Embed Size (px)
DESCRIPTION
Citation preview

John Hunter Hospital, Newcastle, Australia. John Hunter Hospital, Newcastle, Australia. Team consists of Team consists of Reeves GEM, Hayes P, Reeves GEM, Hayes P,
Bastian B, Collins N, Quiquerjee L, Jones C, Bastian B, Collins N, Quiquerjee L, Jones C, Eketone M, Nowlan C, Attia J, Thakkinstian A, Eketone M, Nowlan C, Attia J, Thakkinstian A, Clancy R, Major G, Mathers D, Ratnarajah S, Clancy R, Major G, Mathers D, Ratnarajah S,
Glass J, de Malmanche T, Sutherland D, Bagga Glass J, de Malmanche T, Sutherland D, Bagga H, van der Kallen, Gibson P, and Wark PH, van der Kallen, Gibson P, and Wark P
A New PHASE For Pulmonary Hypertension: Pulmonary Hypertension
And Stress Echocardiography Study
PH
AS
E

Patients with autoimmune disease, and in particular limited systemic sclerosis (CREST syndrome), are at risk of developing pulmonary artery hypertension (PAH) which is associated with a poor prognosis. With improvements in therapy offering improved survival and improved functional capacity, there has been an emphasis on screening to identify patients at risk. Assessment of patients during exercise may enable early identification of patients with this condition.
AimsWe aimed to assess the ability of exercise stress echocardiography to evaluate the change in pulmonary artery pressure in 197 patients with autoimmune disease (Systemic lupus erythematosus (SLE), limited systemic sclerosis (LSS or “CREST”) and diffuse systemic sclerosis (DSS)). Subsequently, 12-month follow-up pressures (pre- and post-exercise) were recorded for a subset of 51 of these individuals to observe the natural history and evolution of PAH.
Methods
Systolic pulmonary artery pressure (sPAP) was estimated using interrogation of the tricuspid incompetence jet before and after exercise. PAH was classified as normal, mild, moderate or severe using echocardiographic assessment of sPAP.
Results
Of the initial 197 patients who underwent SE, 172 (87.3%) had SLE, with 16 (8.1%) having LSS and 9 (4.6%) diagnosed with DSS. Pulmonary pressures rose or remained unchanged in all screened individuals, with a mean rise during stress of 13.8 mmHg (+/- 6.8). Pulmonary artery pressure rose significantly in each of the three subgroups (p < 0.05). Stress echocardiography demonstrated PAH (using a cut-off of >35mmHg) in 80% of all individuals with systemic autoimmunity (mean sPAP 45.6 mmHg 7.2). Using established criteria for severe PAH (sPAP > 55mmHg), this represented a prevalence of 17 / 197 (8.6%). Follow-up SE testing was performed at twelve months in a total of 51 patients, with 30 (58.8%), 10 (19.6 %) and 9 (17.6%) suffering from SLE, LSS, and DSS, respectively. sPAP rose significantly over this time period in 41/51 (80%) patients, and significant pressure rises were measured in all disease subgroups, with an overall rise of 7 mmHg. A significant proportion of patients with normal baseline pressures made the transition to PAH over twelve months (8/51, or 16%), and over the same period 5 (9.8%) moved from mild (< 55mmHg) to severe PAH.
Conclusion
Stress echocardiography is a useful tool in identifying individuals with autoimmune disease who may have underlying pulmonary arterial disease that may be amenable to therapy. We noted a consistent elevation in sPAP across all autoimmune subtypes, suggesting an abnormal pulmonary vascular response to exercise exists in these patients.
Ab
stra
ct

Patients with autoimmune disease, and in particular limited systemic sclerosis (CREST syndrome), are at risk of developing pulmonary artery hypertension (PAH) which is associated with a poor prognosis. With improvements in therapy offering improved survival and improved functional capacity, there has been an emphasis on screening to identify patients at risk. Assessment of patients during exercise may enable early identification of patients with this condition.
The Pulmonary Hypertension Assessment and Screening Evaluation (PHASE-I) study had the following aims: 1. Explore the prevalence of pulmonary
hypertension in individuals with systemic autoimmunity using stress echocardiography as a screening tool.
2. Address whether the heightened risk of PAH is confined to scleroderma variants,
3. Correlate simple clinical markers of exercise capacity with pulmonary haemodynamics during exercise
4. Assess PAH changes over twelve months follow-up
Bac
kgro
un
d &
A
ims

260 subjects were selected randomly from the Hunter Scleroderma-Lupus Autoimmune Resource Centre (SLARC) database, diagnosed with diffuse systemic sclerosis (DSS), limited systemic sclerosis (LSS, also known as CREST), or lupus (SLE), according to ARA criteria.
197 subjects were able to attend for initial stress echocardiographic (SE) screening, and a subgroup of 54 returned for a second SE assessment. Patients were asked to complete the Borg dyspnoea index (BDI), World Health Organisation functional class (WHO) assessments, a standardised “six-minute walk test” (6MWT), and exercise oximetry (oximetry readings recorded at rest (Ox0) and after 6MWT (Ox6)) before proceeding on to formal pulmonary function testing (PFT) including carbon dioxide diffusing capacity (DLCO). Individuals with total lung capacity (TLC) < 60% of predicted were not included for further assessment.
Medians and inter-quartile ranges for post-exercise PAP’s were compared graphically (box-and-whiskers charts) and statistically (Wilcoxon-Mann-Whitney test, with p value < 0.05 regarded as significant).
Met
ho
ds

