Embed Size (px)
Citation preview
NEUROPHYSIOLOGY OF DENTAL PULP
CONTENTS
INTRODUCTION
DEVELOPMENT
ANATOMY
o General features
o Pulps of maxillary teeth
o Pulps of mandibular teeth
o Coronal pulp
o Radicular pulp
o Apical foramen
o Accessory canals
STRUCTURAL FEATURES
FUNCTIONS
o Inductive
o Formative
o Nutritive
o Protective
o Defensive
VASCULAR SUPPLY
INNERVATION
CLINICAL CONSIDERATIONS
THE FUTURE
CONCLUSION
REFERENCES

INTRODUCTION :
Rapid advances in the basic sciences and the development of
sophisticated instrumentation have had a profound effect on one know ledge
of every organ in the body. The dental pulp is no exception. There are some
technical difficulties in deriving information on the dental pulp an organ or
tissue that is difficult to see because it is encased by the hardest materials in
the body.
“WHY MAKE SUCH A BIG ISSUE ABOUT A LITTLE TISSUE? This is
because this little tissue has created a big issue.
The best root filling is the healthy pulp.
The pulp is a soft tissue of mesenchymal origin with specialized cells,
the odontoblasts arranged peripherally in direct contact with the dentin
matrix.
It is enclosed by the rigid mineralized dentin and this admits its
ability to increase in volume during episodes of vasodilatation and increased
tissue presence.
Following tooth development, pulp retains its ability to produce
dentin throughout life. This enables vital pulp to partially compensate for
the losses of enamel or dentin caused by mechanical trauma or disease etc.
Thus, knowledge about pulp provides a firm biological basis for
clinical decision making.
DEVELOPMENT
Pulp is basically derived from the cephalic neural crest.
During the sixth week of embryonic life, tooth formation begins with
the development of the primary epithelial bands in the upper and lower
jaws. This continuous horse-shaped bands of thickened epithelium cry
quickly divides into
o Vestibular lamina
o Dental lamina
Within the dental lamina, continued and localized proliferative activity leads
to the formation of series of epithelial ingrowths into the ectomesenchyme.
(primitive 2 or 3 cell thick layered epithelial covering an embryonic
connective tissue) at sites corresponding to future deciduous teeth.
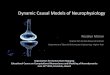
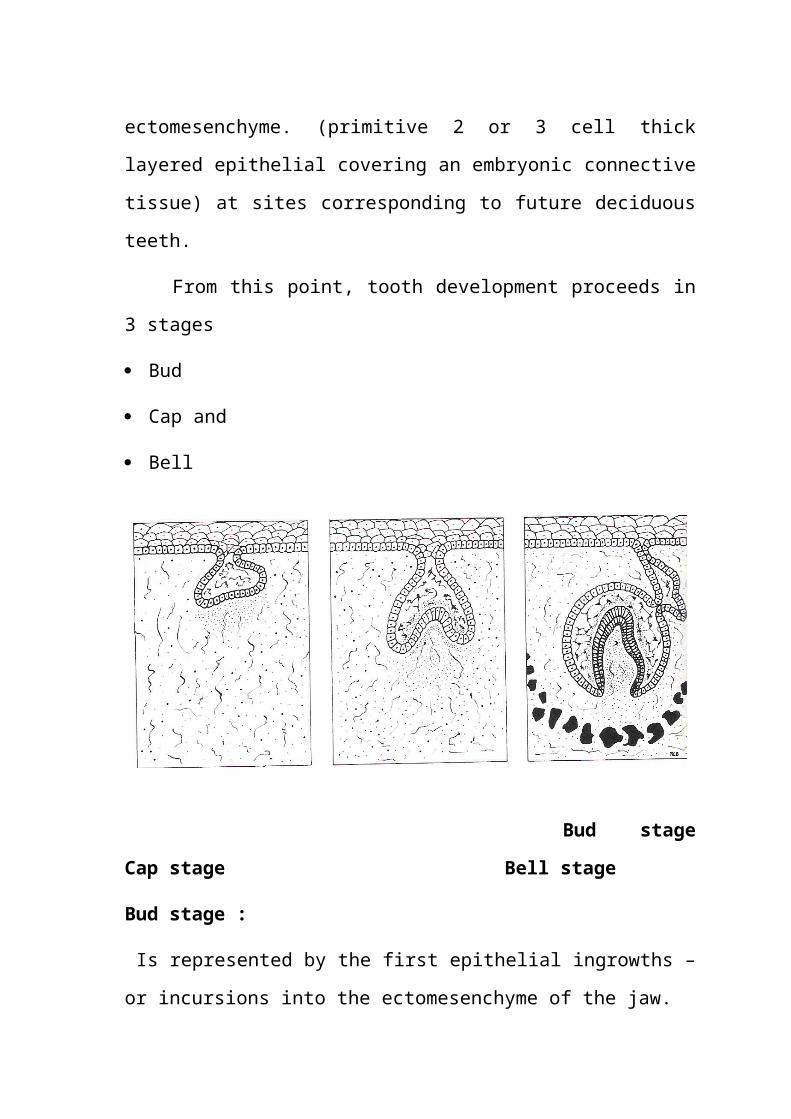
From this point, tooth development proceeds in 3 stages
Bud
Cap and
Bell
Bud stage Cap stage Bell stage
Bud stage :
Is represented by the first epithelial ingrowths – or incursions into the
ectomesenchyme of the jaw.
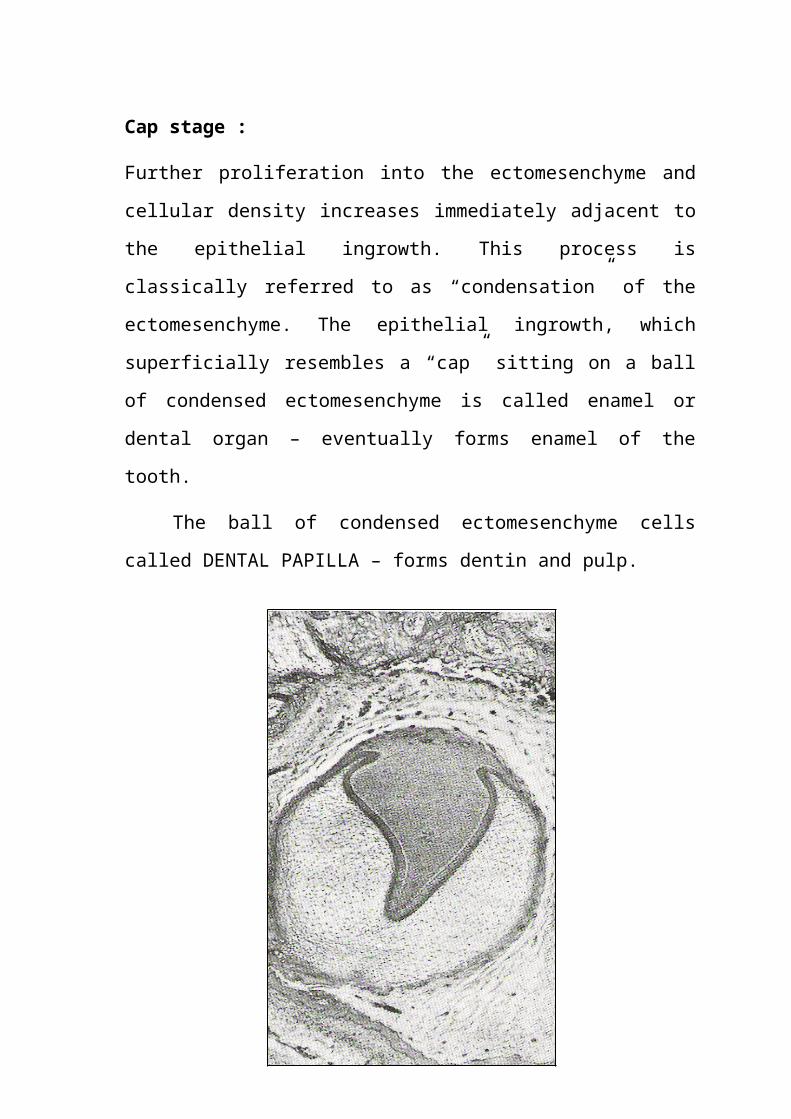
Cap stage :
Further proliferation into the ectomesenchyme and cellular density increases
immediately adjacent to the epithelial ingrowth. This process is classically
referred to as “condensation” of the ectomesenchyme. The epithelial
ingrowth, which superficially resembles a “cap” sitting on a ball of
condensed ectomesenchyme is called enamel or dental organ – eventually
forms enamel of the tooth.
The ball of condensed ectomesenchyme cells called DENTAL
PAPILLA – forms dentin and pulp.
