Embed Size (px)
DESCRIPTION
Imaging trials introduce novel and unique sources of data. Blinded Independent Central Review is primary source of data. - Utilization of standard assessment criteria - Multiple datasets for given patient/visit - Key aspects of CDM for RECIST trials: >>RECIST version >>Site vs. Central review data >>Central review performance
Citation preview

Data Challenges in Imaging Trials – Image Review Data
03April 2013
Kevin Shea Senior Director Clinical Solutions C3i, Inc. [email protected] 610-772-5726

Key Points
» Imaging trials introduce novel and unique sources of data
» Blinded Independent Central Review is primary source of data Utilization of standard assessment criteria
Multiple datasets for given patient/visit
» Key aspects of CDM for RECIST trials: RECIST version
Site vs. Central review data
Central review performance
2 4/3/2013 © 2011 C3i, Inc. Confidential and Proprietary to C3i, Inc.

Agenda
»Background
»Central Image Review
»RECIST
»Data Management Considerations
»Conclusions
2

Background
» Solid tumor oncology trials
» Imaging assessment as surrogate endpoint
» Variations in modality, techniques, reader assessment, training
» Standardization – consistency, repeatability
» RECIST – well-adopted standard
» CDM processes to monitor assessment data – track quality and safety
3

Data Specific to Imaging Trials
Sources of Data » Imaging – X-Ray, CT, MRI, PET, etc.
» Imaging Technician Report
» Radiologist Report
» QA Report
» Imaging Core Lab Dual Read Review
Adjudicator Review
5 4/3/2013 © 2011 C3i, Inc. Confidential and Proprietary to C3i, Inc.

Central Review of Images
Imaging Core Lab » Focus on objectivity and precision
» No role in clinical care of patient
» Limited reader pool
» Training and review of cases – focus on consistency
» BICR – ideal process: dual reader w/ adjudication
» Various quality processes incorporated to enhance consistency and ensure cross-site view of data
13

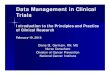
Blinded Independent Central Review
14
Agree
Disagree

Comparison - Site and Central Review
Imaging Site » Clinical focus
» Do not generally utilize RECIST
» Variety of readers
» Not blinded
» Access to all clinical data
» Limited protocol training
Central Review » Focus on imaging
» RECIST w/ limited pool of readers
» Blinded
» Limited access to clinical data
» Image Review Charter
15

RECIST Overview
» Response Evaluation Criteria In Solid Tumors
» Based on WHO criteria (1981)
» Established 2000 (v.1.0), Updated 2009 (v.1.1)
» PII focus, PIII applicability
» Endpoints – ORR, PFS, TTP
» Well-adopted in Imaging Core Labs
» Challenges at AROs and local imaging sites
4

RECIST Parameters
» Serial review – baseline to completion
» Quantify representative tumor burden
» Qualitative assessment of remaining lesions
» Lesion classification
» Consistent assessment categories
» Associate changes in tumor burden with efficacy Response (may require confirmation)
− Time point response
− Best overall response
Progression – Date of progression
5

RECIST Lesion Classifications
» Target Lesions representative of disease
able to reproducibly measure and track over time
» Non-target all other lesions or sites of disease
tracked qualitatively
» New – post-baseline presence of new disease
6

RECIST Target Lesion Selection Criteria
» Uni-dimensional measurement
» Number Maximum of Five Target Lesions
No more than two per organ
» Length ≥ 10 mm LD or 2x slice (extra nodal)
≥15 mm Short Axis Diameter (nodal)
» Lymph Nodes Must be >10 mm to be considered pathological
Must be ≥ 15 mm to be measureable
11

Evaluation Process
» Baseline – establish initial tumor burden, comparator of subsequent time points Target Lesions – Sum of Longest Diameters (SLD)
Non-Target Lesions – document all other disease
» Post-Baseline Target
− Sum Diameters
− Compare to BSL/Prev TPs, Establish nadir
Non-Target – evaluate for substantial change
New – Review for presence
8

RECIST Response Criteria
» CR – Complete Response Disappearance all extra nodal lesions, nodal ≤ 10 mm
» PR – Partial Response 30% reduction in Tumor Burden
» SD – Stable Disease Neither response (CR/PR) or progression (PD)
» PD – Progressive Disease Target-PD – SoD ≥ 20% and ≥ 5 mm from nadir
Non-Target-PD – unequivocal progression
Presence of new lesion
7

RECIST Data
» Generally utilized in PII/PIII Solid Tumor Trials
» Adheres to clearly defined assessment criteria
» Accepts images from different modalities
» Focused on a set of key endpoints
» Both quantitative and qualitative data
» Data must be evaluated and derived at a given timepoint and across all timepoints collected to date
» Study-specific requirements may alter parts of the core algorithm
15 4/3/2013 © 2011 C3i, Inc. Confidential and Proprietary to C3i, Inc.

Data Management Considerations
»RECIST version challenges
»Site vs. Central Review data
»Central Review
16

RECIST Version Challenges
» Migrating to v. 1.1
» Maintaining v.1.0 and v. 1.1 studies
» Target lesions Total number
Number per organ
» Lymph nodes
» Sum of Diameters
» Non-target progression
» New Lesions
17

RECIST Version Impact
»CRF Design
»Derivation procedures
»Edit checks
»Data quality reviews
»Emphasis on training and quality control
»Focus on non-target progression and new lesions
18

Site vs. Central Review
» Comparison of endpoint results
» Concordance noted in previous studies
» Correlation not dependent on techniques
» Intra-study comparisons should be established early
» Track throughout study w/ focus on key events Soft-locks/data safety monitoring
Prior to locking a site
Prior to final DB lock
19

Site vs. Central Review
» Develop processes to analyze: Previous study data
Consistency of sites with central − Distinguish trends
− Establish “normal discordance” rate
Identify outlier sites
» Outlier sites can be reviewed further Re-training
Imaging technique
CMO reviews
20

Evaluation of Central Review Data
» Monitor BICR discordance and adjudication Win-Loss Adjudication Rates
Intra-Reader Variability
Inter-Reader Variability
» Analyze variability Tumor type
Intervention
» Evaluate metrics between RECIST 1.0 and 1.1 studies
21

Management of Central Review Data
» Establish normal levels of variability and discordance for v. 1.0 and v. 1.1
» Analyze for variables
» Assess for suitability in future studies
» Establish parameters for site and central review data based on RECIST version
22

Conclusions
» Imaging trials introduce new sources of data
» Central review of imaging data generates congruent data sets for a given patient/visit but must be analyzed against local imaging site review
» Management and analysis of data in RECIST trials should consider: Version of RECIST utilized
Site vs. Central review data
Central review performance
Happy to discuss:
Kevin Shea, C3i, Inc.
[email protected] or +1 610-772-5726
23