Embed Size (px)
Citation preview

Sudden Cardiac Death inAdolescents
Stefanie R. Ellison, MD
KEYWORDS
� Sudden death � Cardiac death � Electrical cardiac abnormalities� Postoperative cardiac abnormalities � Syncope � Long QT syndrome� Cardiomyopathy � Adolescent death
KEY POINTS
� Hypertrophic cardiomyopathy is the most common case of sudden cardiac death inadolescents.
� A detailed comprehensive history and physical examination, with a detailed family historyand social history, are essential before participation in sports.
� The most common chief complaint of patients with sudden cardiac arrest is fatigue, near-syncope/lightheadedness, chest pain and then palpitations, in decreasing order offrequency.
� Seizures or seizure-like activity of ventricular tachycardia or ventricular fibrillation maydistract physicians from considering these as warning signs of sudden cardiac death.
INTRODUCTIONIncidence
Sudden cardiac death (SCD) is defined as an abrupt, unexpected death resulting from acardiovascular cause. Sudden is generally defined as death that occurs within 1 hour ofthe onset of symptoms, but can also occur within minutes for adolescents and children.The true incidence of adolescent SCD is unknown. Studies have determined the inci-dence to be 0.8 to 6.2 cases per 100,000 population per year.1–6 Resuscitation that re-stores spontaneous circulation defines aborted sudden death. Actual resuscitatedadolescentSCDdataare evenmoredifficult to obtainbecausedatabases are inaccurateand based on diagnosis and diagnostic codes. The US Centers for Disease Control andPrevention has estimated that 2000 patients 25 years of age and younger die from SCDeachyear.7Current studies havealsodemonstrated that the incidenceofSCD inchildrenand adolescents is on the rise.8–10 In fact, SCDoccursmore often in children andadoles-cents than infants because athletic participation increases the risk of SCD for thosewithunderlying cardiovascular disease. Up to 25% of these deaths occur during sports.11
Department of Emergency Medicine, Truman Medical Center, University of Missouri-KansasCity, 2411 Holmes Street, Kansas City, MO 64108-2792, USAE-mail address: [email protected]
Prim Care Clin Office Pract 42 (2015) 57–76http://dx.doi.org/10.1016/j.pop.2014.09.012 primarycare.theclinics.com0095-4543/15/$ – see front matter � 2015 Elsevier Inc. All rights reserved.

Ellison58
A study of high school and college athletes in the United States demonstrated thatSCD occurs in fewer than 1 in 100,000 students.11,12 Studies have further shown thatsports participation in adolescents and young adults is attributable to underlyingcardiac disorders compared with age-related, nonathletic populations.12 More than50% of athletic deaths owing to SCD occur in black athletes. It is also more commonin young male athletes, occurring in a ratio of 1 to 9.13 This may be in part that the mostcommon sports with the occurrence of SCD are football and basketball and femaleparticipation in football differs greatly from that of the male gender.13–15
Patient Evaluation Overview and Pathophysiology
The known underlying cardiac disorders associated with adolescent SCD (Box 1) canbe broken down into 3 categories: (1) Structural/functional, (2) primary electrical
Box 1
Cardiac disorders predisposing adolescents to sudden cardiac death
Structural/functional (in decreasing order of frequency)
Hypertrophic cardiomyopathya
Coronary artery abnormalities
Myocarditis
Arrhythmogenic channelopathies/right ventricular cardiomyopathya
Aortic rupture/Marfan syndromea
Pulmonary hypertension
Dilated cardiomyopathy or restrictive cardiomyopathya
Left ventricular outflow tract obstruction
Postoperative congenital heart diseaseb
Primary electrical abnormalities
Long QT syndromea: Romano Ward, Jervell Lange Nielsen, Acquired
Brugada syndromea
Wolff-Parkinson–White syndrome
Primary or idiopathic ventricular tachycardia/fibrillation
Catecholamine-exercise ventricular tachycardiaa
Heart block-congenital, acquired
Short QT syndromea
Acquired
Commotio cordis
Drugs of abuse—cocaine, stimulants, inhalants, gasoline, glue, nitrites, emetine
Primary pulmonary hypertensiona
Secondary pulmonary hypertension
Atherosclerotic coronary artery disease
a Familial/genetic.b Postoperative congenital heart diseases include tetralogy of Fallot, transposition with
transportation of the great arteries, Fontan operation, hypoplastic left heart syndrome, coarc-tation of the aorta, cardiac transplantation.