DENTAL PAPILLA
Bell stage :
Continued growth leads to the enamel organ resembling a bell as the
undersurface deepens. The cells within the dentin papilla undergo
cytodifferentiation into a peripheral layer of odontoblasts and a central mass
of fibroblasts.
This change is induced by signals originating in the internal enamel
epithelium. Once the odontoblasts begin to lay down dentin, the dental
papilla becomes by convention, the dental pulp.
Vascularization of the developing pulp also starts during this stage,
with branches entering the base of the papilla. The vascularization of the
odontoblast layer increases as dentin is progressively laid down.
Pioneer nerve fibers approach the developing tooth during bud-cap
stage but they penetrate the dental papilla after dentin begins. Here, we see
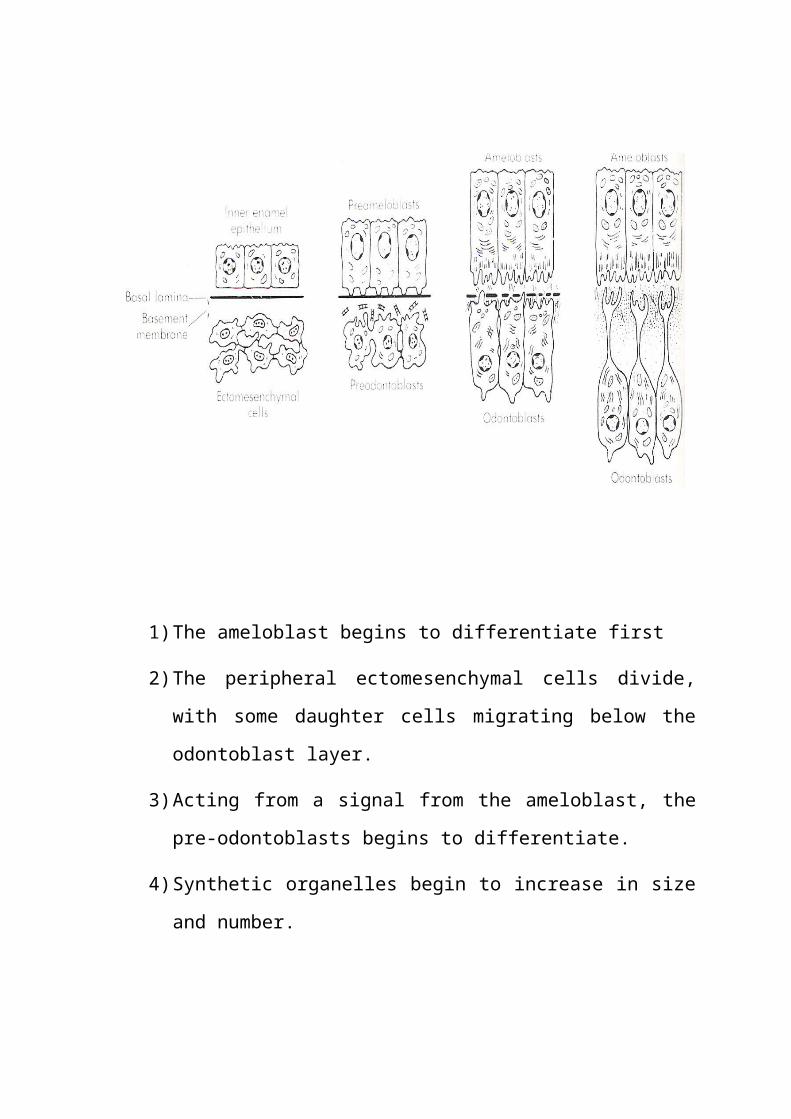
the life cycle of the ameloblast related to that of the odontoblast.
1) The ameloblast begins to differentiate first
2) The peripheral ectomesenchymal cells divide, with some daughter
cells migrating below the odontoblast layer.
3) Acting from a signal from the ameloblast, the pre-odontoblasts begins
to differentiate.
4) Synthetic organelles begin to increase in size and number.
5) Cell becomes polarized, nucleus moves basally. Number of
odontoblastic process begin to form and begins to secrete matrix.
6) Odontoblast retracts as matrix is being laid down, leaving behind a
single main process.
7) Once the first layer of dentin is laid down, the differentiated
ameloblast begins to deposit matrix.
ANATOMY :
General features :
The dental pulp occupies the center of each tooth and shapes itself to
a miniaturization of the tooth.
Every person normally has a total of 52 pulp organs, 32 in the
permanent teeth and 20 in deciduous dentition.
The residence of the pulp is called the pulp cavity surrounded by
dentin on all sides except at the apical foramen.
Total volumes of all the permanent teeth pulp organs is 0.38cc.
Mean volume of a single adult human pulp is 0.02cc.
Molar pulps are 3-4 times larger than incisor pulps.
The pulp cavity may be divided into a coronal portion – the pulp
chamber and a radicular portion – the root canal. In single rooted teeth, the
pulp chamber gradually merges into the root canal, but in multirooted teeth,
there is a single pulp chamber and more than one root canal.
There are canal orifices which are openings in the floor of the pulp
chamber leading into the root canals. They are not separate structures but
are continuous with both the pulp chamber and root canals.
Coronal pulp :
The pulp chamber has a roof, floor, mesial, buccal, lingual and distal
surfaces.
There are pulp horns which are acc extending of the pulp chamber
directly under a cusp or developmental lobe. The number of these of these
horns, thus depends on the cuspal number.
Radicular pulp :
Or the root canal is that portion of the pulp cavity from the canal
orifice to the apical foramen. They are not always straight, and vary in size,
shape and number. It may divided for convenience into the coronal, middle
and apical third portions. The radicular portions of the pulp are continuous
with the periapical connective tissue through the apical foramen.
Apical foramen :
Is an aperture at or near the apex of a root through which the blood
vessels and nerves of the pulp enter or leave the pulp cavity. The anatomy of
this is partially determined by the number and location of apical blood
vessels present at the time of formation of the apex.
The average size of the apical foramen of maxillary teeth in adults is
0.4mm, in mandibular teeth it is 0.3mm. In young, incompletely developed
teeth the apical foramen is funnel shaped, with the wider portion extending
outward. The mouth of the funnel is filled with periodontal tissue that is
later replaced by dentin and cementum. As the root develops, the apical
foramen becomes narrower. The inner surface of the root apex becomes
lined with cementum, which may extend for a short distance into the root
canal (1mm-1.5mm).
Also, the apical foramen is not always the most constricted portion of
the root canal. Constrictions can and do occur before the extremity of the
root is reached. And the apical foramen is not always in the center of the
root apex. It may exit on the mesial, distal, labial or lingual surface of the
root, usually slightly eccentrically. Anatomic studies have shown that the
apical foramen coincides within the anatomic apex in only 17 to 46% of the
cases and it is located on an average of 0.4 to 0.7mm away from the
anatomic apex.
As a general rule, the root apex is completely formed about 2-3 years
after eruption of the tooth.
Accessory canals :
Occasionally, during formation of the root sheath, a break develops in
the continuity of the sheath, producing a small gap. When this occurs,
dentinogenesis does not take place opposite the defect. The result is a small
“accessory canal”. They can become established anywhere along the root
but are found to be most numerous in the apical third. They create a
periodontal-endodontic pathway of communication and a possible portal of
entry in to the pulp if the periodontal tissues lose their integrity (in case of
periodontal disease)
Accessory foramina are also present, which are openings of the
accessory and lateral canals in the root surface.
Pulps of maxillary teeth :
In the central incisor – pulp is somewhat shovel shaped with 3 pulp
horns which are short lateral incisor has 2 pulp horns and the longest pulp is
cuspid with an elliptical cross section buccolingually, with 1 pulp horn. First
premolar has large pulp chamber occlusocervically dividing into 2 smooth
funnel shaped root. The second premolar is similar but has only one root
which tapers at about its midpoint.
Molars :
The pulp chamber of maxillary first molar is the largest in the dental
arch, with 4 pulp horns – mesiobuccal, distobuccal, mesiopalatal and disto
palatal. The arrangement of the pulp horns gives the pulpal root a
rhomboidal shape is cross section, while the pulpal floor is triangular in
cross section.
There are usually 3 roots with usually 3 canals situated in,
mesiobuccal, distobuccal and palatal. The mesiobuccal canal is the
narrowest of the three. The palatal root canal is the largest having the largest
diameter of the three.
Maxillary second molars have a pulp chamber similar to the first
molar except that it is narrower mesiodistally and the 3 root canals are more
closely grouped.
Pulps of mandibular teeth :
The pulp chamber of central incisors in small and flat mesiodistally.
