maltreatment in small communities. Am J Orthopsychiatry 2010;80(1):109-‐14.
21. Wood JN, Medina SP, Feudtner C, Luan X, Localio R, Fieldston ES, et al. Local macroeconomic trends and hospital admissions for child abuse, 2000-‐2009. Pediatrics 2012;130(2):e358-‐64.
22. Zielinski DS. Child maltreatment and adult socioeconomic well-‐being. Child Abuse Negl 2009;33(10):666-‐78.
23. Schuring M, Mackenbach J, Voorham T, Burdorf A. The effect of re-‐employment on perceived health. Journal of Epidemiology and Community Health 2011;65(7):639-‐44.
24. Barling J. A response to Kokko and Pulkkinen"s "Aggression in childhood and long-‐term unemployment in adulthood."". Prevention & Treatment 2000;3(1):No Pagination Specified.
12
25. Kokko K, Pulkkinen L. Aggression in childhood and long-‐term unemployment in adulthood: A cycle of maladaptation and some protective factors. Prevention & Treatment 2000;3(1):No Pagination Specified.
26. Kokko K, Pulkkinen L. Aggression in childhood and long-‐term unemployment in adulthood: A cycle of maladaptation and some protective factors. Developmental Psychology 2000;36(4):463-‐72.
27. O'Connell ME, Boat T, Warner KE, editors. Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities. . Washington, DC: Institute of Medicine; National Research Council, 2009.
28. Prinz RJ, Sanders MR, Shapiro CJ, Whitaker DJ, Lutzker JR. Population-‐based prevention of child maltreatment: The U.S. Triple P System Population Trial. Prevention Science 2009;10(March):1-‐13.
29. Sanders MR, Montgomery DT, Brechman-‐Toussaint ML. The mass media and the prevention of child behavior problems: The evaluation of a television series to promote positive outcome for parents and their children. Journal of Child Psychology & Psychiatry 2000;41(7):939-‐48.
30. Sanders M, Calam R, Durand M, Liversidge T, Carmont SA. Does self-‐directed and web-‐based support for parents enhance the effects of viewing a reality television series based on the Triple P-‐Positive Parenting Programme? J Child Psychol Psychiatry 2008;49(9):924-‐32.
31. Sanders MR, Turner KMT. The role of the media and primary care in the dissemination of evidence-‐based parenting and family support interventions. Behavior Therapist 2002;25(9):156-‐66.
32. Connell S, Sanders MR, Markie-‐Dadds C. Self-‐directed behavioral family intervention for parents of oppositional children in rural and remote areas. Behavior Modification 1997;21(4):379-‐408.
33. Mihalopoulos C, Sanders MR, Turner KMT, Murphy-‐Brennan M, Carter R. Does the Triple P-‐Positive Parenting Program provide value for money? Australia and New Zealand Journal of Psychiatry 2007;41(3):239-‐46.
34. Sanders MR, McFarland M. Treatment of depressed mothers with disruptive children: A controlled evaluation of cognitive behavioral family intervention. Behavior Therapy 2000;31(1):89-‐112.
35. Sanders MR, Ralph A, Sofronoff K, Gardiner P, Thompson R, Dwyer S, et al. Every family: a population approach to reducing behavioral and emotional problems in children making the transition to school. J Prim Prev 2008;29(3):197-‐222.
36. Nicholson JM, Sanders MR. Randomized controlled trial of behavioral family intervention for the treatment of child behavior problems in stepfamilies. Journal of Divorce & Remarriage 1999;30(3-‐4):1-‐23.
37. West F, Sanders MR, Cleghorn GJ, Davies PSW. Randomised clinical trial of a family-‐based lifestyle intervention for childhood obesity involving parents as the exclusive agents of change. Behaviour Research and Therapy 2010;48(12):1170-‐79.
38. Einfeld SL, Stancliffe RJ, Gray KM, Sofronoff K, Rice L, Emerson E, et al. Interventions provided by parents for children with intellectual disabilities in low and middle income countries. Journal of Applied Research in Intellectual Disabilities 2012;25(2):135-‐42.
39. Embry DD. Behavioral Vaccines and Evidence-‐Based Kernels: Nonpharmaceutical Approaches for the Prevention of Mental, Emotional, and Behavioral Disorders. Psychiatric Clinics of North America 2011;34(March):1-‐34.
40. Embry DD. The Good Behavior Game: a best practice candidate as a universal behavioral vaccine. Clinical Child & Family Psychology Review 2002;5(4):273-‐97.
41. Kellam SG, Mackenzie AC, Brown CH, Poduska JM, Wang W, Petras H, et al. The good behavior game and the future of prevention and treatment. Addict Sci Clin Pract 2011;6(1):73-‐84.





