Sudden Cardiac Death in Adolescents 59
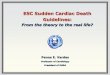
abnormalities, and (3) acquired. Fig. 1 provides a distribution of the most commoncardiac causes of SCD in adolescent athletes.
CARDIAC DISORDERS PREDISPOSING ADOLESCENTS TO SUDDEN CARDIAC DEATH
This section focuses on the most common causes and mechanisms of SCD.
Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy (HCM) affects more than 500,000 people in the UnitedStates and is the most common cause of SCD in adolescents.14,16 Children under 12make up less than 10% of all patients who have this disorder. The Pediatric Cardiomy-opathy Registry reports that HCM occurs at a rate of 5 per 1 million children. HCM isamong the most common inherited cardiac disorders affecting around 1 in 500 peopleand is the number 1 cause of SCD in young athletes.13–16 It is a heterogeneous disor-der, produced by mutations in multiple genes coding for sarcomeric proteins. Inheri-tance is primarily autosomal dominant, with variable penetrance. The annual mortalityowing to HCM is estimated at around 1% to 2 %.16
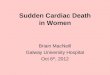
HCM occurs when the muscle fibers of the heart are thickened and do not allow theheart to relax sufficiently for the heart to fill (Fig. 2). With the combination of poor fillingand contractility owing to the stiff nature of the thickened muscles, the patient’s heartmay not pump adequate blood, especially during exercise. Any of the chambers canbecome hypertrophic, but it occurs more frequently in the left ventricle. HCM is alsocharacterized by asymmetric septal hypertrophy with a disarray of ventricular musclefibers, adding to the risk of arrhythmias, even in patients without hypertrophy. It should
Fig. 1. Distribution of cardiovascular causes of sudden death in 1435 young competitiveathletes. From the Minneapolis Heart Institute Foundation Registry, 1980 to 2005. ARVC,arrhythmogenic right ventricular cardiomyopathy; AS, aortic stenosis; CAD, coronary arterydisease; C-M, cardiomyopathy; HD, heart disease; LAD, left anterior descending; LVH, leftventricular hypertrophy; MVP, mitral valve prolapse. (From Maron BJ, Thompson PD, Acker-man MJ, et al. Recommendations and considerations related to preparticipation screeningfor cardiovascular abnormalities in competitive athletes: 2007 update: a scientific statementfrom the American Heart Association Council on Nutrition, Physical Activity, and Meta-bolism: endorsed by the American College of Cardiology Foundation. Circulation2007;115:1645; with permission.)

Fig. 2. Normal heart versus hypertrophic cardiomyopathy anatomy. (From Barnes-JewishHospital. Hypertrophic Cardiomyopathy. Available at: http://www.barnesjewish.org/heart-vascular/hypertrophic-cardiomyopathy. Accessed March 10, 2014.)
Ellison60
also be noted that patients with HCM can have normal chest x-rays because the thick-ening may only occur in the septum. When the thickening includes the septum of theleft ventricular outflow tract, then obstruction during systole can lead to hypertrophicobstructive cardiomyopathy. Only 25% of patients with HCM actually develop hyper-trophic obstructive cardiomyopathy.16,17
The hypertrophic cardiomyopathy electrocardiogramThe chief abnormality associated with HCM is left ventricular hypertrophy and thedegree and distribution of left ventricular hypertrophy is variable ranging from mild(13–15 mm) to severe myocardial thickening (30–60 mm).18 The most commonlyobserved pattern comes from the asymmetrical thickening of the anterior interventric-ular septum. See Fig. 3 for electrocardiographic (ECG) features.
Diagnostic electrocardiographic criteria for hypertrophic cardiomyopathy� Left ventricular hypertrophy is shown by increased precordial voltages andnonspecific ST segment and T-wave changes.
� Asymmetrical septal hypertrophy produces deep, narrow “dagger-like” Q wavesin the lateral (V5-6, I, aVL) and inferior (II, III, aVF) leads. Lateral Q waves are morecommon than inferior Q waves in HCM compared with prior myocardialinfarction.
� Left atrial enlargement, or “P mitrale”, on the ECG.
For 2 additional ECG demonstrations on patients with HCM, please view thefollowing YouTube links detailing the diagnostic criteria by Professor Sanjay Sharma,Consultant Cardiologist in the CYR Center for Inherited Cardiac Diseases:
http://www.youtube.com/watch?v5pEHAotWgePYhttp://www.youtube.com/watch?v5RULjhr4SEjs#t568

Fig. 3. Asymmetrical septal hypertrophy produces “dagger-like Q waves” in the lateral andinferior leads. (From Life in the Fast Lane. Hypertrophic Cardiomyopathy (HCM). Availableat: http://lifeinthefastlane.com/ecg-library/hcm/. Life in the Fast Lane is licensed under a Cre-ative Commons ShareAlike 4.0 International User’s License http://creativecommons.org/licenses/by-sa/4.0/.)
Sudden Cardiac Death in Adolescents 61
Apical hypertrophic cardiomyopathy electrocardiogramApical HCM is less common but still important to diagnose in the screening of ath-letes.17,18 There is localized hypertrophy in the left ventricular apex with classicECG finding as demonstrated in Fig. 4.
Fig. 4. Apical hypertrophic cardiomyopathy. (From Life in the Fast Lane. Hypertrophic Car-diomyopathy (HCM). Available at: http://lifeinthefastlane.com/ecg-library/hcm/. Life in theFast Lane is licensed under a Creative Commons ShareAlike 4.0 International User’s Licensehttp://creativecommons.org/licenses/by-sa/4.0/.)