The three distinct pulp horns present in a recently erupted tooth become
calcified and disappear early in life due to constant masticatory stimulus.
Mandibular lateral incisor is parallel to central incisor but only larger in
dimension. The mandibular cuspid resembles the maxillary cuspid with
smaller dimensions. Only one pulp horn is present in the adult tooth.
Mandibular first premolar has a pulp chamber that is narrow
mesiodistally but wider buccolingually. It has a prominent buccal pulp horn,
and a small lingual pulp horn that may disappear with age. Mandibular
second premolar is similar to the first premolar except that the lingual pulp
horn is more prominent.
The roof the mandibular first molar pulp chamber is often rectangular
in shape with 4 pulp horns – mesiobuccal, distobuccal, mesiolingual and
distolingual and the floor is rhomboidal in shape. Three root canals are
usually present but at times a second distal canal may also be present.
Mandibular second molar has a pulp chamber that is smaller than the
first molar and the roots are closer together. Three root canals are usually
present.
Primary Pulp Organs
Function for a shorter period of time than do permanent pulps.
Average length of time a primary pulp functions is about 8.3 years.
This amount of time can be divided into 3 time periods
1) Pulp organ growth
2) Pulp maturation
3) Pulp regression
1. When crown and roots are developing. 1 year
2. Root is completed till root resorption. 3 yrs 9 months
3. From root resorption till exfoliation. 3 years, 6 months
Permanent Pulp Organs :
During crown formation the pulps of primary and perm teeth are
morphologically identical. It takes 5 years in permanent teeth. During this
time the organs are highly cellular, exhibiting a high mitotic rate specially in

cervical region primary teeth also never attain the same extent of neural
development seen in permanent organ.
STRUCTURAL ELEMENTS
Dental pulp is a loose connective tissue and made up of a
combination of cells embedded in an extra cellular matrix of fibers in a
semifluid gel. It contains 75% by wt of water and 25% organic material.
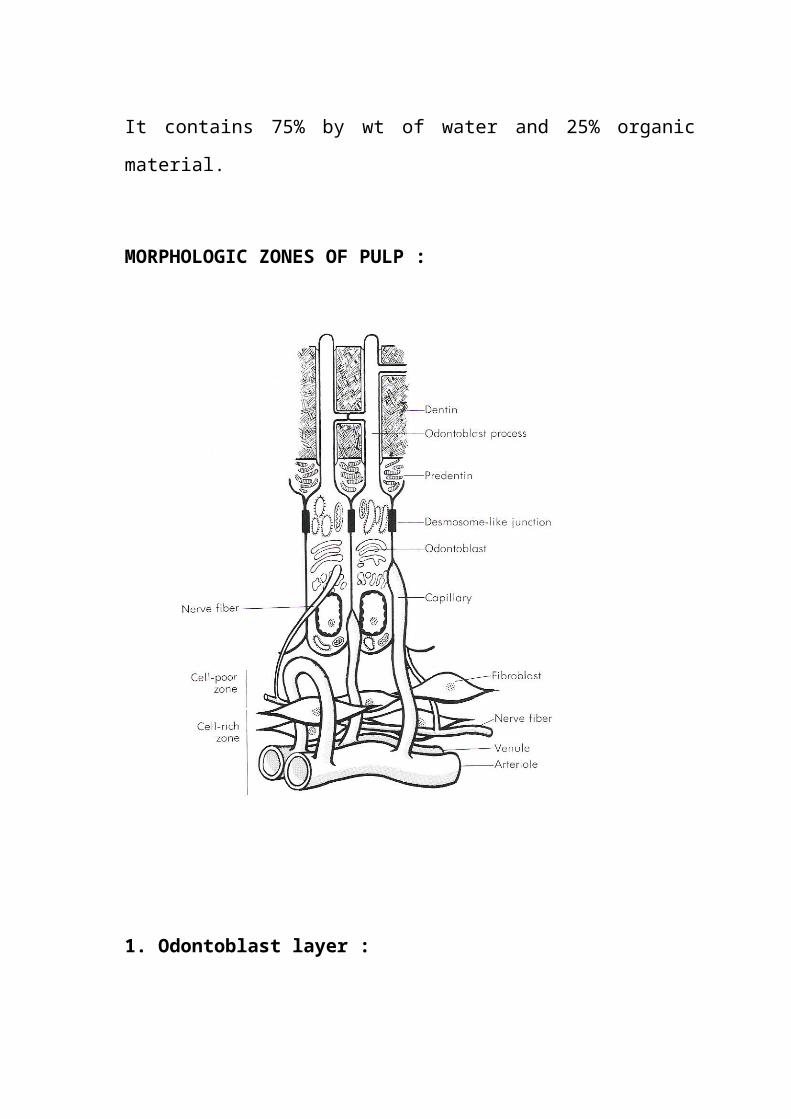
MORPHOLOGIC ZONES OF PULP :
1. Odontoblast layer :
The outermost stratum of cells of healthy pulp is the odontoblast
layer. This layer is located immediately subadjacent to the predentin, the
odontoblast processes, however, pass on through the predentin, into the
dentin.
Consequently, the odontoblast layer is actually composed of the cell
bodies of odontoblasts. Additionally, capillaries, nerve fibers and dendritic
cells may be found among the odontoblasts. This layer is the “EFFECTOR
SYSTEM” of the pulp; all the other elements are either supportive or
protective of the cells forming dentin or programmed to replace them.
In the coronal portion of a young pulp, the odontoblasts assume a tall
columnar form, the tight packing together of these cells – tall and slender
produces the appearance of a palisade. The odontobalsts vary in height;
consequently, their nuclei are not all at the same level and are aligned in a
staggered array. This often produces the appearance of a layer 3-5 cells in
thickness. Between odontoblasts, there are small intercellular spaces,
approximately 300-400 A0 in width. The odontoblast layer in the coronal
pulp contains more cells unit area than in the radicular pulp. Because there
are fewer dentinal tubules per unit area in the root than in the crown of the
tooth, the odontoblast cell bodies are less crowded and are able to spread out
laterally. Between adjacent odontoblasts, there are a series of specialized
cell-to-cell junctions.
Cell poor zone :
Immediately subjacent to the odontoblast layer in the coronal pulp,
there is often a narrow zone approximately 40mm in width that is relatively
free of cells. It is traversed by capillaries, unmyelinated nerve fibers and the
slender cytoplasmic processes of fibroblasts. The presence or absence of the
cell poor zone depends on the functional status of the pulp. It may not be
apparent in young pulps, where dentin forms rapidly, or in older pulps,
where reparative dentin is being produced.
Cell-rich zone :
Usually conspicuous in the subodontoblastic area is a stratum
consisting a relatively high proportion of fibroblasts, compared with a more
central region of the pulp.
It is much more prominent in the coronal pulp than in the radicular
pulp.
Besides fibroblasts, the cell-rich zone may include a number of
macrophages, dendritic cells and lymphocytes. On the basis of evidence
obtained in rats molar teeth, it has been suggested that the cell-rich zone
forms as a result of peripheral migration of cells populating the central
regions of the pulp commencing at about the time of tooth eruption.
Although cell division within the cell-rich zone is a rare occurrence in
normal pulps, death of odontoblasts causes a great increase in the rate of
mitosis. Because irreversibly injured odontoblasts are replaced by cells that
migrate from the cell-rich zone, onto the inner surface of dentin, this mitotic
activity is probably the 1st step in formation of a new odontoblast layer.
Pulp proper :
This is the central mass of the pulp. It contains the larger blood
vessels and nerves. The connective tissue cells in this zone consist of
fibroblasts or pulpal cells.
Supraodontoblast region :
Beginning from the outside, the potential space between the
odontobalst layer and the predentin could be described as the
supraodontoblast layer. 2 structures are located in this region.
1. Unsheathed axons: Found almost exclusively in the crown. These
have been described as the predentinal plexus of BRADLAW. They
are not a true plexus (network) but an area where a number of axons
congregate. It is not clear whether many axons end in this plexus.
But, these axons are in an ideal position to sense changes in fluid
movement then the dentinal tubules as well as changes in the
extracellular fluid composition, which, because of the barrier
properties of the odontoblast layer, will be delayed in reaching the
core of the pulp.
2. Dendritic antigen presenting cells: They are at least 50m long and
have 3 or more main dendritic processes which branch. The dendritic
cells act at least primarily, as antigen presenting cells, stimulating the
division and activity of T-lymphocytes. They initiate primary immune
response. The region, thus, deserves some special mention as (after
the odontoblastic processes) this is the first area at which external
stimuli can be detected in the pulp.