In the first phase of the study, 197 patients were screened for PAH using SE. The mean age was 55.6 (SD=12.5) years and 99% of subjects were females. SLE was the commonest diagnosis (172 out of 197, or 87.3%), followed by LSS (16/197, 8.1%) and DSS (9/197, 4.6%) (Fig 1).
Res
ult
s -
I
Fig 1:Disease Subgroups in Initial Cohort (197 Patients)
87%
8%5%
DSS
LSS
SLE

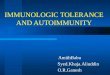
Pulmonary pressures rose or remained unchanged in all screened individuals, with an overall mean rise during stress of 13.8 mmHg ± 6.8. The mean PAP rises for SLE, LSS, and DSS were 14.0 (± 6.7), 14.4 (± 9.5), and 9.7 ( ± 3.6). These mean PAPs were not significantly different between groups (p = 0.42). Stress echocardiography demonstrated PAH (using a cut-off of >35mmHg) in 80% of all individuals with systemic autoimmunity (mean sPAP 45.6 mmHg 7.2). Exercise resulted in a large proportion (121/157, or 77%) of individuals with normal resting PAP reaching the diagnostic threshold (PAPPOST > 35 mmHg) for the diagnosis of PAH. Using established criteria for severe PAH (sPAP > 55mmHg), the prevalence of PAH was 17 / 197 (8.6%), and 29% of these patients (5 / 17) would not have been detected without the stress component of SE.
At twelve months, fifty-one patients undertook a further SE assessment. The mean age was 57.4 (SD=12.5) years, with 96% of subjects being females. In this group, 32 (62.7%), 10 (19.6 %) and 9 (17.6%) suffered from SLE, LSS, and DSS, respectively (Table 1). Fig. 2 demonstrates the presence of aberrant elevation in systolic pulmonary artery pressure with exercise in our study population.
Res
ult
s -
IIF
ig 2
: sP
AP
Ch
ang
e w
ith
E
xerc
ise

Tab
le 1
: B
asel
ine
Fea
ture
s

Odds ratios of having PAH for SLE and LSS patients (respectively) compared with those with DSS were 0.83 (95% CI: 0.18 – 3.96) and 0.33 (95% CI: 0.05 – 2.18) (Table 2)
Res
ult
s -
II
Logistic regression analysis was performed to determine relationships between explanatory variables and PAH. First, univariate analysis was performed for PAH against each explanatory variable in isolation. Variables with p-values < 0.2 or OR 2 (which were BDI, WHO, 6MWT and Raynaud’s) were then simultaneously included into the logistic model. The model’s adequacy was tested for goodness-of-fit using the Pearson method (Pearson chi-square = 41.74, df = 33, p = 0.14). A similar iterative process was employed for PAP.
None of the effect tests reached significance, implying
that the information gleaned from SE testing could not be predicted using baseline clinical variables, and therefore offered new information: however, small study numbers and limited power create the possibility of Type II error.
Tab
le 2
: P
AH
by
Au
toim
mu
ne
Su
bty
pes

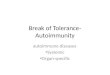
Over the 12 month period of followup, PAPs rose
significantly for all disease subsets. A significant proportion of patients with normal baseline pressures made the transition to PAH over twelve months (8/51, or 16%), and over the same period 5 (9.8%) moved from mild (35 - 55mmHg) to severe PAH.
Fig
3 &
4:
PA
H b
y D
isea
se,
and
(4)
Ove
r T
wel
ve
Mo
nth
s

Patient screening using the SLARC database revealed a high prevalence of exercise induced pulmonary vascular hypertension in this group of patients with systemic autoimmune conditions, with pulmonary pressures rising in all screened individuals.
SE-demonstrated PAH was seen in 80% of all 197 individuals with systemic autoimmunity (using a cut-off of >35 mmHg), affecting 88.9% of DSS, 62.5% of LSS, and 80.8% of patients with SLE.
Using established criteria for severe PAH (PAP > 55 mmHg), this represents a prevalence of 11%, 6% and 9%, respectively.
There was no correlation between PAH and dyspnoea-symptom scores. Despite 75% of the study population falling into low WHO classes (I, II), mild PAH was seen in over 80%.
This study found that the prevalence of PAH is elevated not only in patients with scleroderma, but also in SLE.
This study did not find any correlation of Raynaud's phenomenon or DLCO with either exercise induced PAP elevation or PAH.
Among patients followed up over one year all subgroups demonstrated rises in PAP
In conclusion, SE-defined PAH is common in systemic autoimmune conditions, including, but not confined to, scleroderma. Case-finding through SE-based screening of individuals with systemic autoimmunity may represent an important tool for identification of early PAH, with patient databases representing a powerful diagnostic and research resource.
Su
mm
ary
&
Co
ncl
usi
on
s