Ellison62
Diagnostic electrocardiographic criteria for Apical Hypertrophic Cardiomyopathy� High precordial voltages.� Giant T-wave inversions in the precordial and high lateral leads.
There is an excellent video of a case report of HCM by Amal Mattu of a patient whopresented with syncope: http://www.youtube.com/watch?v5RsNkhr4lhhU.
Coronary Artery Anomalies
Coronary artery anomalies are the secondmost common cause of SCD in adolescentsin the United States.19 The anomaly most often associated with SCD is the left coro-nary artery originating from the right sinus of Valsalva.19–21 The artery then traversesbetween the aorta and pulmonary artery and when a patient exercises, the greatvessels both increase in size and compress the left main coronary artery, causingischemia (Fig. 5). These are difficult to identify with routine echocardiograms andcan require imaging studies or angiography to diagnose. Symptoms include earlyfatigue, angina, or exercise-induced syncope and should direct the clinician to referthe patient for consultation and further studies.
Primary electrical abnormalitiesThere are a variety of primary arrhythmias that are a rare cause of SCD in youngpatients. These include the arrhythmic channelopathies and primary arrhythmiasthat can be determined by ECG. These cases of SCD are often preceded by recurrentsyncope, which can trigger the workup before the arrhythmia gets more malignant.Fig. 6 and Table 1 pair the primary arrhythmia, the features, an example of the diag-nostic ECG, and the treatment for long QT syndrome (LQTS), Brugada syndrome,
Fig. 5. Left coronary anomaly originating in the contralateral sinus. LCA, left coronary ar-tery; RCA, right coronary artery. (From Barriales-Villa R, Morıs de la Tassa C. Anomalıas con-genitas de las arterias coronarias con origen en el seno de Valsalva contralateral: ¿queactitud se debe seguir? [Congenital coronary artery anomalies with origin in the contralat-eral sinus of Valsalva: which approach should we take?]. Rev Esp Cardiol 2006;59(4):365 [inSpanish]; with permission.)

Fig. 6. Electrocardiographs of primary electrical abnormalities. (A) LongQTsyndrome. (B) Bru-gada syndrome. (C) Wolff–Parkinson–White syndrome. (D) Dilated cardiomyopathy ventriculartachycardia/fibrillation. (E) Catecholamine–exercise ventricular tachycardia. (From [A] Image re-printed with permission from Medscape Reference (http://emedicine.medscape.com/), 2014,available at: http://reference.medscape.com/features/slideshow/syncope; and [B,E] From Lifein the Fast Lane. Dilated Cardiomyopathy. Available at: http://lifeinthefastlane.com/ecg-library/dilated-cardiomyopathy/. Life in the Fast Lane is licensed under a Creative CommonsShareAlike 4.0 International User’s License http://creativecommons.org/licenses/by-sa/4.0.)
Sudden Cardiac Death in Adolescents 63
Wolff–Parkinson–White syndrome, and dilated cardiomyopathy, ventricular tachy-cardia, and catecholamine exercise ventricular tachycardia.22–26
Long QT syndromeLQTS is a genetic disorder that occurs in 1 in 2500 to 3000 individuals.25 At least 10genes have been associated with LQTS. Mutations in the genes responsible for potas-sium, sodium, and calcium channels in cardiac muscle have all been implicated incongenital LQTS. Congenital forms of LQTS include Romano–Ward, Jervell–Lange–Nielsen, Andersen, and Timothy syndromes. These are a variety of genetic abnormal-ities in the ion channels that make up an estimated 80% of patients with LQTS.26,27
Many patients with LQTS have a QTc that is within the normal range, making the diag-nosis difficult.28 Obtaining a history of syncope, a family history of LQTS, or SCDshould prompt the clinician to obtain an ECG. It is also helpful to know themedicationsthat cause QT prolongation and put these patients at risk for arrhythmias (Box 2).

Fig. 6. (continued)
Ellison64

Table 1Primary electrical abnormalities: features, electrocardiogram, and treatment
Primary ElectricalAbnormalities Features ECG Treatment
LQTS22–24: RomanoWard, JervellLange Nielsen,acquired
Familial genetic disorderIon channel mutationsPresents in Torsades de pointesRomano Ward is MC inherited LQTSJervell-Lange has congenital deafness
See Fig. 6A21Prolonged QT measures from the onset of the Q wave to
the end of the T wave in Lead IIVaries with heart rate but >0.44 in men, >0.46 in children
and women for HR 50–90/min is prolongedTorsades de pointes can occurCan deteriorate from polymorphic ventricular tachycardia
to ventricular fibrillation
b-Blocker therapyRecommendations on
exercise intensity bya cardiologist
ICD if b-blockers fail
Brugada25
syndromeInherited autosomal dominant arrhythmogenic
syndrome characterized by life-threateningventricular arrhythmias
Genetic mutations are the cause
See Fig. 6BECG abnormalities are from repolarization and
depolarization abnormalitiesST segment coved elevations in the right precordial leadsJ wave amplitude �2 mm followed by a negative T-wave
Placement of ICD
Wolff-ParkinsonWhite26
Owing to �1 more reentrant pathways inducingSVT or atrial fibrillation
Up to 14% associated with malignant tachycardiasMalignant arrhythmias from short reentrant
pathway repolarization or multiple pathways
See Fig. 6CShort PR intervalDelta waves present
Undergo EPT andablation
Dilatedcardiomyopathyventriculartachycardia/fibrillation27
Cardiac dilation and systolic dysfunctionInherited or acquiredLamin AC gene mutations a common cause of
DCM and SCD
See Fig. 6DMarked LVHPoor R wave progressionLeft atrial enlargementRight axis deviation
Permanent pacemakerand ICD placement
Catecholamine-exerciseventriculartachycardia28
Ventricular ectopy induced by exercise oremotional stress
Mutation in gene that encodes Ca-mediatedsarcoplasmic fibers
Lethal in 30%–50% if left untreated
Pre-exercise ECG is usually normal, stress testingrecommended
ECG with exercise (see Fig. 6E)Nonsustained wide ventricular tachycardia
b-Blocker therapyRecommendations on
exercise intensity bya cardiologist
ICD if b-blockers fail
Abbreviations: DCM, dilated cardiomyopathy; ECG, electrocardiograph; EPT, electrophysiologic testing; HR, heart rate; ICD, implantable cardioverter defibrillator;LQTS, long QT syndrome; LVH, left ventricular hypertrophy; MC, most common; SCD, sudden cardiac death; SVT, supraventricular tachycardia.
SuddenCardiacDeath
inAdolesce
nts
65