CELLS
Fibroblasts :
The pulp organ is said to consist of specialized connective tissue
because it lacks elastic fibers. The fibroblasts are the basic cells of the pulp
and also the most numerous cell type. As their name implies, they function
in collagen fiber formation throughout the pulp during the life of the tooth.
They are active in collagen synthesis. The cells synthesize type I and
III collagen as well as proteogycans and glycosaminoglycans.
Fibroblasts of the pulp are said to be like “Peter Pan” because they
never really “grow up”. These cells do seem to remain in a relatively
undifferentiated modality when compared with fibroblasts of other
connective tissue of the body.
They have typical stellate shape and extensive processes that contact
and are joined by intercellular junctions to the processes of other fibroblasts.
In young pulp, the cells divide and are active in protein synthesis, but
in the older pulp, they appear rounded or spindle shaped with short
processes and exhibit fewer intracellular organelles. They are then termed
fibrocytes.
In the course of development, the relative number of cellular elements
in the dental pulp decreases whereas the fibre population increases. The
fibroblasts of the pulp, in addition to forming the pulp matrix, also have the
capability of ingesting and degrading this same matrix. These cells thus
have a dual function with pathways for both synthesis and degradation in
the same cell. Due to this they are responsible for the collagen turnover in
the pulp.
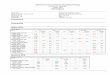
Odontoblasts :
Odontoblasts are the second most prominent cell in the pulp. They
reside adjacent to the predentin with cell bodies in the pulp, and cell
processes in the dentinal tubules. They are approx. 5-7 m in diameter and
25-40 m in length.
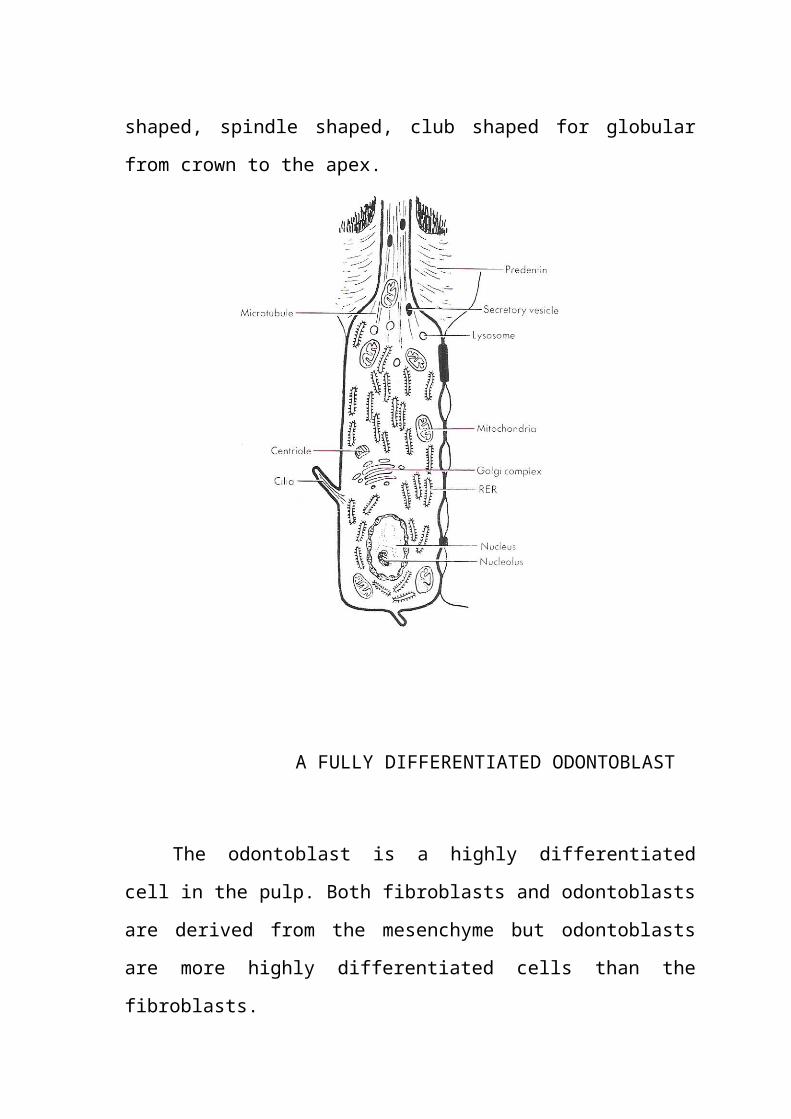
Morphologic variations occur in odontoblasts, ranging from tall
columnar cells in the crown to a low columnar type in the middle of the
root. From an SEM study, French scientists have demonstrated that the
odontoblast cell bodies appear tightly packed in the pulp horn and
successively pear shaped, spindle shaped, club shaped for globular from
crown to the apex.
A FULLY DIFFERENTIATED ODONTOBLAST
The odontoblast is a highly differentiated cell in the pulp. Both
fibroblasts and odontoblasts are derived from the mesenchyme but
odontoblasts are more highly differentiated cells than the fibroblasts.
The main function of the odontoblaasts is the production of dentin.
The cell body manufacturers the matrix material the material is transported
to and secreted from the odontoblastic processes.
Under SEM odontoblasts appear as large, closely aligned,
multilayered sweet potato shaped cells. They average 3-4m in width to 8-
10 m in length. The ultrastructural features of the odontoblast have been
subject to numerous investigations. The cell body of the active odontoblast
has a large, nucleus that may contain up to 4 nucleoli. Nucleus is situated at
the basal end of the cell and is contained within a nuclear envelope. A well
developed golgi complex, centrally located in supranculear cytoplasm
consists of an assembly of smooth walled vesicles and cisternae. Numerous
mitochondria are evenly distributed throughout the cell body.
Rough endoplasmic reticulum is particularly prominent, consisting of
closely stacked cisternae.
Odontoblastic process :
Each process traverses the predentin and then occupies a canaliculus
in the dentin, predominantly filling the lamina of the dentinal tubules. The
odontoblastic process called dentinal fibers or tomes fibers are cytoplasmic
tubular projections, usually devoid of major cytoplasmic organ cells.
Processes are larger at pulpal end than at the periphery (4:1). Microtubules
and microfilaments are the principal components of odontoblastic processes.
Microtubules extend from the cell body out into the process. These straight
structures impart the impression of rigidity.
The plasma membrane of the odontoblastic process closely
approximates the wall of the dentinal tubules. The extent to which the
process extends into dentin has been a controversy. It has been long thought
that the process extends to the full length of dentin (2-3mm).
But ultra structural studies using TEM have described the process as
being limited to the inner third of the dentin with the outer 2/3 rd comprised
of extracellular fluid.
But other studies employing SEM, have described the processes
extending further into the tubule, often as for as the DEJ. More recently,
confocal microscopy using rat molars, concluded that the processes doe not
extend upto the DEJ, except during the early stages of tooth development.
But other studies are warranted.
After the initial dentin formation, the odontoblasts, via the processes
can still modify dentin structure by producing peritubular dentin. This is a
hypermineralized cuff with little organic matrix in the tubule, decreasing the
diameter of the tubule. The odontoblastic processes are bathed by
intercellular fluid from the dental pulp.
Intercellular junctions :
Small regions of the plasma membranes between cells (intercellular
junctions) are visible only by electron microscopy. There are 3 types of
intercellular junctions.
1) Impermeable (tight junction)
2) Adhering (zonula adherence)
3) Communicating (nexuses)
1. Impermeable junctions help the cell maintain a distinct
internal environment. In these junctions, the plasma membranes of
adjacent cells appear to fuse and afford a tight seal between these cells.
Found mainly in the apical part of odontoblasts in young teeth.
2. Adhering junctions are maintained by desomsomes, which are
intercellular bridges seen in light microscopy. There are 3 types of
desomsomes
- Belt
- Spot
- Hemidesmosomes
Spot desmosomes are located in the apical part of the odontoblastic cell
bodies mechanically join odontoblasts together. They promote adhesion
between cells.
3. Communicating junctions also called gap junctions, are
structures that mediate direct transfer of chemical messages between
cells. They enable cells to exchange nutrients and signal molecules for
co-ordination of function. Numerous gap junctions provide low-
resistance pathways through which electrical excitation can pass between
cells.
These junctions are most numerous during the formation of primary
dentin gap junctions crust special proteins called connections in their plasma
membrane which contain pores 15A0 in width gap junctions and
desmosomes have also been observed joining odontoblasts to the processes
of fibroblasts in the subodontoblastic area.
Odontoblastic communications :
The odontoblastic processes are in contact with adjacent processes
through an extensive lateral branch system. The odontoblasts also contact
cells more centrally located in the pulp through fine protoplasmic processes,
possibly owing to the presence of fibronectin, a meditator of cell-to-cell
adhesion. Thus, the odontoblasts may be regarded as part of a mesenchymal
synctium.