Box 2
Examples of commonly used medications that cause acquired QT prolongation
Antiarrhythmics
Amiodarone (Cordarone)
Disopyramide (Norpace)
Dofetilide (Tikosyn)
Ibutilide (Corvert)
Procainamide (Pronestyl)
Quinidine (Quinaglute)
Sotalol (Betapace)
Antipsychotics
Chlorpromazine (Thorazine)
Clozapine (Clozaril)
Haloperidol (Haldol)
Quetiapine (Seroquel)
Risperidone (Risperdal)
Thioridazine (Mellaril)
Antibiotics
Azithromycin (Zithromax)
Ciprofloxacin (Cipro)
Clarithromycin (Biaxin)
Erythromycin (Erythrocin)
Fluconazole (Diflucan)
Gatifloxacin (Tequin)
Itraconazole (Sporanox)
Ketoconazole (Nizoral)
Levofloxacin (Levaquin)
Moxifloxacin (Avelox)
Ofloxacin (Floxin)
Sparfloxacin (Zagam)
Telithromycin (Ketek)
Trimethoprim-Sulfa (Bactrim)
Antidepressants
Amitriptyline (Elavil)
Citalopram (Celexa)
Desipramine (Pertofrane)
Doxepin (Sinequan)
Fluoxetine (Prozac)
Imipramine (Norfranil)
Nortriptyline (Pamelor)
66 Ellison

Paroxetine (Paxil)
Sertraline (Zoloft)
Venlafaxine (Effexor)
Antiemetics
Ondansetron (Zofran)
Prochlorperazine (Compazine)
Data from Ayad R, Assar M, Simpson L, et al. Causes and management of drug-induced long QTsyndrome. Proc (Bayl Univ Med Cent) 2010;23(3):250–5.
Sudden Cardiac Death in Adolescents 67
Congenital Heart Disease Risk
The incidence of sudden death in patients with congenital heart disease is about100 in 100,000 patient-years, owing to arrhythmic, embolic, or circulatory causes.29
Specifically, tetralogy of Fallot is associated with higher incidence rates of known ven-tricular tachycardia and intra-atrial re-entrant tachycardia and a 0.5% to 6% risk ofSCD.30 Patients who are status post Fontan procedure also have high acquiredarrhythmia rates with an increased incidence of SCD.
DIAGNOSIS AND SCREENING: PREPARTICIPATION HISTORY AND PHYSICALEXAMINATION
A detailed comprehensive history and physical examination, with a detailed family his-tory and social history are essential before participation in sports. Although state lawsvary, the law generally requires that before students may participate in organizedsports that individual physicians must use reasonable care in detecting and identifyingmedical abnormalities that may cause sudden death or serious injury.31 It is importantto screen for a history of near syncope, syncope, chest pain, palpitations, lightheaded-ness, and shortness of breath. It is also important to establish a clear and detailed his-tory of SCD in relatives, premature placement of pacemakers, or internal cardiacdefibrillators to adequately inquire about the risk to your patient. Questionnaires andelectronic medical records may assist this detailed history and guide the primarycare physicians or pediatricians to identify undiagnosed patients with SCD risk. Thereis a 3-generation pedigree family history tool available from the US Surgeon General’sFamily History Initiative at www.hhs.gov/familyhistory.
Warning Signs and Symptoms
Symptoms of dizziness, lightheadedness, chest pain, syncope, palpitations, dyspnea,and a family history of SCD were noted in 25% to 61% of the population studied.Deaths were exercise or exertion related in 8% to 33% of the SCD cases.32,33 In 1study, patients complained most often of recent fatigue (44%), followed by near syn-cope or lightheadednesss (30%), chest pain or palpitations (28%), shortness of breath(23%), syncope (18%), or unexplained seizure (23%).33 Seizures or seizurelike activityof ventricular tachycardia or ventricular fibrillation may distract physicians fromconsidering these warning signs of SCD. Neurologic signs and symptoms may directprimary physicians to refer to neurology over making the appropriate referral to cardi-ology. Episodes of syncope or presyncope are the most common presenting signs oflethal ventricular tachyarrhythmias. Coronary artery abnormalities or aortic dissectionpresent with chest pain. Cardiomyopathies that lead to pulmonary congestion oredema may present as “cardiac wheezing” and be misinterpreted as bronchospasm

Ellison68
or reactive airway disease. To guide the physician, the American Heart Association of-fers a 12-element screening tool for preparticipation screening of competitive athletesthat is considered a complete set of questions (Box 3).34
Table 2 demonstrates the number of patients who had symptoms reported to theirphysicians and the timing before SCD. Of this cohort, preparticipation evaluationswere completed in 61% of children an average of 15.6 months before SCD, and awell-child evaluations were completed in 60% of children an average of 12.6 monthsbefore SCD.35
Physical Examination
A detailed physical examination should always be paired with a thorough history andfamily history, even though it does not commonly yield positive findings. Screening is
Box 3
The 12-Element American Heart Association recommendations for preparticipation
cardiovascular screening of competitive athletes
Medical historya
Personal history
1. Exertional chest pain/discomfort
2. Unexplained syncope/near syncopeb
3. Excessive exertional and unexplained dyspnea/fatigue, associated with exercise
4. Prior recognition of a heart murmur
5. Elevated systemic blood pressure
Family history
6. Premature death (sudden and unexpected, or otherwise) before age 50 years owing to heartdisease, in 1 or more relatives
7. Disability from heart disease in a close relative less than 50 years of age
8. Specific knowledge of certain cardiac conditions in family members: hypertrophic or dilatedcardiomyopathy, long QT syndrome or other ion channelopathies, Marfan syndrome, orclinically important arrhythmias
Physical examination
9. Heart murmurc
10. Femoral pulses to exclude aortic coarctation
11. Physical stigmata of Marfan syndrome
12. Brachial artery blood pressure (sitting position)d
a Parental verification is recommended for high school and middle school athletes.b Judged not to be neurocardiogenic (vasovagal); of particular concern when related to
exertion.c Auscultation should be performed in both supine and standing positions (or with Valsalva
maneuver), specifically to identify murmurs of dynamic left ventricular outflow tractobstruction.
d Preferably taken in both arms.From Maron BJ, Thompson PD, Ackerman MJ, et al. Recommendations and considerations
related to preparticipation screening for cardiovascular abnormalities in competitive athletes:2007 update: a scientific statement from the American Heart Association Council on Nutrition,Physical Activity, and Metabolism: endorsed by the American College of Cardiology Founda-tion. Circulation 2007;115:1652; with permission.

Table 2Reported Symptom Prevalence in Children and Young Adults with Sudden Cardiac Arrest(SCA)
SymptomStudy Populationwith Symptom (%)
SCA Victims withSymptoms BeforeTheir Most RecentPhysician Visit (%)
SymptomOnsetBefore SCA(mo)
Fatigue 44 25 21
Near-syncope/lightheadedness 30 22 30
Chest pain/discomfort 28 20 26
Palpitations 28 17 25
Heart murmur 24 — 89
Shortness of breath 23 20 19
Tire more easily than friends 22 — NA
Syncope 18 14 47
Unexplained seizure activity 13 11 71
Decrease in physical activity 11 — NA
Hypertension 3 — 25
One of the above symptoms 72 51 —
Timing of symptoms related to most recent physician visit and SCA is provided.Abbreviation: NA, not applicable.Adapted from Drezner J, Fudge J, Harman K, et al. Warning symptoms and family history in chil-
dren and young adults with sudden cardiac arrest. J Am Board Fam Med 2012;23(4):408–15.
Sudden Cardiac Death in Adolescents 69
designed to identify or raise suspicion of cardiovascular abnormalities that could leadto sudden death. The key elements of the physical examination are as follows.
� Blood pressure measurement.� A complete cardiovascular examination with attention to heart rate, regularity,murmur, gallop, or rub (the presence of a loud systolic heart murmur shouldcreate suspicion for congenital aortic valve stenosis).
� Peripheral circulation and palpation of all pulses may yield positive findings ofcoarctation of the aorta.
� Signs of Marfan syndrome and the inherent risk of aortic dissection. Refer toBox 3 for the elements of the physical examination recommended by the Amer-ican Heart Association.34–37 Box 4 further characterizes the signs and symptomsof structural causes of SCD.
ACQUIRED CAUSESCommotio Cordis
Commotio cordis is a relatively rare cause of SCD that occurs most often in males un-der the age of 18. It is caused by a direct blow over the heart that is timed just beforethe T-wave peak during a vulnerable phase of repolarization.38 Collapse occurs imme-diately or occurs after a brief period of lightheadedness. The rhythm disturbance isusually ventricular fibrillation. Survival rate is low at around 25% to 35% and onlyowing to bystander cardiopulmonary resuscitation and defibrillation.38 Most reportedcases are due to baseball, so chest protectors have been suggested as a preventativemeasure. Additionally, increased education on cardiopulmonary resuscitation and theuse of automated external defibrillators for the community could also potentiallydecrease SCD from commotion cordis.30

Box 4
Signs and symptoms of underlying structural cardiac causes of sudden cardiac death (SCD)
Hypertrophic cardiomyopathy
Can be asymptomatic
Dyspnea
Angina
Presyncope
Syncope
Exercise intolerance or palpitations
Symptoms of heart failure
Hypertrophic obstructive cardiomyopathy: LV outflow tract obstruction
Chest pain
Palpitations
Syncope
Signs of LV heart failure
Arrhythmogenic right ventricular cardiomyopathy
Palpitations
Lightheadedness
Chest pain
Syncope
Signs of heart failure (rare): Shortness of breath, swelling of the feet and ankles, fatigue
Aortic rupture/Marfan syndrome
A tall, thin build
Long arms, legs, fingers, and toes and flexible joints
Scoliosis
Pectus excavatum and pectus carinatum
Teeth that are overcrowded
Flat feet
Micrognathia
Coronary artery abnormalities
Early fatigue
Chest pain or angina
Atypical chest pain and/or syncope that occurs with exercise
Pulmonary hypertension
Dyspnea on exertion
Fatigue
Dizziness
Syncope
Myocarditis
Chest pain
Ellison70