This cellular contact is significant because of an odontoblast is injured,
other odontobalsts are affected. The cells on either side are affected by the
breakdown products of the injured odontoblasts when the dentin is injured
through operative procedures; the normal palisade arrangement of the
odontobalsts is altered resulting in disruption of the continuity of these cells.
Thus, injury to the dentin of the tooth creates a reaction within the pulp.
DEFENCE AND OTHER CELLS :
Some of the cells in the pulp are defence cells. Histiocytes or resting
wandering cells are usually found near the blood vessels. They have long
slender branching processes and are able to withdraw these processes and
change quickly into macrophages when the need arises. Undifferentiated
mesenchymal cells are present in the pulp, as they are in all connective
tissue. They are capable of becoming macrophages during injury. They also
may become fibroblasts, odontoblasts or osteoclasts. Undifferentiated
mesenchymal cells constitute a reservoir of cells upon which a body can cell
to assume functions that are not ordinarily needed.
In the pulp, they are usually found outside the vessel walls. Before
injury, they appear elongated and following injury they differentiated into
macrophages and as such can ingest foreign material.
Characteristically, a macrophage has numerous vesicles, vacuoles and
membrane bound bodies known as lysosomes. The lysosomes contain
various hydrolytic enzymes that air in breakdown of the ingested material.
Other transitional cell forms in the pulp include ameboid cells of
various types and lymphoid wondering cells.
FIBRES
Collagen is the predominant extracellular matrix comprising 25-32%
of dry wt and 3.5% of wet wt of pulp.
Collagen fibres are synthesized by the pulpal fibroblasts.
A single collagen molecule referred to as tropocollagen, consists of 3
polypeptide chains, designated as either a 1 or a 2 depending on their amino
acid composition and sequence.
The different combinations and linkages of chains making up the
tropocollagen molecule have allowed collagen fibres and fibrils to be
classified into a number of types.
Type I – Found in skin, tendon, bone, dentin and pulp 56%
Type II – Found in cartilage
Type III – Found in most unmineralized connective tissue
Type IV and VIII collagen – components of basement membranes
Type V – Constituent of interstitial tissues
Type III collagen constitutes 25%-45% of pulp while type I constitutes
around 50%.
Both type III and type I have a similar 67nm bonding but type I
collagen continues both a1 and a2 molecules chains, type III contains only
a1 chains.
With maturity, collagen fibers of approx 750A0 diameter develop.
In young pulp, small collagen fibers stains black with silver
impregnation stains. Thus, they are referred to as argyrophilic fibers. Fine
argyrophilic fibers arising in the pulp, form spirally twisted bundles that
pass between the odontoblasts and fan out into the unmineralized dentin or
predentin in a delicate meshwork. These fibers called VAN KROFFS fibers
form the fibrillar network of the dentin.
There are 2 prominent patterns of collagen deposition in dental pulp.
- Diffuse (in which collagenous fibers lack definite orientation).
- Bundle type (in which large, coarse bundles run parallel to nerves or
independently).
Coronal pulp tissue has more bundle collagen diffuse collagen.
As the pulp gets older, there is an increase in fiber extent – mainly
type III collagen. Regardless of age, the apical portion of the pulp is usually
more fibrous than the coronal portion. Clinically, the apical pulp tissue has a
whitish appearance due to the predominance of collagen fibers. Once mature
collagen is formed, it is less prone to damage. As the pulp chamber narrows
with age, the collagens inability to disintegrate to accommodate the smaller
lumen results in fibrosis – a congestion that could be called
“CRABGRASS” effect.
Ground substance :
It is dense and gel like in nature, varies in appearance from finely
granular to fibrillar with clear spaces left between various aggregates. It is
composed of both acid mucopolysaccharides and protein polysaccharide
compounds, i.e. glycosaminoglycans and proteoglycans.
20% of the pulpal carbohydrate is in glycosaminoglycans. The
following properties have been attributed to glycosaminoglycans.
- Water retention
- Ion binding and electrolyte distention during mineralization.
- Influence on collagen fibrillogenesis.
The metabolism of the cells and the fibers of the pulp is mediated
through the ground substance. It is a viscid fluid and is described by Engel
(1958) as the “milieu interieur” through which metabolites pass from the
circulation to the cells and through which breakdown products from the
cells come back to venous circulation. Thus, the metabolic role of the
ground substance influences the vitality of the pulp.
In all, the ground substance,
- Influences the spread of infection
- Metabolic changes in cells
- Stability of crystalloids
- Effects of hormones vitamins and other substances
Any changes in the nature or quality of the ground substance directly
influences the spread of inflammation and infection.
1. Van Hassel has demonstrated that local increases in fluid presence are
exactly that – LOCAL-confined to the site of injury or irritation by a
resilient connective tissue. The viscosity of the gelated ground substance
reinforced with collagen fibers does not permit fluids to move readily
from one part of the pulp to another or the presence to be transmitted
through the tissue.
2. The gelated ground substance acts as a barrier against the spread of
microorganisms and toxic products. However, organisms such as the
haemolytic streptococcus can elaborate a spreading factor (the enzyme,
hyaluronidase) that may dissolve the barrier and allow a faster invasion.
3. Although the turgidity of the ground substance resists the spread of
inflammation, the process moves apically by increments from a
particular site. Pressure from the increased tissue fluid collapses the thin
walled veins and venules, causing a vascular stasis and ischemia
resulting in local cellular death.
4. Chemical mediators (eg. proteolytic enzymes, hyaluromidase) edema,
and heat may also alter the quality of the ground substance (hydrolytic
agents).
5. Chemotactic factors, chemicals liberated from injured cells not only alter
the viscosity but also exert chemotactic influence on PMNL’s and
macrophages.
6. The viscosity can be further decreased by an excessive accumulation of
inflammatory fluid (edema) and a localized temperature rise, both
resulting from inflammation.
7. The temperature alters the state of ground substance in much the same
way as in a reversible hydrocolloid, a sol-gel type of interplay. The heat
of an inflamed pulp by separating the molecules diminishes the natural
barrier of the gelated state.
METABOLISM :
The metabolic activity has been studied by measuring the rate of
oxygen consumption and the production of CO2 or lactic acid by pulp tissue
in vitro.
Because of the relatively sparse cellular composition of the pulp, the
rate of oxygen consumption is low in comparison to that of most other
tissues. During active dentinogenesis, metabolic activity is much higher
than after the completion of crown development. The greatest metabolic
activity is found in the region of the odontoblast layer.
In addition to the usual glycolytic pathway, the pulp has the ability to
produce energy though a phosphoglyconate shunt type of carbohydrate
metabolism, suggesting that the pulp may be able to function under varying
degrees of ischemia. This could explain how the pulp manages to withstand
periods of vasoconstriction resulting from the use of infiltration anesthesia
employing the epinephrine – containing local anesthetic agents.
CIRCULATION :
The circulation of blood is the transportation system by means of
which the various cells of the body are supplied with nutrients and the waste
products from the cells are removed for elimination from the body.
Systemic circulation :
From the venae cavae the blood passes into the right atrium and from
there it passes then the right ventricle and into the lungs by way of the
pulmonary artery. The blood is oxygenated in the lungs and returns to the
heart by way of pulmonary vein, to the left atrium and is pumped through
the left ventricle to the aorta. The aorta gives off blood vessels (arteries) that
divide into smaller and smaller branches- the arterioles.
The arterial supply to the pulps of teeth originates from the posterior
superior alveolar, the infaorbital and the inf. alveolar branches of the
internal maxillary artery.
A single artery or several smaller arteries enter the pulps their the
apical foramen or foramina. In addition, numerous smaller vessels enter
through lateral and accessory foramina. Blood is returned to the heart by the
venous system. The pulpal veins together with other venous tributaries form
the pterygoid plexus located posterior to the maxillary tuberosity. The
pterygoid plexus drains into internal maxillary vein and this into the external
or internal jugular vein – superior vena cava – heart.
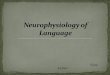
Microcirculation :
The primary function of microcirculation is to transport nutrients to
and to remove metabolic waste products from the tissues. the pulp organ is
extensively vascularized. Blood from the dental artery enters the tooth via
arterioles having diameters of 150m or less. These vessels pass through the
apical foramen or foramina with nerve bundles. Smaller vessels may enter
the pulp via lateral or accessory canals.
The arterioles course up through the central portion of the radicular
pulp and give off branches that spread laterally toward the odontoblast
layer, beneath which they cavity to form a capillary plexus. As the arterioles
pass into the coronal pulp the fan out toward the dentin, diminish in size and
give rise to a capillary network in the subodontoblastic region ranging from
4 to 8m in diameter.