Arrhythmia
Shortness of breath, at rest or during physical activity
Peripheral edema
Fatigue
Other signs and symptoms you would have with a viral infection, such as a headache, bodyaches, joint pain, fever, a sore throat or diarrhea
Dilated cardiomyopathy or restrictive cardiomyopathy
Fatigue and weakness
Dyspnea on exertion or orthopnea
Reduced ability to exercise
Lightheadedness, dizziness or syncope
Persistent cough or wheezing, especially when lying down
Edema
Ascites
Sudden weight gain
Anorexia
Palpitations
Pallor
Abbreviation: LV, left ventricular.Data from Refs.37–39
Sudden Cardiac Death in Adolescents 71
Drugs of Abuse
Performance-enhancing drugs have been linked to SCD in adolescent athletes. Illicitsubstances such as anabolic steroids, stimulants such as ephedra, and peptide hor-mones have been linked to a range of cardiac arrhythmias in healthy subjects.39
Other drugs of abuse such as cocaine, heroin, marijuana, amphetamines, ecstasy,inhalants, gasoline, glue, and emetine have also been known to cause sudden deathin users.40
Electrocardiogram, Echocardiogram, and Genetic Testing
Recent high-profile athlete deaths and the media have placed a greater emphasis onthe need to screen athletes before participating in competitive athletics. The AmericanCollege of Cardiology states that it is only necessary to provide preparticipation eval-uation of athletes to detect possible cardiovascular abnormalities to prevent SCD.34
The use of ECG in the routine testing of the preparticipation evaluation of athletes isnot currently recommended by the American College of Cardiology and remainscontroversial. In 2004 and 2005, European investigators and the International OlympicCommittee recommended the use of the 12-lead ECG as a strategy for screening ath-letes. ECGs are abnormal in more than 90% of patients with HCM and the ECG iseffective at detecting LQTS and Brugada syndrome.4 It should also be rememberedthat the resting ECG is abnormal owing to the changes in the trained athlete’s heart.In addition, exercise-induced conduction abnormalities such as catecholaminergicventricular tachycardia should undergo stress tests because the resting ECG canbe normal.

Ellison72
Routine testing with ECG is recommended during the initial evaluation of any child oryoung adult with syncope. A cardiac cause for syncope was identified in 22 patients(5%), and was LQTS (n 5 14), arrhythmias (n 5 6), and cardiomyopathies (n 5 2).An abnormal history, physical examination, or ECG identified 21 of the 22 patientswith a cardiac cause of syncope (96% sensitivity; 99% negative predictive value).41,42
If the history and physical examination are typical for neurocardiogenic syncope butthe ECG is normal, further testing generally is not needed.
Echocardiogram
Syncope occurring during exercise is an especially ominous sign and warrants a highindex of suspicion for underlying cardiac disease. If the preparticipation history andphysical examination discovers exertional syncope, the diagnostic workup shouldbe performed in consultation with a cardiologist. The workup should include anECG, echocardiogram, stress ECG, and possibly advanced cardiac imaging to identifyand rule out rare structural abnormalities such as arrhythmogenic right ventricular car-diomyopathy or congenital coronary artery anomalies. In a review of 474 athletes witha history of syncope or near syncope discovered during preparticipation screening,33% with syncope that occurred during exercise were found to have a structural car-diac disease known to cause SCD.43
GENETIC CAUSES OF ADOLESCENT SUDDEN CARDIAC DEATH
As Box 1 demonstrates, there are a significant number of familial and genetic condi-tions that are linked with SCD. There is increasing evidence of genetic mutations inseemingly normal and healthy individuals that are linked to SCD. Specifically, HCMand the cardiac channelopathies are now known to be genetic.26–28 There are nowstudies that justify testing of genetic phenotyping of relatives that have died of SCD.Tester and Ackerman27 reported 17 cases demonstrating genetic evidence forLQTS or for catacholaminergic polymorphic ventricular tachycardia mutations; 9(53%) of these cases had a family history of SCD or syncope documented in themedical record. Genetic testing can also serve as a screening tool; testing of familymembers has revealed an additional 151 undiagnosed or asymptomatic diseasecarriers or 8.9 per family.27,44 Postmortem genetic screening, or the “molecularautopsy,” can also be an important method to identify the cause of SCD and to providescreening for at-risk family members. In postmortem genetic testing in cases ofautopsy-negative sudden unexplained death, more than one third of cases were foundto have a pathologic cardiac ion channel mutation.45–48
PREVENTION AND SCREENING PROGRAMS AND EDUCATION
There is proven benefit in the use of ECGs to screen athletes for cardiac abnormalitiesthat put them at risk of SCD. There has been demonstrated success for screening inathletes in Italy, Israel, Japan, and the United States, so currently the American HeartAssociation and American Association of Pediatrics jointly endorse the use of ECGs inthe initial screening of athletes. Fig. 7 provides an example algorithm for Hypertrophiccardiomyopathy cardiac subspecialty evaluation and management. However, studiesexamining the cost effectiveness of screening programs for athletes that include anECG in screening have demonstrated that they are generally unfavorable owing tothe low prevalence and imperfect screening and diagnostic specificity. The costplaced on society reflects a high use of resources that leads to a large number ofhealthy children be referred for follow-up testing.49

Fig. 7. Hypertrophic cardiomyopathy (HCM) cardiac subspecialty evaluation and manage-ment. ECG, electrocardiograph; ECHO, echocardiography; ETT, exercise tolerance test;H1P, history and physical examination; Hx, history; ICD, implantable cardioverter defibril-lator. (From Leslie L, Cohen J, Newburger J, et al. Costs and benefits of targeted screeningfor causes of sudden cardiac death in children and adolescents. Circulation2012;125(21):2626; with permission.)
Sudden Cardiac Death in Adolescents 73
SUMMARY
SCD in adolescents is devastating but potentially preventable. Consistent prepartici-pation screening by primary care physicians and pediatricians with a focus on ahistory of syncope, exertional chest pain, and a family history of SCD paired with aphysical examination can guide the appropriate testing and referral for high-riskpatients. The cost effectiveness of routine screening ECGs is still under debate. Treat-ment and monitoring for underlying cardiac disease can save lives and recommenda-tions for decreased physical activity may also be necessary.
REFERENCES
1. Corrado D, Basso C, Pavei A, et al. Trends in sudden cardiovascular death inyoung competitive athletes after implementation of a preparticipation screeningprogram. JAMA 2006;296:1593–601 CrossRefMedline.
2. Maron BJ, Doerer JJ, Haas TS, et al. Sudden deaths in young competitiveathletes: analysis of 1866 deaths in the United States, 1980–2006. Circulation2009;119:1085–92.
3. Corrado D, Basso C, Schiavon M, et al. Screening for hypertrophic cardiomyop-athy in young athletes. N Engl J Med 1998;339(6):364–9.
4. Driscoll DJ, Edwards WD. Sudden unexpected death in children and adoles-cents. J Am Coll Cardiol 1985;5(Suppl 6):118B–21B.
5. Wren C. Sudden death in children and adolescents. Heart 2002;88(4):426–31.6. Neuspiel DR, Kuller LH. Sudden and un-expected natural death in childhood and
adolescence. JAMA 1985;254(10):1321–5.

Ellison74
7. Kung HC, Hoyert DL, Xu J, et al. Deaths: final data for 2005. Natl Vital Stat Rep2008;56(10):1–120.
8. Shen WK, Edwards WD, Hammill SC, et al. Sudden un- expected nontraumaticdeath in 54 young adults: a 30-year population-based study. Am J Cardiol1995;76(3):148–52.
9. SoRelle R. Jump in sudden deaths reported in younger people during pastdecade. Circulation 2001;103(10):e9019–21.
10. Spurgeon D. Sudden cardiac deaths rise 10% in young Americans. BMJ 2001;322(7286):573.
11. O’Connor FG, Kugler JP, Oriscello RG. Sudden death in young athletes:screening for the needle in a haystack. Am Fam Physician 1998;57:2763–70.
12. Corrado D, Basso C, Rizzoli G, et al. Does sports activity enhance the risk ofsudden death in adolescents and young adults? J Am Coll Cardiol 2003;42(11):1959–63.
13. Maron BJ, Carney KP, Lever HM, et al. Relationship of race to sudden cardiacdeath in competitive athletes with hypertrophic cardiomyopathy. J Am CollCardiol 2003;41:974–80.
14. Maron BJ, Shirani J, Poliac LC, et al. Sudden death in young competitive athletes:clinical, demographic, and pathological profiles. JAMA 1996;276:199–204.
15. Van Camp SP, Bloor CM, Mueller FO, et al. Nontraumatic sports death in highschool and college athletes. Med Sci Sports Exerc 1995;27:641–7.
16. Maron BJ. Hypertrophic cardiomyopathy. Lancet 1997;350(9071):127–33.17. Kelly BS, Mattu A, Brady WJ. Hypertrophic cardiomyopathy: electrocardio-
graphic manifestations and other important considerations for the emergencyphysician. Am J Emerg Med 2007;25(1):72–9.
18. Life in the Fastlane. Hypertrophic cardiomyopathy (HCM). Available at: http://lifeinthefastlane.com/ecg-library/hcm/. Accessed March 8, 2014.
19. Corrado D, Thiene G, Cocco P, et al. Non-atherosclerotic coronary artery diseaseand sudden death in the young. Br Heart J 1992;68:601–7.
20. Nakamura CT, Canete DR, Lau JM. A review of the anomalous origin of the leftcoronary artery from the anterior sinus of Valsalva: is prevention possible? HawaiiMed J 1993;52:294–9.
21. Lipsett J, Cohle SD, Berry PJ, et al. Anomalous coronary arteries: a multicenterpediatric autopsy study. Pediatr Pathol 1994;14:287–300.
22. Wilde A, Antzelevitch C, Borggrefe M, et al. Proposed Diagnostic cretieria for theBrugada Syndrome: consensus report. Circulation 2002;106:2514–9. http://dx.doi.org/10.1161/01.CIR.0000034169.45752.4A.
23. Pappone C, Vicedomini G, Manguso F, et al. Risk of malignant arrhythmias ininitially symptomatic patients with Wolff-Parkinson-White syndrome: results of aprospective long-term electrophysiological follow-up study. Circulation 2012;125:661–8.
24. Dadkhah S, Dowlatshahi S, Sharain K, et al. Exercise induced non-sustainedventricular tachycardia and indication for invasive management. Clin MedInsights Cardiol 2011;5:121–6.
25. Schwartz PJ, Stramba-Badiale M, Crotti L, et al. Prevalence of the congenitallong-QT syndrome. Circulation 2009;120:1761–7.
26. Lehnart SE, Ackerman MJ, Benson DW Jr, et al. Inherited arrhythmias: a NationalHeart, Lung, and Blood Institute and Office of Rare Diseases workshopconsensus report about the diagnosis, phenotyping, molecular mechanisms,and therapeutic approaches for primary cardiomyopathies of gene mutationsaffecting ion channel function. Circulation 2007;116(20):2325–45.