This network provides the odontoblasts with a rich source of
metabolites. There is no Tunica media and adventitia in the capillaries. Are
made up entirely of a single layer flat endothelial cells that is continuous
with the endothelial lining Located on the periphery of the capillaries at
random are pericytes or Rouget) Function of these cells is controversial,
thought to be contractile cells capable of reducing the size of the lumen.
Capillary blood flow in the coronal portion of the pulp is nearly twice that in
the root portion. Moreover, blood flow in the region of the pulp horns is
greater than in other areas of the pulp. In young teeth, during
dentinogenesis, capillaries commonly extend into the odontoblast layer, thus
assuring an adequate supply of nutrients for the metabolically active
odontoblasts and retreat more pulpally once dentinogenesis is completed.
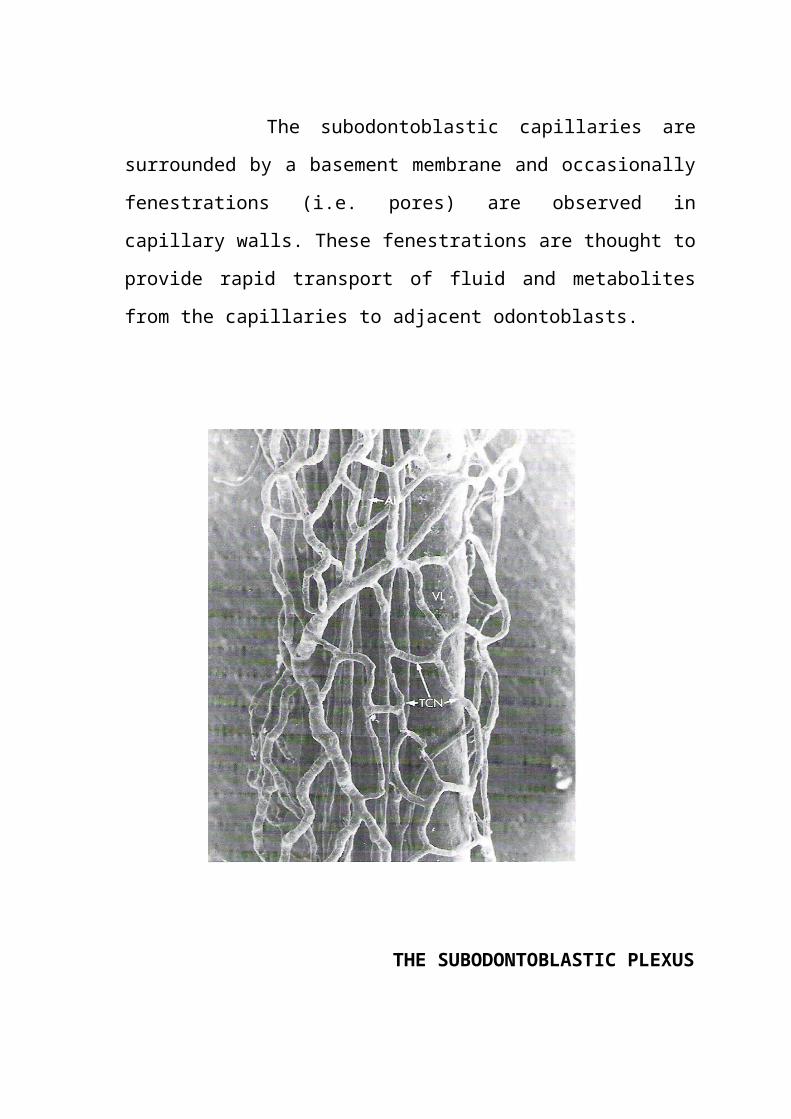
The subodontoblastic capillaries are surrounded by a basement
membrane and occasionally fenestrations (i.e. pores) are observed in
capillary walls. These fenestrations are thought to provide rapid transport of
fluid and metabolites from the capillaries to adjacent odontoblasts.
THE SUBODONTOBLASTIC PLEXUS
In the efferent venous system :
Blood passes from the capillary plexus first into the post capillary
venules and then into larger venules. Venules in the pulp have diameter
comparable to the arterioles but unusually thin walls which make their
lumina large which may facilitate the movement of fluid in or out of the
vessels. The muscular coat of these venules is thin and discontinuous. The
collecting venules become progressively larger as they course to the central
region of the pulp. The largest venules have a diameter of that may reach a
maximum of 200mm, thus they are considerably larger than the anterioles of
the pulp.
Arteriovenous anastomoses (AVA) may be present in both coronal
and radicular pulp. Such vessels provide a direct communication between
arterioles and venules, thus bypassing the capillary bed. The AVA’s are
relatively small venules with a diameter of approximately 10mm.
Among the oral tissues, the young and normal pulp has the highest
volume of blood flow but it is substantially lower than blood flow in the
major visceral organs.
Regulation of pulpal blood flow :
Pulpal blood flow has been estimated to be 20-60ml /min per 100g of
tissue.
Chemical regulation :
Nerves help to regulate the blood supply to the dental pulp.
- Sympathetic (adernregic) nerve fibers liberate norepinephrine which
constricts the vessels.
- Parasympathetic (cholinergic) nerves liberate acetylcholine which
dilates the vessels.
The catecholamines such as epinephrine or norepinephrine exert there
physiologic effects on receptors in the blood vessels, called
“adrenoreceptors”. There are 2 types of adrenoreceptors.
- Alpha ()
- Beta ()
The blood vessels of pulp contain both and adrenoreceptors.
receptors are responsible for contraction and produce vasoconstriction.
Stimulation of receptors causes a relaxation of the vascular musculature.
The pulpal blood vessels contain adrenoreceptors but are poorly equipped
with them.
Blood circulation in an inflamed pulp involves very complex
pathophysiologic reactions.
A unique feature of the pulp is that it is rigidly encased within dentin.
This places it is a low-COMPLIANCE environment, much like the brain,
nail-bed and bone-marrow.
Thus, pulp tissue has limited ability to expand so vasodilatation and
increased vascular permeability evoked during an inflammatory reaction
results in an increase in pulpal hydrostatic pressure.
INNERVATION :
The neuron is the basic cell of the nervous system. Like other cells,
each neuron has a nucleus and surrounding cytoplasm. The neuron has one
relatively long branch – the axon and numerous five branch (dendrites).
The axon transmits brief electrical waves called impulses, the
dendrites receive nerve impulses from other cells. The pulp is heavily
innervated. For eg : appox. 2500 axons enter the apical foramen of a mature
premolar.
Pulp tissue is innervated by the fibers of sensory division of the trigeminal
ganglions and those of autonomic branches of superior cervical ganglion.
The principal function of sensory nerves is to detect stimuli and to
conduct to the C.N.S.
The function of autonomic system is to keep the internal state of the
organism constant and maintain homeostasis.
The sensory system seems to be well suited for signaling potential
damage to the tooth.
The tooth is innervated by a large numbero f myelinated and
unmyelinated nerve fibers.
Meylinated – these have a sheath of myelin, a substance composed largely
of fatty substances as lipids. Myelin sheath functions as an insulator –
deposited by schwann cells.
Unmyelinated – usually found in autonomic nervous system, they
accompany blood vessels. Approximately 80% of nerves are unmyelinated.
Regardless of the nature of sensory stimulus, almost all afferent
impulses from the pulp result in the sensation of pain.
The nerve fibers are seen centrally in the pulp of the root in close
association with the blood vessels. A few fibers leave the central bundles in
the root and travel to the periphery.
Most continue to the coronal pulp where they spread apart and branch
profusely. Most of the branches are in the odontoblastic or subodontoblastic
regions.
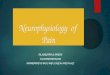
Once they reach the coronal pulp, they fan out beneath the cell-rich
zone, branch into smaller bundles and finally ramify into a plexus of single
nerve axons known as PLEXUS OF RASCHKOW. Full development of
this plexus does not take place until final stages of tooth development.
Branches from this plexus pass into the odontoblastic layer and the
predentin to form the MARGINAL PLEXUS, others continue into dentin
to accompany odontoblastic process into the dentinal tubules.
Ochi and Matsumoto found the approximation of the nerve fibers and
dentinoblastic processes to be about 20nm with no gap junctions or
synapses present.
PLEXUS OF RASCHKOW
Nerve endings do not exist in every tubule. Intratubular nerves appear
in 10%-20% of the tubules in the coronal pulp horn region, compared with
less than 1% at the level of the CE junction and only occasionally nerves are
found in radicular dentin.
Most of these intratubular fibers extend into the dentinal tubules for
only a few mm, but a few may penetrate as for as 100mm.
Nerve fibre types :
The speed with which a nerve impulse passes along a neuron varies
directly with the diameter of the axon the larger the diameter, the faster the
conduction.
Fibers having the largest diameter are classified as A fibers,
intermediate size- B fibers and smallest diameter – C fibers.
The A fibers are myelinated and subdivided into the larger diameter –
A and A-
Intermediate - A
Smaller – AB
Of considerable clinical interest is the evidence that nerve fibers of
the pulp are relatively resistant to necrosis. This apparently because nerve
bundles, in general, are more resistant to autolysis than other tissue
elements. even in degenerating pulps, C fibers might still be able to respond
to stimulated. Also, C fibers are able to function in hypoxia, even after
blood flow has been compromised. This may offer an explanation as to why
instrumentation of non-vital teeth some times causes pain.
Also, it has been observed that removal of pulp by extraction of the
tooth or by pulpectomy and presumably, pulpotomy results in the successive
degeneration of the cell bodies located in the spinal nucleus of the
trigeminal nerve, the main sensory ganglion and the peripheral nerve
leading to the tooth in the socket.
Bernick : observed the effects of caries and restorations on underlying
nerves in the pulp. He found a degeneration of subodontoblastic plexus of
nerves associated with the production of dentin. He concluded that the
terminal nerves in the injured pulp are sensitive to the noxious products of
caries and the restorative procedures. The lack of sensitivity that
accompanies the caries process may be attributable, at least partially, to
degeneration of underlying nerves.
Vitality testing:
ELECTRIC PULP TESTER delivers a current sufficient to overcome
the resistance of enamel and dentin and stimulate the sensory A fibers at the
pulp-dentin border zone. C fibers of the pulp do not respond to the
conventional pulp tester because significantly more current is needed to
stimulate them.
Bender et al found that in anterior teeth, the optimal placement site of
the electrode is the incisal edge of anterior teeth, as the response threshold is
the lowest at that location and increases as the electrode is moved toward
the cervical region of the tooth.
Cold tests using CO2 snow or liquid refrigerants and heat tests
employing heated gutta percha or hot water activate hydrodynamic forces
within the dentinal tubules which in turn excite the interdental A fibers. C
fibers are not activated by these tests unless they produce injury to the pulp.
It has been shown that cold tests do not injure the pulp. Heat tests have a
greater potential to produce injury, but if the tests are used properly, injury
is not likely.
Neuropeptides :
Of immense current interest is the presence of neuropeptides in
sensory nerves. Pulpal nerve fibers contain neuropeptides such as calcitonia
gene-related peptide (CGRP), substance P (SP), neuropeptide Y, neurokinin
A and vasoactive intestinal polypeptide (VIP). Release of these peptides can
be triggered by such things as tissue injury, complement activation, antigen
antibody reactions nerve.
Once released vasoactive peptides produce vascular changes that are
similar to those evoked by histamine and bradykinin (i.e. vasodilatation). In
addition to their neurovascular properties, SP and CGRP contribute to
hyperalgesia and promote wound healing.
LYMPHATICS :
The existence of lymphatics in the pulp has been a matter of debate
because it is not easy to distinguish between venules and lymphatics in
ordinary light micrope techniques. However, techniques using light and
electron microscopy have described lymphatic capillaries in human pulp.
Their fine endothelial structure makes them difficult to see. Main function
of these lymphatic vessels is :
- Removal of interstitial fluid and metabolic waste products.
- To maintain the intrapulpal tissue pressure at a normal level (10mm
of Hg).
These lymphatic vessels follow the course of venules toward apical
foramen. Lymph vessels consist of endothelial lined channels with
discontinuities in their walls and basement membrane. They are
characterized by the absence of RBC’s and presence of lymphocytes.
Lymph vessels draining pulp and periodontal tissues have a common outlet.
They drain into submental, submandibular, and deep cervical lymph nodes
and finally – junction of subclavian and Internal jugular veins.
REGRESSIVE AND AGE CHANGES :
Regressive :
The term regressive is defined as a condition of decreased functional
capability or of returning to a more primitive state.
Older pulps have been described as regressive and as having a
decreased ability to combat and recover from injury. This is because older
pulps have fewer cells, a less extensive vasculature and increased fibrous
elements.
Cell changes :
In addition to the appearance of fewer cells in aging pulp, the cells are
characterized by a decrease in size and number of cytoplasmic organelles.
The fibroblast of an aging pulp exhibits less perinuclear cytoplasm and
passes long, thin cytoplasmic processes. The intracellular organelles are also
reduced in size and number, the mitochondria and endoplasmic reticulum
being good examples of this.
Fibrosis :
The increase in fibers in the pulp organ is gradual and generalized
throughout the organ. Any external trauma such as dental caries or deep
restorations usually causes a localized fibrosis or scarring effect.
The increase in collagen fibers may be more apparent than actual, due
to the decrease in size of the pulp. Which makes the fibers occupy less
space, and hence may become more concentrated without increase in total
volume.
Vascular changes :
Occur in the aging pulp as they do in any organ. Arthrosclerotic
plaques may appear in pulpal vessels. In other cases, the outer diameter of
vessel walls becomes greater as collagen fibers increase in the medial and
adventitial layers.
CALCIFICATIONS :
Calcifications are also found commonly surrounding blood vessels.
Basically, there are 2 distinct types of calcifications.
1) Formed structures – commonly called as pulp stones or denticles.
2) Tiny crystalline masses generally termed diffuse calcifications.
Pulpstones are found predominantly in the coronal portion whereas
calcifications are found in radicular pulp seems to be of diffuse
variety.
Pulp stones :
Pulpstones or denticles are diffuse, or nodular, calcified masses
appearing in either or both the coronal and root portions of the pulp organ.
They usually are asymptomatic unless they impinge on nerve and blood
vessels. They have been seen in functional as well as erupted teeth. Pulp
stones range in size from small, microscopic particles to accretions that
occupy almost the entire chamber.
I. According to their structure, they have been classified as
- True denticles
- False denticles
II. According to the location
- Free
- Attached
- Embedded
True denticles :
They are similar in structure to dentin, in that they have dentinal
tubules and contain the processes of odontoblasts that formed and that exist
on their surface.
True denticles are comparatively rare and are usually located close to
the apical foramen. A theory has been advanced that the development of the
true denticle is caused by inclusion of remnants of the epithelial root sheath
within the pulp. The epithelial remnants induce the cells of the pulp to
differentiate into odontoblasts, which then form the dentin masses called the
pulp stones.
They do not exhibit dentinal tubules but appear instead as concentric
layers of calcified tissue. In some cases, these calcification sites appear
within a bundle of collagen fibers. Other times, they appear in a location in
the pulp free of collagen accumulations. Some false pulp stones
undoubtedly arise around vessels. In the center of these concentric layers of
calcified tissue, there may be remnants of calcified and necrotic cells.
calcification of thrombi in blood vessels, called “PHLEBOLITHS” may also
serve as vili for false denticles. All denticles begin as small nodules but
increase in size by incremental growth on their surfaces. The surrounding
pulp tissue may appear quite normal. Pulp stones may eventually fill
substantial parts of the pulp chamber.
FREE STONES are islands entirely surrounded by pulp tissue.
ATTACHED DENTICLES are partly fused with the dentin.
EMBEDDED DENTICLES are entirely surrounded by dentin.
All are believed to be formed free in the pulp and later to become
attached or embedded as dentin forma. Progresses pulp stones may appear
close to blood vessels and nerve trunks.
Only a relatively small member of pulp stones are sufficiently large
enough to be detected in radiographs. The incidence, as well as the size of
pulp stones increases with age. According to one estimate :
66% - 10-30yrs
80% - 30-50 yrs
90% - over 50 yrs
HISTOLOGICALLY : 2 types of stones are recognized
1) Those that are round or ovoid, with smooth surfaces and concentric
lamellations.
2) Those that assume no particular shape, lack laminations and have
rough surfaces.
Laminated stones appear to grow by the addition of collagen fibrils to
their surfaces, whereas unlaminated stones develop via the mineralization of
preformed collagen fiber bundles.
FUNCTIONS OF PULP :
Inductive :
The primary role of the pulp is to interact with the oral epithelium
cells, which leads to differentiation of the dental lamina and enamel organ
formation. The pulp also interacts with the developing enamel organ as it
determines a particular type of tooth.
Formative :
The pulp organ cells produce the dentin that surrounds and protects
the pulp. The pulpal odontoblasts develop the organic matrix and function in
its calcification. Through the development of the odontoblast processes,
dentin is formed along the tubule wall as well as at the pulp-dentin front and
this process continues throughout the life of the tooth.