Sudden Cardiac Death in Adolescents 75
27. Tester DJ, Ackerman MJ. Postmortem long QT syndrome genetic testing forsudden unexplained death in the young. J Am Coll Cardiol 2007;49(2):240–6.
28. Vincent GM, Timothy KW, Leppert M, et al. The spectrum of symptoms and QTintervals in carriers of the gene for the long-QT syndrome. New Engl J Med1992;327:846–52.
29. Silka MJ, Hardy BG, Menashe VD, et al. A population-based prospective evalu-ation of risk of sudden cardiac death after operation for common congenital heartdefects. J Am Coll Cardiol 1998;32:245–51.
30. Gajewski K, Saul J. Sudden cardiac death in children and adolescents(excluding Sudden Infant Death Syndrome). Ann Pediatr Cardiol 2010;3(2):107–12.
31. MittonMI. Emerging legal issues in sportsmedicine. St John’s L Rev 2002;76:5–86.Available at: http://scholarship.law.stjohns.edu/lawreview/vol76/iss1/2. AccessedMarch 2014.
32. Liberthson RR. Sudden death from cardiac causes in children and young adults.N Engl J Med 1996;334(16):1039–44.
33. Wisten A, Messner T. Symptoms preceding sudden cardiac death in the youngare common but often misinterpreted. Scand Cardiovasc J 2005;39(3):143–9.
34. Maron BJ, Thompson PD, Ackerman MJ, et al. Recommendations and consider-ations related to preparticipation screening for cardiovascular abnormalities incompetitive athletes: 2007 update: a scientific statement from the American HeartAssociation Council on Nutrition, Physical Activity, and Metabolism: endorsed bythe American College of Cardiology Foundation. Circulation 2007;115:1643–55.
35. Drezner J, Fudge J, Harman K, et al. Warning symptoms and family history inchildren and young adults with sudden cardiac arrest. J Am Board Fam Med2012;23(4):408–15.
36. Pelliccia A. Congenital coronary artery anomalies in young patients. Newperspectives for timely identification. J Am Coll Cardiol 2001;37(2):598–600.
37. Maron BJ, Douglas PS, Graham TP, et al. Task Force 1: preparticipationscreening and diagnosis of cardiovascular disease in athletes. J Am Coll Cardiol2005;45:1322–6.
38. Link MS, Wang PJ, Pandian NG, et al. An experimental model of sudden deathdue to low-energy chest-wall impact (commotio cordis). N Engl J Med 1998;338:1805–11.
39. Furlanello F, Bentivegna S, Cappato R, et al. Arrhythmogenic effects of illicitdrugs in athletes. Ital Heart J 2003;4(12):829–37.
40. MontagnanaM, LippiG, FranchiniM, et al. Suddencardiacdeath in youngathletes.Intern Med 2008;47:1–20.
41. Maron BJ, MckennaWJ, Danielson GK. American College of Cardiology/EuropeanSociety of Cardiology clinical expert consensus document on hypertrophic cardio-myopathy. A report of the American College of Cardiology Foundation Task Forceon Clinical Expert Consensus Documents and the European Society of CardiologyCommittee for Practice Guidelines. J Am Coll Cardiol 2003;42:1687–713.
42. Montgomery JV, Harris KM. Relation of electrocardiographic patterns to pheno-typic expression and clinical outcome in hypertrophic cardiomyopathy. Am JCardiol 2005;96:270–5.
43. Ritter S, Tani LY, Etheridge SP, et al. What is the yield of screening echocardiog-raphy in pediatric syncope? Pediatrics 2000;105:E58.
44. Keren A, Syrris P, McKenna WJ. Hypertrophic cardiomyopathy: the genetic deter-minants of clinical disease expression. Nat Clin Pract Cardiovasc Med 2008;5(3):158–68.

Ellison76
45. Colivicchi F, Ammirati F, Santini M. Epidemiology and prognostic implications ofsyncope in young competing athletes. Eur Heart J 2004;25:1749–53.
46. Tan HL, Hofman N, van Langen IM, et al. Sudden unexplained death: heritabilityand diagnostic yield of cardiological and genetic examination in survivingrelatives. Circulation 2005;112(2):207–13.
47. Tester DJ, Spoon DB, Valdivia HH, et al. Targeted mutational analysis of theRyR2-encoded cardiac ryanodine receptor in sudden unexplained death: amolecular autopsy of 49 medical examiner/coroner’s cases. Mayo Clin Proc2004;79:1380–4.
48. Tester DJ, Ackerman MJ. The role of molecular autopsy in unexplained suddencardiac death. Curr Opin Cardiol 2006;21:166–72.
49. Leslie L, Cohen J, Newburger J, et al. The costs and benefits of targetedscreening for causes of sudden cardiac death in children and adolescents.Circulation 2012;125(21):2621–9.