Nutritive :
The pulp nourishes the dentin through the odontoblasts and their
processes and by means of the blood vascular system of the pulp.
Protective :
The sensory nerves in the tooth respond with pain to all stimuli such
as heat, cold, pressure, operative cutting procedures and chemical agents.
The nerves also initiate reflexes that control circulation in the pulp. This
sympathetic function is a reflex, providing stimulation to visceral motor
fibers terminating on the muscles of the blood vessels.
Defensive or reparative :
The pulp is an organ with remarkable reparative abilities. It responds
to irritation, whether mechanical, thermal, chemical or bacterial by
producing reparative dentin and mineralizing any affected dentinal tubules.
Both the reparative dentin created in the pulp and the calcification of the
tubules (sclerosis) are attempts to wall off the pulp from the source of
irritation. Also, the pulp may become inflamed due to bacterial infection or
by cutting action and placement of an irritating restorative material. The
pulp has macrophages, lymphocytes, neutrophils, monocytes and plasma
and mast cells, all of which aid in the repair of the pulp.
PULPAL PATHOLOGY:
As I mentioned before, the pulp is a connective tissue, as found
elsewhere in the body. However, several factors make it unique and thus
alter its ability to respond to irritation :
1) The pulp is almost totally surrounded by a hard tissue (dentin), which
limits the area for expansion and restricts the pulp’s ability to cope
with bacteria, necrotic tissue and inflammation.
2) The pulp possesses a unique cell, the odontoblast, as well as cells that
can differentiate into hard tissue-secreting cells that form more dentin
and / or irritation dentin in an attempt to protect the pulp from injury.
3) The pulp has almost a total lack of collateral circulation which
severely limits its ability to cope with bacteria, necrotic tissue and
inflammation.
In spite of these circumstances, studies have indicated that an injured
pulp has some capacity to recover, but the degree is uncertain.
CLINICAL CONSIDERATIONS :
The causes of pulp inflammation, necrosis and dystrophy, beginning
with the most frequent irritant, micro-organisms are:
Iatral causes :
Cavity preparation :
The heat generated by grinding procedures of tooth structure has
often been cited as the greatest single cause of pulp damage during cavity
preparation. Swerdlow and Stanley pointed out the basic factors in rotary
pointed out the basic factors in rotary instrumentation that cause
temperature rise in the pulp. In order of their importance :
1) FORCE applied by the operator
2) SIZE, SHAPE and CONDITION of the cutting tool
3) Revolutions per minute
4) DURATIONS of actual cutting time
We are bound to think that the ultraspeed (30,000 rpm) instruments of
today are more traumatic to the pulp than the low speed (6,000 rpm)
instruments of the past. This is not true, if adequate air-water coolant is
used. It is possible to “burs” the pulp in 11 seconds of preparation time if air
alone is used as coolant at 200,000 rpm. It should be remembered that the
highest intrapulpal temperatures are reached within the first 10 seconds of
grinding.
Studies have concluded that the demise of the pulp begins with a
chronic lesion turned acute by the insult of cavity preparation. An increase
in interpulpal temperature of 200F may result in irreversible damage. Also,
carbide burs generate less thermal change than diamond instruments and
among the diamond burs – coarse diamonds produce a more pronounced
temperature increase than fine diamonds.
Depth of the preparation is also an important factor. Deeper the
penetration, more is the pulp damage. The degree of pulp response is
inversely proportional to the remaining thickness of dentin.
Pulp horn extensions are a very important consideration. The close
proximity of the pulp to the external surface of the tooth leads to exposure if
the pulp horn is not taken into consideration during cavity cutting. At some
points, the pulp is only 1.5 to 2.0mm away before preparation is even begun.
Sproles in a study reported that 66-96% of the time in the 1st and 2nd
molar teeth the cervical pulp horns presents a real danger in cavity
preparation.
PERIODONTAL STATUS AND PULP :
There is an intimate relationship between the periodontal vascular
plexus and the pulpal blood vessels. Besides vascular communication,
connective tissue fibers run from the dental pulp to the periodontal ligament.
Inflammatory lesions in the pulp may be responses to toxic products
entirely through canal openings that normally are covered with bone and
periodontal but now are exposed to oral fluids. Pulpal inflammation in
periodontally involved teeth can occur from extension of the inflamed
periodontal connective tissue.
Gingival recession may expose the opening. Also deep scaling and
currettage in periodontal treatment may possibly be instrumental in causing
pulp damage. Sensitivity of the teeth after deep scaling and curettage may
be due not only to denudation of the roots of the teeth but also to the
production of inflammatory changes or haemorrhages in the pulps of the
teeth.
During curettage of a periodontal lesion that extends entirely around
the apex of the root, the pulp vessels may be severed and the pulp
devitalized, of a lateral root canal, especially in the furcation area, causing
pain and possible spread of infection into the pulp.
ORTHODONTIC FORCE AND PULP :
In theory, the application of light sustained force to the crown of a
tooth should produce a periodontal reaction but share little, if any, effect on
the pulp. There is probably a modest and transient inflammatory response
within the pulp, at least at the beginning of the treatment.
There are occasional reports of tooth vitality during orthodontic
treatment. Poor control of orthodontic force could be the culprit. If a tooth is
subjected to heavy, continuous force, a sequence of abrupt movement
occurs. A large enough abrupt movement of the root apex could severe the
blood vessels as they enter. As proof that orthodontic tooth movement does
affect pulp viability.
Hamersky and colleagues found 27% depression in pulp tissue
respiration as a result of orthodontic force application. Tooth preparations
for crowns require removal of most of tooth enamel. Dentinal tubules are
opened by the tooth preparation and the prepared teeth are more susceptible
to dehydration. Minimal tooth drying is suggested to avoid pulpal damage
from tooth dehydration. It is mandatory that all crowns and fixed prosthesis
are checked for occlusion while seating, thus eliminating the problem of
occlusal prematurities.
Preparation in vital dentin usually makes use of local anesthesia
necessary. As a result, the appropriate nerve mediated vascular responses to
the preparation trauma will be attenuated for a while. This is not regarded as
a serious problem. Because pulpal never are only blocked for a few minutes
after injection. However, when a vasoconstrictor (epinephrine /adrenaline)
is used, there will be a long lasting period of reduction in basal blood flow.
Infiltration anesthesia in upper front tooth region may lower blood perfusion
of the pulp in adjacent teeth by 70-80% for more than 1hour. These changes
are not as prominent with a mandibular block but the pulp is likely to be
vulnerable to the clinical procedures directed to tooth structure. It is
therefore advisable to avid catecholamine vasoconstrictor when preparing
for restorations in teeth with vital pulp.
THE FUTURE :
Pulp death seems to be on the increase, or perhaps only an apparent
increase owing to an awareness of the value of the treated pulpless tooth.
With routine examination and early treatment, with a cautious
temperate approach to all restorative procedures and with a sensible use of
filling materials, the dentist can prevent a great deal of pulp death.
Prevention of pulp injury:
The “dentistogenic” or iatrogenic cause accounts for an
embarrassingly high percentage of the pulp injury and death reflected in the
A.D.A. report.
The university of Connecticut reported that “previous restorative
treatment” was the major etiologic factor leading to root canal therapy.
There are many day-to-day insults leried against the pulp that can be
prevented.
1) Depth of cavity and crown preparation.
2) Width and extension of cavity and crown preparation.
3) Heat damage and dessication during cavity preparation.
4) Chemical injury through medicaments
5) Toxic cavity liners and bases
6) Toxic filling materials
7) Prevention of microleakage
Recent advances:
Pulp cells may hold the key to treatment in Parkinsons disease.
- A study in may issue of European journal of neuroscience shows
dental pulp cells provide great support for nerve cells lost in
Parkisons disease and could be transplanted directly into the affected
parts of the brains.
- This study was the first to test the post-natal stem cells from the more
readily available tooth pulp in the nervous system.
- “Noscat” has also studied dental pulp stem cells as a treatment for
spinal cord injuries.
- However, many years are left for this therapy to be treated in people
for cure.
CONCLUSION :
It is to correlate clinical practice with basic science because
ultimately, an underpinning of basic sciences leads to the most effective
clinical treatment “Dentistry without basic sciences is only a craft but with
good foundation in these sciences, it is a learned profession”.
As heart is to the body, the pulp is to the tooth, providing a constant
source of nutrition to maintain the vitality of a tooth. Every precaution
should be taken to preserve vitality of the pulp.
REFERENCES :
- Stephen Cohen “Pathways of pulp” 8th edn
- John Ingle “Endodontics” 5th edn
- Orbans “Oral Histology”
- Seltzer “The dental pulp” 2nd edn
- “Review of dental pulp – Clinical considerations”. Quintessence Int
1982: 135-137.